

Exploring the Impact of Nutrition on Non-Alcoholic Fatty Liver Disease Management: Unveiling the Roles of Various Foods, Food Components, and Compounds

 ,
,  ,
,
Abstract
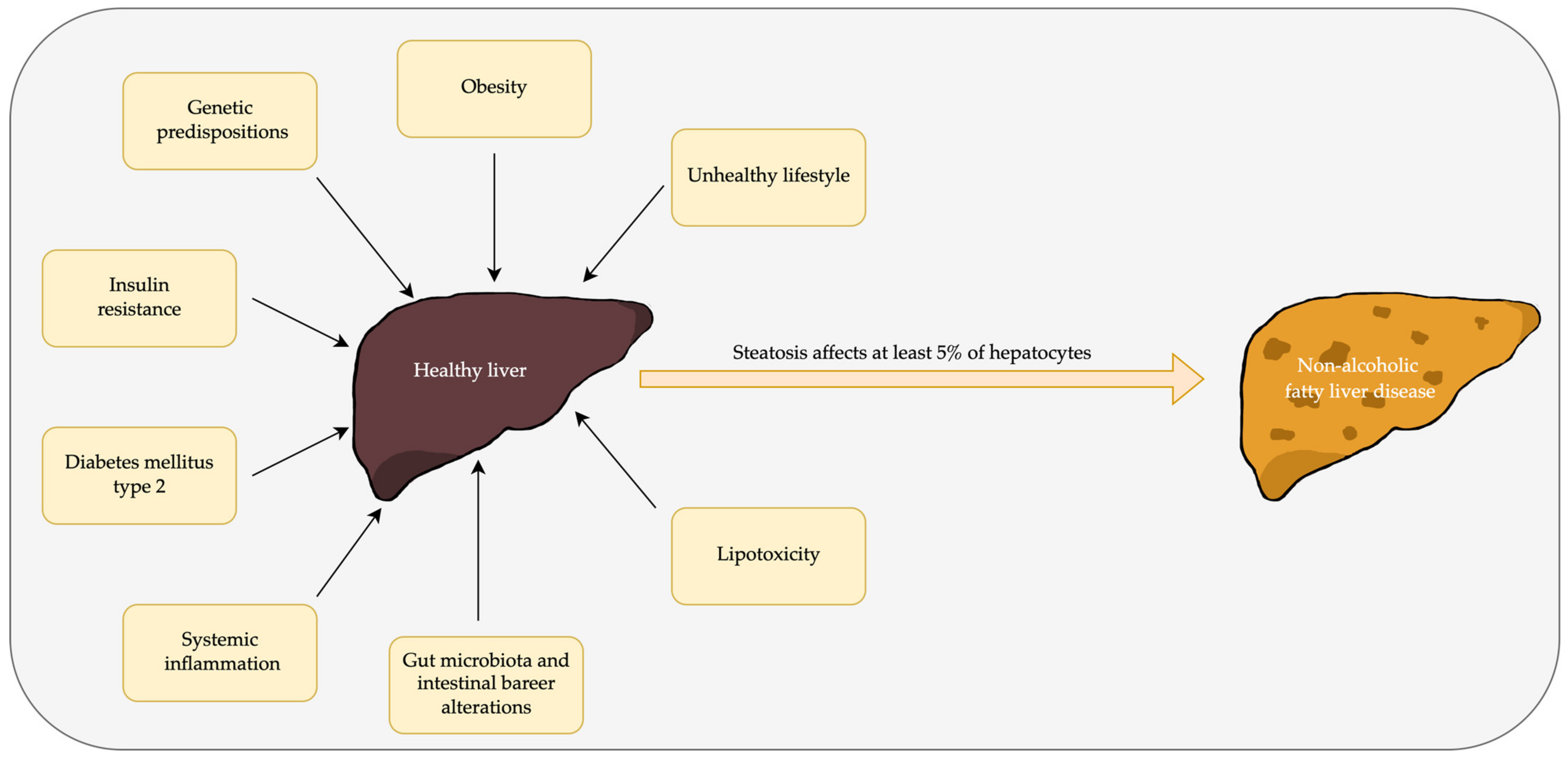
1. Introduction
2. Materials and Methods
2.1. Focal Question
2.2. Language
2.3. Databases
2.4. Study Extraction
2.5. Data Extraction
2.6. Quality Assesment
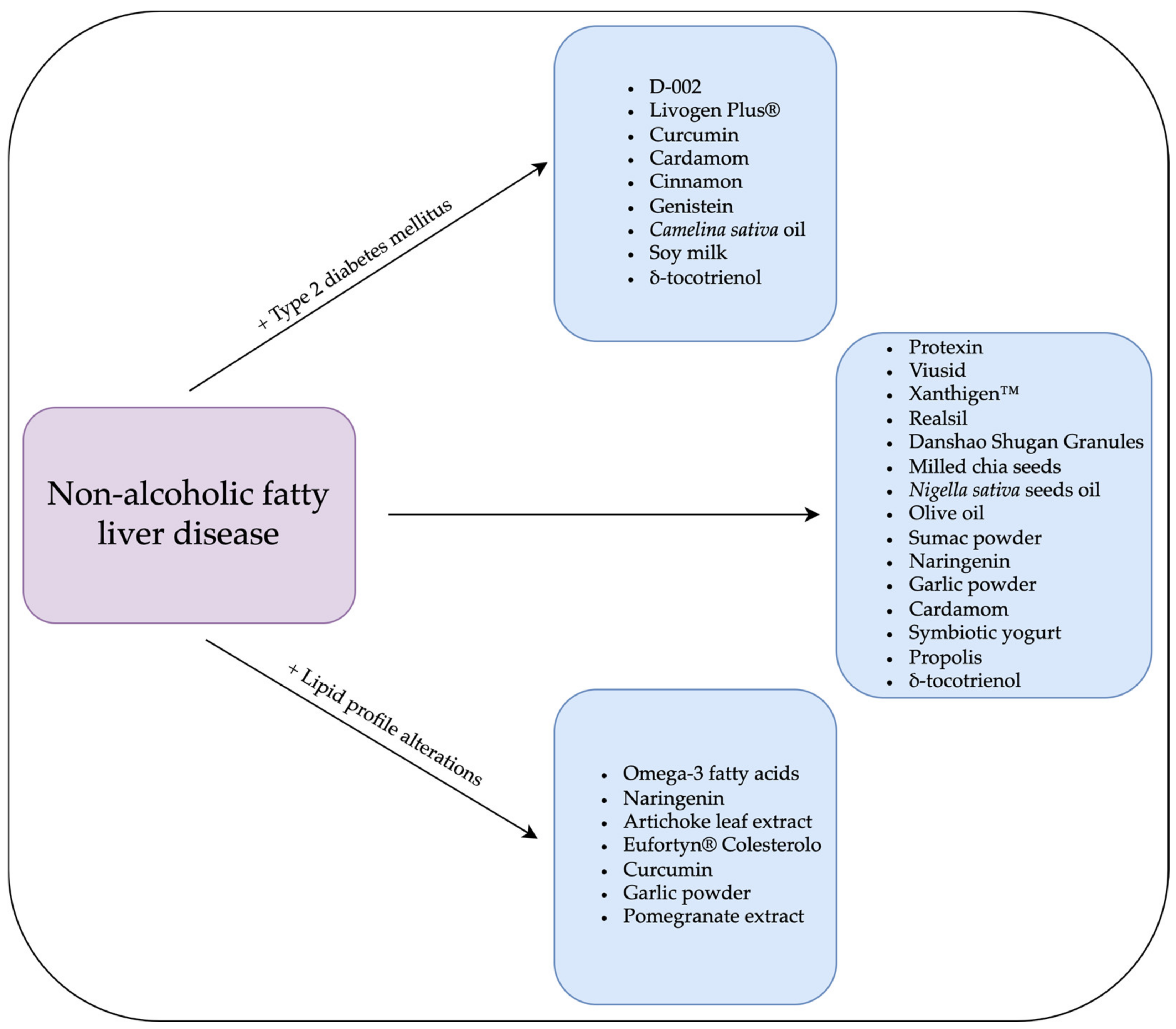
3. A Brief Description of the Substances and Their Usefulness in NAFLD Therapy
3.1. Plants
3.1.1. Silybin
3.1.2. Danshao Shugan Granules (DSSG)
3.1.3. Dihydromyricetin
3.1.4. Anthocyanin
3.1.5. Chia
3.1.6. Zataria Multiflora
3.1.7. Fenugreek
3.1.8. Nigella sativa
3.1.9. Camelina sativa
3.1.10. Garcinia cambogia
3.1.11. Chlorella Vulgaris
3.1.12. Coffee
3.1.13. Green Tea
3.1.14. Genistein
3.1.15. Sesame Oil
3.1.16. Olive Oil
3.1.17. Oat
3.1.18. Pinitol
3.1.19. Sumac
3.1.20. Berberine
3.1.21. Mastiha
3.2. Fruits, Vegetables, Flowers, and Spices
3.2.1. Fruits
Cranberry
Pomegranate
Naringenin
Bergamot Citrus
Cornelian Cherry
3.2.2. Vegetables
Garlic
Purslane
Artichoke
3.2.3. Flowers and Spices
Sour Tea
Magnolia
Cinnamon
Cardamom
Curcumin
3.3. Other
3.3.1. Citrulline
3.3.2. Yogurts
3.3.3. Soy milk
3.3.4. Propolis
3.3.5. Omega Fatty Acids
3.3.6. Vitamins
3.3.7. Food-Based Compositions
4. Probiotics, Prebiotics, and Synbiotics
4.1. Probiotics and Prebiotics
4.2. Synbiotics
5. Limitations of Studies Focused on Food-Derived Treatment Strategies for NAFLD
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Riazi, K.; Azhari, H.; Charette, J.H.; Underwood, F.E.; King, J.A.; Afshar, E.E.; Swain, M.G.; Congly, S.E.; Kaplan, G.G.; Shaheen, A.-A. The Prevalence and Incidence of NAFLD Worldwide: A Systematic Review and Meta-Analysis. Lancet Gastroenterol. Hepatol. 2022, 7, 851–861. [Google Scholar] [CrossRef] [PubMed]
- Haidari, F.; Hojhabrimanesh, A.; Helli, B.; Seyedian, S.-S.; Ahmadi-Angali, K. An Energy-Restricted High-Protein Diet Supplemented with β-Cryptoxanthin Alleviated Oxidative Stress and Inflammation in Nonalcoholic Fatty Liver Disease: A Randomized Controlled Trial. Nutr. Res. 2020, 73, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Abdelbasset, W.K.; Tantawy, S.A.; Kamel, D.M.; Alqahtani, B.A.; Elnegamy, T.E.; Soliman, G.S.; Ibrahim, A.A. Effects of High-Intensity Interval and Moderate-Intensity Continuous Aerobic Exercise on Diabetic Obese Patients with Nonalcoholic Fatty Liver Disease: A Comparative Randomized Controlled Trial. Medicine 2020, 99, e19471. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.; Rhee, H.; Kim, Y.; Lee, M.; Lee, B.-W.; Kang, E.S.; Cha, B.-S.; Choi, J.-Y.; Lee, Y. Ezetimibe Combination Therapy with Statin for Non-Alcoholic Fatty Liver Disease: An Open-Label Randomized Controlled Trial (ESSENTIAL Study). BMC Med. 2022, 20, 93. [Google Scholar] [CrossRef] [PubMed]
- Frankowski, R.; Kobierecki, M.; Wittczak, A.; Różycka-Kosmalska, M.; Pietras, T.; Sipowicz, K.; Kosmalski, M. Type 2 Diabetes Mellitus, Non-Alcoholic Fatty Liver Disease, and Metabolic Repercussions: The Vicious Cycle and Its Interplay with Inflammation. Int. J. Mol. Sci. 2023, 24, 9677. [Google Scholar] [CrossRef]
- Frenette, C.; Kayali, Z.; Mena, E.; Mantry, P.S.; Lucas, K.J.; Neff, G.; Rodriguez, M.; Thuluvath, P.J.; Weinberg, E.; Bhandari, B.R.; et al. Emricasan to Prevent New Decompensation in Patients with NASH-Related Decompensated Cirrhosis. J. Hepatol. 2021, 74, 274–282. [Google Scholar] [CrossRef]
- Kato, T.; Honda, Y.; Kurita, Y.; Iwasaki, A.; Sato, T.; Kessoku, T.; Uchiyama, S.; Ogawa, Y.; Ohkubo, H.; Higurashi, T.; et al. Lubiprostone Improves Intestinal Permeability in Humans, a Novel Therapy for the Leaky Gut: A Prospective Randomized Pilot Study in Healthy Volunteers. PLoS ONE 2017, 12, e0175626. [Google Scholar] [CrossRef]
- Mohamad Nor, M.H.; Ayob, N.; Mokhtar, N.M.; Raja Ali, R.A.; Tan, G.C.; Wong, Z.; Shafiee, N.H.; Wong, Y.P.; Mustangin, M.; Nawawi, K.N.M. The Effect of Probiotics (MCP® BCMC® Strains) on Hepatic Steatosis, Small Intestinal Mucosal Immune Function, and Intestinal Barrier in Patients with Non-Alcoholic Fatty Liver Disease. Nutrients 2021, 13, 3192. [Google Scholar] [CrossRef]
- Song, Q.; Zhang, X. The Role of Gut–Liver Axis in Gut Microbiome Dysbiosis Associated NAFLD and NAFLD-HCC. Biomedicines 2022, 10, 524. [Google Scholar] [CrossRef]
- Buzzetti, E.; Pinzani, M.; Tsochatzis, E.A. The Multiple-Hit Pathogenesis of Non-Alcoholic Fatty Liver Disease (NAFLD). Metabolism 2016, 65, 1038–1048. [Google Scholar] [CrossRef]
- Jegatheesan, P.; Beutheu, S.; Ventura, G.; Nubret, E.; Sarfati, G.; Bergheim, I.; De Bandt, J.-P. Citrulline and Nonessential Amino Acids Prevent Fructose-Induced Nonalcoholic Fatty Liver Disease in Rats. J. Nutr. 2015, 145, 2273–2279. [Google Scholar] [CrossRef]
- Fathi, M.; Alavinejad, P.; Haidari, Z.; Amani, R. The Effects of Zinc Supplementation on Metabolic Profile and Oxidative Stress in Overweight/Obese Patients with Non-Alcoholic Fatty Liver Disease: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Trace Elem. Med. Biol. 2020, 62, 126635. [Google Scholar] [CrossRef]
- Kosmalski, M.; Frankowski, R.; Ziółkowska, S.; Różycka-Kosmalska, M.; Pietras, T. What’s New in the Treatment of Non-Alcoholic Fatty Liver Disease (NAFLD). J. Clin. Med. 2023, 12, 1852. [Google Scholar] [CrossRef]
- Byrne, C.D.; Targher, G. NAFLD as a Driver of Chronic Kidney Disease. J. Hepatol. 2020, 72, 785–801. [Google Scholar] [CrossRef]
- Björkström, K.; Widman, L.; Hagström, H. Risk of Hepatic and Extrahepatic Cancer in NAFLD: A Population-based Cohort Study. Liver Int. 2022, 42, 820–828. [Google Scholar] [CrossRef]
- Caussy, C.; Aubin, A.; Loomba, R. The Relationship Between Type 2 Diabetes, NAFLD, and Cardiovascular Risk. Curr. Diab Rep. 2021, 21, 15. [Google Scholar] [CrossRef]
- Kosmalski, M.; Drzewoski, J.; Szymczak-Pajor, I.; Zieleniak, A.; Mikołajczyk-Solińska, M.; Kasznicki, J.; Śliwińska, A. Irisin Is Related to Non-Alcoholic Fatty Liver Disease (NAFLD). Biomedicines 2022, 10, 2253. [Google Scholar] [CrossRef]
- Calabrese, F.M.; Disciglio, V.; Franco, I.; Sorino, P.; Bonfiglio, C.; Bianco, A.; Campanella, A.; Lippolis, T.; Pesole, P.L.; Polignano, M.; et al. A Low Glycemic Index Mediterranean Diet Combined with Aerobic Physical Activity Rearranges the Gut Microbiota Signature in NAFLD Patients. Nutrients 2022, 14, 1773. [Google Scholar] [CrossRef] [PubMed]
- Francque, S.M.; Marchesini, G.; Kautz, A.; Walmsley, M.; Dorner, R.; Lazarus, J.V.; Zelber-Sagi, S.; Hallsworth, K.; Busetto, L.; Frühbeck, G.; et al. Non-Alcoholic Fatty Liver Disease: A Patient Guideline. JHEP Rep. 2021, 3, 100322. [Google Scholar] [CrossRef] [PubMed]
- Yoneda, M.; Honda, Y.; Ogawa, Y.; Kessoku, T.; Kobayashi, T.; Imajo, K.; Ozaki, A.; Nogami, A.; Taguri, M.; Yamanaka, T.; et al. Comparing the Effects of Tofogliflozin and Pioglitazone in Non-Alcoholic Fatty Liver Disease Patients with Type 2 Diabetes Mellitus (ToPiND Study): A Randomized Prospective Open-Label Controlled Trial. BMJ Open Diab. Res. Care 2021, 9, e001990. [Google Scholar] [CrossRef] [PubMed]
- Phrueksotsai, S.; Pinyopornpanish, K.; Euathrongchit, J.; Leerapun, A.; Phrommintikul, A.; Buranapin, S.; Chattipakorn, N.; Thongsawat, S. The Effects of Dapagliflozin on Hepatic and Visceral Fat in Type 2 Diabetes Patients with Non-alcoholic Fatty Liver Disease. J. Gastroenterol. Hepatol. 2021, 36, 2952–2959. [Google Scholar] [CrossRef] [PubMed]
- Granato, D.; Barba, F.J.; Bursać Kovačević, D.; Lorenzo, J.M.; Cruz, A.G.; Putnik, P. Functional Foods: Product Development, Technological Trends, Efficacy Testing, and Safety. Annu. Rev. Food Sci. Technol. 2020, 11, 93–118. [Google Scholar] [CrossRef] [PubMed]
- Sachdeva, V.; Roy, A.; Bharadvaja, N. Current Prospects of Nutraceuticals: A Review. Curr. Pharm. Biotechnol. 2020, 21, 884–896. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Gazak, R.; Walterova, D.; Kren, V. Silybin and Silymarin—New and Emerging Applications in Medicine. Curr. Med. Chem. 2007, 14, 315–338. [Google Scholar] [CrossRef]
- Tamayo, C.; Diamond, S. Review of Clinical Trials Evaluating Safety and Efficacy of Milk Thistle (Silybum marianum [L.] Gaertn.). Integr. Cancer Ther. 2007, 6, 146–157. [Google Scholar] [CrossRef]
- Disario, A.; Bendia, E.; Taffetani, S.; Omenetti, A.; Candelaresi, C.; Marzioni, M.; Deminicis, S.; Benedetti, A. Hepatoprotective and Antifibrotic Effect of a New Silybin–Phosphatidylcholine–Vitamin E Complex in Rats. Dig. Liver Dis. 2005, 37, 869–876. [Google Scholar] [CrossRef]
- Maghrani, M.; Zeggwagh, N.-A.; Lemhadri, A.; El Amraoui, M.; Michel, J.-B.; Eddouks, M. Study of the Hypoglycaemic Activity of Fraxinus Excelsior and Silybum Marianum in an Animal Model of Type 1 Diabetes Mellitus. J. Ethnopharmacol. 2004, 91, 309–316. [Google Scholar] [CrossRef]
- Loguercio, C.; Andreone, P.; Brisc, C.; Brisc, M.C.; Bugianesi, E.; Chiaramonte, M.; Cursaro, C.; Danila, M.; de Sio, I.; Floreani, A.; et al. Silybin Combined with Phosphatidylcholine and Vitamin E in Patients with Nonalcoholic Fatty Liver Disease: A Randomized Controlled Trial. Free Radic. Biol. Med. 2012, 52, 1658–1665. [Google Scholar] [CrossRef]
- Wah Kheong, C.; Nik Mustapha, N.R.; Mahadeva, S. A Randomized Trial of Silymarin for the Treatment of Nonalcoholic Steatohepatitis. Clin. Gastroenterol. Hepatol. 2017, 15, 1940–1949.e8. [Google Scholar] [CrossRef]
- Wang, H.; Xu, Z.; Wang, Q.; Shu, S. Danshao Shugan Granule Therapy for Non-Alcoholic Fatty Liver Disease. Lipids Health Dis. 2022, 21, 76. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q. Effect of Danshao Huaxian Capsule on Expression of Matrix Metalloproteinase-1 and Tissue Inhibitor of Metalloproteinase-1 in Fibrotic Liver of Rats. World J. Gastroenterol. 2005, 11, 4953. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.-K. Effect of Danshao Huaxian Capsule on Gremlin and Bone Morphogenetic Protein-7 Expression in Hepatic Fibrosis in Rats. World J. Gastroenterol. 2014, 20, 14875. [Google Scholar] [CrossRef]
- Cheng, M.-L.; Lu, T.; Yao, Y.-M.; Geng, X.-X. Danshao Huaxian Capsule in Treatment of Decompensated Cirrhosis Resulting from Chronic Hepatitis B. Hepatobiliary Pancreat. Dis. Int. 2006, 5, 48–51. [Google Scholar]
- Sun, Y.; Liu, S.; Yang, S.; Chen, C.; Yang, Y.; Lin, M.; Liu, C.; Wang, W.; Zhou, X.; Ai, Q.; et al. Mechanism of Dihydromyricetin on Inflammatory Diseases. Front. Pharmacol. 2022, 12, 794563. [Google Scholar] [CrossRef]
- Guo, Z.; Chen, X.; Huang, Z.; Chen, D.; Yu, B.; He, J.; Yan, H.; Zheng, P.; Luo, Y.; Yu, J.; et al. Effect of Dietary Dihydromyricetin Supplementation on Lipid Metabolism, Antioxidant Capacity and Skeletal Muscle Fiber Type Transformation in Mice. Anim. Biotechnol. 2022, 33, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Zhao, X.; Wan, J.; Ran, L.; Qin, Y.; Wang, X.; Gao, Y.; Shu, F.; Zhang, Y.; Liu, P.; et al. Dihydromyricetin Improves Glucose and Lipid Metabolism and Exerts Anti-Inflammatory Effects in Nonalcoholic Fatty Liver Disease: A Randomized Controlled Trial. Pharmacol. Res. 2015, 99, 74–81. [Google Scholar] [CrossRef]
- Zhang, H.; Xu, Z.; Zhao, H.; Wang, X.; Pang, J.; Li, Q.; Yang, Y.; Ling, W. Anthocyanin Supplementation Improves Anti-Oxidative and Anti-Inflammatory Capacity in a Dose–Response Manner in Subjects with Dyslipidemia. Redox Biol. 2020, 32, 101474. [Google Scholar] [CrossRef] [PubMed]
- Bakuradze, T.; Tausend, A.; Galan, J.; Groh, I.A.M.; Berry, D.; Tur, J.A.; Marko, D.; Richling, E. Antioxidative Activity and Health Benefits of Anthocyanin-Rich Fruit Juice in Healthy Volunteers. Free Radic. Res. 2019, 53, 1045–1055. [Google Scholar] [CrossRef]
- Zhang, P.-W.; Chen, F.-X.; Li, D.; Ling, W.-H.; Guo, H.-H. A CONSORT-Compliant, Randomized, Double-Blind, Placebo-Controlled Pilot Trial of Purified Anthocyanin in Patients With Nonalcoholic Fatty Liver Disease. Medicine 2015, 94, e758. [Google Scholar] [CrossRef]
- Alwosais, E.Z.M.; Al-Ozairi, E.; Zafar, T.A.; Alkandari, S. Chia Seed (Salvia hispanica L.) Supplementation to the Diet of Adults with Type 2 Diabetes Improved Systolic Blood Pressure: A Randomized Controlled Trial. Nutr. Health 2021, 27, 181–189. [Google Scholar] [CrossRef]
- Silva Figueiredo, P.; Inada, A.; Ribeiro Fernandes, M.; Granja Arakaki, D.; Freitas, K.; Avellaneda Guimarães, R.; Aragão do Nascimento, V.; Aiko Hiane, P. An Overview of Novel Dietary Supplements and Food Ingredients in Patients with Metabolic Syndrome and Non-Alcoholic Fatty Liver Disease. Molecules 2018, 23, 877. [Google Scholar] [CrossRef] [PubMed]
- Medina-Urrutia, A.; Lopez-Uribe, A.R.; El Hafidi, M.; González-Salazar, M.d.C.; Posadas-Sánchez, R.; Jorge-Galarza, E.; del Valle-Mondragón, L.; Juárez-Rojas, J.G. Chia (Salvia hispanica)-Supplemented Diet Ameliorates Non-Alcoholic Fatty Liver Disease and Its Metabolic Abnormalities in Humans. Lipids Health Dis. 2020, 19, 96. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, A.; Gholamhoseinian, A.; Fallah, H. Zataria multiflora Increases Insulin Sensitivity and PPARγ Gene Expression in High Fructose Fed Insulin Resistant Rats. Iran. J. Basic. Med. Sci. 2014, 17, 263–270. [Google Scholar] [PubMed]
- Sajed, H.; Sahebkar, A.; Iranshahi, M. Zataria multiflora Boiss. (Shirazi Thyme)—An Ancient Condiment with Modern Pharmaceutical Uses. J. Ethnopharmacol. 2013, 145, 686–698. [Google Scholar] [CrossRef] [PubMed]
- Simbar, M.; Azarbad, Z.; Mojab, F.; Alavi Majd, H. A Comparative Study of the Therapeutic Effects of the Zataria multiflora Vaginal Cream and Metronidazole Vaginal Gel on Bacterial Vaginosis. Phytomedicine 2008, 15, 1025–1031. [Google Scholar] [CrossRef]
- Alavinezhad, A.; Ghorani, V.; Rajabi, O.; Boskabady, M.H. Zataria multiflora Affects Clinical Symptoms, Oxidative Stress and Cytokines in Asthmatic Patient: A Randomized, Double Blind, Placebo-Controlled, Phase II Clinical Trial. Cytokine 2020, 133, 155169. [Google Scholar] [CrossRef]
- Zamani, N.; Shams, M.; Nimrouzi, M.; Zarshenas, M.M.; Abolhasani Foroughi, A.; Fallahzadeh Abarghooei, E.; Fattahi, M.R. The Effects of Zataria multiflora Boiss. (Shirazi Thyme) on Nonalcoholic Fatty Liver Disease and Insulin Resistance: A Randomized Double-Blind Placebo-Controlled Clinical Trial. Complement. Ther. Med. 2018, 41, 118–123. [Google Scholar] [CrossRef]
- Abolghasemi, J.; Farboodniay Jahromi, M.A.; Hossein Sharifi, M.; Mazloom, Z.; Hosseini, L.; Zamani, N.; Nimrouzi, M. Effects of Zataria oxymel on Obesity, Insulin Resistance and Lipid Profile: A Randomized, Controlled, Triple-Blind Trial. J. Integr. Med. 2020, 18, 401–408. [Google Scholar] [CrossRef]
- Gong, J.; Fang, K.; Dong, H.; Wang, D.; Hu, M.; Lu, F. Effect of Fenugreek on Hyperglycaemia and Hyperlipidemia in Diabetes and Prediabetes: A Meta-Analysis. J. Ethnopharmacol. 2016, 194, 260–268. [Google Scholar] [CrossRef]
- Nagulapalli Venkata, K.C.; Swaroop, A.; Bagchi, D.; Bishayee, A. A Small Plant with Big Benefits: Fenugreek (Trigonella foenum-graecum Linn.) for Disease Prevention and Health Promotion. Mol. Nutr. Food Res. 2017, 61, 1600950. [Google Scholar] [CrossRef] [PubMed]
- Geberemeskel, G.A.; Debebe, Y.G.; Nguse, N.A. Antidiabetic Effect of Fenugreek Seed Powder Solution (Trigonella foenum-graecum L.) on Hyperlipidemia in Diabetic Patients. J. Diabetes Res. 2019, 2019, 8507453. [Google Scholar] [CrossRef] [PubMed]
- Babaei, A.; Taghavi, S.; Mohammadi, A.; Mahdiyar, M.; Iranpour, P.; Ejtehadi, F.; Mohagheghzadeh, A. Comparison of the Efficacy of Oral Fenugreek Seeds Hydroalcoholic Extract versus Placebo in Nonalcoholic Fatty Liver Disease; a Randomized, Triple-Blind Controlled Pilot Clinical Trial. Indian. J. Pharmacol. 2020, 52, 86. [Google Scholar] [CrossRef] [PubMed]
- Rashidmayvan, M.; Vandyousefi, S.; Barati, M.; Salamat, S.; Ghodrat, S.; Khorasanchi, M.; Jahan-Mihan, A.; Nattagh-Eshtivani, E.; Mohammadshahi, M. The Effect of Nigella Sativa Supplementation on Cardiometabolic Outcomes in Patients with Non-Alcoholic Fatty Liver: A Randomized Double-Blind, Placebo-Controlled Trial. Complement. Ther. Clin. Pract. 2022, 48, 101598. [Google Scholar] [CrossRef]
- Tang, G.; Zhang, L.; Tao, J.; Wei, Z. Effect of Nigella sativa in the Treatment of Nonalcoholic Fatty Liver Disease: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Phytother. Res. 2021, 35, 4183–4193. [Google Scholar] [CrossRef] [PubMed]
- Razmpoosh, E.; Safi, S.; Nadjarzadeh, A.; Fallahzadeh, H.; Abdollahi, N.; Mazaheri, M.; Nazari, M.; Salehi-Abargouei, A. The Effect of Nigella sativa Supplementation on Cardiovascular Risk Factors in Obese and Overweight Women: A Crossover, Double-Blind, Placebo-Controlled Randomized Clinical Trial. Eur. J. Nutr. 2021, 60, 1863–1874. [Google Scholar] [CrossRef]
- Darand, M.; Darabi, Z.; Yari, Z.; Saadati, S.; Hedayati, M.; Khoncheh, A.; Hosseini-Ahangar, B.; Alavian, S.M.; Hekmatdoost, A. Nigella sativa and Inflammatory Biomarkers in Patients with Non-Alcoholic Fatty Liver Disease: Results from a Randomized, Double-Blind, Placebo-Controlled, Clinical Trial. Complement. Ther. Med. 2019, 44, 204–209. [Google Scholar] [CrossRef]
- Khonche, A.; Huseini, H.F.; Gholamian, M.; Mohtashami, R.; Nabati, F.; Kianbakht, S. Standardized Nigella sativa Seed Oil Ameliorates Hepatic Steatosis, Aminotransferase and Lipid Levels in Non-Alcoholic Fatty Liver Disease: A Randomized, Double-Blind and Placebo-Controlled Clinical Trial. J. Ethnopharmacol. 2019, 234, 106–111. [Google Scholar] [CrossRef]
- Hussain, M.; Tunio, A.G.; Akhtar, L.; Shaikh, G.S. Effects of Nigella sativa on Various Parameters in Patients of Non-Alcoholic Fatty Liver Disease. J. Ayub Med. Coll. Abbottabad 2017, 29, 403–407. [Google Scholar]
- Neupane, D.; Lohaus, R.H.; Solomon, J.K.Q.; Cushman, J.C. Realizing the Potential of Camelina sativa as a Bioenergy Crop for a Changing Global Climate. Plants 2022, 11, 772. [Google Scholar] [CrossRef]
- Karvonen, H.M.; Aro, A.; Tapola, N.S.; Salminen, I.; Uusitupa, M.I.J.; Sarkkinen, E.S. Effect of [Alpha ]-Linolenic Acid[Ndash ]Rich Camelina sativa Oil on Serum Fatty Acid Composition and Serum Lipids in Hypercholesterolemic Subjects. Metabolism 2002, 51, 1253–1260. [Google Scholar] [CrossRef] [PubMed]
- de Mello, V.D.; Dahlman, I.; Lankinen, M.; Kurl, S.; Pitkänen, L.; Laaksonen, D.E.; Schwab, U.S.; Erkkilä, A.T. The Effect of Different Sources of Fish and Camelina sativa Oil on Immune Cell and Adipose Tissue MRNA Expression in Subjects with Abnormal Fasting Glucose Metabolism: A Randomized Controlled Trial. Nutr. Diabetes 2019, 9, 1. [Google Scholar] [CrossRef]
- Erkkilä, A.T.; Manninen, S.; Fredrikson, L.; Bhalke, M.; Holopainen, M.; Ruuth, M.; Lankinen, M.; Käkelä, R.; Öörni, K.; Schwab, U.S. Lipidomic Changes of LDL after Consumption of Camelina sativa Oil, Fatty Fish and Lean Fish in Subjects with Impaired Glucose Metabolism—A Randomized Controlled Trial. J. Clin. Lipidol. 2021, 15, 743–751. [Google Scholar] [CrossRef] [PubMed]
- Musazadeh, V.; Dehghan, P.; Saleh-Ghadimi, S.; Abbasalizad Farhangi, M. Omega 3-rich Camelina sativa Oil in the Context of a Weight Loss Program Improves Glucose Homeostasis, Inflammation and Oxidative Stress in Patients with NAFLD: A Randomised Placebo-controlled Clinical Trial. Int. J. Clin. Pract. 2021, 75, e14744. [Google Scholar] [CrossRef]
- Kavyani, M.; Saleh-Ghadimi, S.; Dehghan, P.; Abbasalizad Farhangi, M.; Khoshbaten, M. Co-Supplementation of Camelina Oil and a Prebiotic Is More Effective for in Improving Cardiometabolic Risk Factors and Mental Health in Patients with NAFLD: A Randomized Clinical Trial. Food Funct. 2021, 12, 8594–8604. [Google Scholar] [CrossRef] [PubMed]
- Espirito Santo, B.L.S.d.; Santana, L.F.; Kato Junior, W.H.; de Araújo, F.d.O.; Bogo, D.; Freitas, K.d.C.; Guimarães, R.d.C.A.; Hiane, P.A.; Pott, A.; Filiú, W.F.d.O.; et al. Medicinal Potential of Garcinia Species and Their Compounds. Molecules 2020, 25, 4513. [Google Scholar] [CrossRef]
- Vasques, C.A.R.; Schneider, R.; Klein-Júnior, L.C.; Falavigna, A.; Piazza, I.; Rossetto, S. Hypolipemic Effect of Garcinia Cambogia in Obese Women: Hypolipemic Effect of Garcinia cambogia. Phytother. Res. 2014, 28, 887–891. [Google Scholar] [CrossRef]
- Chong, P.; Beah, Z.; Grube, B.; Riede, L. IQP-GC-101 Reduces Body Weight and Body Fat Mass: A Randomized, Double-Blind, Placebo-Controlled Study. Phytother. Res. 2014, 28, 1520–1526. [Google Scholar] [CrossRef]
- Arefhosseini, S.; Tutunchi, H.; Nomi-Golzar, S.; Mahboob, S.; Pouretedal, Z.; Ebrahimi-Mameghani, M. The Effect of Hydroxy Citric Acid Supplementation with Calorie-Restricted Diet on Metabolic, Atherogenic and Inflammatory Biomarkers in Women with Non-Alcoholic Fatty Liver Disease: A Randomized Controlled Clinical Trial. Food Funct. 2022, 13, 5124–5134. [Google Scholar] [CrossRef]
- de Mello-Sampayo, C.; Corvo, M.L.; Mendes, R.; Duarte, D.; Lucas, J.; Pinto, R.; Batista, A.P.; Raymundo, A.; Silva-Lima, B.; Bandarra, N.M.; et al. Insights on the Safety of Carotenogenic Chlorella vulgaris in Rodents. Algal Res. 2013, 2, 409–415. [Google Scholar] [CrossRef]
- Ebrahimi-Mameghani, M.; Aliashrafi, S.; Javadzadeh, Y.; AsghariJafarabadi, M. The Effect of Chlorella vulgaris Supplementation on Liver Enzymes, Serum Glucose and Lipid Profile in Patients with Non-Alcoholic Fatty Liver Disease. Health Promot. Perspect. 2014, 4, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Panahi, Y.; Ghamarchehreh, M.E.; Beiraghdar, F.; Zare, R.; Jalalian, H.R.; Sahebkar, A. Investigation of the Effects of Chlorella vulgaris Supplementation in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized Clinical Trial. Hepatogastroenterology 2012, 59, 2099–2103. [Google Scholar] [CrossRef]
- Safe, S.; Kothari, J.; Hailemariam, A.; Upadhyay, S.; Davidson, L.A.; Chapkin, R.S. Health Benefits of Coffee Consumption for Cancer and Other Diseases and Mechanisms of Action. Int. J. Mol. Sci. 2023, 24, 2706. [Google Scholar] [CrossRef]
- Déchamp, E.; Breitler, J.-C.; Leroy, T.; Etienne, H. Coffee (Coffea arabica L.). In Agrobacterium Protocols; Wang, K., Ed.; Methods in Molecular Biology; Springer: New York, NY, USA, 2015; Volume 1224, pp. 275–291. ISBN 978-1-4939-1657-3. [Google Scholar]
- Mansour, A.; Mohajeri-Tehrani, M.R.; Samadi, M.; Qorbani, M.; Merat, S.; Adibi, H.; Poustchi, H.; Hekmatdoost, A. Effects of Supplementation with Main Coffee Components Including Caffeine and/or Chlorogenic Acid on Hepatic, Metabolic, and Inflammatory Indices in Patients with Non-Alcoholic Fatty Liver Disease and Type 2 Diabetes: A Randomized, Double-Blind, Placebo-Controlled, Clinical Trial. Nutr. J. 2021, 20, 35. [Google Scholar] [CrossRef] [PubMed]
- Cossiga, V.; Lembo, V.; Guarino, M.; Tuccillo, C.; Morando, F.; Pontillo, G.; Fiorentino, A.; Caporaso, N.; Morisco, F. Berberis aristata, Elaeis guineensis and Coffea canephora Extracts Modulate the Insulin Receptor Expression and Improve Hepatic Steatosis in NAFLD Patients: A Pilot Clinical Trial. Nutrients 2019, 11, 3070. [Google Scholar] [CrossRef] [PubMed]
- Hosseinabadi, S.; Rafraf, M.; Asghari, S.; Asghari-Jafarabadi, M.; Vojouhi, S. Effect of Green Coffee Extract Supplementation on Serum Adiponectin Concentration and Lipid Profile in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized, Controlled Trial. Complement. Ther. Med. 2020, 49, 102290. [Google Scholar] [CrossRef]
- Khan, N.; Mukhtar, H. Multitargeted Therapy of Cancer by Green Tea Polyphenols. Cancer Lett. 2008, 269, 269–280. [Google Scholar] [CrossRef]
- Stangl, V.; Lorenz, M.; Stangl, K. The Role of Tea and Tea Flavonoids in Cardiovascular Health. Mol. Nutr. Food Res. 2006, 50, 218–228. [Google Scholar] [CrossRef]
- Wolfram, S. Effects of Green Tea and EGCG on Cardiovascular and Metabolic Health. J. Am. Coll. Nutr. 2007, 26, 373S–388S. [Google Scholar] [CrossRef]
- Sakata, R.; Nakamura, T.; Torimura, T.; Ueno, T.; Sata, M. Green Tea with High-Density Catechins Improves Liver Function and Fat Infiltration in Non-Alcoholic Fatty Liver Disease (NAFLD) Patients: A Double-Blind Placebo-Controlled Study. Int. J. Mol. Med. 2013, 32, 989–994. [Google Scholar] [CrossRef]
- Jaiswal, N.; Akhtar, J.; Singh, S.P.; Ahsan, F.; Badruddeen. An Overview on Genistein and Its Various Formulations. Drug Res. 2019, 69, 305–313. [Google Scholar] [CrossRef]
- Guevara-Cruz, M.; Godinez-Salas, E.T.; Sanchez-Tapia, M.; Torres-Villalobos, G.; Pichardo-Ontiveros, E.; Guizar-Heredia, R.; Arteaga-Sanchez, L.; Gamba, G.; Mojica-Espinosa, R.; Schcolnik-Cabrera, A.; et al. Genistein Stimulates Insulin Sensitivity through Gut Microbiota Reshaping and Skeletal Muscle AMPK Activation in Obese Subjects. BMJ Open Diab Res. Care 2020, 8, e000948. [Google Scholar] [CrossRef] [PubMed]
- Squadrito, F.; Marini, H.; Bitto, A.; Altavilla, D.; Polito, F.; Adamo, E.B.; D’Anna, R.; Arcoraci, V.; Burnett, B.P.; Minutoli, L.; et al. Genistein in the Metabolic Syndrome: Results of a Randomized Clinical Trial. J. Clin. Endocrinol. Metab. 2013, 98, 3366–3374. [Google Scholar] [CrossRef] [PubMed]
- Amanat, S.; Ashkar, F.; Eftekhari, M.H.; Tanideh, N.; Doaei, S.; Gholamalizadeh, M.; Koohpeyma, F.; Mokhtari, M. The Effect of Genistein on Insulin Resistance, Inflammatory Factors, Lipid Profile, and Histopathologic Indices in Rats with Polycystic Ovary Syndrome. Clin. Exp. Reprod. Med. 2021, 48, 236–244. [Google Scholar] [CrossRef]
- Amanat, S.; Eftekhari, M.H.; Fararouei, M.; Bagheri Lankarani, K.; Massoumi, S.J. Genistein Supplementation Improves Insulin Resistance and Inflammatory State in Non-Alcoholic Fatty Liver Patients: A Randomized, Controlled Trial. Clin. Nutr. 2018, 37, 1210–1215. [Google Scholar] [CrossRef]
- Bhaskaran, S.; Santanam, N.; Penumetcha, M.; Parthasarathy, S. Inhibition of Atherosclerosis in Low-Density Lipoprotein Receptor-Negative Mice by Sesame Oil. J. Med. Food 2006, 9, 487–490. [Google Scholar] [CrossRef]
- Periasamy, S.; Chien, S.-P.; Chang, P.-C.; Hsu, D.-Z.; Liu, M.-Y. Sesame Oil Mitigates Nutritional Steatohepatitis via Attenuation of Oxidative Stress and Inflammation: A Tale of Two-Hit Hypothesis. J. Nutr. Biochem. 2014, 25, 232–240. [Google Scholar] [CrossRef]
- Sankar, D.; Sambandam, G.; Ramakrishna Rao, M.; Pugalendi, K.V. Modulation of Blood Pressure, Lipid Profiles and Redox Status in Hypertensive Patients Taking Different Edible Oils. Clin. Chim. Acta 2005, 355, 97–104. [Google Scholar] [CrossRef]
- Atefi, M.; Entezari, M.H.; Vahedi, H.; Hassanzadeh, A. Sesame Oil Ameliorates Alanine Aminotransferase, Aspartate Aminotransferase, and Fatty Liver Grade in Women with Nonalcoholic Fatty Liver Disease Undergoing Low-Calorie Diet: A Randomized Double-Blind Controlled Trial. Int. J. Clin. Pract. 2022, 2022, 4982080. [Google Scholar] [CrossRef]
- Romani, A.; Ieri, F.; Urciuoli, S.; Noce, A.; Marrone, G.; Nediani, C.; Bernini, R. Health Effects of Phenolic Compounds Found in Extra-Virgin Olive Oil, By-Products, and Leaf of Olea europaea L. Nutrients 2019, 11, 1776. [Google Scholar] [CrossRef]
- Guasch-Ferré, M.; Hu, F.B.; Martínez-González, M.A.; Fitó, M.; Bulló, M.; Estruch, R.; Ros, E.; Corella, D.; Recondo, J.; Gómez-Gracia, E.; et al. Olive Oil Intake and Risk of Cardiovascular Disease and Mortality in the Predimed Study. BMC Med. 2014, 12, 78. [Google Scholar] [CrossRef] [PubMed]
- Hussein, O. Monounsaturated Fat Decreases Hepatic Lipid Content in Non-Alcoholic Fatty Liver Disease in Rats. World J. Gastroenterol. 2007, 13, 361. [Google Scholar] [CrossRef] [PubMed]
- Rezaei, S.; Akhlaghi, M.; Sasani, M.R.; Barati Boldaji, R. Olive Oil Lessened Fatty Liver Severity Independent of Cardiometabolic Correction in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized Clinical Trial. Nutrition 2019, 57, 154–161. [Google Scholar] [CrossRef]
- Sofi, F.; Giangrandi, I.; Cesari, F.; Corsani, I.; Abbate, R.; Gensini, G.F.; Casini, A. Effects of a 1-Year Dietary Intervention with n-3 Polyunsaturated Fatty Acid-Enriched Olive Oil on Non-Alcoholic Fatty Liver Disease Patients: A Preliminary Study. Int. J. Food Sci. Nutr. 2010, 61, 792–802. [Google Scholar] [CrossRef] [PubMed]
- Nigam, P.; Bhatt, S.; Misra, A.; Chadha, D.S.; Vaidya, M.; Dasgupta, J.; Pasha, Q.M.A. Effect of a 6-Month Intervention with Cooking Oils Containing a High Concentration of Monounsaturated Fatty Acids (Olive and Canola Oils) Compared with Control Oil in Male Asian Indians with Nonalcoholic Fatty Liver Disease. Diabetes Technol. Ther. 2014, 16, 255–261. [Google Scholar] [CrossRef]
- Butler, J.; Usman, M.S.; Khan, M.S.; Greene, S.J.; Friede, T.; Vaduganathan, M.; Filippatos, G.; Coats, A.J.S.; Anker, S.D. Efficacy and Safety of SGLT2 Inhibitors in Heart Failure: Systematic Review and Meta-analysis. ESC Heart Fail. 2020, 7, 3298–3309. [Google Scholar] [CrossRef]
- Gilissen, L.; van der Meer, I.; Smulders, M. Why Oats Are Safe and Healthy for Celiac Disease Patients. Med. Sci. 2016, 4, 21. [Google Scholar] [CrossRef]
- Korczak, R.; Kocher, M.; Swanson, K.S. Effects of Oats on Gastrointestinal Health as Assessed by in Vitro, Animal, and Human Studies. Nutr. Rev. 2020, 78, 343–363. [Google Scholar] [CrossRef]
- Storz, M.A.; Küster, O. Hypocaloric, Plant-Based Oatmeal Interventions in the Treatment of Poorly-Controlled Type 2 Diabetes: A Review. Nutr. Health 2019, 25, 281–290. [Google Scholar] [CrossRef]
- Schweinlin, A.; Ulbrich, S.; Stauß, S.; Teutsch, M.; Walle, H.; Basrai, M.; Bischoff, S. Vergleich einer kommerziell erhältlichen, Formula-basierten, mit Haferballaststoffen angereicherten Ernährungstherapie mit einer isokalorischen diätetischen Therapie ohne Formula zur Therapie der nicht-alkoholischen Fettlebererkrankung (NAFLD)—Eine randomisierte, kontrollierte Interventionsstudie. Z. Gastroenterol. 2018, 56, 1247–1256. [Google Scholar] [CrossRef]
- Zhou, Y.; Park, C.-M.; Cho, C.-W.; Song, Y.-S. Protective Effect of Pinitol against D-Galactosamine-Induced Hepatotoxicity in Rats Fed on a High-Fat Diet. Biosci. Biotechnol. Biochem. 2008, 72, 1657–1666. [Google Scholar] [CrossRef]
- Singh, R.K.; Pandey, B.L.; Tripathi, M.; Pandey, V.B. Anti-inflammatory effect of (+)-pinitol. Fitoterapia 2001, 72, 168–170. [Google Scholar] [CrossRef] [PubMed]
- Geethan, P.K.M.A.; Prince, P.S.M. Antihyperlipidemic Effect of D-Pinitol on Streptozotocin-Induced Diabetic Wistar Rats. J. Biochem. Mol. Toxicol. 2008, 22, 220–224. [Google Scholar] [CrossRef]
- Lee, E.; Lim, Y.; Kwon, S.W.; Kwon, O. Pinitol Consumption Improves Liver Health Status by Reducing Oxidative Stress and Fatty Acid Accumulation in Subjects with Non-Alcoholic Fatty Liver Disease: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Nutr. Biochem. 2019, 68, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Rayne, S.; Mazza, G. Biological Activities of Extracts from Sumac (Rhus spp.): A Review. Plant. Foods Hum. Nutr. 2007, 62, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Kazemi, S.; Shidfar, F.; Ehsani, S.; Adibi, P.; Janani, L.; Eslami, O. The Effects of Sumac (Rhus coriaria L.) Powder Supplementation in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized Controlled Trial. Complement. Ther. Clin. Pract. 2020, 41, 101259. [Google Scholar] [CrossRef] [PubMed]
- Kong, W.; Wei, J.; Abidi, P.; Lin, M.; Inaba, S.; Li, C.; Wang, Y.; Wang, Z.; Si, S.; Pan, H.; et al. Berberine Is a Novel Cholesterol-Lowering Drug Working through a Unique Mechanism Distinct from Statins. Nat. Med. 2004, 10, 1344–1351. [Google Scholar] [CrossRef]
- Yin, J.; Xing, H.; Ye, J. Efficacy of Berberine in Patients with Type 2 Diabetes Mellitus. Metabolism 2008, 57, 712–717. [Google Scholar] [CrossRef]
- Yan, H.-M.; Xia, M.-F.; Wang, Y.; Chang, X.-X.; Yao, X.-Z.; Rao, S.-X.; Zeng, M.-S.; Tu, Y.-F.; Feng, R.; Jia, W.-P.; et al. Efficacy of Berberine in Patients with Non-Alcoholic Fatty Liver Disease. PLoS ONE 2015, 10, e0134172. [Google Scholar] [CrossRef]
- Kanoni, S.; Kumar, S.; Amerikanou, C.; Kurth, M.J.; Stathopoulou, M.G.; Bourgeois, S.; Masson, C.; Kannt, A.; Cesarini, L.; Kontoe, M.-S.; et al. Nutrigenetic Interactions Might Modulate the Antioxidant and Anti-Inflammatory Status in Mastiha-Supplemented Patients with NAFLD. Front. Immunol. 2021, 12, 683028. [Google Scholar] [CrossRef]
- Papada, E.; Kaliora, A.C. Kaliora Antioxidant and Anti-Inflammatory Properties of Mastiha: A Review of Preclinical and Clinical Studies. Antioxidants 2019, 8, 208. [Google Scholar] [CrossRef]
- Amerikanou, C.; Papada, E.; Gioxari, A.; Smyrnioudis, I.; Kleftaki, S.-A.; Valsamidou, E.; Bruns, V.; Banerjee, R.; Trivella, M.G.; Milic, N.; et al. Mastiha Has Efficacy in Immune-Mediated Inflammatory Diseases through a MicroRNA-155 Th17 Dependent Action. Pharmacol. Res. 2021, 171, 105753. [Google Scholar] [CrossRef]
- Amerikanou, C.; Kanoni, S.; Kaliora, A.C.; Barone, A.; Bjelan, M.; D’Auria, G.; Gioxari, A.; Gosalbes, M.J.; Mouchti, S.; Stathopoulou, M.G.; et al. Effect of Mastiha Supplementation on NAFLD: The mast4health Randomised, Controlled Trial. Mol. Nutr. Food Res. 2021, 65, 2001178. [Google Scholar] [CrossRef] [PubMed]
- Basu, A.; Betts, N.M.; Ortiz, J.; Simmons, B.; Wu, M.; Lyons, T.J. Low-Energy Cranberry Juice Decreases Lipid Oxidation and Increases Plasma Antioxidant Capacity in Women with Metabolic Syndrome. Nutr. Res. 2011, 31, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Narwojsz, A.; Tańska, M.; Mazur, B.; Borowska, E.J. Fruit Physical Features, Phenolic Compounds Profile and Inhibition Activities of Cranberry Cultivars (Vaccinium macrocarpon) Compared to Wild-Grown Cranberry (Vaccinium Oxycoccus). Plant. Foods Hum. Nutr. 2019, 74, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Novotny, J.A.; Baer, D.J.; Khoo, C.; Gebauer, S.K.; Charron, C.S. Cranberry Juice Consumption Lowers Markers of Cardiometabolic Risk, Including Blood Pressure and Circulating C-Reactive Protein, Triglyceride, and Glucose Concentrations in Adults. J. Nutr. 2015, 145, 1185–1193. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.T.; Chan, Y.C.; Lin, C.W.; Lee, W.J.; Sheu, W.H.-H. Effect of Cranberry Extracts on Lipid Profiles in Subjects with Type 2 Diabetes. Diabet. Med. 2008, 25, 1473–1477. [Google Scholar] [CrossRef]
- Shidfar, F.; Heydari, I.; Hajimiresmaiel, S.J.; Hosseini, S.; Shidfar, S.; Amiri, F. The Effects of Cranberry Juice on Serum Glucose, ApoB, ApoA-I, Lp(a), and Paraoxonase-1 Activity in Type 2 Diabetic Male Patients. J. Res. Med. Sci. 2012, 17, 355–360. [Google Scholar]
- Masnadi Shirazi, K.; Shirinpour, E.; Masnadi Shirazi, A.; Nikniaz, Z. Effect of Cranberry Supplementation on Liver Enzymes and Cardiometabolic Risk Factors in Patients with NAFLD: A Randomized Clinical Trial. BMC Complement. Med. Ther. 2021, 21, 283. [Google Scholar] [CrossRef]
- Hormoznejad, R.; Mohammad Shahi, M.; Rahim, F.; Helli, B.; Alavinejad, P.; Sharhani, A. Combined Cranberry Supplementation and Weight Loss Diet in Non-Alcoholic Fatty Liver Disease: A Double-Blind Placebo-Controlled Randomized Clinical Trial. Int. J. Food Sci. Nutr. 2020, 71, 991–1000. [Google Scholar] [CrossRef]
- Melgarejo-Sánchez, P.; Núñez-Gómez, D.; Martínez-Nicolás, J.J.; Hernández, F.; Legua, P.; Melgarejo, P. Pomegranate Variety and Pomegranate Plant Part, Relevance from Bioactive Point of View: A Review. Bioresour. Bioprocess. 2021, 8, 2. [Google Scholar] [CrossRef]
- Banihani, S.A.; Makahleh, S.M.; El-Akawi, Z.; Al-Fashtaki, R.A.; Khabour, O.F.; Gharibeh, M.Y.; Saadah, N.A.; Al-Hashimi, F.H.; Al-Khasieb, N.J. Fresh Pomegranate Juice Ameliorates Insulin Resistance, Enhances β-Cell Function, and Decreases Fasting Serum Glucose in Type 2 Diabetic Patients. Nutr. Res. 2014, 34, 862–867. [Google Scholar] [CrossRef]
- Goodarzi, R.; Jafarirad, S.; Mohammadtaghvaei, N.; Dastoorpoor, M.; Alavinejad, P. The Effect of Pomegranate Extract on Anthropometric Indices, Serum Lipids, Glycemic Indicators, and Blood Pressure in Patients with Nonalcoholic Fatty Liver Disease: A Randomized Double-blind Clinical Trial. Phytother. Res. 2021, 35, 5871–5882. [Google Scholar] [CrossRef] [PubMed]
- Naeini, F.; Namkhah, Z.; Ostadrahimi, A.; Tutunchi, H.; Hosseinzadeh-Attar, M.J. A Comprehensive Systematic Review of the Effects of Naringenin, a Citrus-Derived Flavonoid, on Risk Factors for Nonalcoholic Fatty Liver Disease. Adv. Nutr. 2021, 12, 413–428. [Google Scholar] [CrossRef] [PubMed]
- Naeini, F.; Namkhah, Z.; Tutunchi, H.; Rezayat, S.M.; Mansouri, S.; Yaseri, M.; Hosseinzadeh-Attar, M.J. Effects of Naringenin Supplementation on Cardiovascular Risk Factors in Overweight/Obese Patients with Nonalcoholic Fatty Liver Disease: A Pilot Double-Blind, Placebo-Controlled, Randomized Clinical Trial. Eur. J. Gastroenterol. Hepatol. 2022, 34, 345–353. [Google Scholar] [CrossRef]
- Namkhah, Z.; Naeini, F.; Rezayat, S.M.; Yaseri, M.; Mansouri, S.; Hosseinzadeh-Attar, M.J. Does Naringenin Supplementation Improve Lipid Profile, Severity of Hepatic Steatosis and Probability of Liver Fibrosis in Overweight/Obese Patients with NAFLD? A Randomised, Double-blind, Placebo-controlled, Clinical Trial. Int. J. Clin. Pract. 2021, 75, e14852. [Google Scholar] [CrossRef]
- Nauman, M.C.; Johnson, J.J. Clinical Application of Bergamot (Citrus bergamia) for Reducing High Cholesterol and Cardiovascular Disease Markers. Integr. Food Nutr. Metab. 2019, 6. [Google Scholar] [CrossRef] [PubMed]
- Mollace, V.; Sacco, I.; Janda, E.; Malara, C.; Ventrice, D.; Colica, C.; Visalli, V.; Muscoli, S.; Ragusa, S.; Muscoli, C.; et al. Hypolipemic and Hypoglycaemic Activity of Bergamot Polyphenols: From Animal Models to Human Studies. Fitoterapia 2011, 82, 309–316. [Google Scholar] [CrossRef]
- Capomolla, A.S.; Janda, E.; Paone, S.; Parafati, M.; Sawicki, T.; Mollace, R.; Ragusa, S.; Mollace, V. Atherogenic Index Reduction and Weight Loss in Metabolic Syndrome Patients Treated with A Novel Pectin-Enriched Formulation of Bergamot Polyphenols. Nutrients 2019, 11, 1271. [Google Scholar] [CrossRef]
- Ferro, Y.; Maurotti, S.; Mazza, E.; Pujia, R.; Sciacqua, A.; Musolino, V.; Mollace, V.; Pujia, A.; Montalcini, T. Citrus bergamia and Cynara cardunculus Reduce Serum Uric Acid in Individuals with Non-Alcoholic Fatty Liver Disease. Medicina 2022, 58, 1728. [Google Scholar] [CrossRef]
- Ferro, Y.; Montalcini, T.; Mazza, E.; Foti, D.; Angotti, E.; Gliozzi, M.; Nucera, S.; Paone, S.; Bombardelli, E.; Aversa, I.; et al. Randomized Clinical Trial: Bergamot Citrus and Wild Cardoon Reduce Liver Steatosis and Body Weight in Non-Diabetic Individuals Aged Over 50 Years. Front. Endocrinol. 2020, 11, 494. [Google Scholar] [CrossRef]
- Sangsefidi, Z.S.; Hosseinzadeh, M.; Ranjbar, A.M.; Akhondi-Meybodi, M.; Fallahzadeh, H.; Mozaffari-Khosravi, H. The Effect of Total Anthocyanin-Base Standardized (Cornus mas L.) Fruit Extract on Liver Function, Tumor Necrosis Factor α, Malondealdehyde, and Adiponectin in Patients with Non-Alcoholic Fatty Liver: A Study Protocol for a Double-Blind Randomized Clinical Trial. Nutr. J. 2019, 18, 39. [Google Scholar] [CrossRef]
- Sangsefidi, Z.S.; Yarhosseini, F.; Hosseinzadeh, M.; Ranjbar, A.; Akhondi-Meybodi, M.; Fallahzadeh, H.; Mozaffari-Khosravi, H. The Effect of (Cornus mas L.) Fruit Extract on Liver Function among Patients with Nonalcoholic Fatty Liver: A Double-blind Randomized Clinical Trial. Phytother. Res. 2021, 35, 5259–5268. [Google Scholar] [CrossRef] [PubMed]
- Sangouni, A.A.; Sangsefidi, Z.S.; Yarhosseini, F.; Hosseinzadeh, M.; Akhondi-Meybodi, M.; Ranjbar, A.; Madadizadeh, F.; Mozaffari-Khosravi, H. Effect of Cornus Mas L. Fruit Extract on Lipid Accumulation Product and Cardiovascular Indices in Patients with Non-Alcoholic Fatty Liver Disease: A Double-Blind Randomized Controlled Trial. Clin. Nutr. ESPEN 2022, 47, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Sangouni, A.A.; Alizadeh, M.; Jamalzehi, A.; Parastouei, K. Effects of Garlic Powder Supplementation on Metabolic Syndrome Components, Insulin Resistance, Fatty Liver Index, and Appetite in Subjects with Metabolic Syndrome: A Randomized Clinical Trial. Phytother. Res. 2021, 35, 4433–4441. [Google Scholar] [CrossRef]
- Kim, H.-N.; Kang, S.-G.; Roh, Y.K.; Choi, M.-K.; Song, S.-W. Efficacy and Safety of Fermented Garlic Extract on Hepatic Function in Adults with Elevated Serum Gamma-Glutamyl Transpeptidase Levels: A Double-Blind, Randomized, Placebo-Controlled Trial. Eur. J. Nutr. 2017, 56, 1993–2002. [Google Scholar] [CrossRef]
- Sangouni, A.A.; Mohammad Hosseini Azar, M.R.; Alizadeh, M. Effect of Garlic Powder Supplementation on Hepatic Steatosis, Liver Enzymes and Lipid Profile in Patients with Non-Alcoholic Fatty Liver Disease: A Double-Blind Randomised Controlled Clinical Trial. Br. J. Nutr. 2020, 124, 450–456. [Google Scholar] [CrossRef]
- Sabzghabaee, A.; Kelishadi, R.; Jelokhanian, H.; Asgary, S.; Ghannadi, A.; Badri, S. Clinical Effects of Portulaca Oleracea Seeds on Dyslipidemia in Obese Adolescents: A Triple-Blinded Randomized Controlled Trial. Med. Arh. 2014, 68, 195. [Google Scholar] [CrossRef]
- El-Sayed, M.-I.K. Effects of Portulaca Oleracea L. Seeds in Treatment of Type-2 Diabetes Mellitus Patients as Adjunctive and Alternative Therapy. J. Ethnopharmacol. 2011, 137, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Wainstein, J.; Landau, Z.; Dayan, Y.B.; Jakubowicz, D.; Grothe, T.; Perrinjaquet-Moccetti, T.; Boaz, M. Purslane Extract and Glucose Homeostasis in Adults with Type 2 Diabetes: A Double-Blind, Placebo-Controlled Clinical Trial of Efficacy and Safety. J. Med. Food 2016, 19, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Gheflati, A.; Adelnia, E.; Nadjarzadeh, A. The clinical effects of purslane (Portulaca oleracea) seeds on metabolic profiles in patients with nonalcoholic fatty liver disease: A randomized controlled clinical trial. Phytother. Res. 2019, 33, 1501–1509. [Google Scholar] [CrossRef]
- Darvish Damavandi, R.; Shidfar, F.; Najafi, M.; Janani, L.; Masoodi, M.; Akbari-Fakhrabadi, M.; Dehnad, A. Effect of Portulaca oleracea (Purslane) Extract on Liver Enzymes, Lipid Profile, and Glycemic Status in Nonalcoholic Fatty Liver Disease: A Randomized, Double-blind Clinical Trial. Phytother. Res. 2021, 35, 3145–3156. [Google Scholar] [CrossRef] [PubMed]
- Rezazadeh, K.; Aliashrafi, S.; Asghari-Jafarabadi, M.; Ebrahimi-Mameghani, M. Antioxidant Response to Artichoke Leaf Extract Supplementation in Metabolic Syndrome: A Double-Blind Placebo-Controlled Randomized Clinical Trial. Clin. Nutr. 2018, 37, 790–796. [Google Scholar] [CrossRef]
- Bundy, R.; Walker, A.F.; Middleton, R.W.; Wallis, C.; Simpson, H.C.R. Artichoke Leaf Extract (Cynara scolymus) Reduces Plasma Cholesterol in Otherwise Healthy Hypercholesterolemic Adults: A Randomized, Double Blind Placebo Controlled Trial. Phytomedicine 2008, 15, 668–675. [Google Scholar] [CrossRef] [PubMed]
- Majnooni, M.B.; Ataee, M.; Bahrami, G.; Heydarpour, F.; Aneva, I.Y.; Farzaei, M.H.; Ahmadi-Juoibari, T. The Effects of Co-administration of Artichoke Leaf Extract Supplementation with Metformin and Vitamin E in Patients with Nonalcoholic Fatty Liver Disease: A Randomized Clinical Trial. Phytother. Res. 2021, 35, 6324–6334. [Google Scholar] [CrossRef]
- Panahi, Y.; Kianpour, P.; Mohtashami, R.; Atkin, S.L.; Butler, A.E.; Jafari, R.; Badeli, R.; Sahebkar, A. Efficacy of Artichoke Leaf Extract in Non-Alcoholic Fatty Liver Disease: A Pilot Double-Blind Randomized Controlled Trial. Phytother. Res. 2018, 32, 1382–1387. [Google Scholar] [CrossRef]
- Mozaffari-Khosravi, H.; Ahadi, Z.; Barzegar, K. The Effect of Green Tea and Sour Tea on Blood Pressure of Patients with Type 2 Diabetes: A Randomized Clinical Trial. J. Diet. Suppl. 2013, 10, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Mozaffari-Khosravi, H.; Jalali-Khanabadi, B.-A.; Afkhami-Ardekani, M.; Fatehi, F.; Noori-Shadkam, M. The Effects of Sour Tea (Hibiscus sabdariffa) on Hypertension in Patients with Type II Diabetes. J. Hum. Hypertens. 2009, 23, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Mozaffari-Khosravi, H.; Jalali-Khanabadi, B.-A.; Afkhami-Ardekani, M.; Fatehi, F. Effects of Sour Tea (Hibiscus sabdariffa) on Lipid Profile and Lipoproteins in Patients with Type II Diabetes. J. Altern. Complement. Med. 2009, 15, 899–903. [Google Scholar] [CrossRef]
- Izadi, F.; Farrokhzad, A.; Tamizifar, B.; Tarrahi, M.J.; Entezari, M.H. Effect of Sour Tea Supplementation on Liver Enzymes, Lipid Profile, Blood Pressure, and Antioxidant Status in Patients with Non-alcoholic Fatty Liver Disease: A Double-blind Randomized Controlled Clinical Trial. Phytother. Res. 2021, 35, 477–485. [Google Scholar] [CrossRef]
- Lee, Y.-J.; Lee, Y.M.; Lee, C.-K.; Jung, J.K.; Han, S.B.; Hong, J.T. Therapeutic Applications of Compounds in the Magnolia Family. Pharmacol. Ther. 2011, 130, 157–176. [Google Scholar] [CrossRef] [PubMed]
- Kalman, D.S.; Feldman, S.; Feldman, R.; Schwartz, H.I.; Krieger, D.R.; Garrison, R. Effect of a Proprietary Magnolia and Phellodendronextract on Stress Levels in Healthy Women: A Pilot, Double-Blind, Placebo-Controlled Clinical Trial. Nutr. J. 2008, 7, 11. [Google Scholar] [CrossRef] [PubMed]
- Peters, A.L.; Stunz, L.L.; Meyerholz, D.K.; Mohan, C.; Bishop, G.A. Latent Membrane Protein 1, the EBV-Encoded Oncogenic Mimic of CD40, Accelerates Autoimmunity in B6.Sle1 Mice. J. Immunol. 2010, 185, 4053–4062. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.Y.; Sohn, J.H.; Baek, Y.H.; Cho, Y.K.; Kim, Y.; Kim, H. New Botanical Drug, HL Tablet, Reduces Hepatic Fat as Measured by Magnetic Resonance Spectroscopy in Patients with Nonalcoholic Fatty Liver Disease: A Placebo-Controlled, Randomized, Phase II Trial. World J. Gastroenterol. 2017, 23, 5977. [Google Scholar] [CrossRef] [PubMed]
- Maierean, S.M.; Serban, M.-C.; Sahebkar, A.; Ursoniu, S.; Serban, A.; Penson, P.; Banach, M. The Effects of Cinnamon Supplementation on Blood Lipid Concentrations: A Systematic Review and Meta-Analysis. J. Clin. Lipidol. 2017, 11, 1393–1406. [Google Scholar] [CrossRef]
- Lu, T.; Sheng, H.; Wu, J.; Cheng, Y.; Zhu, J.; Chen, Y. Cinnamon Extract Improves Fasting Blood Glucose and Glycosylated Hemoglobin Level in Chinese Patients with Type 2 Diabetes. Nutr. Res. 2012, 32, 408–412. [Google Scholar] [CrossRef]
- Askari, F.; Rashidkhani, B.; Hekmatdoost, A. Cinnamon May Have Therapeutic Benefits on Lipid Profile, Liver Enzymes, Insulin Resistance, and High-Sensitivity C-Reactive Protein in Nonalcoholic Fatty Liver Disease Patients. Nutr. Res. 2014, 34, 143–148. [Google Scholar] [CrossRef]
- Kazemi, S.; Yaghooblou, F.; Siassi, F.; Rahimi Foroushani, A.; Ghavipour, M.; Koohdani, F.; Sotoudeh, G. Cardamom Supplementation Improves Inflammatory and Oxidative Stress Biomarkers in Hyperlipidemic, Overweight, and Obese Pre-Diabetic Women: A Randomized Double-Blind Clinical Trial: Cardamom Supplementation in Pre-Diabetic Women. J. Sci. Food Agric. 2017, 97, 5296–5301. [Google Scholar] [CrossRef]
- Aghasi, M.; Koohdani, F.; Qorbani, M.; Nasli-Esfahani, E.; Ghazi-Zahedi, S.; Khoshamal, H.; Keshavarz, A.; Sotoudeh, G. Beneficial Effects of Green Cardamom on Serum SIRT1, Glycemic Indices and Triglyceride Levels in Patients with Type 2 Diabetes Mellitus: A Randomized Double-blind Placebo Controlled Clinical Trial. J. Sci. Food Agric. 2019, 99, 3933–3940. [Google Scholar] [CrossRef]
- Qiblawi, S.; Dhanarasu, S.; Al-Islam, M. Chemopreventive Effect of Cardamom (Elettaria cardamomum L.) Against Benzo(a)Pyrene-Induced Forestomach Papillomagenesis in Swiss Albino Mice. J. Environ. Pathol. Toxicol. Oncol. 2015, 34, 95–104. [Google Scholar] [CrossRef]
- Daneshi-Maskooni, M.; Keshavarz, S.A.; Qorbani, M.; Mansouri, S.; Alavian, S.M.; Badri-Fariman, M.; Jazayeri-Tehrani, S.A.; Sotoudeh, G. Green Cardamom Supplementation Improves Serum Irisin, Glucose Indices, and Lipid Profiles in Overweight or Obese Non-Alcoholic Fatty Liver Disease Patients: A Double-Blind Randomized Placebo-Controlled Clinical Trial. BMC Complement. Altern. Med. 2019, 19, 59. [Google Scholar] [CrossRef] [PubMed]
- Chashmniam, S.; Mirhafez, S.R.; Dehabeh, M.; Hariri, M.; Azimi Nezhad, M.; Nobakht, M.; Gh, B.F. A Pilot Study of the Effect of Phospholipid Curcumin on Serum Metabolomic Profile in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized, Double-Blind, Placebo-Controlled Trial. Eur. J. Clin. Nutr. 2019, 73, 1224–1235. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.G.; Sahebkar, A.; Fogacci, F.; Bove, M.; Giovannini, M.; Borghi, C. Effects of Phytosomal Curcumin on Anthropometric Parameters, Insulin Resistance, Cortisolemia and Non-Alcoholic Fatty Liver Disease Indices: A Double-Blind, Placebo-Controlled Clinical Trial. Eur. J. Nutr. 2020, 59, 477–483. [Google Scholar] [CrossRef]
- Rahmani, S.; Asgary, S.; Askari, G.; Keshvari, M.; Hatamipour, M.; Feizi, A.; Sahebkar, A. Treatment of Non-Alcoholic Fatty Liver Disease with Curcumin: A Randomized Placebo-Controlled Trial: Curcumin Supplementation for NAFLD. Phytother. Res. 2016, 30, 1540–1548. [Google Scholar] [CrossRef]
- Panahi, Y.; Kianpour, P.; Mohtashami, R.; Jafari, R.; Simental-Mendía, L.E.; Sahebkar, A. Curcumin Lowers Serum Lipids and Uric Acid in Subjects With Nonalcoholic Fatty Liver Disease: A Randomized Controlled Trial. J. Cardiovasc. Pharmacol. 2016, 68, 223–229. [Google Scholar] [CrossRef]
- Saberi-Karimian, M.; Keshvari, M.; Ghayour-Mobarhan, M.; Salehizadeh, L.; Rahmani, S.; Behnam, B.; Jamialahmadi, T.; Asgary, S.; Sahebkar, A. Effects of Curcuminoids on Inflammatory Status in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized Controlled Trial. Complement. Ther. Med. 2020, 49, 102322. [Google Scholar] [CrossRef]
- Saadati, S.; Sadeghi, A.; Mansour, A.; Yari, Z.; Poustchi, H.; Hedayati, M.; Hatami, B.; Hekmatdoost, A. Curcumin and Inflammation in Non-Alcoholic Fatty Liver Disease: A Randomized, Placebo Controlled Clinical Trial. BMC Gastroenterol. 2019, 19, 133. [Google Scholar] [CrossRef]
- Jegatheesan, P.; Beutheu, S.; Freese, K.; Waligora-Dupriet, A.-J.; Nubret, E.; Butel, M.-J.; Bergheim, I.; De Bandt, J.-P. Preventive Effects of Citrulline on Western Diet-Induced Non-Alcoholic Fatty Liver Disease in Rats. Br. J. Nutr. 2016, 116, 191–203. [Google Scholar] [CrossRef] [PubMed]
- El-Kirsh, A.A.A.; Abd El-Wahab, H.M.F.; Abd-Ellah Sayed, H.F. The Effect of L-Arginine or L-Citrulline Supplementation on Biochemical Parameters and the Vascular Aortic Wall in High-Fat and High-Cholesterol-Fed Rats: Role of L-arginine or L-citrulline on HFC-Fed Rats. Cell Biochem. Funct. 2011, 29, 414–428. [Google Scholar] [CrossRef]
- Darabi, Z.; Darand, M.; Yari, Z.; Hedayati, M.; Faghihi, A.; Agah, S.; Hekmatdoost, A. Inflammatory Markers Response to Citrulline Supplementation in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized, Double Blind, Placebo-Controlled, Clinical Trial. BMC Res. Notes 2019, 12, 89. [Google Scholar] [CrossRef]
- Kok, C.R.; Hutkins, R. Yogurt and Other Fermented Foods as Sources of Health-Promoting Bacteria. Nutr. Rev. 2018, 76, 4–15. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Feng, R.; Yang, X.; Dai, J.; Huang, M.; Ji, X.; Li, Y.; Okekunle, A.P.; Gao, G.; Onwuka, J.U.; et al. Yogurt Improves Insulin Resistance and Liver Fat in Obese Women with Nonalcoholic Fatty Liver Disease and Metabolic Syndrome: A Randomized Controlled Trial. Am. J. Clin. Nutr. 2019, 109, 1611–1619. [Google Scholar] [CrossRef] [PubMed]
- Bakhshimoghaddam, F.; Shateri, K.; Sina, M.; Hashemian, M.; Alizadeh, M. Daily Consumption of Synbiotic Yogurt Decreases Liver Steatosis in Patients with Nonalcoholic Fatty Liver Disease: A Randomized Controlled Clinical Trial. J. Nutr. 2018, 148, 1276–1284. [Google Scholar] [CrossRef] [PubMed]
- Nabavi, S.; Rafraf, M.; Somi, M.H.; Homayouni-Rad, A.; Asghari-Jafarabadi, M. Effects of Probiotic Yogurt Consumption on Metabolic Factors in Individuals with Nonalcoholic Fatty Liver Disease. J. Dairy. Sci. 2014, 97, 7386–7393. [Google Scholar] [CrossRef]
- Liu, S.; Zhang, M.; Feng, F.; Tian, Z. Toward a “Green Revolution” for Soybean. Mol. Plant. 2020, 13, 688–697. [Google Scholar] [CrossRef]
- Maleki, Z.; Jazayeri, S.; Eslami, O.; Shidfar, F.; Hosseini, A.F.; Agah, S.; Norouzi, H. Effect of Soy Milk Consumption on Glycemic Status, Blood Pressure, Fibrinogen and Malondialdehyde in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized Controlled Trial. Complement. Ther. Med. 2019, 44, 44–50. [Google Scholar] [CrossRef]
- George, K.S.; Muñoz, J.; Akhavan, N.S.; Foley, E.M.; Siebert, S.C.; Tenenbaum, G.; Khalil, D.A.; Chai, S.C.; Arjmandi, B.H. Is Soy Protein Effective in Reducing Cholesterol and Improving Bone Health? Food Funct. 2020, 11, 544–551. [Google Scholar] [CrossRef]
- Eslami, O.; Shidfar, F.; Maleki, Z.; Jazayeri, S.; Hosseini, A.F.; Agah, S.; Ardiyani, F. Effect of Soy Milk on Metabolic Status of Patients with Nonalcoholic Fatty Liver Disease: A Randomized Clinical Trial. J. Am. Coll. Nutr. 2019, 38, 51–58. [Google Scholar] [CrossRef]
- Sforcin, J.M. Biological Properties and Therapeutic Applications of Propolis: Properties and Applications of Propolis. Phytother. Res. 2016, 30, 894–905. [Google Scholar] [CrossRef]
- Huang, S.; Zhang, C.-P.; Wang, K.; Li, G.; Hu, F.-L. Recent Advances in the Chemical Composition of Propolis. Molecules 2014, 19, 19610–19632. [Google Scholar] [CrossRef]
- Soleimani, D.; Rezaie, M.; Rajabzadeh, F.; Gholizadeh Navashenaq, J.; Abbaspour, M.; Miryan, M.; Razmpour, F.; Ranjbar, G.; Rezvani, R.; Jarahi, L.; et al. Protective Effects of Propolis on Hepatic Steatosis and Fibrosis among Patients with Nonalcoholic Fatty Liver Disease (NAFLD) Evaluated by Real-time Two-dimensional Shear Wave Elastography: A Randomized Clinical Trial. Phytother. Res. 2021, 35, 1669–1679. [Google Scholar] [CrossRef] [PubMed]
- Cussons, A.J.; Watts, G.F.; Mori, T.A.; Stuckey, B.G.A. Omega-3 Fatty Acid Supplementation Decreases Liver Fat Content in Polycystic Ovary Syndrome: A Randomized Controlled Trial Employing Proton Magnetic Resonance Spectroscopy. J. Clin. Endocrinol. Metab. 2009, 94, 3842–3848. [Google Scholar] [CrossRef] [PubMed]
- Manousopoulou, A.; Scorletti, E.; Smith, D.E.; Teng, J.; Fotopoulos, M.; Roumeliotis, T.I.; Clough, G.F.; Calder, P.C.; Byrne, C.D.; Garbis, S.D. Marine Omega-3 Fatty Acid Supplementation in Non-Alcoholic Fatty Liver Disease: Plasma Proteomics in the Randomized WELCOME* Trial. Clin. Nutr. 2019, 38, 1952–1955. [Google Scholar] [CrossRef] [PubMed]
- Scorletti, E.; Bhatia, L.; McCormick, K.G.; Clough, G.F.; Nash, K.; Hodson, L.; Moyses, H.E.; Calder, P.C.; Byrne, C.D.; On behalf of the WELCOME Study Investigators. Effects of Purified Eicosapentaenoic and Docosahexaenoic Acids in Nonalcoholic Fatty Liver Disease: Results from the WELCOME* Study. Hepatology 2014, 60, 1211–1221. [Google Scholar] [CrossRef]
- Rodriguez, D.; Lavie, C.J.; Elagizi, A.; Milani, R.V. Update on Omega-3 Polyunsaturated Fatty Acids on Cardiovascular Health. Nutrients 2022, 14, 5146. [Google Scholar] [CrossRef]
- Saini, R.K.; Keum, Y.-S. Omega-3 and Omega-6 Polyunsaturated Fatty Acids: Dietary Sources, Metabolism, and Significance—A Review. Life Sci. 2018, 203, 255–267. [Google Scholar] [CrossRef]
- Tobin, D.; Brevik-Andersen, M.; Qin, Y.; Innes, J.; Calder, P. Evaluation of a High Concentrate Omega-3 for Correcting the Omega-3 Fatty Acid Nutritional Deficiency in Non-Alcoholic Fatty Liver Disease (CONDIN). Nutrients 2018, 10, 1126. [Google Scholar] [CrossRef]
- Zhu, F.-S.; Liu, S.; Chen, X.-M.; Huang, Z.-G.; Zhang, D.-W. Effects of N-3 Polyunsaturated Fatty Acids from Seal Oils on Nonalcoholic Fatty Liver Disease Associated with Hyperlipidemia. World J. Gastroenterol. 2008, 14, 6395. [Google Scholar] [CrossRef]
- Šmíd, V.; Dvořák, K.; Šedivý, P.; Kosek, V.; Leníček, M.; Dezortová, M.; Hajšlová, J.; Hájek, M.; Vítek, L.; Bechyňská, K.; et al. Effect of Omega-3 Polyunsaturated Fatty Acids on Lipid Metabolism in Patients With Metabolic Syndrome and NAFLD. Hepatol. Commun. 2022, 6, 1336–1349. [Google Scholar] [CrossRef]
- Sangouni, A.A.; Orang, Z.; Mozaffari-Khosravi, H. Effect of Omega-3 Supplementation on Fatty Liver and Visceral Adiposity Indices in Diabetic Patients with Non-Alcoholic Fatty Liver Disease: A Randomized Controlled Trial. Clin. Nutr. ESPEN 2021, 44, 130–135. [Google Scholar] [CrossRef]
- Song, L.; Zhao, X.G.; Ouyang, P.L.; Guan, Q.; Yang, L.; Peng, F.; Du, H.; Yin, F.; Yan, W.; Yu, W.J.; et al. Combined Effect of n-3 Fatty Acids and Phytosterol Esters on Alleviating Hepatic Steatosis in Non-Alcoholic Fatty Liver Disease Subjects: A Double-Blind Placebo-Controlled Clinical Trial. Br. J. Nutr. 2020, 123, 1148–1158. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y.; Zhou, Y.; Chen, S.-H.; Zhao, X.-L.; Ran, L.; Zeng, X.-L.; Wu, Y.; Chen, J.-L.; Kang, C.; Shu, F.-R.; et al. Fish Oil Supplements Lower Serum Lipids and Glucose in Correlation with a Reduction in Plasma Fibroblast Growth Factor 21 and Prostaglandin E2 in Nonalcoholic Fatty Liver Disease Associated with Hyperlipidemia: A Randomized Clinical Trial. PLoS ONE 2015, 10, e0133496. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi-Mameghani, M.; Jamali, H.; Mahdavi, R.; Kakaei, F.; Abedi, R.; Kabir-Mamdooh, B. Conjugated Linoleic Acid Improves Glycemic Response, Lipid Profile, and Oxidative Stress in Obese Patients with Non-Alcoholic Fatty Liver Disease: A Randomized Controlled Clinical Trial. Croat. Med. J. 2016, 57, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Hosseinpour-Arjmand, S.; Amirkhizi, F.; Ebrahimi-Mameghani, M. The Effect of Alpha-Lipoic Acid on Inflammatory Markers and Body Composition in Obese Patients with Non-Alcoholic Fatty Liver Disease: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Clin. Pharm. Ther. 2019, 44, 258–267. [Google Scholar] [CrossRef]
- Brancaccio, M.; Mennitti, C.; Cesaro, A.; Fimiani, F.; Vano, M.; Gargiulo, B.; Caiazza, M.; Amodio, F.; Coto, I.; D’Alicandro, G.; et al. The Biological Role of Vitamins in Athletes’ Muscle, Heart and Microbiota. Int. J. Environ. Res. Public Health 2022, 19, 1249. [Google Scholar] [CrossRef]
- Talari, H.R.; Molaqanbari, M.R.; Mokfi, M.; Taghizadeh, M.; Bahmani, F.; Tabatabaei, S.M.H.; Sharifi, N. The Effects of Vitamin B12 Supplementation on Metabolic Profile of Patients with Non-Alcoholic Fatty Liver Disease: A Randomized Controlled Trial. Sci. Rep. 2022, 12, 14047. [Google Scholar] [CrossRef]
- Aller, R.; Izaola, O.; Gómez, S.; Tafur, C.; González, G.; Berroa, E.; Mora, N.; González, J.M.; de Luis, D.A. Effect of Silymarin plus Vitamin E in Patients with Non-Alcoholic Fatty Liver Disease. A Randomized Clinical Pilot Study. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 3118–3124. [Google Scholar]
- Kim, G.H.; Chung, J.W.; Lee, J.H.; Ok, K.S.; Jang, E.S.; Kim, J.; Shin, C.M.; Park, Y.S.; Hwang, J.-H.; Jeong, S.-H.; et al. Effect of Vitamin E in Nonalcoholic Fatty Liver Disease with Metabolic Syndrome: A Propensity Score-Matched Cohort Study. Clin. Mol. Hepatol. 2015, 21, 379. [Google Scholar] [CrossRef]
- Papapostoli, I.; Lammert, F.; Stokes, C.S. Effect of Short-Term Vitamin D Correction on Hepatic Steatosis as Quantified by Controlled Attenuation Parameter (CAP). J. Gastrointest. Liver Dis. 2016, 25, 175–181. [Google Scholar] [CrossRef]
- Rahimpour, Z.; Hoseini, R.; Behpour, N. Alterations of Liver Enzymes and Lipid Profile in Response to Exhaustive Eccentric Exercise: Vitamin D Supplementation Trial in Overweight Females with Non-Alcoholic Fatty Liver Disease. BMC Gastroenterol. 2022, 22, 372. [Google Scholar] [CrossRef]
- Sharifi, N.; Amani, R.; Hajiani, E.; Cheraghian, B. Does Vitamin D Improve Liver Enzymes, Oxidative Stress, and Inflammatory Biomarkers in Adults with Non-Alcoholic Fatty Liver Disease? A Randomized Clinical Trial. Endocrine 2014, 47, 70–80. [Google Scholar] [CrossRef]
- Barchetta, I.; Del Ben, M.; Angelico, F.; Di Martino, M.; Fraioli, A.; La Torre, G.; Saulle, R.; Perri, L.; Morini, S.; Tiberti, C.; et al. No Effects of Oral Vitamin D Supplementation on Non-Alcoholic Fatty Liver Disease in Patients with Type 2 Diabetes: A Randomized, Double-Blind, Placebo-Controlled Trial. BMC Med. 2016, 14, 92. [Google Scholar] [CrossRef] [PubMed]
- Pervez, M.A.; Khan, D.A.; Mirza, S.A.; Slehria, A.U.R.; Nisar, U.; Aamir, M. Comparison of Delta-Tocotrienol and Alpha-Tocopherol Effects on Hepatic Steatosis and Inflammatory Biomarkers in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized Double-Blind Active-Controlled Trial. Complement. Ther. Med. 2022, 70, 102866. [Google Scholar] [CrossRef] [PubMed]
- Pervez, M.A.; Khan, D.A.; Slehria, A.U.R.; Ijaz, A. Delta-Tocotrienol Supplementation Improves Biochemical Markers of Hepatocellular Injury and Steatosis in Patients with Nonalcoholic Fatty Liver Disease: A Randomized, Placebo-Controlled Trial. Complement. Ther. Med. 2020, 52, 102494. [Google Scholar] [CrossRef]
- Illnait, J.; Rodríguez, I.; Mendoza, S.; Fernández, Y.; Mas, R.; Miranda, M.; Piñera, J.; Fernández, J.C.; Mesa, M.; Fernández, L.; et al. Effects of D-002, a Mixture of High Molecular Weight Beeswax Alcohols, on Patients with Nonalcoholic Fatty Liver Disease. Korean J. Intern. Med. 2013, 28, 439. [Google Scholar] [CrossRef] [PubMed]
- Ferro, Y.; Pujia, R.; Mazza, E.; Lascala, L.; Lodari, O.; Maurotti, S.; Pujia, A.; Montalcini, T. A New Nutraceutical (Livogen Plus®) Improves Liver Steatosis in Adults with Non-Alcoholic Fatty Liver Disease. J. Transl. Med. 2022, 20, 377. [Google Scholar] [CrossRef] [PubMed]
- Abidov, M.; Ramazanov, Z.; Seifulla, R.; Grachev, S. The Effects of XanthigenTM in the Weight Management of Obese Premenopausal Women with Non-Alcoholic Fatty Liver Disease and Normal Liver Fat. Diabetes Obes. Metab. 2010, 12, 72–81. [Google Scholar] [CrossRef]
- Fogacci, F.; Rizzoli, E.; Giovannini, M.; Bove, M.; D’Addato, S.; Borghi, C.; Cicero, A.F.G. Effect of Dietary Supplementation with Eufortyn® Colesterolo Plus on Serum Lipids, Endothelial Reactivity, Indexes of Non-Alcoholic Fatty Liver Disease and Systemic Inflammation in Healthy Subjects with Polygenic Hypercholesterolemia: The ANEMONE Study. Nutrients 2022, 14, 2099. [Google Scholar] [CrossRef]
- Gomez, E.V.; DE Miranda, A.R.; Oramas, B.G.; Soler, E.A.; Navarro, R.L.; Bertot, L.C.; Garcia, A.Y.; Vazquez, M.D.R.A. Clinical Trial: A Nutritional Supplement Viusid, in Combination with Diet and Exercise, in Patients with Nonalcoholic Fatty Liver Disease. Aliment. Pharmacol. Ther. 2009, 30, 999–1009. [Google Scholar] [CrossRef]
- Albillos, A.; De Gottardi, A.; Rescigno, M. The Gut-Liver Axis in Liver Disease: Pathophysiological Basis for Therapy. J. Hepatol. 2020, 72, 558–577. [Google Scholar] [CrossRef] [PubMed]
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. The International Scientific Association for Probiotics and Prebiotics Consensus Statement on the Scope and Appropriate Use of the Term Probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef] [PubMed]
- Kobyliak, N.; Abenavoli, L.; Mykhalchyshyn, G.; Kononenko, L.; Boccuto, L.; Kyriienko, D.; Dynnyk, O. A Multi-Strain Probiotic Reduces the Fatty Liver Index, Cytokines and Aminotransferase Levels in NAFLD Patients: Evidence from a Randomized Clinical Trial. J. Gastrointest. Liver Dis. 2018, 27, 41–49. [Google Scholar] [CrossRef]
- Behrouz, V.; Aryaeian, N.; Zahedi, M.J.; Jazayeri, S. Effects of Probiotic and Prebiotic Supplementation on Metabolic Parameters, Liver Aminotransferases, and Systemic Inflammation in Nonalcoholic Fatty Liver Disease: A Randomized Clinical Trial. J. Food Sci. 2020, 85, 3611–3617. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.B.; Jun, D.W.; Kang, B.-K.; Lim, J.H.; Lim, S.; Chung, M.-J. Randomized, Double-Blind, Placebo-Controlled Study of a Multispecies Probiotic Mixture in Nonalcoholic Fatty Liver Disease. Sci. Rep. 2019, 9, 5688. [Google Scholar] [CrossRef]
- Gibson, G.R.; Hutkins, R.; Sanders, M.E.; Prescott, S.L.; Reimer, R.A.; Salminen, S.J.; Scott, K.; Stanton, C.; Swanson, K.S.; Cani, P.D.; et al. Expert Consensus Document: The International Scientific Association for Probiotics and Prebiotics (ISAPP) Consensus Statement on the Definition and Scope of Prebiotics. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 491–502. [Google Scholar] [CrossRef] [PubMed]
- Chong, C.Y.L.; Orr, D.; Plank, L.D.; Vatanen, T.; O’Sullivan, J.M.; Murphy, R. Randomised Double-Blind Placebo-Controlled Trial of Inulin with Metronidazole in Non-Alcoholic Fatty Liver Disease (NAFLD). Nutrients 2020, 12, 937. [Google Scholar] [CrossRef]
- Abhari, K.; Saadati, S.; Yari, Z.; Hosseini, H.; Hedayati, M.; Abhari, S.; Alavian, S.M.; Hekmatdoost, A. The Effects of Bacillus Coagulans Supplementation in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized, Placebo-Controlled, Clinical Trial. Clin. Nutr. ESPEN 2020, 39, 53–60. [Google Scholar] [CrossRef]
- Eslamparast, T.; Poustchi, H.; Zamani, F.; Sharafkhah, M.; Malekzadeh, R.; Hekmatdoost, A. Synbiotic Supplementation in Nonalcoholic Fatty Liver Disease: A Randomized, Double-Blind, Placebo-Controlled Pilot Study. Am. J. Clin. Nutr. 2014, 99, 535–542. [Google Scholar] [CrossRef]
- Mofidi, F.; Poustchi, H.; Yari, Z.; Nourinayyer, B.; Merat, S.; Sharafkhah, M.; Malekzadeh, R.; Hekmatdoost, A. Synbiotic Supplementation in Lean Patients with Non-Alcoholic Fatty Liver Disease: A Pilot, Randomised, Double-Blind, Placebo-Controlled, Clinical Trial. Br. J. Nutr. 2017, 117, 662–668. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Group * | NAFLD Diagnosis | Substance | Duration | Results ** | Possible Mechanism |
|---|---|---|---|---|---|---|
| Loguercio et al. [29] (2012) | 138 patients with NAFLD (69 in treatment group) | Histology–liver biopsy | Realsil (94 mg of silybin and 194 mg of phosphatidylcholine) + 89.28 mg vitamin E acetate 50% (30 mg of α-tocopherol) | 12 months | Normalization of ALT and AST ↓: GGT, HOMA-IR, improvement in liver histology | Antioxidant activity which may lead to decline in membrane lipid peroxidation and restoration of glutathione levels |
| Wang et al. [31] (2022) | 260 patients with NAFLD (130 in the DSSG group) | B-ultrasound | DSSG in 12 g package, 2 packages/time, 3 times per day | 16 weeks | ↓: TC, TG, ALT, AST, GGT, FPG Improvement in B-USG | Inhibition of lipid peroxidation; decline in NF-κB expression in liver |
| Chen et al. [37] (2015) | 60 patients with NAFLD (30 in treatment group) | B-ultrasound | Dihydromyricetin in dose 150 mg twice a day | 3 months | ↑: Adiponectin ↓: ALT, AST, GGT, LDL-C, apo-B, HOMA-IR, TNF- α, CK-18, FGF-21 | Prevention of hepatocyte apoptosis; regulation of antioxidant properties; decline in proinflammatory cytokine levels |
| Zhang et al. [40] (2015) | 74 patients with NAFLD (1:1 with placebo) | USG | Anthocyanin in dose 80 mg in capsule, two capsules twice a day | 12 weeks | ↓: ALT, CK-18, myeloperoxidase, 2 h OGTT, plasma glucose and HOMA-IR | Antioxidant and anti-inflammatory properties; improvement in IR |
| Medina-Urrutia et al. [43] (2020) | 25 patients with NAFLD | CT imaging | Milled chia seeds 25 g per day | 2 weeks of dietary stabilization and 8 weeks of chia supplementation | ↑: L: SAR, ALA plasma concertation, dietary fiber consumption ↓: VAF, BW, BMI, WC, TC, non-HDL, FFA | Fiber may lead to improvements in intestinal barrier which may further promote intestinal transit slowdown, production of GLP-1, and favor the sensation of satiety |
| Zamani et al. [48] (2018) | 85 patients with NAFLD (45 in treatment group) | USG | Zataria multiflora powder 700 mg twice a day | 12 weeks | ↓: Serum insulin, IR, SBP, DBP | IR, and serum TG levels improvements through increase in PPAR-γ expression; increase in adiponectin leads to gluconeogenesis decline |
| Khonche et al. [58] (2019) | 120 patients (60 patients in treatment group) | USG | 2.5 mL standardized Nigella sativa seed oil every 12 h | 3 months | ↑: HDL-C ↓: Grade of hepatic steatosis, ALT, AST, TG, LDL-C | PPAR-γ upregulation; anti-inflammatory, antifibrotic and antioxidant properties |
| Musazadeh et al. [64] (2021) | 43 patients with NAFLD (22 in CSO group) | USG | Camelina sativa oil in dose 20 g per day + calorie restricted diet | 12 weeks | ↑: HDL-C ↓: hs-CRP, insulin, HOMA-IR, QUICKI, LPS, TAC, SOD, GSH-Px, MDA, 8-iso-PGF2α | Omega-3 fatty acids in CSO may lead to induction of GLP-1; CSO leads to decrease in energy intake, and inflammation |
| Arefhosseini et al. [69] (2022) | 40 overweight/obese females with NAFLD (21 in HCA group) | USG | Garcinia cambogia extract (HCA) in connection with calorie restriction diet | 8 weeks | ↑: HDL-C ↓: BW, WC, HC, FPG, LDL-C, TG, TG/HDL-c ratio | Improvement in lipid profile due to suppression of ATP-citrate lyase and appetite; enhancement of glycogen deposition in the liver; anti-obesity properties due to regulation of serotonin levels, reduction in de novo lipogenesis, reduction in leptin, and insulin levels in plasma |
| Ebrahimi-Mameghani [71] et al. (2014) | 55 NAFLD patients (29 in intervention group) | USG | Chlorella vulgaris 300 mg in tables per day + vitamin E 400 mg per day | 8 weeks | ↓: BW, liver enzymes, FPG, ALP, TG, TC, LDL-C | Possible effect related to BW reduction; improvements in glucose metabolism by boost of glucose uptake |
| Cossiga et al. [76] (2019) | 49 NAFLD patients (26 in plant extracts supplementation group) | Transient elastography | Berberis aristata (588 mg), Elaeis guineensis (143 mg) and decaffeinated green coffee by Coffea canephora (67 mg) extracts in dose 1 table per day | 6 months | ↓: serum glucose, insulin, HOMA-IR, CAP | Modulation of serum insulin receptor levels by activation of protein kinase C; insulin sensitizing effect through the activation of AMPK |
| Sakata et al. [81] (2013) | 17 patients with NAFLD (12 in green tea supplementation group) | USG and CT | Green tea in dose 700 mL per day, containing above 1 g catechin | 12 weeks | ↑: L: SAR ↓: BF, ALT, urinary 8-isoprostane excretion | Decline in hepatic oxidation stress; inhibition of lipase which leads to decrease in glucose and fat absorption; improvements in liver lipid metabolism by increase in mRNA expression of peroxisomal, and mitochondrial β-oxidizing enzymes |
| Amanat et al. [86] (2018) | 78 patients with NAFLD (41 in genistein group) | USG | Genistein in dose 250 mg per day | 8 weeks | ↓: Serum insulin, HOMA-IR, MDA, TNF-α, IL-6, WHR, BF, TG | Increase in glucose uptake by promotion of glucose transporter type 4 translocation to a membrane; activation of AMPK; upregulation of genes related to antioxidant properties by NF-κB and Nrf2 transcription factors |
| Atefi et al. [90] (2022) | 53 females with NAFLD (27 in sesame oil group) | USG | Sesame oil supplementation in dose 30 mg per day + low-calorie diet | 12 weeks | ↓: BW, BMI, WC, fatty liver grade, AST, ALT | Inhibiting matrix metalloproteinases-2, 9 activities and upregulating PPAR-γ expression; antioxidant properties; reduction in lipogenic enzymes mRNA expression, and induction of mRNA expression of enzymes related to fatty acid oxidation, e.g., CoA dehydrogenases, acyl-CoA oxidase, or 3-hydroxyacyl CoA dehydrogenase |
| Rezaei et al. [94] (2019) | 54 patients with NAFLD (26 in olive oil group) | USG | Olive oil in dose 20 g per day + recommendation of hypocaloric diet | 12 weeks | ↓: Fatty liver grade in USG, BW, WC, BP, AST, TG, fat mass | Antioxidant properties; action of omega-3 fatty acids; increase in post-prandial β-oxidation of fatty acids; improvements in IR |
| Schweinlin et al. [101] (2018) | 36 patients with NAFLD (17 in oat enriched diet group) | FLI | Restricted diet + oat intake | 12 weeks | ↓: BMI, hepatorenal index, BP | Improvements in gut microbiota, which may be related to fiber intake |
| Lee et al. [105] (2019) | 76 patients with NAFLD (27 in pinitol high dose group) | USG | Pinitol in dose 500 mg per day | 12 weeks | ↑: GSH-Px ↓: Liver fat amount, MDA, AST, ALT, GGT, postprandial TG | Increase in liver antioxidant enzyme activities, e.g., GSH; decline in the rate of glutathione turnover |
| Kazemi et al. [107] (2020) | 80 patients with NAFLD (1:1 with placebo) | Hepatic fibrosis grade based on FibroScan device and ALT level | Sumac powder in dose 2 g per day + calorie deficit diet | 12 weeks | ↑: QUICKI ↓: liver fibrosis score, ALT, AST, hs-CRP, MDA, FPG, HbA1c, HOMA-IR, serum insulin | Inhibition of α-glucosidase and pancreatic α-amylase; suppression of lipogenic factor genes; stimulation of AMPK and lipolysis; increase in PPAR-γ gene expression |
| Yan et al. [110] (2015) | 155 patients with NAFLD (55 in berberine group) | Proton magnetic resonance spectroscopy | Berberine in dose 500 mg 3 times per day + lifestyle intervention | 16 weeks | ↓: HFC, BW, WC, HOMA-IR, TC, TG, ALT | Mechanism is still unclear, but may be linked to expression of genes related to glucose and lipid metabolism such as CPT-1, GCK, or MTTP |
| Amerikanou et al. [114] (2021) | 98 patients with NAFLD (41 in mastiha group) | LiverMultiScan technique | Mastiha in dose 350 mg three times per day | 6 months | Positive effects on intestinal microbiota, improvement in lipid metabolite levels Additionally, in severely obese subjects, ↓ liver fibrosis score, liver inflammation | Reduction in expression of genes related to collagen (Col1a1 and Col4a1); decline in inflammatory and endotoxin-producing bacteria; increase in anti-inflammatory bacteria |
| Study | Group * | Diagnosis | Substance | Duration | Results ** | Possible Mechanism |
|---|---|---|---|---|---|---|
| Hormoznejad et al. [121] (2020) | 41 patients with NAFLD (20 in cranberry group) | USG | Vaccinium macrocarpon extract in tablets (144 mg) twice a day + weight-loss diet | 12 weeks | ↓: ALT, insulin, HOMA-IR | Decrease in hepatic inflammation, as evidenced by decreased TNF- α, NF-κB, COX2, and IκB mRNA expression; inhibition of release of TNF- α, IL-1β, IL-6, and IL-8 from lipopolysaccharide |
| Goodarzi et al. [124] (2021) | 44 patients with NAFLD (22 in pomegranate extract group) | USG | Pomegranate extract in dose 225 mg twice a day | 12 weeks | ↑: HDL-C ↓: TC, TG, LDL to HDL ratio, FPG, HOMA-IR, DBP, BMI, BW, WC | Anti-obesity effect gained by decrease in pancreatic lipase activity and energy intake, reduction in fat absorption and elevation of its fecal secretion; agonist action on PPAR-α and PPAR-γ; decrease in resistin secretion |
| Namkhah et al. [127] (2021) | 44 patients with NAFLD (22 in naringenin group) | USG | Naringenin in dose 100 mg twice a day | 4 weeks | ↑: HDL-C ↓: BW, BMI, TG, TC, LDL-C, NAFLD grade | Inhibition of overproduction of VLD; modification of expression of genes related to lipid metabolism: upregulation the expression of PPAR-α and PPAR-γ genes, modulation of CPT1α, SREBF1c genes, and HMG-CoA reductase; alterations in collagen deposition, modulation of oxidative stress and inflammatory process |
| Ferro et al. [132] (2020) | 86 patients with liver steatosis (45 in intervention group) | Transient elastography | Bergamot polyphenol fraction and Cynara Cardunculus extract in dose 300 mg per day | 12 weeks | ↓: BW, BMI CAP score decreased only in subjects over 50 years | Regulating the potential of the mitochondrial membrane and oxidative phosphorylation; upregulation of antioxidant-related genes; anti-inflammatory properties |
| Sangouni et al. [138] (2020) | 88 patients with NAFLD (45 in garlic group) | USG | 400 mg of garlic powder four times a day | 12 weeks | ↑: HDL-C ↓: Liver steatosis, ALT, GGT, TC, TG, LDL | Lipogenesis modulation by lowering the activity of enzymes involved in hepatic fat synthesis; decrease in insulin resistance, activity of NF-κB pathway, and oxidative stress |
| Damavandi et al. [143] (2021) | 71 patients with NAFLD (37 in purslane group) | USG | Purslane extract, 300 mg once a day | 12 weeks | ↓: ALT, AST, GGT, FPG, TG, LDL-C | Improvements in glucose uptake and fatty acid metabolism; increase in insulin secretion from β-cells; activation of AMPK and PI3K pathways in skeletal muscles; upregulation of GLUT-4 gene expression; enhancing GLP-1 concentration; inhibition of pancreatic lipase activity, decrease in ACC activity |
| Panahi et al. [147] (2018) | 81 patients with NAFLD (41 in artichoke group) | USG | Artichoke leaf extracts in dose 600 mg per day | 2 months | ↑: Hepatic vein flow, AST/ALT ratio ↓: Portal vein diameter, liver size, ALT, AST, total bilirubin, LDL-C, TC, TG, HDL-C, non-HDL-C, BMI, WC, APRI | Enhancement of expression of the following genes: malic enzyme 1, decorin, cytochrome P450, family 1, subfamily a, polypeptide 2 and nicotinamide phosphoribosyltransferase, which leads to improvements in fatty acids metabolism, inflammation, and liver fibrosis |
| Izadi et al. [151] (2021) | 61 patients with NAFLD (30 in sour tea group) | USG | Sour tea powder in capsule in dose 450 mg | 8 weeks | ↓: TG, ALT, AST, SBP, DBP, TAC | Mechanisms are not fully understood; probably improvements are due to an inhibition of fatty acid synthesis, decrease in lipogenesis, improvements in mitochondrial activity and β-oxidation, decrease in production of reactive oxygen species, proinflammatory cytokines and chemokines in liver |
| Jeong et al. [155] (2017) | 60 patients with NAFLD (20 in 400 mg dose of HL) | USG | Magnolia officinalis extract–HL tablet in dose 400 mg per day | 12 weeks | ↓: HFC | Anti-inflammatory and antioxidant properties; induction of apoptosis of the activated hepatic stellate cells; inhibition of liver toxicity and lipid accumulation |
| Askari et al. [158] (2014) | 45 patients with NAFLD (23 in intervention group) | USG | Cinnamon in dose 750 mg twice a day | 12 weeks | ↓: HOMA-IR, FPG, TC, TG, ALT, AST, GGT, hs-CRP | Reduction in post-prandial glucose absorption gained due to inhibition of pancreatic α-amylase and α-glucosidase; stimulation of glucose metabolism and glucose uptake by improving glucose transporter-4; decrease in gluconeogenesis and improvement in IR |
| Daneshi-Maskooni et al. (2019) [162] | 87 patients with NAFLD (43 in cardamom group) | USG | Cardamom in dose 1 g three times per day with meals | 3 months | ↑: Irisin, HDL, QUICKI ↓: fasting insulin, TG, HOMA-IR, fatty liver grade | Increase in antioxidant capability, PPAR-γ expression; decrease in inflammation and cholesterol synthesis; improvement in IR |
| Rahmani et al. [165] (2016) | 77 patients with NAFLD (37 in curcumin group) | USG | Amorphous dispersion curcumin formulation in dose 500 mg per day (equal to 70 mg of curcumin) | 8 weeks | ↓: HFC, BMI, TC, LDL-C, TG, ALT, AST, FPG, HbA1c | Inhibition of oxidative stress and NF-κB; downregulation of pro-inflammatory cytokines, COX-2, collagen 1, inducible nitric oxide synthase, and ICAM-1; improvements in acyl-CoA oxidase activity and lipid peroxidation through glutathione level modulation |
| Study | Group * | Diagnosis | Substance | Duration | Results ** | Possible Mechanism |
|---|---|---|---|---|---|---|
| Darabi et al. [171] (2019) | 44 patients with NAFLD (22 in citrulline group) | Fibroscan | Citrulline in dose 500 mg four times a day | 12 weeks | ↓: TNF-α, hs-CRP, NF-κB, ALT, liver steatosis | Reduction in TLR4 gene expression may lead to decrease in NF-kB activation and TNF-α production; decrease in oxidative stress by increase in SOD may lead to reduction in ERK1/2 signaling activation, and what follows this is a decrease in NF-kB activity and TNF-α production; protection against hepatic lipid peroxidation |
| Bakhshimoghaddam et al. [174] (2018) | 102 patients with NAFLD (34 in symbiotic yogurt group) | USG | 300 g of symbiotic yogurt (containing 108 colony-forming units Bifidobacterium animalis/mL and 1.5 g inulin) per day | 24 weeks | ↓: NAFLD grade (USG), ALT, AST, ALP, GGT | Modulation of intestinal microbiota, and improvements in gut barrier; improvements in insulin resistance; improvements in post-prandial absorption of micro- and macronutrients, including antioxidants; increased production of GLP-2 |
| Maleki et al. [177] (2019) | 62 patients with NAFLD (31 in soy milk group) | USG | Soy milk in dose 240 mL per day + 500 calorie-deficit diet | 8 weeks | ↑: QUICKI ↓: Serum insulin, SBP, DBP, HOMA-IR | Decrease in intestinal alpha-glucosidase and protein tyrosine kinase activity; increased glucose uptake by glucose transporter type 4; inhibition of lipogenesis by decrease in ChREBP, SREBP1, LXR, and RXR expression |
| Soleimani et al. [182] (2021) | 54 patients with NAFLD (27 in propolis group) | Elastography | Propolis tablets (250 mg twice a day) | 4 months | ↓: Liver stiffness, hs-CRP | Impact on cholesterol metabolism by upregulation of Apo A1 and ATP-binding cassette transporters A1 and G1 gene expression; inhibition of HMG-COA reductase gene expression; anti-inflammatory properties due to Nrf-2 activation, inhibition of IκBα, JNK, ERK1/2, and p38MAPK phosphorylation |
| Qin et al. [193] (2015) | 70 patients with NAFLD (36 patients in fish oil group) | USG | Fish oil in 1g capsules, two capsules twice per day | 3 months | ↑: Adiponectin ↓: TG, TC, apolipoprotein B, glucose, ALT, GGT, TNF- α, FGF21, leukotrienes B, cytokeratin 18 fragment M30, prostaglandin E2 | Anti-inflammatory effects, decrease in NF-kB activity; inhibition of prostaglandin E2 leads to improvements in lipid profile |
| Rahimpour et al. [201] (2022) | 22 overweight women with NAFLD (11 in vitamin D group) | USG | Vitamin D in dose 2000 IU per day + eccentric exhaustive exercise training at the beginning and at the endpoint | 6 weeks | ↓: BW, BMI, WHR, body fat percentage | Increase in lipoprotein lipase activity; inhibition of serum parathyroid hormone; improvement in calcium homeostasis as calcium affects bile acids to excrete fatty acids; improvement in IR; inhibition of lipogenesis and improvement in fatty acid oxidation |
| Pervez et al. [205] (2020) | 71 patients with NAFLD (35 in δ-tocotrienol group) | USG | δ-tocotrienol in dose 300 mg twice a day | 24 weeks | ↓: FLI, HOMA-IR, hs-CRP, MDA, ALT, AST, hepatic steatosis | Upregulation of PPAR α and δ, and downregulation of fatty acid biosynthesis enzymes, e.g., HMGC, which leads to inhibition of adipogenesis; decrease in leptin level; increase in adiponectin |
| Study | Nutraceutical | Composition | Group * | Diagnosis | Duration | Results ** | Possible Mechanism |
|---|---|---|---|---|---|---|---|
| Illnait et al. [206] (2013) | D-002–substance derived from beeswax in dose 50 mg twice a day + low fat, low energy diet | Mixture of six of the higher aliphatic alcohols (C26, C26, C28, C30, C32, and C34) | 44 patients with NAFLD (22 in D-002 group) | USG | 24 weeks | ↑: Plasma total antioxidant status ↓: HOMA-IR, insulin, liver steatosis Normalization of liver echo pattern in USG (7 patients), symptoms improvement (12 patients) | Antioxidant properties; improvement of IR probably through AMP-kinase activation, which leads to metabolic gene regulation and decline of AMP-mediated insulin secretion by pancreatic β-cells |
| Ferro et al. [207] (2022) | Livogen Plus® 6 capsules per day | Doses for 6 capsules: 667 mg of Curcuma longa extract complexed with γ-cyclodextrin, 667 mg of refined fish oil concentrate, 400 mg of BPF and wild type Cynara Cardunculus extract, 334 mg of black seed oil of Nigella sativa, 267 mg of standardized fraction of root of Picrorhiza kurroa, 200 mg reduced GHS and SAMe, 167 mg of Artichoke leaf extract, Indole-3-carbinol and silybin phospholipids, 127 mg of milk thistle fruit dry extract, and other natural compounds | 127 patients with NAFLD (62 in Livogen Plus group) | Transient elastography | 12 weeks | ↓: CAP, DBP, insulin, HOMA-IR Improvement in liver steatosis shown only in subjects with severe NAFLD | Antioxidant properties; prevention of lipid peroxidation; stimulation of mitochondrial β-oxidation |
| Abidov et al. [208] (2010) | Xanthigen™ 3 capsules per day + calorie restricted diet | 100 mg pomegranate seed oil + 100 mg brown marine algae containing 0.8 mg fucoxanthin | 72 obese females with NAFLD (36 in Xanthigen group) | Magnetic hepatic ultrasound scanning + image-guided proton magnetic resonance spectroscopy | 16 weeks | ↓: BW, WC, body fat content, HFC, CRP, TG, ALT, AST, GGT | Promotion of hepatic fatty acids β-oxidation; increase in resting energy expenditure; weight loss, which promotes decrease in inflammatory cytokines |
| Fogacci et al. [209] (2022) | Eufortyn® Colesterolo Plus 1 tablet per day + 1-month Mediterranean diet standardization before start of the study | Doses per tablet: 1000 mg of Phytosome Bergamot Polyphenolic fraction, 100 mg of Cynara cardunculus L. dry extract, 20 mg of Cynara scolymus L. dry extract, 25 mg of Coenzyme Q10 phytosome and 5 mg of zinc | 56 healthy subjects with polygenic hypercholesterolemia (28 in nutraceutical group) | 8 weeks | ↓: TC, LDL-C, LDL-C to HDL-C ratio, hs-CRP, WC, lipid accumulation products, FLI | Anti-inflammatory and antioxidant properties; inhibition of HMG-CoA reductase; interaction with liver SREPBs and ACAT; increase in bile acids excretion to feces; improvements in endothelial function; regulation of VEGF, ET-1, eNOS genes expression | |
| Vilar Gomez et al. [210] (2009) | Viusid oral sachets 50 g per day + hypocaloric diet + aerobic exercise | 666 mg of malic acid 33 mg of glycyrrhizic acid 666 mg of glucosamine 2 mg of calcium pantothenate 20 mg of ascorbic acid 666 mg of arginine 333 mg of glycine 66 μg of folic acid 600 mg of pyrodoxal 0.3 μg of cyanocobalamine 5 mg of zinc sulphate | 60 patients with NAFLD (30 in Viusid group) | Liver biopsy + histology | 6 months | ↓: NAS, histological: steatosis, hepatocyte ballooning and lobular inflammation | Viusid mechanisms of action remain unclear however may be related to improvements in methylation reactions in hepatocytes, e.g., production of glutathione and improvements in cell membrane integrity, anti-inflammatory, and antioxidant properties |
| Study | Preparate + Dosage | Group * | Diagnosis | Duration | Results ** | Possible Mechanism |
|---|---|---|---|---|---|---|
| Kobyliak et al. [213] (2018) | Symbiter (14 genera’s of probiotic species: Bifidobacterium, Lactobacillus, Lactococcus, and Propionibacterium) in dose 10 g per day | 58 patients with T2DM and NAFLD (30 in probiotic group) | USG | 8 weeks | ↓: FLI, AST, GGT, TNF-α, IL-6, TG | Improvements in intestinal microbiota and gut permeability; decrease in JNK activity in liver; reduction in inflammatory markers |
| Ahn et al. [215] (2019) | Probiotic composed with: Lactobacillus acidophilus, L. rhamnosus, L. paracasei, Pediococcus pentosaceus, Bifidobacterium lactis, and B. breve | 68 obese NAFLD patients (32 in probiotics group) | MRI | 12 weeks | ↓: IHF, TG However, after adjusting to BW changes, there were no differences between probiotic and placebo groups | Correction of intestinal dysbiosis by production of lactic acids, promotion of molecular immunity, and changes in intestinal environment |
| Abhari et al. [218] (2020) | 109 Bacillus coagulans spore (GBI-30) plus 0.4 g inulin per day | 53 patients with NAFLD (22 in symbiotic group) | Fibroscan | 12 weeks | ↓: liver steatosis, ALT, GGT, TNF-α, NF-κB | Amelioration of inflammation by reducing pathogenic bacteria in gut and improving intestinal barrier |
| Eslamparast et al. [219] (2014) | Protexin containing 7 strains of bacteria: (Lactobacillus casei, Lactobacillus rhamnosus, Streptococcus thermophilus, Bifidobacterium breve, Lactobacillus acidophilus, Bifidobacterium longum, and Lactobacillus bulgaricus), fructooligosaccharide, probiotic cultures magnesium stearate and a vegetable capsule | 58 patients with NAFLD (26 in symbiotic group) | Fibroscan | 28 weeks | ↓: liver fibrosis score, TNF-α, NF-κB, hs-CRP, GGT, ALT, AST, | Modulation of intestinal microbiota; reduction in serum inflammatory cytokines levels; decrease in JNK and NF-κB activity; improvement in IR through decline of endotoxins and intestinal toxins levels and increasing pH of feces |
| Mofidi et al. [220] (2017) | Protexin (the composition same as line above) | 50 lean NAFLD patients (25 in symbiotic group) | Fibroscan | 28 weeks | ↓: liver fibrosis, liver steatosis, FPG, AST hs-CRP, NF-κB |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kosmalski, M.; Frankowski, R.; Deska, K.; Różycka-Kosmalska, M.; Pietras, T. Exploring the Impact of Nutrition on Non-Alcoholic Fatty Liver Disease Management: Unveiling the Roles of Various Foods, Food Components, and Compounds. Nutrients 2023, 15, 2838. https://doi.org/10.3390/nu15132838
Kosmalski M, Frankowski R, Deska K, Różycka-Kosmalska M, Pietras T. Exploring the Impact of Nutrition on Non-Alcoholic Fatty Liver Disease Management: Unveiling the Roles of Various Foods, Food Components, and Compounds. Nutrients. 2023; 15(13):2838. https://doi.org/10.3390/nu15132838
Chicago/Turabian StyleKosmalski, Marcin, Rafał Frankowski, Kacper Deska, Monika Różycka-Kosmalska, and Tadeusz Pietras. 2023. "Exploring the Impact of Nutrition on Non-Alcoholic Fatty Liver Disease Management: Unveiling the Roles of Various Foods, Food Components, and Compounds" Nutrients 15, no. 13: 2838. https://doi.org/10.3390/nu15132838
APA StyleKosmalski, M., Frankowski, R., Deska, K., Różycka-Kosmalska, M., & Pietras, T. (2023). Exploring the Impact of Nutrition on Non-Alcoholic Fatty Liver Disease Management: Unveiling the Roles of Various Foods, Food Components, and Compounds. Nutrients, 15(13), 2838. https://doi.org/10.3390/nu15132838