
A Retrospective Study of Complications of Enteral Feeding in Critically Ill Children on Noninvasive Ventilation

 ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Results
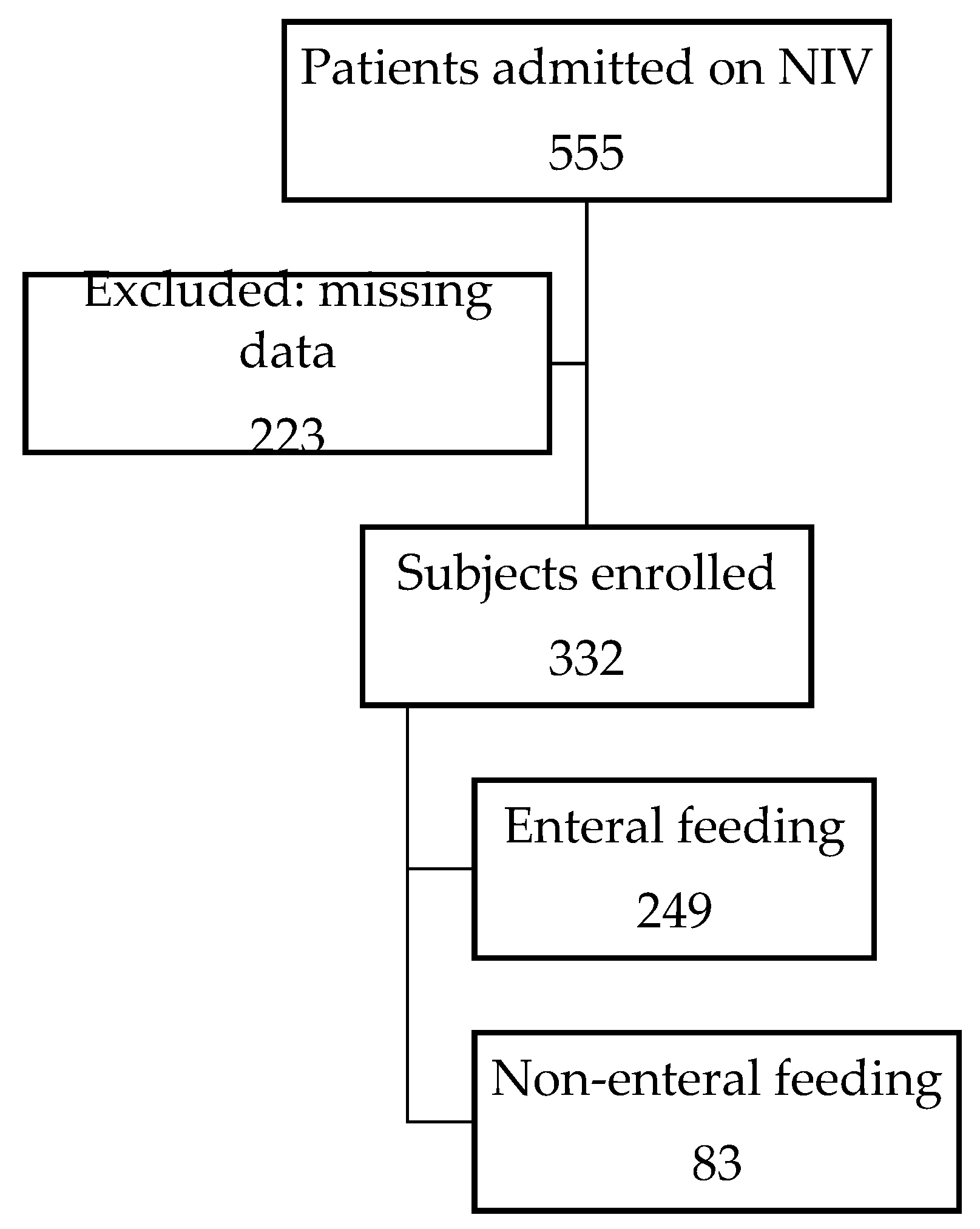
3.1. Demographics
3.2. Description of Vital Signs and Noninvasive Respiratory Support

{kind=link}
{kind=link}
{kind=link}
| Characteristics | Statistic | <1 Year | 1–5 Years | 5–10 Years | >10 Years |
|---|---|---|---|---|---|
| Number of patients | N (%) | 130 (39) | 83 (25) | 46 (14) | 73 (22) |
| Sex, male | N (%) | 85 (65) | 56 (68) | 29 (63) | 34 (47) |
| Weight, kg | MD (Q1, Q3) | 4.6 (3.6, 5.9) | 11 (9.4, 13.9) | 22.2 (18, 25.9) | 43 (32, 55) |
| NIV settings, cmH2O | |||||
| CPAP | MD (Q1, Q3) | 7 (6, 7) | 6 (6, 8) | 7 (6, 8) | 7 (6, 10) |
| BiPAP (EPAP) | MD (Q1, Q3) | 7 (6, 7) | 7 (6, 8) | 7 (6, 8) | 7 (6, 8) |
| BiPAP (IPAP) | MD (Q1, Q3) | 14 (12, 15) | 14 (12, 16) | 14 (12, 14) | 14 (12, 16) |
| FiO2 | MD (Q1, Q3) | 0.3 (0.25, 0.4) | 0.35 (0.25, 0.6) | 0.35 (0.3, 0.45) | 0.35 (0.3, 0.5) |
| Vital signs | |||||
| Heart rate | MD (Q1, Q3) | 143 (131, 161) | 132 (114, 149) | 123 (104, 140) | 115 (93, 138) |
| Respiratory rate | MD (Q1, Q3) | 36 (30, 52) | 34 (25, 41) | 35 (25, 41) | 24 (20, 30) |
| SBP, mmHg | MD (Q1, Q3) | 94 (85, 107) | 105 (94, 115) | 104 (95, 114) | 106 (97, 117) |
| DBP, mmHg | MD (Q1, Q3) | 55 (47, 67) | 59 (48, 71) | 62 (51, 71) | 63 (50, 71) |
| Oxygen saturation, % | MD (Q1, Q3) | 98 (96, 100) | 98 (95, 100) | 97 (95, 98) | 97 (95, 99) |
| On enteral feeds | N (%) | 96 (74) | 65 (78) | 37 (80) | 51 (70) |
| Complication | N (%) | 56 (43.1) | 31 (37.3) | 14 (30.4) | 31 (42.5) |
| PICU LOS, days | MD (Q1, Q3) | 5 (2, 9) | 3 (1, 6) | 2 (1, 4) | 2 (1, 7) |
| Hospital LOS, days | MD (Q1, Q3) | 15 (6, 44) | 8 (4, 24) | 10 (6, 22) | 11 (7, 18) |
| Deaths | N (%) | 5 (4) | 8 (10) | 3 (6) | 5 (7) |
3.3. Complications
3.4. Factors’ Relationship with First Complication
3.5. Factors’ Relationship with Any Complication
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Ibiebele, I.; Algert, C.S.; Bowen, J.R.; Roberts, C.L. Pediatric admissions that include intensive care: A population-based study. BMC Health Serv. Res. 2018, 18, 264. [Google Scholar] [CrossRef] [PubMed]
- Haut, C. Pediatric Noninvasive Ventilation. J. Pediatr. Intensive Care 2015, 4, 121–127. [Google Scholar] [CrossRef]
- Wolfler, A.; Calderini, E.; Iannella, E.; Conti, G.; Biban, P.; Dolcini, A.; Pirozzi, N.; Racca, F.; Pettenazzo, A.; Salvo, I.; et al. Evolution of Noninvasive Mechanical Ventilation Use: A Cohort Study among Italian PICUs. Pediatr. Crit. Care Med. 2015, 16, 418–427. [Google Scholar] [CrossRef] [PubMed]
- Yaman, A.; Kendirli, T.; Ödek, Ç.; Ateş, C.; Taşyapar, N.; Güneş, M.; İnce, E. Efficacy of noninvasive mechanical ventilation in prevention of intubation and reintubation in the pediatric intensive care unit. J. Crit. Care 2016, 32, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Ganu, S.S.; Gautam, A.; Wilkins, B.; Egan, J. Increase in use of non-invasive ventilation for infants with severe bronchiolitis is associated with decline in intubation rates over a decade. Intensive Care Med. 2012, 38, 1177–1183. [Google Scholar] [CrossRef]
- Morley, S.L. Non-invasive ventilation in paediatric critical care. Paediatr. Respir. Rev. 2016, 20, 24–31. [Google Scholar] [CrossRef]
- Egbuta, C.; Easley, R.B. Update on ventilation management in the Pediatric Intensive Care Unit. Paediatr. Anaesth. 2022, 32, 354–362. [Google Scholar] [CrossRef]
- Kogo, M.; Nagata, K.; Morimoto, T.; Ito, J.; Sato, Y.; Teraoka, S.; Fujimoto, D.; Nakagawa, A.; Otsuka, K.; Tomii, K. Enteral Nutrition Is a Risk Factor for Airway Complications in Subjects Undergoing Noninvasive Ventilation for Acute Respiratory Failure. Respir. Care 2017, 62, 459–467. [Google Scholar] [CrossRef]
- Terzi, N.; Darmon, M.; Reignier, J.; Ruckly, S.; Garrouste-Orgeas, M.; Lautrette, A.; Azoulay, E.; Mourvillier, B.; Argaud, L.; Papazian, L.; et al. Initial nutritional management during noninvasive ventilation and outcomes: A retrospective cohort study. Crit. Care 2017, 21, 293. [Google Scholar] [CrossRef]
- Leroue, M.K.; Good, R.J.; Skillman, H.E.; Czaja, A.S. Enteral Nutrition Practices in Critically Ill Children Requiring Noninvasive Positive Pressure Ventilation. Pediatr. Crit. Care Med. 2017, 18, 1093–1098. [Google Scholar] [CrossRef]
- Lenihan, A.; Ramos, V.; Nemec, N.; Lukowski, J.; Lee, J.; Kendall, K.M.; Mahapatra, S. A Retrospective Analysis of Feeding Practices and Complications in Patients with Critical Bronchiolitis on Non-Invasive Respiratory Support. Children 2021, 8, 410. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.M.; Skillman, H.E.; Irving, S.Y.; Coss-Bu, J.A.; Vermilyea, S.; Farrington, E.A.; McKeever, L.; Hall, A.M.; Goday, P.S.; Braunschweig, C. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: Society of Critical Care Medicine and American Society for Parenteral and Enteral Nutrition. JPEN J. Parenter. Enter. Nutr. 2017, 41, 706–742. [Google Scholar] [CrossRef] [PubMed]
- Tume, L.N.; Valla, F.V.; Joosten, K.; Jotterand Chaparro, C.; Latten, L.; Marino, L.V.; Macleod, I.; Moullet, C.; Pathan, N.; Rooze, S.; et al. Nutritional support for children during critical illness: European Society of Pediatric and Neonatal Intensive Care (ESPNIC) metabolism, endocrine and nutrition section position statement and clinical recommendations. Intensive Care Med. 2020, 46, 411–425. [Google Scholar] [CrossRef]
- Canarie, M.F.; Barry, S.; Carroll, C.L.; Hassinger, A.; Kandil, S.; Li, S.; Pinto, M.; Valentine, S.L.; Faustino, E.V.; Northeast Pediatric Critical Care Research Consortium. Risk Factors for Delayed Enteral Nutrition in Critically Ill Children. Pediatr. Crit. Care Med. 2015, 16, e283–e289. [Google Scholar] [CrossRef] [PubMed]
- Sbaih, N.; Hawthorne, K.; Lutes, J.; Cavallazzi, R. Nutrition Therapy in Non-intubated Patients with Acute Respiratory Failure. Curr. Nutr. Rep. 2021, 10, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Halvorson, E.E.; Chandler, N.; Neiberg, R.; Ervin, S.E. Association of NPO Status and Type of Nutritional Support on Weight and Length of Stay in Infants Hospitalized with Bronchiolitis. Hosp. Pediatr. 2013, 3, 366–370. [Google Scholar] [CrossRef] [PubMed]
- Weisgerber, M.C.; Lye, P.S.; Nugent, M.; Li, S.H.; De Fouw, K.; Gedeit, R.; Simpson, P.; Gorelick, M.H. Relationship between caloric intake and length of hospital stay for infants with bronchiolitis. Hosp. Pediatr. 2013, 3, 24–30. [Google Scholar] [CrossRef]
- Singer, P.; Rattanachaiwong, S. To eat or to breathe? The answer is both! Nutritional management during noninvasive ventilation. Crit. Care 2018, 22, 27. [Google Scholar] [CrossRef]
- Shadman, K.A.; Kelly, M.M.; Edmonson, M.B.; Sklansky, D.J.; Nackers, K.; Allen, A.; Barreda, C.B.; Thurber, A.S.; Coller, R.J. Feeding during High-Flow Nasal Cannula for Bronchiolitis: Associations with Time to Discharge. J. Hosp. Med. 2019, 14, E43–E48. [Google Scholar] [CrossRef]
- Tume, L.N.; Valla, F.V. Enteral Feeding in Children on Noninvasive Ventilation Is Feasible, but Clinicians Remain Fearful. Pediatr. Crit. Care Med. 2017, 18, 1175–1176. [Google Scholar] [CrossRef]
- Bambi, S.; Mati, E.; De Felippis, C.; Lucchini, A. Enteral Nutrition during Noninvasive Ventilation: We Should Go Deeper in the Investigation. Respir. Care 2017, 62, 1118–1119. [Google Scholar] [CrossRef] [PubMed]
- Sochet, A.A.; Nunez, M.; Wilsey, M.J.; Morrison, J.M.; Bessone, S.K.; Nakagawa, T.A. Enteral Nutrition Improves Vital Signs in Children with Bronchiolitis on Noninvasive Ventilation. Hosp. Pediatr. 2021, 11, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.M.; McAleer, D.; Hamilton, S.; Naples, E.; Leavitt, K.; Mitchell, P.; Duggan, C. Challenges to optimal enteral nutrition in a multidisciplinary pediatric intensive care unit. JPEN J. Parenter. Enter. Nutr. 2010, 34, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Tume, L.N.; Eveleens, R.D.; Mayordomo-Colunga, J.; López, J.; Verbruggen, S.C.A.T.; Fricaudet, M.; Smith, C.; Garcia Cusco, M.G.; Latten, L.; Valla, F.V.; et al. Enteral Feeding of Children on Noninvasive Respiratory Support: A Four-Center European Study. Pediatr. Crit. Care Med. 2021, 22, e192–e202. [Google Scholar] [CrossRef]
- Alibrahim, O.; Rehder, K.J.; Miller, A.G.; Rotta, A.T. Mechanical Ventilation and Respiratory Support in the Pediatric Intensive Care Unit. Pediatr. Clin. N. Am. 2022, 69, 587–605. [Google Scholar] [CrossRef]
- Komeswaran, K.; Khanal, A.; Powell, K.; Caprirolo, G.; Majcina, R.; Robbs, R.S.; Basnet, S. Enteral Feeding for Children on Bilevel Positive Pressure Ventilation for Status Asthmaticus. J. Pediatr. Intensive Care 2023, 12, 31–36. [Google Scholar] [CrossRef]
- Kogo, M.; Nagata, K.; Morimoto, T.; Ito, J.; Sato, Y.; Teraoka, S.; Fujimoto, D.; Nakagawa, A.; Otsuka, K.; Tomii, K. Enteral Nutrition during Noninvasive Ventilation: We Should Go Deeper in the Investigation—Reply. Respir. Care 2017, 62, 1119–1120. [Google Scholar] [CrossRef]
- Yasuda, H.; Kondo, N.; Yamamoto, R.; Asami, S.; Abe, T.; Tsujimoto, H.; Tsujimoto, Y.; Kataoka, Y. Monitoring of gastric residual volume during enteral nutrition. Cochrane Database Syst. Rev. 2021, 9, CD013335. [Google Scholar] [CrossRef]
- Leder, S.B.; Siner, J.M.; Bizzarro, M.J.; McGinley, B.M.; Lefton-Greif, M.A. Oral Alimentation in Neonatal and Adult Populations Requiring High-Flow Oxygen via Nasal Cannula. Dysphagia 2016, 31, 154–159. [Google Scholar] [CrossRef]
- Reintam Blaser, A.; Starkopf, J.; Alhazzani, W.; Berger, M.M.; Casaer, M.P.; Deane, A.M.; Fruhwald, S.; Hiesmayr, M.; Ichai, C.; Jakob, S.M.; et al. Early enteral nutrition in critically ill patients: ESICM clinical practice guidelines. Intensive Care Med. 2017, 43, 380–398. [Google Scholar] [CrossRef]



| Baseline | New FiO2 |
|---|---|
| <30% | ≥50% |
| 31–40% | ≥60% |
| 51–60% | ≥70% |
| 61–70% | ≥80% |
| 71–80% | ≥90% |
| >80% | 100% |
| Characteristics | Statistic | No Enteral Feeding | Enteral Feeding | p-Value |
|---|---|---|---|---|
| Number of patients | N (%) | 83 (25) | 249 (75) | |
| Sex, male | N (%) | 48 (58) | 156 (62) | 0.43 |
| Age, years | MD (Q1, Q3) | 2 (0.3, 11) | 2 (0.3, 8) | 0.39 |
| Weight, kg | MD (Q1, Q3) | 11 (5, 27) | 10 (5, 24) | 0.96 |
| NIV settings, cmH2O | ||||
| CPAP (EPAP) | MD (Q1, Q3) | 7 (6, 7) | 7 (6, 8) | 0.36 |
| BiPAP (EPAP) | MD (Q1, Q3) | 7 (6, 8) | 7 (6, 8) | 0.94 |
| BiPAP (IPAP) | MD (Q1, Q3) | 14 (12, 16) | 14 (12, 15) | 0.13 |
| FiO2 | MD (Q1, Q3) | 0.35 (0.3, 0.5) | 0.3 (0.25, 0.45) | 0.32 |
| Vital signs | ||||
| Heart rate | MD (Q1, Q3) | 130 (109, 149) | 135 (113, 153) | 0.40 |
| Respiratory rate | MD (Q1, Q3) | 32 (24, 38) | 34 (25, 44) | 0.26 |
| SBP, mmHg | MD (Q1, Q3) | 97 (89, 107) | 103 (91, 114) | 0.12 |
| DBP, mmHg | MD (Q1, Q3) | 55 (46, 64) | 59 (49, 70) | 0.08 |
| Oxygen saturation, % | MD (Q1, Q3) | 97 (95, 100) | 98 (95, 99) | 0.94 |
| PICU length of stay, days | MD (Q1, Q3) | 5 (1, 10) | 3 (1, 6) | 0.02 |
| Hospital length of stay, days | MD (Q1, Q3) | 17 (8, 40) | 10 (5, 22) | 0.26 |
| Deaths | N (%) | 8 (10) | 13 (5) | 0.15 |
| Complication | N (%) | 60 (72) | 72 (29) | <0.01 |
| Vital Signs | Statistic | Feeding Decision | Complication | p-Value |
|---|---|---|---|---|
| Heart rate | MD (Q1, Q3) | 129 (110, 148) | 132 (115, 151) | <0.01 |
| Respiratory rate | MD (Q1, Q3) | 34 (24, 45) | 30 (24, 42) | 0.21 |
| SBP, mmHg | MD (Q1, Q3) | 98 (86, 111) | 100 (87, 112) | 0.07 |
| DBP, mmHg | MD (Q1, Q3) | 55 (46, 67) | 58 (48, 69) | 0.20 |
| Oxygen saturation, % | MD (Q1, Q3) | 97 (93, 99) | 94 (88, 98) | <0.01 |
| Characteristics | Statistic | No Enteral Feeding | Enteral Feeding | p-Value |
|---|---|---|---|---|
| Number of patients | N | 60 | 72 | |
| Sex, male | N (%) | 33 (55) | 51 (71) | 0.06 |
| Age, years | MD (Q1, Q3) | 1 (0.2, 11) | 2 (0.4, 8) | 0.71 |
| Weight, kg | MD (Q1, Q3) | 8 (5, 25) | 10 (5, 22) | 0.76 |
| NIV settings, cmH2O | ||||
| CPAP | MD (Q1, Q3) | 7 (6, 7) | 6 (5, 8) | 0.65 |
| BiPAP (EPAP) | MD (Q1, Q3) | 7 (6, 8) | 7 (6, 8) | 0.35 |
| BiPAP (IPAP) | MD (Q1, Q3) | 14 (12, 16) | 14 (12, 16) | 0.47 |
| FiO2 | MD (Q1, Q3) | 0.35 (0.3, 0.5) | 0.36 (0.3, 0.53) | 0.63 |
| Vital signs | ||||
| Heart rate | MD (Q1, Q3) | 130 (109, 149) | 136 (114, 152) | 0.33 |
| Respiratory rate | MD (Q1, Q3) | 32 (24, 38) | 34 (25, 47) | 0.17 |
| SBP, mmHg | MD (Q1, Q3) | 97 (89, 107) | 97 (86, 112) | 0.89 |
| DBP, mmHg | MD (Q1, Q3) | 55 (46, 64) | 56 (46, 67) | 0.83 |
| Oxygen saturation, % | MD (Q1, Q3) | 97 (95, 99) | 96 (93, 99) | 0.19 |
| PICU length of stay, days | MD (Q1, Q3) | 8 (5, 14) | 6 (3, 12) | 0.21 |
| Hospital length of stay, days | MD (Q1, Q3) | 21 (10, 44) | 15 (8, 39) | 0.99 |
| Deaths | N (%) | 6 (10) | 8 (11) | 0.84 |
| Characteristics | STAT | Complication | No Complication | Univariate | Multivariate | |
|---|---|---|---|---|---|---|
| p | OR | p | ||||
| Number of patients | N | 132 | 200 | |||
| Sex, male | N (%) | 84 (63.6) | 120 (60) | 0.50 | ||
| Age, years | M (±SD) | 4.82 (±5.73) | 4.86 (±5.48) | 0.95 | ||
| Weight, kg | M (±SD) | 17.7 (±18.6) | 18.0 (±17.9) | 0.86 | ||
| NIV, BiPAP | N (%) | 23 (17.4) | 96 (48) | <0.01 | 5.33 | <0.01 |
| NIV settings, cmH2O | N (%) | 109 (82.6) | 104 (52) | |||
| CPAP (EPAP) | M (±SD) | 7 (±2) | 7 (±1) | 0.26 | ||
| BiPAP (EPAP) | M (±SD) | 7 (±1) | 7 (±1) | 0.22 | ||
| BiPAP (IPAP) | M (±SD) | 14 (±2) | 13 (±2) | 0.12 | ||
| FiO2 | M (±SD) | 0.42 (±0.18) | 0.35 (±0.17) | <0.01 | 6.00 | 0.03 |
| No enteral feeds | N (%) | 60 (45) | 23 (11.5) | <0.01 | 0.01 | 1.00 |
| Feeds rate, mL/kg | ||||||
| 1 h | M (±SD) | 3.84 (±4.78) | 6.81 (±5.87) | <0.01 | 0.90 | 0.21 |
| 4 h | M (±SD) | 9.95 (±9.25) | 15.12 (±12.8) | <0.01 | 0.95 | 0.16 |
| Vital signs | ||||||
| Heart rate | M (±SD) | 132 (±29) | 133 (±30) | 0.91 | ||
| Respiratory rate | M (±SD) | 36 (±16) | 35 (±33) | 0.90 | ||
| SBP, mmHg | M (±SD) | 98 (±16) | 104 (±17) | <0.01 | 0.98 | 0.05 |
| DBP, mmHg | M (±SD) | 57 (±15) | 62 (±16) | <0.01 | 0.99 | 0.39 |
| Oxygen saturation, % | M (±SD) | 95 (±5) | 97 (±5) | <0.01 | 0.96 | 0.22 |
| Characteristics | STAT | Complication | No Complication | Univariate | Multivariate | |
|---|---|---|---|---|---|---|
| p | OR | p | ||||
| Number of events | N | 290 | 200 | |||
| No enteral feeds | N (%) | 104 (36) | 23 (11.5) | <0.01 | 3.56 | <0.01 |
| Feeds rate, mL/kg | ||||||
| 1 h | M (±SD) | 3.30 (±4.91) | 6.03 (±5.94) | <0.01 | 0.92 | 0.12 |
| 4 h | M (±SD) | 8.36 (±11) | 13.39 (±13) | <0.01 | 1.01 | 0.79 |
| Vital signs | ||||||
| Heart rate | M (±SD) | 132 (±27) | 126 (±23) | 0.01 | 1.01 | 0.12 |
| Respiratory rate | M (±SD) | 35 (±15) | 34 (±11) | 0.6 | ||
| SBP, mmHg | M (±SD) | 100 (±17) | 102 (±14) | 0.09 | 1 | 0.74 |
| DBP, mmHg | M (±SD) | 59 (±15) | 59 (±10) | 0.59 | ||
| Oxygen saturation, % | M (±SD) | 91 (±13) | 97 (±4) | <0.01 | 0.82 | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sierra-Colomina, M.; Yehia, N.A.; Mahmood, F.; Parshuram, C.; Mtaweh, H. A Retrospective Study of Complications of Enteral Feeding in Critically Ill Children on Noninvasive Ventilation. Nutrients 2023, 15, 2817. https://doi.org/10.3390/nu15122817
Sierra-Colomina M, Yehia NA, Mahmood F, Parshuram C, Mtaweh H. A Retrospective Study of Complications of Enteral Feeding in Critically Ill Children on Noninvasive Ventilation. Nutrients. 2023; 15(12):2817. https://doi.org/10.3390/nu15122817
Chicago/Turabian StyleSierra-Colomina, Montserrat, Nagam Anna Yehia, Farhan Mahmood, Christopher Parshuram, and Haifa Mtaweh. 2023. "A Retrospective Study of Complications of Enteral Feeding in Critically Ill Children on Noninvasive Ventilation" Nutrients 15, no. 12: 2817. https://doi.org/10.3390/nu15122817
APA StyleSierra-Colomina, M., Yehia, N. A., Mahmood, F., Parshuram, C., & Mtaweh, H. (2023). A Retrospective Study of Complications of Enteral Feeding in Critically Ill Children on Noninvasive Ventilation. Nutrients, 15(12), 2817. https://doi.org/10.3390/nu15122817