


Lipid Peroxidation and Antioxidative Capacity Are Unaltered in Transitional Breast Milk Exposed to Light from Women Giving Birth to Preterm Infants before 32 Weeks of Gestation
 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
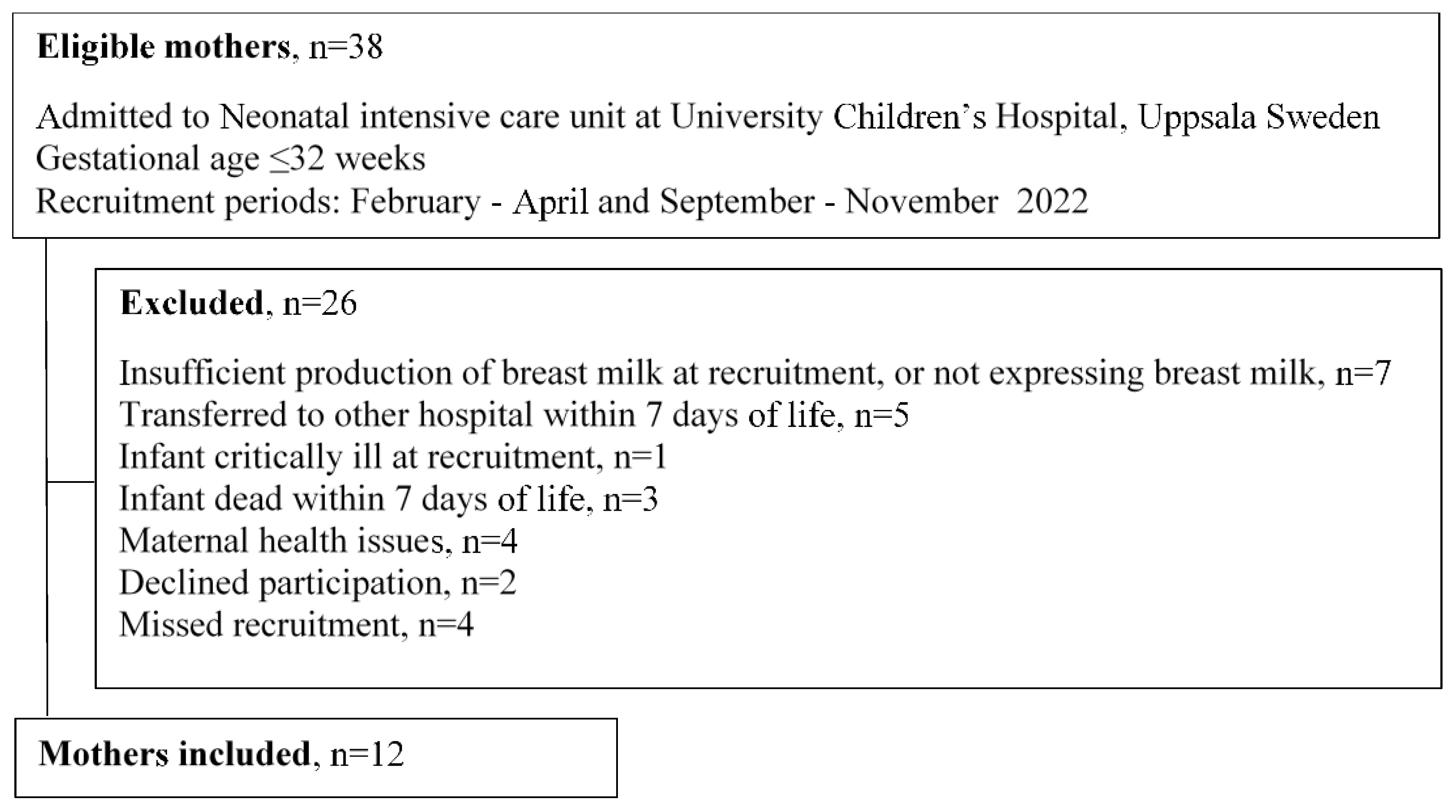
2.1. Subjects
2.2. Collection of Breast Milk
2.3. Light Exposure of Breast Milk
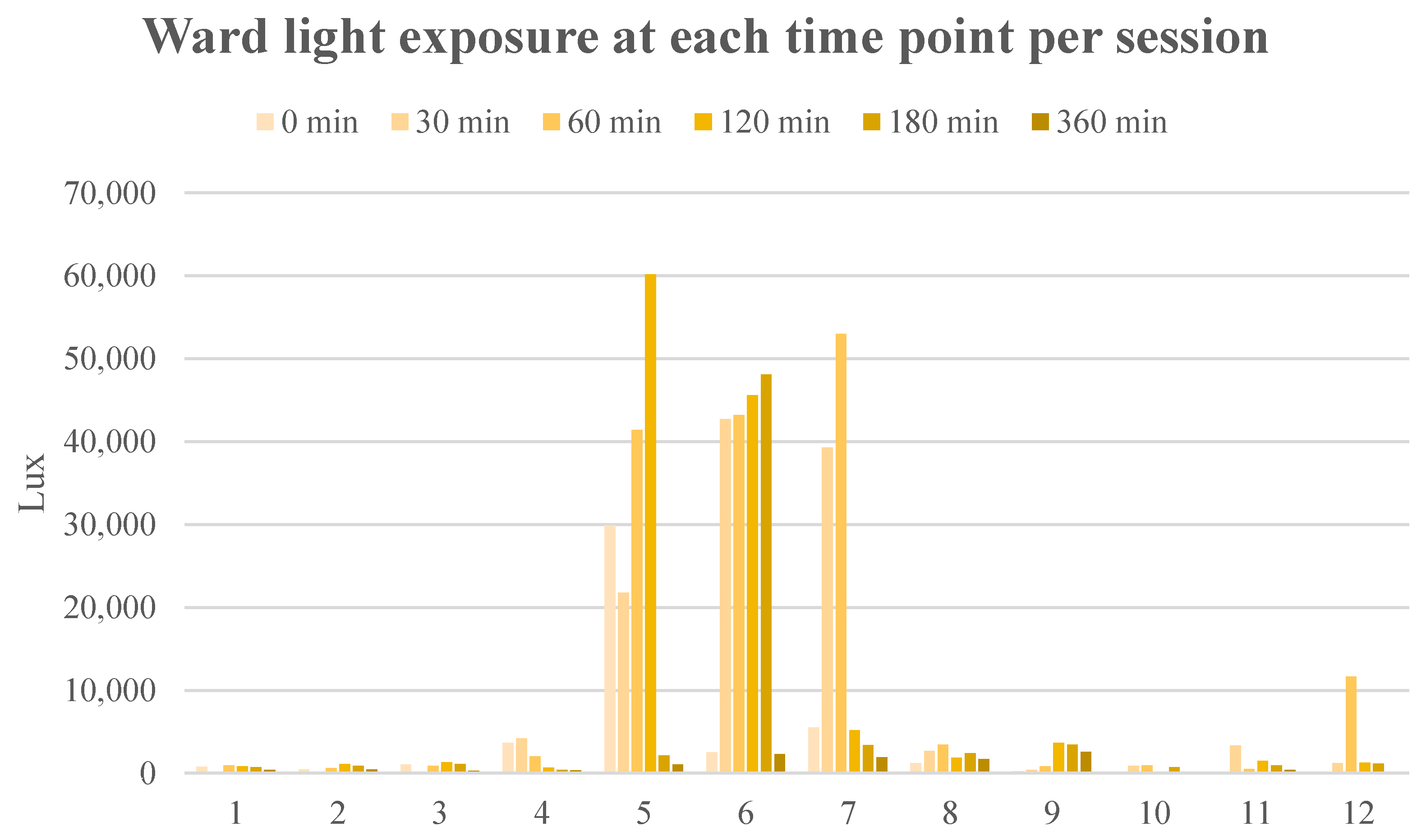
2.3.1. Light Exposure Measurements
2.3.2. Syringe Samples Kept at Room Temperature
- A.
- 5 × 1 mL syringes light-protected with aluminum foil.
- B.
- 5 × 1 mL syringes exposed to standard daytime lighting in the NICU.
- C.
- 5 × 1 mL syringes exposed to phototherapy with two light sources: one was 38 cm above and one was directly underneath (Giraffe® Blue Spot PT Lite, GE Healthcare, Chicago, IL, USA and BiliSoft® Blue LED Fiberoptic Blanket Phototherapy, GE Healthcare, Chicago, IL, USA, respectively).
2.3.3. Nasogastric Tube Administration Simulation
2.4. Breast Milk Quantification of Lipid Peroxides, Antioxidants and Macro-Nutrient Content
2.4.1. Lipid Peroxides
Malondialdehyde
4-Hydroxynonenal
2.4.2. Total Antioxidant Capacity
2.4.3. Macro-Nutrient Content
2.5. Statistical Analysis
3. Results
3.1. Subjects
3.2. Breast Milk Analysis
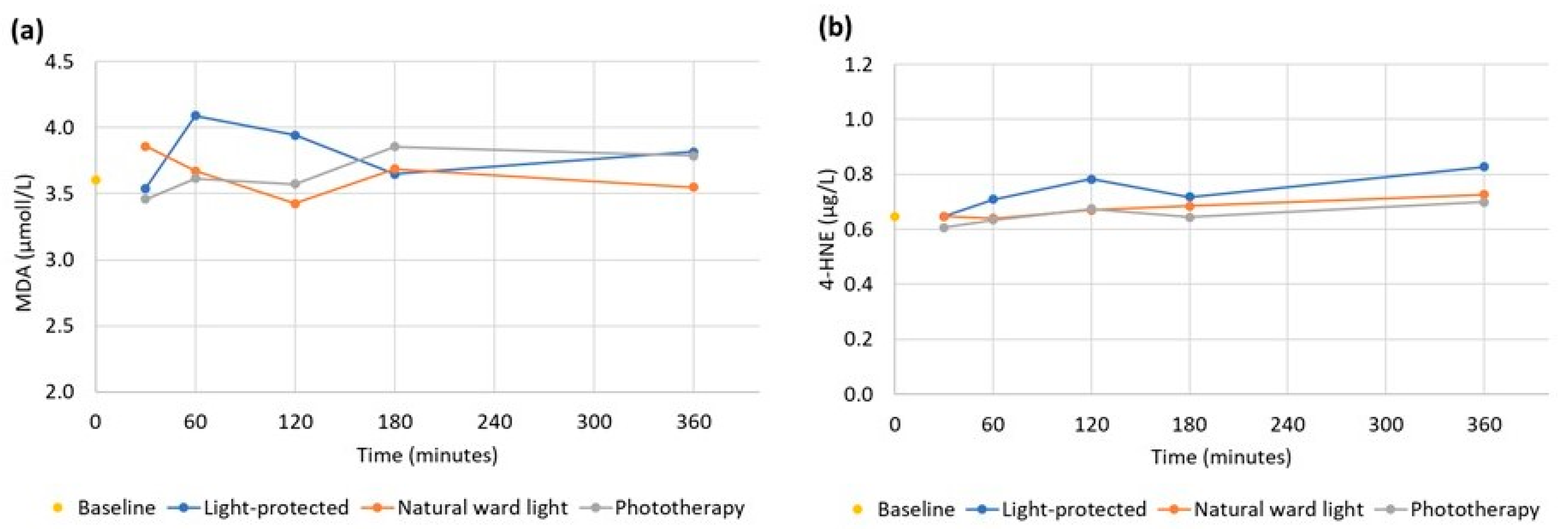
3.2.1. Lipid Peroxides
MDA Syringe Samples
MDA Nasogastric Tube Samples
4-HNE Syringe Samples
4-HNE Nasogastric Tube Samples
3.2.2. Total Antioxidative Capacity
TAC Syringe Samples
TAC Nasogastric Tube Samples
3.2.3. Macro-Nutrient Content in the Breast Milk
3.3. Light Meter Results
4. Discussion
4.1. Lipid Peroxides
4.2. Total Antioxidant Capacity
4.3. Macro-Nutrient Content
4.4. Storage Time/Light Conditions
4.5. Strengths and Weaknesses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Breastfeeding WPRO. Available online: https://www.who.int/westernpacific/health-topics/breastfeeding (accessed on 7 May 2023).
- Nuzzi, G.; Trambusti, I.; DI Cicco, M.E.; Peroni, D.G. Breast Milk: More than Just Nutrition! Minerva Pediatr. 2021, 73, 111–114. [Google Scholar] [CrossRef] [PubMed]
- Friel, J.K.; Martin, S.M.; Langdon, M.; Herzberg, G.R.; Buettner, G.R. Milk from Mothers of Both Premature and Full-Term Infants Provides Better Antioxidant Protection than Does Infant Formula. Pediatr. Res. 2002, 51, 612–618. [Google Scholar] [CrossRef] [PubMed]
- Hård, A.; Nilsson, A.K.; Lund, A.; Hansen-Pupp, I.; Smith, L.E.H.; Hellström, A. Review Shows That Donor Milk Does Not Promote the Growth and Development of Preterm Infants as Well as Maternal Milk. Acta Paediatr. 2019, 108, 998–1007. [Google Scholar] [CrossRef] [PubMed]
- Hanson, C.; Lyden, E.; Furtado, J.; Van Ormer, M.; Anderson-Berry, A. A Comparison of Nutritional Antioxidant Content in Breast Milk, Donor Milk, and Infant Formulas. Nutrients 2016, 8, 681. [Google Scholar] [CrossRef]
- Ballard, O.; Morrow, A.L. Human Milk Composition: Nutrients and Bioactive Factors. Pediatr. Clin. N. Am. 2013, 60, 49–74. [Google Scholar] [CrossRef]
- Andreas, N.J.; Kampmann, B.; Mehring Le-Doare, K. Human Breast Milk: A Review on Its Composition and Bioactivity. Early Hum. Dev. 2015, 91, 629–635. [Google Scholar] [CrossRef]
- Marnett, L.J. Lipid Peroxidation—DNA Damage by Malondialdehyde. Mutat. Res. Mol. Mech. Mutagen. 1999, 424, 83–95. [Google Scholar] [CrossRef]
- Ayala, A.; Muñoz, M.F.; Argüelles, S. Lipid Peroxidation: Production, Metabolism, and Signaling Mechanisms of Malondialdehyde and 4-Hydroxy-2-Nonenal. Oxid. Med. Cell. Longev. 2014, 2014, 360438. [Google Scholar] [CrossRef]
- Esterbauer, H.; Eckl, P.; Ortner, A. Possible Mutagens Derived from Lipids and Lipid Precursors. Mutat. Res. Genet. Toxicol. 1990, 238, 223–233. [Google Scholar] [CrossRef]
- Gila-Diaz, A.; Arribas, S.M.; Algara, A.; Martín-Cabrejas, M.A.; López de Pablo, Á.L.; Sáenz de Pipaón, M.; Ramiro-Cortijo, D. A Review of Bioactive Factors in Human Breastmilk: A Focus on Prematurity. Nutrients 2019, 11, 1307. [Google Scholar] [CrossRef]
- Autor, A.P.; Frank, L.; Roberts, R.J. Developmental Characteristics of Pulmonary Superoxide Dismutase: Relationship to Idiopathic Respiratory Distress Syndrome. Pediatr. Res. 1976, 10, 154–158. [Google Scholar] [CrossRef]
- Poggi, C.; Dani, C. Antioxidant Strategies and Respiratory Disease of the Preterm Newborn: An Update. Oxid. Med. Cell. Longev. 2014, 2014, 721043. [Google Scholar] [CrossRef]
- Gitto, E.; Pellegrino, S.; D’Arrigo, S.; Barberi, I.; Reiter, R.J. Oxidative Stress in Resuscitation and in Ventilation of Newborns. Eur. Respir. J. 2009, 34, 1461–1469. [Google Scholar] [CrossRef] [PubMed]
- El-Farrash, R.A.; El-Shimy, M.S.; Tawfik, S.; Nada, A.S.; Salem, D.A.D.; Gallo, M.S.M.; Abd-Elmohsen, E.W. Effect of Phototherapy on Oxidant/Antioxidant Status: A Randomized Controlled Trial. Free Radic. Res. 2019, 53, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Perez, M.; Robbins, M.E.; Revhaug, C.; Saugstad, O.D. Oxygen Radical Disease in the Newborn, Revisited: Oxidative Stress and Disease in the Newborn Period. Free Radic. Biol. Med. 2019, 142, 61–72. [Google Scholar] [CrossRef]
- Elkabany, Z.A.; El-Farrash, R.A.; Shinkar, D.M.; Ismail, E.A.; Nada, A.S.; Farag, A.S.; Elsayed, M.A.; Salama, D.H.; Macken, E.L.; Gaballah, S.A. Oxidative Stress Markers in Neonatal Respiratory Distress Syndrome: Advanced Oxidation Protein Products and 8-Hydroxy-2-Deoxyguanosine in Relation to Disease Severity. Pediatr. Res. 2020, 87, 74–80. [Google Scholar] [CrossRef]
- Negi, R.; Pande, D.; Karki, K.; Kumar, A.; Khanna, R.S.; Khanna, H.D. A Novel Approach to Study Oxidative Stress in Neonatal Respiratory Distress Syndrome. BBA Clin. 2014, 3, 65–69. [Google Scholar] [CrossRef]
- Hoff, D.S.; Michaelson, A.S. Effects of Light Exposure on Total Parenteral Nutrition and Its Implications in the Neonatal Population. J. Pediatr. Pharmacol. Ther. JPPT 2009, 14, 132–143. [Google Scholar] [CrossRef] [PubMed]
- Chessex, P.; Laborie, S.; Lavoie, J.-C.; Rouleau, T. Photoprotection of Solutions of Parenteral Nutrition Decreases the Infused Load as Well as the Urinary Excretion of Peroxides in Premature Infants. Semin. Perinatol. 2001, 25, 55–59. [Google Scholar] [CrossRef]
- Chessex, P.; Laborie, S.; Nasef, N.; Masse, B.; Lavoie, J.-C. Shielding Parenteral Nutrition From Light Improves Survival Rate in Premature Infants. J. Parenter. Enter. Nutr. 2017, 41, 378–383. [Google Scholar] [CrossRef]
- Hartman, C.; Shamir, R.; Simchowitz, V.; Lohner, S.; Cai, W.; Decsi, T.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; et al. ESPGHAN/ESPEN/ESPR/CSPEN Guidelines on Pediatric Parenteral Nutrition: Complications. Clin. Nutr. 2018, 37, 2418–2429. [Google Scholar] [CrossRef]
- Lapillonne, A.; Mis, N.F.; Goulet, O.; van den Akker, C.H.P.; Wu, J.; Koletzko, B.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; et al. ESPGHAN/ESPEN/ESPR/CSPEN Guidelines on Pediatric Parenteral Nutrition: Lipids. Clin. Nutr. 2018, 37, 2324–2336. [Google Scholar] [CrossRef] [PubMed]
- Unal, S.; Demirel, N.; Yaprak Sul, D.; Ulubas Isik, D.; Erol, S.; Neselioglu, S.; Erel, O.; Bas, A.Y. The Consequence of Phototherapy Exposure on Oxidative Stress Status of Expressed Human Milk. J. Matern. Fetal Neonatal Med. 2019, 32, 46–50. [Google Scholar] [CrossRef] [PubMed]
- van Zoeren-Grobben, D.; Moison, R.M.; Ester, W.M.; Berger, H.M. Lipid Peroxidation in Human Milk and Infant Formula: Effect of Storage, Tube Feeding and Exposure to Phototherapy. Acta Paediatr. 1993, 82, 645–649. [Google Scholar] [CrossRef]
- Abcam Lipid Peroxidation (MDA) Assay Kit. Available online: https://www.abcam.com/ps/products/-118/ab118970/documents/Lipid-Peroxidation-MDA-assay-protocol-book-v11f-ab118970%20(website).pdf (accessed on 7 May 2023).
- Nordic Biosite Human 4-HNE(4-Hydroxynonenal) ELISA Kit. Available online: https://nordicbiosite.com/product/EKX-W727S9-96/Human-4HNE4Hydroxynonenal-ELISA-Kit (accessed on 7 May 2023).
- Abcam Total Antioxidant Capacity Assay Kit. Available online: https://www.abcam.com/ps/products/65/ab65329/documents/-total-antioxidant-capacity-assay-kit-protocol-book-v11-ab65329%20(website).pdf (accessed on 7 May 2023).
- Casadio, Y.S.; Williams, T.M.; Lai, C.T.; Olsson, S.E.; Hepworth, A.R.; Hartmann, P.E. Evaluation of a Mid-Infrared Analyzer for the Determination of the Macronutrient Composition of Human Milk. J. Hum. Lact. 2010, 26, 376–383. [Google Scholar] [CrossRef]
- Cardoso, M.; Virella, D.; Papoila, A.L.; Alves, M.; Macedo, I.; E Silva, D.; Pereira-da-Silva, L. Individualized Fortification Based on Measured Macronutrient Content of Human Milk Improves Growth and Body Composition in Infants Born Less than 33 Weeks: A Mixed-Cohort Study. Nutrients 2023, 15, 1533. [Google Scholar] [CrossRef]
- Nessel, I.; De Rooy, L.; Khashu, M.; Murphy, J.L.; Dyall, S.C. Long-Chain Polyunsaturated Fatty Acids and Lipid Peroxidation Products in Donor Human Milk in the United Kingdom: Results From the LIMIT 2-Centre Cross-Sectional Study. JPEN J. Parenter. Enter. Nutr. 2020, 44, 1501–1509. [Google Scholar] [CrossRef]
- Picaud, J.C.; Steghens, J.P.; Auxenfans, C.; Barbieux, A.; Laborie, S.; Claris, O. Lipid Peroxidation Assessment by Malondialdehyde Measurement in Parenteral Nutrition Solutions for Newborn Infants: A Pilot Study. Acta Paediatr. 2004, 93, 241–245. [Google Scholar] [CrossRef]
- Miloudi, K.; Comte, B.; Rouleau, T.; Montoudis, A.; Levy, E.; Lavoie, J.-C. The Mode of Administration of Total Parenteral Nutrition and Nature of Lipid Content Influence the Generation of Peroxides and Aldehydes. Clin. Nutr. Edinb. Scotl. 2012, 31, 526–534. [Google Scholar] [CrossRef] [PubMed]
- Păduraru, L.; Dimitriu, D.C.; Avasiloaiei, A.L.; Moscalu, M.; Zonda, G.I.; Stamatin, M. Total Antioxidant Status in Fresh and Stored Human Milk from Mothers of Term and Preterm Neonates. Pediatr. Neonatol. 2018, 59, 600–605. [Google Scholar] [CrossRef]
- Akdag, A.; Sari, F.N.; Dizdar, E.A.; Uras, N.; Isikoglu, S.; Erel, O.; Dilmen, U. Storage at −80 °C Preserves the Antioxidant Capacity of Preterm Human Milk. J. Clin. Lab. Anal. 2014, 28, 415–418. [Google Scholar] [CrossRef] [PubMed]
- Silvestre, D.; Miranda, M.; Muriach, M.; Almansa, I.; Jareño, E.; Romero, F.J. Frozen Breast Milk at -20 Degrees C and -80 Degrees C: A Longitudinal Study of Glutathione Peroxidase Activity and Malondialdehyde Concentration. J. Hum. Lact. 2010, 26, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Sari, F.N.; Akdag, A.; Dizdar, E.A.; Uras, N.; Erdeve, O.; Erel, O.; Dilmen, U. Antioxidant Capacity of Fresh and Stored Breast Milk: Is −80 °C Optimal Temperature for Freeze Storage? J. Matern. Fetal Neonatal Med. 2012, 25, 777–782. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean (SD) | Median (Range) | n (%) | |
|---|---|---|---|
| Maternal characteristics: | |||
| Age (years) | 29.7 (6.6) | 28.5 (18–42) | - |
| Pre-pregnancy BMI | 26.2 (8.4) | 22.7 (17.3–42) | - |
| Mode of delivery cesarean section | 10 (83%) | ||
| Infant characteristics: | |||
| Girls | - | - | 8 (66%) |
| Weight (g) | 1095 (435) | 1038 (545–1717) | - |
| Length (cm) | 36.3 (3.9) | 36.5 (30–41) | - |
| Head circumference (cm) | 25.8 (3.3) | 26 (20–31) | - |
| Gestational age (weeks + days) | 28 + 1 (2 + 2) | 28 + 2 (24 + 5–31 + 0) | - |
| Postnatal age at study (days) | 9.1 (2.2) | 9 (6–13) | - |
| Nutrient | Mean ± SD | Median | Range | Pearson’s Coefficient Correlations r | ||
|---|---|---|---|---|---|---|
| MDA | 4-HNE | TAC | ||||
| Lipid (g) | 4.12 ± 1.4 | 4.18 | 1.5–7.3 | 0.69 | 0.65 | 0.46 |
| Protein (g) | 1.65 ± 0.3 | 1.60 | 1.1–2.2 | 0.50 | 0.54 | 0.33 |
| Lactose (g) | 7.93 ± 0.2 | 7.85 | 7.6–8.3 | −0.31 | −0.20 | −0.51 |
| Energy (kcal) | 78.7 ± 14 | 78.0 | 53–111 | 0.67 | 0.64 | 0.43 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Norrgrann, M.; Hörnfeldt, M.; Latheef, F.; Blomqvist, Y.T.; Larsson, A.; Paulsson, M.; Diderholm, B. Lipid Peroxidation and Antioxidative Capacity Are Unaltered in Transitional Breast Milk Exposed to Light from Women Giving Birth to Preterm Infants before 32 Weeks of Gestation. Nutrients 2023, 15, 2818. https://doi.org/10.3390/nu15122818
Norrgrann M, Hörnfeldt M, Latheef F, Blomqvist YT, Larsson A, Paulsson M, Diderholm B. Lipid Peroxidation and Antioxidative Capacity Are Unaltered in Transitional Breast Milk Exposed to Light from Women Giving Birth to Preterm Infants before 32 Weeks of Gestation. Nutrients. 2023; 15(12):2818. https://doi.org/10.3390/nu15122818
Chicago/Turabian StyleNorrgrann, Moa, Malin Hörnfeldt, Faiza Latheef, Ylva Thernström Blomqvist, Anders Larsson, Mattias Paulsson, and Barbro Diderholm. 2023. "Lipid Peroxidation and Antioxidative Capacity Are Unaltered in Transitional Breast Milk Exposed to Light from Women Giving Birth to Preterm Infants before 32 Weeks of Gestation" Nutrients 15, no. 12: 2818. https://doi.org/10.3390/nu15122818
APA StyleNorrgrann, M., Hörnfeldt, M., Latheef, F., Blomqvist, Y. T., Larsson, A., Paulsson, M., & Diderholm, B. (2023). Lipid Peroxidation and Antioxidative Capacity Are Unaltered in Transitional Breast Milk Exposed to Light from Women Giving Birth to Preterm Infants before 32 Weeks of Gestation. Nutrients, 15(12), 2818. https://doi.org/10.3390/nu15122818