
Multivitamin/Multimineral Supplementation Prevents or Reverses Decline in Vitamin Biomarkers and Cellular Energy Metabolism in Healthy Older Men: A Randomized, Double-Blind, Placebo-Controlled Study

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
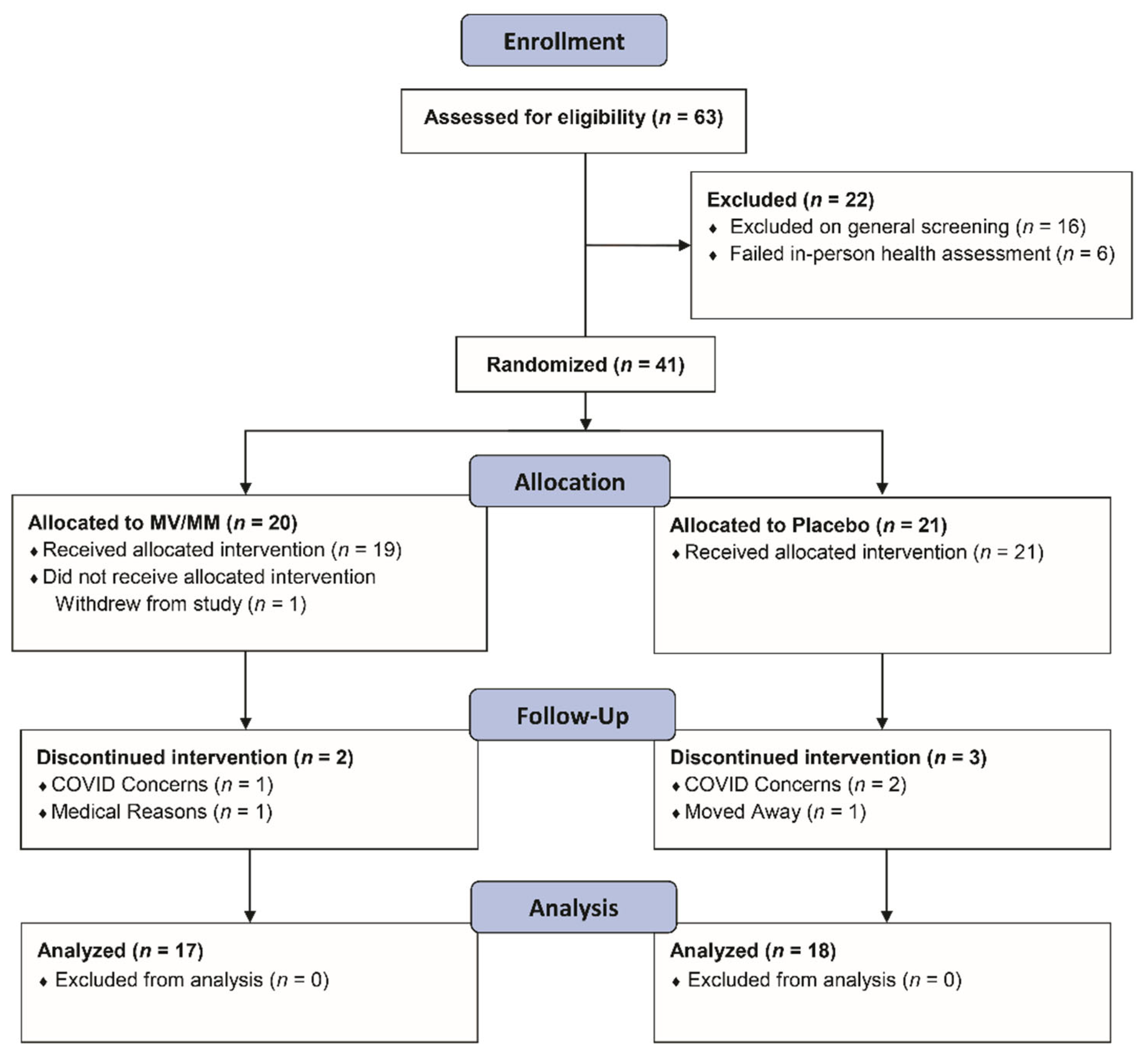
2.1. Study Design
2.2. Participants
2.3. Primary and Secondary Outcomes
2.4. Statistics
3. Results
3.1. Healthy Older Men Have Suboptimal to Optimal Micronutrient Intake and Vitamin Biomarker Status
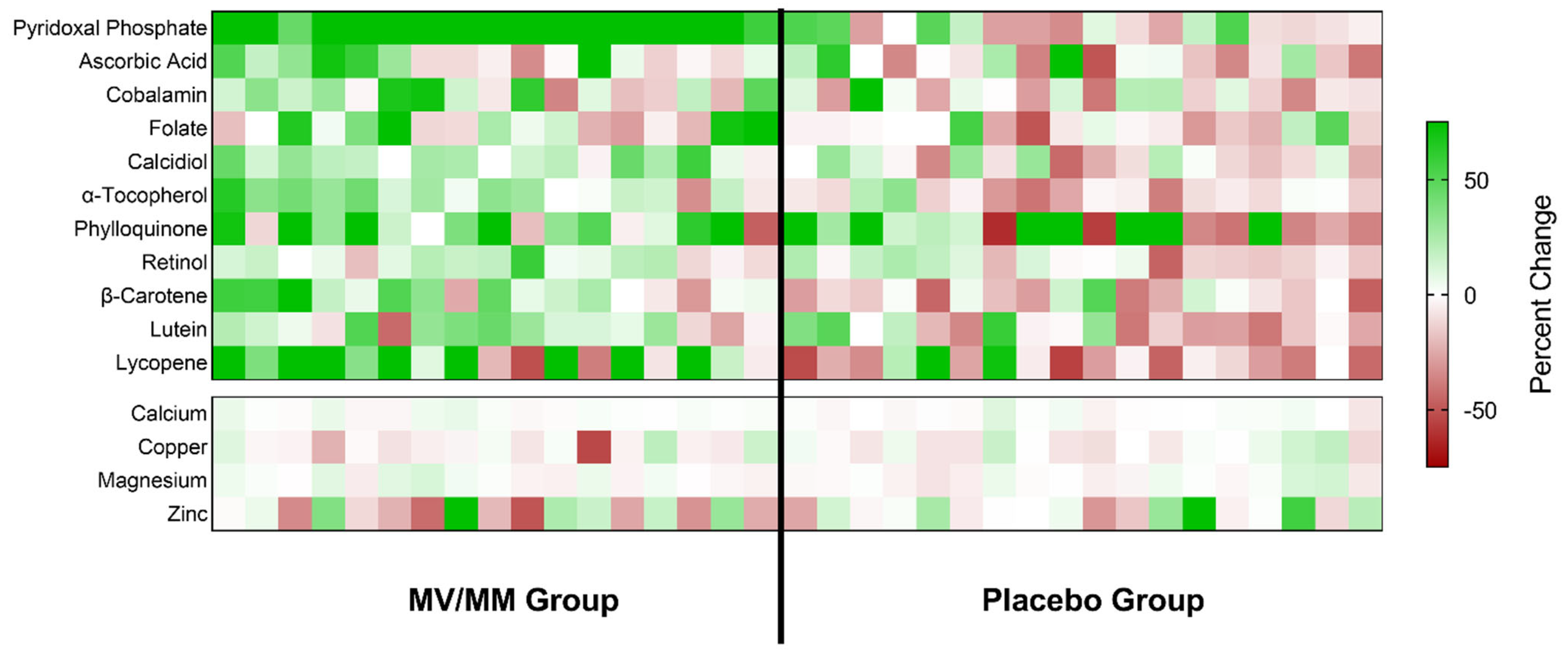
3.2. MV/MM Supplementation Improves and/or Prevents Declines in Blood Vitamin Biomarker Status
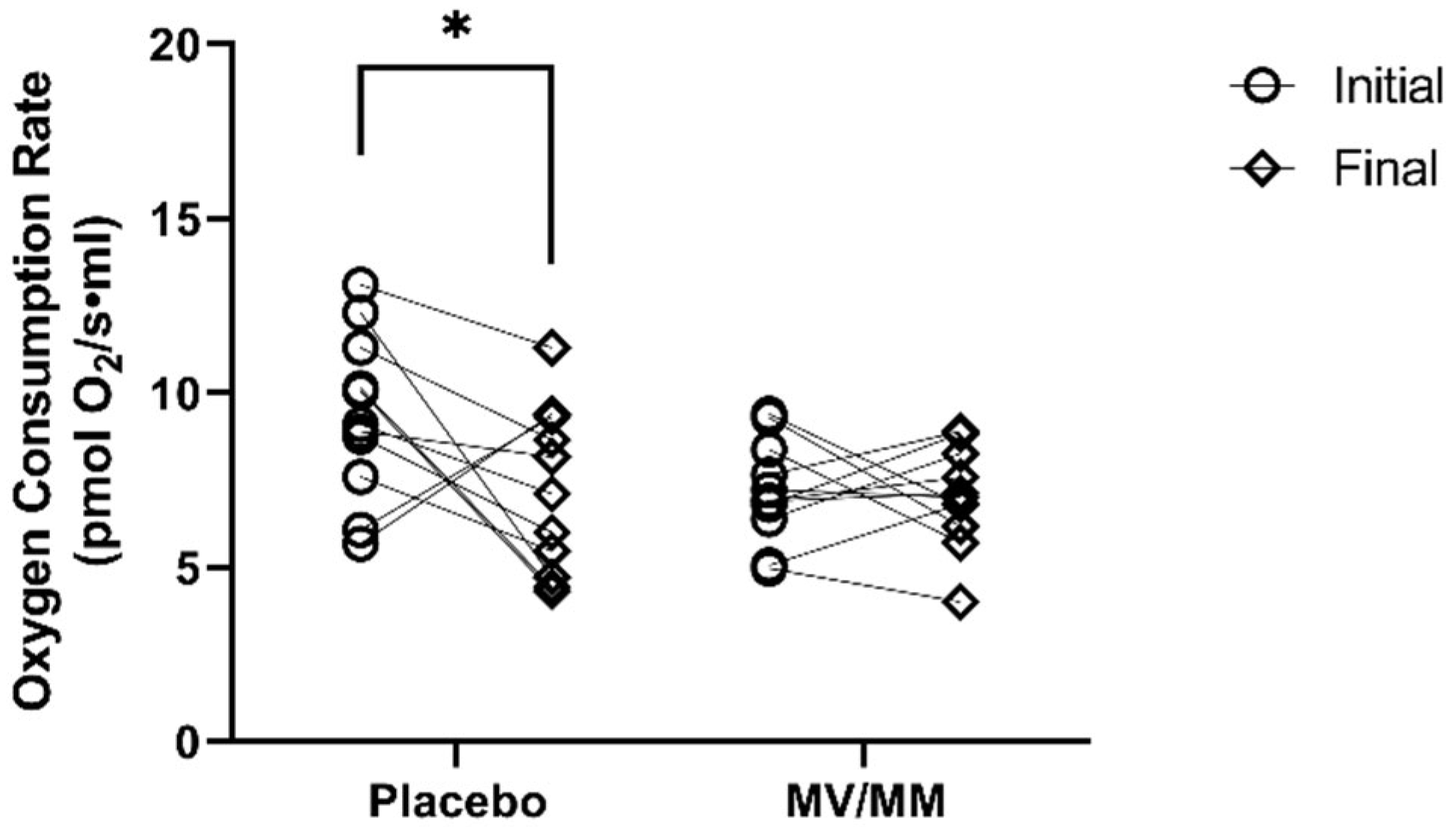
3.3. MV/MM Supplementation Prevents Decline in Cellular O2 Consumption
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bienz, D.; Cori, H.; Hornig, D. Adequate dosing of micronutrients for different age groups in the life cycle. Food Nutr. Bull. 2003, 24, S7–S15. [Google Scholar] [CrossRef] [PubMed]
- Blumberg, J.B.; Frei, B.B.; Fulgoni, V.L.; Weaver, C.M.; Zeisel, S.H. Impact of Frequency of Multi-Vitamin/Multi-Mineral Supplement Intake on Nutritional Adequacy and Nutrient Deficiencies in U.S. Adults. Nutrients 2017, 9, 849. [Google Scholar] [CrossRef] [PubMed]
- Taani, M.H.; Apchemengich, I.; Sima, C.D. Malnutrition–Sarcopenia Syndrome and Self-Management Behaviors in Continuing-Care Retirement Community Residents. Geriatrics 2021, 7, 9. [Google Scholar] [CrossRef]
- Dickerson, R.N. Protein Requirements during Hypocaloric Nutrition for the Older Patient With Critical Illness and Obesity: An Approach to Clinical Practice. Nutr. Clin. Pract. 2020, 35, 617–626. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, M.L.; Coppinger, T.; Lacey, S.; Arsenic, T.; McCarthy, A.L. The nutritional status and dietary intake of free-living seniors: A cross-sectional study. Clin. Nutr. ESPEN 2021, 43, 478–486. [Google Scholar] [CrossRef]
- Bailey, R.L.; Gahche, J.J.; Lentino, C.V.; Dwyer, J.T.; Engel, J.S.; Thomas, P.R.; Betz, J.M.; Sempos, C.T.; Picciano, M.F. Dietary supplement use in the United States, 2003–2006. J. Nutr. 2011, 141, 261–266. [Google Scholar] [CrossRef]
- Wallace, T.C.; McBurney, M.; Fulgoni, V.L., 3rd. Multivitamin/mineral supplement contribution to micronutrient intakes in the United States, 2007–2010. J. Am. Coll. Nutr. 2014, 33, 94–102. [Google Scholar] [CrossRef]
- Wallace, T.C.; Frankenfeld, C.L.; Frei, B.; Shah, A.V.; Yu, C.-R.; Van Klinken, B.J.-W.; Adeleke, M. Multivitamin/Multimineral Supplement Use is Associated with Increased Micronutrient Intakes and Biomarkers and Decreased Prevalence of Inadequacies and Deficiencies in Middle-Aged and Older Adults in the United States. J. Nutr. Gerontol. Geriatr. 2019, 38, 307–328. [Google Scholar] [CrossRef]
- Krasinski, S.D.; Russell, R.M.; Samloff, I.M.; Jacob, R.A.; Dallal, G.E.; McGandy, R.B.; Hartz, S.C. Fundic Atrophic Gastritis in an Elderly Population: Effect on Hemoglobin and Several Serum Nutritional Indicators. J. Am. Geriatr. Soc. 1986, 34, 800–806. [Google Scholar] [CrossRef]
- Kasper, H. Vitamin absorption in the elderly. Int. J. Vitam. Nutr. Res. 1999, 69, 169–172. [Google Scholar] [CrossRef]
- Morley, J.E. Decreased food intake with aging. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56 (Suppl. 2), 81–88. [Google Scholar] [CrossRef] [PubMed]
- Porter, K.M.; Hoey, L.; Hughes, C.F.; Ward, M.; Clements, M.; Strain, J.; Cunningham, C.; Casey, M.C.; Tracey, F.; O’Kane, M.; et al. Associations of atrophic gastritis and proton-pump inhibitor drug use with vitamin B-12 status, and the impact of fortified foods, in older adults. Am. J. Clin. Nutr. 2021, 114, 1286–1294. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, A.M.L.; Dynesen, A.W.; Heitmann, B.L. Older age, smoking, tooth loss and denture-wearing but neither xerostomia nor salivary gland hypofunction are associated with low intakes of fruit and vegetables in older Danish adults. J. Nutr. Sci. 2021, 10, e47. [Google Scholar] [CrossRef]
- Warman, D.J.; Jia, H.; Kato, H. The Potential Roles of Probiotics, Resistant Starch, and Resistant Proteins in Ameliorating Inflammation during Aging (Inflammaging). Nutrients 2022, 14, 747. [Google Scholar] [CrossRef]
- Bigman, G. Age-related Smell and Taste Impairments and Vitamin D Associations in the U.S. Adults National Health and Nutrition Examination Survey. Nutrients 2020, 12, 984. [Google Scholar] [CrossRef]
- Chen, O.; Rogers, G.T.; McKay, D.L.; Maki, K.C.; Blumberg, J.B. The Effect of Multi-Vitamin/Multi-Mineral Supplementation on Nutritional Status in Older Adults Receiving Drug Therapies: A Double-Blind, Placebo-Controlled Trial. J. Diet Suppl. 2022, 19, 20–33. [Google Scholar] [CrossRef] [PubMed]
- Russell, R.M. Factors in Aging that Effect the Bioavailability of Nutrients. J. Nutr. 2001, 131, 1359S–1361S. [Google Scholar] [CrossRef]
- Banic, M.; Plesko, S.; Urek, M.; Babic, Z.; Kardum, D. Immunosenescence, Inflammaging and Resilience: An Evolutionary Perspective of Adaptation in the Light of COVID-19 Pandemic. Psychiatr. Danub. 2021, 33, 427–431. [Google Scholar]
- Santoro, A.; Bientinesi, E.; Monti, D. Immunosenescence and inflammaging in the aging process: Age-related diseases or longevity? Ageing Res. Rev. 2021, 71, 101422. [Google Scholar] [CrossRef]
- Teissier, T.; Boulanger, E.; Cox, L.S. Interconnections between Inflammageing and Immunosenescence during Ageing. Cells 2022, 11, 359. [Google Scholar] [CrossRef]
- Madeira, T.; Severo, M.; Correia, D.; Lopes, C.; Clara, J.G. Nutritional intake and malnutrition in institutionalised and non-institutionalised older adults. Br. J. Nutr. 2021, 128, 921–931. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Song, P.K.; Zhao, L.Y.; Sun, Y.; Yu, K.; Yin, J.; Pang, S.J.; Liu, Z.; Man, Q.Q.; He, L.; et al. Malnutrition in Relation with Dietary, Geographical, and Socioeconomic Factors among Older Chinese. Biomed. Environ. Sci. 2021, 34, 337–347. [Google Scholar] [PubMed]
- Blumberg, J.B.; Frei, B.; Fulgoni, V.L.; Weaver, C.M.; Zeisel, S.H. Contribution of Dietary Supplements to Nutritional Adequacy in Various Adult Age Groups. Nutrients 2017, 9, 1325. [Google Scholar] [CrossRef] [PubMed]
- Biesalski, H.K.; Drewnowski, A.; Dwyer, J.T.; Eggersdorfer, M.; Strain, J.J.; Weber, P. Sustainable Nutrition in a Changing World; Springer International Publishing: Cham, Switzerland, 2017; p. 1. [Google Scholar]
- Park, S.; Johnson, M.A.; Fischer, J.G. Vitamin and Mineral Supplements: Barriers and Challenges for Older Adults. J. Nutr. Elder. 2008, 27, 297–317. [Google Scholar] [CrossRef]
- Seah, Y.-E.C.; Ho, S.F.; Ang, A.S.H.; Bacud, J.P.; Rosario, B.H. Nurse-Initiated Fall and Osteoporosis Screening for Older Adults in the Emergency Department. Cureus 2023, 15, e36001. [Google Scholar] [CrossRef] [PubMed]
- Selhub, J.; Jacques, P.F.; Wilson, P.W.; Rush, D.; Rosenberg, I.H. Vitamin status and intake as primary determinants of homocysteinemia in an elderly population. JAMA 1993, 270, 2693–2698. [Google Scholar] [CrossRef] [PubMed]
- Avenell, A.; Campbell, M.K.; Cook, J.A.; Hannaford, P.C.; Kilonzo, M.M.; McNeill, G.; Milne, A.C.; Ramsay, C.R.; Seymour, D.G.; Stephen, A.I.; et al. Effect of multivitamin and multimineral supplements on morbidity from infections in older people (MAVIS trial): Pragmatic, randomised, double blind, placebo controlled trial. BMJ 2005, 331, 324–329. [Google Scholar] [CrossRef]
- DiNicolantonio, J.J.; Bhutani, J.; O’Keefe, J.H. The health benefits of vitamin K. Open Heart 2015, 2, e000300. [Google Scholar] [CrossRef]
- Fantacone, M.L.; Lowry, M.B.; Uesugi, S.L.; Michels, A.J.; Choi, J.; Leonard, S.W.; Gombart, S.K.; Gombart, J.S.; Bobe, G.; Gombart, A.F. The Effect of a Multivitamin and Mineral Supplement on Immune Function in Healthy Older Adults: A Double-Blind, Randomized, Controlled Trial. Nutrients 2020, 12, 2447. [Google Scholar] [CrossRef]
- Harris, E.; Macpherson, H.; Pipingas, A. Improved Blood Biomarkers but No Cognitive Effects from 16 Weeks of Multivitamin Supplementation in Healthy Older Adults. Nutrients 2015, 7, 3796–3812. [Google Scholar] [CrossRef]
- Myint, P.K.; Smith, R.D.; Luben, R.N.; Surtees, P.G.; Wainwright, N.W.J.; Wareham, N.J.; Khaw, K.-T. Lifestyle behaviours and quality-adjusted life years in middle and older age. Age Ageing 2011, 40, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Kopec, R.E.; Schweiggert, R.M.; Riedl, K.M.; Carle, R.; Schwartz, S.J. Comparison of high-performance liquid chromatography/tandem mass spectrometry and high-performance liquid chromatography/photo-diode array detection for the quantitation of carotenoids, retinyl esters, alpha-tocopherol and phylloquinone in chylomicron-rich fractions of human plasma. Rapid Commun. Mass Spectrom. 2013, 27, 1393–1402. [Google Scholar] [PubMed]
- Li, S.; Tang, X.; Lu, Y.; Xu, J.; Chen, J.; Chen, H. An improved method for the separation of carotenoids and carotenoid isomers by liquid chromatography–mass spectrometry. J. Sep. Sci. 2020, 44, 539–548. [Google Scholar] [CrossRef]
- Usui, Y.; Tanimura, H.; Nishimura, N.; Kobayashi, N.; Okanoue, T.; Ozawa, K. Vitamin K concentrations in the plasma and liver of surgical patients. Am. J. Clin. Nutr. 1990, 51, 846–852. [Google Scholar] [CrossRef] [PubMed]
- Frei, B.; England, L.; Ames, B.N. Ascorbate is an outstanding antioxidant in human blood plasma. Proc. Natl. Acad. Sci. USA 1989, 86, 6377–6381. [Google Scholar] [CrossRef]
- Harrington, J.M.; Young, D.J.; Essader, A.S.; Sumner, S.J.; Levine, K.E. Analysis of Human Serum and Whole Blood for Mineral Content by ICP-MS and ICP-OES: Development of a Mineralomics Method. Biol. Trace Element Res. 2014, 160, 132–142. [Google Scholar] [CrossRef]
- Dougherty, K.A.; Schall, J.I.; Kawchak, D.A.; Green, M.H.; Ohene-Frempong, K.; Zemel, B.S.; Stallings, V.A. No improvement in suboptimal vitamin A status with a randomized, double-blind, placebo-controlled trial of vitamin A supplementation in children with sickle cell disease. Am. J. Clin. Nutr. 2012, 96, 932–940. [Google Scholar] [CrossRef]
- Stach, K.; Stach, W.; Augoff, K. Vitamin B6 in Health and Disease. Nutrients 2021, 13, 3229. [Google Scholar] [CrossRef]
- Chen, M.Y.; Rose, C.E.; Qi, Y.P.; Williams, J.L.; Yeung, L.F.; Berry, R.J.; Hao, L.; Cannon, M.J.; Crider, K.S. Defining the plasma folate concentration associated with the red blood cell folate concentration threshold for optimal neural tube defects prevention: A population-based, randomized trial of folic acid supplementation. Am. J. Clin. Nutr. 2019, 109, 1452–1461. [Google Scholar] [CrossRef]
- Fothergill, A.; Crider, K.S.; Rose, C.E.; Bose, B.; Guetterman, H.M.; Johnson, C.B.; Jabbar, S.; Zhang, M.; Pfeiffer, C.M.; Qi, Y.P.; et al. Estimating the serum folate concentration that corresponds to the red blood cell folate concentration threshold associated with optimal neural tube defects prevention: A population-based biomarker survey in Southern India. Am. J. Clin. Nutr. 2023, 117, 985–997. [Google Scholar] [CrossRef]
- Raghuvanshi, D.S.; Chakole, S.; Kumar, M. Relationship Between Vitamins and Diabetes. Cureus 2023, 15, e36815. [Google Scholar] [CrossRef] [PubMed]
- McCall, S.J.; Clark, A.B.; Luben, R.N.; Wareham, N.J.; Khaw, K.T.; Myint, P.K. Plasma Vitamin C Levels: Risk Factors for Deficiency and Association with Self-Reported Functional Health in the European Prospective Investigation into Cancer-Norfolk. Nutrients 2019, 11, 1552. [Google Scholar] [CrossRef] [PubMed]
- Schmidt-Gayk, H.; Bouillon, R.; Roth, H.J. Measurement of vitamin D and its metabolites (calcidiol and calcitriol) and their clinical significance. Scand. J. Clin. Lab. Investig. 1997, 227, 35–45. [Google Scholar] [CrossRef]
- Cuerq, C.; Restier, L.; Drai, J.; Blond, E.; Roux, A.; Charriere, S.; Michalski, M.-C.; Di Filippo, M.; Levy, E.; Lachaux, A.; et al. Establishment of reference values of α-tocopherol in plasma, red blood cells and adipose tissue in healthy children to improve the management of chylomicron retention disease, a rare genetic hypocholesterolemia. Orphanet J. Rare Dis. 2016, 11, 114. [Google Scholar] [CrossRef]
- Fusaro, M.; Gallieni, M.; Rizzo, M.A.; Stucchi, A.; Delanaye, P.; Cavalier, E.; Moyses, R.M.A.; Jorgetti, V.; Iervasi, G.; Giannini, S.; et al. Vitamin K plasma levels determination in human health. Clin. Chem. Lab. Med. 2016, 55, 789–799. [Google Scholar] [CrossRef]
- Vega-Cabello, V.; Struijk, E.A.; Caballero, F.F.; Lana, A.; Arias-Fernández, L.; Banegas, J.R.; Artalejo, F.R.; Lopez-Garcia, E. Dietary Micronutrient Adequacy and Risk of Multimorbidity in Community-dwelling Older Adults. Am. J. Clin. Nutr. 2023; in press. [Google Scholar]
- Jang, D.H.; Shofer, F.S.; Weiss, S.L.; Becker, L.B. Impairment of mitochondrial respiration following ex vivo cyanide exposure in peripheral blood mononuclear cells. Clin. Toxicol. 2016, 54, 303–307. [Google Scholar] [CrossRef]
- Divakaruni, A.S.; Jastroch, M. A practical guide for the analysis, standardization and interpretation of oxygen consumption measurements. Nat. Metab. 2022, 4, 978–994. [Google Scholar] [CrossRef]
- Schmidt, C.A.; Fisher-Wellman, K.H.; Neufer, P.D. From OCR and ECAR to energy: Perspectives on the design and interpretation of bioenergetics studies. J. Biol. Chem. 2021, 297, 101140. [Google Scholar] [CrossRef]
- Whitton, C.; Ramos-García, C.; Kirkpatrick, S.I.; Healy, J.D.; Dhaliwal, S.S.; Boushey, C.J.; Collins, C.E.; Rollo, M.E.; Kerr, D.A. A Systematic Review Examining Contributors to Misestimation of Food and Beverage Intake Based on Short-Term Self-Report Dietary Assessment Instruments Administered to Adults. Adv. Nutr. 2022, 13, 2620–2665. [Google Scholar] [CrossRef]
- Lyon, P.; Strippoli, V.; Fang, B.; Cimmino, L. B Vitamins and One-Carbon Metabolism: Implications in Human Health and Disease. Nutrients 2020, 12, 2867. [Google Scholar] [CrossRef]
- Mason, J.B.; Miller, J.W. The Effects of Vitamins B12, B6, and Folate on Blood Homocysteine Levels. Ann. N. Y. Acad. Sci. 1992, 669, 197–203; discussion 203–204. [Google Scholar] [CrossRef] [PubMed]
- Baker, L.D.; Manson, J.E.; Rapp, S.R.; Sesso, H.D.; Gaussoin, S.A.; Shumaker, S.A.; Espeland, M.A. Effects of cocoa extract and a multivitamin on cognitive function: A randomized clinical trial. Alzheimer’s Dement. 2022, 19, 1308–1319. [Google Scholar] [CrossRef] [PubMed]
- Gerrior, S.; Juan, W.; Basiotis, P. An Easy Approach to Calculating Estimated Energy Requirements. In Prev. Chronic Dis.; 2006. Available online: http://www.cdc.gov/pcd/issues/2006/oct/06_0034.htm (accessed on 19 May 2023).




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Placebo (n = 18) 1 | MV/MM (n = 17) 1 | p-Value 2 |
|---|---|---|---|
| Age, years | 73 (5) | 71 (3) | 0.08 |
| BMI, kg/m2 | 28.3 (3.6) | 26.3 (3.6) | 0.13 |
| Systolic Blood Pressure, mm Hg | 132 (14) | 122 (10) | 0.03 |
| Diastolic Blood Pressure, mm Hg | 77 (7) | 75 (6) | 0.32 |
| Prior MV/MM use, n | 8 | 5 | 0.49 |
| Triglycerides, mg/dL 3 | 113 (52) | 76 (30) | 0.02 |
| Total Cholesterol, mg/dL 3 | 179 (28) | 178 (31) | 0.93 |
| HDL Cholesterol, mg/dL 3 | 53 (8) | 66 (10) | 0.0002 |
| LDL Cholesterol, mg/dL 3 | 103 (26) | 96 (25) | 0.44 |
| Glucose, mg/dL | 105 (8) | 100 (8) | 0.10 |
| Hb A1c, % | 5.6 (0.3) | 5.5 (0.3) | 0.29 |
| Ferritin, ng/mL | 95 (73) | 68 (31) | 0.17 |
| Biomarker | Status Category 1 | Participants 2 |
|---|---|---|
| Retinol (Vitamin A) | Deficiency, <0.7 μM Suboptimal, <1.05 μM | 0 (0%) 0 (0%) |
| Pyridoxal Phosphate (Vitamin B6) | Deficiency, <4.9 ng/mL Suboptimal, <8.9 ng/mL | 0 (0%) 8 (24%) |
| Folate, RBC (Vitamin B9) | Deficiency, <150 ng/mL Suboptimal, <400 ng/mL | 0 (0%) 7 (21%) |
| Cobalamin (Vitamin B12) | Deficiency, < 200 pg/mL Suboptimal, <500 pg/mL | 0 (0%) 24 (69%) |
| Ascorbic Acid (Vitamin C) | Deficiency, <11.4 μM Suboptimal, <50 μM | 0 (0%) 20 (57%) |
| Calicidiol (Vitamin D3) | Deficiency, <12 ng/mL Insufficiency, <20 ng/mL Suboptimal, <30 ng/mL | 1 (3%) 3 (9%) 14 (40%) |
| α-tocopherol (Vitamin E) | Deficiency, <12 μM Suboptimal, <30 μM | 0 (0%) 14 (43%) |
| Phylloquinone (Vitamin K) | Deficiency, <0.5 μM Suboptimal, <1.0 μM | 4 (11%) 4 (11%) |
| Biomarker | Placebo Group (n = 18) 1 | MV/MM Group (n = 17) 1 | |||
|---|---|---|---|---|---|
| Baseline | Final | Baseline | Final | p-Value 2 | |
| Water-soluble Vitamins | |||||
| Pyridoxal Phosphate, ng/mL | 14.6 (10.6) | 15.2 (12.9) | 11.9 (3.4) | 28.7 (9.2) | <0.0001 |
| Ascorbic Acid, μM | 42 (14) | 42 (19) | 54 (18) | 58 (14) | 0.52 |
| Cobalamin, pg/mL | 485 (134) | 501 (314) | 428 (129) | 480 (150) | 0.39 |
| Folate, RBC, ng/mL | 537 (155) | 504 (127) | 640 (209) | 695 (169) | 0.16 |
| Lipid-soluble Vitamins | |||||
| α-Tocopherol, μM | 35 (9) | 31 (6) | 30 (9) | 35 (9) | 0.01 |
| Calcidiol, ng/mL | 28 (11) | 27 (11) | 32 (11) | 38 (13) | 0.0005 |
| Phylloquinone, nM | 2.0 (1.5) | 1.9 (1.6) | 1.5 (1.1) | 2.0 (1.5) | 0.80 |
| Retinol, μM | 6.2 (1.7) | 5.8 (1.3) | 6.3 (2.3) | 6.7 (1.9) | 0.06 |
| Carotenoids | |||||
| β-Carotene, μM | 0.41 (0.17) | 0.36 (0.19) | 0.39 (0.17) | 0.45 (0.23) | 0.01 |
| Lutein, μM | 1.8 (0.7) | 1.7 (0.6) | 1.9 (1.2) | 2.0 (0.8) | 0.18 |
| Lycopene, μM | 0.31 (0.23) | 0.24 (0.14) | 0.31 (0.29) | 0.36 (0.29) | 0.26 |
| Minerals | |||||
| Calcium, μg/mL | 55 (2) | 55 (2) | 55 (2) | 56 (3) | 0.13 |
| Copper, μg/mL | 0.62 (0.09) | 0.62 (0.08) | 0.66 (0.15) | 0.61 (0.06) | 0.41 |
| Magnesium, μg/mL | 11.5 (0.9) | 11.4 (0.7) | 11.6 (0.9) | 11.7 (0.9) | 0.47 |
| Zinc, μg/mL | 0.50 (0.12) | 0.53 (0.13) | 0.56 (0.13) | 0.53 (0.16) | 0.33 |
| Biomarker | Status Category | Placebo (n = 18) 2 | MV/MM (n = 17) | ||
|---|---|---|---|---|---|
| Initial | Final | Initial | Final | ||
| Retinol | Deficiency 3, <0.7 μM Suboptimal 3, <1.05 μM | 0 (0%) 0 (0%) | 0 (0%) 0 (0%) | 0 (0%) 0 (0%) | 0 (0%) 0 (0%) |
| Pyridoxal Phosphate | Deficiency, <4.9 ng/mL Suboptimal, <8.9 ng/mL | 0 (0%) 5 (29%) | 1 (6%) 6 (35%) | 0 (0%) 3 (18%) | 0 (0%) 0 (0%) |
| Folate, RBC | Deficiency, <150 ng/mL Suboptimal, <400 ng/mL | 0 (0%) 5 (29%) | 0 (0%) 5 (29%) | 0 (0%) 2 (12%) | 0 (0%) 0 (0%) |
| Cobalamin | Deficiency, <200 pg/mL Suboptimal, <500 pg/mL | 0 (0%) 10 (56%) | 0 (0%) 13 (73%) | 0 (0%) 14 (82%) | 0 (0%) 12 (71%) |
| Ascorbic Acid | Deficiency, <11.4 μM Suboptimal, <50 μM | 0 (0%) 13 (73%) | 1 (6%) 11 (61%) | 0 (0%) 7 (41%) | 0 (0%) 3 (18%) |
| Calcidiol | Deficiency, <12 ng/mL Insufficiency, <20 ng/mL Suboptimal, <30 ng/mL | 1 (6%) 1 (6%) 9 (50%) | 0 (0%) 6 (34%) 6 (34%) | 0 (0%) 2 (12%) 5 (29%) | 0 (0%) 0 (0%) 5 (29%) |
| α-tocopherol | Deficiency, <12 μM Suboptimal, <30 μM | 0 (0%) 5 (28%) | 0 (0%) 8 (44%) | 0 (0%) 9 (53%) | 0 (0%) 6 (35%) |
| Phylloquinone | Deficiency, <0.5 μM Suboptimal, <1.0 μM | 1 (6%) 2 (11%) | 0 (0%) 7 (39%) | 3 (18%) 2 (12%) | 0 (0%) 4 (24%) |
| Total (at least one) | |||||
| Deficiency | 1 (6%) | 2 (11%) | 3 (18%) | 0 (0%) | |
| Insufficiency | 1 (6%) | 3 (17%) | 2 (12%) | 0 (0%) | |
| Suboptimal | 17 (94%) | 13 (72%) | 11 (65%) | 15 (88%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Michels, A.J.; Butler, J.A.; Uesugi, S.L.; Lee, K.; Frei, B.B.; Bobe, G.; Magnusson, K.R.; Hagen, T.M. Multivitamin/Multimineral Supplementation Prevents or Reverses Decline in Vitamin Biomarkers and Cellular Energy Metabolism in Healthy Older Men: A Randomized, Double-Blind, Placebo-Controlled Study. Nutrients 2023, 15, 2691. https://doi.org/10.3390/nu15122691
Michels AJ, Butler JA, Uesugi SL, Lee K, Frei BB, Bobe G, Magnusson KR, Hagen TM. Multivitamin/Multimineral Supplementation Prevents or Reverses Decline in Vitamin Biomarkers and Cellular Energy Metabolism in Healthy Older Men: A Randomized, Double-Blind, Placebo-Controlled Study. Nutrients. 2023; 15(12):2691. https://doi.org/10.3390/nu15122691
Chicago/Turabian StyleMichels, Alexander J., Judy A. Butler, Sandra L. Uesugi, Ken Lee, Balz B. Frei, Gerd Bobe, Kathy R. Magnusson, and Tory M. Hagen. 2023. "Multivitamin/Multimineral Supplementation Prevents or Reverses Decline in Vitamin Biomarkers and Cellular Energy Metabolism in Healthy Older Men: A Randomized, Double-Blind, Placebo-Controlled Study" Nutrients 15, no. 12: 2691. https://doi.org/10.3390/nu15122691
APA StyleMichels, A. J., Butler, J. A., Uesugi, S. L., Lee, K., Frei, B. B., Bobe, G., Magnusson, K. R., & Hagen, T. M. (2023). Multivitamin/Multimineral Supplementation Prevents or Reverses Decline in Vitamin Biomarkers and Cellular Energy Metabolism in Healthy Older Men: A Randomized, Double-Blind, Placebo-Controlled Study. Nutrients, 15(12), 2691. https://doi.org/10.3390/nu15122691