
The Effect of Fermentable, Oligosaccharides, Disaccharides, Monosaccharides, and Polyols (FODMAP) Meals on Transient Lower Esophageal Relaxations (TLESR) in Gastroesophageal Reflux Disease (GERD) Patients with Overlapping Irritable Bowel Syndrome (IBS)

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Study Design
2.3. Interventional Meals
2.4. Breath Tests
2.5. Evaluation of TLESRs
2.6. Statistical Analysis
3. Results
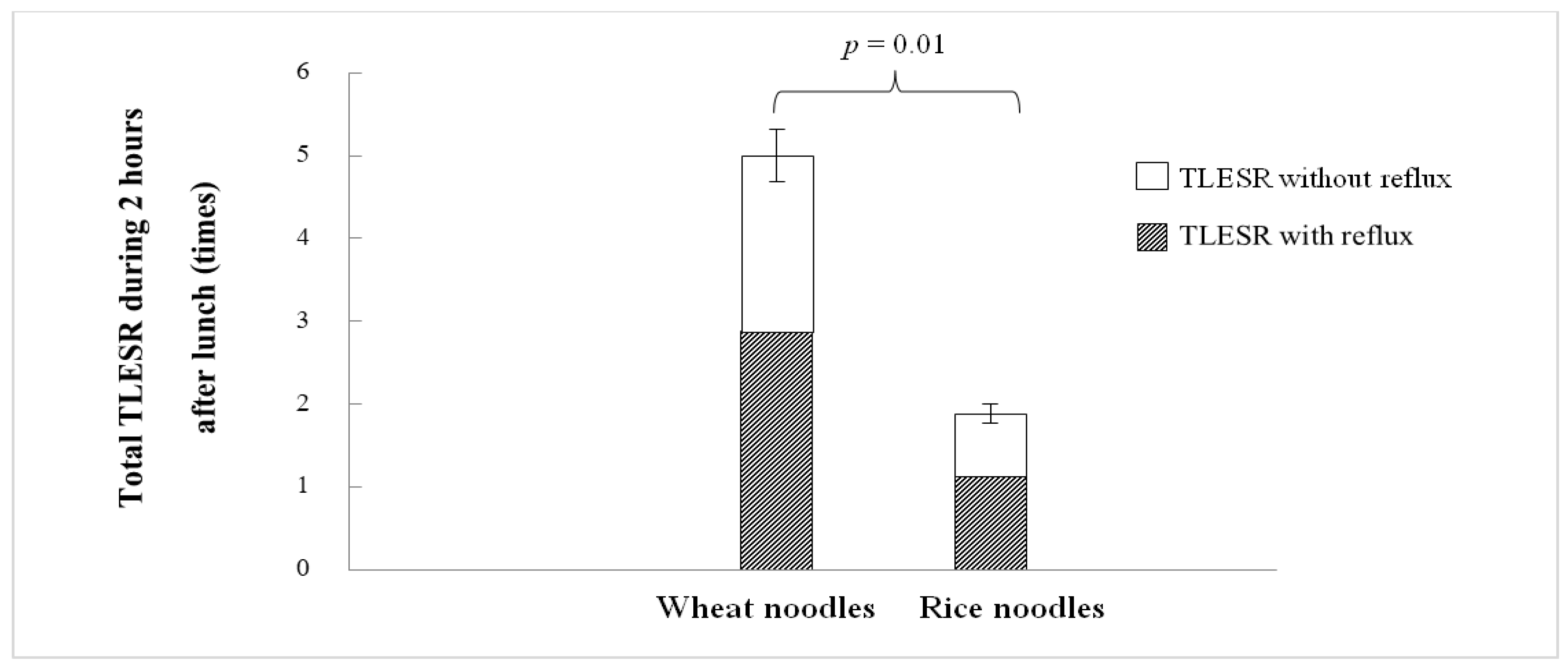
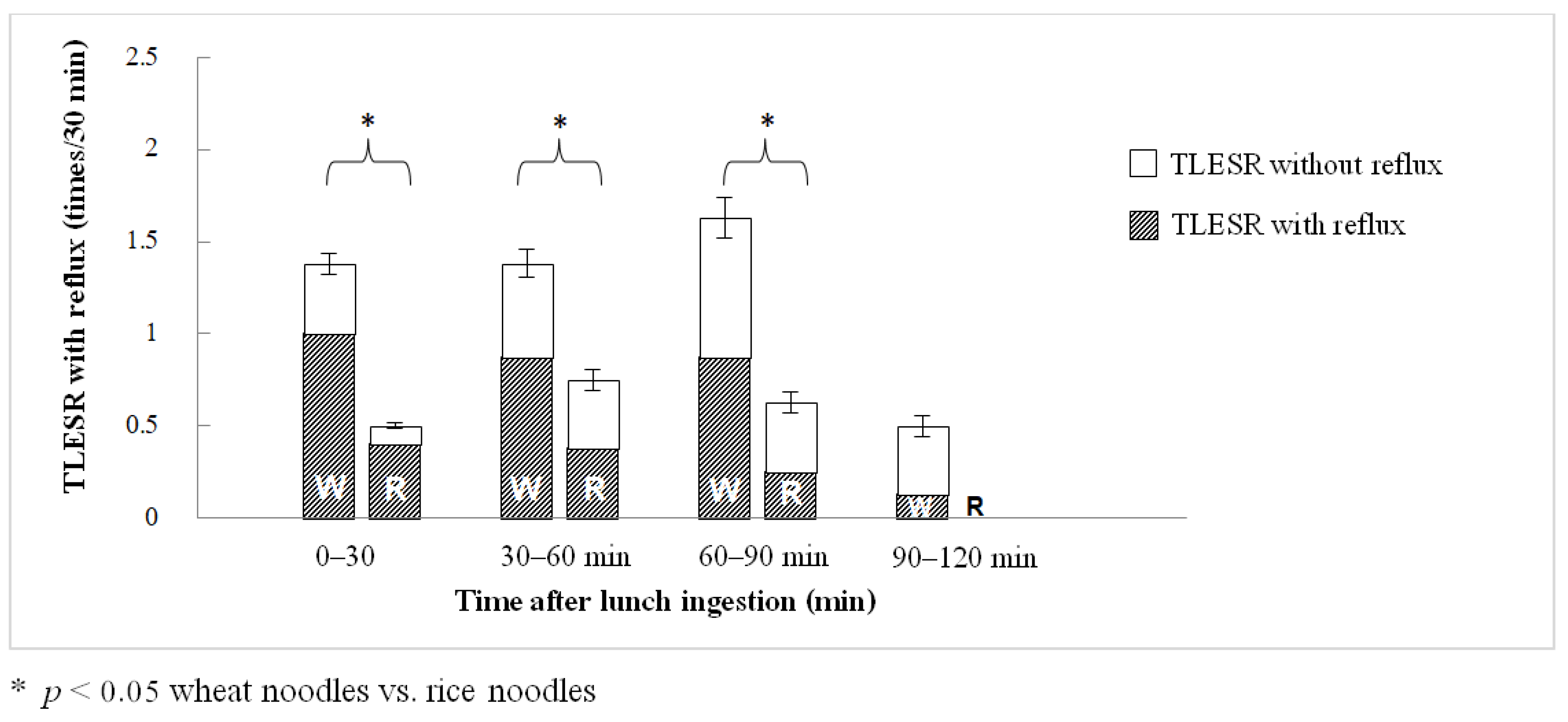
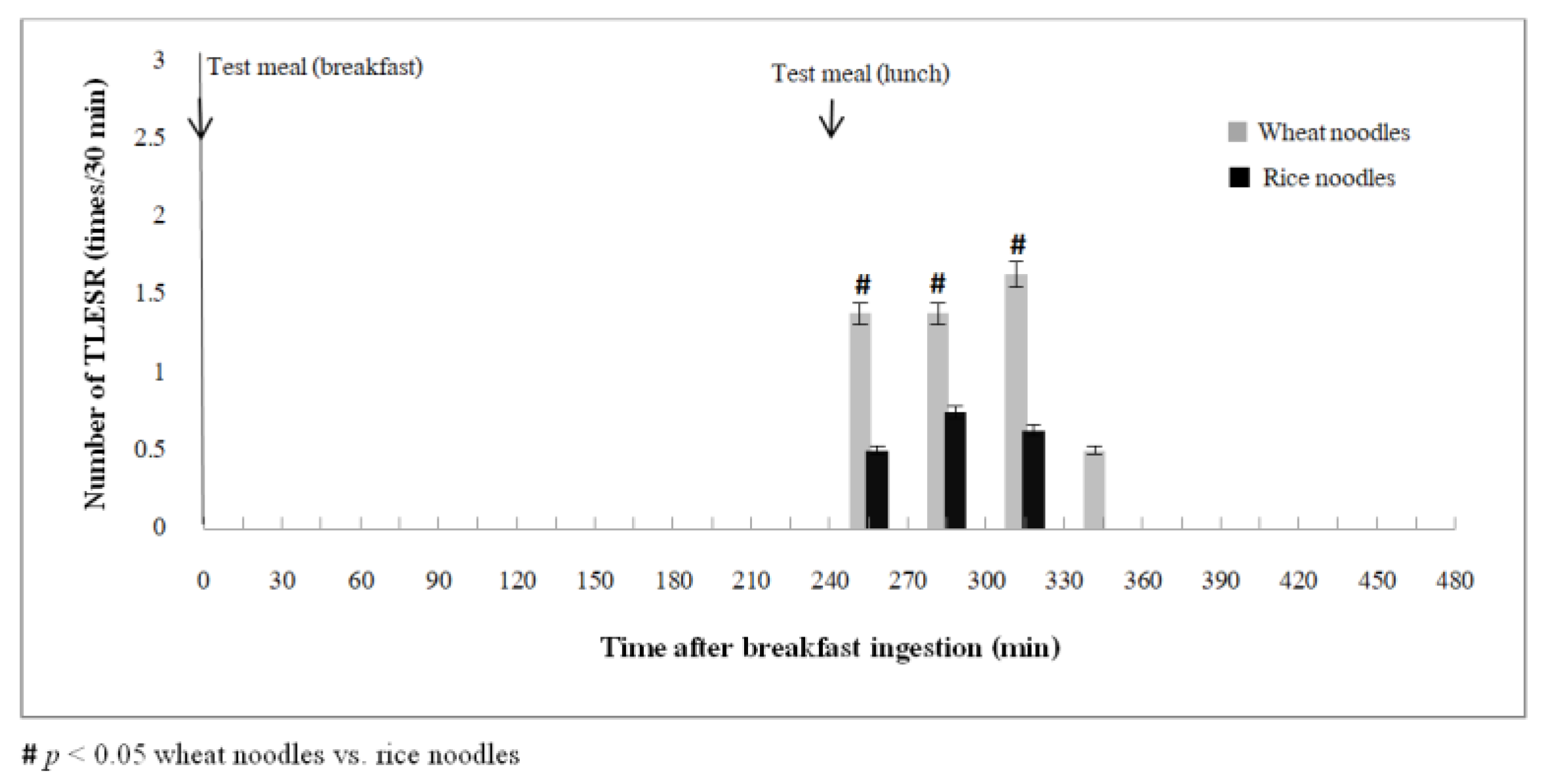
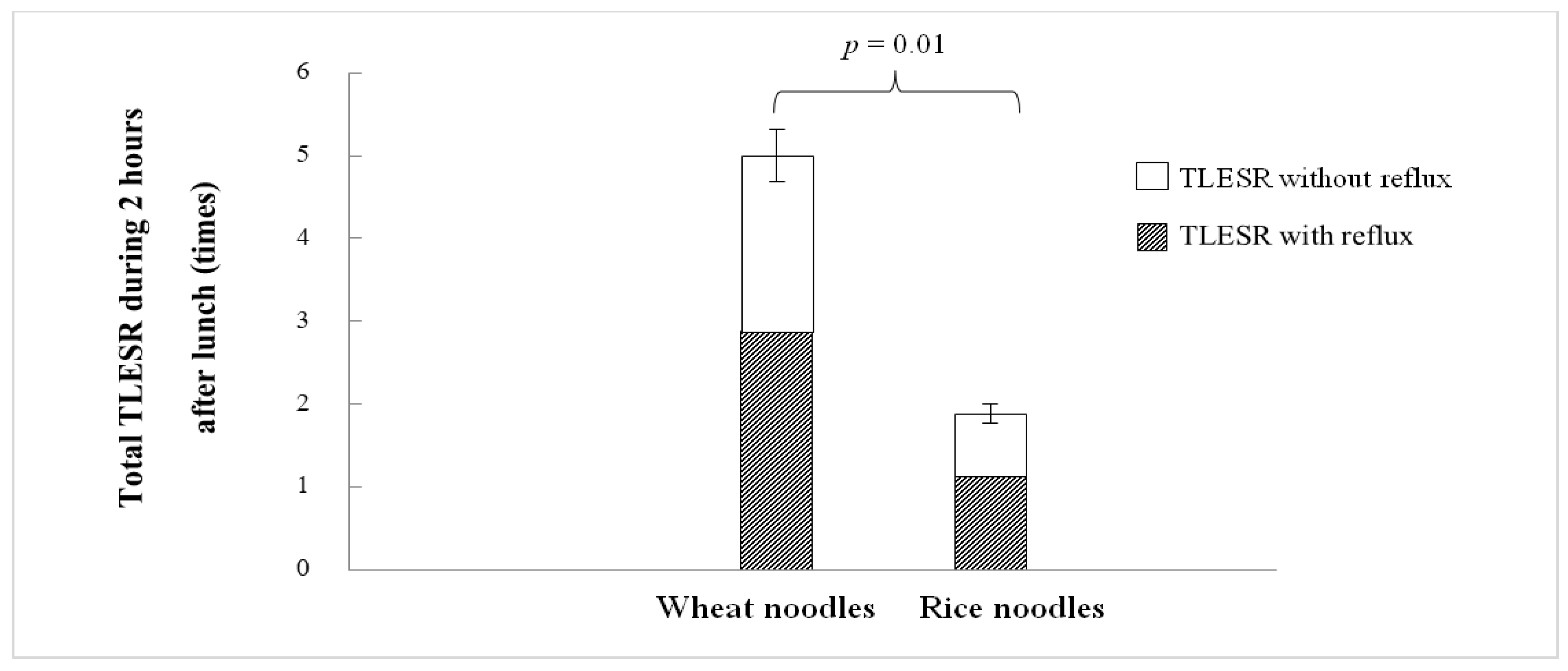
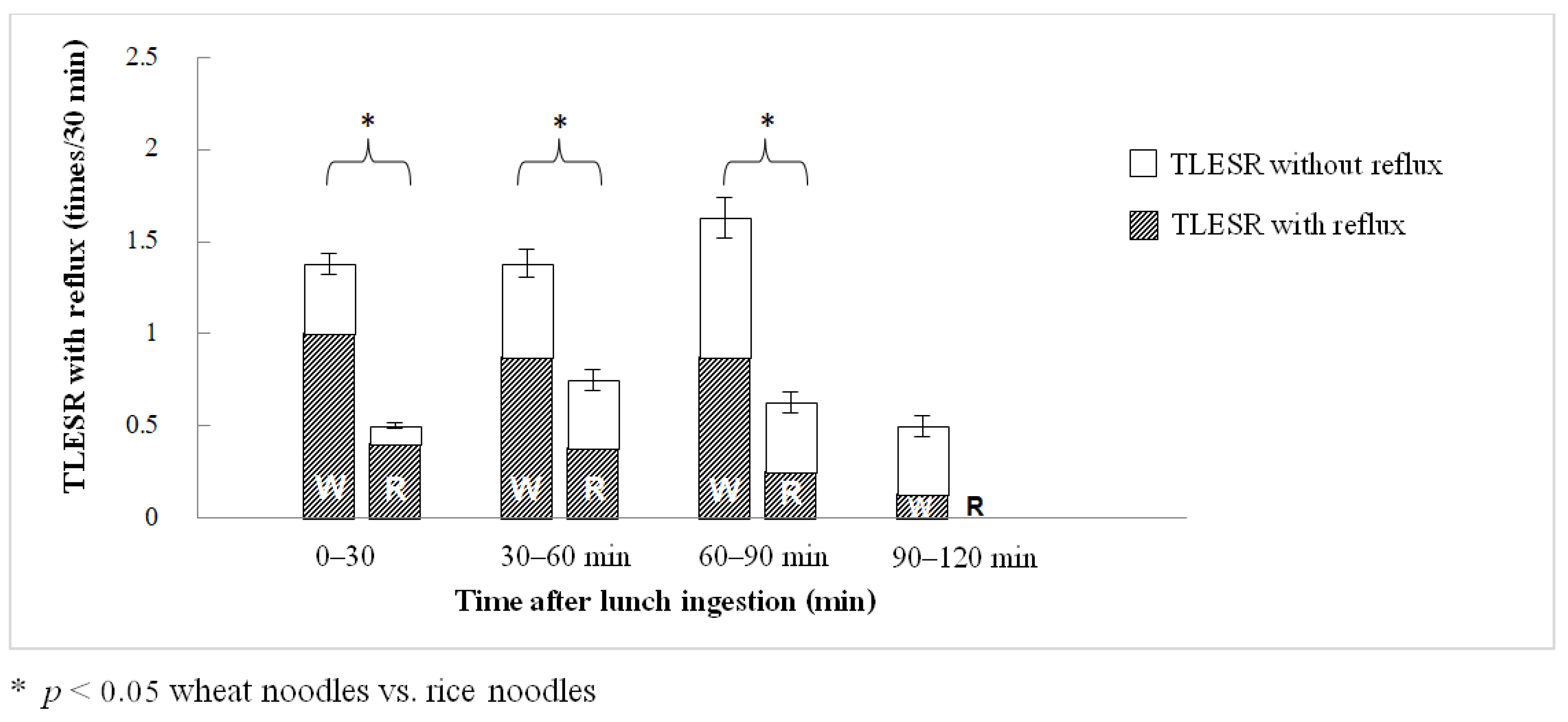
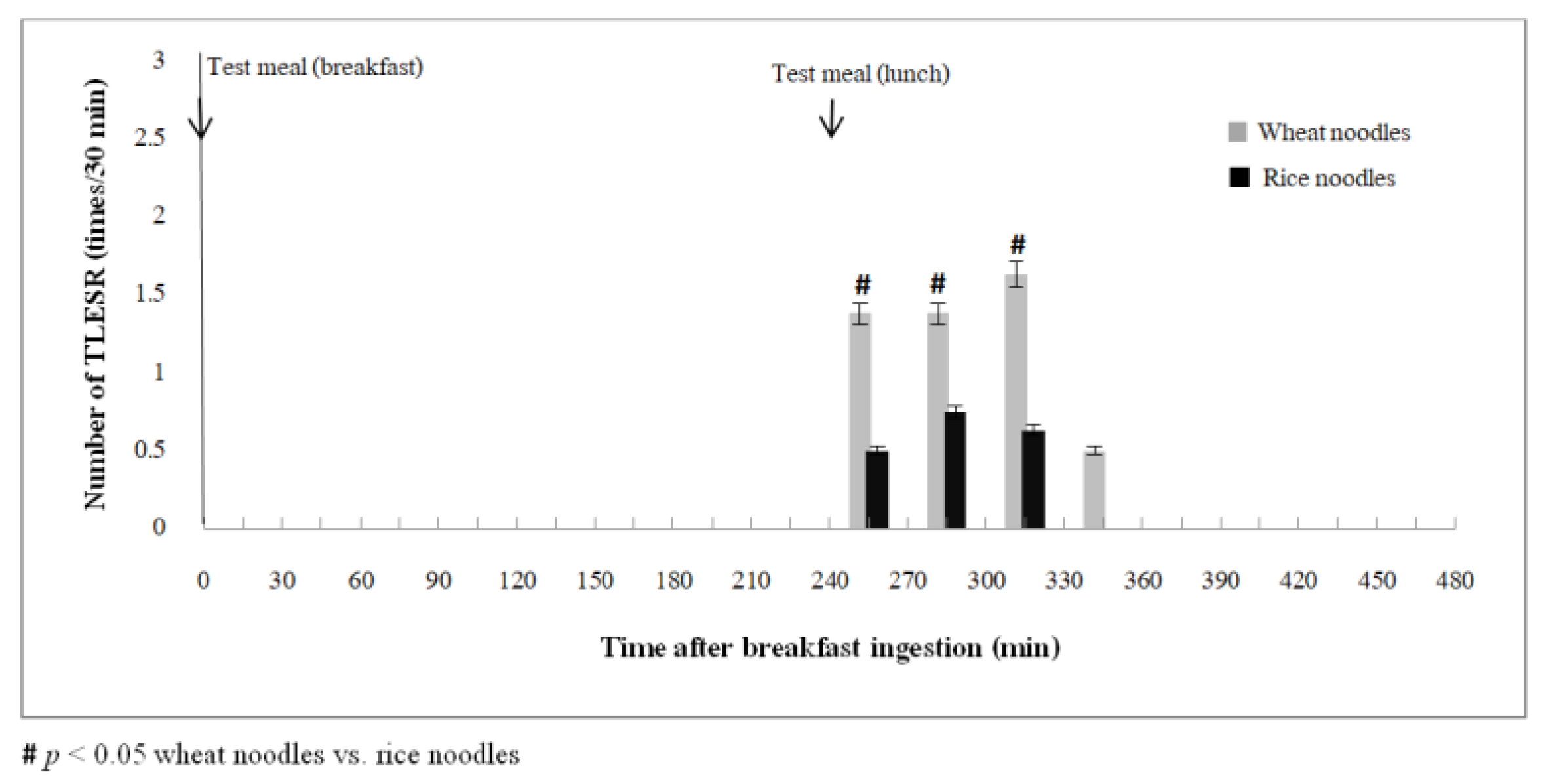
3.1. Effects of Wheat vs. Rice Ingestion on TLESR
3.2. Effects of Wheat vs. Rice Ingestion on GER and Other GI Symptoms
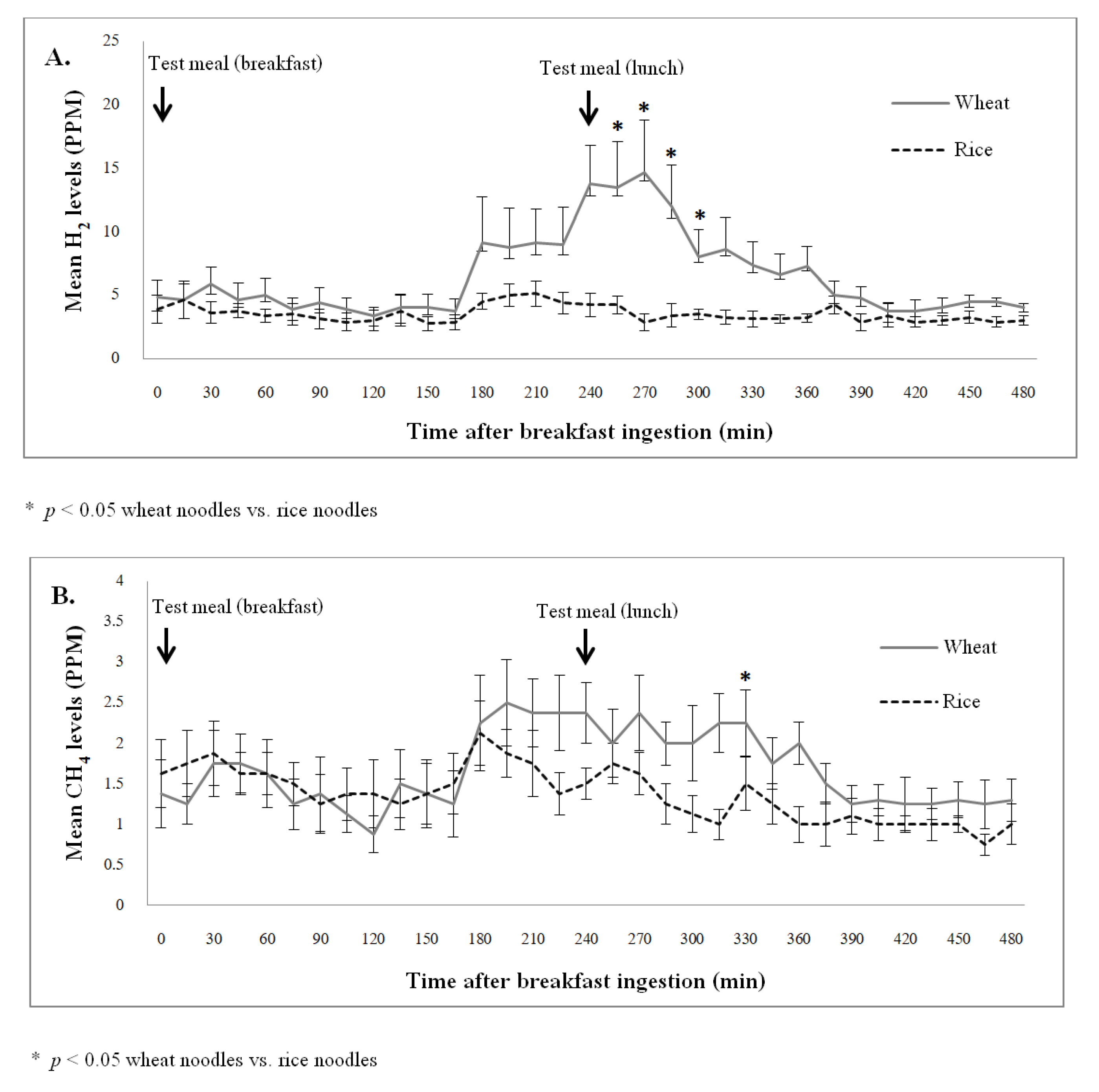
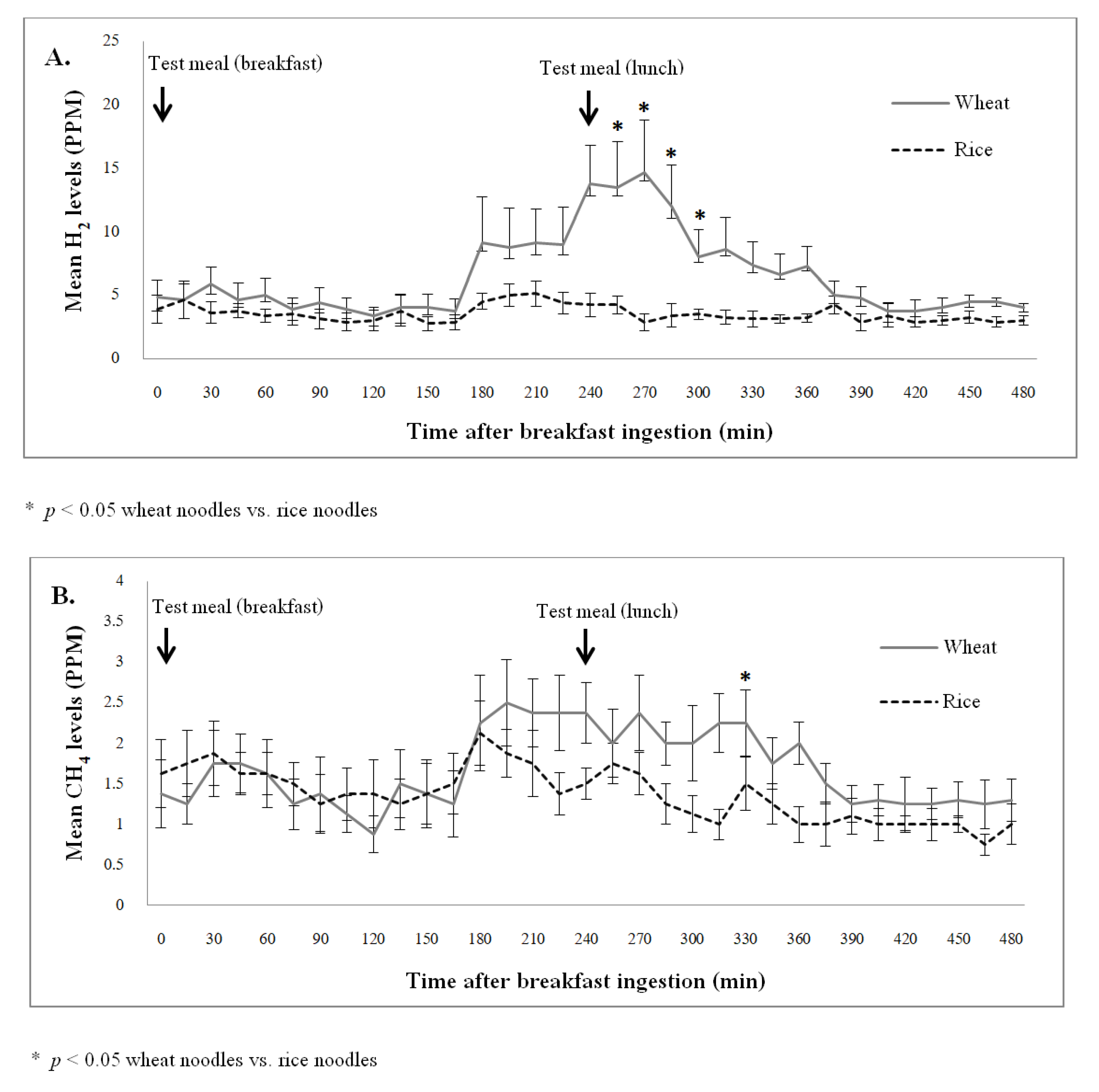
3.3. Effects of Wheat vs. Rice Ingestion on Intestinal Gas Production
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Lovell, R.M.; Ford, A. Prevalence of gastro-esophageal reflux-type symptoms in individuals with irritable bowel syndrome in the community: A meta-analysis. Am. J. Gastroenterol. 2012, 107, 1793–1801. [Google Scholar] [CrossRef] [PubMed]
- Nastaskin, I.; Mehdikhani, E.; Conklin, J.; Park, S.; Pimentel, M. Studying the overlap between IBS and GERD: A systematic review of the literature. Dig. Dis. Sci. 2006, 51, 2113–2120. [Google Scholar] [CrossRef] [PubMed]
- Mönnikes, H.; Heading, R.C.; Schmitt, H.; Doerfler, H. Influence of irritable bowel syndrome on treatment outcome in gastroesophageal reflux disease. World J. Gastroenterol. 2011, 17, 3235–3241. [Google Scholar] [CrossRef] [PubMed]
- McIntosh, K.; Reed, D.E.; Schneider, T.; Dang, F.; Keshteli, A.H.; De Palma, G.; Madsen, K.; Bercik, P.; Vanner, S. FODMAPs alter symptoms and the metabolome of patients with IBS: A randomised controlled trial. Gut 2017, 66, 1241–1251. [Google Scholar] [CrossRef] [PubMed]
- Patcharatrakul, T.; Juntrapirat, A.; Lakananurak, N.; Gonlachanvit, S. Effect of Structural Individual Low-FODMAP Dietary Advice vs. Brief Advice on a Commonly Recommended Diet on IBS Symptoms and Intestinal Gas Production. Nutrients 2019, 11, 2856. [Google Scholar] [CrossRef] [Green Version]
- Wilson, B.; Rossi, M.; Kanno, T.; Parkes, G.C.; Anderson, S.; Mason, A.J.; Irving, P.M.; Lomer, M.C.; Whelan, K. β-Galactooligosaccharide in Conjunction with Low FODMAP Diet Improves Irritable Bowel Syndrome Symptoms but Reduces Fecal Bifidobacteria. Am. J. Gastroenterol. 2020, 115, 906–915. [Google Scholar] [CrossRef] [PubMed]
- Böhn, L.; Störsrud, S.; Liljebo, T.; Collin, L.; Lindfors, P.; Törnblom, H.; Simrén, M. Diet low in FODMAPs reduces symptoms of irritable bowel syndrome as well as traditional dietary advice: A randomized controlled trial. Gastroenterology 2015, 149, 1399–1407.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eswaran, S.L.; Chey, W.D.; Han-Markey, T.; Ball, S.; Jackson, K. A Randomized Controlled Trial Comparing the Low FODMAP Diet vs. Modified NICE Guidelines in US Adults with IBS-D. Am. J. Gastroenterol. 2016, 111, 1824–1832. [Google Scholar] [CrossRef] [PubMed]
- Goyal, O.; Batta, S.; Nohria, S.; Kishore, H.; Goyal, P.; Sehgal, R.; Sood, A. Low fermentable oligosaccharide, disaccharide, monosaccharide, and polyol diet in patients with diarrhea-predominant irritable bowel syndrome: A prospective, randomized trial. J. Gastroenterol. Hepatol. 2021, 36, 2107–2115. [Google Scholar] [CrossRef]
- Halmos, E.P.; Power, V.A.; Shepherd, S.J.; Gibson, P.R.; Muir, J.G. A diet low in fodmaps reduces symptoms of irritable bowel syndrome. Gastroenterology 2014, 146, 67–75.e5. [Google Scholar] [CrossRef]
- Harvie, R.M.; Chisholm, A.W.; Bisanz, J.E.; Burton, J.P.; Herbison, P.; Schultz, K.; Schultz, M. Long-term irritable bowel syndrome symptom control with reintroduction of selected FODMAPs. World J. Gastroenterol. 2017, 23, 4632–4643. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, N.; Ankersen, D.V.; Felding, M.; Wachmann, H.; Végh, Z.; Molzen, L.; Burisch, J.; Andersen, J.R.; Munkholm, P. Low-FODMAP diet reduces irritable bowel symptoms in patients with inflammatory bowel disease. World J. Gastroenterol. 2017, 23, 3356–3366. [Google Scholar] [CrossRef] [PubMed]
- Staudacher, H.M.; Lomer, M.C.; Anderson, J.L.; Barrett, J.S.; Muir, J.G.; Irving, P.M.; Whelan, K. Fermentable carbohydrate restriction reduces luminal bifidobacteria and gastrointestinal symptoms in patients with irritable bowel syndrome. J. Nutr. 2012, 142, 1510–1518. [Google Scholar] [CrossRef]
- Staudacher, H.M.; Lomer, M.C.E.; Farquharson, F.M.; Louis, P.; Fava, F.; Franciosi, E.; Scholz, M.; Tuohy, K.M.; Lindsay, J.O.; Irving, P.M.; et al. A Diet Low in FODMAPs Reduces Symptoms in Patients with Irritable Bowel Syndrome and A Probiotic Restores Bifidobacterium Species: A Randomized Controlled Trial. Gastroenterology 2017, 153, 936–947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zahedi, M.J.; Behrouz, V.; Azimi, M. Low fermentable oligo-di-mono-saccharides and polyols diet versus general dietary advice in patients with diarrhea-predominant irritable bowel syndrome: A randomized controlled trial. J. Gastroenterol. Hepatol. 2018, 33, 1192–1199. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Feng, L.; Wang, X.; Fox, M.; Luo, L.; Du, L.; Chen, B.; Chen, X.; He, H.; Zhu, S.; et al. Low fermentable oligosaccharides, disaccharides, monosaccharides, and polyols diet compared with traditional dietary advice for diarrhea-predominant irritable bowel syndrome: A parallel-group, randomized controlled trial with analysis of clinical and microbiological factors associated with patient outcomes. Am. J. Clin. Nutr. 2021, 113, 1531–1545. [Google Scholar] [CrossRef] [PubMed]
- Katz, P.O.; Gerson, L.B.; Vela, M.F. Guidelines for the diagnosis and management of gastroesophageal reflux disease. Am. J. Gastroenterol. 2013, 108, 308–328. [Google Scholar] [CrossRef]
- Ness-Jensen, E.; Hveem, K.; El-Serag, H.; Lagergren, J. Lifestyle Intervention in Gastroesophageal Reflux Disease. Clin. Gastroenterol. Hepatol. 2015, 14, 175–182.e3. [Google Scholar] [CrossRef] [Green Version]
- Fox, M.; Barr, C.; Nolan, S.; Lomer, M.; Anggiansah, A.; Wong, T. The effects of dietary fat and calorie density on esophageal acid exposure and reflux symptoms. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2007, 5, 439–444.e1. [Google Scholar] [CrossRef]
- Sethi, S.; Richter, J.E. Diet and gastroesophageal reflux disease: Role in pathogenesis and management. Curr. Opin. Gastroenterol. 2017, 33, 107–111. [Google Scholar] [CrossRef]
- Ropert, A.; Cherbut, C.; Roze, C.; Le Quellec, A.; Holst, J.J.; Fu-Cheng, X.; Varannes, S.B.D.; Galmiche, J.P. Colonic fermentation and proximal gastric tone in humans. Gastroenterology 1996, 111, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Zerbib, F.; Varannes, S.B.D.; Rozé, D.C.; Galmiche, J.P. Simultaneous study of tones of the lower esophageal sphincter and proximal stomach in healthy humans. Gastroentérologie Clin. Biol. 1996, 20, 1078–1083. [Google Scholar]
- Piche, T.; Zerbib, F.; Varannes, S.B.D.; Cherbut, C.; Anini, Y.; Roze, C.; Le Quellec, A.; Galmiche, J.-P. Modulation by colonic fermentation of LES function in humans. Am. J. Physiol. Liver Physiol. 2000, 278, G578–G584. [Google Scholar] [CrossRef] [PubMed]
- Zerbib, F.; Varannes, S.B.D.; Scarpignato, C.; Leray, V.; D’Amato, M.; Rozé, C.; Galmiche, J.-P. Endogenous cholecystokinin in postprandial lower esophageal sphincter function and fundic tone in humans. Am. J. Physiol. Content 1998, 275, G1266–G1273. [Google Scholar] [CrossRef]
- Linlawan, S.; Patcharatrakul, T.; Gonlachanvit, S. Effect of Rice, Wheat and Mung Bean Ingestion on Intestinal Gas Production and Postprandial Gastrointestinal Symptoms in Non-constipation Irritable Bowel Syndrome Patients. Nutrients 2019, 11, 2061. [Google Scholar] [CrossRef] [Green Version]
- USDA. Food Data Central. Available online: https://ndb.nal.usda.gov/ndb/search/list (accessed on 10 March 2020).
- Simren, M.; Stotzer, P.O. Use and abuse of hydrogen breath tests. Gut 2006, 55, 297–303. [Google Scholar] [CrossRef]
- Roman, S.; Zerbib, F.; Belhocine, K.; Varannes, S.B.D.; Mion, F. High resolution manometry to detect transient lower oesophageal sphincter relaxations: Diagnostic accuracy compared with perfused-sleeve manometry, and the definition of new detection criteria. Aliment. Pharmacol. Ther. 2011, 34, 384–393. [Google Scholar] [CrossRef]
- Piche, T.; Varannes, S.B.D.; Sacher-Huvelin, S.; Holst, J.J.; Cuber, J.C.; Galmiche, J.P. Colonic fermentation influences lower esophageal sphincter function in gastroesophageal reflux disease. Gastroenterology 2003, 124, 894–902. [Google Scholar] [CrossRef]
- Shepherd, S.J.; Gibson, P.R. Fructose malabsorption and symptoms of irritable bowelsyndrome: Guidelines for effective dietary management. Am. Diet. Assoc. 2006, 106, 1631–1639. [Google Scholar] [CrossRef]
- Patcharatrakul, T.; Linlawan, S.; Plaidum, S.; Gonlachanvit, S. The Effect of Rice vs. Wheat Ingestion on Postprandial Gastroesophageal Reflux (GER) Symptoms in Patients with Overlapping GERD-Irritable Bowel Syndrome (IBS). Foods 2021, 11, 26. [Google Scholar] [CrossRef]
- Gonlachanvit, S. Are rice and spicy diet good for functional gastrointestinal disorders? J. Neurogastroenterol. Motil. 2010, 16, 131–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houghton, L.A.; Lea, R.; Agrawal, A.; Reilly, B.; Whorwell, P. Relationship of abdominal bloating to distention in irritable bowel syndrome and effect of bowel habit. Gastroenterology 2006, 131, 1003–1010. [Google Scholar] [CrossRef] [PubMed]
- Rivière, P.; Vauquelin, B.; Rolland, E.; Melchior, C.; Roman, S.; Varannes, S.B.D.; Mion, F.; Gourcerol, G.; Sacher-Huvelin, S.; Zerbib, F. Low FODMAPs diet or usual dietary advice for the treatment of refractory gastroesophageal reflux disease: An open-labeled randomized trial. Neurogastroenterol. Motil. 2021, 33, e14181. [Google Scholar] [CrossRef] [PubMed]
- Geysen, H.; Gielis, E.; Deloose, E.; Vanuytsel, T.; Tack, J.; Biesiekierski, J.R.; Pauwels, A. Acute administration of fructans increases the number of transient lower esophageal sphincter relaxations in healthy volunteers. Neurogastroenterol. Motil. 2019, 32, e13727. [Google Scholar] [CrossRef] [PubMed]
- Marciani, L.; Pritchard, S.E.; Hellier-Woods, C.; Costigan, C.; Hoad, C.; Gowland, P.; Spiller, R.C. Delayed gastric emptying and reduced postprandial small bowel water content of equicaloric whole meal bread versus rice meals in healthy subjects: Novel MRI insights. Eur. J. Clin. Nutr. 2013, 67, 754–758. [Google Scholar] [CrossRef]
- Patcharatrakul, T.; Kriengkirakul, C.; Chaiwattanarat, T.; Gonlachanvit, S. Acute Effects of Red Chili, a Natural Capsaicin Receptor Agonist, on Gastric Accommodation and Upper Gastrointestinal Symptoms in Healthy Volunteers and Gastroesophageal Reflux Disease Patients. Nutrients 2020, 12, 3740. [Google Scholar] [CrossRef]
- Di Stefano, M.; Maffè, G.C.; Bergonzi, M.; Mengoli, C.; Formagnana, P.; Di Sabatino, A.; Corazza, G.R. The effect of gluten on intestinal fermentation, gastric and gallbladder emptying in healthy volunteers. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2015, 47, 751–756. [Google Scholar] [CrossRef]
- Anderson, I.H.; Levine, A.S.; Levitt, M.D. Incomplete absorption of the carbohydrate in all-purpose wheat flour. N. Engl. J. Med. 1981, 304, 891–892. [Google Scholar] [CrossRef]
- Usai, P.; Manca, R.; Cuomo, R.; Lai, M.A.; Russo, L.; Boi, M.F. Effect of gluten-free diet on preventing recurrence of gastroesophageal reflux disease-related symptoms in adult celiac patients with nonerosive reflux disease. J. Gastroenterol. Hepatol. 2008, 23, 1368–1372. [Google Scholar] [CrossRef]
- Di Stefano, M.; Mengoli, C.; Bergonzi, M.; Miceli, E.; Pagani, E.; Corazza, G.R. Hydrogen breath test in patients with severe constipation: The interference of the mixing of intestinal content. Neurogastroenterol. Motil. 2014, 26, 1754–1760. [Google Scholar] [CrossRef]
- Baran, M.; Cagan Appak, Y.; Karakoyun, M.; Yalcinkaya, S.; Eliacik, K.; Dundar, B.N. The overlap of gastroesophageal reflux disease and functional constipation in children: The efficacy of constipation treatment. Eur. J. Gastroenterol. Hepatol. 2017, 29, 1264–1268. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, M.; Salari, R.; Rad, M.A.; Salehi, M.; Birjandi, B.; Salari, M. Comparing the Effect of Psyllium Seed on Gastroesophageal Reflux Disease with Oral Omeprazole in Patients With Functional Constipation. J. Evid.-Based Integr. Med. 2018, 23, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Wheat Noodles (n = 8) | Rice Noodles (n = 8) | |
|---|---|---|
| GERD symptoms (Visual analog scale 0–10) | ||
| Heartburn | 1.0 (1.0–1.8) | 1.0 (1.0–1.0) |
| Regurgitation | 2.0 (1.0–3.0) | 2.0 (2.0–2.8) |
| Other GI symptoms (Visual analog scale 0–10) | ||
| Bloating | 3.5 (2.3–4.0) | 2.5 (1.3–3.0) |
| Satiety | 3.0 (2.0–3.8) | 2.0 (0.3–4.0) |
| Abdominal pain | 1.5 (1.0–2.0) | 1.0 (1.0–2.0) |
| Stool urgency | 1.0 (1.0–1.0) | 1.5 (1.0–2.0) |
| Nausea/Vomiting | 2.0 (2.0–3.8) | 2.0 (2.0–3.0) |
| Belching | 2.0 (1.3–3.8) | 2.0 (2.0–2.0) |
| Chest discomfort | 0.00 | 0.00 |
| Flatulence | 1.0 (1.0–1.8) | 1.0 (1.0–1.0) |
| Overall GI symptoms (Visual analog scale 0–10) | 6.0 (5.3–7.0) | 5.0 (4.3–6.0) |
| GERD, Gastroesophageal reflux disease; GI, Gastrointestinal |
| Wheat Noodles (n = 8) | Rice Noodles (n = 8) | |
|---|---|---|
| Overall GI symptoms (Visual analog scale 0–10) * | 7.0 (6.0–8.8) | 4.5 (3.3–6.0) |
| Average postprandial GI symptom scores (Visual analog scale 0–10) | ||
| Heartburn | 2.0 (0.1–3.6) | 0.3 (0.0–1.6) |
| Regurgitation * | 1.5 (0.0–6.1) | 0.3 (0.0–0.9) |
| Bloating * | 7.3 (6.1–7.9) | 3.0 (0.3–5.8) |
| Satiety * | 7.5 (6.6–8.9) | 3.5 (1.1–6.1) |
| Abdominal pain | 0.8 (0.0–2.1) | 0.3 (0.0–1.6) |
| Stool urgency | 0.3 (0.0–1.6) | 0.0 (0.0–0.5) |
| Nausea/Vomiting | 0.5 (0.1–1.9) | 0.3 (0.0–0.9) |
| Belching * | 3.5 (0.3–6.9) | 0.5 (0.1–0.9) |
| Chest discomfort | 0.3 (0.0–1.0) | 0.3 (0.0–0.5) |
| Flatulence | 1.0 (0.6–2.1) | 1.3 (0.5–1.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plaidum, S.; Patcharatrakul, T.; Promjampa, W.; Gonlachanvit, S. The Effect of Fermentable, Oligosaccharides, Disaccharides, Monosaccharides, and Polyols (FODMAP) Meals on Transient Lower Esophageal Relaxations (TLESR) in Gastroesophageal Reflux Disease (GERD) Patients with Overlapping Irritable Bowel Syndrome (IBS). Nutrients 2022, 14, 1755. https://doi.org/10.3390/nu14091755
Plaidum S, Patcharatrakul T, Promjampa W, Gonlachanvit S. The Effect of Fermentable, Oligosaccharides, Disaccharides, Monosaccharides, and Polyols (FODMAP) Meals on Transient Lower Esophageal Relaxations (TLESR) in Gastroesophageal Reflux Disease (GERD) Patients with Overlapping Irritable Bowel Syndrome (IBS). Nutrients. 2022; 14(9):1755. https://doi.org/10.3390/nu14091755
Chicago/Turabian StylePlaidum, Suppawatsa, Tanisa Patcharatrakul, Wachinee Promjampa, and Sutep Gonlachanvit. 2022. "The Effect of Fermentable, Oligosaccharides, Disaccharides, Monosaccharides, and Polyols (FODMAP) Meals on Transient Lower Esophageal Relaxations (TLESR) in Gastroesophageal Reflux Disease (GERD) Patients with Overlapping Irritable Bowel Syndrome (IBS)" Nutrients 14, no. 9: 1755. https://doi.org/10.3390/nu14091755
APA StylePlaidum, S., Patcharatrakul, T., Promjampa, W., & Gonlachanvit, S. (2022). The Effect of Fermentable, Oligosaccharides, Disaccharides, Monosaccharides, and Polyols (FODMAP) Meals on Transient Lower Esophageal Relaxations (TLESR) in Gastroesophageal Reflux Disease (GERD) Patients with Overlapping Irritable Bowel Syndrome (IBS). Nutrients, 14(9), 1755. https://doi.org/10.3390/nu14091755