
Breast Cancer Diet “BCD”: A Review of Healthy Dietary Patterns to Prevent Breast Cancer Recurrence and Reduce Mortality

 ,
,  , and
, and
Abstract
:1. Introduction
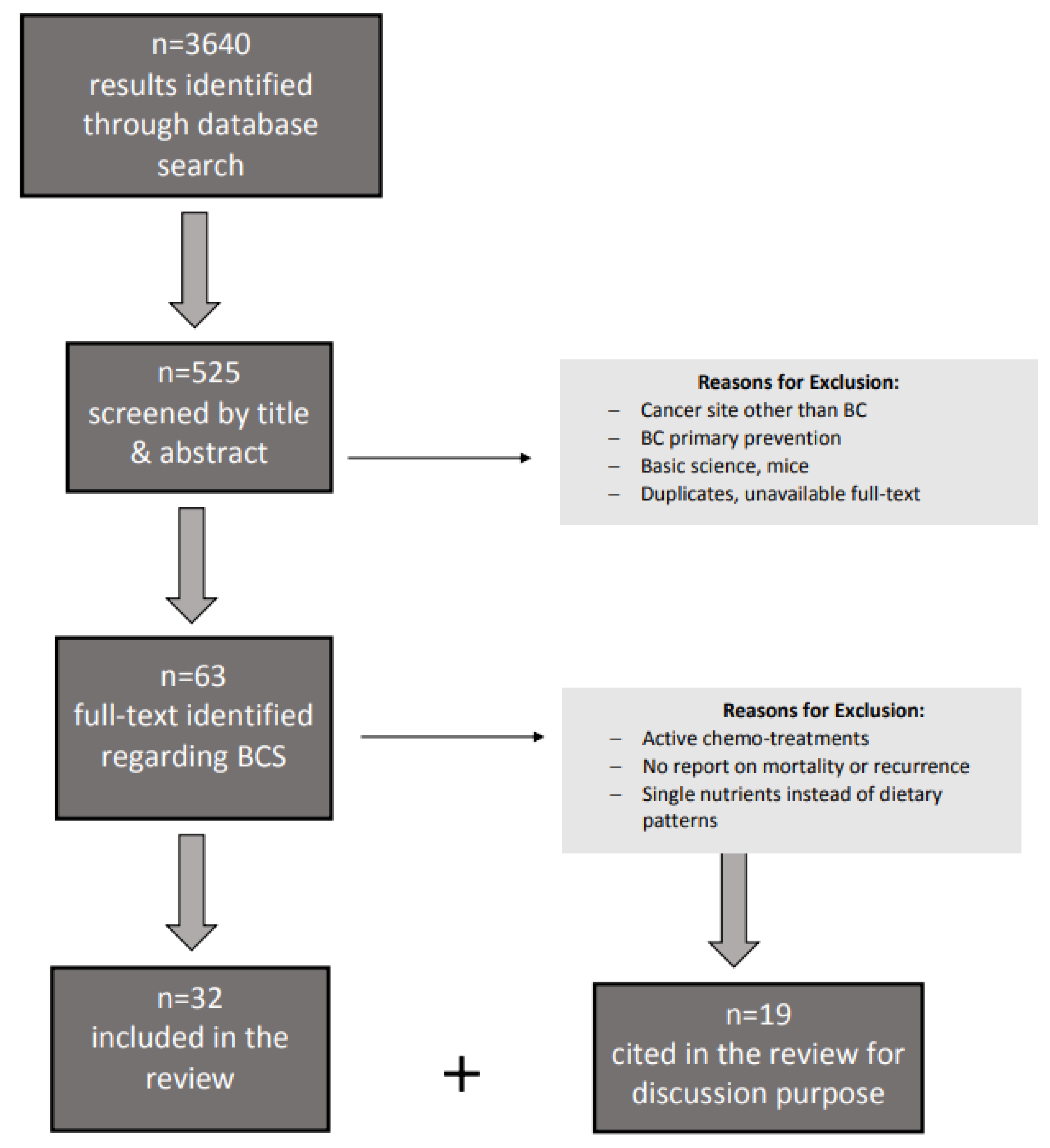
2. Methods
3. Results
4. The Role of Diet Quality in Breast Cancer Survivors
5. Breast Cancer Relation with Insulin Resistance, Dietary Carbohydrate, and Glycemic Index/Glycemic Load
6. Discussion
Weight Gain and Weight Management during and after BC Diagnosis
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Dietary Index and Dietary Pattern Description
References
- World Cancer Research Fund/American Institute for Cancer Research. Continuous Update Project Expert Report 2018. Diet, Nutrition, Physical Activity and Breast Cancer. Available online: dietandcancerreport.org (accessed on 25 November 2021).
- Shaikh, H.; Bradhurst, P.; Ma, L.X.; Tan, S.Y.; Egger, S.J.; Vardy, J.L. Body weight management in overweight and obese breast cancer survivors. Cochrane Database Syst. Rev. 2020, 12, CD012110. [Google Scholar] [CrossRef] [PubMed]
- De Cicco, P.; Catani, M.V.; Gasperi, V.; Sibilano, M.; Quaglietta, M.; Savini, I. Nutrition and Breast Cancer: A Literature Review on Prevention, Treatment and Recurrence. Nutrients 2019, 11, 1514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barone, I.; Giordano, C.; Bonofiglio, D.; Ando, S.; Catalano, S. The weight of obesity in breast cancer progression and metastasis: Clinical and molecular perspectives. In Seminars in Cancer Biology; Academic Press: Cambridge, MA, USA, 2019. [Google Scholar]
- Iyengar, N.M.; Arthur, R.; Manson, J.E.; Chlebowski, R.T.; Kroenke, C.H.; Peterson, L.; Cheng, T.-Y.D.; Feliciano, E.C.; Lane, D.; Luo, J.; et al. Association of Body Fat and Risk of Breast Cancer in Postmenopausal Women with Normal Body Mass Index. JAMA Oncol. 2019, 5, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Bao, W.; Liu, B.; Caan, B.J.; Lane, D.S.; Millen, A.E.; Simon, M.S.; Thomson, C.A.; Tinker, L.F.; Van Horn, L.V.; et al. Changes in Overall Diet Quality in Relation to Survival in Postmenopausal Women with Breast Cancer: Results from the Women’s Health Initiative. J. Acad. Nutr. Diet. 2018, 118, 1855–1863.e6. [Google Scholar] [CrossRef]
- Wang, F.; Cai, H.; Gu, K.; Shi, L.; Yu, D.; Zhang, M.; Zheng, W.; Zheng, Y.; Bao, P.-P.; Shu, X.-O. Adherence to Dietary Recommendations among Long-Term Breast Cancer Survivors and Cancer Outcome Associations. Cancer Epidemiol. Biomark. Prev. 2019, 29, 386–395. [Google Scholar] [CrossRef]
- Farvid, M.S.; Holmes, M.D.; Chen, W.Y.; Rosner, B.A.; Tamimi, R.M.; Willett, W.C.; Eliassen, A.H. Postdiagnostic Fruit and Vegetable Consumption and Breast Cancer Survival: Prospective Analyses in the Nurses’ Health Studies. Cancer Res. 2020, 80, 5134–5143. [Google Scholar] [CrossRef]
- Porciello, G.; Montagnese, C.; Crispo, A.; Grimaldi, M.; Libra, M.; Vitale, S.; Palumbo, E.; Pica, R.; Calabrese, I.; Cubisino, S.; et al. Mediterranean diet and quality of life in women treated for breast cancer: A baseline analysis of DEDiCa multicentre trial. PLoS ONE 2020, 15, e0239803. [Google Scholar] [CrossRef] [PubMed]
- Zucchetto, A.; Serraino, D.; Shivappa, N.; Hébert, J.R.; Stocco, C.; Puppo, A.; Falcini, F.; Panato, C.; Dal Maso, L.; Polesel, J. Dietary inflammatory index before diagnosis and survival in an Italian cohort of women with breast cancer. Br. J. Nutr. 2017, 117, 1456–1462. [Google Scholar] [CrossRef] [Green Version]
- Jang, H.; Chung, M.S.; Kang, S.S.; Park, Y. Association between the Dietary Inflammatory Index and Risk for Cancer Recurrence and Mortality among Patients with Breast Cancer. Nutrients 2018, 10, 1095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.; Quiambao, A.L.; Lee, J.; Ro, J.; Lee, E.-S.; Jung, S.-Y.; Sung, M.-K.; Kim, J. Dietary Inflammatory Index and Risk of Breast Cancer Based on Hormone Receptor Status: A Case-Control Study in Korea. Nutrients 2019, 11, 1949. [Google Scholar] [CrossRef] [Green Version]
- Chlebowski, R.T.; Aragaki, A.K.; Anderson, G.L.; Thomson, C.A.; Manson, J.E.; Simon, M.S.; Howard, B.V.; Rohan, T.E.; Snetselar, L.; Lane, D.; et al. Low-Fat Dietary Pattern and Breast Cancer Mortality in the Women’s Health Initiative Randomized Controlled Trial. J. Clin. Oncol. 2017, 35, 2919–2926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, J.L.M.; Hansen, L.; Thomsen, B.L.R.; Christiansen, L.R.; Dragsted, L.O.; Olsen, A. Pre- and post-diagnostic intake of whole grain and dairy products and breast cancer prognosis: The Danish Diet, Cancer and Health cohort. Breast Cancer Res. Treat. 2019, 179, 743–753. [Google Scholar] [CrossRef] [PubMed]
- Castro-Quezada, I.; Villegas, A.S.; Martínez-González, M.Á.; Salas-Salvadó, J.; Corella, D.; Estruch, R.; Schröder, H.; Álvarez-Pérez, J.; Ruiz-López, M.D.; Artacho, R.; et al. Glycemic index, glycemic load and invasive breast cancer incidence in postmenopausal women: The PREDIMED study. Eur. J. Cancer Prev. 2016, 25, 524–532. [Google Scholar] [CrossRef] [PubMed]
- McCullough, M.L.; Gapstur, S.M.; Shah, R.; Campbell, P.T.; Wang, Y.; Doyle, C.; Gaudet, M.M. Pre- and postdiagnostic diet in relation to mortality among breast cancer survivors in the CPS-II Nutrition Cohort. Cancer Causes Control 2016, 27, 1303–1314. [Google Scholar] [CrossRef]
- Ramirez, A.G.; Parma, D.L.; Muñoz, E.; Mendoza, K.D.; Harb, C.; Holden, A.E.; Wargovich, M. An anti-inflammatory dietary intervention to reduce breast cancer recurrence risk: Study design and baseline data. Contemp. Clin. Trials 2017, 57, 1–7. [Google Scholar] [CrossRef]
- Wu, T.; Seaver, P.; Lemus, H.; Hollenbach, K.; Wang, E.; Pierce, J.P. Associations between Dietary Acid Load and Biomarkers of Inflammation and Hyperglycemia in Breast Cancer Survivors. Nutrients 2019, 11, 1913. [Google Scholar] [CrossRef] [Green Version]
- Finocchiaro, C.; Ossola, M.; Monge, T.; Fadda, M.; Brossa, L.; Caudera, V.; De Francesco, A. Effect of specific educational program on dietary change and weight loss in breast-cancer survivors. Clin. Nutr. 2015, 35, 864–870. [Google Scholar] [CrossRef]
- Thompson, H.J.; Sedlacek, S.M.; Playdon, M.C.; Wolfe, P.; McGinley, J.N.; Paul, D.; Lakoski, S.G. Weight Loss Interventions for Breast Cancer Survivors: Impact of Dietary Pattern. PLoS ONE 2015, 10, e0127366. [Google Scholar] [CrossRef]
- Skouroliakou, M.; Grosomanidis, D.; Massara, P.; Kostara, C.; Papandreou, P.; Ntountaniotis, D.; Xepapadakis, G. Serum antioxidant capacity, biochemical profile and body composition of breast cancer survivors in a randomized Mediterranean dietary intervention study. Eur. J. Nutr. 2017, 57, 2133–2145. [Google Scholar] [CrossRef]
- Parada, H.; Sun, X.; Tse, C.-K.; Olshan, A.F.; Troester, M.A. Lifestyle Patterns and Survival Following Breast Cancer in the Carolina Breast Cancer Study. Epidemiology 2019, 30, 83–92. [Google Scholar] [CrossRef]
- Dittus, K.L.; Harvey, J.R.; Bunn, J.Y.; Kokinda, N.D.; Wilson, K.M.; Priest, J.; Pratley, R.E. Impact of a behaviorally-based weight loss intervention on parameters of insulin resistance in breast cancer survivors. BMC Cancer 2018, 18, 351. [Google Scholar] [CrossRef] [Green Version]
- Toledo, E.; Salas-Salvado, J.; Donat-Vargas, C.; Buil-Cosiales, P.; Estruch, R.; Ros, E.; Corella, D.; Fito, M.; Hu, F.B.; Aros, F.; et al. Mediterranean diet and invasive breast cancer risk among women at high cardiovascular risk in the predimed trial: A randomized clinical trial. JAMA Intern. Med. 2015, 175, 1752–1760. [Google Scholar] [CrossRef] [PubMed]
- Ricceri, F.; Fasanelli, F.; Giraudo, M.T.; Sieri, S.; Tumino, R.; Mattiello, A.; Vagliano, L.; Masala, G.; Quirós, J.R.; Travier, N.; et al. Risk of second primary malignancies in women with breast cancer: Results from the European prospective investigation into cancer and nutrition (EPIC). Int. J. Cancer 2015, 137, 940–948. [Google Scholar] [CrossRef] [PubMed]
- Hamer, J.; Warner, E. Lifestyle modifications for patients with breast cancer to improve prognosis and optimize overall health. Can. Med. Assoc. J. 2017, 189, E268–E274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maliniak, M.L.; Patel, A.V.; McCullough, M.L.; Campbell, P.T.; Leach, C.R.; Gapstur, S.M.; Gaudet, M.M. Obesity, physical activity, and breast cancer survival among older breast cancer survivors in the Cancer Prevention Study-II Nutrition Cohort. Breast Cancer Res. Treat. 2017, 167, 133–145. [Google Scholar] [CrossRef]
- Jochems, S.H.J.; Van Osch, F.H.M.; Bryan, R.; Wesselius, A.; Van Schooten, F.J.; Cheng, K.K.; Zeegers, M. Impact of dietary patterns and the main food groups on mortality and recurrence in cancer survivors: A systematic review of current epidemiological literature. BMJ Open 2017, 8, e014530. [Google Scholar] [CrossRef]
- Kwan, M.L.; Weltzien, E.; Kushi, L.H.; Castillo, A.; Slattery, M.L.; Caan, B.J. Dietary Patterns and Breast Cancer Recurrence and Survival Among Women With Early-Stage Breast Cancer. J. Clin. Oncol. 2009, 27, 919–926. [Google Scholar] [CrossRef] [Green Version]
- Shi, Z.; Rundle, A.; Genkinger, J.M.; Cheung, Y.K.; Ergas, I.J.; Roh, J.M.; Kushi, L.H.; Kwan, M.L.; Greenlee, H. Distinct trajectories of fruits and vegetables, dietary fat, and alcohol intake following a breast cancer diagnosis: The Pathways Study. Breast Cancer Res. Treat. 2019, 179, 229–240. [Google Scholar] [CrossRef]
- Augustin, L.S.; Libra, M.; Crispo, A.; Grimaldi, M.; De Laurentiis, M.; Rinaldo, M.; D’Aiuto, M.; Catalano, F.; Banna, G.; Ferrau’, F.; et al. Low glycemic index diet, exercise and vitamin D to reduce breast cancer recurrence (DEDiCa): Design of a clinical trial. BMC Cancer 2017, 17, 69. [Google Scholar] [CrossRef] [Green Version]
- Ghose, A.; Kundu, R.; Toumeh, A.; Hornbeck, C.; Mohamed, I. A Review of Obesity, Insulin Resistance, and the Role of Exercise in Breast Cancer Patients. Nutr. Cancer 2015, 67, 197–202. [Google Scholar] [CrossRef]
- Mullie, P.; Koechlin, A.; Boniol, M.; Autier, P.; Boyle, P. Relation between Breast Cancer and High Glycemic Index or Glycemic Load: A Meta-analysis of Prospective Cohort Studies. Crit. Rev. Food Sci. Nutr. 2014, 56, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Schlesinger, S.; Chan, D.S.; Vingeliene, S.; Vieira, A.R.; Abar, L.; Polemiti, E.; Stevens, C.A.; Greenwood, D.C.; Aune, D.; Norat, T. Carbohydrates, glycemic index, glycemic load, and breast cancer risk: A systematic review and dose–response meta-analysis of prospective studies. Nutr. Rev. 2017, 75, 420–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amadou, A.; Degoul, J.; Hainaut, P.; Chajes, V.; Biessy, C.; Mejia, G.T.; Huybrechts, I.; Macia, H.M.; Ortega, C.; Angeles-Llerenas, A.; et al. Dietary Carbohydrate, Glycemic Index, Glycemic Load, and Breast Cancer Risk Among Mexican Women. Epidemiology 2015, 26, 917–924. [Google Scholar] [CrossRef] [PubMed]
- Terranova, C.O.; Protani, M.M.; Reeves, M.M. Overall Dietary Intake and Prognosis after Breast Cancer: A Systematic Review. Nutr. Cancer 2018, 70, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Braakhuis, A.J.; Campion, P.; Bishop, K.S. Reducing Breast Cancer Recurrence: The Role of Dietary Polyphenolics. Nutrients 2016, 8, 547. [Google Scholar] [CrossRef] [PubMed]
- Tsaban, G.; Meir, A.Y.; Rinott, E.; Zelicha, H.; Kaplan, A.; Shalev, A.; Katz, A.; Rudich, A.; Tirosh, A.; Shelef, I.; et al. The effect of green Mediterranean diet on cardiometabolic risk; a randomised controlled trial. Heart 2020, 107, 1054–1061. [Google Scholar] [CrossRef]
- Morris, P.G.; Hudis, C.A.; Giri, D.; Morrow, M.; Falcone, D.J.; Zhou, X.K.; Du, B.; Brogi, E.; Crawford, C.B.; Kopelovich, L.; et al. Inflammation and Increased Aromatase Expression Occur in the Breast Tissue of Obese Women with Breast Cancer. Cancer Prev. Res. 2011, 4, 1021–1029. [Google Scholar] [CrossRef] [Green Version]
- Iyengar, N.M.; Morris, P.G.; Zhou, X.K.; Gucalp, A.; Giri, D.; Harbus, M.D.; Falcone, D.J.; Krasne, M.; Vahdat, L.T.; Subbaramaiah, K.; et al. Menopause Is a Determinant of Breast Adipose Inflammation. Cancer Prev. Res. 2015, 8, 349–358. [Google Scholar] [CrossRef] [Green Version]
- Kabat, G.C.; Kim, M.Y.; Lee, J.S.; Ho, G.Y.; Going, S.B.; Beebe-Dimmer, J.; Manson, J.E.; Chlebowski, R.T.; Rohan, T.E. Metabolic Obesity Phenotypes and Risk of Breast Cancer in Postmenopausal Women. Cancer Epidemiol. Biomark. Prev. 2017, 26, 1730–1735. [Google Scholar] [CrossRef] [Green Version]
- Pierobon, M.; Frankenfeld, C. Obesity as a risk factor for triple-negative breast cancers: A systematic review and meta-analysis. Breast Cancer Res. Treat. 2012, 137, 307–314. [Google Scholar] [CrossRef]
- Harborg, S.; Zachariae, R.; Olsen, J.; Johannsen, M.; Cronin-Fenton, D.; Bøggild, H.; Borgquist, S. Overweight and prognosis in triple-negative breast cancer patients: A systematic review and meta-analysis. NPJ Breast Cancer 2021, 7, 119. [Google Scholar] [CrossRef] [PubMed]
- Limon-Miro, A.T.; Lopez-Teros, V.; Astiazaran-Garcia, H. Dietary Guidelines for Breast Cancer Patients: A Critical Review. Adv. Nutr. 2017, 8, 613–623. [Google Scholar] [CrossRef]
- Zheng, J.; Tabung, F.K.; Zhang, J.; Liese, A.D.; Shivappa, N.; Ockene, J.K.; Caan, B.; Kroenke, C.H.; Hébert, J.R.; Steck, S.E. Association between Post-Cancer Diagnosis Dietary Inflammatory Potential and Mortality among Invasive Breast Cancer Survivors in the Women’s Health Initiative. Cancer Epidemiol. Biomark. Prev. 2018, 27, 454–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalledsøe, L.; Dragsted, L.O.; Hansen, L.; Kyrø, C.; Grønbæk, H.; Tjønneland, A.; Olsen, A. The insulin-like growth factor family and breast cancer prognosis: A prospective cohort study among postmenopausal women in Denmark. Growth Horm. IGF Res. 2018, 44, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Demark-Wahnefried, W.; Rogers, L.Q.; Gibson, J.; Harada, S.; Frugé, A.; Oster, R.; Grizzle, W.E.; Norian, L.A.; Yang, E.S.; Della Manna, D.; et al. Randomized trial of weight loss in primary breast cancer: Impact on body composition, circulating biomarkers and tumor characteristics. Int. J. Cancer 2019, 146, 2784–2796. [Google Scholar] [CrossRef] [PubMed]
- Adams, B.D.; Arem, H.; Hubal, M.; Cartmel, B.; Li, F.; Harrigan, M.; Sanft, T.; Cheng, C.J.; Pusztai, L.; Irwin, M.L. Exercise and weight loss interventions and miRNA expression in women with breast cancer. Breast Cancer Res. Treat. 2018, 170, 55–67. [Google Scholar] [CrossRef]
- Zhang, S.; Ikramuddin, S.; Beckwith, H.C.; Sheka, A.C.; Wirth, K.M.; Blaes, A.H. The Impact of Bariatric Surgery on Breast Cancer Recurrence: Case Series and Review of Literature. Obes. Surg. 2019, 30, 780–785. [Google Scholar] [CrossRef] [Green Version]
- Basen-Engquist, K.M.; Raber, M.; Carmack, C.L.; Arun, B.; Brewster, A.M.; Fingeret, M.; Schembre, S.M.; Harrison, C.; Perkins, H.Y.; Li, Y.; et al. Feasibility and efficacy of a weight gain prevention intervention for breast cancer patients receiving neoadjuvant chemotherapy: A randomized controlled pilot study. Support. Care Cancer 2020, 28, 5821–5832. [Google Scholar] [CrossRef]
- Travier, N.; Buckland, G.; Vendrell, J.J.; Fernandez-Veledo, S.; Peiró, I.; Del Barco, S.; Pernas, S.; Zamora, E.; Bellet, M.; Margeli, M.; et al. Changes in metabolic risk, insulin resistance, leptin and adiponectin following a lifestyle intervention in overweight and obese breast cancer survivors. Eur. J. Cancer Care 2018, 27, e12861. [Google Scholar] [CrossRef]
- Tollosa, D.N.; Holliday, E.; Hure, A.; Tavener, M.; James, E.L. A 15-year follow-up study on long-term adherence to health behaviour recommendations in women diagnosed with breast cancer. Breast Cancer Res. Treat. 2020, 182, 727–738. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Reference | Subjects (n) | Methods | Main Outcome | Dietary Index/Pattern |
|---|---|---|---|---|
| Sun et al. [6] | 2295 postmenopausal women with invasive BC | HEI-2010 score assessed over a 12-year follow-up in the WHI (women’s health initiative) study | Decreased diet quality after BC diagnosis was associated with higher risk of death from breast cancer | Healthy Eating Index (HEI)-2010 |
| Wang et al. [7] | 3450 5-year BCS | Adherence scores to CHFP-2007, CHFP-2016, modified DASH, and HEI-2015 | Higher adherence to CHFP and DASH dietary guidelines associated with reduced risk of overall death and BCr-specific recurrence or death among long-term BCS | Chinese Food Pagoda (CHFP) Healthy Eating Index (HEI) 2015 DASH diet |
| Farvid et al. [8] | 8927 women with stage I–III BC identified during follow-up of the | Assessing post-diagnostic fruit and vegetable consumption in the Nurses’ Health Study (NHS; 1980–2010) and NHSII (1991–2011) with FFQ every four years | High fruit and vegetable consumption may be associated with better overall survival among BC patients, but not breast cancer-specific mortality. High fruit juice consumption may be associated with poorer prognosis. | |
| Porciello et al. [9] | 309 women (stages I–III, mean age 52 ± 1 years, BMI 27 ± 7 kg/m2). | HRQoL was assessed with questionnaires measuring physical, mental, emotional and social factors: EQ-5D-3L, EORTC QLQ-C30, EORTC QLQ-BR23. | Higher adherence (PREDIMED score > 7) to the MedDiet in BCS is associated with better QoL (physical functioning, sleep, pain, well-being) | Mediterranean Diet (MD) |
| Zucchetto et al. [10] | 1453 women | Retrospective cohort study FFQ over 12.6 years FU | No association between the inflammatory potential of diet and the survival of BC women. | Dietary Inflammatory Index (DII) |
| Jang et al. [11] | 511 women undergoing BC-surgery | 213 months follow-up | Anti-inflammatory diets may decrease the risk of cancer recurrence and overall mortality in BCS particularly in younger age, premenopausal status, obesity, HR+, tumor size > 2 cm, and lymph node metastasis. | Dietary Inflammatory Index (DII) |
| Lee et al. [12] | 364 BC patients and 364 age-matched controls | FFQ | Higher DII scores were related to an increased risk of BC for ER+/ PR+ tumors regardless of menopausal status, but not for ER-/PR- status. | Dietary Inflammatory Index (DII) |
| Chlebowski et al. [13] | 48,835 postmenopausal women, aged 50–79 years, with no prior breast cancer, | 8.5 years FU in the WHI DM trial: Usual diet comparison group (60%) vs. dietary intervention group (40%) with reduced fat intake to 20% of energy and increase vegetable, fruit, and grain intake. | Low fat dietary pattern may reduce the risk of death for breast cancer in postmenopausal women. | Low-Fat Diet |
| Andersen et al. [14] | 1965 women with BC | FFQ obtained up to three times, pre- and post-diagnostic, over a period of 18 years (median FU 7 years) | Pre-diagnostic intake of oatmeal/muesli was associated with lower all-cause mortality, and post-diagnostic intake of rye bread was associated with higher breast cancer specific mortality | |
| Castro-Quezada et al. [15] | 4010 women, aged 60–80 years, at high risk for CVD disease, initially free from BC | 137-item FFQ obtained in the PREvención con DIeta MEDiterránea (PREDIMED) study, International Tables of Glycemic Index (GI) and Glycemic Load (GL) values | No associations were found between baseline dietary GI/GL and invasive breast cancer incidence in postmenopausal women | |
| McCullough et al. [16] | 4452 women with locally and regionally staged breast cancer | A nine-point score reflecting concordance with ACS dietary recommendations was calculated pre and post diagnosis | Diets consistent with ACS guidelines were not associated with breast cancer-specific mortality, but with other causes of mortality. | ACS recommendations for cancer prevention |
| Zheng et al. [17] | 2150 postmenopausal women with invasive BC, aged 50–79 years | FFQ on average 1.5 years after diagnosis a median 13.3 years of follow-up | Consuming a more anti-inflammatory diet after breast cancer diagnosis may be a means for reducing risk of death from CVD | Dietary Inflammatory Index (DII) |
| Wu et al. [18] | 3042 BCS | Cross-sectional study with dietary intake in the Women’s Healthy Eating and Living (WHEL) Study | Positive associations between dietary acid load and CRP and HbA1c in BCS, as strong risk factors for BC recurrence and comorbidities | Dietary acid load (DAL) |
| Finocchiaro et al. [19] | 100 BCS | MD intervention with a 6 month follow-up | MD is effective in reducing BMI and waist circumference, and enhancing healthy lifestyle in BCS | Mediterranean Diet (MD) |
| Thompson et al. [20] | 249 post-menopausal BCS | 6-month non-randomized, controlled weight loss intervention with two dietary interventions, LFD and LCD | Loss of body weight and fat mass was effective irrespective of dietary approach on a structured program with monthly assessments | Low-fat (LFD) Low-carbohydrate diet (LCD) |
| Skouroliakou [21] | 70 BCS randomized to MD or control group for 6 months | Anthropometric and biochemical parameters (vitamin C, vitamin A, a-tocopherol and CoQ10 levels, dietary intake and adherence to MD | MD ameliorate serum antioxidant capacity, body composition and glycemic profile of postmenopausal BCS | Mediterranean Diet (MD) |
| Parada et al. [22] | 1808 women with invasive BC | Interviews to assess lifestyle and dietary patterns in the Carolina Breast Cancer Study Phases I/II, 13-year FU | The unhealthy (vs. healthy) behavior and diet pattern was associated with all-cause mortality and with BC-specific mortality | |
| Dittus et al. [23] | 74 post-menopausal BCS, age ≤ 65 years | A 24-week Internet-based behavioral weight loss (BWL) intervention | Behaviorally based weight loss interventions can result in improvements in biomarkers in BCS who achieved ≥5% weight loss and demonstrated significant improvements in insulin resistance | |
| Toledo [24] | 4282 women at high cardiovascular disease risk, aged 60–80 years | Randomized, single-blind, controlled trial with a low-fat diet (control) vs. 2 MD diet intervention 1:1:1 with 4.8 years FU | Beneficial effect of a Mediterranean diet supplemented with extra-virgin olive oil in the primary prevention of BC | Mediterranean Diet (MD) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cava, E.; Marzullo, P.; Farinelli, D.; Gennari, A.; Saggia, C.; Riso, S.; Prodam, F. Breast Cancer Diet “BCD”: A Review of Healthy Dietary Patterns to Prevent Breast Cancer Recurrence and Reduce Mortality. Nutrients 2022, 14, 476. https://doi.org/10.3390/nu14030476
Cava E, Marzullo P, Farinelli D, Gennari A, Saggia C, Riso S, Prodam F. Breast Cancer Diet “BCD”: A Review of Healthy Dietary Patterns to Prevent Breast Cancer Recurrence and Reduce Mortality. Nutrients. 2022; 14(3):476. https://doi.org/10.3390/nu14030476
Chicago/Turabian StyleCava, Edda, Paolo Marzullo, Deborah Farinelli, Alessandra Gennari, Chiara Saggia, Sergio Riso, and Flavia Prodam. 2022. "Breast Cancer Diet “BCD”: A Review of Healthy Dietary Patterns to Prevent Breast Cancer Recurrence and Reduce Mortality" Nutrients 14, no. 3: 476. https://doi.org/10.3390/nu14030476
APA StyleCava, E., Marzullo, P., Farinelli, D., Gennari, A., Saggia, C., Riso, S., & Prodam, F. (2022). Breast Cancer Diet “BCD”: A Review of Healthy Dietary Patterns to Prevent Breast Cancer Recurrence and Reduce Mortality. Nutrients, 14(3), 476. https://doi.org/10.3390/nu14030476