
Dietary Quality of Women of Reproductive Age in Low-Income Settings: A Cross-Sectional Study in Kyrgyzstan


Abstract
:1. Introduction
Literature Review on Nutrition in Kyrgyzstan
2. Materials and Methods
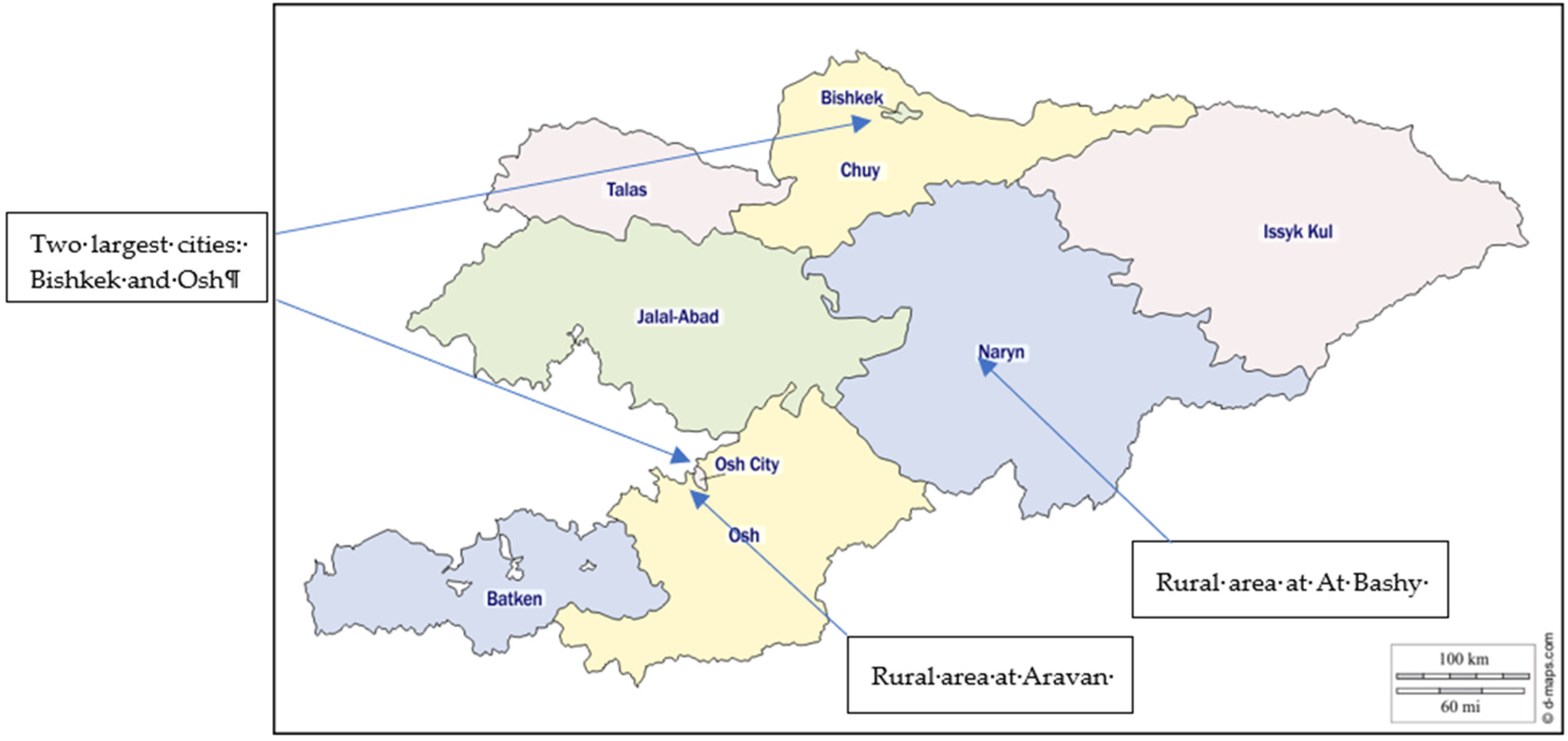
2.1. Study Area
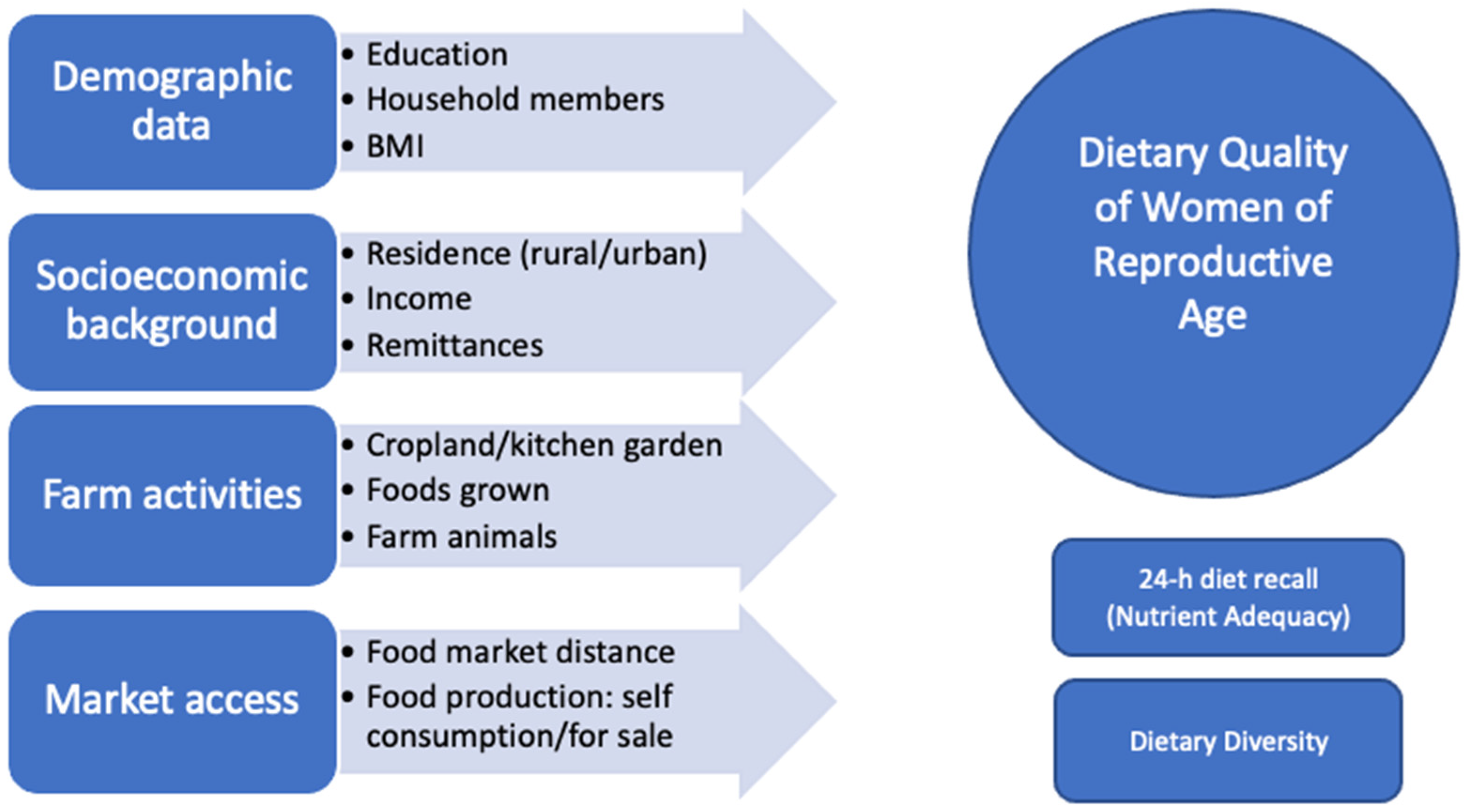
2.2. Questionnaire
2.3. Anthropometric Measurements
2.4. Nutrient Adequacy Ratio
2.5. Dietary Diversity Score
2.6. Data Analysis
3. Results
3.1. Socio-Economic Characteristics of WRAs
3.2. Nutritional Status
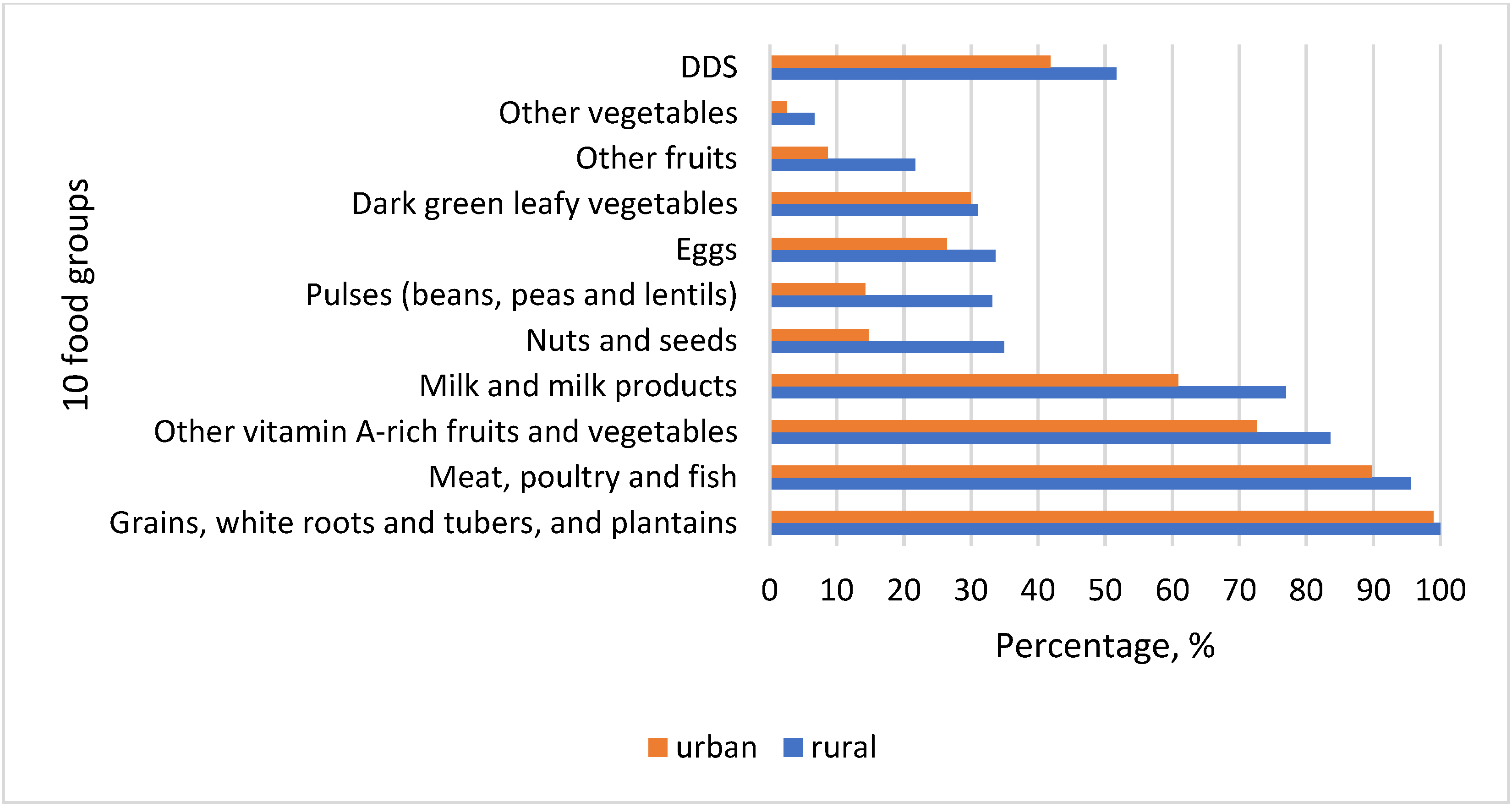
3.3. Individual Food Consumption and Diet Diversity Score (DDS)
3.4. Nutrient Intake and Diet Quality
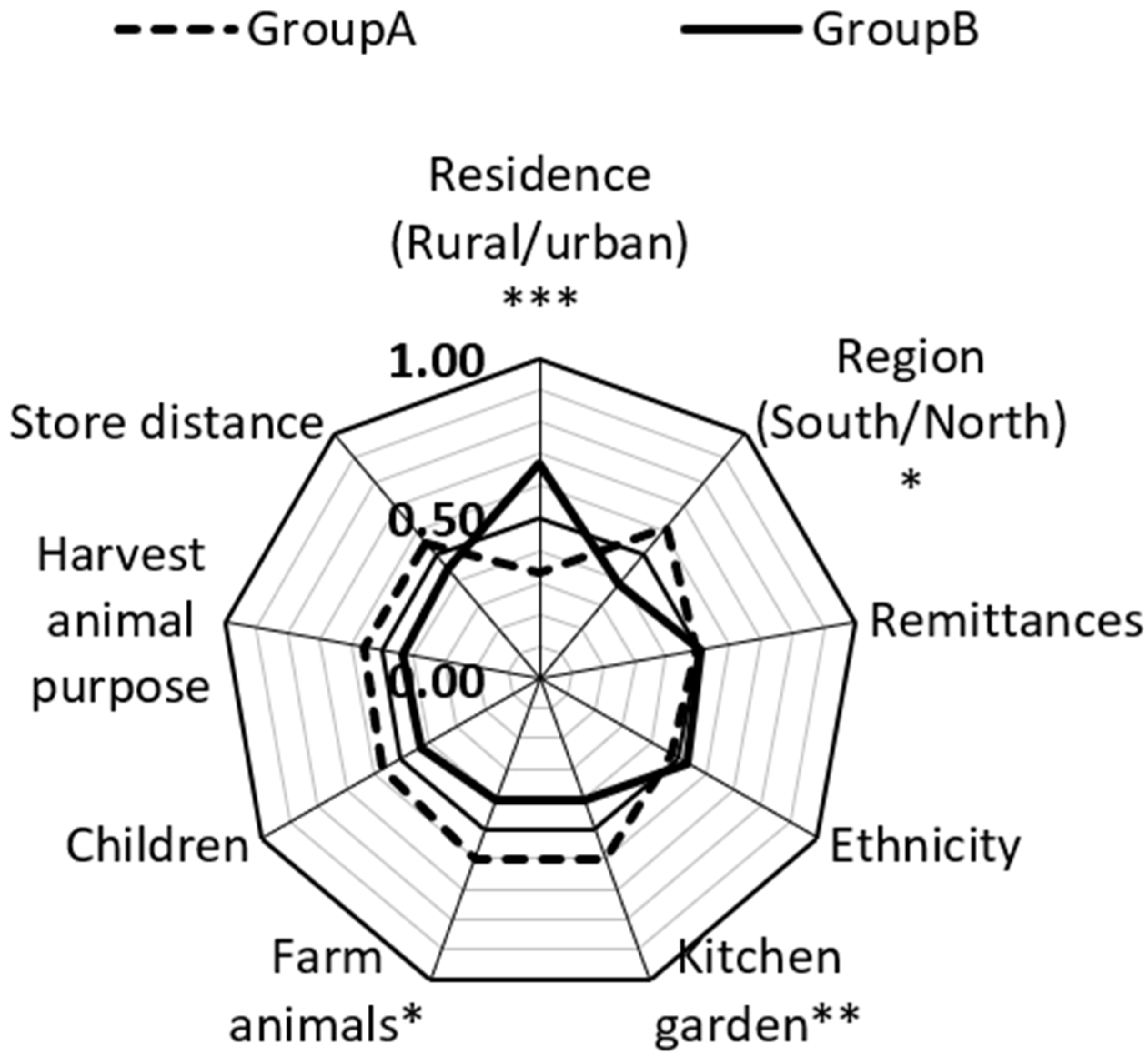
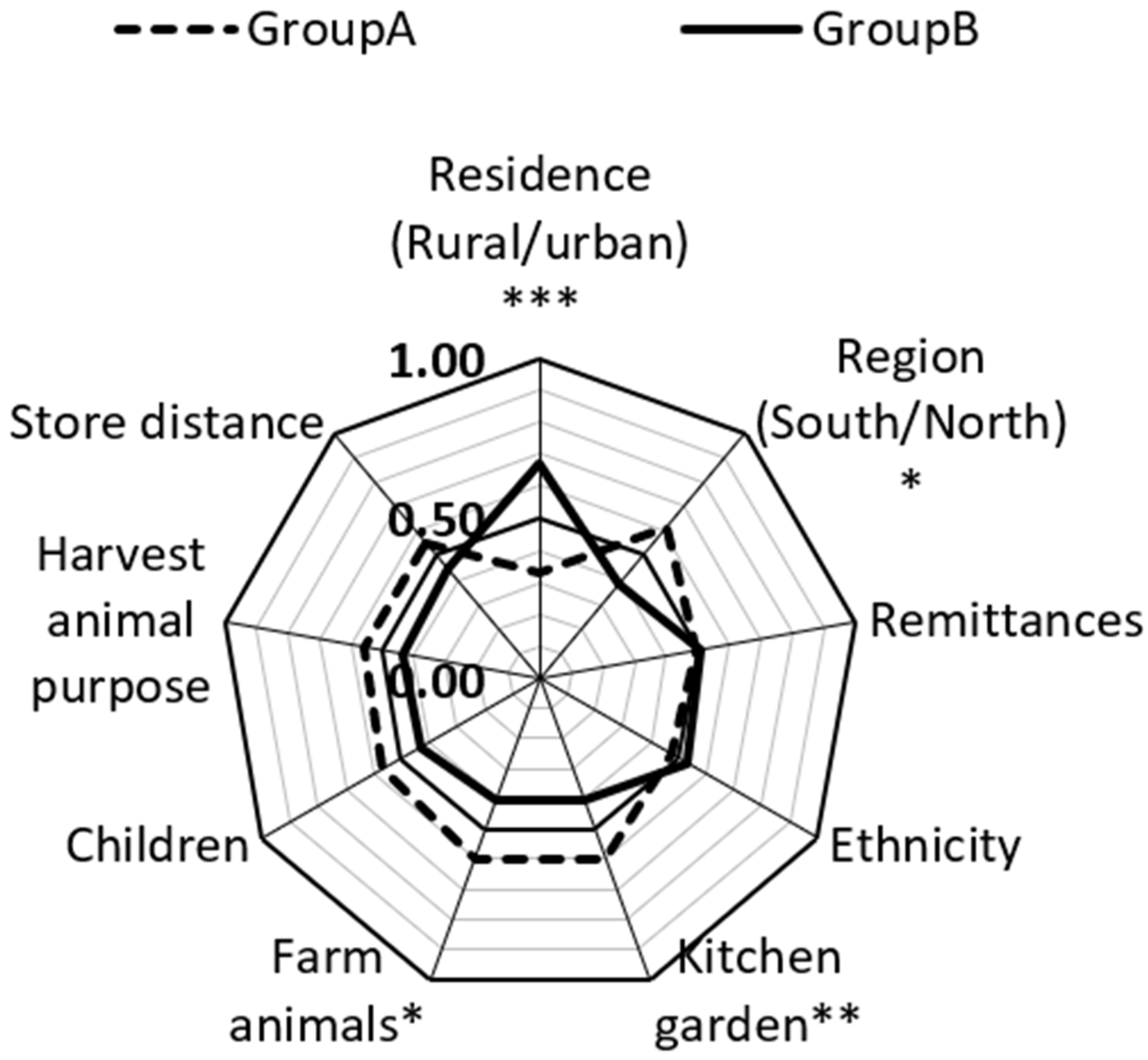
Analysis of Dietary Diversity Concerning Some Socio-Economic and Farm Variables
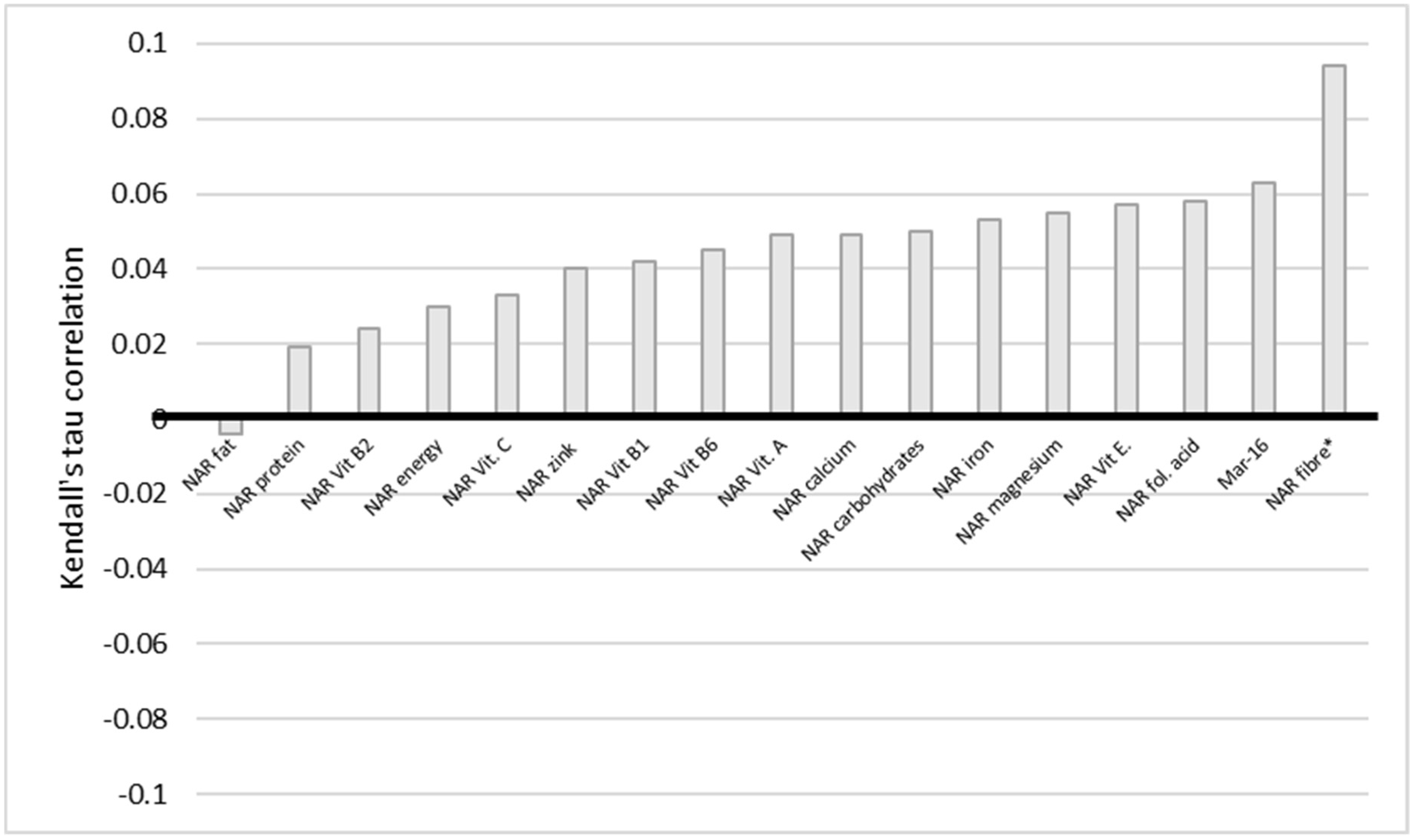
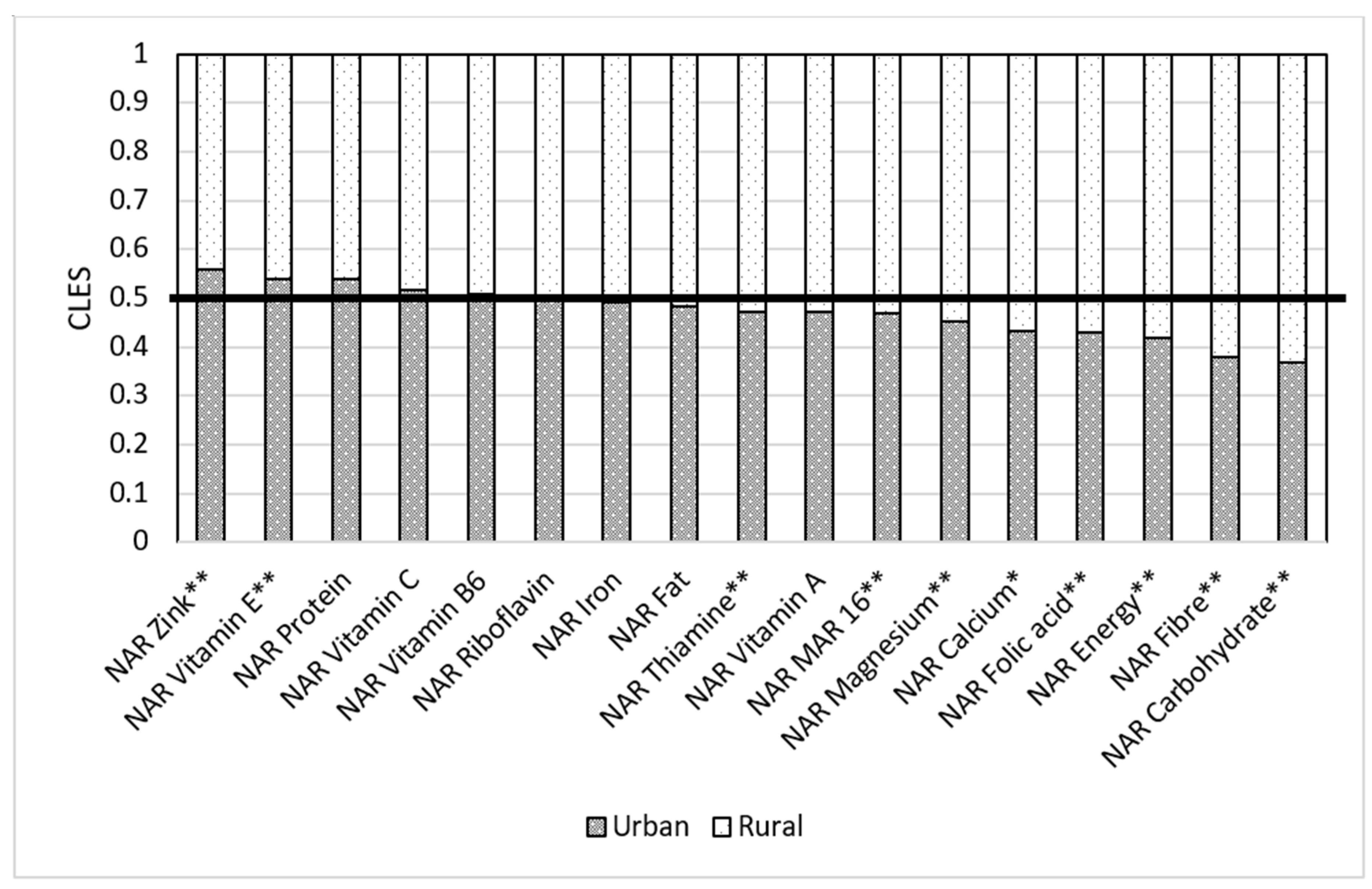
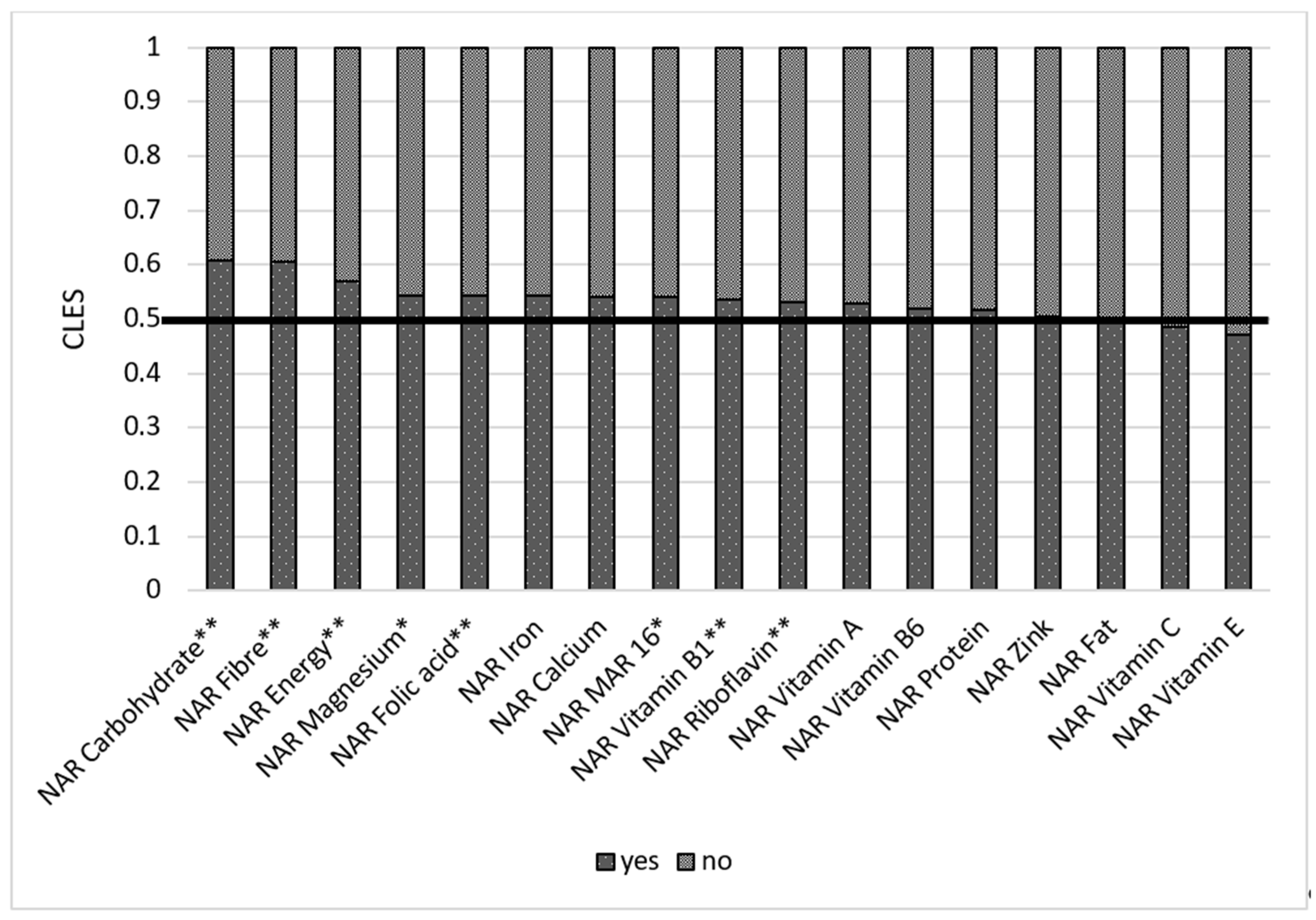
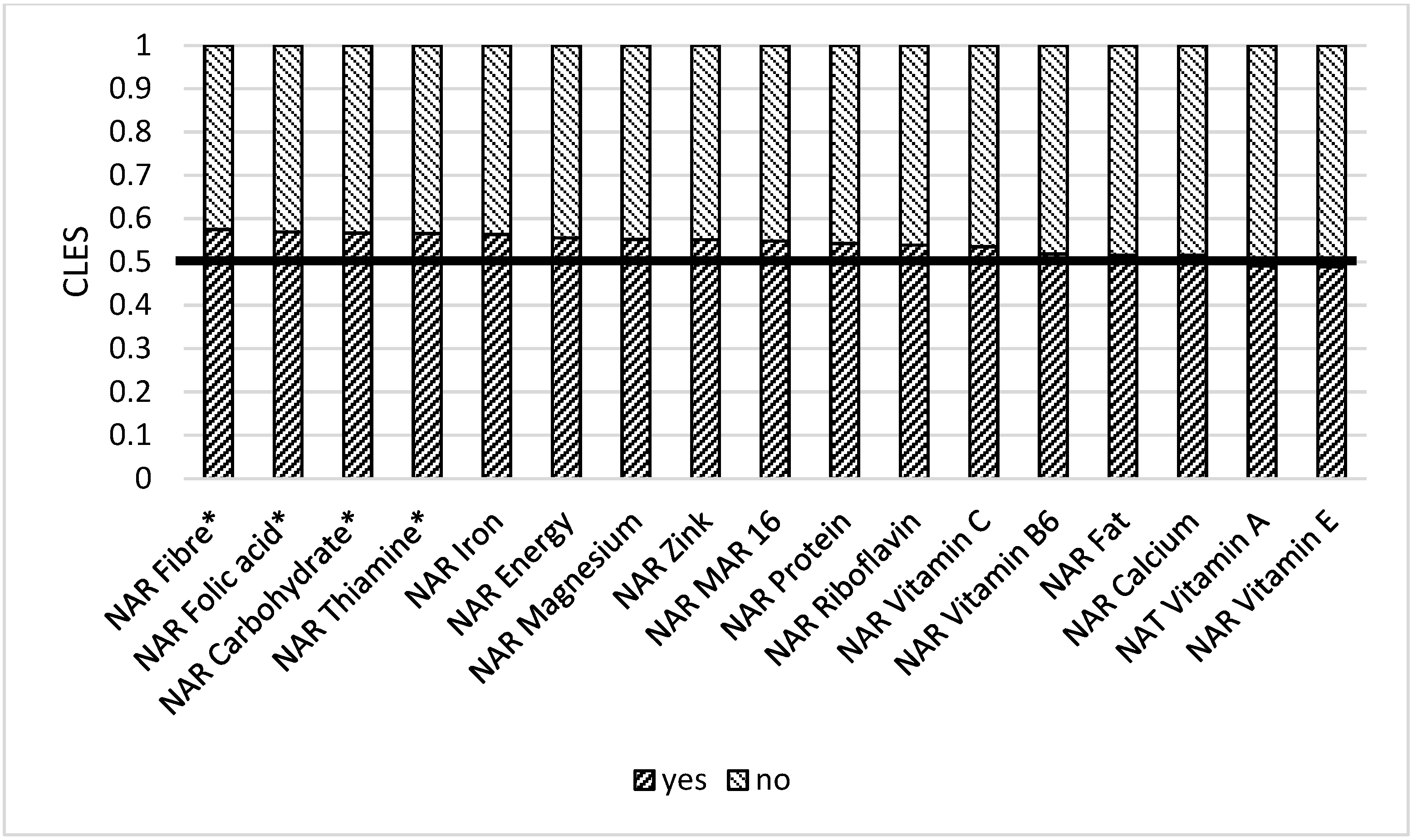
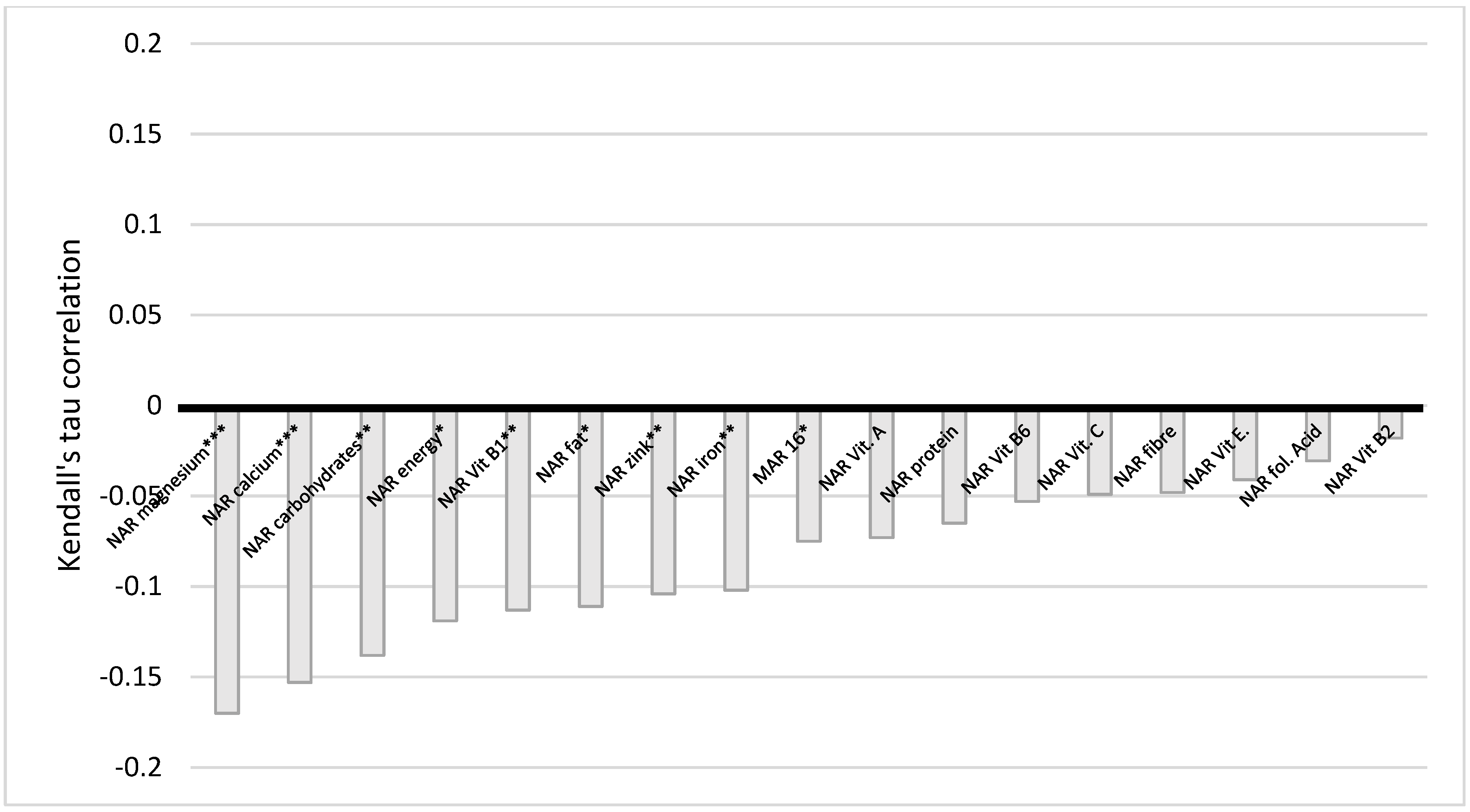
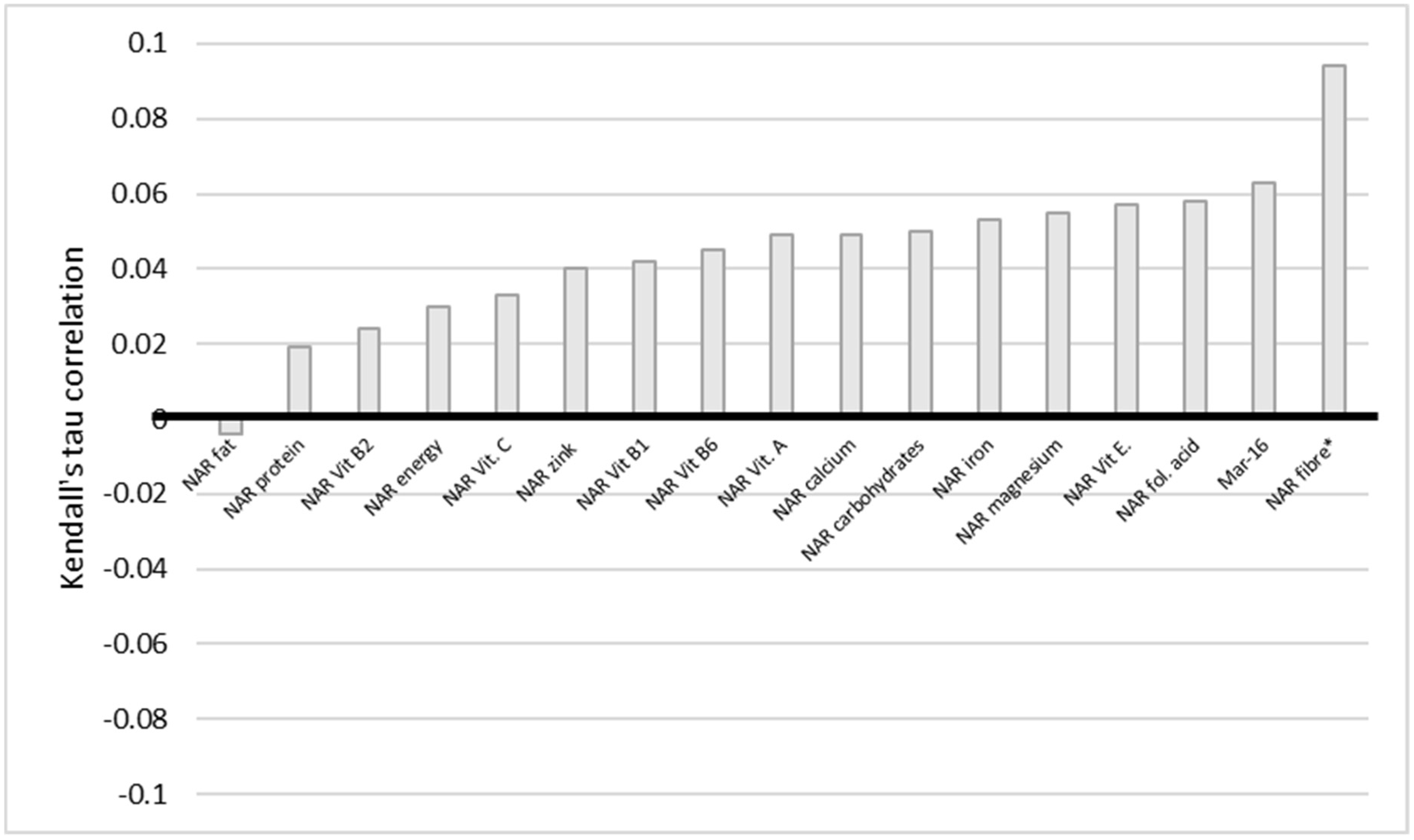
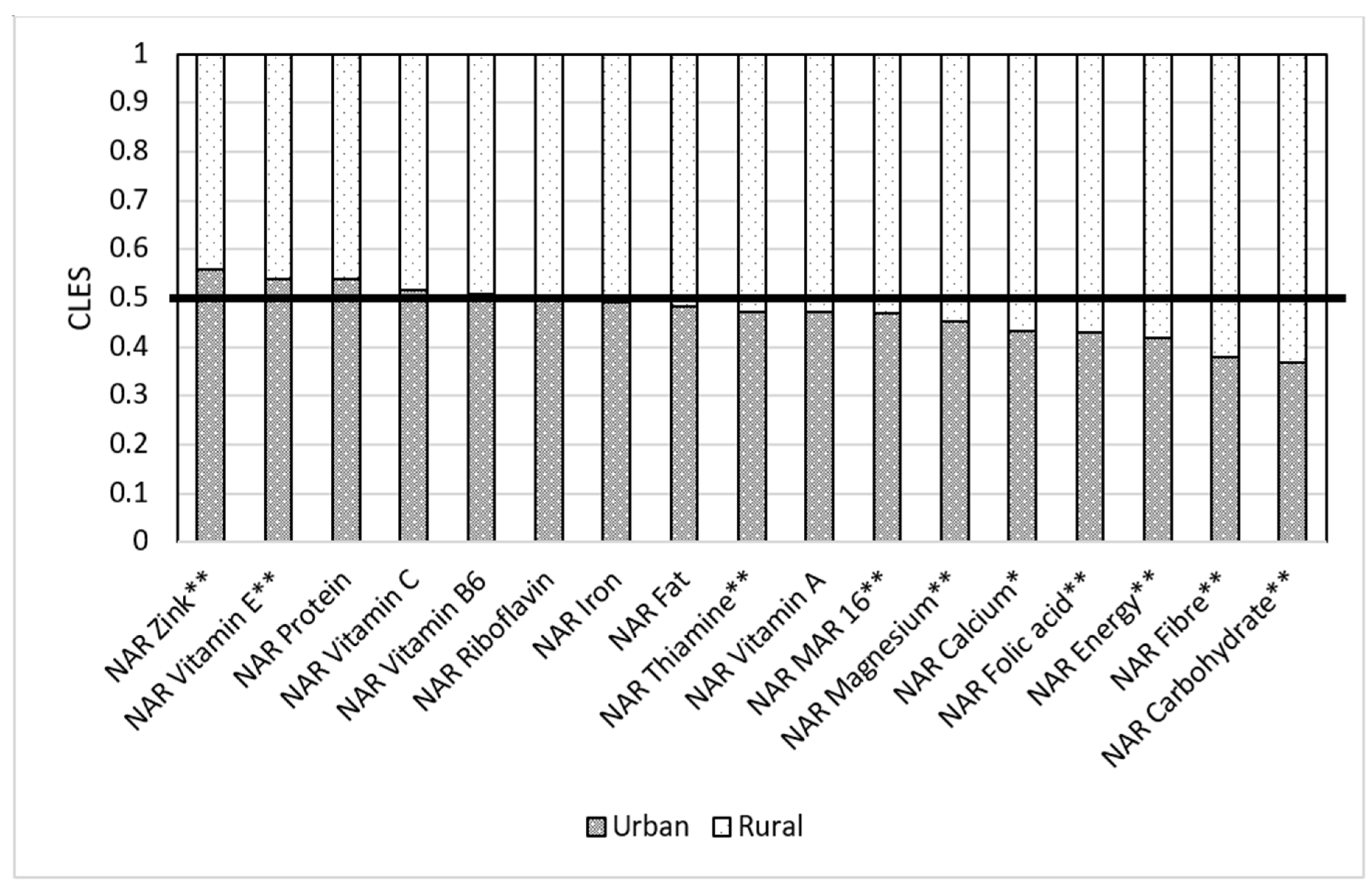
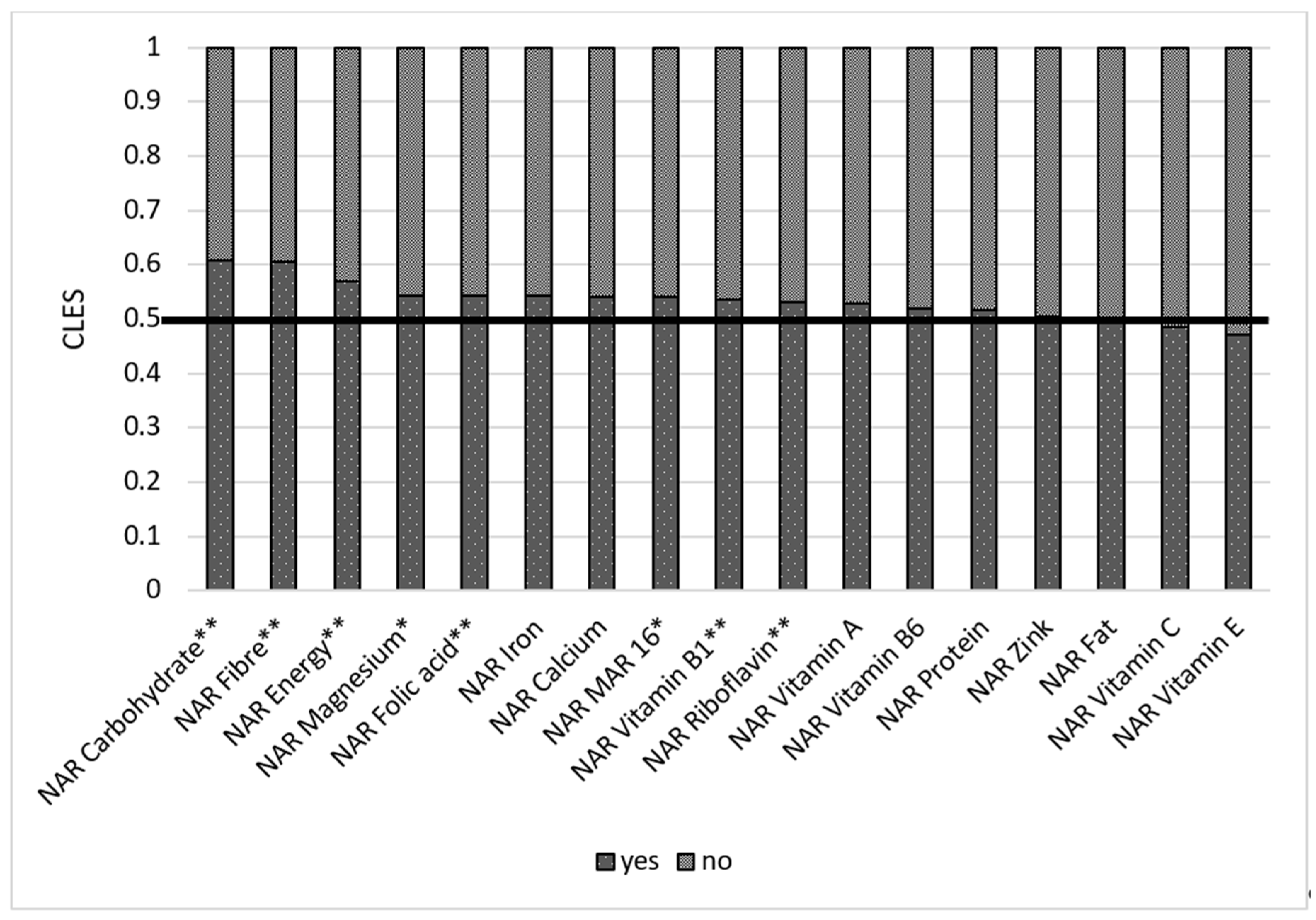
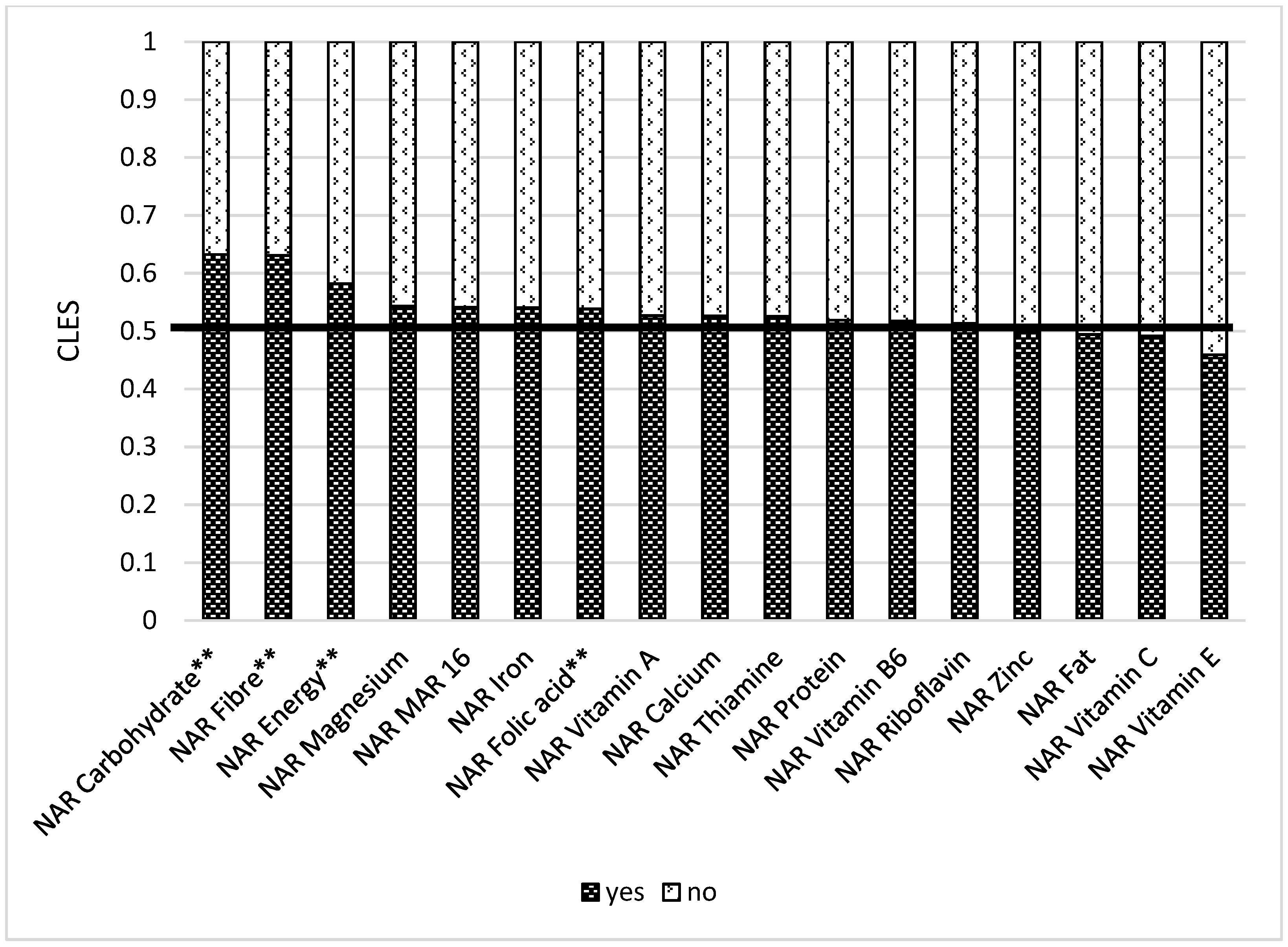
3.5. Nutrient Adequacy Ratio and Its Socio-Economic Factors
4. Discussion
4.1. Socio-Economic Factors and Nutrition Adequacy
4.2. Farm Determinants and Market Access
4.3. Urbanization
4.4. Strengths and Limitations of this Study
5. Conclusions
- Teach household members including women on the organization of nutrition, food storage, planning of food intake for a week, and food preservation training at the household level.
- Inclusion of nutrition classes in the curricula in kindergartens, schools, and universities. This is vital for establishing healthy eating behaviors for future mothers.
- Agriculture should be diversified in the mountainous areas of Kyrgyzstan.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- FAO; IFAD; UNICEF; WFP; WHO. The State of Food Security and Nutrition in the World 2021. In Transforming Food Systems for Food Security, Improved Nutrition and Affordable Healthy Diets for All; FAO: Rome, Italy, 2021. [Google Scholar] [CrossRef]
- Pinstrup-Andersen, P. Agricultural research and policy for better health and nutrition in developing countries: A food systems approach. Agric. Econ. 2007, 37, 187–198. [Google Scholar] [CrossRef] [Green Version]
- Gómez, M.I.; Barrett, C.; Raney, T.; Pinstrup-Andersen, P.; Meerman, J.; Croppenstedt, A.; Carisma, B.; Thompson, B. Post-green revolution food systems and the triple burden of malnutrition. Food Policy 2013, 42, 129–138. [Google Scholar] [CrossRef] [Green Version]
- Nabuuma, D.; Ekesa, B.; Faber, M.; Mbhenyane, X. Community perspectives on food security and dietary diversity among rural smallholder farmers: A qualitative study in central Uganda. J. Agric. Food Res. 2021, 5, 100183. [Google Scholar] [CrossRef]
- Charrondière, U.R.; Stadlmayr, B.; Rittenschober, D.; Mouille, B.; Nilsson, E.; Medhammar, E.; Olango, T.; Eisenwagen, S.; Persijn, D.; Ebanks, K.; et al. FAO/INFOODS food composition database for biodiversity. Food Chem. 2013, 140, 408–412. [Google Scholar] [CrossRef]
- Ahmed, T.; Hossain, M.; Sanin, K.I. Global Burden of Maternal and Child Undernutrition and Micronutrient Deficiencies. Ann. Nutr. Metab. 2012, 61, 8–17. [Google Scholar] [CrossRef]
- Zanello, G.; Shankar, B.; Poole, N. Buy or make? Agricultural production diversity, markets and dietary diversity in Afghanistan. Food Policy 2019, 87, 101731. [Google Scholar] [CrossRef]
- Shin, H.; Lee, Y.-N.; Lee, S.J.; Jang, Y.K. Evaluation of a Community-based Child (Infants and Toddlers) Health Promotion Pilot Project in a Migrant Village in Kyrgyzstan. Child Health Nurs. Res. 2019, 25, 406–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruel, M.T. Operationalizing Dietary Diversity: A Review of Measurement Issues and Research Priorities. J. Nutr. 2003, 133, 3911S–3926S. [Google Scholar] [CrossRef]
- Savy, M.; Martin-Prével, Y.; Sawadogo, P.; Kameli, Y.; Delpeuch, F. Use of variety/diversity scores for diet quality measurement: Relation with nutritional status of women in a rural area in Burkina Faso. Eur. J. Clin. Nutr. 2005, 59, 703–716. [Google Scholar] [CrossRef] [Green Version]
- Ghattas, H. Food Security and Nutrition in the Context of the Nutrition Transition; Technical Paper; FAO: Rome, Italy, 2014. Available online: https://www.fao.org/3/i3862e/i3862e.pdf (accessed on 13 September 2021).
- Miller, B.D.D.; Welch, R.M. Food system strategies for preventing micronutrient malnutrition. Food Policy 2013, 42, 115–128. [Google Scholar] [CrossRef] [Green Version]
- Cortés-Albornoz, M.C.; García-Guáqueta, D.P.; Velez-Van-Meerbeke, A.; Talero-Gutiérrez, C. Maternal Nutrition and Neurodevelopment: A Scoping Review. Nutrients 2021, 13, 3530. [Google Scholar] [CrossRef] [PubMed]
- Bath, S.C.; Walter, A.; Taylor, A.; Wright, J.; Rayman, M.P. Iodine deficiency in pregnant women living in the South East of the UK: The influence of diet and nutritional supplements on iodine status. Br. J. Nutr. 2014, 111, 1622–1631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bender, D.A. Nutritional Biochemistry of the Vitamins, 2nd ed.; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2003. [Google Scholar]
- Johnson, L.J.; Meacham, S.L.; Kruskall, L.J. The Antioxidants-Vitamin C, Vitamin E, Selenium, and Carotenoids. J. Agromed. 2003, 9, 65–82. [Google Scholar] [CrossRef] [PubMed]
- Huskisson, E.; Maggini, S.; Ruf, M. The Role of Vitamins and Minerals in Energy Metabolism and Well-Being. J. Int. Med. Res. 2007, 35, 277–289. [Google Scholar] [CrossRef]
- Deutsche Gesellschaft für Ernährung. Reference Values—Referenzwerte-Tool. Ger. Nutr. Soc. 2021. Available online: https://www.dge.de/wissenschaft/referenzwerte/?L= (accessed on 15 September 2021).
- O’Dell, B.L.; Sunde, R.A. (Eds.) Handbook of Nutritionally Essential Mineral Elements; CRC Press: Boca Raton, FL, USA, 1997. [Google Scholar] [CrossRef]
- WHO Bank Group. Lower Middle Income Countries. 2019. Available online: https://data.worldbank.org/income-level/lower-middle-income (accessed on 6 November 2019).
- Popkin, B.M.; Corvalan, C.; Grummer-Strawn, L.M. Dynamics of the double burden of malnutrition and the changing nutrition reality. Lancet 2020, 395, 65–74. [Google Scholar] [CrossRef]
- Capacci, S.; Mazzocchi, M.; Shankar, B.; Traill, B. The Triple Burden of Malnutrition in Europe and Central Asia: A Multivariate Analysis, FAO Regional Office for Europe and Central Asia, Policy Studies on Rural Transition No. 2013-7. 2013. Available online: https://www.fao.org/3/CA1810EN/ca1810en.pdf (accessed on 15 September 2021).
- United Nations and University of Central Asia (Institute of Public Policy and Administration), Bishkek, Kyrgyzstan. Food Security and Nutrition in Kyrgyzstan: Problems and Possible Solutions: Policy Brief. 2019. Available online: https://kyrgyzstan.un.org/sites/default/files/2019-09/DD_Food%20Security%20and%20Nutrition_Policy%20Brief_ENG.pdf (accessed on 20 September 2021).
- Otunchieva, A.; Borbodoev, J.; Ploeger, A. The Transformation of Food Culture on the Case of Kyrgyz Nomads—A Historical Overview. Sustainability 2021, 13, 8371. [Google Scholar] [CrossRef]
- Kamali, M.; Wright, J.E.; Akseer, N.; Tasic, H.; Conway, K.; Brar, S.; Imanalieva, C.; Maritz, G.; Rizvi, A.; Stanbekov, B.; et al. Trends and determinants of newborn mortality in Kyrgyzstan: A Countdown country case study. Lancet Glob. Health 2021, 9, e352–e360. [Google Scholar] [CrossRef]
- Toichuev, R.M.; Zhilova, L.V.; Paizildaev, T.R.; Khametova, M.S.; Rakhmatillaev, A.; Sakibaev, K.S.; Madykova, Z.A.; Toichueva, A.U.; Schlumpf, M.; Weber, R.; et al. Organochlorine pesticides in placenta in Kyrgyzstan and the effect on pregnancy, childbirth, and newborn health. Environ. Sci. Pollut. Res. 2017, 25, 31885–31894. [Google Scholar] [CrossRef] [PubMed]
- WHO. Prevalence of Anaemia in Pregnant Women Estimates by Country. 2017. Available online: http://apps.who.int/gho/data/node.main.ANEMIA1?lang=en (accessed on 6 November 2019).
- WHO. Prevalence of Anaemia in Women of Reproductive Age Estimates by Country. 2017. Available online: https://apps.who.int/gho/data/node.main.ANEMIA3?lang=en (accessed on 6 November 2019).
- WHO. Body Mass Index (BMI). 2017. Available online: https://apps.who.int/gho/data/node.main.BMIANTHROPOMETRY?lang=en (accessed on 6 November 2017).
- Kyrgyz Republic Demographic and Health Survey 2012; National Statistical Committee of the Kyrgyz Republic (NSC); Ministry of Health: Bishkek, Kyrgyz Republic; ICF International: Calverton, MD, USA, 2013.
- Ruel, M. Food Security and Nutrition: Linkages and Complementarities. In The Road to Good Nutrition; Eggersdorfer, M., Kraemer, K., Ruel, M., van Ameringen, M., Biesalski, H.K., Bloem, M., Chen, J., Lateef, A., Mannar, V., Eds.; KARGER: Basel, Switzerland, 2013; pp. 24–38. [Google Scholar] [CrossRef]
- Minja, E.G.; Swai, J.K.; Mponzi, W.; Ngowo, H.; Okumu, F.; Gerber, M.; Pühse, U.; Long, K.Z.; Utzinger, J.; Lang, C.; et al. Dietary diversity among households living in Kilombero district, in Morogoro region, South-Eastern Tanzania. J. Agric. Food Res. 2021, 5, 100171. [Google Scholar] [CrossRef]
- Torheim, L.E.; Ouattara, F.; Diarra, M.M.; Thiam, F.D.; Barikmo, I.; Hatløy, A.; Oshaug, A. Nutrient adequacy and dietary diversity in rural Mali: Association and determinants. Eur. J. Clin. Nutr. 2004, 58, 594–604. [Google Scholar] [CrossRef] [Green Version]
- Olabisi, M.; Obekpa, H.O.; Liverpool-Tasie, L.S.O. Is growing your own food necessary for dietary diversity? Evidence from Nigeria. Food Policy 2021, 104, 102144. [Google Scholar] [CrossRef]
- Matita, M.; Chirwa, E.W.; Johnston, D.; Mazalale, J.; Smith, R.; Walls, H. Does household participation in food markets increase dietary diversity? Evidence from rural Malawi. Glob. Food Secur. 2021, 28, 100486. [Google Scholar] [CrossRef]
- Mulenga, B.P.; Ngoma, H.; Nkonde, C. Produce to eat or sell: Panel data structural equation modeling of market participation and food dietary diversity in Zambia. Food Policy 2021, 102, 102035. [Google Scholar] [CrossRef]
- Ochieng, J.; Afari-Sefa, V.; Lukumay, P.J.; Dubois, T. Determinants of dietary diversity and the potential role of men in improving household nutrition in Tanzania. PLoS ONE 2017, 12, e0189022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonis-Profumo, G.; Stacey, N.; Brimblecombe, J. Measuring women’s empowerment in agriculture, food production, and child and maternal dietary diversity in Timor-Leste. Food Policy 2021, 102, 102102. [Google Scholar] [CrossRef]
- Weerasekara, P.C.; Withanachchi, C.R.; Ginigaddara, G.A.S.; Ploeger, A. Understanding Dietary Diversity, Dietary Practices and Changes in Food Patterns in Marginalised Societies in Sri Lanka. Foods 2020, 9, 1659. [Google Scholar] [CrossRef]
- Gupta, S.; Sunder, N.; Pingali, P.L. Market Access, Production Diversity, and Diet Diversity: Evidence from India. Food Nutr. Bull. 2020, 41, 167–185. [Google Scholar] [CrossRef] [PubMed]
- Vijay, J.; Patel, K.K. Recommendations to scale up dietary diversity data at household and individual level in India. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102310. [Google Scholar] [CrossRef] [PubMed]
- Wigle, J.M.; Akseer, N.; Mogilevskii, R.; Brar, S.; Conway, K.; Enikeeva, Z.; Iamshchikova, M.; Islam, M.; Kirbasheva, D.; Rappaport, A.I.; et al. Drivers of stunting reduction in the Kyrgyz Republic: A country case study. Am. J. Clin. Nutr. 2020, 112, 830S–843S. [Google Scholar] [CrossRef] [PubMed]
- Bhutta, Z.A.; Akseer, N.; Keats, E.C.; Vaivada, T.; Baker, S.; Horton, S.E.; Katz, J.; Menon, P.; Piwoz, E.; Shekar, M.; et al. How countries can reduce child stunting at scale: Lessons from exemplar countries. Am. J. Clin. Nutr. 2020, 112, 894S–904S. [Google Scholar] [CrossRef]
- Katanoda, K.; Kim, H.-S.; Matsumura, Y. New Quantitative Index for Dietary Diversity (QUANTIDD) and its annual changes in the Japanese. Nutrients 2006, 22, 283–287. [Google Scholar] [CrossRef]
- Kennedy, G.; Ballard, T.; Dop, M.C.; European Union. Guidelines for Measuring Household and Individual Dietary Diversity; Food and Agriculture Organization of the United Nations: Rome, Italy, 2011.
- Minimum Dietary Diversity for Women; FAO: Rome, Italy, 2021.
- Rathnayake, K.M.; Madushani, P.; Silva, K.R. Use of dietary diversity score as a proxy indicator of nutrient adequacy of rural elderly people in Sri Lanka. BMC Res. Notes 2012, 5, 469. [Google Scholar] [CrossRef] [Green Version]
- Martin-Prével, Y. Moving Forwad on Choosing a Standard Opeational Indicator of Women’s Dietary Diversity; Food and Agriculture Organization of the United Nations: Rome, Italy, 2015; ISBN 978-92-5-108883-8.
- Zhao, W.; Yu, K.; Tan, S.; Zheng, Y.; Zhao, A.; Wang, P.; Zhang, Y. Dietary diversity scores: An indicator of micronutrient inadequacy instead of obesity for Chinese children. BMC Public Health 2017, 17, 440. [Google Scholar] [CrossRef] [Green Version]
- Betz, F.; Lauermann, M.; Cyffka, B. Open Source Riverscapes: Analyzing the Corridor of the Naryn River in Kyrgyzstan Based on Open Access Data. Remote Sens. 2020, 12, 2533. [Google Scholar] [CrossRef]
- Map of Kyrgyzstan. 2021. Available online: https://d-maps.com/carte.php?num_car=53871&lang=en (accessed on 20 October 2021).
- Muñoz, R.; Okuniev, D. Typeform; Barcelona, Spain, 2012; Available online: https://www.typeform.com (accessed on 10 March 2020).
- Erhardt, J.; Gross, R. NutriSurvey; EBISpro: Willstätt, Germany, 2007; Available online: http://www.nutrisurvey.de (accessed on 10 November 2019).
- Ibragimova, S.S. Kyrgyz Modern Cuisine; KSE: Frunze, Kyrgyzstan, 1991. [Google Scholar]
- INDDEX Project. Data4Diets: Building Blocks for Diet-Related Food Security Analysis; Tufts University: Boston, MA, USA, 2018. Available online: https://inddex.nutrition.tufts.edu/data4diets (accessed on 24 October 2021).
- R Core Team, Version 4.1.2; Vienna, Austria, 2020. Available online: https://www.R-project.org/ (accessed on 20 June 2021).
- R Studio Team, Version 1.4.1103; Boston, MA, USA, 2020. Available online: http://www.rstudio.com/ (accessed on 20 June 2021).
- Dick, J.M. Chemical composition and the potential for proteomic transformation in cancer, hypoxia, and hyperosmotic stress. PeerJ 2017, 5, e3421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jafari, M.; Ansari-Pour, N. Why, When and How to Adjust Your P Values? Cell J. 2019, 20, 604–607. [Google Scholar] [CrossRef] [PubMed]
- Ngo, J.; Serra-Majem, L. Hunger and Malnutrition. In Encyclopedia of Food Security and Sustainability; Ferranti, P., Berry, E.M., Anderson, J.R., Eds.; Elsevier: Amsterdam, The Netherlands, 2019; pp. 315–335. [Google Scholar] [CrossRef]
- Bamji, M.S.; Murty, P.V.V.S.; Sudhir, P.D. Nutritionally sensitive agriculture—An approach to reducing hidden hunger. Eur. J. Clin. Nutr. 2020, 75, 1001–1009. [Google Scholar] [CrossRef] [PubMed]
- Christian, P.; Smith, E.R.; Zaidi, A. Addressing inequities in the global burden of maternal undernutrition: The role of targeting. BMJ Glob. Health 2020, 5, e002186. [Google Scholar] [CrossRef] [Green Version]
- Yeneabat, T.; Adugna, H.; Asmamaw, T.; Wubetu, M.; Admas, M.; Hailu, G.; Bedaso, A.; Amare, T. Maternal dietary diversity and micronutrient adequacy during pregnancy and related factors in East Gojjam Zone, Northwest Ethiopia, 2016. BMC Pregnancy Childbirth 2019, 19, 173. [Google Scholar] [CrossRef]
- Hasanah, A.; Mendolia, S.; Yerokhin, O. Labour Migration, Food Expenditure, and Household Food Security in Eastern Indonesia. Econ. Rec. 2017, 93, 122–143. [Google Scholar] [CrossRef]
- Moniruzzaman, M. The Impact of remittances on household food security: Evidence from a survey in Bangladesh. Migr. Dev. 2020, 1–20. [Google Scholar] [CrossRef]
- Harris-Fry, H.; Paudel, P.; Harrisson, T.; Shrestha, N.; Jha, S.; Beard, B.J.; Copas, A.; Shrestha, B.P.; Manandhar, D.S.; Costello, A.M.D.L.; et al. Participatory Women’s Groups with Cash Transfers Can Increase Dietary Diversity and Micronutrient Adequacy during Pregnancy, whereas Women’s Groups with Food Transfers Can Increase Equity in Intrahousehold Energy Allocation. J. Nutr. 2018, 148, 1472–1483. [Google Scholar] [CrossRef] [PubMed]
- Blakstad, M.M.; Mosha, D.; Bellows, A.L.; Canavan, C.R.; Chen, J.T.; Mlalama, K.; Noor, R.A.; Kinabo, J.; Masanja, H.; Fawzi, W.W. Home gardening improves dietary diversity, a cluster-randomized controlled trial among Tanzanian women. Matern. Child Nutr. 2020, 17, e13096. [Google Scholar] [CrossRef]
- Mitchell, S.; Shaw, D. The worldwide epidemic of female obesity. Best Pr. Res. Clin. Obstet. Gynaecol. 2015, 29, 289–299. [Google Scholar] [CrossRef]
- Stender, S. Trans fat in foods in Iran, South-Eastern Europe, Caucasia and Central Asia: A market basket investigation. Food Policy 2020, 96, 101877. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Region | North | South | ||
|---|---|---|---|---|
| Location | Bishkek | At Bashi | Osh | Aravan |
| Urban/rural | Urban | Rural | Urban | Rural |
| N of respondents | 99 | 90 | 98 | 136 |
| Geographical coordinates | 42.87′ N 74.59′ E | 41.16′ N 75.80′ E | 40.52′ N 72.79′ E | 40.51′ N 72.49′ E |
| Characteristic | Rural n (%) | Urban n (%) | Total Value n (%) |
|---|---|---|---|
| Age (years): | |||
| 18–27 | 50 (22.1%) | 77 (39%) | 127 (30.0%) |
| 28–39 | 96 (42.5%) | 66 (33.5%) | 162 (38.3%) |
| 40–49 | 80 (35.4%) | 54 (27.4%) | 134 (31.7%) |
| Ethnicity: | |||
| Kyrgyz | 105 (46.5%) | 182 (92.3%) | 287 (67.7%) |
| Non-Kyrgyz | 121 (53.5%) | 15 (7.6%) | 136 (32.3%) |
| Education: | |||
| Primary Education | 35 (15.5%) | 8 (4%) | 43 (10.2%) |
| Secondary Education | 104 (46%) | 66 (33.5%) | 170 (40.2%) |
| Vocational School | 25 (11%) | 16 (8.1%) | 41 (9.7%) |
| Higher Education | 60 (26.5%) | 107 (54.3%) | 167 (39.5%) |
| Marital status: | |||
| Single | 29 (12.8%) | 66 (33.5%) | 95 (22.5%) |
| Married | 189 (83.6%) | 120 (60.9%) | 309 (73.0%) |
| Divorced | 8 (3.5%) | 11 (5.6%) | 19 (4.5%) |
| Household Income (KG soms) *: | |||
| 0–5000 | 32 (14.2%) | 21 (10.6%) | 53 (12.5%) |
| 5000–10,000 | 82 (36.3%) | 42 (21.3%) | 124 (29.3%) |
| 10,001–20,000 | 67 (29.6%) | 66 (33.5%) | 133 (31.4%) |
| 20,001–30,000 | 29 (12.8%) | 55 (27.9%) | 84 (19.9%) |
| 30,001–40,000 | 10 (4.4%) | 10 (5%) | 20 (4.7%) |
| 40,000 and More | 6 (2.7%) | 3 (1.5%) | 9 (2.1%) |
| Family Size: | |||
| 4 or Less | 55 (24.3%) | 116 (58.9%) | 171 (40.4%) |
| More than 4 | 171 (75.7%) | 81 (41.1%) | 252 (59.6%) |
| Receive remittances: | |||
| Yes | 67 (29.6%) | 26 (13.2%) | 93 (22.0%) |
| No | 159 (70.4%) | 171 (86.8%) | 330 (78.0%) |
| BMI level (kg/m2): | |||
| Underweight | 13 (5.7%) | 19 (9.6%) | 32 (7.6%) |
| Normal Weight | 118 (52.2%) | 118 (59.9%) | 236 (55.8%) |
| Overweight | 59 (26.1%) | 44 (22.3%) | 103 (24.3%) |
| Obese | 36 (15.9%) | 16 (8.1%) | 52 (12.3%) |
| Mean (±SD) | 24.82 (±4.47) | 23.52 (±4.82) | 24.21 (±4.68) |
| Children: | |||
| Yes | 175 (77.4%) | 98 (49.7%) | 273 (64.5%) |
| No | 51 (22.6%) | 99 (50.3%) | 150 (35.5%) |
| Source of income: | |||
| Employment | 97 (42.9%) | 155 (78.7%) | 252 (59.6%) |
| Agriculture | 65 (29%) | 6 (3%) | 71 (16.8%) |
| Remittances | 41 (18.1%) | 22 (11.2%) | 63 (14.9%) |
| Private Business | 17 (7.5%) | 10 (5%) | 27 (6.4%) |
| Government Support | 6 (2.6%) | 4 (2%) | 10 (2.4%) |
| Food Groups | Reported and Locally Consumed Foods |
|---|---|
| Grains, white roots and tubers, and plantains | Wheat, rice, buckwheat, pearl barley, wheat bread, pasta products, potato, oatmeal, radish |
| Meat, poultry and fish | Beef, mutton, goat, chicken, sausage products (sosiska, kolbasa), smoked sausage, horse sausage (chuchuk), liver, stomach, intestine, canned fish |
| Other Vitamin A-rich fruits and vegetables | Carrot, sweet red pepper, pumpkin, apricot, dried apricot, peach, persimmon, melon |
| Milk and milk products | Cow milk, ayran, kefir, dried suzmo (kurut), concentrated ayran (suzmo), cream (kajmak, smetana), ghee (sary maj), fermented mare’s milk (kymyz), quark (tvorog), cheese |
| Nuts and seeds | Walnuts, peanuts, pistachios, sunflower seeds |
| Pulses (Beans, peas and lentils) | Red beans, chickpeas, mung beans, lentils |
| Eggs | Chicken eggs |
| Dark green leafy vegetables | Dill, coriander, parsley, green garlic, green onion, grape leaves, rhubarb, chives |
| Other fruits | Apple, banana, dried fruits, oranges, cherries, quince, pomegranate, prune, raspberries, sandthorn, currant berries |
| Other vegetables | Cabbage, garlic, cucumber, tomato, onion, eggplant, beetroot |
| Nutrient | Rural (n = 226) | Urban (n = 197) | Total Group | RDI | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | NAR Russia | NAR DGE | Mean ± SD | NAR Russia | NAR DGE | Mean ± SD | NAR Russia | NAR DGE | Russia | DGE | |
| Energy (kcal) | 1731.42 ± 569.4 | 0.81 | 0.79 | 1551.58 ± 611.26 | 0.72 | 0.71 | 1647.66 ± 595.36 | 0.77 | 0.75 | 2150 | 2200 |
| Protein (g) | 58.14 ± 21.51 | 0.89 | 1.12 | 61.51 ± 30.00 | 0.95 | 1.25 | 59.71 ± 25.84 | 0.92 | 1.18 | 65 | 50.70 |
| Fat (g) | 61.98 ± 31.98 | 0.86 | 0.85 | 59.68 ± 30.89 | 0.83 | 0.81 | 60.91 ± 31.46 | 0.85 | 0.83 | 72 | 73.3 |
| Carbohydrates (g) | 231.57 ± 89.99 | 0.74 | 0.84 | 188.67 ± 86.41 | 0.61 | 0.69 | 211.59 ± 90.80 | 0.68 | 0.77 | 311 | 275 |
| Fiber (g) | 17.99 ± 7.04 | 0.90 | 0.60 | 14.90 ± 6.91 | 0.74 | 0.50 | 16.55 ± 7.14 | 0.83 | 0.55 | 20 | 30 |
| Vitamin A (µg) | 910.09 ± 997.47 | 1.01 | 1.30 | 820.24 ± 665.65 | 0.91 | 1.17 | 868.24 ± 859.24 | 0.96 | 1.24 | 900 | 700 |
| Vitamin E. (mg) | 11.20 ± 8.02 | 0.75 | 0.93 | 12.34 ± 8.94 | 0.82 | 1.03 | 11.73 ± 8.47 | 0.78 | 0.98 | 15 | 12 |
| Vitamin B1 (mg) | 0.62 ± 0.28 | 0.41 | 0.62 | 0.59 ± 0.35 | 0.39 | 0.59 | 0.60 ± 0.31 | 0.40 | 0.60 | 1.5 | 1 |
| Vitamin B2 (mg) | 0.78 ± 0.33 | 0.43 | 0.71 | 0.77 ± 0.33 | 0.43 | 0.70 | 0.77 ± 0.33 | 0.43 | 0.70 | 1.8 | 1.1 |
| Vitamin B6 (mg) | 0.92 ± 0.36 | 0.46 | 0.66 | 0.93 ± 0.43 | 0.46 | 0.66 | 0.92 ± 0.39 | 0.46 | 0.66 | 2 | 1.4 |
| Fol. acid (µg) | 165.2 ± 74.17 | 0.41 | 0.55 | 145.75 ± 79.53 | 0.36 | 0.49 | 156.14 ± 77.24 | 0.39 | 0.52 | 400 | 300 |
| Vitamin C (mg) | 42.01 ± 36.84 | 0.47 | 0.44 | 44.52 ± 45.98 | 0.49 | 0.47 | 43.18 ± 41.31 | 0.48 | 0.45 | 90 | 95 |
| Calcium (mg) | 323.16 ± 161.04 | 0.32 | 0.32 | 286.13 ± 132.01 | 0.29 | 0.29 | 305.92 ± 149.21 | 0.31 | 0.31 | 1000 | 1000 |
| Magnesium (mg) | 198.82 ± 72.59 | 0.50 | 0.65 | 185.24 ± 82.05 | 0.46 | 0.61 | 192.50 ± 77.35 | 0.48 | 0.63 | 400 | 305 |
| Iron (mg) | 10.08 ± 3.61 | 0.56 | 0.67 | 9.93 ± 4.42 | 0.55 | 0.66 | 10.01 ± 4.00 | 0.56 | 0.67 | 18 | 15 |
| Zinc (mg) | 9.25 ± 3.75 | 0.77 | 1.16 | 10.19 ± 5.34 | 0.85 | 1.27 | 9.69 ± 4.58 | 0.81 | 1.21 | 12 | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Otunchieva, A.; Smanalieva, J.; Ploeger, A. Dietary Quality of Women of Reproductive Age in Low-Income Settings: A Cross-Sectional Study in Kyrgyzstan. Nutrients 2022, 14, 289. https://doi.org/10.3390/nu14020289
Otunchieva A, Smanalieva J, Ploeger A. Dietary Quality of Women of Reproductive Age in Low-Income Settings: A Cross-Sectional Study in Kyrgyzstan. Nutrients. 2022; 14(2):289. https://doi.org/10.3390/nu14020289
Chicago/Turabian StyleOtunchieva, Aiperi, Jamila Smanalieva, and Angelika Ploeger. 2022. "Dietary Quality of Women of Reproductive Age in Low-Income Settings: A Cross-Sectional Study in Kyrgyzstan" Nutrients 14, no. 2: 289. https://doi.org/10.3390/nu14020289
APA StyleOtunchieva, A., Smanalieva, J., & Ploeger, A. (2022). Dietary Quality of Women of Reproductive Age in Low-Income Settings: A Cross-Sectional Study in Kyrgyzstan. Nutrients, 14(2), 289. https://doi.org/10.3390/nu14020289