
Sex-Specific Associations between Serum Ferritin and Osteosarcopenic Obesity in Adults Aged over 50 Years

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
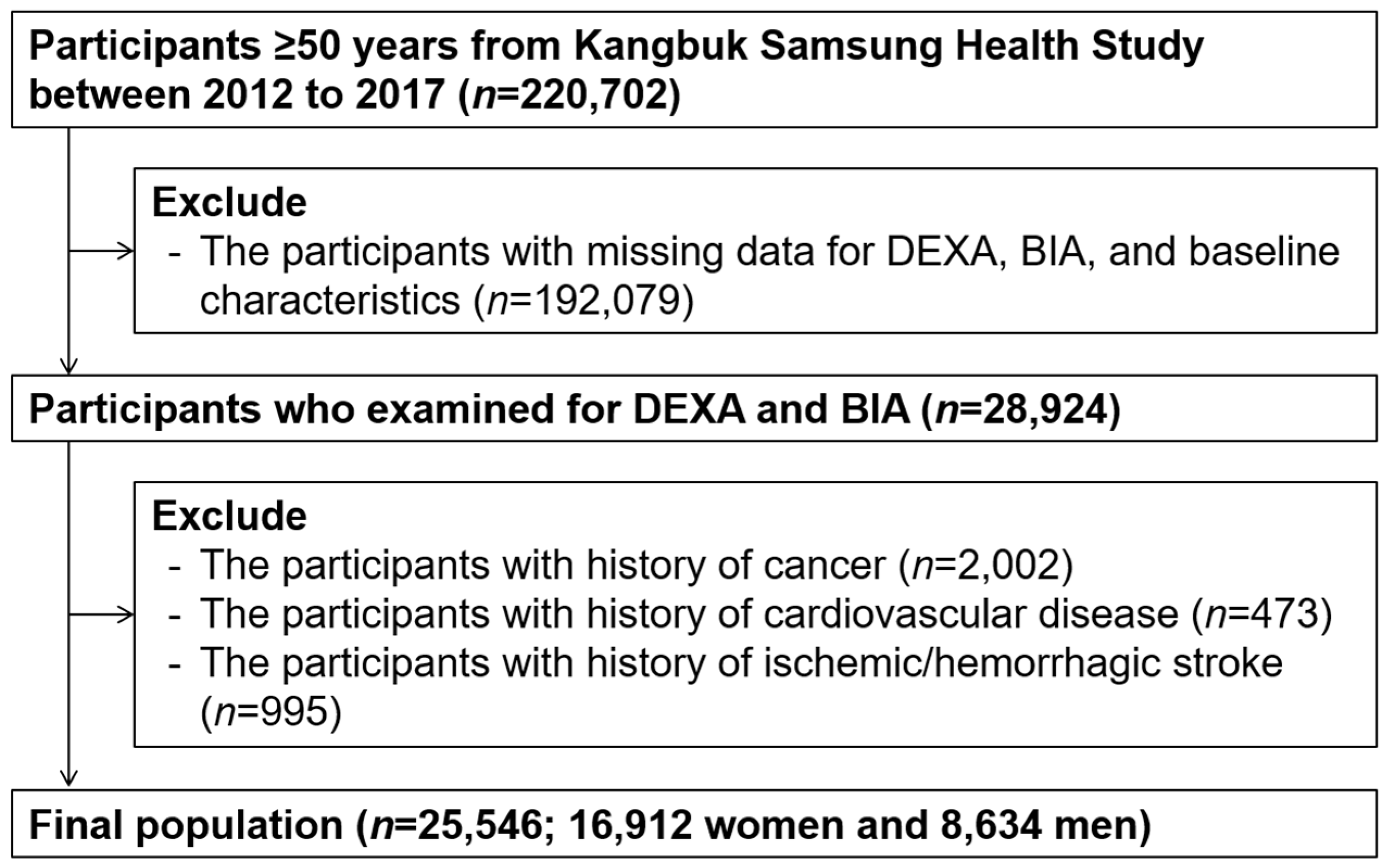
2.1. Study Participants
2.2. Measurements
2.3. Determination of Adverse Body Composition and Osteosarcopenic Obesity
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Population
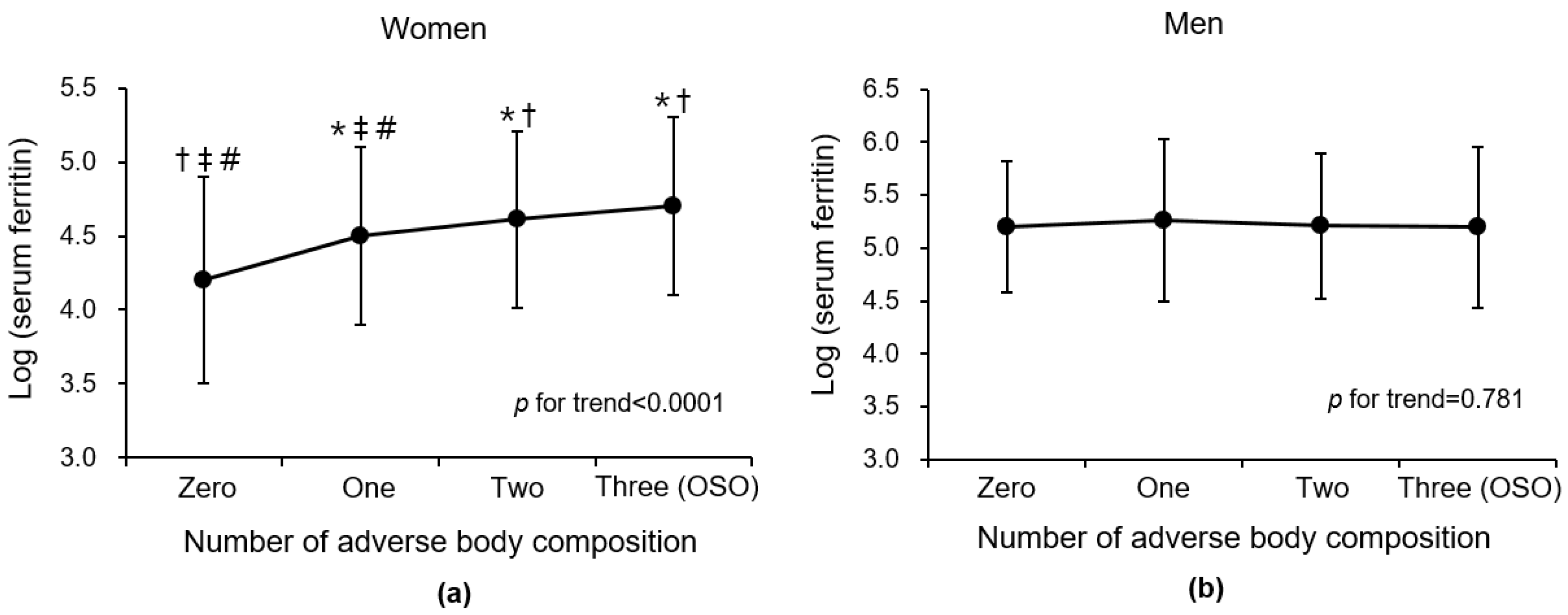
3.2. Relationship of Serum Ferritin with Adverse Body Composition Including Osteosarcopenic Obesity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kelly, O.J.; Gilman, J.C.; Boschiero, D.; Ilich, J.Z. Osteosarcopenic obesity: Current knowledge, revised identification criteria and treatment principles. Nutrients 2019, 11, 747. [Google Scholar] [CrossRef] [PubMed]
- Ormsbee, M.J.; Prado, C.M.; Ilich, J.Z.; Purcell, S.; Siervo, M.; Folsom, A.; Panton, L. Osteosarcopenic obesity: The role of bone, muscle, and fat on health. J. Cachexia Sarcopenia Muscle 2014, 5, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Ilich, J.Z.; Inglis, J.E.; Kelly, O.J.; McGee, D.L. Osteosarcopenic obesity is associated with reduced handgrip strength, walking abilities, and balance in postmenopausal women. Osteoporos Int. 2015, 26, 2587–2595. [Google Scholar] [CrossRef]
- Chen, X.; Kong, C.; Yu, H.; Gong, J.; Lan, L.; Zhou, L.; Gong, J.; Liu, P.; Xu, L.; Deng, Q. Association between osteosarcopenic obesity and hypertension among four minority populations in China: A cross-sectional study. BMJ Open 2019, 9, e026818. [Google Scholar] [CrossRef]
- Kim, J.; Lee, Y.; Kye, S.; Chung, Y.S.; Lee, O. Association of serum vitamin D with osteosarcopenic obesity: Korea National Health and Nutrition Examination Survey 2008–2010. J. Cachexia Sarcopenia Muscle 2017, 8, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Zhang, W.; Han, P.; Kohzuki, M.; Guo, Q. Osteosarcopenic obesity associated with poor physical performance in the elderly Chinese community. Clin. Interv. Aging 2020, 15, 1343–1352. [Google Scholar] [CrossRef] [PubMed]
- Mo, D.; Hsieh, P.; Yu, H.; Zhou, L.; Gong, J.; Xu, L.; Liu, P.; Chen, G.; Chen, Z.; Deng, Q. Osteosarcopenic obesity and its relationship with dyslipidemia in women from different ethnic groups of China. Arch. Osteoporos 2018, 13, 65. [Google Scholar] [CrossRef]
- Chen, M.L. The Growing Costs and Burden of Family Caregiving of Older Adults: A Review of Paid Sick Leave and Family Leave Policies. Gerontologist 2016, 56, 391–396. [Google Scholar] [CrossRef]
- Specchia, M.L.; Veneziano, M.A.; Cadeddu, C.; Ferriero, A.M.; Mancuso, A.; Ianuale, C.; Parente, P.; Capri, S.; Ricciardi, W. Economic impact of adult obesity on health systems: A systematic review. Eur. J. Public Health 2015, 25, 255–262. [Google Scholar] [CrossRef]
- Puntarulo, S. Iron, oxidative stress and human health. Mol. Asp. Med. 2005, 26, 299–312. [Google Scholar] [CrossRef]
- Reddy, M.B.; Clark, L. Iron, oxidative stress, and disease risk. Nutr. Rev. 2004, 62, 120–124. [Google Scholar] [CrossRef] [PubMed]
- Arosio, P.; Levi, S. Ferritin, iron homeostasis, and oxidative damage. Free Radic. Biol. Med. 2002, 33, 457–463. [Google Scholar] [CrossRef]
- Saito, H. Metabolism of Iron Stores. Nagoya J. Med. Sci. 2014, 76, 235–254. [Google Scholar] [PubMed]
- Branco, R.G.; Garcia, P.C. Ferritin and c-reactive protein as markers of systemic inflammation in sepsis. Pediatr. Crit. Care Med. 2017, 18, 194–196. [Google Scholar] [CrossRef]
- Mainous, A.G., III; Wells, B.J.; Everett, C.J.; Gill, J.M.; King, D.E. Association of ferritin and lipids with C-reactive protein. Am. J. Cardiol. 2004, 93, 559–562. [Google Scholar] [CrossRef]
- Khan, A.; Khan, W.M.; Ayub, M.; Humayun, M.; Haroon, M. Ferritin is a marker of inflammation rather than iron deficiency in overweight and obese people. J. Obes. 2016, 2016, 1937320. [Google Scholar] [CrossRef]
- Nakagawa, C.; Inaba, M.; Ishimura, E.; Yamakawa, T.; Shoji, S.; Okuno, S. Association of increased serum ferritin with impaired muscle strength/quality in hemodialysis patients. J. Ren. Nutr. 2016, 26, 253–257. [Google Scholar] [CrossRef]
- Zhao, G. Is iron accumulation a possible risk factor for sarcopenia? Biol. Trace Elem. Res. 2018, 186, 379–383. [Google Scholar] [CrossRef]
- Abril-Ulloa, V.; Flores-Mateo, G.; Sola-Alberich, R.; Manuel-y-Keenoy, B.; Arija, V. Ferritin levels and risk of metabolic syndrome: Meta-analysis of observational studies. BMC Public Health 2014, 14, 483. [Google Scholar] [CrossRef]
- Shim, Y.S.; Kang, M.J.; Oh, Y.J.; Baek, J.W.; Yang, S.; Hwang, I.T. Association of serum ferritin with insulin resistance, abdominal obesity, and metabolic syndrome in Korean adolescent and adults: The Korean National Health and Nutrition Examination Survey, 2008 to 2011. Medicine 2017, 96, e6179. [Google Scholar] [CrossRef]
- Kim, B.J.; Lee, S.H.; Koh, J.M.; Kim, G.S. The association between higher serum ferritin level and lower bone mineral density is prominent in women >/=45 years of age (KNHANES 2008-2010). Osteoporos Int. 2013, 24, 2627–2637. [Google Scholar] [CrossRef] [PubMed]
- Snozek, C.L.H.; Spears, G.M.; Porco, A.B.; Erb, S.; Kaleta, E.J.; Bryant, S.C.; Baumann, N.A. Updated ferritin reference intervals for the Roche Elecsys(R) immunoassay. Clin. Biochem. 2021, 87, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Casale, G.; Bonora, C.; Migliavacca, A.; Zurita, I.E.; de Nicola, P. Serum ferritin and ageing. Age Aging 1981, 10, 119–122. [Google Scholar] [CrossRef] [PubMed]
- Altamura, S.; Muckenthaler, M.U. Iron toxicity in diseases of aging: Alzheimer’s disease, Parkinson’s disease and atherosclerosis. J. Alzheimers Dis. 2009, 16, 879–895. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, E.D. Iron toxicity: New conditions continue to emerge. Oxid. Med. Cell Longev. 2009, 2, 107–109. [Google Scholar] [CrossRef] [PubMed]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sport. Exerc. 2007, 39, 1423–1434. [Google Scholar] [CrossRef]
- Buttarello, M.; Pajola, R.; Novello, E.; Mezzapelle, G.; Plebani, M. Evaluation of the hypochromic erythrocyte and reticulocyte hemoglobin content provided by the Sysmex XE-5000 analyzer in diagnosis of iron deficiency erythropoiesis. Clin. Chem. Lab. Med. CCLM 2016, 54, 1939–1945. [Google Scholar] [CrossRef]
- Laboratory Findings in Different Stages of Iron Deficiency. Available online: https://www.uptodate.com/contents/image?imageKey=HEME%2F76236&source=Graphic_Panel (accessed on 23 September 2022).
- Papamanoli, A.; Kalogeropoulos, A.P.; Hotelling, J.; Yoo, J.; Grewal, P.; Predun, W.; Jacob, R.P.; Cao, K.; Marcos, L.A.; Skopicki, H.A. Association of Serum Ferritin Levels and Methylprednisolone Treatment With Outcomes in Nonintubated Patients With Severe COVID-19 Pneumonia. JAMA Netw. Open 2021, 4, e2127172. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.S.; Lin, S.M.; Huang, T.C.; Chao, J.C.; Chen, Y.C.; Pan, W.H.; Bai, C.H. Serum ferritin and risk of the metabolic syndrome: A population-based study. Asia Pac. J. Clin. Nutr. 2013, 22, 400–407. [Google Scholar]
- Kim, T.H.; Hwang, H.J.; Kim, S.H. Relationship between serum ferritin levels and sarcopenia in Korean females aged 60 years and older using the fourth Korea National Health and Nutrition Examination Survey (KNHANES IV-2, 3), 2008–2009. PLoS ONE 2014, 9, e90105. [Google Scholar] [CrossRef]
- Yoo, K.D.; Ko, S.H.; Park, J.E.; Ahn, Y.B.; Yim, H.W.; Lee, W.C.; Park, Y.M. High serum ferritin levels are associated with metabolic risk factors in non-obese Korean young adults: Korean National Health and Nutrition Examination Survey (KNHANES) IV. Clin. Endocrinol. 2012, 77, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Kanis, J.A. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: Synopsis of a WHO report. WHO Study Group. Osteoporos Int. 1994, 4, 368–381. [Google Scholar] [CrossRef] [PubMed]
- Soen, S.; Fukunaga, M.; Sugimoto, T.; Sone, T.; Fujiwara, S.; Endo, N.; Gorai, I.; Shiraki, M.; Hagino, H.; Hosoi, T.; et al. Japan Osteoporosis Society Joint Review Committee for the Revision of the Diagnostic Criteria for Primary, O. Diagnostic criteria for primary osteoporosis: Year 2012 revision. J. Bone Miner. Metab. 2013, 31, 247–257. [Google Scholar] [CrossRef]
- Romero-Corral, A.; Somers, V.K.; Sierra-Johnson, J.; Thomas, R.J.; Collazo-Clavell, M.L.; Korinek, J.; Allison, T.G.; Batsis, J.A.; Sert-Kuniyoshi, F.H.; Lopez-Jimenez, F. Accuracy of body mass index in diagnosing obesity in the adult general population. Int. J. Obes. 2008, 32, 959–966. [Google Scholar] [CrossRef] [PubMed]
- Dickey, R.A.; Bartuska, D.; Bray, G.W.; Callaway, C.W.; Davidson, E.T.; Feld, S.; Ferraro, R.T.; Hodgson, S.F.; Jellinger, P.S.; Kennedy, F.P. AACE/ACE Position statement on the prevention, diagnosis, and treatment of obesity (1998 revision). Endocr. Pract. 1998, 4, 297–350. [Google Scholar]
- WHO Study Group. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO Study Group. World Health Organ. Tech. Rep. Ser. 1994, 843, 368–381. [Google Scholar]
- Kim, Y.S.; Lee, Y.; Chung, Y.S.; Lee, D.J.; Joo, N.S.; Hong, D.; Song, G.; Kim, H.J.; Choi, Y.J.; Kim, K.M. Prevalence of sarcopenia and sarcopenic obesity in the Korean population based on the Fourth Korean National Health and Nutritional Examination Surveys. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 1107–1113. [Google Scholar] [CrossRef]
- Janssen, I.; Heymsfield, S.B.; Ross, R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J. Am. Geriatr. Soc. 2002, 50, 889–896. [Google Scholar] [CrossRef]
- Batsis, J.A.; Mackenzie, T.A.; Lopez-Jimenez, F.; Bartels, S.J. Sarcopenia, sarcopenic obesity, and functional impairments in older adults: National Health and Nutrition Examination Surveys 1999–2004. Nutr. Res. 2015, 35, 1031–1039. [Google Scholar] [CrossRef] [PubMed]
- Ho-Pham, L.T.; Campbell, L.V.; Nguyen, T.V. More on body fat cutoff points. Mayo Clin. Proc. 2011, 86, 584, author reply 584–585. [Google Scholar] [CrossRef]
- Che, J.; Yang, J.; Zhao, B.; Zhang, G.; Wang, L.; Peng, S.; Shang, P. The effect of abnormal iron metabolism on osteoporosis. Biol. Trace Elem. Res. 2020, 195, 353–365. [Google Scholar] [CrossRef]
- Nikonorov, A.A.; Skalnaya, M.G.; Tinkov, A.A.; Skalny, A.V. Mutual interaction between iron homeostasis and obesity pathogenesis. J. Trace Elem. Med. Biol. 2015, 30, 207–214. [Google Scholar] [CrossRef]
- Balogh, E.; Tolnai, E.; Nagy, B., Jr.; Nagy, B.; Balla, G.; Balla, J.; Jeney, V. Iron overload inhibits osteogenic commitment and differentiation of mesenchymal stem cells via the induction of ferritin. Biochim. Biophys. Acta 2016, 1862, 1640–1649. [Google Scholar] [CrossRef]
- Tsay, J.; Yang, Z.; Ross, F.P.; Cunningham-Rundles, S.; Lin, H.; Coleman, R.; Mayer-Kuckuk, P.; Doty, S.B.; Grady, R.W.; Giardina, P.J.; et al. Bone loss caused by iron overload in a murine model: Importance of oxidative stress. Blood 2010, 116, 2582–2589. [Google Scholar] [CrossRef]
- Reardon, T.F.; Allen, D.G. Iron injections in mice increase skeletal muscle iron content, induce oxidative stress and reduce exercise performance. Exp. Physiol. 2009, 94, 720–730. [Google Scholar] [CrossRef]
- Tinkov, A.A.; Polyakova, V.S.; Nikonorov, A.A. Chronic administration of iron and copper potentiates adipogenic effect of high fat diet in Wistar rats. Biometals 2013, 26, 447–463. [Google Scholar] [CrossRef]
- Zhang, W.C.B.; Xing, Y.; Shao, B. Serum Ferritin and the Risk of Metabolic Syndrome: A Systematic Review and Dose-Response Meta-Analysis of Cross-sectional Studies. Biomed. Environ. Sci. 2021, 34, 623–631. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.K.; Kim, Y.; Kim, Y.I. Association of serum ferritin with metabolic syndrome and diabetes mellitus in the South Korean general population according to the Korean National Health and Nutrition Examination Survey 2008. Metabolism 2011, 60, 1416–1424. [Google Scholar] [CrossRef]
- Ostlund, R.E., Jr.; Yang, J.W.; Klein, S.; Gingerich, R. Relation between plasma leptin concentration and body fat, gender, diet, age, and metabolic covariates. J. Clin. Endocrinol. Metab. 1996, 81, 3909–3913. [Google Scholar]
- Couillard, C.; Mauriege, P.; Prud’homme, D.; Nadeau, A.; Tremblay, A.; Bouchard, C.; Despres, J.P. Plasma leptin concentrations: Gender differences and associations with metabolic risk factors for cardiovascular disease. Diabetologia 1997, 40, 1178–1184. [Google Scholar] [CrossRef]
- Blaak, E. Gender differences in fat metabolism. Curr. Opin. Clin. Nutr. Metab. Care 2001, 4, 499–502. [Google Scholar] [CrossRef]
- Lundsgaard, A.M.; Kiens, B. Gender differences in skeletal muscle substrate metabolism—Molecular mechanisms and insulin sensitivity. Front. Endocrinol. 2014, 5, 195. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Total | Women | Men | p-Value a |
|---|---|---|---|---|
| Number of subjects (n) | 25,546 | 16,912 | 8634 | |
| Age (years) | 58.74 (6.58) | 58.28 (6.44) | 59.64 (6.76) | <0.0001 |
| Height (cm) | 160.79 (7.91) | 156.63 (5.25) | 168.94 (5.54) | <0.0001 |
| Weight (kg) | 61.16 (10.15) | 56.98 (7.87) | 69.35 (9.07) | <0.0001 |
| BMI (kg/m2) | 23.58 (2.98) | 23.23 (3.04) | 24.27 (2.73) | <0.0001 |
| Fat mass (kg) | 18.24 (5.51) | 18.98 (5.52) | 16.78 (5.19) | <0.0001 |
| Percent body fat (%) | 29.75 (7.05) | 32.78 (5.87) | 23.83 (5.16) | <0.0001 |
| ASM (kg) | 17.60 (4.64) | 15.19 (1.97) | 22.33 (4.74) | <0.0001 |
| SMI b (kg/m2) | 6.72 (1.27) | 6.17 (0.58) | 7.80 (1.53) | <0.0001 |
| Current smoker (%) | 10.4 (n = 2296) | 1.7 (n = 236) | 25.9 (n = 2060) | <0.0001 |
| Heavy drinking c (%) | 16.5 (n = 3509) | 3.2 (n = 432) | 39.5 (n = 3077) | <0.0001 |
| Regular physical activity d (%) | 23.4 (n = 5968) | 21.8 (n = 3692) | 26.4 (n = 2276) | <0.0001 |
| Comorbidities | ||||
| Hypertension (%) | 24.8 (n = 6343) | 21.1 (n = 3561) | 32.2 (n = 2782) | <0.0001 |
| Diabetes (%) | 8.6 (n = 2207) | 6.4 (n = 1076) | 13.1 (n = 1131) | <0.0001 |
| Dyslipidemia (%) | 29.9 (n = 7631) | 29.7 (n = 5030) | 30.1 (n = 2601) | 0.527 |
| Laboratory findings | ||||
| Ferritin (ng/mL) | 150.86 (122.50) | 111.38 (76.55) | 228.19 (154.56) | <0.0001 |
| Low (40) (%) | 8.8 (n = 2214) | 12.0 (n = 2002) | 2.5 (n = 212) | |
| Normal (40–200) (%) | 68.4 (n = 17,273) | 78.2 (n = 13,059) | 49.2 (n = 4214) | <0.0001 |
| High (200) (%) | 22.9 (n = 5774) | 9.8 (n = 1633) | 48.3 (n = 4141) | |
| Iron (μg/dL) | 111.61 (37.48) | 104.25 (33.92) | 126.02 (39.85) | <0.0001 |
| Low () (%) | 6.3 (n = 844) | 8.0 (n = 701) | 3.2 (n = 143) | |
| Normal (60–150) (%) | 80.6 (n = 10,726) | 83.9 (n = 7385) | 74.1 (n = 3341) | 0.258 |
| High (150) (%) | 13.1 (n = 1739) | 8.1 (n = 713) | 22.7 (n = 1026) | |
| TIBC (μg/dL) | 306.18 (41.55) | 307.96 (42.08) | 302.72 (40.26) | <0.0001 |
| Total cholesterol (mg/dL) | 200.90 (37.88) | 205.18 (37.38) | 287.98 (36.63) | <0.0001 |
| LDL (mg/dL) | 132.01 (35.59) | 134.36 (35.72) | 127.39 (34.86) | <0.0001 |
| HDL (mg/dL) | 60.48 (16.44) | 63.84 (16.34) | 53.90 (14.53) | <0.0001 |
| Triglycerides (mg/dL) | 111.12 (66.95) | 103.98 (58.82) | 125.11 (78.67) | <0.0001 |
| Fasting glucose (mg/dL) | 99.24 (17.18) | 97.40 (15.59) | 102.85 (19.44) | <0.0001 |
| HbA1c (%) | 5.78 (0.64) | 5.75 (0.58) | 5.85 (0.73) | <0.0001 |
| Creatinine (mg/dL) | 0.78 (0.22) | 0.69 (0.15) | 0.95 (0.23) | <0.0001 |
| Albumin (g/dL) | 4.60 (0.25) | 4.58 (0.25) | 4.64 (0.25) | <0.0001 |
| AST (IU/L) | 25.20 (12.40) | 24.21 (10.75) | 27.15 (14.93) | <0.0001 |
| ALT (IU/L) | 23.73 (15.09) | 21.59 (13.42) | 27.94 (17.15) | <0.0001 |
| Number of Adverse Body Compositions | Tertiles (T) of Serum Ferritin (ng/mL) | p for Trend | ||
|---|---|---|---|---|
| Women (n = 16,912) | T1 (n = 5556) (<74.50) | T2 (n = 5568) (≥74.5, <125.0) | T3 (n = 5570) (≥125.0) | |
| 0 (%) | 39.3 (2182) | 29.7 (1652) | 25.8 (1437) | <0.0001 |
| 1 (%) | 42.0 (2336) | 45.5 (2531) | 48.2 (2684) | |
| 2 (%) | 17.0 (943) | 22.7 (1263) | 23.5 (1309) | |
| 3 (=OSO) (%) | 1.7 (95) | 2.2 (122) | 2.5 (140) | |
| Men (n = 8634) | T1 (n = 2862) | T2 (n = 2855) | T3 (n = 2850) | |
| (<153.5) | (≥153.5, <248.0) | (≥248.0) | ||
| 0 (%) | 35.5 (1015) | 36.8 (1050) | 30.7 (876) | 0.125 |
| 1 (%) | 42.5 (1216) | 42.1 (1202) | 48.5 (1382) | |
| 2 (%) | 18.6 (531) | 18.5 (528) | 17.5 (498) | |
| 3 (=OSO) (%) | 3.5 (100) | 2.6 (75) | 3.3 (94) | |
| Adverse Body Composition a | Crude | Adjusted OR b | ||
|---|---|---|---|---|
| OR (95% CI) | p for Trend | OR (95% CI) | p for Trend | |
| Women (n = 16,912) | ||||
| <0.0001 | <0.0001 | ||
| T1 (lowest) | 1 (ref.) | 1 (ref.) | ||
| T2 (middle) | 1.43 (1.31–1.55) | 1.20 (1.08–1.34) | ||
| T3 (highest) | 1.74 (1.60–1.90) | 1.33 (1.20–1.49) | ||
| <0.0001 | <0.0001 | ||
| T1 | 1 (ref.) | 1 (ref.) | ||
| T2 | 1.76 (1.59–1.96) | 1.36 (1.19–1.56) | ||
| T3 | 2.10 (1.89–2.34) | 1.43 (1.24–1.64) | ||
| <0.0001 | 0.014 | ||
| T1 | 1 (ref.) | 1 (ref.) | ||
| T2 | 1.69 (1.28–2.23) | 1.46 (1.03–2.06) | ||
| T3 | 2.23 (1.71–2.92) | 1.52 (1.07–2.14) | ||
| Men (n = 8634) | ||||
| 0.147 | 0.411 | ||
| T1 | 1 (ref.) | 1 (ref.) | ||
| T2 | 0.95 (0.85–1.07) | 0.96 (0.84–1.10) | ||
| T3 | 1.31 (1.16–1.48) | 1.23 (1.07–1.41) | ||
| 0.946 | 0.285 | ||
| T1 | 1 (ref.) | 1 (ref.) | ||
| T2 | 0.96 (0.82–1.11) | 1.04 (0.88–1.23) | ||
| T3 | 1.08 (0.93–1.26) | 1.17 (0.98–1.40) | ||
| 0.230 | 0.757 | ||
| T1 | 1 (ref.) | 1 (ref.) | ||
| T2 | 0.72 (0.53–0.99) | 0.91 (0.63–1.30) | ||
| T3 | 1.08 (0.81–1.46) | 1.33 (0.94–1.90) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, S.-J.; Lim, H.S.; Lee, M.-Y.; Lee, Y.-T.; Yoon, K.J.; Park, C.-H. Sex-Specific Associations between Serum Ferritin and Osteosarcopenic Obesity in Adults Aged over 50 Years. Nutrients 2022, 14, 4023. https://doi.org/10.3390/nu14194023
Chung S-J, Lim HS, Lee M-Y, Lee Y-T, Yoon KJ, Park C-H. Sex-Specific Associations between Serum Ferritin and Osteosarcopenic Obesity in Adults Aged over 50 Years. Nutrients. 2022; 14(19):4023. https://doi.org/10.3390/nu14194023
Chicago/Turabian StyleChung, Sung-Joon, Han Sol Lim, Mi-Yeon Lee, Yong-Taek Lee, Kyung Jae Yoon, and Chul-Hyun Park. 2022. "Sex-Specific Associations between Serum Ferritin and Osteosarcopenic Obesity in Adults Aged over 50 Years" Nutrients 14, no. 19: 4023. https://doi.org/10.3390/nu14194023
APA StyleChung, S.-J., Lim, H. S., Lee, M.-Y., Lee, Y.-T., Yoon, K. J., & Park, C.-H. (2022). Sex-Specific Associations between Serum Ferritin and Osteosarcopenic Obesity in Adults Aged over 50 Years. Nutrients, 14(19), 4023. https://doi.org/10.3390/nu14194023