
Linking the Low-Density Lipoprotein-Cholesterol (LDL) Level to Arsenic Acid, Dimethylarsinic, and Monomethylarsonic: Results from a National Population-Based Study from the NHANES, 2003–2020

Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Study Population
2.3. Urine Arsenic Assessment
2.4. Total Cholesterol (TC) and Low-Density Lipoprotein Cholesterol (LDL-C)
2.5. Other Variables
2.6. Statistical Analysis
3. Results
3.1. Participant Characteristics
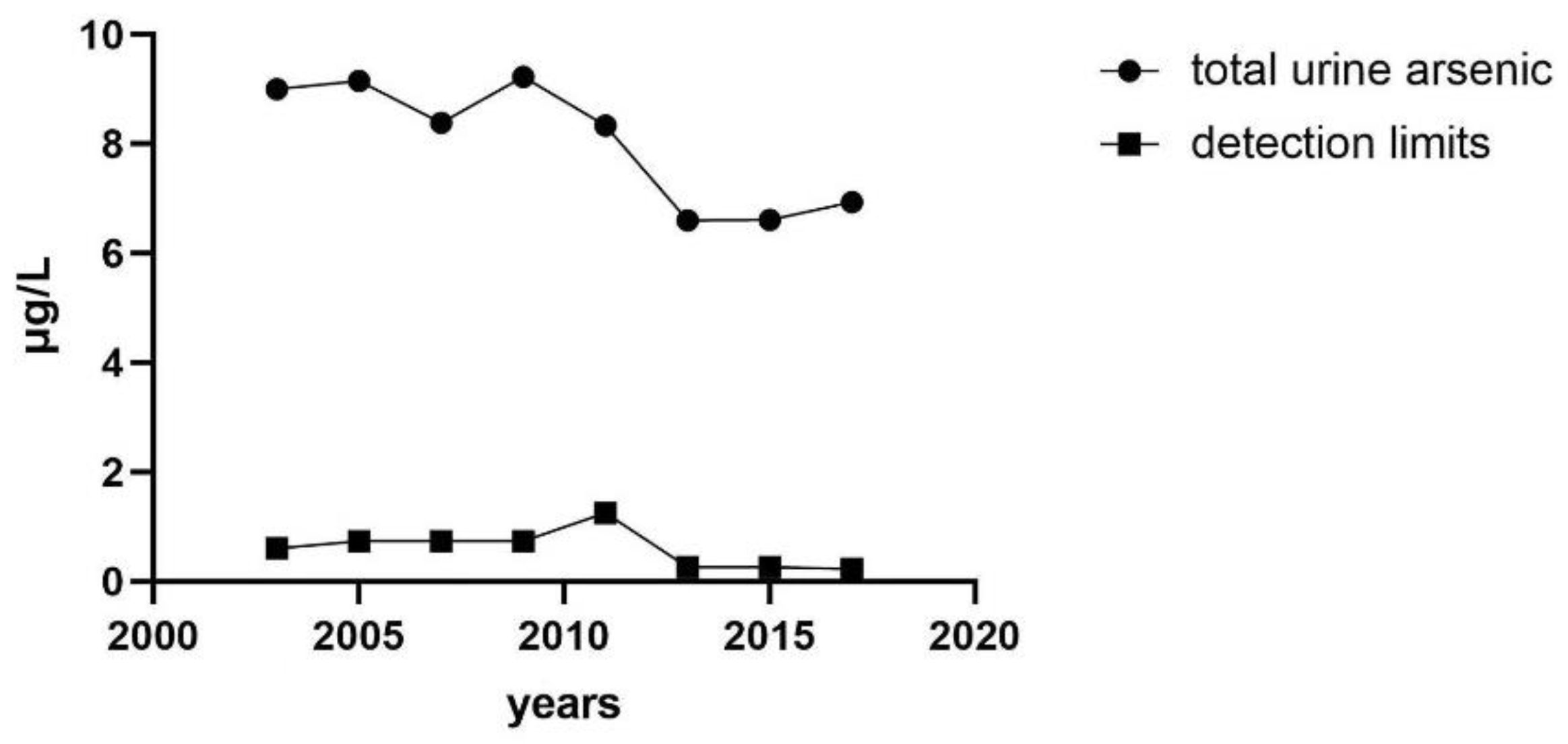
3.2. Median Concentration of Urinary Total Arsenic Varies with Years
3.3. Association of Urinary Total Arsenic with TC and LDL-C
3.4. Six Different Speciated Arsenics were Analyzed
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Liu, Y.; Zhong, X.; Shen, J.; Jiao, L.; Tong, J.; Zhao, W.; Du, K.; Gong, S.; Liu, M.; Wei, M. Elevated serum TC and LDL-C levels in Alzheimer’s disease and mild cognitive impairment: A meta-analysis study. Brain Res. 2020, 1727, 146554. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Liu, Q.; Guo, X.; Wang, W.; Yu, B.; Liang, B.; Zhou, Y.; Dong, H.; Lin, J. The role of remnant cholesterol beyond low-density lipoprotein cholesterol in diabetes mellitus. Cardiovasc. Diabetol. 2022, 21, 117. [Google Scholar] [CrossRef] [PubMed]
- Fang, F.; Zhan, Y.; Hammar, N.; Shen, X.; Wirdefeldt, K.; Walldius, G.; Mariosa, D. Lipids, Apolipoproteins, and the Risk of Parkinson Disease. Circ. Res. 2019, 125, 643–652. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Jiang, L.Y.; Yang, H.; Song, B.L. Intracellular Cholesterol Transport by Sterol Transfer Proteins at Membrane Contact Sites. Trends Biochem. Sci. 2019, 44, 273–292. [Google Scholar] [CrossRef]
- Wong, L.H.; Gatta, A.T.; Levine, T.P. Lipid transfer proteins: The lipid commute via shuttles, bridges and tubes. Nat. Rev. Mol. Cell Biol. 2019, 20, 85–101. [Google Scholar] [CrossRef]
- Luo, J.; Yang, H.; Song, B.L. Mechanisms and regulation of cholesterol homeostasis. Nat. Rev. Mol. Cell Biol. 2020, 21, 225–245. [Google Scholar] [CrossRef]
- Bruckert, E.; Rosenbaum, D. Lowering LDL-cholesterol through diet: Potential role in the statin era. Curr. Opin. Lipidol. 2011, 22, 43–48. [Google Scholar] [CrossRef]
- Palma-Lara, I.; Martínez-Castillo, M.; Quintana-Pérez, J.C.; Arellano-Mendoza, M.G.; Tamay-Cach, F.; Valenzuela-Limón, O.L.; García-Montalvo, E.A.; Hernández-Zavala, A. Arsenic exposure: A public health problem leading to several cancers. Regul. Toxicol. Pharmacol. 2020, 110, 104539. [Google Scholar] [CrossRef]
- Grau-Perez, M.; Navas-Acien, A.; Galan-Chilet, I.; Briongos-Figuero, L.S.; Morchon-Simon, D.; Bermudez, J.D.; Crainiceanu, C.M.; de Marco, G.; Rentero-Garrido, P.; Garcia-Barrera, T.; et al. Arsenic exposure, diabetes-related genes and diabetes prevalence in a general population from Spain. Environ. Pollut. 2018, 235, 948–955. [Google Scholar] [CrossRef]
- Zhou, M.; Zhao, E.; Huang, R. Association of urinary arsenic with insulin resistance: Cross-sectional analysis of the National Health and Nutrition Examination Survey, 2015–2016. Ecotoxicol. Environ. Saf. 2022, 231, 113218. [Google Scholar] [CrossRef]
- Moon, K.; Guallar, E.; Navas-Acien, A. Arsenic exposure and cardiovascular disease: An updated systematic review. Curr. Atheroscler. Rep. 2012, 14, 542–555. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, J.S.; Perez, V.; Garry, M.R.; Alexander, D.D. Association of low-level arsenic exposure in drinking water with cardiovascular disease: A systematic review and risk assessment. Toxicology 2014, 323, 78–94. [Google Scholar] [CrossRef] [PubMed]
- Basu, A.; Mitra, S.; Chung, J.; Guha Mazumder, D.N.; Ghosh, N.; Kalman, D.; von Ehrenstein, O.S.; Steinmaus, C.; Liaw, J.; Smith, A.H. Creatinine, diet, micronutrients, and arsenic methylation in West Bengal, India. Environ. Health Perspect. 2011, 119, 1308–1313. [Google Scholar] [CrossRef] [PubMed]
- Yao, X.; Steven Xu, X.; Yang, Y.; Zhu, Z.; Zhu, Z.; Tao, F.; Yuan, M. Stratification of population in NHANES 2009–2014 based on exposure pattern of lead, cadmium, mercury, and arsenic and their association with cardiovascular, renal and respiratory outcomes. Environ. Int. 2021, 149, 106410. [Google Scholar] [CrossRef] [PubMed]
- Bulka, C.M.; Persky, V.W.; Daviglus, M.L.; Durazo-Arvizu, R.A.; Argos, M. Multiple metal exposures and metabolic syndrome: A cross-sectional analysis of the National Health and Nutrition Examination Survey 2011–2014. Environ. Res. 2019, 168, 397–405. [Google Scholar] [CrossRef]
- Shiue, I. Higher urinary heavy metal, phthalate, and arsenic but not parabens concentrations in people with high blood pressure, U.S. NHANES, 2011–2012. Int. J. Environ. Res. Public Health 2014, 11, 5989–5999. [Google Scholar] [CrossRef]
- Wang, X.; Mukherjee, B.; Park, S.K. Associations of cumulative exposure to heavy metal mixtures with obesity and its comorbidities among U.S. adults in NHANES 2003–2014. Environ. Int. 2018, 121 Pt 1, 683–694. [Google Scholar] [CrossRef]
- Jones, M.R.; Tellez-Plaza, M.; Sharrett, A.R.; Guallar, E.; Navas-Acien, A. Urine arsenic and hypertension in US adults: The 2003–2008 National Health and Nutrition Examination Survey. Epidemiology 2011, 22, 153–161. [Google Scholar] [CrossRef]
- Nigra, A.E.; Moon, K.A.; Jones, M.R.; Sanchez, T.R.; Navas-Acien, A. Urinary arsenic and heart disease mortality in NHANES 2003–2014. Environ. Res. 2021, 200, 111387. [Google Scholar] [CrossRef]
- Huang, Y.L.; Hsueh, Y.M.; Huang, Y.K.; Yip, P.K.; Yang, M.H.; Chen, C.J. Urinary arsenic methylation capability and carotid atherosclerosis risk in subjects living in arsenicosis-hyperendemic areas in southwestern Taiwan. Sci. Total Environ. 2009, 407, 2608–2614. [Google Scholar] [CrossRef]
- Caldwell, K.L.; Jones, R.L.; Verdon, C.P.; Jarrett, J.M.; Caudill, S.P.; Osterloh, J.D. Levels of urinary total and speciated arsenic in the US population: National Health and Nutrition Examination Survey 2003–2004. J. Expo. Sci. Environ. Epidemiol. 2009, 19, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2021 Update: A Report From the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef] [PubMed]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Ro, S.H.; Bae, J.; Jang, Y.; Myers, J.F.; Chung, S.; Yu, J.; Natarajan, S.K.; Franco, R.; Song, H.S. Arsenic Toxicity on Metabolism and Autophagy in Adipose and Muscle Tissues. Antioxidants 2022, 11, 689. [Google Scholar] [CrossRef]
- Wei, S.; Qiu, T.; Yao, X.; Wang, N.; Jiang, L.; Jia, X.; Tao, Y.; Wang, Z.; Pei, P.; Zhang, J.; et al. Arsenic induces pancreatic dysfunction and ferroptosis via mitochondrial ROS-autophagy-lysosomal pathway. J. Hazard Mater. 2020, 384, 121390. [Google Scholar] [CrossRef]
- Abhyankar, L.N.; Jones, M.R.; Guallar, E.; Navas-Acien, A. Arsenic exposure and hypertension: A systematic review. Environ. Health Perspect. 2012, 120, 494–500. [Google Scholar] [CrossRef]
- Pánico, P.; Velasco, M.; Salazar, A.M.; Picones, A.; Ortiz-Huidobro, R.I.; Guerrero-Palomo, G.; Salgado-Bernabé, M.E.; Ostrosky-Wegman, P.; Hiriart, M. Is Arsenic Exposure a Risk Factor for Metabolic Syndrome? A Review of the Potential Mechanisms. Front. Endocrinol. 2022, 13, 878280. [Google Scholar] [CrossRef]
- Kondo, T.; Nakano, Y.; Adachi, S.; Murohara, T. Effects of Tobacco Smoking on Cardiovascular Disease. Circ. J. 2019, 83, 1980–1985. [Google Scholar] [CrossRef]
- Mostofsky, E.; Chahal, H.S.; Mukamal, K.J.; Rimm, E.B.; Mittleman, M.A. Alcohol and Immediate Risk of Cardiovascular Events: A Systematic Review and Dose-Response Meta-Analysis. Circulation 2016, 133, 979–987. [Google Scholar] [CrossRef]
- North, B.J.; Sinclair, D.A. The intersection between aging and cardiovascular disease. Circ. Res. 2012, 110, 1097–1108. [Google Scholar] [CrossRef] [PubMed]
- Yue, Y.; Nair, N.; Quinones, S.; Kordas, K.; Desai, G. Associations of total urinary arsenic with total cholesterol and high-density lipoprotein among 12–17-year-old participants from the 2009–2016 NHANES cycles: A cross-sectional study. Int. J. Hyg. Environ. Health 2022, 242, 113950. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.C.; Su, P.H.; Sun, C.W.; Liu, H.J.; Chang, C.L.; Wang, S.L. Early-life arsenic exposure promotes atherogenic lipid metabolism in adolescence: A 15-year birth cohort follow-up study in central Taiwan. Environ. Int. 2018, 118, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Suman, S.; Sharma, P.; Kumar, R.; Singh, S.K.; Bose, N.; Ghosh, A.; Rahman, M.M.; Polya, D.A.; Mondal, D. Assessment of hypertension association with arsenic exposure from food and drinking water in Bihar, India. Ecotoxicol. Environ. Saf. 2021, 223, 112572. [Google Scholar] [CrossRef]
- Jiang, Q.; Xiao, Y.; Long, P.; Li, W.; Yu, Y.; Liu, Y.; Liu, K.; Zhou, L.; Wang, H.; Yang, H.; et al. Associations of plasma metal concentrations with incident dyslipidemia: Prospective findings from the Dongfeng-Tongji cohort. Chemosphere 2021, 285, 131497. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Li, M.; Tian, X.; Xie, J.; Liu, P.; Ying, X.; Wang, M.; Yuan, J.; Gao, Y.; Tian, F.; et al. Effects of arsenic exposure on lipid metabolism: A systematic review and meta-analysis. Toxicol. Mech. Methods 2021, 31, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Nasab, H.; Rajabi, S.; Eghbalian, M.; Malakootian, M.; Hashemi, M.; Mahmoudi-Moghaddam, H. Association of As, Pb, Cr, and Zn urinary heavy metals levels with predictive indicators of cardiovascular disease and obesity in children and adolescents. Chemosphere 2022, 294, 133664. [Google Scholar] [CrossRef]
- Wu, M.M.; Chiou, H.Y.; Hsueh, Y.M.; Hong, C.T.; Su, C.L.; Chang, S.F.; Huang, W.L.; Wang, H.T.; Wang, Y.H.; Hsieh, Y.C.; et al. Effect of plasma homocysteine level and urinary monomethylarsonic acid on the risk of arsenic-associated carotid atherosclerosis. Toxicol. Appl. Pharmacol. 2006, 216, 168–175. [Google Scholar] [CrossRef]
- Mendez, M.A.; González-Horta, C.; Sánchez-Ramírez, B.; Ballinas-Casarrubias, L.; Cerón, R.H.; Morales, D.V.; Terrazas, F.A.; Ishida, M.C.; Gutiérrez-Torres, D.S.; Saunders, R.J.; et al. Chronic Exposure to Arsenic and Markers of Cardiometabolic Risk: A Cross-Sectional Study in Chihuahua, Mexico. Environ. Health Perspect. 2016, 124, 104–111. [Google Scholar] [CrossRef]
- Rotter, I.; Kosik-Bogacka, D.; Dołęgowska, B.; Safranow, K.; Lubkowska, A.; Laszczyńska, M. Relationship between the concentrations of heavy metals and bioelements in aging men with metabolic syndrome. Int. J. Environ. Res. Public Health 2015, 12, 3944–3961. [Google Scholar] [CrossRef]
- Hsueh, Y.M.; Wu, W.L.; Huang, Y.L.; Chiou, H.Y.; Tseng, C.H.; Chen, C.J. Low serum carotene level and increased risk of ischemic heart disease related to long-term arsenic exposure. Atherosclerosis 1998, 141, 249–257. [Google Scholar] [CrossRef]
- Calatayud, M.; Gimeno-Alcañiz, J.V.; Vélez, D.; Devesa, V. Trivalent arsenic species induce changes in expression and levels of proinflammatory cytokines in intestinal epithelial cells. Toxicol. Lett. 2014, 224, 40–46. [Google Scholar] [CrossRef]
- Wang, C.; Ning, Z.; Wan, F.; Huang, R.; Chao, L.; Kang, Z.; Yang, F.; Zhong, G.; Li, Y.; Pan, J.; et al. Characterization of the cellular effects and mechanism of arsenic trioxide-induced hepatotoxicity in broiler chickens. Toxicol. In Vitro 2019, 61, 104629. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H. The potential biological mechanisms of arsenic-induced diabetes mellitus. Toxicol. Appl. Pharmacol. 2004, 197, 67–83. [Google Scholar] [CrossRef] [PubMed]
- Ishaq, A.; Gulzar, H.; Hassan, A.; Kamran, M.; Riaz, M.; Parveen, A.; Chattha, M.S.; Walayat, N.; Fatima, S.; Afzal, S.; et al. Ameliorative mechanisms of turmeric-extracted curcumin on arsenic (As)-induced biochemical alterations, oxidative damage, and impaired organ functions in rats. Environ. Sci. Pollut. Res. Int. 2021, 28, 66313–66326. [Google Scholar] [CrossRef] [PubMed]
- Harmon, M.E.; Lewis, J.; Miller, C.; Hoover, J.; Ali, A.S.; Shuey, C.; Cajero, M.; Lucas, S.; Pacheco, B.; Erdei, E.; et al. Arsenic association with circulating oxidized low-density lipoprotein in a Native American community. J. Toxicol. Environ. Health A 2018, 81, 535–548. [Google Scholar] [CrossRef]
- Vergara-Gerónimo, C.A.; León Del Río, A.; Rodríguez-Dorantes, M.; Ostrosky-Wegman, P.; Salazar, A.M. Arsenic-protein interactions as a mechanism of arsenic toxicity. Toxicol. Appl. Pharmacol. 2021, 431, 115738. [Google Scholar] [CrossRef]
- Galvez-Fernandez, M.; Sanchez-Saez, F.; Domingo-Relloso, A.; Rodriguez-Hernandez, Z.; Tarazona, S.; Gonzalez-Marrachelli, V.; Grau-Perez, M.; Morales-Tatay, J.M.; Amigo, N.; Garcia-Barrera, T.; et al. Gene-environment interaction analysis of redox-related metals and genetic variants with plasma metabolic patterns in a general population from Spain: The Hortega Study. Redox Biol. 2022, 52, 102314. [Google Scholar] [CrossRef]
- Jiang, X.; Yu, W.; Wu, S.; Tang, L.; Zhong, G.; Wan, F.; Lan, J.; Zhang, H.; Pan, J.; Tang, Z.; et al. Arsenic (III) and/or Antimony (III) induced disruption of calcium homeostasis and endoplasmic reticulum stress resulting in apoptosis in mice heart. Ecotoxicol. Environ. Saf. 2021, 220, 112394. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. (%) a | Urine Arsenic Median (IQR)-μg/L | p Value c |
|---|---|---|---|
| Overall | 6633 | 7.86 (4.07–17.57) | |
| Sex | <0.001 | ||
| Male | 3247 (49.0) | 8.74 (4.55–18.77) | |
| Female | 3386 (51.0) | 7.20 (3.70–16.00) | |
| Age (year) | 0.055 | ||
| 20–39 | 2201 (33.2) | 7.53 (4.03–15.84) | |
| 40–59 | 2138 (32.2) | 7.96 (4.02–17.34) | |
| ≥60 | 2294 (34.6) | 8.27 (4.15–18.58) | |
| Race | <0.001 | ||
| Mexican American | 1071 (16.2) | 7.34 (3.99–13.50) | |
| Other Hispanic | 638 (9.6) | 10.38 (5.13–20.59) | |
| Non-Hispanic White | 2818 (42.5) | 6.54 (3.52–14.04) | |
| Non-Hispanic Black | 1395 (21.0) | 8.70 (4.73–22.02) | |
| Other Races | 711 (10.7) | 13.13 (5.15–35.12) | |
| Marital status | <0.001 | ||
| With partner | 4030 (60.8) | 8.48 (4.36–18.40) | |
| Without partner | 2603 (39.2) | 7.18 (3.74–16.12) | |
| education | 0.004 | ||
| High school and below | 3229 (48.7) | 7.47 (3.99–16.20) | |
| Above high school | 3404 (51.3) | 8.23 (4.15–18.76) | |
| Diastolic blood pressure (mmHg) | 0.841 | ||
| <90 | 6265 (94.5) | 7.88 (4.03–17.50) | |
| ≥90 | 368 (5.5) | 7.66 (4.41–18.63) | |
| Systolic blood pressure (mmHg) | 0.835 | ||
| <140 | 5516 (83.2) | 7.85 (4.08–17.25) | |
| ≥140 | 1117 (16.8) | 7.98 (4.05–19.02) | |
| BMI (kg/m2) b | 0.678 | ||
| <25 | 1959 (29.5) | 8.00 (3.82–19.18) | |
| 25-30 | 2260 (34.1) | 8.00 (4.15–17.64) | |
| ≥30 | 2414 (36.4) | 7.66 (4.21–16.67) | |
| TC (mg/dL) | 0.889 | ||
| <200 | 3999 (60.3) | 7.87 (4.09–7.23) | |
| ≥200 | 2634 (39.7) | 7.79 (4.06–17.90) | |
| LDL-C (mg/dL) | 0.117 | ||
| <100 | 2474 (37.3) | 7.64 (3.93–16.94) | |
| ≥100 | 4159 (62.7) | 8.02 (4.14–17.99) | |
| Creatinine (mg/dL) | <0.001 | ||
| <80 | 2187 (33.0) | 4.05 (2.20–8.94) | |
| 80–140 | 2281 (34.4) | 8.53 (4.67–18.18) | |
| >144 | 2165 (32.6) | 11.93 (7.00–26.43) | |
| Cotinine (ng/dL) | 0.001 | ||
| <0.015 | 1351 (20.4) | 8.12 (4.22–16.80) | |
| 0.015–10.0 | 3954 (59.6) | 8.00 (4.18–18.67) | |
| >10.0 | 1328 (20.0) | 7.30 (3.77–14.70) | |
| Hypertension | 0.201 | ||
| Yes | 2366 (35.7) | 8.09 (4.23–18.00) | |
| No | 4267 (64.3) | 7.76 (3.99–17.20) | |
| Diabetes | 0.840 | ||
| Yes | 842 (12.7) | 7.72 (4.24–16.24) | |
| No | 5626 (84.8) | 7.86 (4.03–17.62) | |
| Boardline | 165 (2.5) | 8.17 (4.21–18.32) | |
| Kidney disease | 0.316 | ||
| Yes | 208 (3.1) | 7.26 (4.37–16.42) | |
| no | 6425 (96.9) | 7.89 (4.07–17.60) | |
| Smoking | 0.007 | ||
| Yes | 3028 (45.7) | 7.58 (3.95–16.47) | |
| No | 3605 (54.3) | 8.14 (4.18–18.32) | |
| Drinking | <0.001 | ||
| Yes | 5141 (51.4) | 8.10 (4.21–18.00) | |
| No | 1492 (14.9) | 7.21 (3.80–15.80) |
| Serum Lipids | β-Coefficients (95% CI a) | p Value | |
|---|---|---|---|
| TC (mg/dL) | Model 1 b | 2.42 (1.48, 3.36) | <0.001 |
| Model 2 c | 2.38 (1.44, 3.31 | <0.001 | |
| LDL-C (mg/dL) | Model 1 b | 0.94 (0.13, 1.76) | 0.024 |
| Model 2 c | 0.95 (0.14, 1.77) | 0.022 |
| 70th Versus 30th Percentile | 80th Versus 20th Percentile | ||||
|---|---|---|---|---|---|
| Urinary total arsenic (μg/L) | 14.40/4.70 | 22.00/3.49 | |||
| TC | Model 1 a | 1.17 (1.02, 1.35) | 1 [Reference] | 1.28 (1.08, 1.52) | 1 [Reference] |
| Model 2 b | 1.21 (1.05, 1.39) | 1 [Reference] | 1.34 (1.13, 1.59) | 1 [Reference] | |
| LDL-C | Model 3 c | 1.15 (1.00, 1.32) | 1 [Reference] | 1.12 (1.03, 1.22) | 1 [Reference] |
| Model 4 d | 1.23 (1.06, 1.41) | 1 [Reference] | 1.36 (1.15, 1.62) | 1 [Reference] |
| Quartile 1 | Quartile 2 | Quartile 3 | Quartile 4 | p Value for Trend | ||
|---|---|---|---|---|---|---|
| Urinary total arsenic (μg/L) | <4.07 | 4.07–7.86 | 7.86–17.57 | >17.57 | ||
| TC | Model 1 a | 1 [reference] | 1.14 (0.98, 1.32) | 1.13 (0.98, 1.32) | 1.24 (1.07, 1.45) | 0.020 |
| Model 2 b | 1 [reference] | 1.16 (1.00, 1.34) | 1.17 (1.00, 1.36) | 1.29 (1.11, 1.50) | 0.007 | |
| LDL-C | Model 3 c | 1 [reference] | 1.10 (0.95, 1.27) | 1.11 (0.95, 1.29) | 1.20 (1.03, 1.40) | 0.041 |
| Model 4 d | 1 [reference] | 1.13 (0.97, 1.31) | 1.16 (0.99, 1.35) | 1.29 (1.10, 1.51) | 0.005 |
| Speciated Arsenics | Median (IQR)-μg/L | 80th versus 20th Percentile | OR (95% CI) of TC | OR (95% CI) of LDL-C |
|---|---|---|---|---|
| Arsenous acid | 0.80 (0.34, 0.85) | 0.85/0.08 | 0.99 (0.81, 1.21) | 1.20 (0.98, 1.46) |
| Arsenic acid | 0.62 (0.56, 0.71) | 0.71/0.56 | 1.35 (1.02, 1.79) * | 1.22 (0.91, 1.62) |
| Arsenobetaine | 1.29 (0.82, 6.58) | 9.37/0.82 | 0.99 (0.87, 1.13) | 0.87 (0.74, 1.02) |
| Arsenocholine | 0.32 (0.08, 0.42) | 0.42/0.08 | 1.11 (0.84, 1.41) | 1.15 (0.87, 1.52) |
| Dimethylarsinic | 3.65 (2.11, 6.40) | 7.39/1.87 | 1.09 (0.94, 1.28) | 1.20 (1.03, 1.41) * |
| Monomethylarsonic | 0.64 (0.56, 1.00) | 1.13/0.36 | 1.14 (0.97, 1.34) | 1.30 (1.11, 1.52) (***) |
| Speciated Arsenics | OR (95% CI) of TC | OR (95% CI) of LDL-C | ||
|---|---|---|---|---|
| Model1 a | Model2 b | Model3 c | Model4 d | |
| Arsenous acid | 1.13 (0.91, 1.38) | 1.17 (0.95, 1.44) | 1.23 (1.00, 1.51) * | 1.23 (1.01, 1.52) * |
| Arsenic acid | 1.44 (1.08, 1.92) * | 1.46 (1.10, 1.95) (**) | 1.24 (0.93, 1.66) | 1.23 (0.92, 1.65) |
| Arsenobetaine | 1.07 (0.93, 1.23) | 1.07 (0.93, 1.23) | 0.93 (0.79, 1.09) | 0.91 (0.77, 1.07) |
| Arsenocholine | 1.20 (0.90, 1.60) | 1.19 (0.89, 1.59) | 1.21 (0.91, 1.61) | 1.20 (0.90, 1.59) |
| Dimethylarsinic | 1.50 (1.25, 1.79) *** | 1.47 (1.23, 1.76) *** | 1.37 (1.15, 1.64) (***) | 1.34 (1.12, 1.61 (***) |
| Monomethylarsonic | 1.38 (1.16, 1.64) *** | 1.36 (1.15, 1.62) *** | 1.44 (1.22, 1.71) *** | 1.43 (1.21, 1.70) *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qu, C.; Huang, R. Linking the Low-Density Lipoprotein-Cholesterol (LDL) Level to Arsenic Acid, Dimethylarsinic, and Monomethylarsonic: Results from a National Population-Based Study from the NHANES, 2003–2020. Nutrients 2022, 14, 3993. https://doi.org/10.3390/nu14193993
Qu C, Huang R. Linking the Low-Density Lipoprotein-Cholesterol (LDL) Level to Arsenic Acid, Dimethylarsinic, and Monomethylarsonic: Results from a National Population-Based Study from the NHANES, 2003–2020. Nutrients. 2022; 14(19):3993. https://doi.org/10.3390/nu14193993
Chicago/Turabian StyleQu, Can, and Ruixue Huang. 2022. "Linking the Low-Density Lipoprotein-Cholesterol (LDL) Level to Arsenic Acid, Dimethylarsinic, and Monomethylarsonic: Results from a National Population-Based Study from the NHANES, 2003–2020" Nutrients 14, no. 19: 3993. https://doi.org/10.3390/nu14193993
APA StyleQu, C., & Huang, R. (2022). Linking the Low-Density Lipoprotein-Cholesterol (LDL) Level to Arsenic Acid, Dimethylarsinic, and Monomethylarsonic: Results from a National Population-Based Study from the NHANES, 2003–2020. Nutrients, 14(19), 3993. https://doi.org/10.3390/nu14193993