
Nutrition Behavior and Physical Activity of Middle-Aged and Older Adults in Saudi Arabia

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants and Recruitment
2.3. Questionnaire
2.4. Data Analysis
2.5. Sample Size Calculation
2.6. Statistical Analysis
3. Results
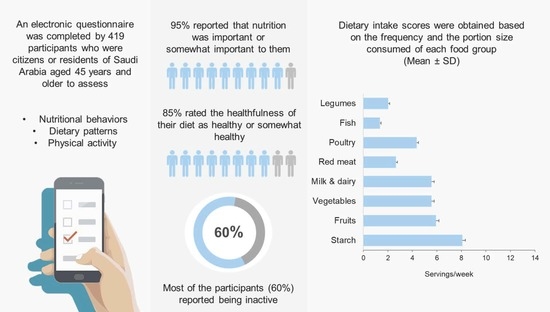
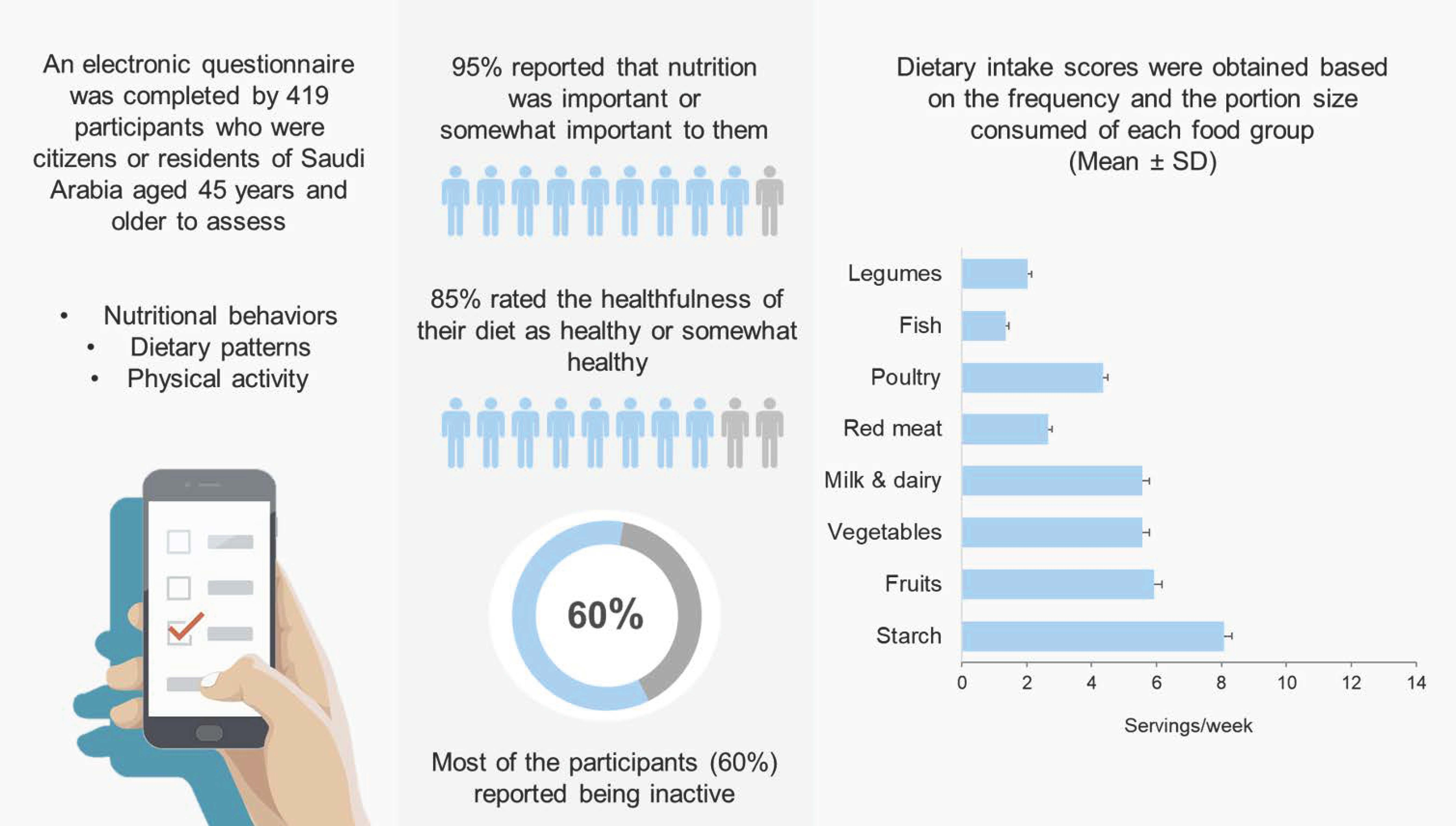
3.1. Characteristics of the Study Participants
3.2. Dietary Behavior Self-Evaluation
3.3. Dietary Intake Assessment
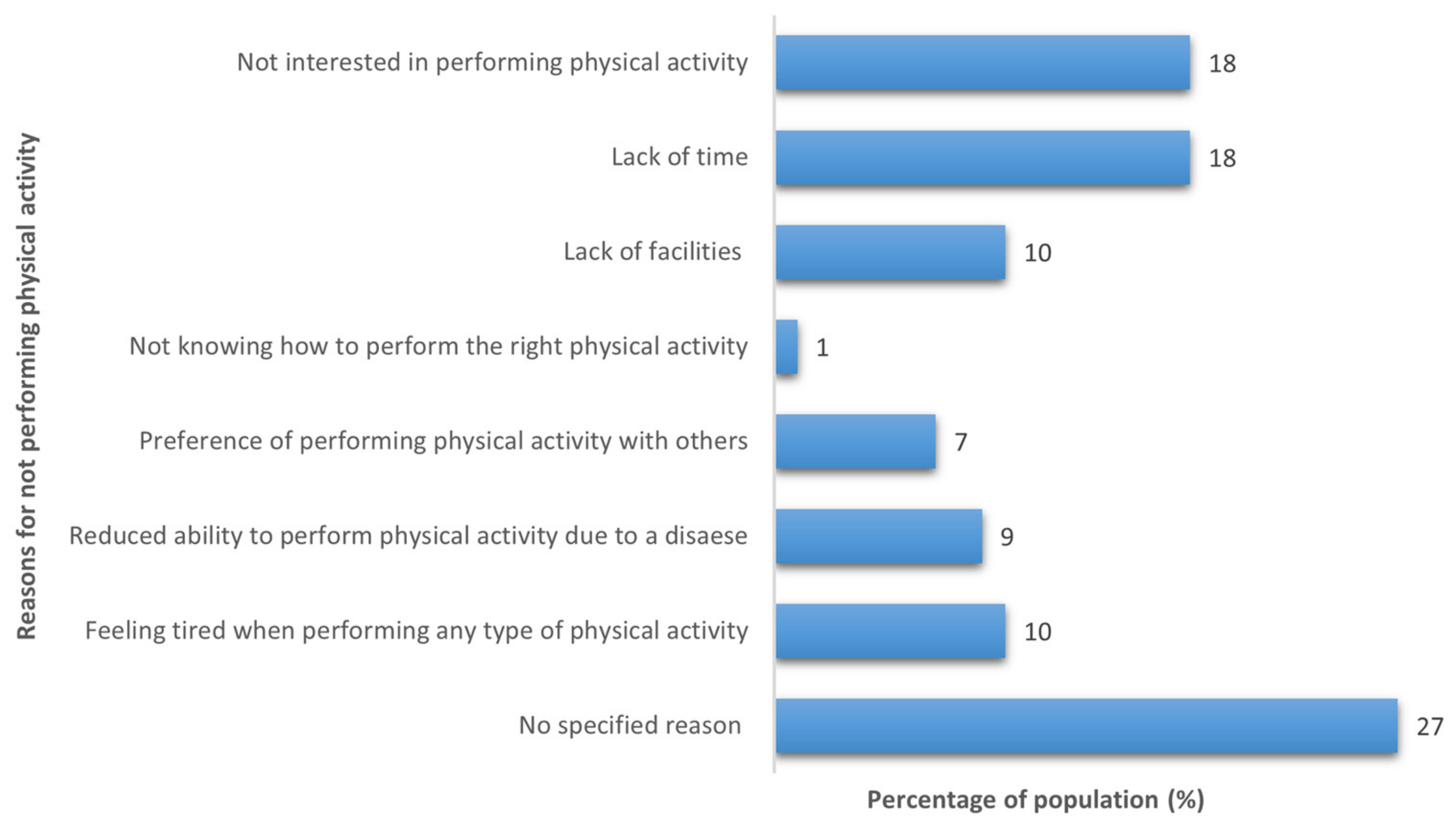
3.4. Physical Activity Assessment
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Ageing and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 11 November 2021).
- United Nations. UNData: A World of Information. Available online: https://data.un.org/en/iso/sa.html (accessed on 21 August 2021).
- Colloca, G.; Santoro, M.; Gambassi, G. Age-Related Physiologic Changes and Perioperative Management of Elderly Patients. Surg. Oncol. 2010, 19, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Frontera, W.R. Physiologic Changes of the Musculoskeletal System with Aging: A Brief Review. Phys. Med. Rehabil. Clin. N. Am. 2017, 28, 705–711. [Google Scholar] [CrossRef]
- Franco, O.H.; Karnik, K.; Osborne, G.; Ordovas, J.M.; Catt, M.; Van Der Ouderaa, F. Changing Course in Ageing Research: The Healthy Ageing Phenotype. Maturitas 2009, 63, 13–19. [Google Scholar] [CrossRef]
- Black, M.; Bowman, M. Nutrition and Healthy Aging. Clin. Geriatr. Med. 2020, 36, 655–669. [Google Scholar] [CrossRef]
- Roberts, S.B.; Silver, R.E.; Das, S.K.; Fielding, R.A.; Gilhooly, C.H.; Jacques, P.F.; Kelly, J.M.; Mason, J.B.; McKeown, N.M.; Reardon, M.A.; et al. Healthy Aging—Nutrition Matters: Start Early and Screen Often. Adv. Nutr. 2021, 12, 1438–1448. [Google Scholar] [CrossRef]
- Chiuve, S.; Fung, T.; Rimm, E.; Hu, F.; McCullough, M.; Wang, M.; Stampfer, M.; Willett, W. Alternative Dietary Indices Both Strongly Predict Risk of Chronic Disease. J. Nutr. 2012, 142, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Moradi-Lakeh, M.; El Bcheraoui, C.; Afshin, A.; Daoud, F.; Almazroa, M.A.; Al Saeedi, M.; Basulaiman, M.; Memish, Z.A.; Al Rabeeah, A.A.; Mokdad, A.H. Diet in Saudi Arabia: Findings from a Nationally Representative Survey. Public Health Nutr. 2017, 20, 1075–1081. [Google Scholar] [CrossRef]
- General Authority for Statistics Kingdom of Saudi Arabia. Population by Age Groups, and Gender Mid Year 2020. Available online: https://www.stats.gov.sa/en/6768 (accessed on 12 November 2021).
- Kiefte-De Jong, J.C.; Mathers, J.C.; Franco, O.H. Nutrition and Healthy Ageing: The Key Ingredients. Proc. Nutr. Soc. 2014, 73, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Gille, D.; Bütikofer, U.; Chollet, M.; Schmid, A.; Altintzoglou, T.; Honkanen, P.; Stoffers, H.; Walther, B.; Piccinali, P. Nutrition Behavior of the Middle-Aged and Elderly: Compliance with Dietary Recommendations of the Food Pyramid. Clin. Nutr. 2016, 35, 638–644. [Google Scholar] [CrossRef]
- Andersen, D.; Baird, S.; Bates, T.; Chapel, D.L.; Cline, A.D.; Ganesh, S.N.; Garner, M.; Grant, B.L.; Hamilton, K.K.; Jablonski, K.; et al. Academy of Nutrition and Dietetics: Revised 2017 Standards of Practice in Nutrition Care and Standards of Professional Performance for Registered Dietitian Nutritionists. J. Acad. Nutr. Diet. 2018, 118, 132–140.e15. [Google Scholar] [CrossRef]
- Winter, J.E.; Mcnaughton, S.A.; Nowson, C.A. Older Adults’ Attitudes to Food and Nutrition: A Qualitative Study. J. aging Res. Clin. Pract. 2016, 5, 114–119. [Google Scholar] [CrossRef]
- Ball, L.; Desbrow, B.; Leveritt, M. An Exploration of Individuals’ Preferences for Nutrition Care’from Australian Primary Care Health Professionals. Artic. Aust. J. Prim. Health 2013, 20, 113–120. [Google Scholar] [CrossRef]
- Dumas, A.A.; Lapointe, A.; Desroches, S. Users, Uses, and Effects of Social Media in Dietetic Practice: Scoping Review of the Quantitative and Qualitative Evidence. J. Med. Internet Res. 2018, 20. [Google Scholar] [CrossRef]
- Adamski, M.; Truby, H.; Klassen, K.M.; Cowan, S.; Gibson, S. Using the Internet: Nutrition Information-Seeking Behaviours of Lay People Enrolled in a Massive Online Nutrition Course. Nutrients 2020, 12, 750. [Google Scholar] [CrossRef]
- Cash, T.; Desbrow, B.; Leveritt, M.; Ball, L. Utilization and Preference of Nutrition Information Sources in Australia. Heal. Expect. 2015, 18, 2288–2295. [Google Scholar] [CrossRef]
- Arfaoui, L.; Alkhaldy, A.; Alareeshi, A.; Alsaadi, G.; Alhendi, S.; Alghanmi, A.; Alghafari, W.; Assidi, M. Assessment of Knowledge and Self-Reported Use of Nutrition Facts Labels, Nutrient Content, and Health Claims among Saudi Adult Consumers. J. Multidiscip. Healthc. 2021, 14, 2959. [Google Scholar] [CrossRef]
- Miller, L.M.S.; Applegate, E.; Beckett, L.A.; Wilson, M.D.; Gibson, T.N. Age Differences in the Use of Serving Size Information on Food Labels: Numeracy or Attention? Public Health Nutr. 2017, 20, 786. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Healthy Diet. Available online: https://apps.who.int/iris/bitstream/handle/10665/325828/EMROPUB_2019_en_23536.pdf (accessed on 10 July 2022).
- Sahyoun, N.R.; Zhang, X.L.; Serdula, M.K. Barriers to the Consumption of Fruits and Vegetables among Older Adults. J. Nutr. Elder. 2006, 24, 5–21. [Google Scholar] [CrossRef]
- Nicklett, E.J.; Kadell, A.R. Fruit and Vegetable Intake among Older Adults: A Scoping Review. Maturitas 2013, 75, 305–312. [Google Scholar] [CrossRef]
- Drewnowski, A.; Shultz, J.M. Impact of Aging on Eating Behaviors, Food Choices, Nutrition, and Health Status. J. Nutr. Health Aging 2001, 5, 75–79. [Google Scholar]
- El Bcheraoui, C.; Basulaiman, M.; AlMazroa, M.A.; Tuffaha, M.; Daoud, F.; Wilson, S.; Al Saeedi, M.Y.; Alanazi, F.M.; Ibrahim, M.E.; Ahmed, E.M.; et al. Fruit and Vegetable Consumption among Adults in Saudi Arabia, 2013. Nutr. Diet. Suppl. 2015, 7, 41–49. [Google Scholar] [CrossRef]
- Bowman, S. Low Economic Status Is Associated with Suboptimal Intakes of Nutritious Foods by Adults in the National Health and Nutrition Examination Survey 1999-2002. Nutr. Res. 2007, 27, 515–523. [Google Scholar] [CrossRef]
- Muhammad, A.; D’Souza, A.; Meade, B.; Micha, R.; Mozaffarian, D. How Income and Food Prices Influence Global Dietary Intakes by Age and Sex: Evidence from 164 Countries. BMJ Glob. Health 2017, 2, e000184. [Google Scholar] [CrossRef]
- Carbone, J.W.; Pasiakos, S.M. Dietary Protein and Muscle Mass: Translating Science to Application and Health Benefit. Nutrients 2019, 11, 1136. [Google Scholar] [CrossRef]
- Kouvari, M.; Tyrovolas, S.; Panagiotakos, D.B. Red Meat Consumption and Healthy Ageing: A Review. Maturitas 2016, 84, 17–24. [Google Scholar] [CrossRef]
- Alsufiani, H.M.; Kumosani, T.A.; Ford, D.; Mathers, J.C. Dietary Patterns, Nutrient Intakes, and Nutritional and Physical Activity Status of Saudi Older Adults: A Narrative Review. J. Aging Res. Lifestyle 2015, 4, 2–11. [Google Scholar] [CrossRef]
- Wardle, J.; Haase, A.M.; Steptoe, A.; Nillapun, M.; Jonwutiwes, K.; Bellisle, F. Gender Differences in Food Choice: The Contribution of Health Beliefs and Dieting. Ann. Behav. Med. 2004, 27, 107–116. [Google Scholar] [CrossRef]
- DicksonSpillmann, M.; Siegrist, M. Consumers’ Knowledge of Healthy Diets and Its Correlation with Dietary Behaviour. J. Hum. Nutr. Diet. 2011, 24, 54–60. [Google Scholar] [CrossRef]
- Trondsen, T.; Braaten, T.; Lund, E.; Eggen, A.E. Consumption of Seafood—the Influence of Overweight and Health Beliefs. Food Qual. Prefer. 2004, 15, 361–374. [Google Scholar] [CrossRef]
- Burger, J.; Gochfeld, M.; Batang, Z.; Alikunhi, N.; Al-Jahdali, R.; Al-Jebreen, D.; Aziz, M.A.M.; Al-Suwailem, A. Fish Consumption Behavior and Rates in Native and Non-Native People in Saudi Arabia. Environ. Res. 2014, 133, 141–148. [Google Scholar] [CrossRef]
- Alqahtani, B.A.; Alenazi, A.M.; Alhowimel, A.S.; Elnaggar, R.K. The Descriptive Pattern of Physical Activity in Saudi Arabia: Analysis of National Survey Data. Int. Health 2021, 13, 232–239. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N | % |
|---|---|---|
| Age (years) | ||
| 45–54 | 194 | 46 |
| 55–64 | 169 | 40 |
| ≥65 | 56 | 14 |
| Mean ± SD | 55.5 ± 7 | |
| Gender | ||
| Male | 278 | 66 |
| Female | 141 | 34 |
| Nationality | ||
| Saudi | 382 | 91 |
| Non-Saudi 2 | 37 | 9 |
| Region | ||
| Western Region | 262 | 63 |
| Central Region | 98 | 23 |
| Eastern Region | 33 | 8 |
| Northern Region | 9 | 2 |
| Southern Region | 17 | 4 |
| Marital status | ||
| Single | 24 | 6 |
| Married | 362 | 86 |
| Divorced | 21 | 5 |
| Widower | 12 | 3 |
| Living situation | ||
| Living alone | 158 | 38 |
| Living with others | 261 | 62 |
| Education level | ||
| High school education or less | 81 | 19 |
| University education | 253 | 61 |
| Higher education | 85 | 20 |
| Work status | ||
| Employed | 161 | 38 |
| Freelance job | 27 | 7 |
| Retired | 184 | 44 |
| Unemployed | 47 | 11 |
| Income (SR) | ||
| <2000 | 37 | 9 |
| 2000–5000 | 34 | 8 |
| 5000–7000 | 23 | 6 |
| 7000–10,000 | 48 | 11 |
| >10,000 | 277 | 66 |
| Main medical diagnosis | ||
| No diseases | 153 | 37 |
| Heart diseases | 144 | 34 |
| Respiratory disorders | 25 | 6 |
| Gastrointestinal diseases | 29 | 7 |
| Cancer | 10 | 3 |
| Renal disorders | 9 | 2 |
| Liver disorders | 4 | 1 |
| Diabetes | 102 | 24 |
| Iron deficiency anemia | 19 | 4 |
| Osteoporosis | 29 | 7 |
| Others 3 | 23 | 5 |
| Smoking | ||
| Yes | 93 | 22 |
| No | 257 | 61 |
| Ex-smoker | 69 | 17 |
| BMI category 4 | ||
| Underweight | 4 | 1 |
| Normal | 84 | 20 |
| Overweight | 171 | 41 |
| Obese | 160 | 38 |
| Variables | How Important is Nutrition for You? | How Would You Rate the Healthfulness of Your Overall Diet? | ||||
|---|---|---|---|---|---|---|
| Important | Somewhat Important | Not Important | Healthy | Somewhat Healthy | Not Healthy | |
| Total (%) | 65 | 30 | 5 | 19 | 66 | 15 |
| Age (years) | ||||||
| 45–54 | 122 (29) | 59 (14) | 13 (3) | 30 (7) | 125 (30) | 39 (9) |
| 55–64 | 110 (26) | 52 (12) | 7 (2) | 38 (9) | 116 (28) | 15 (4) |
| ≥65 | 40 (10) | 15 (4) | 1 (0) | 14 (3) | 34 (8) | 8 (2) |
| p-value | 0.517 | 0.022 | ||||
| Gender | ||||||
| Male | 184 (44) | 84 (20) | 10 (2) | 56 (13) | 180 (43) | 42 (10) |
| Female | 88 (21) | 42 (10) | 11 (3) | 26 (6) | 95 (23) | 20 (5) |
| p-value | 0.173 | 0.865 | ||||
| Marital status | ||||||
| Single | 14 (3) | 8 (2) | 2 (0) | 5 (1) | 13 (3) | 6 (1) |
| Married | 239 (57) | 108 (26) | 15 (4) | 72 (17) | 240 (57) | 50 (12) |
| Divorced | 9 (2) | 9 (2) | 3 (1) | 5 (1) | 12 (3) | 4 (1) |
| Widower | 10 (3) | 1 (0) | 1 (0) | 0 (0) | 10 (3) | 2 (1) |
| p-value | 0.090 | 0.412 | ||||
| Living situation | ||||||
| Living alone | 101 (24) | 52 (12) | 5 (1) | 29 (7) | 110 (26) | 19 (5) |
| Living with others | 171 (41) | 74 (18) | 16 (4) | 53 (12) | 165 (40) | 43 (10) |
| p-value | 0.294 | 0.346 | ||||
| Education | ||||||
| High school or less | 51 (12) | 24 (6) | 6 (3) | 18 (4) | 51 (12) | 12 (3) |
| University education | 160 (38) | 79 (19) | 14 (2) | 46 (11) | 168 (40) | 39 (9) |
| Higher education | 61 (15) | 23 (5) | 1 (0) | 18 (4) | 56 (14) | 11 (3) |
| p-value | 0.319 | 0.906 | ||||
| Work status | ||||||
| Employed | 107 (26) | 45 (11) | 9 (2) | 27 (6) | 105 (25) | 29 (7) |
| Freelance Job | 18 (4) | 9 (2) | 0 (0) | 6 (2) | 17 (4) | 4 (1) |
| Retired | 120 (29) | 56 (13) | 8 (2) | 39 (9) | 122 (29) | 23 (5) |
| Unemployed | 27 (6) | 16 (4) | 4 (1) | 10 (2) | 31 (8) | 6 (2) |
| p-value | 0.698 | 0.806 | ||||
| Income (SR) | ||||||
| <2000 | 19 (5) | 14 (3) | 4 (1) | 10 (2) | 22 (5) | 5 (1) |
| 2000–5000 | 22 (5) | 8 (2) | 4 (1) | 7 (1) | 20 (5) | 7 (2) |
| 5000–7000 | 14 (3) | 8 (2) | 1 (1) | 3 (1) | 13 (3) | 7 (2) |
| 7000–10,000 | 26 (6) | 16 (4) | 6 (1) | 4 (1) | 32 (8) | 12 (3) |
| >10,000 | 191 (46) | 80 (19) | 6 (1) | 58 (14) | 188 (45) | 31 (7) |
| p-value | 0.011 | 0.038 | ||||
| BMI category 2 | ||||||
| Underweight | 2 (0) | 2 (0) | 0 (0) | 0 (0) | 2 (0) | 2 (0) |
| Normal weight | 53 (13) | 26 (6) | 5 (1) | 23 (5) | 54 (13) | 7 (2) |
| Overweight | 110 (26) | 53 (13) | 8 (2) | 35 (8) | 115 (28) | 21 (5) |
| Obese | 107 (26) | 45 (11) | 8 (2) | 24 (6) | 104 (25) | 32 (8) |
| p-value | 0.959 | 0.068 | ||||
| Variables | Starch | Fruits | Vegetables | Milk and Dairy Products | Red Meat | Poultry | Fish | Legumes |
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | 8.09 ± 0.24 | 5.92 ± 0.25 | 5.57 ± 0.22 | 5.56 ± 0.23 | 2.65 ± 0.13 | 4.34 ± 0.16 | 1.36 ± 0.08 | 2.03 ± 0.12 |
| Age (years) | ||||||||
| 45–54 | 7.92 ± 0.35 | 4.28 ± 0.33 | 4.77 ± 0.30 | 5.74 ± 0.36 | 2.59 ± 0.22 | 4.79 ± 0.26 | 1.10 ± 0.12 | 2.09 ± 0.21 |
| 55–64 | 8.02 ± 0.37 | 7.25 ± 0.41 | 6.44 ± 0.37 | 5.43 ± 0.35 | 2.57 ± 0.18 | 3.96 ± 0.24 | 1.58 ± 0.13 | 1.89 ± 0.14 |
| ≥65 | 8.90 ± 0.67 | 7.61 ± 0.70 | 5.75 ± 0.60 | 5.32 ± 0.55 | 3.07 ± 0.43 | 3.95 ± 0.39 | 1.61 ± 0.18 | 2.23 ± 0.30 |
| p-value | 0.817 | <0.001 | 0.027 | 0.542 | 0.267 | 0.089 | <0.001 | 0.143 |
| Gender | ||||||||
| Male | 8.14 ± 0.29 | 5.52 ± 0.30 | 5.20 ± 0.26 | 5.40 ± 0.27 | 2.94 ± 0.17 | 4.78 ± 0.21 | 1.54 ± 0.10 | 2.25 ± 0.15 |
| Female | 7.99 ± 0.40 | 6.12 ± 0.46 | 6.30 ± 0.41 | 5.88 ± 0.43 | 2.06 ± 0.22 | 3.48 ± 0.26 | 1.02 ± 0.12 | 1.59 ± 0.17 |
| p-value | 0.903 | 0.948 | 0.035 | 0.649 | <0.001 | <0.001 | <0.001 | <0.001 |
| Marital status | ||||||||
| Single | 8.06 ± 1.20 | 3.54 ± 0.81 | 5.22 ± 0.93 | 4.14 ± 0.90 | 1.91 ± 0.45 | 2.68 ± 0.41 | 1.35 ± 0.35 | 1.56 ± 0.31 |
| Married | 8.13 ± 0.25 | 6.08 ± 0.27 | 5.65 ± 0.24 | 5.56 ± 0.25 | 2.76 ± 0.15 | 4.57 ± 0.18 | 1.42 ± 0.09 | 2.10 ± 0.13 |
| Divorced | 6.97 ± 0.95 | 6.12 ± 1.22 | 4.98 ± 1.08 | 6.85 ± 0.88 | 2.59 ± 0.71 | 3.21 ± 0.72 | 0.83 ± 0.21 | 1.50 ± 0.31 |
| Widower | 9.00 ± 1.35 | 5.67 ± 1.60 | 4.96 ± 1.38 | 6.29 ± 1.78 | 0.87 ± 0.17 | 2.75 ± 0.67 | 0.41 ± 0.10 | 1.83 ± 0.60 |
| p-value | 0.698 | 0.112 | 0.655 | 0.094 | 0.009 | 0.002 | 0.002 | 0.633 |
| Living situation | ||||||||
| Living alone | 8.31 ± 0.38 | 6.51 ± 0.42 | 5.78 ± 0.37 | 5.49 ± 0.37 | 2.74 ± 0.24 | 4.25 ± 0.25 | 1.41 ± 0.12 | 1.87 ± 0.14 |
| Living with others | 7.95 ± 0.31 | 5.56 ± 0.32 | 5.45 ± 0.28 | 5.60 ± 0.29 | 2.59 ± 0.16 | 4.40 ± 0.22 | 1.33 ± 0.11 | 2.13 ± 0.17 |
| p-value | 0.423 | 0.045 | 0.504 | 0.888 | 0.982 | 0.808 | 0.194 | 0.599 |
| Education | ||||||||
| High school or less | 7.09 ± 0.50 | 5.53 ± 0.58 | 5.74 ± 0.50 | 5.90 ± 0.58 | 2.45 ± 0.30 | 4.63 ± 0.42 | 1.01 ± 0.10 | 2.09 ± 0.28 |
| University education | 8.13 ± 0.31 | 5.86 ± 0.33 | 5.26 ± 0.28 | 5.55 ± 0.29 | 2.66 ± 0.18 | 4.30 ± 0.21 | 1.38 ± 0.11 | 2.12 ± 0.17 |
| Higher education | 8.91 ± 0.55 | 6.50 ± 0.56 | 6.34 ± 0.52 | 5.26 ± 0.51 | 2.80 ± 0.31 | 4.19 ± 0.33 | 1.64 ± 0.22 | 1.70 ± 0.16 |
| p-value | 0.130 | 0.246 | 0.167 | 0.800 | 0.407 | 0.919 | 0.165 | 0.858 |
| Work status | ||||||||
| Employed | 8.59 ± 0.40 | 5.34 ± 0.41 | 4.87 ± 0.33 | 5.66 ± 0.38 | 2.93 ± 0.25 | 5.10 ± 0.30 | 1.20 ± 0.14 | 2.14 ± 0.21 |
| Freelance Job | 8.18 ± 0.96 | 4.77 ± 0.89 | 5.50 ± 0.89 | 5.07 ± 0.84 | 2.90 ± 0.61 | 3.66 ± 0.55 | 1.70 ± 0.37 | 1.85 ± 0.49 |
| Retired | 7.80 ± 0.35 | 6.80 ± 0.38 | 6.03 ± 0.35 | 5.59 ± 0.33 | 2.59 ± 0.18 | 3.96 ± 0.21 | 1.61 ± 0.13 | 2.04 ± 0.15 |
| Unemployed | 7.43 ± 0.65 | 5.13 ± 0.78 | 6.23 ± 0.70 | 5.41 ± 0.79 | 1.75 ± 0.33 | 3.66 ± 0.54 | 0.74 ± 0.08 | 1.68 ± 0.40 |
| p-value | 0.547 | 0.005 | 0.127 | 0.830 | 0.043 | 0.005 | 0.001 | 0.147 |
| Income (SR) | ||||||||
| <2000 | 7.20 ± 0.77 | 4.71 ± 0.87 | 5.79 ± 0.76 | 5.82 ± 0.94 | 2.10 ± 0.45 | 3.56 ± 0.60 | 0.82 ± 0.13 | 1.70 ± 0.41 |
| 2000–5000 | 7.01 ± 0.85 | 3.93 ± 0.86 | 5.54 ± 0.77 | 5.55 ± 0.87 | 2.14 ± 0.49 | 4.02 ± 0.60 | 1.52 ± 0.42 | 1.63 ± 0.33 |
| 5000–7000 | 10.2 ± 0.97 | 5.65 ± 1.24 | 4.30 ± 0.82 | 7.02 ± 1.02 | 1.80 ± 0.27 | 3.87 ± 0.66 | 1.10 ± 0.23 | 2.76 ± 0.62 |
| 7000–10,000 | 7.42 ± 0.68 | 6.31 ± 0.79 | 5.13 ± 0.71 | 5.81 ± 0.71 | 2.11 ± 0.39 | 3.66 ± 0.43 | 0.89 ± 0.14 | 1.44 ± 0.20 |
| >10,000 | 8.28 ± 0.29 | 6.28 ± 0.30 | 5.73 ± 0.27 | 5.36 ± 0.27 | 2.94 ± 0.17 | 4.65 ± 0.20 | 1.52 ± 0.11 | 2.16 ± 0.15 |
| p-value | 0.115 | 0.004 | 0.438 | 0.594 | 0.001 | 0.033 | 0.012 | 0.017 |
| BMI category 2 | ||||||||
| Underweight | 4.75 ± 0.75 | 5.88 ± 3.04 | 5.25 ± 2.98 | 5.13 ± 3.04 | 1.37 ± 0.37 | 4.75 ± 3.09 | 0.62 ± 0.23 | 1.50 ± 0.28 |
| Normal weight | 7.64 ± 0.53 | 5.76 ± 0.58 | 5.22 ± 0.48 | 5.30 ± 0.51 | 2.55 ± 0.29 | 3.71 ± 0.30 | 1.35 ± 0.12 | 1.72 ± 0.22 |
| Overweight | 7.69 ± 0.37 | 5.91 ± 0.38 | 5.88 ± 0.35 | 5.29 ± 0.36 | 2.67 ± 0.23 | 4.28 ± 0.25 | 1.57 ± 0.17 | 2.15 ± 0.20 |
| Obese | 8.83 ± 0.39 | 6.02 ± 0.43 | 5.44 ± 0.36 | 6.00 ± 0.38 | 2.70 ± 0.22 | 4.74 ± 0.29 | 1.17 ± 0.09 | 2.07 ± 0.19 |
| p-value | 0.094 | 0.929 | 0.657 | 0.356 | 0.873 | 0.371 | 0.487 | 0.636 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naaman, R.K. Nutrition Behavior and Physical Activity of Middle-Aged and Older Adults in Saudi Arabia. Nutrients 2022, 14, 3994. https://doi.org/10.3390/nu14193994
Naaman RK. Nutrition Behavior and Physical Activity of Middle-Aged and Older Adults in Saudi Arabia. Nutrients. 2022; 14(19):3994. https://doi.org/10.3390/nu14193994
Chicago/Turabian StyleNaaman, Rouba Khalil. 2022. "Nutrition Behavior and Physical Activity of Middle-Aged and Older Adults in Saudi Arabia" Nutrients 14, no. 19: 3994. https://doi.org/10.3390/nu14193994
APA StyleNaaman, R. K. (2022). Nutrition Behavior and Physical Activity of Middle-Aged and Older Adults in Saudi Arabia. Nutrients, 14(19), 3994. https://doi.org/10.3390/nu14193994