
Factors Associated with Food Insecurity in Latin America and the Caribbean Countries: A Cross-Sectional Analysis of 13 Countries


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
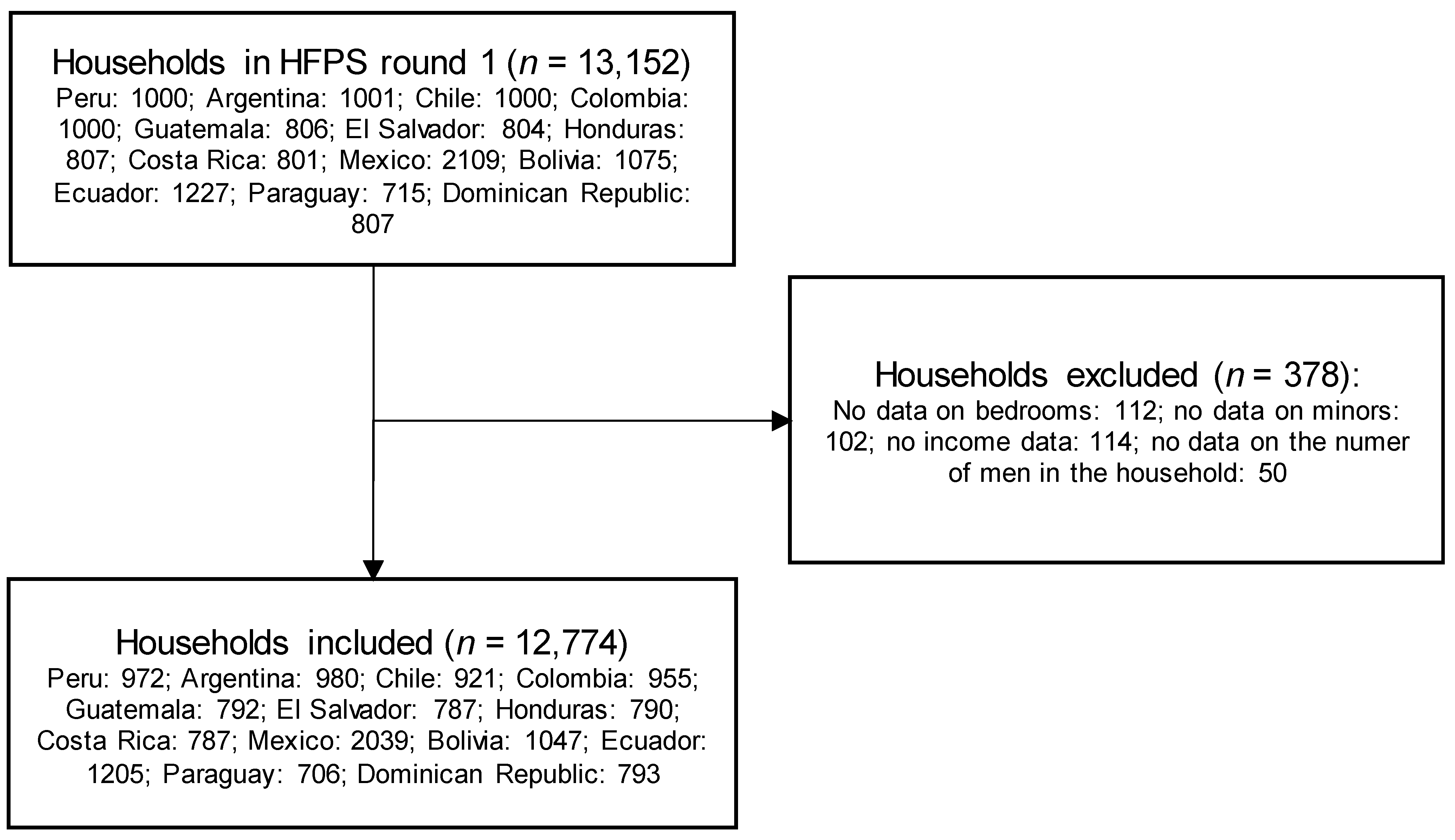
2.2. Setting and Participants
2.3. Measures
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Coleman-Jensen, A.; Rabbitt, M.P.; Gregory, C.A.; Singh, A. Household Food Security in the United States in 2020; U.S. Department of Agriculture, Economic Research Service: Washington, DC, USA, 2021.
- Arora, N.K.; Mishra, I. Current Scenario and Future Directions for Sustainable Development Goal 2: A Roadmap to Zero Hunger. Environ. Sustain. 2022, 5, 129–133. [Google Scholar] [CrossRef]
- FAO; IFAD; UNICEF; WFP; WHO. The State of Food Security and Nutrition in the World 2022; FAO: Rome, Italy, 2022; ISBN 978-92-5-136499-4. [Google Scholar]
- O’Meara, L.; Turner, C.; Coitinho, D.C.; Oenema, S. Consumer Experiences of Food Environments during the COVID-19 Pandemic: Global Insights from a Rapid Online Survey of Individuals from 119 Countries. Glob. Food Secur. 2022, 32, 100594. [Google Scholar] [CrossRef] [PubMed]
- The World Bank Food Security Update. Available online: https://www.worldbank.org/en/topic/agriculture/brief/food-security-update (accessed on 26 June 2022).
- United Nations. Policy Brief: The Impact of COVID-19 on Latin America and the Caribbean; United Nations Sustainable Development Group: New York, NY, USA, 2020. [Google Scholar]
- FAO; IFAD; UNICEF; WFP; WHO. The State of Food Security and Nutrition in the World 2020; FAO: Rome, Italy; IFAD: Rome, Italy; UNICEF: Rome, Italy; WFP: Rome, Italy; WHO: Rome, Italy, 2020; ISBN 978-92-5-132901-6. [Google Scholar]
- FAO; IFAD; UNICEF; WFP; WHO. The State of Food Security and Nutrition in the World 2021; FAO: Rome, Italy; IFAD: Rome, Italy; UNICEF: Rome, Italy; WFP: Rome, Italy; WHO: Rome, Italy, 2021; ISBN 978-92-5-134325-8. [Google Scholar]
- Benites-Zapata, V.A.; Urrunaga-Pastor, D.; Solorzano-Vargas, M.L.; Herrera-Añazco, P.; Uyen-Cateriano, A.; Bendezu-Quispe, G.; Toro-Huamanchumo, C.J.; Hernandez, A.V. Prevalence and Factors Associated with Food Insecurity in Latin America and the Caribbean during the First Wave of the COVID-19 Pandemic. Heliyon 2021, 7, e08091. [Google Scholar] [CrossRef]
- Das, S.; Rasul, M.G.; Hossain, M.S.; Khan, A.-R.; Alam, M.A.; Ahmed, T.; Clemens, J.D. Acute Food Insecurity and Short-Term Coping Strategies of Urban and Rural Households of Bangladesh during the Lockdown Period of COVID-19 Pandemic of 2020: Report of a Cross-Sectional Survey. BMJ Open 2020, 10, e043365. [Google Scholar] [CrossRef] [PubMed]
- Dondi, A.; Candela, E.; Morigi, F.; Lenzi, J.; Pierantoni, L.; Lanari, M. Parents’ Perception of Food Insecurity and of Its Effects on Their Children in Italy Six Months after the COVID-19 Pandemic Outbreak. Nutrients 2020, 13, 121. [Google Scholar] [CrossRef]
- Kent, K.; Murray, S.; Penrose, B.; Auckland, S.; Visentin, D.; Godrich, S.; Lester, E. Prevalence and Socio-Demographic Predictors of Food Insecurity in Australia during the COVID-19 Pandemic. Nutrients 2020, 12, 2682. [Google Scholar] [CrossRef]
- Niles, M.T.; Bertmann, F.; Belarmino, E.H.; Wentworth, T.; Biehl, E.; Neff, R. The Early Food Insecurity Impacts of COVID-19. Nutrients 2020, 12, 2096. [Google Scholar] [CrossRef]
- Inter-American Institute for Cooperation on Agriculture Frame of Reference. Family Farming in the Americas: Guiding Principles and Concepts of IICA’s Technical Cooperation; IICA: Turrialba, Costa Rica, 2017. [Google Scholar]
- Pawlak, K.; Kołodziejczak, M. The Role of Agriculture in Ensuring Food Security in Developing Countries: Considerations in the Context of the Problem of Sustainable Food Production. Sustainability 2020, 12, 5488. [Google Scholar] [CrossRef]
- FAO; FIDA; OPS; WFP; UNICEF. Panorama de la Seguridad Alimentaria y Nutricional en América Latina y el Caribe 2020; FAO: Rome, Italy; OPS: Rome, Italy; WFP: Rome, Italy; UNICEF: Rome, Italy, 2020; ISBN 978-92-5-133665-6. [Google Scholar]
- Gaudin, Y.; Pareyón Noguez, R. Brechas Estructurales En América Latina y El Caribe: Una Perspectiva Conceptual-Metodológica; CEPAL: Vitacura, Santiago de Chile, 2020. [Google Scholar]
- Hernández-Vásquez, A.; Visconti-Lopez, F.J.; Chacón-Torrico, H.; Azañedo, D. COVID-19 and Food Insecurity in Latin America and the Caribbean. J. Hunger. Environ. Nutr. 2022, 1–8. [Google Scholar] [CrossRef]
- Cañari-Casaño, J.L.; Cochachin-Henostroza, O.; Elorreaga, O.A.; Dolores-Maldonado, G.; Aquino-Ramírez, A.; Huaman-Gil, S.; Giribaldi-Sierralta, J.P.; Aparco, J.P.; Antiporta, D.A.; Penny, M.E. Social Predictors of Food Insecurity during the Stay-at-Home Order Due to the COVID-19 Pandemic in Peru. Results from a Cross-Sectional Web-Based Survey. Public Glob. Health 2021. preprint. [Google Scholar]
- Gaitán-Rossi, P.; Vilar-Compte, M.; Teruel, G.; Pérez-Escamilla, R. Food Insecurity Measurement and Prevalence Estimates during the COVID-19 Pandemic in a Repeated Cross-Sectional Survey in Mexico. Public Health Nutr. 2021, 24, 412–421. [Google Scholar] [CrossRef] [PubMed]
- Manfrinato, C.V.; Marino, A.; Condé, V.F.; Franco, M.d.C.P.; Stedefeldt, E.; Tomita, L.Y. High Prevalence of Food Insecurity, the Adverse Impact of COVID-19 in Brazilian Favela. Public Health Nutr. 2021, 24, 1210–1215. [Google Scholar] [CrossRef]
- Flores Cruz, R. COVID-19 High Frequency Phone Surveys in Latin America; World Bank: Washington, DC, USA, 2021. [Google Scholar]
- Mejía-Mantilla, C.; Oliveiri, S. COVID-19 in LAC. High Frequency Phone Surveys; Technical Note; World Bank: Washington, DC, USA, 2021. [Google Scholar]
- Food and Agriculture Organization of the United Nations Food Insecurity Experience Scale. Available online: https://www.fao.org/in-action/voices-of-the-hungry/fies/en/ (accessed on 26 June 2022).
- Agamile, P. COVID-19 Lockdown and Exposure of Households to Food Insecurity in Uganda: Insights from a National High Frequency Phone Survey. Eur. J. Dev. Res. 2022. [Google Scholar] [CrossRef]
- Dasgupta, S.; Robinson, E.J.Z. Impact of COVID-19 on Food Insecurity Using Multiple Waves of High Frequency Household Surveys. Sci. Rep. 2022, 12, 1865. [Google Scholar] [CrossRef]
- Tefera, S.A.; Tadesse, T.B.; Asmare, G.W. Prevalence of Household Food Insecurity in Ethiopia during the COVID-19 Pandemic: Evidence from Panel Data. Sci. Afr. 2022, 16, e01141. [Google Scholar] [CrossRef] [PubMed]
- Carle, A.C. Fitting Multilevel Models in Complex Survey Data with Design Weights: Recommendations. BMC Med. Res. Methodol. 2009, 9, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gujarati, D.N.; Porter, D.C. Basic Econometrics, 5th ed.; McGraw-Hill Irwin: Boston, MA, USA, 2009; ISBN 978-0-07-337577-9. [Google Scholar]
- Rivera, J.A.; Barquera, S.; González-Cossío, T.; Olaiz, G.; Sepúlveda, J. Nutrition Transition in Mexico and in Other Latin American Countries. Nutr. Rev. 2004, 62, S149–S157. [Google Scholar] [CrossRef]
- CEPAL. Cómo Evitar que la Crisis del COVID-19 se Transforme en una Crisis Alimentaria: Acciones Urgentes Contra el Hambre en América Latina y el Caribe; CEPAL: Vitacura, Santiago de Chile, 2020. [Google Scholar]
- Niles, M.T.; Beavers, A.W.; Clay, L.A.; Dougan, M.M.; Pignotti, G.A.; Rogus, S.; Savoie-Roskos, M.R.; Schattman, R.E.; Zack, R.M.; Acciai, F.; et al. A Multi-Site Analysis of the Prevalence of Food Insecurity in the United States, before and during the COVID-19 Pandemic. Curr. Dev. Nutr. 2021, 5, nzab135. [Google Scholar] [CrossRef]
- Kleve, S.; Bennett, C.J.; Davidson, Z.E.; Kellow, N.J.; McCaffrey, T.A.; O’Reilly, S.; Enticott, J.; Moran, L.J.; Harrison, C.L.; Teede, H.; et al. Food Insecurity Prevalence, Severity and Determinants in Australian Households during the COVID-19 Pandemic from the Perspective of Women. Nutrients 2021, 13, 4262. [Google Scholar] [CrossRef]
- Aguiar, A.; Maia, I.; Pinto, M.; Duarte, R. Food Insecurity in Portugal during the COVID-19 Pandemic: Prevalence and Associated Sociodemographic Characteristics. Port. J. Public Health 2022, 40, 35–42. [Google Scholar] [CrossRef]
- Shuvo, S.D.; Hossain, M.S.; Riazuddin, M.; Mazumdar, S.; Roy, D. Factors Influencing Low-Income Households’ Food Insecurity in Bangladesh during the COVID-19 Lockdown. PLoS ONE 2022, 17, e0267488. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, P.H.; Kachwaha, S.; Pant, A.; Tran, L.M.; Ghosh, S.; Sharma, P.K.; Shastri, V.D.; Escobar-Alegria, J.; Avula, R.; Menon, P. Impact of COVID-19 on Household Food Insecurity and Interlinkages with Child Feeding Practices and Coping Strategies in Uttar Pradesh, India: A Longitudinal Community-Based Study. BMJ Open 2021, 11, e048738. [Google Scholar] [CrossRef] [PubMed]
- Elsahoryi, N.; Al-Sayyed, H.; Odeh, M.; McGrattan, A.; Hammad, F. Effect of COVID-19 on Food Security: A Cross-Sectional Survey. Clin. Nutr. ESPEN 2020, 40, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Picchioni, F.; Goulao, L.F.; Roberfroid, D. The Impact of COVID-19 on Diet Quality, Food Security and Nutrition in Low and Middle Income Countries: A Systematic Review of the Evidence. Clin. Nutr. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Andrade, C. The Limitations of Online Surveys. Indian J. Psychol. Med. 2020, 42, 575–576. [Google Scholar] [CrossRef] [PubMed]
- Arndt, C.; Davies, R.; Gabriel, S.; Harris, L.; Makrelov, K.; Robinson, S.; Levy, S.; Simbanegavi, W.; van Seventer, D.; Anderson, L. COVID-19 Lockdowns, Income Distribution, and Food Security: An Analysis for South Africa. Glob. Food Secur. 2020, 26, 100410. [Google Scholar] [CrossRef]
- Paslakis, G.; Dimitropoulos, G.; Katzman, D.K. A Call to Action to Address COVID-19–Induced Global Food Insecurity to Prevent Hunger, Malnutrition, and Eating Pathology. Nutr. Rev. 2021, 79, 114–116. [Google Scholar] [CrossRef] [PubMed]
- de Cássia Ribeiro-Silva, R.; Pereira, M.; Campello, T.; Aragão, É.; de Medeiros Guimarães, J.M.; Ferreira, A.J.; Barreto, M.L.; dos Santos, S.M.C. Implicações Da Pandemia COVID-19 Para a Segurança Alimentar e Nutricional No Brasil. Ciênc. Saúde Coletiva 2020, 25, 3421–3430. [Google Scholar] [CrossRef]
- FAO; ECLAC. Food Systems and COVID-19 in Latin America and the Caribbean: Food Consumption Patterns and Malnutrition; CEPAL: Vitacura, Santiago de Chile, 2020. [Google Scholar]
- Aburto, T.C.; Pedraza, L.S.; Sánchez-Pimienta, T.G.; Batis, C.; Rivera, J.A. Discretionary Foods Have a High Contribution and Fruit, Vegetables, and Legumes Have a Low Contribution to the Total Energy Intake of the Mexican Population. J. Nutr. 2016, 146, 1881S–1887S. [Google Scholar] [CrossRef] [Green Version]
- Graziano da Silva, J.; Jales, M.; Rapallo, R.; Díaz-Bonilla, E.; Girardi, G.; del Grossi, M.; Luiselli, C.; Sotomayor, O.; Rodríguez, A.; Rodrigues, M. Food Systems in Latin America and the Caribbean: Challenges in a Post-Pandemic World; Food & Agriculture Organization: Rome, Italy, 2021; ISBN 92-5-134857-X. [Google Scholar]
- Kansiime, M.K.; Tambo, J.A.; Mugambi, I.; Bundi, M.; Kara, A.; Owuor, C. COVID-19 Implications on Household Income and Food Security in Kenya and Uganda: Findings from a Rapid Assessment. World Dev. 2021, 137, 105199. [Google Scholar] [CrossRef]
- Abay, K.A.; Berhane, G.; Hoddinott, J.; Tafere, K. COVID-19 and Food Security in Ethiopia: Do Social Protection Programs Protect? World Bank: Washington, DC, USA, 2020. [Google Scholar]
- Kesar, S.; Abraham, R.; Lahoti, R.; Nath, P.; Basole, A. Pandemic, Informality, and Vulnerability: Impact of COVID-19 on Livelihoods in India. Can. J. Dev. Stud. Rev. Can. D’études du Développement 2021, 42, 145–164. [Google Scholar] [CrossRef]
- de Brauw, A.; Hirvonen, K.; Abate, G.T. Food and Nutrition Security in Addis Ababa, Ethiopia during COVID-19 Pandemic: July 2020 Report; ESSP Working Paper 148; International Food Policy Research Institute: Washington, DC, USA, 2020. [Google Scholar]
- Harris, J.; Depenbusch, L.; Pal, A.A.; Nair, R.M.; Ramasamy, S. Food System Disruption: Initial Livelihood and Dietary Effects of COVID-19 on Vegetable Producers in India. Food Sec. 2020, 12, 841–851. [Google Scholar] [CrossRef] [PubMed]
- Abate, G.T.; de Brauw, A.; Hirvonen, K. Food and Nutrition Security in Addis Ababa, Ethiopia during COVID-19 Pandemic: June 2020 Report; ESSP Working Paper 145; International Food Policy Research Institute (IFPRI): Washington, DC, USA, 2020. [Google Scholar]
- Hirvonen, K.; Brauw, A.; Abate, G.T. Food Consumption and Food Security during the COVID-19 Pandemic in Addis Ababa. Am. J. Agric. Econ. 2021, 103, 772–789. [Google Scholar] [CrossRef] [PubMed]
- Mahmud, M.; Riley, E. Household Response to an Extreme Shock: Evidence on the Immediate Impact of the COVID-19 Lockdown on Economic Outcomes and Well-Being in Rural Uganda. World Dev. 2021, 140, 105318. [Google Scholar] [CrossRef]
- CEPAL. La Autonomía Económica de las Mujeres en la Recuperación Sostenible y con Igualdad; CEPAL: Vitacura, Santiago de Chile, 2021. [Google Scholar]
- Ghanbari Movahed, R.; Maleki Fard, F.; Gholamrezai, S.; Pakravan-Charvadeh, M.R. The Impact of COVID-19 Pandemic on Food Security and Food Diversity of Iranian Rural Households. Front. Public Health 2022, 10, 862043. [Google Scholar] [CrossRef] [PubMed]
- Kent, K.; Alston, L.; Murray, S.; Honeychurch, B.; Visentin, D. The Impact of the COVID-19 Pandemic on Rural Food Security in High Income Countries: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2022, 19, 3235. [Google Scholar] [CrossRef]
- Rodríguez-Ramírez, S.; Gaona-Pineda, E.B.; Martínez-Tapia, B.; Romero-Martínez, M.; Mundo-Rosas, V.; Shamah-Levy, T. Inseguridad Alimentaria y Percepción de Cambios en la Alimentación en Hogares Mexicanos Durante el Confinamiento Por la Pandemia de COVID-19. Salud Publica Mex. 2021, 63, 763–772. [Google Scholar] [CrossRef] [PubMed]
- Cejudo, G.M.; Michel, C.L.; de los Cobos, P. Policy Responses to the Pandemic for COVID-19 in Latin America and the Caribbean: The Use of Cash Transfer Programs and Social Protection Information Systems. In UNDP Latin America and the Caribbean COVID-19 Policy Document Series (24); UNDP: New York, NY, USA, 2020. [Google Scholar]
- Hox, J.J.; De Leeuw, E.D. A Comparison of Nonresponse in Mail, Telephone, and Face-to-Face Surveys: Applying Multilevel Modeling to Meta-Analysis. Qual. Quant. 1994, 28, 329–344. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics of the Household | All Countries | Peru | Argentina | Chile | Colombia | Guatemala | El Salvador | Honduras | Costa Rica | Mexico | Bolivia | Ecuador | Paraguay | Dominican Republic |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % | % | % | % | % | % | % | % | % | % | % | % | % | % | |
| Overall (n) | 12.774 | 972 | 980 | 921 | 955 | 792 | 787 | 790 | 787 | 2039 | 1047 | 1205 | 706 | 793 |
| Location of the household | ||||||||||||||
| Non-capital | 47.2 | 56.6 | 63.3 | 48.7 | 64.1 | 70.9 | 76.9 | 64 | 73.4 | 24.8 | 27.8 | 39.4 | 70.9 | 66.7 |
| Capital | 52.8 | 43.4 | 36.7 | 51.3 | 35.9 | 29.1 | 23.1 | 36 | 26.6 | 75.2 | 72.2 | 60.6 | 29.1 | 33.3 |
| Mean of bedrooms (SD) | 2.3 (1.0) | 2.3 (1.3) | 2.2 (0.6) | 2.6 (1.1) | 2.4 (0.7) | 2.4 (1.7) | 2.1 (1.9) | 2.3 (2.1) | 2.5 (1.9) | 2.3 (0.7) | 2.4 (2.1) | 2.2 (1.4) | 2.6 (2.3) | 2.3 (1.2) |
| Mean number of individuals aged between 5 and 18 years (SD) | 1.2 (1.3) | 1.3 (1.3) | 0.7 (0.9) | 0.9 (1.2) | 1.1 (0.8) | 1.7 (2.1) | 1.2 (2.1) | 1.6 (2.8) | 1.0 (2.4) | 1.2 (0.9) | 1.5 (2.3) | 1.1 (1.5) | 1.3 (2.6) | 1.2 (1.8) |
| Mean number of male individuals (SD) | 1.9 (1.2) | 2.2 (1.3) | 1.4 (0.8) | 1.7 (1.2) | 1.9 (0.8) | 2.3 (1.8) | 1.9 (1.9) | 2.1 (2.5) | 1.8 (2.4) | 1.9 (0.8) | 2.4 (2.4) | 2.1 (1.7) | 2.0 (2.4) | 1.9 (1.6) |
| Illness, accident, or death of an income-earning household member * | ||||||||||||||
| No | 96.8 | 95.5 | 98.5 | 95.5 | 97.0 | 96.0 | 95.2 | 95.8 | 97.9 | 97.1 | 97.9 | 93.8 | 97.3 | 95.0 |
| Yes | 3.2 | 4.5 | 1.5 | 4.5 | 3.0 | 4.0 | 4.8 | 4.2 | 2.1 | 2.9 | 2.1 | 6.2 | 2.7 | 5.0 |
| Health expenditure associated with COVID-19 or another illness * | ||||||||||||||
| No | 90.9 | 88.4 | 94.3 | 90.3 | 91.4 | 92.5 | 91.7 | 93.4 | 93.8 | 90.5 | 90.6 | 84.9 | 94.5 | 90.7 |
| Yes | 9.1 | 11.6 | 5.7 | 9.7 | 8.6 | 7.5 | 8.3 | 6.6 | 6.2 | 9.5 | 9.4 | 15.1 | 5.5 | 9.3 |
| Rising prices of food consumed in household * | ||||||||||||||
| No | 22.0 | 11.7 | 19.5 | 26.9 | 17.7 | 25.1 | 26.2 | 21.4 | 54.6 | 23.5 | 27.6 | 19.1 | 24.2 | 29.8 |
| Yes | 78.0 | 88.3 | 80.5 | 73.1 | 82.3 | 74.9 | 73.8 | 78.6 | 45.4 | 76.5 | 72.4 | 80.9 | 75.8 | 70.2 |
| Family income * | ||||||||||||||
| Increased | 3.4 | 1.0 | 9.2 | 5.1 | 3.3 | 3.3 | 2.8 | 2.7 | 2.5 | 1.5 | 4.0 | 1.2 | 2.9 | 7.3 |
| Remained equal | 33.5 | 16.8 | 49.6 | 39.1 | 24.6 | 25.3 | 28.0 | 28.2 | 33.8 | 37.7 | 24.6 | 24.7 | 31.6 | 32.6 |
| Reduced | 63.1 | 82.1 | 41.2 | 55.8 | 72.1 | 71.4 | 69.3 | 69.2 | 63.7 | 60.8 | 71.4 | 74.2 | 65.4 | 60.1 |
| Job loss by a household member * | ||||||||||||||
| No | 57.4 | 27.1 | 78.0 | 59.4 | 39.2 | 48.2 | 46.1 | 49.6 | 57.3 | 64.1 | 59.8 | 63.0 | 59.3 | 65.2 |
| Yes | 42.6 | 72.9 | 22.0 | 40.6 | 60.8 | 51.8 | 53.9 | 50.4 | 42.7 | 35.9 | 40.2 | 37.0 | 40.7 | 34.8 |
| Household member received cash, a check, or transfer ** | ||||||||||||||
| No | 90.5 | 84.9 | 90.1 | 91.6 | 88.3 | 96.7 | 72.3 | 98.0 | 85.4 | 96.0 | 62.8 | 95.5 | 70.8 | 90.5 |
| Yes | 9.5 | 15.1 | 9.9 | 8.4 | 11.7 | 3.3 | 27.1 | 2.0 | 14.6 | 4.0 | 37.2 | 4.5 | 29.2 | 9.5 |
| Question(s) | All Countries% (95% CI) |
|---|---|
| Q1 | 32.7 (31.4–34.0) |
| Q2 | 24.3 (23.1–25.5) |
| Q3 | 27.8 (26.6–29.0) |
| Q4 | 10.3 (9.5–11.2) |
| Q1 and Q2 | 21.1 (19.9–22.2) |
| Q1 and Q3 | 22.7 (21.6–23.9) |
| Q1 and Q4 | 9.3 (8.5–10.2) |
| Q2 and Q3 | 20.1 (19.0–21.2) |
| Q2 and Q4 | 8.8 (8.1–9.7) |
| Q3 and Q4 | 9.1 (8.4–10.0) |
| Q1 and Q2 and Q3 | 18.0 (17.0–19.1) |
| Q2 and Q3 and Q4 | 8.1 (7.4–8.9) |
| Q1 and Q2 and Q4 | 8.4 (7.6–9.2) |
| Q1 and Q3 and Q4 | 8.5 (7.7–9.3) |
| Q1 and Q2 and Q3 and Q4 | 7.8 (7.1–8.6) |
| Q1 or Q2 or Q3 or Q4 | 39.2 (37.9–40.6) |
| Bivariate Model | Adjusted Model 1 | Adjusted Model 2 | ||||
|---|---|---|---|---|---|---|
| Variable | PR (95% CI) | p-Value | aPR (95% CI) | p-Value | aPR (95% CI) | p-Value |
| Location of the household | ||||||
| Non-capital | Ref. | Ref. | Ref. | |||
| Capital | 0.75 (0.69–0.80) | <0.001 | 0.82 (0.77–0.86) | <0.001 | 0.82 (0.77–0.86) | <0.001 |
| Number of rooms | 0.84 (0.80–0.89) | <0.001 | 0.84 (0.81–0.87) | <0.001 | 0.84 (0.81–0.87) | <0.001 |
| Number of individuals aged 5 to 18 years | 1.12 (1.09–1.15) | <0.001 | 1.07 (1.05–1.10) | <0.001 | 1.07 (1.06–1.10) | <0.001 |
| Number of individual men | 1.07 (1.05–1.09) | <0.001 | 1.04 (1.03–1.05) | <0.001 | 1.04 (1.03–1.05) | <0.001 |
| Illness, accident, or death of an income-earning household member* | ||||||
| No | Ref. | Ref. | Ref. | |||
| Yes | 1.38 (1.22–1.57) | <0.001 | 1.13 (1.02–1.25) | 0.022 | 1.13 (1.03–1.25) | 0.025 |
| Health expenditure associated with COVID-19 or another illness * | ||||||
| No | Ref. | Ref. | Ref. | |||
| Yes | 1.38 (1.27–1.49) | <0.001 | 1.21 (1.12–1.30) | <0.001 | 1.21 (1.12–1.30) | <0.001 |
| Rising prices of food consumed in household * | ||||||
| No | Ref. | Ref. | Ref. | |||
| Yes | 1.98 (1.75–2.24) | <0.001 | 1.54 (1.38–1.71) | <0.001 | 1.54 (1.38–1.71) | <0.001 |
| Family income e * | ||||||
| Increased | Ref. | Ref. | Ref. | |||
| Remained equal | 0.79 (0.63–0.99) | 0.041 | 0.89 (0.73–1.09) | 0.273 | 0.90 (0.74–1.10) | 0.308 |
| Reduced | 1.53 (1.23–1.89) | <0.001 | 1.27 (1.03–1.55) | 0.023 | 1.27 (1.03–1.56) | 0.022 |
| Job loss by a household member * | ||||||
| No | Ref. | Ref. | Ref. | |||
| Yes | 2.16 (1.92–2.43) | <0.001 | 1.71 (1.57–1.86) | <0.001 | 1.75 (1.59–1.93) | <0.001 |
| Household member received cash, a check, or transfer ¶ | ||||||
| No | Ref. | Ref. | Ref. | |||
| Yes | 1.14 (0.99–1.31) | 0.073 | 1.03 (0.91–1.16) | 0.640 | 1.16 (0.96–1.40) | 0.127 |
| Job loss # Transfers | ||||||
| Yes # Yes | 0.84 (0.71–0.99) | 0.043 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Vásquez, A.; Visconti-Lopez, F.J.; Vargas-Fernández, R. Factors Associated with Food Insecurity in Latin America and the Caribbean Countries: A Cross-Sectional Analysis of 13 Countries. Nutrients 2022, 14, 3190. https://doi.org/10.3390/nu14153190
Hernández-Vásquez A, Visconti-Lopez FJ, Vargas-Fernández R. Factors Associated with Food Insecurity in Latin America and the Caribbean Countries: A Cross-Sectional Analysis of 13 Countries. Nutrients. 2022; 14(15):3190. https://doi.org/10.3390/nu14153190
Chicago/Turabian StyleHernández-Vásquez, Akram, Fabriccio J. Visconti-Lopez, and Rodrigo Vargas-Fernández. 2022. "Factors Associated with Food Insecurity in Latin America and the Caribbean Countries: A Cross-Sectional Analysis of 13 Countries" Nutrients 14, no. 15: 3190. https://doi.org/10.3390/nu14153190
APA StyleHernández-Vásquez, A., Visconti-Lopez, F. J., & Vargas-Fernández, R. (2022). Factors Associated with Food Insecurity in Latin America and the Caribbean Countries: A Cross-Sectional Analysis of 13 Countries. Nutrients, 14(15), 3190. https://doi.org/10.3390/nu14153190