
A Combination of Lactoplantibacillus plantarum Strains CECT7527, CECT7528, and CECT7529 Plus Monacolin K Reduces Blood Cholesterol: Results from a Randomized, Double-Blind, Placebo-Controlled Study

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
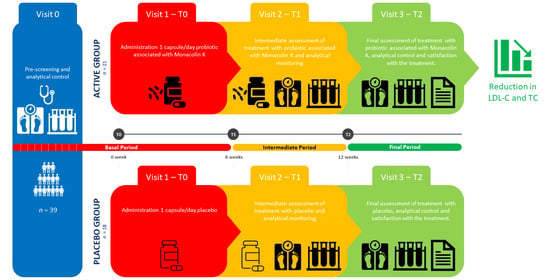
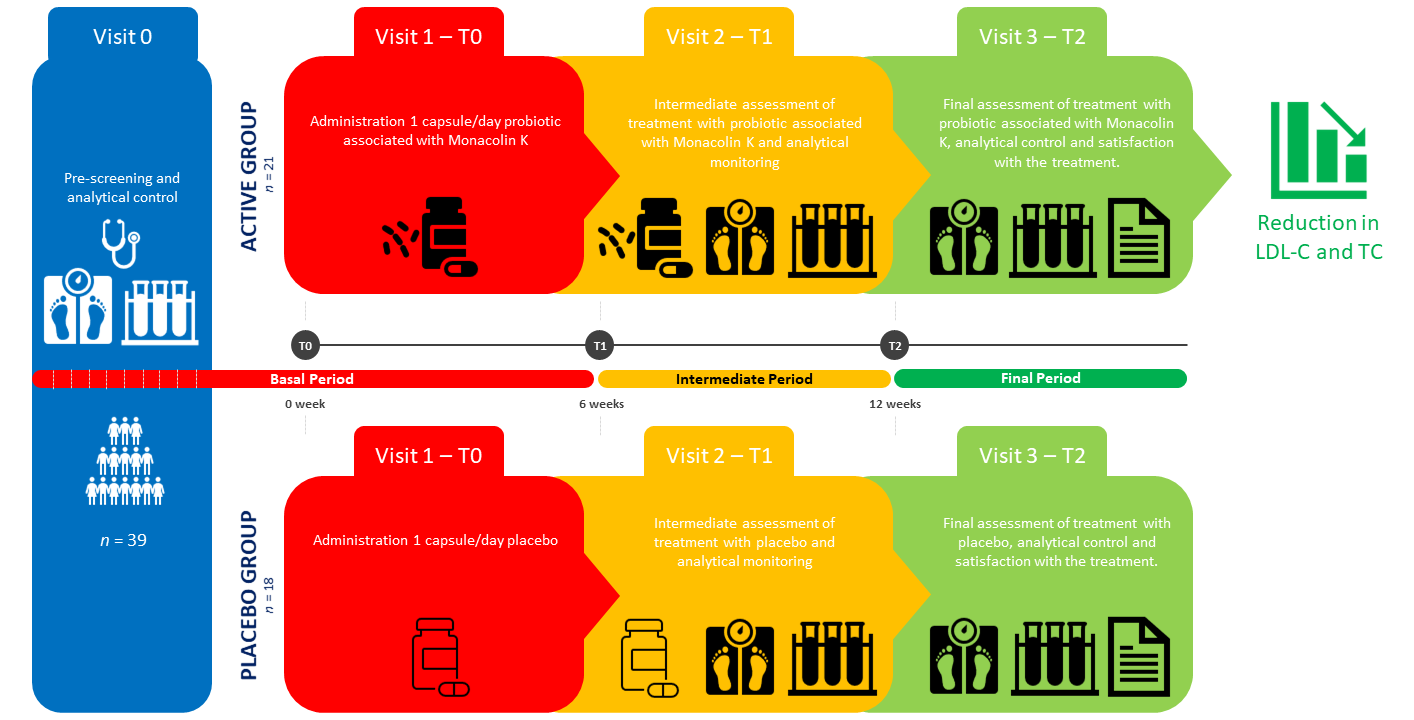
2.1. Study Design and Ethics
2.2. Study Procedures
2.3. Study Products
2.4. Study Population and Sample Size
2.5. Study Outcomes
2.6. Statistical Analyses
3. Results
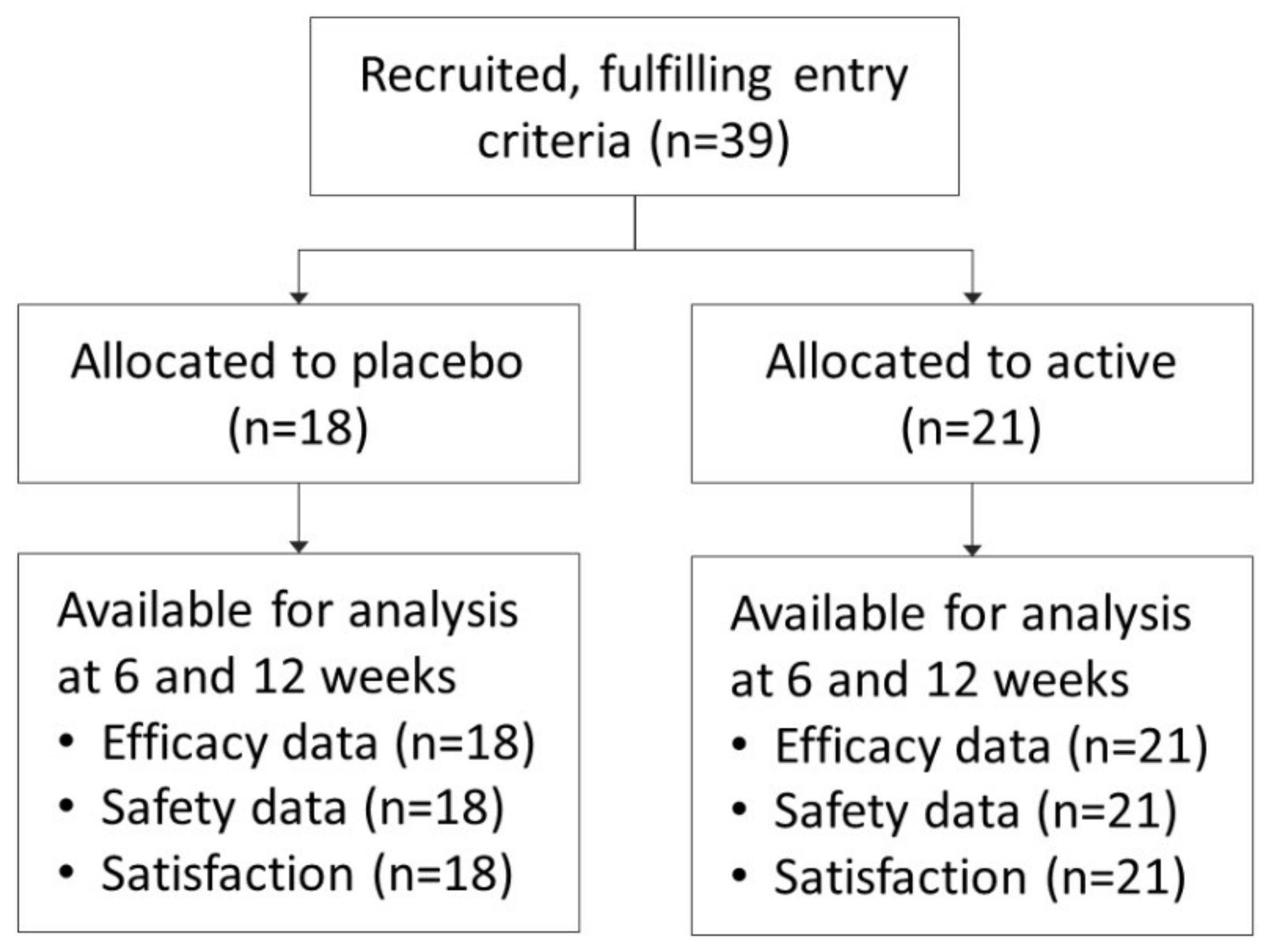
3.1. Study Sample
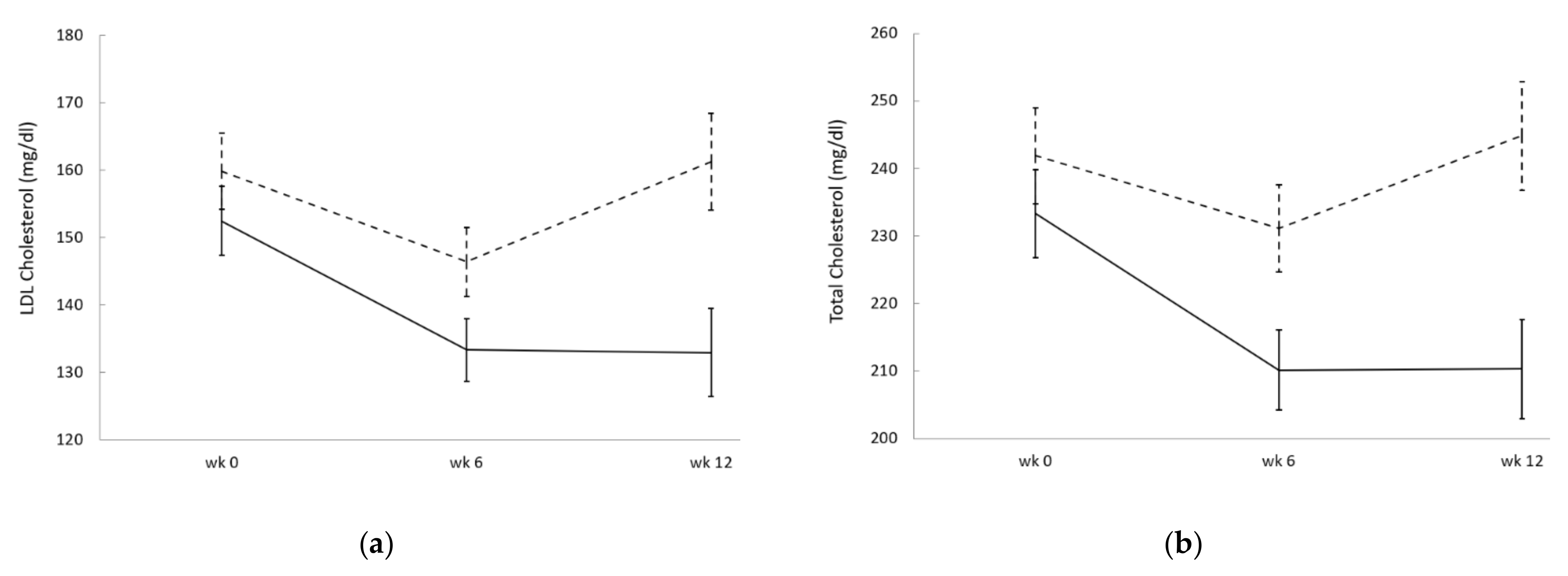
3.2. Efficacy
3.3. Safety and Product Satisfaction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Media Centre: Cardiovascular Diseases. Available online: https://www.who.int/nmh/publications/fact_sheet_cardiovascular_en.pdf (accessed on 6 March 2021).
- Ference, B.A.; Ginsberg, H.N.; Graham, I.; Ray, K.K.; Packard, C.J.; Bruckert, E.; Hegele, R.A.; Krauss, R.M.; Raal, F.J.; Schunkert, H.; et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur. Heart J. 2017, 38, 2459–2472. [Google Scholar] [CrossRef]
- Silverman, M.G.; Ference, B.A.; Im, K.; Wiviott, S.D.; Giugliano, R.P.; Grundy, S.M.; Braunwald, E.; Sabatine, M.S. Association Between Lowering LDL-C and Cardiovascular Risk Reduction Among Different Therapeutic Interventions: A Systematic Review and Meta-analysis. JAMA 2016, 316, 1289–1297. [Google Scholar] [CrossRef]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll Cardiol. 2019, 73, e285–e350. [Google Scholar] [CrossRef] [PubMed]
- Mach, F.; Baigent, C.; Catapano, A.; Koskinas, K.; Casula, M.; Badimon, L.; Chapman, M.; De Backer, G.; Delgado, V.; Ference, B.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur. Heart J. 2019, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Mills, E.J.; Rachlis, B.; Wu, P.; Devereaux, P.J.; Arora, P.; Perri, D. Primary prevention of cardiovascular mortality and events with statin treatments: A network meta-analysis involving more than 65,000 patients. J. Am. Coll Cardiol. 2008, 52, 1769–1781. [Google Scholar] [CrossRef] [PubMed]
- Yebyo, H.G.; Aschmann, H.E.; Puhan, M.A. Finding the Balance Between Benefits and Harms When Using Statins for Primary Prevention of Cardiovascular Disease: A Modeling Study. Ann. Intern. Med. 2019, 170, 1–10. [Google Scholar] [CrossRef]
- Nissen, S.E.; Stroes, E.; Dent-Acosta, R.E.; Rosenson, R.S.; Lehman, S.J.; Sattar, N.; Preiss, D.; Bruckert, E.; Ceska, R.; Lepor, N.; et al. Efficacy and Tolerability of Evolocumab vs Ezetimibe in Patients With Muscle-Related Statin Intolerance: The GAUSS-3 Randomized Clinical Trial. JAMA 2016, 315, 1580–1590. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Plutzky, J.; Skentzos, S.; Morrison, F.; Mar, P.; Shubina, M.; Turchin, A. Discontinuation of statins in routine care settings: A cohort study. Ann. Intern. Med. 2013, 158, 526–534. [Google Scholar] [CrossRef]
- Yebyo, H.G.; Aschmann, H.E.; Kaufmann, M.; Puhan, M.A. Comparative effectiveness and safety of statins as a class and of specific statins for primary prevention of cardiovascular disease: A systematic review, meta-analysis, and network meta-analysis of randomized trials with 94,283 participants. Am. Heart J. 2019, 210, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Cai, R.; Yuan, Y.; Sun, J.; Xia, W.; Huang, R.; Tian, S.; Dong, X.; Shen, Y.; Wang, S. Statins worsen glycemic control of T2DM in target LDL-c level and LDL-c reduction dependent manners: A meta-analysis. Expert Opin. Pharmacother. 2016, 17, 1839–1849. [Google Scholar] [CrossRef]
- Saeed, K.M.I. Prevalence of Risk Factors for Non-Communicable Diseases in the Adult Population of Urban Areas in Kabul City, Afghanistan. Cent. Asian J. Glob. Health 2013, 2, 69. [Google Scholar] [CrossRef]
- Zhang, H.; Plutzky, J.; Shubina, M.; Turchin, A. Continued Statin Prescriptions After Adverse Reactions and Patient Outcomes: A Cohort Study. Ann. Intern. Med. 2017, 167, 221–227. [Google Scholar] [CrossRef]
- Ward, N.C.; Pang, J.; Ryan, J.D.M.; Watts, G.F. Nutraceuticals in the management of patients with statin-associated muscle symptoms, with a note on real-world experience. Clin. Cardiol. 2018, 41, 159–165. [Google Scholar] [CrossRef]
- Bianconi, V.; Mannarino, M.R.; Sahebkar, A.; Cosentino, T.; Pirro, M. Cholesterol-Lowering Nutraceuticals Affecting Vascular Function and Cardiovascular Disease Risk. Curr. Cardiol. Rep. 2018, 20, 53. [Google Scholar] [CrossRef]
- Le Roy, T.; Lecuyer, E.; Chassaing, B.; Rhimi, M.; Lhomme, M.; Boudebbouze, S.; Ichou, F.; Haro Barcelo, J.; Huby, T.; Guerin, M.; et al. The intestinal microbiota regulates host cholesterol homeostasis. BMC Biol. 2019, 17, 94. [Google Scholar] [CrossRef]
- Molinero, N.; Ruiz, L.; Sanchez, B.; Margolles, A.; Delgado, S. Intestinal Bacteria Interplay With Bile and Cholesterol Metabolism: Implications on Host Physiology. Front. Physiol. 2019, 10, 185. [Google Scholar] [CrossRef]
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Zhang, Q.; Ren, Y.; Ruan, Z. Effect of probiotic Lactobacillus on lipid profile: A systematic review and meta-analysis of randomized, controlled trials. PLoS ONE 2017, 12, e0178868. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Wittouck, S.; Salvetti, E.; Franz, C.; Harris, H.M.B.; Mattarelli, P.; O’Toole, P.W.; Pot, B.; Vandamme, P.; Walter, J.; et al. A taxonomic note on the genus Lactobacillus: Description of 23 novel genera, emended description of the genus Lactobacillus Beijerinck 1901, and union of Lactobacillaceae and Leuconostocaceae. Int. J. Syst. Evol. Microbiol. 2020, 70, 2782–2858. [Google Scholar] [CrossRef] [PubMed]
- Ruscica, M.; Pavanello, C.; Gandini, S.; Macchi, C.; Botta, M.; Dall’Orto, D.; Del Puppo, M.; Bertolotti, M.; Bosisio, R.; Mombelli, G.; et al. Nutraceutical approach for the management of cardiovascular risk—A combination containing the probiotic Bifidobacterium longum BB536 and red yeast rice extract: Results from a randomized, double-blind, placebo-controlled study. Nutr. J. 2019, 18, 13. [Google Scholar] [CrossRef]
- Mazza, A.; Schiavon, L.; Rigatelli, G.; Torin, G.; Montanaro, F.; Lenti, S. The short-term supplementation of monacolin K improves the lipid and metabolic patterns of hypertensive and hypercholesterolemic subjects at low cardiovascular risk. Food Funct. 2018, 9, 3845–3852. [Google Scholar] [CrossRef] [PubMed]
- Derosa, G.; D’Angelo, A.; Maffioli, P. Coenzyme q10 liquid supplementation in dyslipidemic subjects with statin-related clinical symptoms: A double-blind, randomized, placebo-controlled study. Drug Des. Dev. Ther. 2019, 13, 3647–3655. [Google Scholar] [CrossRef]
- Fuentes, M.C.; Lajo, T.; Carrion, J.M.; Cune, J. Cholesterol-lowering efficacy of Lactobacillus plantarum CECT 7527, 7528 and 7529 in hypercholesterolaemic adults. Br. J. Nutr. 2013, 109, 1866–1872. [Google Scholar] [CrossRef] [PubMed]
- Seong, S.J.; Ohk, B.; Kang, W.Y.; Gwon, M.R.; Kim, B.K.; Cho, S.; Yang, D.H.; Lee, H.W.; Yoon, Y.R. Pharmacokinetic Drug Interactions Between Amlodipine, Valsartan, and Rosuvastatin in Healthy Volunteers. Adv. Ther. 2019, 36, 1642–1656. [Google Scholar] [CrossRef] [PubMed]
- Gude, D. Angiotensin-converting enzyme inhibitors in lipid metabolism and atherosclerosis: An ace up the sleeve? J. Sci. Soc. 2014, 41, 59–60. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Committee for Medicinal Products for Human Use. Guideline on Adjustment for Baseline Covariates in Clinical Trials; Technical report, EMA/CHMP/295050/2013; European Medicines Agency: London, UK, 2015. [Google Scholar]
- Guardia Serecigni, J.; Jiménez Arriero, M.; Pascual Pastor, F.; Flórez Menéndez, G.; Contel Guillamón, M. Guías Clinicas SOCIDROGALCOHOL Basadas en la EVIDENCIA CIENTÍFICA, 2nd ed.; Socidrogalcohol, Ed.; Socidrogalcohol: Valencia, Spain, 2008; p. 165. [Google Scholar]
- Fuentes, M.C.; Lajo, T.; Carrión, J.M.; Cuñé, J. A randomized clinical trial evaluating a proprietary mixture of Lactobacillus plantarum strains for lowering cholesterol. Mediterranean J. Nutr. Metab. 2016, 9, 125–135. [Google Scholar] [CrossRef]
- Bosch, M.; Fuentes, M.C.; Audivert, S.; Bonachera, M.A.; Peiro, S.; Cune, J. Lactobacillus plantarum CECT 7527, 7528 and 7529: Probiotic candidates to reduce cholesterol levels. J. Sci. Food Agric. 2014, 94, 803–809. [Google Scholar] [CrossRef]
- Mukerji, P.; Roper, J.M.; Stahl, B.; Smith, A.B.; Burns, F.; Rae, J.C.; Yeung, N.; Lyra, A.; Svard, L.; Saarinen, M.T.; et al. Safety evaluation of AB-LIFE((R)) (Lactobacillus plantarum CECT 7527, 7528 and 7529): Antibiotic resistance and 90-day repeated-dose study in rats. Food Chem. Toxicol. 2016, 92, 117–128. [Google Scholar] [CrossRef]
- Endo, A. The discovery and development of HMG-CoA reductase inhibitors. J. Lipid Res. 1992, 33, 1569–1582. [Google Scholar] [CrossRef]
- Gerards, M.C.; Terlou, R.J.; Yu, H.; Koks, C.H.; Gerdes, V.E. Traditional Chinese lipid-lowering agent red yeast rice results in significant LDL reduction but safety is uncertain—A systematic review and meta-analysis. Atherosclerosis 2015, 240, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zhang, J.; Shi, Y.; Grimsgaard, S.; Alraek, T.; Fonnebo, V. Chinese red yeast rice (Monascus purpureus) for primary hyperlipidemia: A meta-analysis of randomized controlled trials. Chin. Med. 2006, 1, 4. [Google Scholar] [CrossRef] [PubMed]
- Dujovne, C.A. Red Yeast Rice Preparations: Are They Suitable Substitutions for Statins? Am. J. Med. 2017, 130, 1148–1150. [Google Scholar] [CrossRef] [PubMed]
- Fogacci, F.; Banach, M.; Mikhailidis, D.P.; Bruckert, E.; Toth, P.P.; Watts, G.F.; Reiner, Z.; Mancini, J.; Rizzo, M.; Mitchenko, O.; et al. Safety of red yeast rice supplementation: A systematic review and meta-analysis of randomized controlled trials. Pharmacol. Res. 2019, 143, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Xiao, L.; Pan, G. An important intestinal transporter that regulates the enterohepatic circulation of bile acids and cholesterol homeostasis: The apical sodium-dependent bile acid transporter (SLC10A2/ASBT). Clin. Res. Hepatol. Gastroenterol. 2017, 41, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Joyce, S.A.; MacSharry, J.; Casey, P.G.; Kinsella, M.; Murphy, E.F.; Shanahan, F.; Hill, C.; Gahan, C.G. Regulation of host weight gain and lipid metabolism by bacterial bile acid modification in the gut. Proc. Natl. Acad. Sci. USA 2014, 111, 7421–7426. [Google Scholar] [CrossRef] [PubMed]
- Long, S.L.; Gahan, C.G.M.; Joyce, S.A. Interactions between gut bacteria and bile in health and disease. Mol. Aspects Med. 2017, 56, 54–65. [Google Scholar] [CrossRef]
- Espadaler, J.; Audivert, S.; Navarro-Tapia, E.; Buj, D. Demographic and Clinical Charactersitics Influencing the Effects of a Cholesterol-Lowering Probiotic. In Proceedings of the 10th Workshop on Probiotics and Prebiotics, Las Palmas de Gran Canaria, Spain, 6–8 February 2019; p. 6. [Google Scholar]
- Kullisaar, T.; Zilmer, K.; Salum, T.; Rehema, A.; Zilmer, M. The use of probiotic L. fermentum ME-3 containing Reg’Activ Cholesterol supplement for 4 weeks has a positive influence on blood lipoprotein profiles and inflammatory cytokines: An open-label preliminary study. Nutr. J. 2016, 15, 93. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Wang, Z. Treatment satisfaction with different weight loss methods among respondents with obesity. Clin. Obes. 2016, 6, 161–170. [Google Scholar] [CrossRef]
- Calugi, S.; Marchesini, G.; El Ghoch, M.; Gavasso, I.; Dalle Grave, R. The association between weight maintenance and session-by-session diet adherence, weight loss and weight-loss satisfaction. Eat. Weight Disord. 2020, 25, 127–133. [Google Scholar] [CrossRef]
- Talbert, R.L. New therapeutic options in the National Cholesterol Education Program Adult Treatment Panel III. Am. J. Manag. Care 2002, 8, S301–S307. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Total Sample (n = 39) | Placebo (n = 18) | Active (n = 21) | ||||
|---|---|---|---|---|---|---|
| Age (mean and SD) | 51.9 | (±11.8) | 48.8 | (±12.2) | 54.5 | (±9.0) |
| Sex (female, %) | 14 | (35.9%) | 5 | (27.8%) | 9 | (42.9%) |
| TC (mean and SD) | 237.3 | (±28.9) | 232.7 | (±32.9) | 241.1 | (±25.3) |
| LDL-C (mean and SD) | 155.9 | (±22.4) | 153.3 | (±28.0) | 158.1 | (±16.6) |
| HDL-C (mean and SD) | 55.5 | (±14.1) | 59.2 | (±18.6) | 52.4 | (±7.9) |
| TG (mean and SD) | 143 | (±67.7) | 122.2 | (±37.4) | 160.9 | (±82.5) |
| Glycemia (mean and SD) | 92.6 | (±12.7) | 95.8 | (±10.0) | 89.8 | (±14.3) |
| Hemoglobin (mean and SD) | 15.6 | (±1.1) | 15.8 | (±1.1) | 15.5 | (±1.2) |
| Waist perimeter (mean and SD) | 96.9 | (±11.1) | 95.9 | (±13.4) | 97.7 | (±8.9) |
| Body Mass Index (mean and SD) | 27.1 | (±4.1) | 26.6 | (±4.5) | 27.5 | (±3.8) |
| Body Fat (%) (mean and SD) | 27.8 | (±6.2) | 26.0 | (±4.4) | 29.3 | (±7.2) |
| Smoking habit (yes, %) | 14 | (35.9%) | 5 | (27.8%) | 9 | (42.9%) |
| Alcohol consumption 1 (yes, %) | 25 | (64.1%) | 11 | (61.1%) | 14 | (66.7%) |
| Antihypertensive treatment (yes, %) | 1 | (2.6%) | 1 | (5.6%) | 0 | (0.0%) |
| Recent hypercholesterolemia treatment (yes, %) | 21 | (53.8%) | 4 | (22.2%) | 17 | (81.0%) |
| Family history of hypercholesterolemia (yes, %) | 13 | (33.3%) | 6 | (66.7%) | 7 | (66.7%) |
| Placebo (n = 18) | Active (n = 21) | |||||
|---|---|---|---|---|---|---|
| Mean | SEM | p-Value | Mean | SEM | p-Value | |
| TC (mg/dL), week 6 | −13.4 | 6.4 | 0.766 | −20.9 | 5.7 | 0.007 |
| TC (mg/dL), week 12 | −2.8 | 9.4 | −18.0 | 6.0 | ||
| LDL-C (mg/dL), week 6 | −17.1 | 5.8 | 0.571 | −16.0 | 5.0 | 0.008 |
| LDL-C (mg/dL), week 12 | −3.6 | 6.2 | −15.3 | 5.2 | ||
| HDL-C (mg/dL), week 6 | −1.2 | 1.3 | 0.847 | 0.1 | 1.4 | 0.004 |
| HDL-C (mg/dL), week 12 | 0.4 | 2.0 | 3.1 | 1.0 | ||
| TG (mg/dL), week 6 | 3.3 | 10.1 | 0.370 | −32.4 | 15.1 | 0.015 |
| TG (mg/dL), week 12 | 10.7 | 11.6 | −30.3 | 11.4 | ||
| Body weight (kg), week 12 | −0.4 | 0.4 | 0.249 | −1.4 | 0.4 | <0.001 |
| BMI (kg/m2), week 12 | −0.2 | 0.1 | 0.215 | −0.5 | 0.1 | 0.001 |
| Body Fat (%), week 12 | −0.8 | 0.4 | 0.061 | −1.3 | 0.4 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guerrero-Bonmatty, R.; Gil-Fernández, G.; Rodríguez-Velasco, F.J.; Espadaler-Mazo, J. A Combination of Lactoplantibacillus plantarum Strains CECT7527, CECT7528, and CECT7529 Plus Monacolin K Reduces Blood Cholesterol: Results from a Randomized, Double-Blind, Placebo-Controlled Study. Nutrients 2021, 13, 1206. https://doi.org/10.3390/nu13041206
Guerrero-Bonmatty R, Gil-Fernández G, Rodríguez-Velasco FJ, Espadaler-Mazo J. A Combination of Lactoplantibacillus plantarum Strains CECT7527, CECT7528, and CECT7529 Plus Monacolin K Reduces Blood Cholesterol: Results from a Randomized, Double-Blind, Placebo-Controlled Study. Nutrients. 2021; 13(4):1206. https://doi.org/10.3390/nu13041206
Chicago/Turabian StyleGuerrero-Bonmatty, Rafael, Guadalupe Gil-Fernández, Francisco José Rodríguez-Velasco, and Jordi Espadaler-Mazo. 2021. "A Combination of Lactoplantibacillus plantarum Strains CECT7527, CECT7528, and CECT7529 Plus Monacolin K Reduces Blood Cholesterol: Results from a Randomized, Double-Blind, Placebo-Controlled Study" Nutrients 13, no. 4: 1206. https://doi.org/10.3390/nu13041206
APA StyleGuerrero-Bonmatty, R., Gil-Fernández, G., Rodríguez-Velasco, F. J., & Espadaler-Mazo, J. (2021). A Combination of Lactoplantibacillus plantarum Strains CECT7527, CECT7528, and CECT7529 Plus Monacolin K Reduces Blood Cholesterol: Results from a Randomized, Double-Blind, Placebo-Controlled Study. Nutrients, 13(4), 1206. https://doi.org/10.3390/nu13041206