
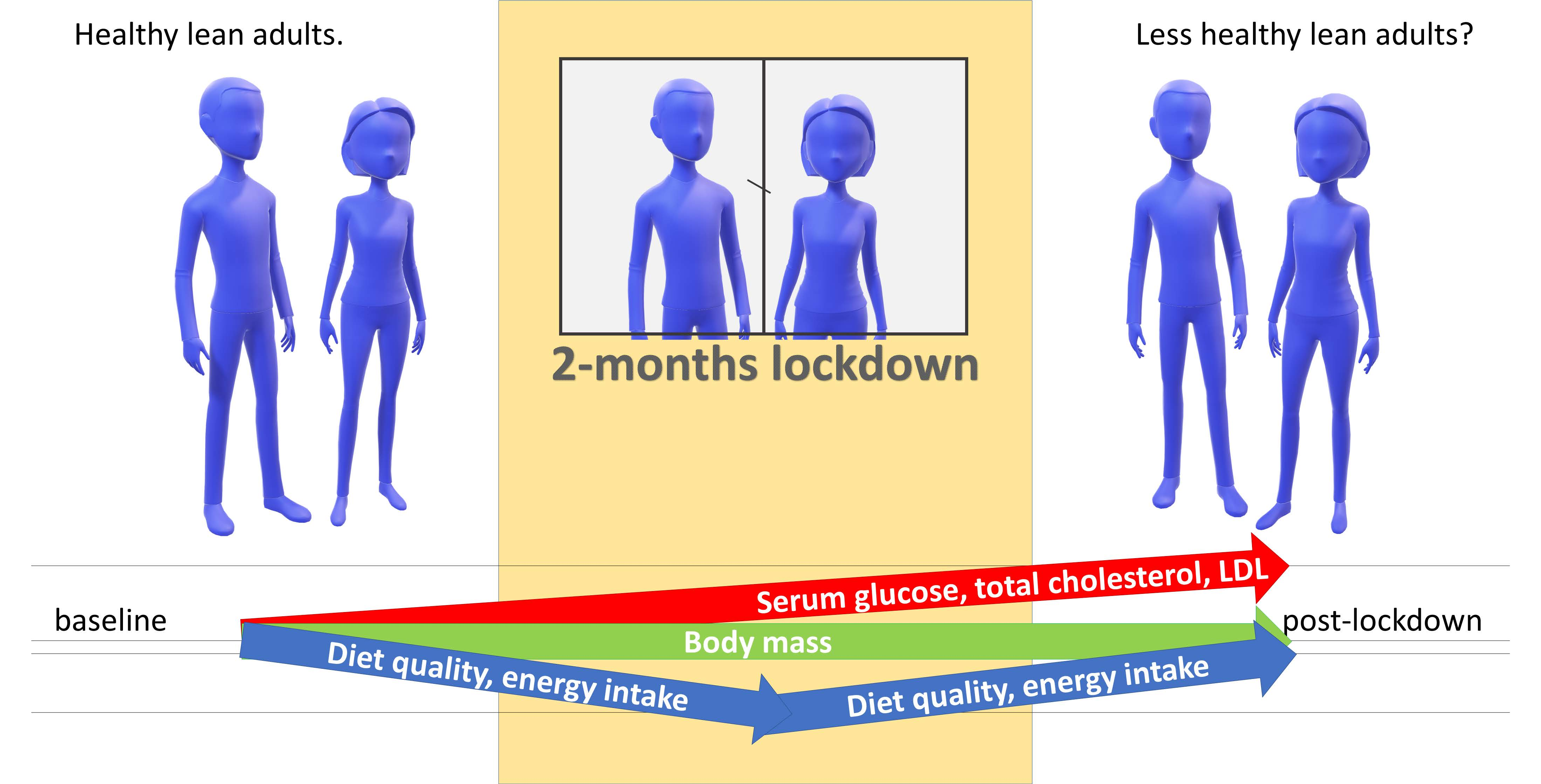
The Impact of COVID-19-Related Lockdown on Diet and Serum Markers in Healthy Adults

 , ,
, , 
Abstract

1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Subjects
2.3. Dietary Assessment
2.4. Lifestyle and Socio-Economic Questionnaire
2.5. Physical Activity Questionnaire
2.6. Anthropometric Measurements
2.7. Serum Markers
2.8. Statistical Analysis
3. Results
3.1. Subjects’ Baseline Characteristics
3.2. Lifestyle and Socio-Economic Changes during Lockdown
3.3. Changes in Nutrition and Physical Activity during and Post-Lockdown
3.4. Anthropometric Characteristics
3.5. Significant Changes in Serum Markers Post-Lockdown
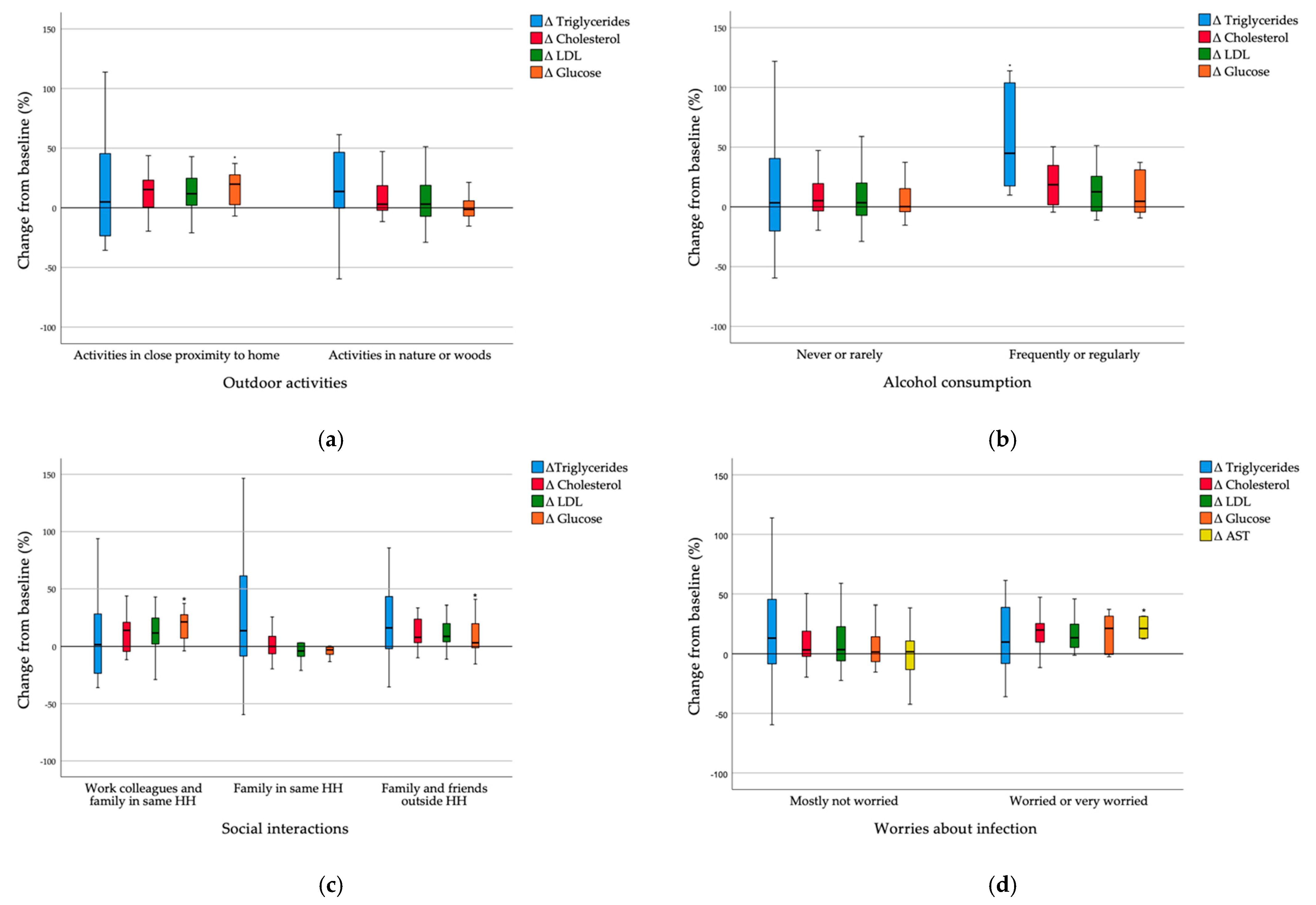
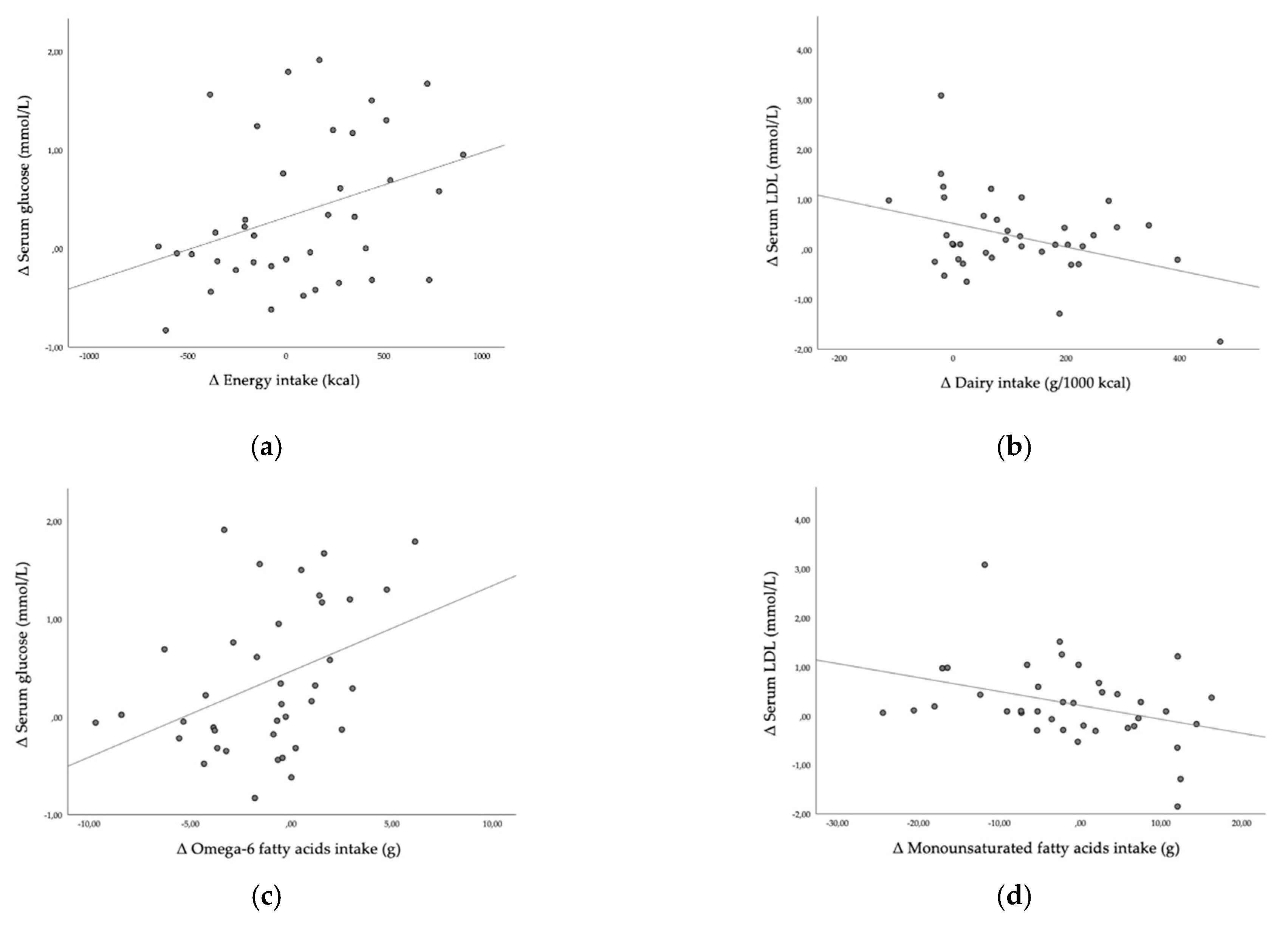
3.6. Correlations between Food Quality and Serum Marker Changes Due to Lockdown
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 9 April 2020).
- Sandford, A. Coronavirus: Half of Humanity on Lockdown in 90 Countries. Available online: https://www.euronews.com/2020/04/02/coronavirus-in-europe-spain-s-death-toll-hits-10-000-after-record-950-new-deaths-in-24-hou (accessed on 12 May 2020).
- Rehman, H.; Ahmad, M.I. COVID-19: Quarantine, Isolation, and Lifestyle Diseases. Arch. Physiol. Biochem. 2020. [Google Scholar] [CrossRef] [PubMed]
- Vlada Republike Slovenije. Slovenija Razglasila Epidemijo Novega Koronavirusa. Available online: https://www.gov.si/novice/2020-03-12-slovenija-razglasila-epidemijo-novega-koronavirusa/ (accessed on 18 June 2020).
- Odlok o Preklicu Epidemije Nalezljive Bolezni SARS-CoV-2 (COVID-19)/Ordinance on the Revocation of the COVID-19 Epidemic. Uradni list RS, št. 68/20. Available online: http://pisrs.si (accessed on 25 January 2021).
- Cetron, M.; Maloney, S.; Koppaka, R.; Simone, P. Isolation and Quarantine: Containment Strategies for SARS 2003; National Academies Press: Washington, DC, USA, 2004. [Google Scholar]
- Dignum, F.; Dignum, V.; Davidsson, P.; Ghorbani, A.; van der Hurk, M.; Jensen, M.; Kammler, C.; Lorig, F.; Ludescher, L.G.; Melchior, A.; et al. Analysing the Combined Health, Social and Economic Impacts of the Corovanvirus Pandemic Using Agent-Based Social Simulation. Minds Mach. 2020, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Pearl, R.L. Weight Stigma and the “Quarantine-15”. Obesity 2020. [Google Scholar] [CrossRef]
- Abbas, A.M.; Kamel, M.M. Dietary Habits in Adults during Quarantine in the Context of COVID-19 Pandemic. Obes Med. 2020, 19, 100254. [Google Scholar] [CrossRef]
- Mattioli, A.V.; Ballerini Puviani, M.; Nasi, M.; Farinetti, A. COVID-19 Pandemic: The Effects of Quarantine on Cardiovascular Risk. Eur. J. Clin. Nutr. 2020, 74, 852–855. [Google Scholar] [CrossRef]
- Dramatično Stanje v Izropanih Slovenskih Trgovinah. Available online: https://novice.svet24.si/clanek/novice/slovenija/5e6a83b45c265/foto-dramaticno-stanje-v-izropanih-slovenskih-trgovinah-police-prazne-roba-v-skladiscih (accessed on 9 April 2020).
- Childs, C.E.; Calder, P.C.; Miles, E.A. Diet and Immune Function. Nutrients 2019, 11, 1933. [Google Scholar] [CrossRef]
- Noncommunicable Diseases: Risk Factors. Available online: https://www.who.int/data/gho/data/themes/topics/topic-details/GHO/ncd-risk-factors (accessed on 1 March 2021).
- Eckel, R.H.; Alberti, K.; Grundy, S.M.; Zimmet, P.Z. The Metabolic Syndrome. Lancet 2010, 375, 181–183. [Google Scholar] [CrossRef]
- Bizjak, M.; Jenko-Pražnikar, Z.; Koroušić Seljak, B. Development and Validation of an Electronic FFQ to Assess Food Intake in the Slovene Population. Public Health Nutr. 2014, 17, 1729–1737. [Google Scholar] [CrossRef] [PubMed]
- Korošec, M.; Golob, T.; Bertoncelj, J.; Stibilj, V.; Seljak, B. The Slovenian Food Composition Database. Food Chem. 2013, 140, 495–499. [Google Scholar] [CrossRef]
- Souci, S.W.; Fachmann, W.; Kraut, H. Food Composition and Nutrition Tables; Medpharm: Centurion, South Africa, 2000. [Google Scholar]
- Reedy, J.; Lerman, J.L.; Krebs-Smith, S.M.; Kirkpatrick, S.I.; Pannucci, T.E.; Wilson, M.M.; Subar, A.F.; Kahle, L.L.; Tooze, J.A. Evaluation of the Healthy Eating Index-2015. J. Acad. Nutr. Diet. 2018, 118, 1622–1633. [Google Scholar] [CrossRef]
- Center for Nutrition Policy and Promotion. How the HEI Is Scored | USDA-FNS. Available online: https://www.fns.usda.gov/how-hei-scored (accessed on 30 July 2020).
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Tuck, M.K.; Chan, D.W.; Chia, D.; Godwin, A.K.; Grizzle, W.E.; Krueger, K.E.; Rom, W.; Sanda, M.; Sorbara, L.; Stass, S.; et al. Standard Operating Procedures for Serum and Plasma Collection: Early Detection Research Network Consensus Statement Standard Operating Procedure Integration Working Group. J. Proteome Res. 2009, 8, 113–117. [Google Scholar] [CrossRef]
- Huang, P.L. A Comprehensive Definition for Metabolic Syndrome. Dis. Models Mech. 2009, 2, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Yi, S.-W.; Yi, J.-J.; Ohrr, H. Total Cholesterol and All-Cause Mortality by Sex and Age: A Prospective Cohort Study among 12.8 Million Adults. Sci. Rep. 2019, 9, 1596. [Google Scholar] [CrossRef]
- Lewington, S.; Whitlock, G.; Clarke, R.; Sherliker, P.; Emberson, J.; Halsey, J.; Qizilbash, N.; Peto, R.; Collins, R.; Prospective Studies Collaboration. Blood Cholesterol and Vascular Mortality by Age, Sex, and Blood Pressure: A Meta-Analysis of Individual Data from 61 Prospective Studies with 55,000 Vascular Deaths. Lancet 2007, 370, 1829–1839. [Google Scholar] [CrossRef] [PubMed]
- Yi, S.-W.; Park, S.; Lee, Y.; Park, H.-J.; Balkau, B.; Yi, J.-J. Association between Fasting Glucose and All-Cause Mortality According to Sex and Age: A Prospective Cohort Study. Sci. Rep. 2017, 7, 8194. [Google Scholar] [CrossRef]
- De Guia, R.M.; Rose, A.J.; Herzig, S. Glucocorticoid Hormones and Energy Homeostasis. Horm. Mol. Biol. Clin. Investig. 2014, 19, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Pouso, S.; Borja, Á.; Fleming, L.E.; Gómez-Baggethun, E.; White, M.P.; Uyarra, M.C. Contact with Blue-Green Spaces during the COVID-19 Pandemic Lockdown Beneficial for Mental Health. Sci. Total Environ. 2021, 756, 143984. [Google Scholar] [CrossRef]
- Ghesquière, L.; Garabedian, C.; Drumez, E.; Lemaître, M.; Cazaubiel, M.; Bengler, C.; Vambergue, A. Effects of COVID-19 Pandemic Lockdown on Gestational Diabetes Mellitus: A Retrospective Study. Diabetes Metab. 2020, 101201. [Google Scholar] [CrossRef]
- Barchetta, I.; Cimini, F.A.; Bertoccini, L.; Ceccarelli, V.; Spaccarotella, M.; Baroni, M.G.; Cavallo, M.G. Effects of Work Status Changes and Perceived Stress Onglycaemiccontrol in Individuals with Type 1 Diabetes during COVID-19 Lockdown in Italy. Diabetes Res. Clin. Pract. 2020, 170, 108513. [Google Scholar] [CrossRef] [PubMed]
- Biancalana, E.; Parolini, F.; Mengozzi, A.; Solini, A. Short-Term Impact of COVID-19 Lockdown on Metabolic Control of Patients with Well-Controlled Type 2 Diabetes: A Single-Centre Observational Study. Acta Diabetol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Bonora, B.M.; Boscari, F.; Avogaro, A.; Bruttomesso, D.; Fadini, G.P. Glycaemic Control Among People with Type 1 Diabetes During Lockdown for the SARS-CoV-2 Outbreak in Italy. Diabetes 2020, 1–11. [Google Scholar] [CrossRef]
- Grabia, M.; Markiewicz-Żukowska, R.; Puścion-Jakubik, A.; Bielecka, J.; Nowakowski, P.; Gromkowska-Kępka, K.; Mielcarek, K.; Socha, K. The Nutritional and Health Effects of the COVID-19 Pandemic on Patients with Diabetes Mellitus. Nutrients 2020, 12, 3013. [Google Scholar] [CrossRef] [PubMed]
- Prabhu Navis, J.; Leelarathna, L.; Mubita, W.; Urwin, A.; Rutter, M.K.; Schofield, J.; Thabit, H. Impact of COVID-19 Lockdown on Flash and Real-Time Glucose Sensor Users with Type 1 Diabetes in England. Acta Diabetol. 2020. [Google Scholar] [CrossRef]
- Aragona, M.; Rodia, C.; Bertolotto, A.; Campi, F.; Coppelli, A.; Giannarelli, R.; Bianchi, C.; Dardano, A.; Del Prato, S. Type 1 Diabetes and COVID-19: The “Lockdown Effect”. Diabetes Res. Clin. Pract. 2020, 170, 108468. [Google Scholar] [CrossRef]
- Onvani, S.; Haghighatdoost, F.; Surkan, P.J.; Larijani, B.; Azadbakht, L. Adherence to the Healthy Eating Index and Alternative Healthy Eating Index Dietary Patterns and Mortality from All Causes, Cardiovascular Disease and Cancer: A Meta-Analysis of Observational Studies. J. Hum. Nutr. Diet. 2017, 30, 216–226. [Google Scholar] [CrossRef] [PubMed]
- Barbaresko, J.; Koch, M.; Schulze, M.B.; Nöthlings, U. Dietary Pattern Analysis and Biomarkers of Low-Grade Inflammation: A Systematic Literature Review. Nutr. Rev. 2013, 71, 511–527. [Google Scholar] [CrossRef]
- Lamarche, B.; Brassard, D.; Lapointe, A.; Laramée, C.; Kearney, M.; Côté, M.; Bélanger-Gravel, A.; Desroches, S.; Lemieux, S.; Plante, C. Changes in Diet Quality and Food Security among Adults during the COVID-19–Related Early Lockdown: Results from NutriQuébec. Am. J. Clin. Nutr. 2021. [Google Scholar] [CrossRef]
- Rodríguez-Pérez, C.; Molina-Montes, E.; Verardo, V.; Artacho, R.; García-Villanova, B.; Guerra-Hernández, E.J.; Ruíz-López, M.D. Changes in Dietary Behaviours during the COVID-19 Outbreak Confinement in the Spanish COVIDiet Study. Nutrients 2020, 12, 1730. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating Habits and Lifestyle Changes during COVID-19 Lockdown: An Italian Survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Fogacci, F.; Giovannini, M.; Mezzadri, M.; Grandi, E.; Borghi, C.; The Brisighella Heart Study Group. COVID-19-Related Quarantine Effect on Dietary Habits in a Northern Italian Rural Population: Data from the Brisighella Heart Study. Nutrients 2021, 13, 309. [Google Scholar] [CrossRef]
- Anto, L.; Warykas, S.W.; Torres-Gonzalez, M.; Blesso, C.N. Milk Polar Lipids: Underappreciated Lipids with Emerging Health Benefits. Nutrients 2020, 12, 1001. [Google Scholar] [CrossRef]
- Hooper, L.; Martin, N.; Abdelhamid, A.; Smith, G.D. Reduction in Saturated Fat Intake for Cardiovascular Disease. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]
- Koska, J.; Ozias, M.K.; Deer, J.; Kurtz, J.; Salbe, A.D.; Harman, S.M.; Reaven, P.D. A Human Model of Dietary Saturated Fatty Acid Induced Insulin Resistance. Metab. Clin. Exp. 2016, 65, 1621–1628. [Google Scholar] [CrossRef] [PubMed]
- Górnicka, M.; Drywień, M.E.; Zielinska, M.A.; Hamułka, J. Dietary and Lifestyle Changes During COVID-19 and the Subsequent Lockdowns among Polish Adults: A Cross-Sectional Online Survey PLifeCOVID-19 Study. Nutrients 2020, 12, 2324. [Google Scholar] [CrossRef]
- Błaszczyk-Bębenek, E.; Jagielski, P.; Bolesławska, I.; Jagielska, A.; Nitsch-Osuch, A.; Kawalec, P. Nutrition Behaviors in Polish Adults before and during COVID-19 Lockdown. Nutrients 2020, 12, 3084. [Google Scholar] [CrossRef]
- Kriaucioniene, V.; Bagdonaviciene, L.; Rodríguez-Pérez, C.; Petkeviciene, J. Associations between Changes in Health Behaviours and Body Weight during the COVID-19 Quarantine in Lithuania: The Lithuanian COVIDiet Study. Nutrients 2020, 12, 3119. [Google Scholar] [CrossRef] [PubMed]
- Kahleova, H.; Lloren, J.I.; Mashchak, A.; Hill, M.; Fraser, G.E. Meal Frequency and Timing Are Associated with Changes in Body Mass Index in Adventist Health Study 2. J. Nutr. 2017, 147, 1722–1728. [Google Scholar] [CrossRef]
- Sidor, A.; Rzymski, P. Dietary Choices and Habits during COVID-19 Lockdown: Experience from Poland. Nutrients 2020, 12, 1657. [Google Scholar] [CrossRef]
- Husain, W.; Ashkanani, F. Does COVID-19 Change Dietary Habits and Lifestyle Behaviours in Kuwait: A Community-Based Cross-Sectional Study. Env. Health Prev. Med. 2020, 25, 61. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Cinelli, G.; Bigioni, G.; Soldati, L.; Attinà, A.; Bianco, F.F.; Caparello, G.; Camodeca, V.; Carrano, E.; et al. Psychological Aspects and Eating Habits during COVID-19 Home Confinement: Results of EHLC-COVID-19 Italian Online Survey. Nutrients 2020, 12, 2152. [Google Scholar] [CrossRef]
- Van de Wiel, A. The Effect of Alcohol on Postprandial and Fasting Triglycerides. Int. J. Vasc. Med. 2012. [Google Scholar] [CrossRef]
- Ruíz-Roso, M.B.; de Carvalho Padilha, P.; Matilla-Escalante, D.C.; Brun, P.; Ulloa, N.; Acevedo-Correa, D.; Arantes Ferreira Peres, W.; Martorell, M.; Rangel Bousquet Carrilho, T.; de Oliveira Cardoso, L.; et al. Changes of Physical Activity and Ultra-Processed Food Consumption in Adolescents from Different Countries during Covid-19 Pandemic: An Observational Study. Nutrients 2020, 12, 2289. [Google Scholar] [CrossRef] [PubMed]
- Cheikh Ismail, L.; Osaili, T.M.; Mohamad, M.N.; Al Marzouqi, A.; Jarrar, A.H.; Abu Jamous, D.O.; Magriplis, E.; Ali, H.I.; Al Sabbah, H.; Hasan, H.; et al. Eating Habits and Lifestyle during COVID-19 Lockdown in the United Arab Emirates: A Cross-Sectional Study. Nutrients 2020, 12, 3314. [Google Scholar] [CrossRef]
- Biswas, A.; Oh, P.I.; Faulkner, G.E.; Bajaj, R.R.; Silver, M.A.; Mitchell, M.S.; Alter, D.A. Sedentary Time and Its Association with Risk for Disease Incidence, Mortality, and Hospitalization in Adults: A Systematic Review and Meta-Analysis. Ann. Intern. Med. 2015, 162, 123–132. [Google Scholar] [CrossRef]
- Kujala, U.M.; Mäkinen, V.-P.; Heinonen, I.; Soininen, P.; Kangas, A.J.; Leskinen, T.H.; Rahkila, P.; Würtz, P.; Kovanen, V.; Cheng, S.; et al. Long-Term Leisure-Time Physical Activity and Serum Metabolome. Circulation 2013, 127, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, M.; Ponzo, V.; Rosato, R.; Scumaci, E.; Goitre, I.; Benso, A.; Belcastro, S.; Crespi, C.; De Michieli, F.; Ghigo, E.; et al. Changes in Weight and Nutritional Habits in Adults with Obesity during the “Lockdown” Period Caused by the COVID-19 Virus Emergency. Nutrients 2020, 12, 2016. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Pugliese, G.; Framondi, L.; Di Matteo, R.; Laudisio, D.; Savastano, S.; Colao, A.; Muscogiuri, G. Does Sars-Cov-2 Threaten Our Dreams? Effect of Quarantine on Sleep Quality and Body Mass Index. J. Transl. Med. 2020, 18, 318. [Google Scholar] [CrossRef] [PubMed]
- Önmez, A.; Gamsızkan, Z.; Özdemir, Ş.; Kesikbaş, E.; Gökosmanoğlu, F.; Torun, S.; Cinemre, H. The Effect of COVID-19 Lockdown on Glycemic Control in Patients with Type 2 Diabetes Mellitus in Turkey. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 1963–1966. [Google Scholar] [CrossRef]
- Lange, K.W.; Nakamura, Y. Lifestyle Factors in the Prevention of COVID-19. Glob. Health J. 2020, 4, 146–152. [Google Scholar] [CrossRef]
- Hamer, M.; Kivimäki, M.; Gale, C.R.; Batty, G.D. Lifestyle Risk Factors, Inflammatory Mechanisms, and COVID-19 Hospitalization: A Community-Based Cohort Study of 387,109 Adults in UK. Brain Behav. Immun. 2020, 87, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Hariyanto, T.I.; Kurniawan, A. Dyslipidemia Is Associated with Severe Coronavirus Disease 2019 (COVID-19) Infection. Diabetes Metab. Syndr. 2020, 14, 1463–1465. [Google Scholar] [CrossRef]
- Erener, S. Diabetes, Infection Risk and COVID-19. Mol. Metab. 2020, 39, 101044. [Google Scholar] [CrossRef]
- Apicella, M.; Campopiano, M.C.; Mantuano, M.; Mazoni, L.; Coppelli, A.; Prato, S.D. COVID-19 in People with Diabetes: Understanding the Reasons for Worse Outcomes. Lancet Diabetes Endocrinol. 2020, 8, 782–792. [Google Scholar] [CrossRef]
- De la Iglesia, R.; Loria-Kohen, V.; Zulet, M.A.; Martinez, J.A.; Reglero, G.; Ramirez de Molina, A. Dietary Strategies Implicated in the Prevention and Treatment of Metabolic Syndrome. Int. J. Mol. Sci. 2016, 17, 1877. [Google Scholar] [CrossRef] [PubMed]
- Strollo, F.; Macchi, C.; Eberini, I.; Masini, M.A.; Botta, M.; Vassilieva, G.; Nichiporuk, I.; Monici, M.; Santucci, D.; Celotti, F.; et al. Body Composition and Metabolic Changes during a 520-Day Mission Simulation to Mars. J. Endocrinol. Investig. 2018, 41, 1267–1273. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Mean ± SD |
|---|---|
| n | 38 |
| Age (years) | 36.3 ± 10.1 |
| Height (cm) | 170.8 ± 8.3 |
| Body mass (kg) | 65.8 ± 10.2 |
| BMI (kg/m2) | 22.5 ± 2.7 |
| Gender | % |
| Female | 63.2 |
| Male | 36.8 |
| Education | % |
| High school diploma | 16.2 |
| Bachelor’s degree | 70.3 |
| Master’s degree or PhD | 13.5 |
| Marital Status | % |
| Single | 18.9 |
| In a relationship or married | 81.1 |
| Living Arrangement | % |
| Alone | 10.8 |
| With partner | 35.1 |
| With partner and children | 40.5 |
| With parents | 13.5 |
| Smoking | % |
| Never | 67.6 |
| Occasionally | 24.3 |
| Regularly | 8.1 |
| Alcohol Consumption | % |
| Never | 16.2 |
| Occasionally | 75.7 |
| Regularly | 5.4 |
| Meat Consumption | % |
| Regular meat consumption | 55.3 |
| No meat consumption | 44.7 |
| General Lifestyle Changes during Lockdown | % |
| Lifestyle did not change at all | 5.4 |
| Lifestyle changed a little | 56.8 |
| Lifestyle changed a lot | 32.4 |
| Lifestyle changed completely | 5.4 |
| Changes in working conditions during lockdown | % |
| No changes | 33.3 |
| Work from home, previously partially worked from home | 11.1 |
| Work from home, previously never worked from home | 13.9 |
| Partially work from home and partially at the workplace | 11.1 |
| Not working, receiving compensation | 22.2 |
| Not working, not receiving compensation | 8.3 |
| Changes in socio-economic status during lockdown | % |
| Received 0–50% of baseline monthly income | 16.2 |
| Received 80% of baseline monthly income | 16.2 |
| Received 90–100% of baseline monthly income | 67.6 |
| Visiting the grocery store during lockdown | % |
| Less than once per week | 35.1 |
| Once per week | 48.6 |
| Twice per week | 13.5 |
| More than twice per week | 2.7 |
| Activities outdoors during lockdown | % |
| Activities in close proximity to home | 27.0 % |
| Activities in the nature and woods | 73.0 % |
| Baseline | Lockdown | Post-Lockdown | p Value * | |
|---|---|---|---|---|
| Energy intake (kcal) | 2296.78 ± 873.26 | 1891.03 ± 678.13 a | 2248.17 ± 576.76 c | 0.002 |
| Total fruits (g/1000 kcal) | 109.79 ± 102.00 | 113.57 ± 101.45 | 108.75 ± 67.38 | 0.916 |
| Whole fruits (g/1000 kcal) | 85.77 ± 78.25 | 90.51 ± 78.49 | 83.13 ± 62.66 | 0.829 |
| Total vegetables (g/1000 kcal) | 507.16 ± 377.07 | 581.21 ± 411.26 | 134.05 ± 92.13 b,c | <0.001 |
| Greens and beans (g/1000 kcal) | 76.57 ± 113.65 | 54.04 ± 57.01 | 22.39 ± 23.31 b,c | 0.002 |
| Whole grains (g/1000 kcal) | 23.14 ± 24.75 | 21.11 ± 24.41 | 28.85 ± 29.30 | 0.319 |
| Dairy (g/1000 kcal) | 60.70 ± 69.39 | 64.65 ± 67.59 | 172.98 ± 143.27 b,c | <0.001 |
| Total protein food (g/1000 kcal) | 88.95 ± 66.92 | 69.31 ± 46.38 a | 54.55 ± 33.47 b | 0.002 |
| Seafood and plant proteins (g/1000 kcal) | 49.27 ± 39.97 | 35.37 ± 28.92 a | 29.91 ± 22.52 b | 0.002 |
| Fatty acids (PUFA+MUFA)/SFA) | 1.98 ± 1.34 | 1.77 ± 1.20 a | 1.54 ± 0.78 b | 0.026 |
| Refined grains (g/1000 kcal) | 29.67 ± 28.17 | 39.81 ± 37.58 a | 52.72 ± 48.19 b | 0.006 |
| Sodium (g/1000 kcal) | 0.95 ± 0.44 | 1.12 ± 0.73 | 1.19 ± 0.54 b | 0.071 |
| Added sugar (%EI) | 10.93 ± 6.08 | 12.39 ± 6.67 | 4.84 ± 3.93 b,c | <0.001 |
| Saturated fats (%EI) | 10.98 ± 7.46 | 11.82 ± 8.47 | 13.23 ± 8.79 b,c | 0.001 |
| HEI | 64.59 ± 15.76 | 61.08 ± 13.42 a | 63.26 ± 15.22 | 0.203 |
| Variable (Unit) | Baseline | Post-Lockdown | p Value * |
|---|---|---|---|
| Energy density (kcal/g) * | 1.15 ± 0.32 | 0.81 ± 0.27 | 0.000 |
| Protein (g) | 86.47 ± 36.45 | 87.25 ± 36.45 | 0.567 |
| Carbohydrate (g) | 241.18 ± 151.18 | 249.45 ± 131.06 | 0.456 |
| Fat (g) | 89.29 ± 35.63 | 93.01 ± 41.82 | 0.345 |
| Dietary fibre (g) * | 28.35 ± 17.30 | 31.49 ± 17.95 | 0.046 |
| Dietary fibre (g/1000 kcal) * | 12.81 ± 6.45 | 14.15 ± 7.82 | 0.031 |
| Soluble fibre (g) | 5.54 ± 4.49 | 6.02 ± 3.84 | 0.272 |
| Unsoluble fibre (g) | 10.93 ± 8.70 | 12.23 ± 8.18 | 0.197 |
| Sugar (g) | 80.62 ± 55.72 | 76.70 ± 48.44 | 0.690 |
| Free sugar (g) | 33.53 ± 29.16 | 29.70 ± 27.88 | 0.464 |
| Starch (g) * | 68.13 ± 62.95 | 84.17 ± 58.09 | 0.048 |
| Plant protein (g) | 37.26 ± 24.89 | 40.82 ± 24.46 | 0.065 |
| Saturated fatty acids (g) * | 26.54 ± 18.82 | 31.76 ± 20.68 | 0.003 |
| Monounsaturated fatty acids (g) | 28.55 ± 14.23 | 27.07 ± 12.73 | 0.378 |
| Polyunsaturated fatty acids (g) | 13.25 ± 7.84 | 12.43 ± 6.10 | 0.421 |
| Omega-6 fatty acids (g) * | 7.29 ± 5.95 | 6.05 ± 4.26 | 0.042 |
| Omega-3 fatty acids (g) | 1.45 ± 1.59 | 1.50 ± 1.26 | 0.357 |
| Omega-3/omega-6 ratio * | 0.27 ± 0.39 | 0.29 ± 0.18 | 0.023 |
| Cholesterol (mg) | 323.35 ± 376.50 | 316.96 ± 356.47 | 0.328 |
| Vitamin C (mg) | 135.40 ± 99.23 | 110.94 ± 70.30 | 0.232 |
| Vitamin D (μg) | 4.08 ± 3.45 | 4.61 ± 5.08 | 0.637 |
| Vitamin E (mg) | 12.51 ± 7.72 | 10.83 ± 4.78 | 0.255 |
| Riboflavin—vitamin B2 (mg) * | 1.65 ± 0.62 | 2.00 ± 0.76 | 0.003 |
| Niacin—vitamin B3 (mg) * | 20.10 ± 10.99 | 29.56 ± 12.26 | 0.000 |
| Biotin—vitamin B7 (μg) | 35.78 ± 20.41 | 38.97 ± 19.10 | 0.076 |
| Folate (μg) * | 360.91 ± 175.88 | 442.64 ± 225.83 | 0.001 |
| Vitamin B12 (μg) | 5.02 ± 6.62 | 5.70 ± 13.54 | 0.983 |
| Calcium (mg) | 855.04 ± 373.67 | 938.57 ± 468.35 | 0.421 |
| Iron (mg) | 17.23 ± 7.38 | 18.24 ± 6.55 | 0.210 |
| Magnesium (mg) * | 407.79 ± 224.65 | 560.13 ± 224.44 | 0.000 |
| Zinc (mg) | 10.56 ± 5.35 | 11.54 ± 4.46 | 0.062 |
| Copper (μg) * | 1865.12 ± 923.61 | 2429.81 ± 1144.20 | 0.001 |
| Alcohol (g) | 6.41 ± 11.96 | 5.88 ± 10.02 | 0.387 |
| Total-ORAC (μmol/TE) * | 8346.48 ± 6271.20 | 10874.57 ± 6949.49 | 0.005 |
| Baseline | Post-Lockdown | p Value | |
|---|---|---|---|
| Body mass (kg) | 65.8 ± 10.2 | 66.3 ± 10.5 | 0.342 |
| Body fat percentage (%) | 22.2 ± 7.6 | 22.4 ± 7.2 | 0.639 |
| Fat mass (kg) | 14.7 ± 5.5 | 14.8 ± 5.2 | 0.711 |
| Fat free mass (kg) | 51.1 ± 8.9 | 51.4 ± 9.6 | 0.400 |
| Muscle mass (kg) | 48.5 ± 8.5 | 48.8 ± 9.1 | 0.442 |
| BMI (kg/m2) | 22.5 ± 2.7 | 22.7 ± 2.6 | 0.413 |
| Visceral index | 3.8 ± 2.3 | 3.7 ± 2.3 | 0.059 |
| Total body water (kg) | 36.6 ± 6.3 | 36.8 ± 6.8 | 0.695 |
| Total body water (%) | 55.8 ± 6.2 | 55.5 ± 5.4 | 0.987 |
| Phase angle | 6.00 ± 0.7 | 6.00 ± 0.6 | 0.883 |
| Baseline | Post-Lockdown | p Value * | Slovenian Reference Values | ∆ | |
|---|---|---|---|---|---|
| Glucose (mmol/L) * | 4.850 ± 0.425 | 5.210 ± 0.698 | 0.005 | 3.6–6.1 | 0.361 ± 0.746 |
| Total cholesterol (mmol/L) * | 5.447 ± 3.523 | 5.947 ± 3.445 | 0.003 | 4.0–5.2 | 0.500 ± 0.985 |
| HDL (mmol/L) | 2.008 ± 0.402 | 2.075 ± 0.592 | 0.375 | >1.4 | 0.067 ± 0.459 |
| LDL (mmol/L) * | 3.852 ± 3.614 | 4.102 ± 3.560 | 0.049 | 2.0–3.3 | 0.250 ± 0.815 |
| Triglycerides (mmol/L) | 0.953 ± 0.574 | 1.138 ± 0.640 | 0.054 | 0.6–1.7 | 0.186 ± 0.679 |
| CRP (mg/L) * | 0.941 ± 1.315 | 0.635 ± 1.108 | 0.008 | 0.0–8.0 | −0.306 ± 1.591 |
| Iron (μmol/L) | 23.263 ± 10.663 | 25.905 ± 9.850 | 0.283 | M 10.6–28.3, W 6.6–26.0 | 2.642 ± 11.887 |
| AST (U/L) | 22.150 ± 6.606 | 23.613 ± 10.701 | 0.658 | M < 34.8, W < 31.2 | 1.463 ± 10.270 |
| Total bilirubin (μmol/L) | 8.405 ± 5.369 | 9.768 ± 5.422 | 0.066 | 0.0–17.0 | 1.363 ± 4.330 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bogataj Jontez, N.; Novak, K.; Kenig, S.; Petelin, A.; Jenko Pražnikar, Z.; Mohorko, N. The Impact of COVID-19-Related Lockdown on Diet and Serum Markers in Healthy Adults. Nutrients 2021, 13, 1082. https://doi.org/10.3390/nu13041082
Bogataj Jontez N, Novak K, Kenig S, Petelin A, Jenko Pražnikar Z, Mohorko N. The Impact of COVID-19-Related Lockdown on Diet and Serum Markers in Healthy Adults. Nutrients. 2021; 13(4):1082. https://doi.org/10.3390/nu13041082
Chicago/Turabian StyleBogataj Jontez, Nives, Karin Novak, Saša Kenig, Ana Petelin, Zala Jenko Pražnikar, and Nina Mohorko. 2021. "The Impact of COVID-19-Related Lockdown on Diet and Serum Markers in Healthy Adults" Nutrients 13, no. 4: 1082. https://doi.org/10.3390/nu13041082
APA StyleBogataj Jontez, N., Novak, K., Kenig, S., Petelin, A., Jenko Pražnikar, Z., & Mohorko, N. (2021). The Impact of COVID-19-Related Lockdown on Diet and Serum Markers in Healthy Adults. Nutrients, 13(4), 1082. https://doi.org/10.3390/nu13041082