
Sarcopenic Dysphagia: A Narrative Review from Diagnosis to Intervention

 ,
,  ,
, 

Abstract
1. Introduction
2. Definition
2.1. Sarcopenia
2.2. Dysphagia
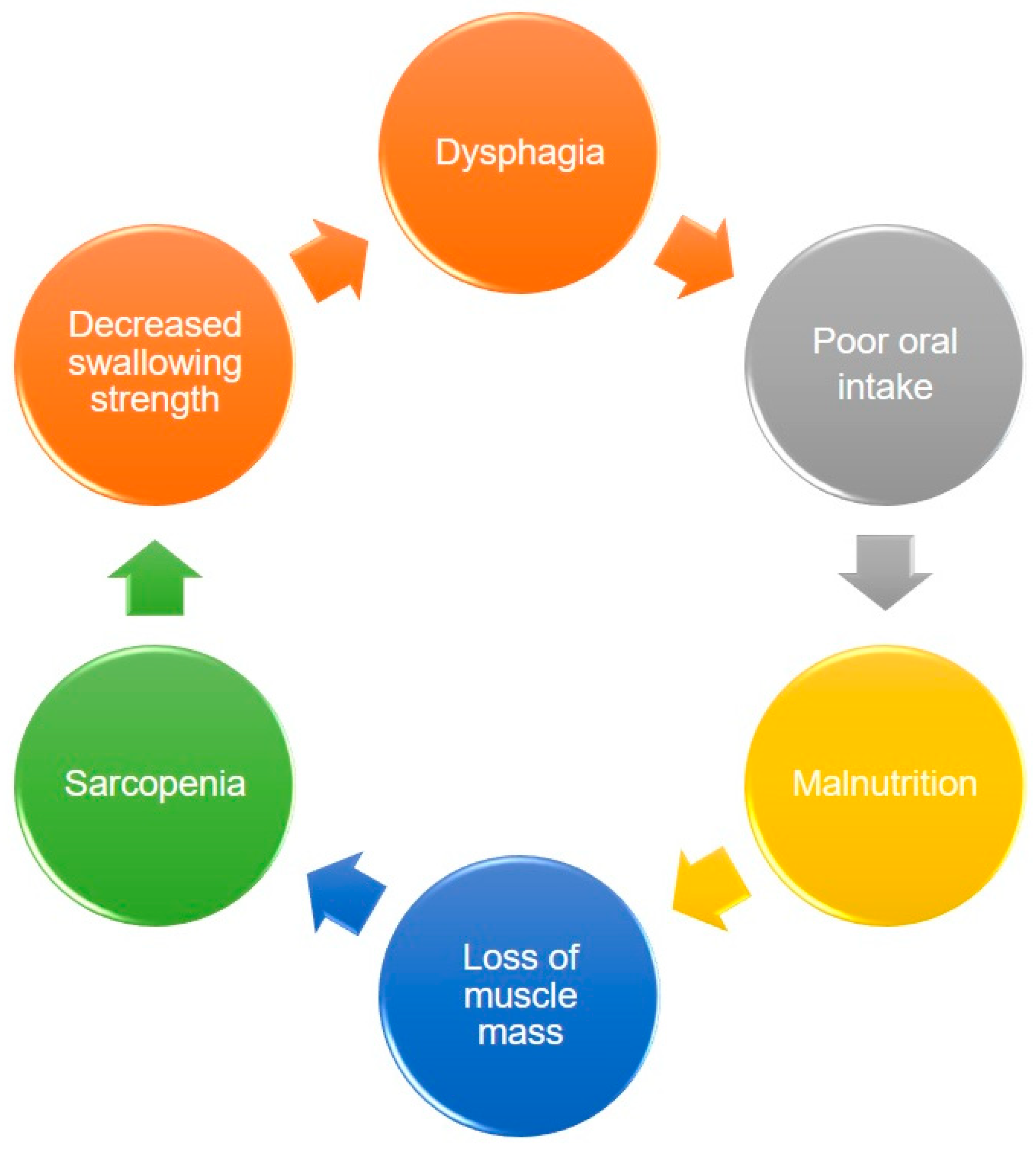
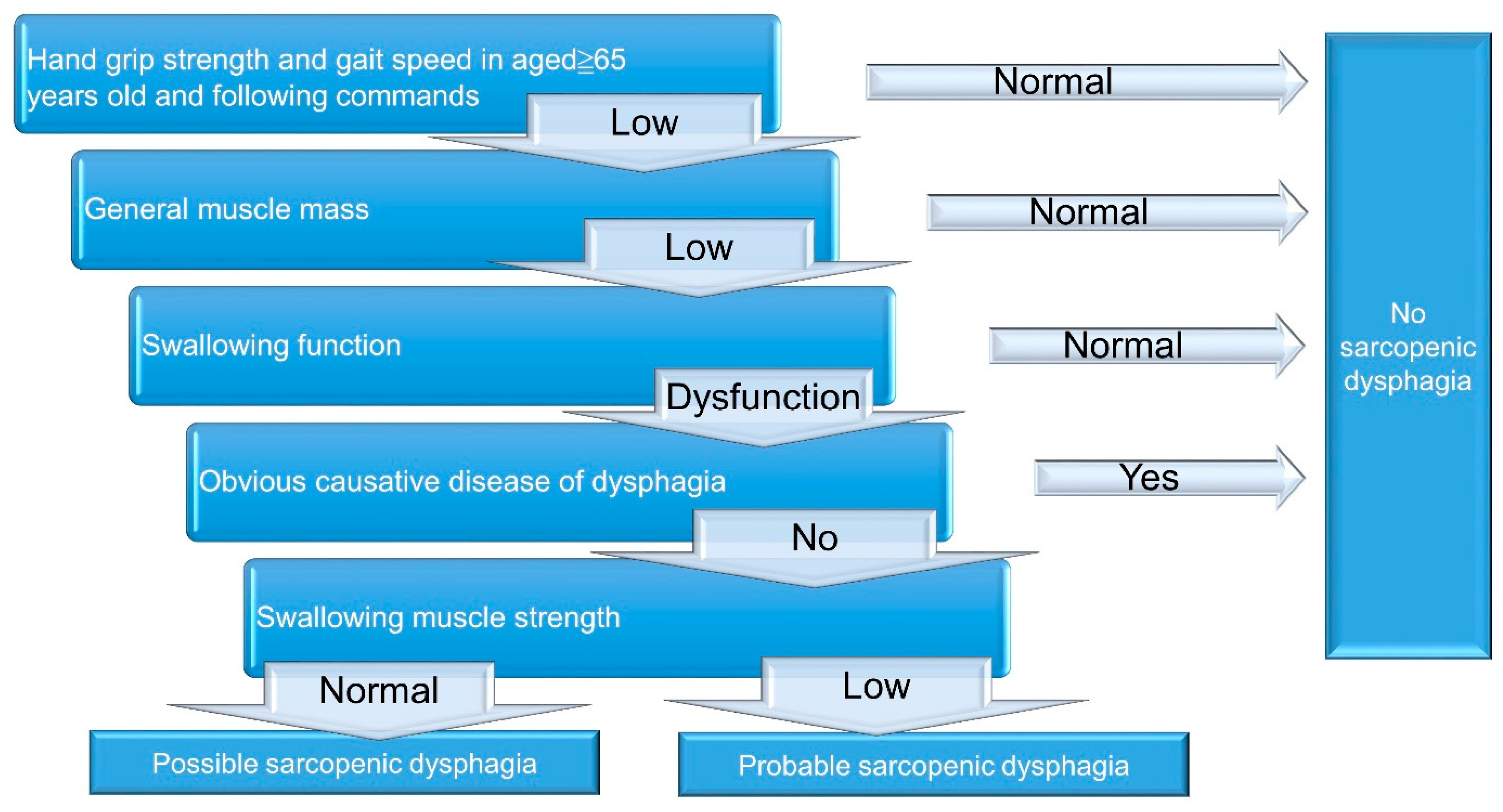
2.3. Sarcopenic Dysphagia
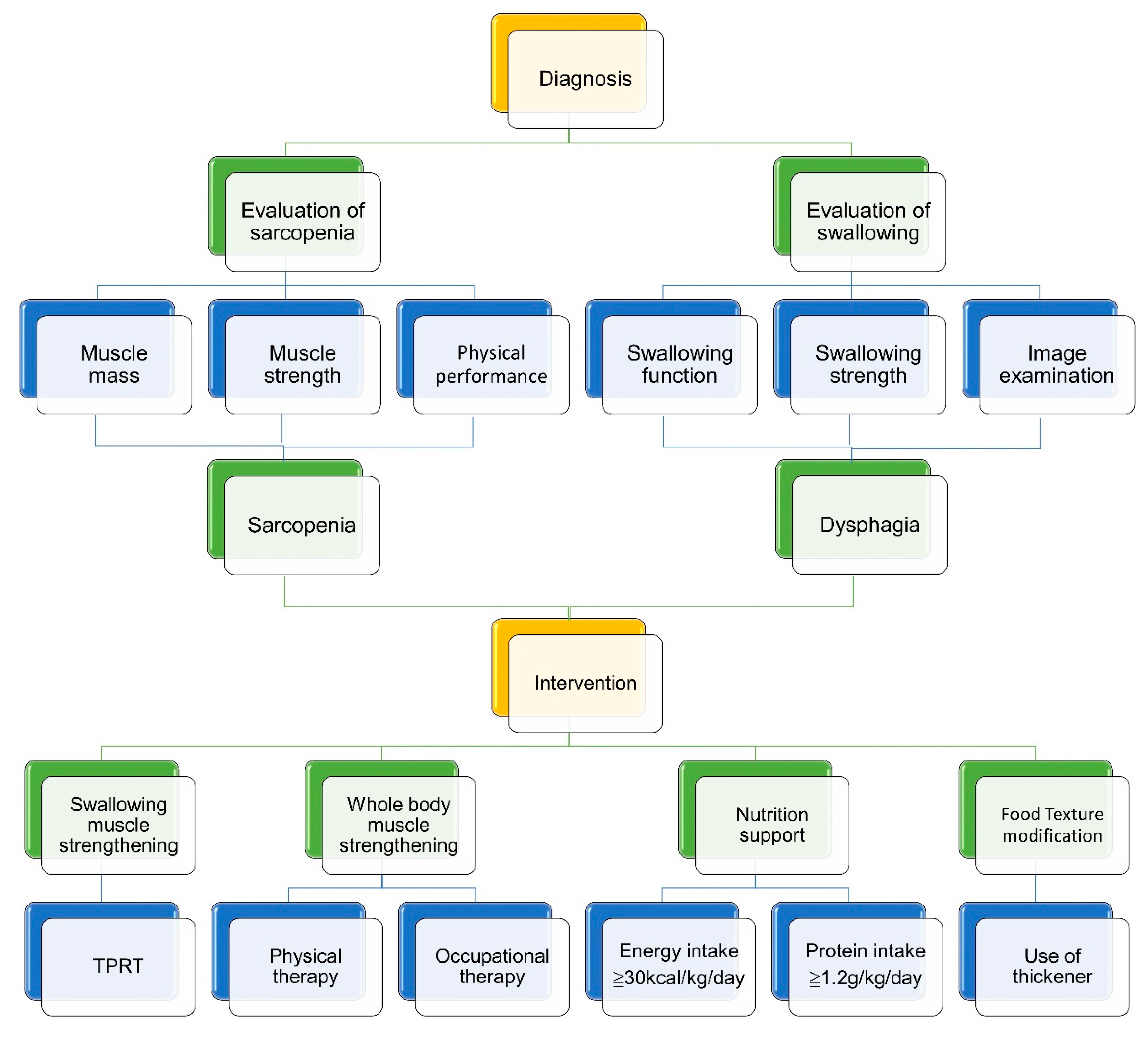
3. Tools for the Evaluation of Sarcopenic Dysphagia
3.1. Overview
3.2. Swallowing Function Evaluation: Questionnaires & Swallowing Tests
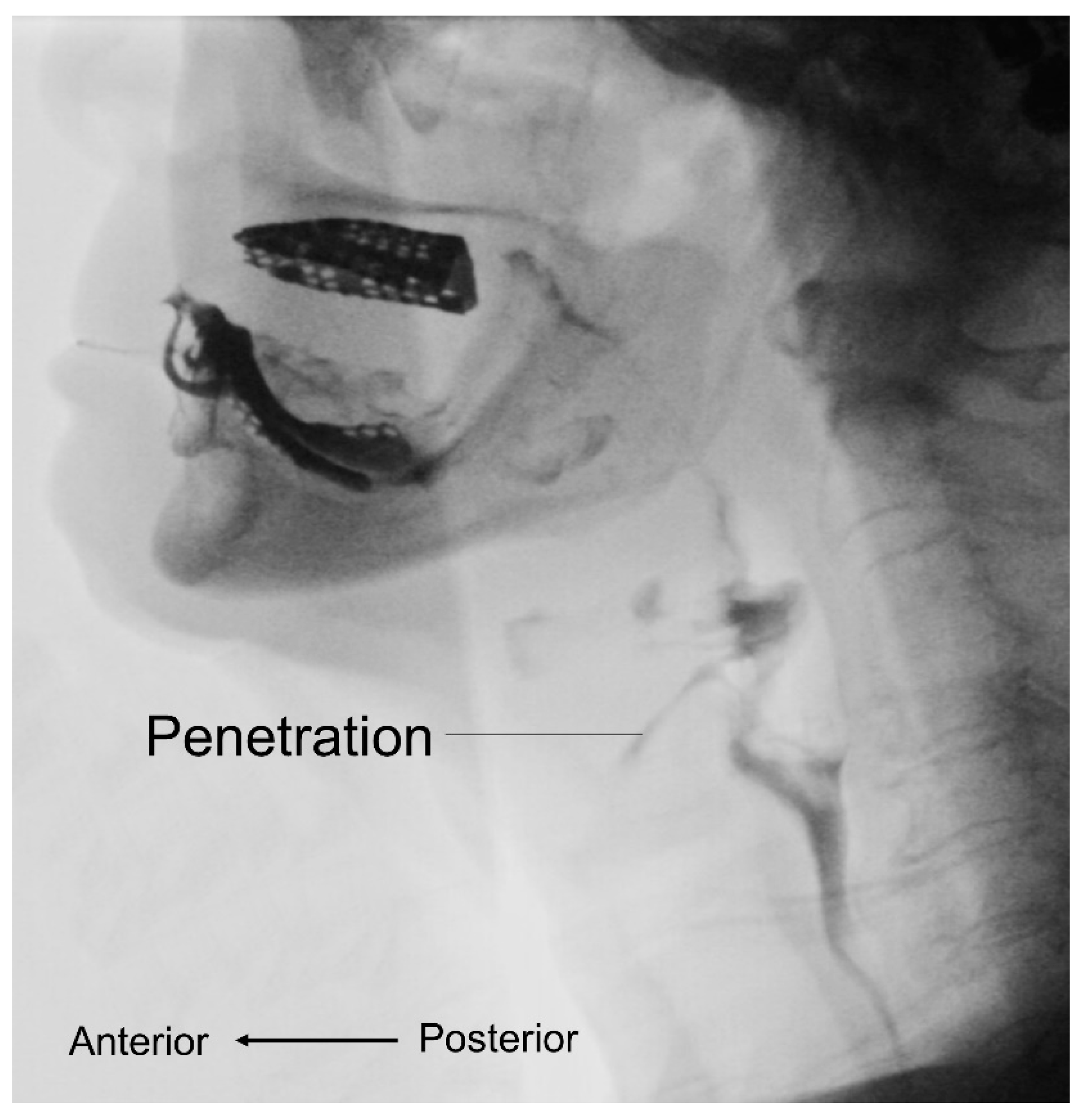
3.3. Videofluoroscopic Swallow Study
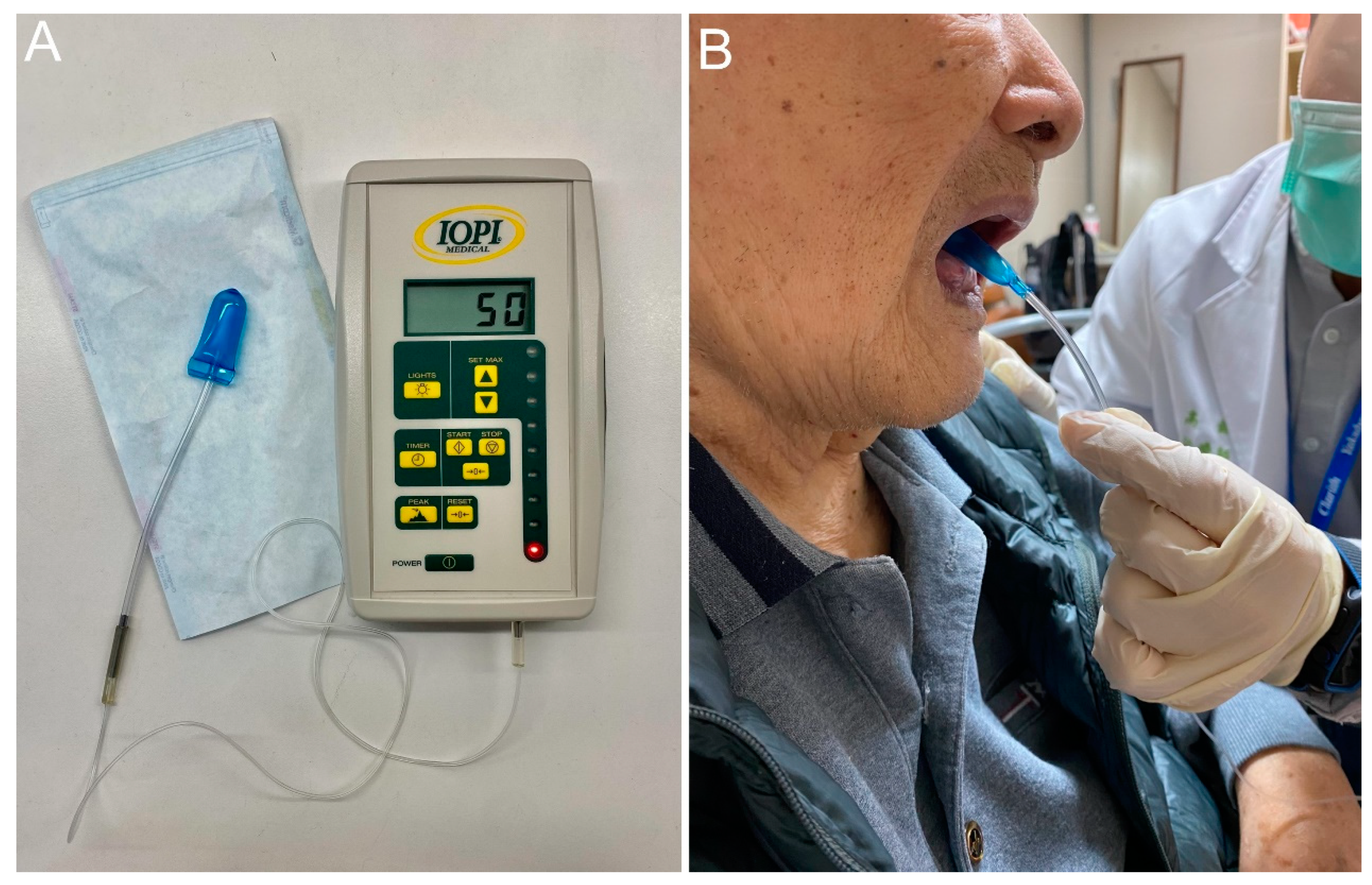
3.4. Maximal Isometric Tongue Pressure
3.5. Jaw-Opening Force
3.6. Lip Force
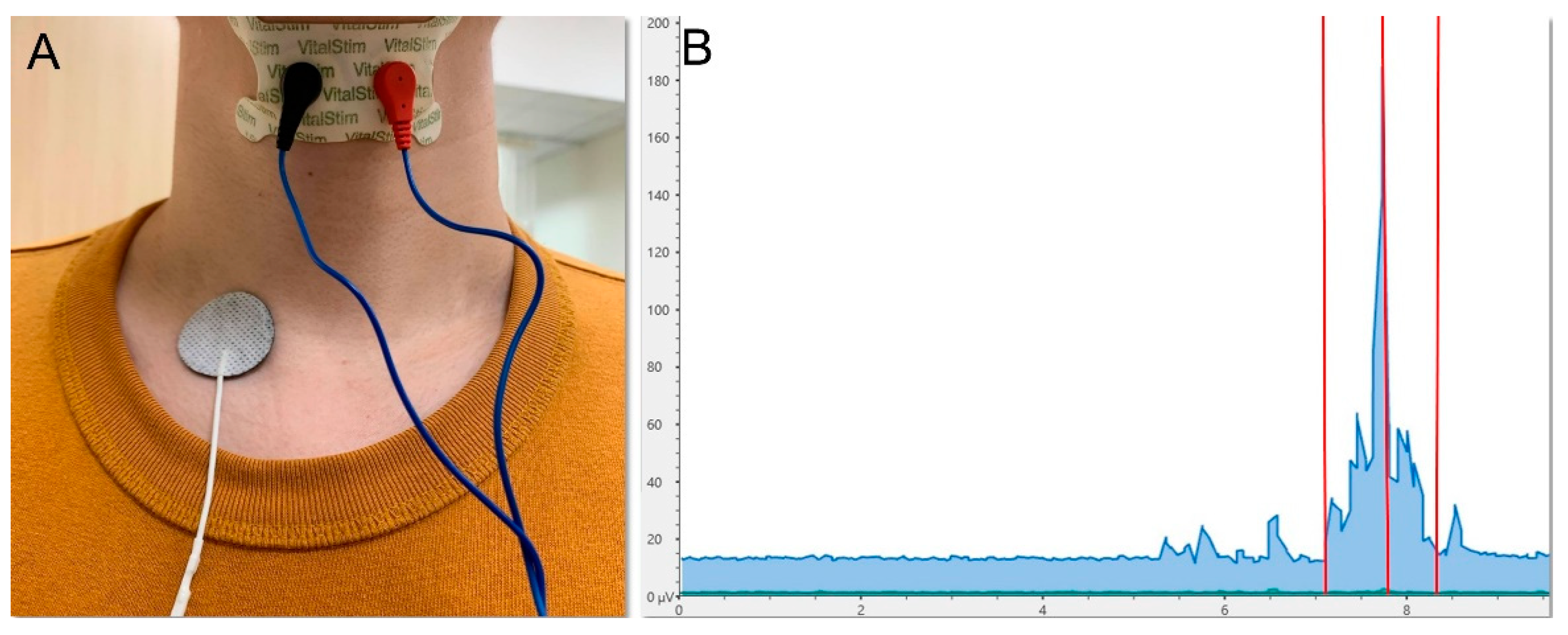
3.7. Surface Electromyography
3.8. High-Resolution Manometry
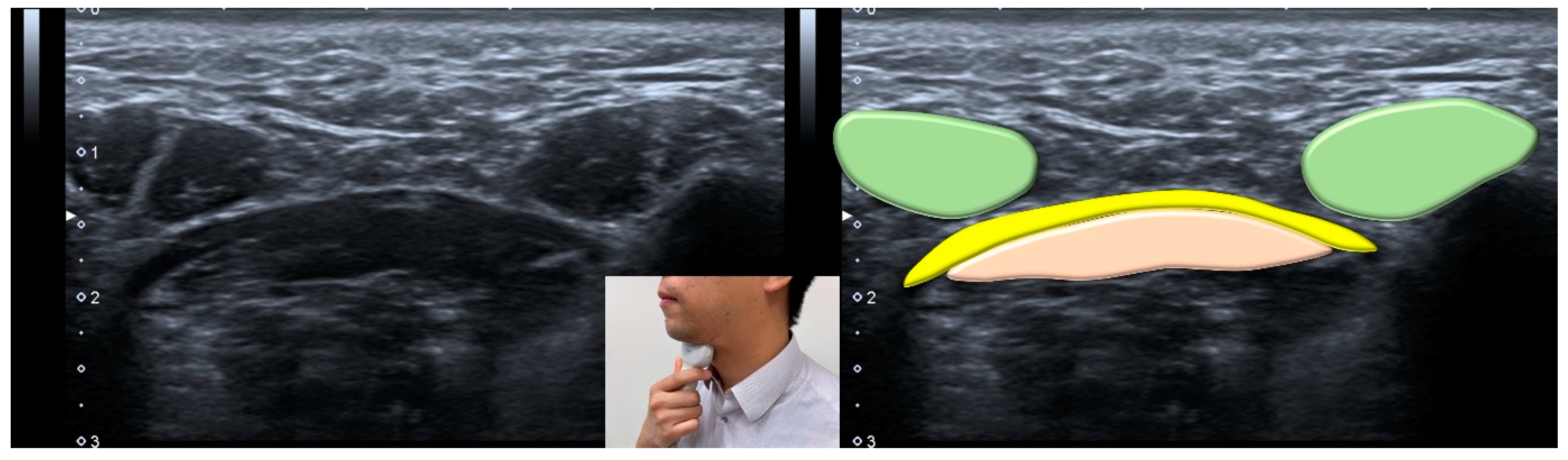
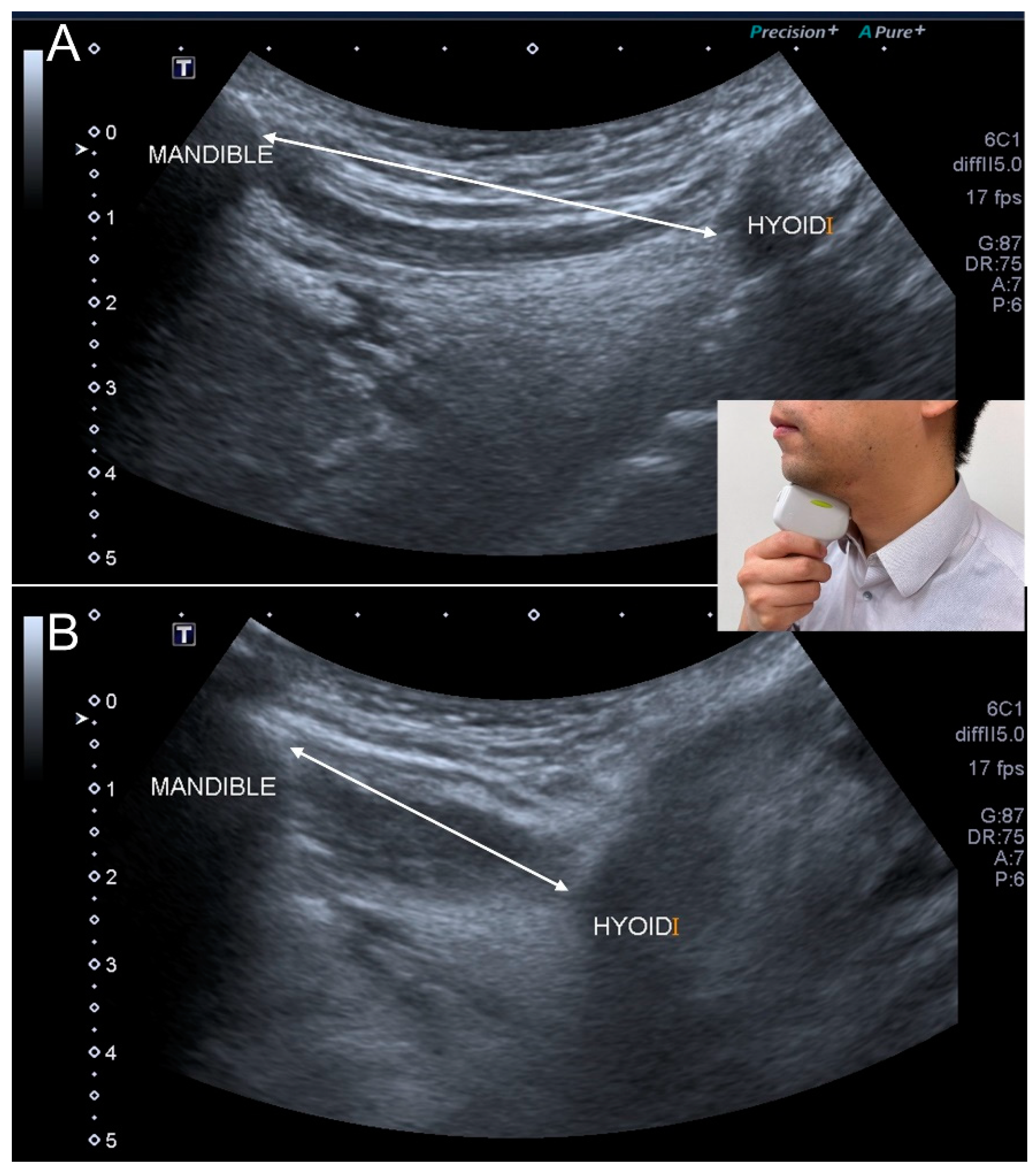
3.9. Ultrasonography
3.10. Magnetic Resonance Imaging
4. Intervention
4.1. Overview
4.2. Swallowing Muscle Strengthening
4.3. Nutrition Support
4.4. Physical and Occupational Therapy
4.5. Texture Modification of Food
5. Future Perspectives
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef]
- Rosenberg, I.H. Sarcopenia: Origins and clinical relevance. J. Nutr. 1997, 127, 990S–991S. [Google Scholar] [CrossRef]
- Fujishima, I.; Fujiu-Kurachi, M.; Arai, H.; Hyodo, M.; Kagaya, H.; Maeda, K.; Mori, T.; Nishioka, S.; Oshima, F.; Ogawa, S.; et al. Sarcopenia and dysphagia: Position paper by four professional organizations. Geriatr. Gerontol. Int. 2019, 19, 91–97. [Google Scholar] [CrossRef]
- Maeda, K.; Takaki, M.; Akagi, J. Decreased Skeletal Muscle Mass and Risk Factors of Sarcopenic Dysphagia: A Prospective Observational Cohort Study. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 1290–1294. [Google Scholar] [CrossRef]
- Cha, S.; Kim, W.S.; Kim, K.W.; Han, J.W.; Jang, H.C.; Lim, S.; Paik, N.J. Sarcopenia is an Independent Risk Factor for Dysphagia in Community-Dwelling Older Adults. Dysphagia 2019, 34, 692–697. [Google Scholar] [CrossRef]
- Vandewoude, M.F.; Alish, C.J.; Sauer, A.C.; Hegazi, R.A. Malnutrition-sarcopenia syndrome: Is this the future of nutrition screening and assessment for older adults? J. Aging Res. 2012, 2012, 651570. [Google Scholar] [CrossRef]
- Grimby, G.; Saltin, B. The ageing muscle. Clin. Physiol. 1983, 3, 209–218. [Google Scholar] [CrossRef]
- Pizzoferrato, M.; de Sire, R.; Ingravalle, F.; Mentella, M.C.; Petito, V.; Martone, A.M.; Landi, F.; Miggiano, G.A.D.; Mele, M.C.; Lopetuso, L.R.; et al. Characterization of Sarcopenia in an IBD Population Attending an Italian Gastroenterology Tertiary Center. Nutrients 2019, 11, 2281. [Google Scholar] [CrossRef]
- Nardone, O.M.; de Sire, R.; Petito, V.; Testa, A.; Villani, G.; Scaldaferri, F.; Castiglione, F. Inflammatory Bowel Diseases and Sarcopenia: The Role of Inflammation and Gut Microbiota in the Development of Muscle Failure. Front. Immunol. 2021, 12, 694217. [Google Scholar] [CrossRef]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 601. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Landi, F.; Schneider, S.M.; Zuniga, C.; Arai, H.; Boirie, Y.; Chen, L.K.; Fielding, R.A.; Martin, F.C.; Michel, J.P.; et al. Prevalence of and interventions for sarcopenia in ageing adults: A systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing 2014, 43, 748–759. [Google Scholar] [CrossRef]
- Ogawa, N.; Mori, T.; Fujishima, I.; Wakabayashi, H.; Itoda, M.; Kunieda, K.; Shigematsu, T.; Nishioka, S.; Tohara, H.; Yamada, M.; et al. Ultrasonography to Measure Swallowing Muscle Mass and Quality in Older Patients With Sarcopenic Dysphagia. J. Am. Med. Dir. Assoc. 2018, 19, 516–522. [Google Scholar] [CrossRef]
- Shiozu, H.; Higashijima, M.; Koga, T. Association of sarcopenia with swallowing problems, related to nutrition and activities of daily living of elderly individuals. J. Phys. Ther. Sci. 2015, 27, 393–396. [Google Scholar] [CrossRef]
- Dellis, S.; Papadopoulou, S.; Krikonis, K.; Zigras, F. Sarcopenic Dysphagia. A Narrative Review. J. Frailty Sarcopenia Falls 2018, 3, 1–7. [Google Scholar] [CrossRef]
- Baijens, L.W.; Clave, P.; Cras, P.; Ekberg, O.; Forster, A.; Kolb, G.F.; Leners, J.C.; Masiero, S.; Mateos-Nozal, J.; Ortega, O.; et al. European Society for Swallowing Disorders—European Union Geriatric Medicine Society white paper: Oropharyngeal dysphagia as a geriatric syndrome. Clin. Interv. Aging 2016, 11, 1403–1428. [Google Scholar] [CrossRef]
- White, G.N.; O’Rourke, F.; Ong, B.S.; Cordato, D.J.; Chan, D.K. Dysphagia: Causes, assessment, treatment, and management. Geriatrics 2008, 63, 15–20. [Google Scholar]
- Dodds, W.J. Physiology of swallowing. Dysphagia 1989, 3, 171–178. [Google Scholar] [CrossRef]
- Tamura, F.; Kikutani, T.; Tohara, T.; Yoshida, M.; Yaegaki, K. Tongue thickness relates to nutritional status in the elderly. Dysphagia 2012, 27, 556–561. [Google Scholar] [CrossRef]
- Feng, X.; Todd, T.; Lintzenich, C.R.; Ding, J.; Carr, J.J.; Ge, Y.; Browne, J.D.; Kritchevsky, S.B.; Butler, S.G. Aging-related geniohyoid muscle atrophy is related to aspiration status in healthy older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 853–860. [Google Scholar] [CrossRef]
- Molfenter, S.M.; Amin, M.R.; Branski, R.C.; Brumm, J.D.; Hagiwara, M.; Roof, S.A.; Lazarus, C.L. Age-Related Changes in Pharyngeal Lumen Size: A Retrospective MRI Analysis. Dysphagia 2015, 30, 321–327. [Google Scholar] [CrossRef]
- Wakabayashi, H. Presbyphagia and Sarcopenic Dysphagia: Association between Aging, Sarcopenia, and Deglutition Disorders. J. Frailty Aging 2014, 3, 97–103. [Google Scholar] [CrossRef]
- Nishioka, S.; Okamoto, T.; Takayama, M.; Urushihara, M.; Watanabe, M.; Kiriya, Y.; Shintani, K.; Nakagomi, H.; Kageyama, N. Malnutrition risk predicts recovery of full oral intake among older adult stroke patients undergoing enteral nutrition: Secondary analysis of a multicentre survey (the APPLE study). Clin. Nutr. 2017, 36, 1089–1096. [Google Scholar] [CrossRef]
- Mori, T.; Fujishima, I.; Wakabayashi, H.; Oshima, F.; Itoda, M.; Kunieda, K.; Kayashita, J.; Nishioka, S.; Sonoda, A.; Kuroda, Y.; et al. Development, reliability, and validity of a diagnostic algorithm for sarcopenic dysphagia. JCSM Clin. Rep. 2017, 2, 1–10. [Google Scholar] [CrossRef]
- Wakabayashi, H.; Takahashi, R.; Murakami, T. The Prevalence and Prognosis of Sarcopenic Dysphagia in Patients Who Require Dysphagia Rehabilitation. J. Nutr. Health Aging 2019, 23, 84–88. [Google Scholar] [CrossRef]
- Belafsky, P.C.; Mouadeb, D.A.; Rees, C.J.; Pryor, J.C.; Postma, G.N.; Allen, J.; Leonard, R.J. Validity and reliability of the Eating Assessment Tool (EAT-10). Ann. Otol. Rhinol. Laryngol. 2008, 117, 919–924. [Google Scholar] [CrossRef]
- Wakabayashi, H.; Takahashi, R.; Watanabe, N.; Oritsu, H.; Shimizu, Y. Prevalence of sarcopenia and its association with dysphagia in cancer patients who require rehabilitation. J. Rehabil. Med. 2017, 49, 682–685. [Google Scholar] [CrossRef]
- Firat Ozer, F.; Akin, S.; Soysal, T.; Gokcekuyu, B.M.; Erturk Zararsiz, G. Relationship Between Dysphagia and Sarcopenia with Comprehensive Geriatric Evaluation. Dysphagia 2021, 36, 140–146. [Google Scholar] [CrossRef]
- Saitoh, E.; Pongpipatpaiboon, K.; Inamoto, Y.; Kagaya, H. Dysphagia Evaluation and Treatment; Springer: Singapore, 2018; Available online: https://link.springer.com/book/10.1007/978-981-10-5032-9 (accessed on 18 October 2021).
- O’Neil, K.H.; Purdy, M.; Falk, J.; Gallo, L. The Dysphagia Outcome and Severity Scale. Dysphagia 1999, 14, 139–145. [Google Scholar] [CrossRef]
- Yoshimatsu, Y. Predictive Roles of the Repetitive Saliva Swallowing Test (RSST) in Aspiration Pneumonia and Other Respiratory Diseases. In Aspiration Pneumonia; Springer: Singapore, 2020; pp. 131–141. [Google Scholar] [CrossRef]
- Persson, E.; Wardh, I.; Ostberg, P. Repetitive Saliva Swallowing Test: Norms, Clinical Relevance and the Impact of Saliva Secretion. Dysphagia 2019, 34, 271–278. [Google Scholar] [CrossRef]
- Crary, M.A.; Mann, G.D.; Groher, M.E. Initial psychometric assessment of a functional oral intake scale for dysphagia in stroke patients. Arch. Phys. Med. Rehabil. 2005, 86, 1516–1520. [Google Scholar] [CrossRef]
- Nagano, A.; Maeda, K.; Shimizu, A.; Nagami, S.; Takigawa, N.; Ueshima, J.; Suenaga, M. Association of Sarcopenic Dysphagia with Underlying Sarcopenia Following Hip Fracture Surgery in Older Women. Nutrients 2020, 12, 1365. [Google Scholar] [CrossRef]
- Maeda, K.; Akagi, J. Sarcopenia is an independent risk factor of dysphagia in hospitalized older people. Geriatr. Gerontol. Int. 2016, 16, 515–521. [Google Scholar] [CrossRef]
- Silva, P.B.; Ramos, G.H.A.; Petterle, R.R.; Borba, V.Z.C. Sarcopenia as an early complication of patients with head and neck cancer with dysphagia. Eur. J. Cancer Care 2021, 30, e13343. [Google Scholar] [CrossRef]
- Kunieda, K.; Ohno, T.; Fujishima, I.; Hojo, K.; Morita, T. Reliability and validity of a tool to measure the severity of dysphagia: The Food Intake LEVEL Scale. J. Pain Symptom Manag. 2013, 46, 201–206. [Google Scholar] [CrossRef]
- Wakabayashi, H.; Matsushima, M.; Uwano, R.; Watanabe, N.; Oritsu, H.; Shimizu, Y. Skeletal muscle mass is associated with severe dysphagia in cancer patients. J. Cachexia Sarcopenia Muscle 2015, 6, 351–357. [Google Scholar] [CrossRef]
- Wakabayashi, H.; Takahashi, R.; Watanabe, N.; Oritsu, H.; Shimizu, Y. Prevalence of skeletal muscle mass loss and its association with swallowing function after cardiovascular surgery. Nutrition 2017, 38, 70–73. [Google Scholar] [CrossRef]
- Yoshimura, Y.; Wakabayashi, H.; Bise, T.; Tanoue, M. Prevalence of sarcopenia and its association with activities of daily living and dysphagia in convalescent rehabilitation ward inpatients. Clin. Nutr. 2018, 37, 2022–2028. [Google Scholar] [CrossRef]
- Suzuki, M.; Kimura, Y.; Otobe, Y.; Kikuchi, T.; Masuda, H.; Taguchi, R.; Tanaka, S.; Narita, Y.; Shino, S.; Kusumi, H.; et al. Relationship between Sarcopenia and Swallowing Capacity in Community-Dwelling Older Women. Gerontology 2020, 66, 549–552. [Google Scholar] [CrossRef]
- Tohara, H.; Saitoh, E.; Mays, K.A.; Kuhlemeier, K.; Palmer, J.B. Three tests for predicting aspiration without videofluorography. Dysphagia 2003, 18, 126–134. [Google Scholar] [CrossRef]
- Yagi, N.; Oku, Y.; Nagami, S.; Yamagata, Y.; Kayashita, J.; Ishikawa, A.; Domen, K.; Takahashi, R. Inappropriate Timing of Swallow in the Respiratory Cycle Causes Breathing-Swallowing Discoordination. Front. Physiol. 2017, 8, 676. [Google Scholar] [CrossRef]
- Murakami, K.; Hirano, H.; Watanabe, Y.; Edahiro, A.; Ohara, Y.; Yoshida, H.; Kim, H.; Takagi, D.; Hironaka, S. Relationship between swallowing function and the skeletal muscle mass of older adults requiring long-term care. Geriatr. Gerontol. Int. 2015, 15, 1185–1192. [Google Scholar] [CrossRef]
- Zenner, P.M.; Losinski, D.S.; Mills, R.H. Using cervical auscultation in the clinical dysphagia examination in long-term care. Dysphagia 1995, 10, 27–31. [Google Scholar] [CrossRef]
- Sudo, E.; Tanuma, S.; Sudo, E.; Takahashi, Y.; Yoshida, A.; Kobayashi, C.; Ohama, Y. The usefulness of the water swallowing test and videofluorography in swallowing rehabilitation in patients with cerebrovascular disease. Nihon Ronen Igakkai Zasshi 2002, 39, 427–432. [Google Scholar] [CrossRef][Green Version]
- Sagawa, K.; Kikutani, T.; Tamura, F.; Yoshida, M. Factors related to skeletal muscle mass in the frail elderly. Odontology 2017, 105, 91–95. [Google Scholar] [CrossRef]
- Hashida, N.; Shamoto, H.; Maeda, K.; Wakabayashi, H.; Suzuki, M.; Fujii, T. Rehabilitation and nutritional support for sarcopenic dysphagia and tongue atrophy after glossectomy: A case report. Nutrition 2017, 35, 128–131. [Google Scholar] [CrossRef]
- Nakayama, E.; Tohara, H.; Sato, M.; Hino, H.; Sakai, M.; Nagashima, Y.; Kimura, M.; Watanabe, M.; Ooshima, M. Time Course and Recovery of the Movements of Hyoid Bone and Thyroid Cartilage During Swallowing in a Patient With Sarcopenic Dysphagia. Am. J. Phys. Med. Rehabil. 2020, 99, e64–e67. [Google Scholar] [CrossRef]
- Miyashita, T.; Kikutani, T.; Nagashima, K.; Igarashi, K.; Tamura, F. The effects of sarcopenic dysphagia on the dynamics of swallowing organs observed on videofluoroscopic swallowing studies. J. Oral Rehabil. 2020, 47, 584–590. [Google Scholar] [CrossRef]
- Maeda, K.; Akagi, J. Decreased tongue pressure is associated with sarcopenia and sarcopenic dysphagia in the elderly. Dysphagia 2015, 30, 80–87. [Google Scholar] [CrossRef]
- Sakai, K.; Nakayama, E.; Tohara, H.; Maeda, T.; Sugimoto, M.; Takehisa, T.; Takehisa, Y.; Ueda, K. Tongue Strength is Associated with Grip Strength and Nutritional Status in Older Adult Inpatients of a Rehabilitation Hospital. Dysphagia 2017, 32, 241–249. [Google Scholar] [CrossRef]
- Kaji, A.; Hashimoto, Y.; Kobayashi, Y.; Sakai, R.; Okamura, T.; Miki, A.; Hamaguchi, M.; Kuwahata, M.; Yamazaki, M.; Fukui, M. Sarcopenia is associated with tongue pressure in older patients with type 2 diabetes: A cross-sectional study of the KAMOGAWA-DM cohort study. Geriatr. Gerontol. Int. 2019, 19, 153–158. [Google Scholar] [CrossRef]
- Suzuki, M.; Koyama, S.; Kimura, Y.; Ishiyama, D.; Otobe, Y.; Nishio, N.; Ichikawa, T.; Kunieda, Y.; Ohji, S.; Ito, D.; et al. Relationship between characteristics of skeletal muscle and oral function in community-dwelling older women. Arch. Gerontol. Geriatr. 2018, 79, 171–175. [Google Scholar] [CrossRef]
- Kobuchi, R.; Okuno, K.; Kusunoki, T.; Inoue, T.; Takahashi, K. The relationship between sarcopenia and oral sarcopenia in elderly people. J. Oral Rehabil. 2020, 47, 636–642. [Google Scholar] [CrossRef]
- Chang, K.V.; Wu, W.T.; Chen, L.R.; Wang, H.I.; Wang, T.G.; Han, D.S. Suboptimal Tongue Pressure Is Associated with Risk of Malnutrition in Community-Dwelling Older Individuals. Nutrients 2021, 13, 1821. [Google Scholar] [CrossRef]
- Chen, K.C.; Lee, T.M.; Wu, W.T.; Wang, T.G.; Han, D.S.; Chang, K.V. Assessment of Tongue Strength in Sarcopenia and Sarcopenic Dysphagia: A Systematic Review and Meta-Analysis. Front. Nutr. 2021, 8, 684840. [Google Scholar] [CrossRef]
- Machida, N.; Tohara, H.; Hara, K.; Kumakura, A.; Wakasugi, Y.; Nakane, A.; Minakuchi, S. Effects of aging and sarcopenia on tongue pressure and jaw-opening force. Geriatr. Gerontol. Int. 2017, 17, 295–301. [Google Scholar] [CrossRef]
- Sakai, K.; Nakayama, E.; Tohara, H.; Takahashi, O.; Ohnishi, S.; Tsuzuki, H.; Hayata, M.; Takehisa, T.; Takehisa, Y.; Ueda, K. Diagnostic accuracy of lip force and tongue strength for sarcopenic dysphagia in older inpatients: A cross-sectional observational study. Clin. Nutr. 2019, 38, 303–309. [Google Scholar] [CrossRef]
- Vaiman, M.; Eviatar, E.; Segal, S. Evaluation of normal deglutition with the help of rectified surface electromyography records. Dysphagia 2004, 19, 125–132. [Google Scholar] [CrossRef]
- Sakai, K.; Nakayama, E.; Rogus-Pulia, N.; Takehisa, T.; Takehisa, Y.; Urayama, K.Y.; Takahashi, O. Submental Muscle Activity and Its Role in Diagnosing Sarcopenic Dysphagia. Clin. Interv. Aging 2020, 15, 1991–1999. [Google Scholar] [CrossRef]
- Nativ-Zeltzer, N.; Kahrilas, P.J.; Logemann, J.A. Manofluorography in the evaluation of oropharyngeal dysphagia. Dysphagia 2012, 27, 151–161. [Google Scholar] [CrossRef]
- Kunieda, K.; Fujishima, I.; Wakabayashi, H.; Ohno, T.; Shigematsu, T.; Itoda, M.; Oshima, F.; Mori, T.; Ogawa, N.; Ogawa, S. Relationship Between Tongue Pressure and Pharyngeal Function Assessed Using High-Resolution Manometry in Older Dysphagia Patients with Sarcopenia: A Pilot Study. Dysphagia 2021, 36, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Dodds, W.J.; Stewart, E.T.; Logemann, J.A. Physiology and radiology of the normal oral and pharyngeal phases of swallowing. AJR Am. J. Roentgenol. 1990, 154, 953–963. [Google Scholar] [CrossRef]
- Gervasio, A.; D’Orta, G.; Mujahed, I.; Biasio, A. Sonographic anatomy of the neck: The suprahyoid region. J. Ultrasound 2011, 14, 130–135. [Google Scholar] [CrossRef]
- Mori, T.; Wakabayashi, H.; Ogawa, N.; Fujishima, I.; Oshima, F.; Itoda, M.; Kunieda, K.; Shigematsu, T.; Nishioka, S.; Tohara, H.; et al. The Mass of Geniohyoid Muscle Is Associated with Maximum Tongue Pressure and Tongue Area in Patients with Sarcopenic Dysphagia. J. Nutr. Health Aging 2021, 25, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, N.; Wakabayashi, H.; Mori, T.; Fujishima, I.; Oshima, F.; Itoda, M.; Kunieda, K.; Shigematsu, T.; Nishioka, S.; Tohara, H.; et al. Digastric muscle mass and intensity in older patients with sarcopenic dysphagia by ultrasonography. Geriatr. Gerontol. Int. 2021, 21, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Chen, P.Y.; Wang, Y.C.; Wang, T.G.; Han, D.S. Decreased swallowing function in the sarcopenic elderly without clinical dysphagia: A cross-sectional study. BMC Geriatr. 2020, 20, 419. [Google Scholar] [CrossRef]
- Sakai, K.; Katayama, M.; Nakajima, J.; Inoue, S.; Koizumi, K.; Okada, S.; Suga, S.; Nomura, T.; Matsuura, N. Temporal muscle thickness is associated with the severity of dysphagia in patients with acute stroke. Arch. Gerontol. Geriatr. 2021, 96, 104439. [Google Scholar] [CrossRef]
- Nakao, Y.; Uchiyama, Y.; Honda, K.; Yamashita, T.; Saito, S.; Domen, K. Age-related composition changes in swallowing-related muscles: A Dixon MRI study. Aging Clin. Exp. Res. 2021. [Google Scholar] [CrossRef]
- Nakao, Y.; Yamashita, T.; Honda, K.; Katsuura, T.; Hama, Y.; Nakamura, Y.; Ando, K.; Ishikura, R.; Kodama, N.; Uchiyama, Y.; et al. Association Among Age-Related Tongue Muscle Abnormality, Tongue Pressure, and Presbyphagia: A 3D MRI Study. Dysphagia 2021, 36, 483–491. [Google Scholar] [CrossRef]
- Koyama, T.; Shamoto, H.; Anzai, H.; Koganei, Y.; Maeda, K.; Wakabayashi, H. Multidisciplinary Comprehensive Care for Early Recommencement of Oral Intake in Older Adults With Severe Pneumonia. J. Gerontol. Nurs. 2016, 42, 21–29. [Google Scholar] [CrossRef]
- Bakhtiyari, J.; Sarraf, P.; Nakhostin-Ansari, N.; Tafakhori, A.; Logemann, J.; Faghihzadeh, S.; Harirchian, M.H. Effects of early intervention of swallowing therapy on recovery from dysphagia following stroke. Iran. J. Neurol. 2015, 14, 119–124. [Google Scholar]
- Clave, P.; Shaker, R. Dysphagia: Current reality and scope of the problem. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 259–270. [Google Scholar] [CrossRef]
- Kim, H.D.; Choi, J.B.; Yoo, S.J.; Chang, M.Y.; Lee, S.W.; Park, J.S. Tongue-to-palate resistance training improves tongue strength and oropharyngeal swallowing function in subacute stroke survivors with dysphagia. J. Oral Rehabil. 2017, 44, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Robbins, J.; Gangnon, R.E.; Theis, S.M.; Kays, S.A.; Hewitt, A.L.; Hind, J.A. The effects of lingual exercise on swallowing in older adults. J. Am. Geriatr. Soc. 2005, 53, 1483–1489. [Google Scholar] [CrossRef] [PubMed]
- Namiki, C.; Hara, K.; Tohara, H.; Kobayashi, K.; Chantaramanee, A.; Nakagawa, K.; Saitou, T.; Yamaguchi, K.; Yoshimi, K.; Nakane, A.; et al. Tongue-pressure resistance training improves tongue and suprahyoid muscle functions simultaneously. Clin. Interv. Aging 2019, 14, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Nagano, A.; Nishioka, S.; Wakabayashi, H. Rehabilitation Nutrition for Iatrogenic Sarcopenia and Sarcopenic Dysphagia. J. Nutr. Health Aging 2019, 23, 256–265. [Google Scholar] [CrossRef]
- Gielen, E.; Beckwee, D.; Delaere, A.; De Breucker, S.; Vandewoude, M.; Bautmans, I.; Sarcopenia Guidelines Development Group of the Belgian Society of Gerontology and Geriatrics (BSGG). Nutritional interventions to improve muscle mass, muscle strength, and physical performance in older people: An umbrella review of systematic reviews and meta-analyses. Nutr. Rev. 2021, 79, 121–147. [Google Scholar] [CrossRef]
- Uno, C.; Maeda, K.; Wakabayashi, H.; Nishioka, S.; Ogawa, N.; Okamoto, T.; Hoyano, K.; Momosaki, R. Nutritional status change and activities of daily living in elderly pneumonia patients admitted to acute care hospital: A retrospective cohort study from the Japan Rehabilitation Nutrition Database. Nutrition 2020, 71, 110613. [Google Scholar] [CrossRef]
- Nagano, A.; Maeda, K.; Koike, M.; Murotani, K.; Ueshima, J.; Shimizu, A.; Inoue, T.; Sato, K.; Suenaga, M.; Ishida, Y.; et al. Effects of Physical Rehabilitation and Nutritional Intake Management on Improvement in Tongue Strength in Sarcopenic Patients. Nutrients 2020, 12, 3104. [Google Scholar] [CrossRef]
- Shimizu, A.; Fujishima, I.; Maeda, K.; Wakabayashi, H.; Nishioka, S.; Ohno, T.; Nomoto, A.; Kayashita, J.; Mori, N.; The Japanese Working Group On Sarcopenic, D. Nutritional Management Enhances the Recovery of Swallowing Ability in Older Patients with Sarcopenic Dysphagia. Nutrients 2021, 13, 596. [Google Scholar] [CrossRef] [PubMed]
- Tanıgör, G.; Eyigor, S. Evaluation of dysphagia in patients with sarcopenia in a rehabilitation setting: Insights from the vicious cycle. Eur. Geriatr. Med. 2020, 11, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Maeda, K.; Akagi, J. Treatment of Sarcopenic Dysphagia with Rehabilitation and Nutritional Support: A Comprehensive Approach. J. Acad. Nutr. Diet 2016, 116, 573–577. [Google Scholar] [CrossRef]
- Carrion, S.; Roca, M.; Costa, A.; Arreola, V.; Ortega, O.; Palomera, E.; Serra-Prat, M.; Cabre, M.; Clave, P. Nutritional status of older patients with oropharyngeal dysphagia in a chronic versus an acute clinical situation. Clin. Nutr. 2017, 36, 1110–1116. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Criteria |
|---|---|
| 1 | Presence of dysphagia |
| 2 | Presence of whole-body sarcopenia |
| 3 | The results of imaging tests (computed tomography, magnetic resonance imaging, ultrasonography) are consistent with loss of swallowing muscle mass |
| 4 | The causes of dysphagia are excluded except for sarcopenia |
| 5 | The main cause of dysphagia is considered to be sarcopenia |
| Evaluating Target | Tools |
|---|---|
| Muscle mass | Dual-energy X-ray absorptiometry (DXA), bioimpedance analysis (BIA) |
| Muscle strength | Dynamometer |
| Physical performance | Six-minute walk test (6MWT), Short Physical Performance Battery score (SPPB), five-time chair stand test (5TSTS), timed up-and-go test (TUG), 400 m walk test (400MWT) |
| Swallowing function | Eating Assessment Tool (EAT-10), dysphagia severity scale (DSS), repetitive saliva swallowing Test (RSST), Functional Oral Intake Scale (FOIS), Food Intake Level Scale (FILS), modified water swallowing test (MWST), videofluoroscopy swallowing study (VFSS) |
| Swallowing muscle strength | JMS tongue pressure measuring instrument (JMS, Hiroshima, Japan), Iowa Oral Performance Instrument (IOPI), jaw-opening force trainer KT2016 (Livet Inc., Tokyo, Japan), Lip de Cum (Cosmo Instruments Co., Ltd., Tokyo, Japan), surface electromyography(sEMG), high-resolution manometry (HRM) |
| Swallowing muscle mass | Ultrasonography, magnetic resonance imaging (MRI) |
| Evaluating Tool | Cut-Off Point |
|---|---|
| Muscle mass | |
| Dual-energy X-ray absorptiometry(DXA) | <7.0 kg/m2 in men and <5.5 kg/m2 in women a <7.0 kg/m2 in men and <5.4 kg/m2 in women b |
| Bioimpedance analysis (BIA) | <7.0 kg/m2 in men and <5.5 kg/m2 in women a <7.0 kg/m2 in men and <5.7 kg/m2 in women b |
| Muscle strength | |
| Dynamometer | <27 kg for men and <16 kg for women a <28 kg for men and <18 kg for women b |
| Physical Performance | |
| 6 min walk | <0.8 m/s a <1.0 m/s b |
| Short Physical Performance Battery | ≤8 a ≤9 b |
| 5-time chair stand test | ≥15 s a ≥12 s b |
| Timed up-and-go test | ≥20 s a |
| 400 m walk | ≥6 min a |
| Swallowing function | |
| Eating Assessment Tool (EAT-10) | ≥3 |
| Dysphagia severity scale (DSS) | ≤4 |
| Repetitive saliva swallowing Test (RSST) | ≤2 |
| Functional Oral Intake Scale (FOIS) | ≤5 |
| Food Intake Level Scale (FILS) | Not available |
| Modified water swallowing test (MWST) | Not available |
| Videofluoroscopy swallowing study (VFSS) | Not available |
| Swallowing muscle strength | |
| Maximal isometric tongue pressure | <20 kPa |
| Jaw-opening force | Not available |
| Lip force | <10.4 Newton for men and <8.5 Newton for women |
| Surface electromyography (sEMG) | <387.09% of jaw open contraction for maximal amplitude <1.96 s for total duration |
| High-resolution manometry (HRM) | Not available |
| Swallowing muscle mass | |
| Ultrasonography | <1536 mm2 for the cross-sectional area of the tongue muscle <75.1 mm2 for the cross-sectional area of the digastric muscle |
| Magnetic resonance imaging (MRI) | Not available |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, K.-C.; Jeng, Y.; Wu, W.-T.; Wang, T.-G.; Han, D.-S.; Özçakar, L.; Chang, K.-V. Sarcopenic Dysphagia: A Narrative Review from Diagnosis to Intervention. Nutrients 2021, 13, 4043. https://doi.org/10.3390/nu13114043
Chen K-C, Jeng Y, Wu W-T, Wang T-G, Han D-S, Özçakar L, Chang K-V. Sarcopenic Dysphagia: A Narrative Review from Diagnosis to Intervention. Nutrients. 2021; 13(11):4043. https://doi.org/10.3390/nu13114043
Chicago/Turabian StyleChen, Kuan-Cheng, Ying Jeng, Wei-Ting Wu, Tyng-Guey Wang, Der-Sheng Han, Levent Özçakar, and Ke-Vin Chang. 2021. "Sarcopenic Dysphagia: A Narrative Review from Diagnosis to Intervention" Nutrients 13, no. 11: 4043. https://doi.org/10.3390/nu13114043
APA StyleChen, K.-C., Jeng, Y., Wu, W.-T., Wang, T.-G., Han, D.-S., Özçakar, L., & Chang, K.-V. (2021). Sarcopenic Dysphagia: A Narrative Review from Diagnosis to Intervention. Nutrients, 13(11), 4043. https://doi.org/10.3390/nu13114043