Chronotype and Adherence to the Mediterranean Diet in Obesity: Results from the Opera Prevention Project


 ,
, 
 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Settings, Participants and Protocol
2.2. Sample Size Justification and Power
2.3. Data Collection
2.3.1. Anthropometric Parameters
2.3.2. Adherence to the Mediterranean Diet
2.3.3. Assessment of Chronotype
2.4. Statistical Analysis
3. Results
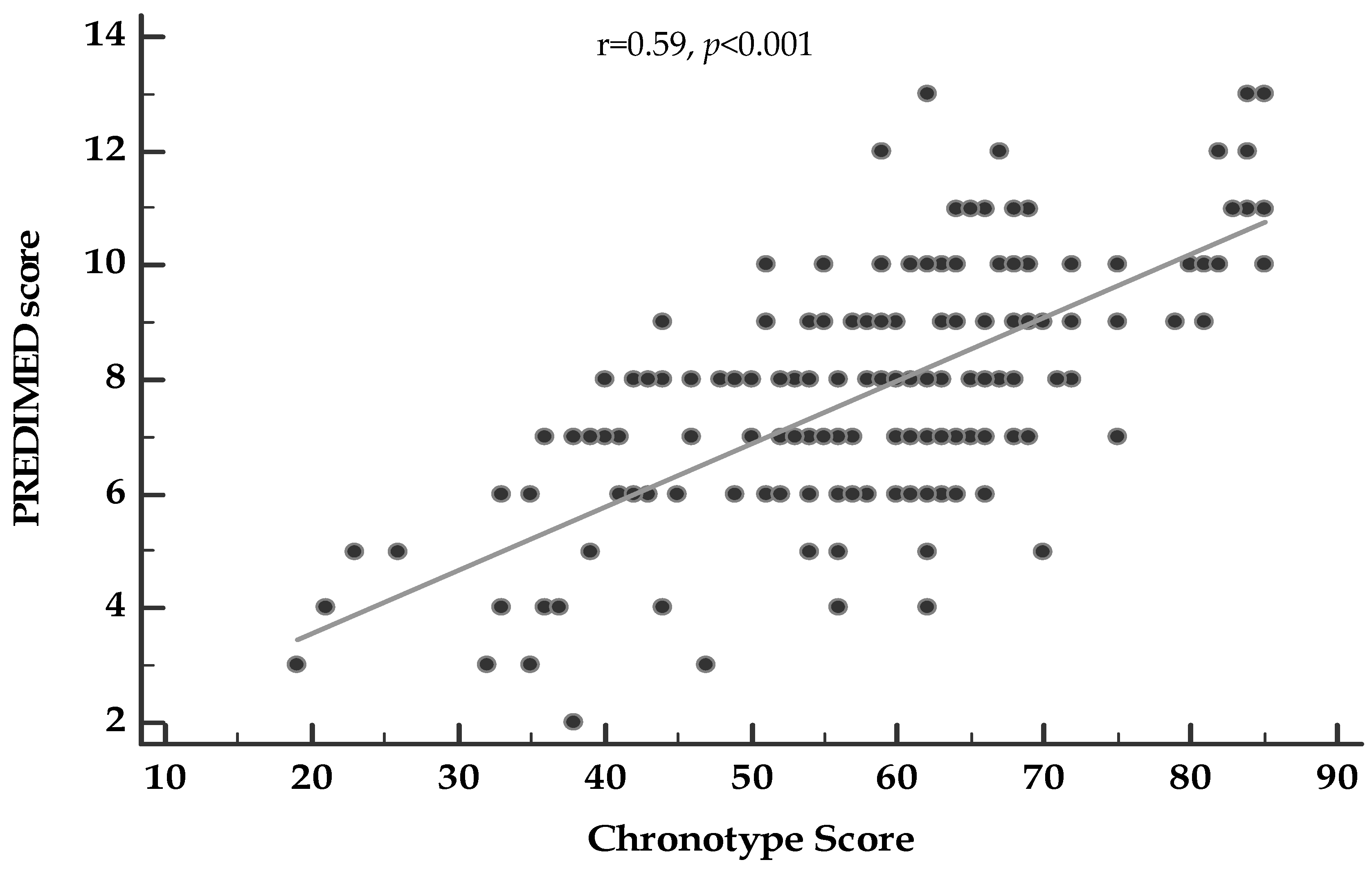
Correlation Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Mongrain, V.; Lavoie, S.; Selmaoui, B.; Paquet, J.; Dumont, M. Phase relationships between sleep-wake cycle and underlying circadian rhythms in morningness-eveningness. J. Biol. Rhythms. 2004, 19, 248–257. [Google Scholar] [CrossRef] [PubMed]
- Adan, A.; Natale, V. Gender differences in morningness-even preference. Chronobiol. Int. 2002, 19, 709–720. [Google Scholar] [CrossRef] [PubMed]
- Horne, J.A.; Ostberg, O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int. J. Chronobiol. 1976, 4, 97–110. [Google Scholar] [PubMed]
- Makarem, N.; Paul, J.; Giardina, E.V.; Liao, M.; Aggarwal, B. Evening chronotype is associated with poor cardiovascular health and adverse health behaviors in a diverse population of women. Chronobiol. Int. 2020, 1–13. [Google Scholar] [CrossRef]
- Yu, J.H.; Yun, C.H.; Ahn, J.H.; Suh, S.; Cho, H.J.; Lee, S.K.; Yoo, H.J.; Seo, J.A.; Kim, S.G.; Choi, K.M.; et al. Evening chronotype is associated with metabolic disorders and body composition in middle-aged adults. J. Clin. Endocrinol. Metab. 2015, 100, 1494–1502. [Google Scholar] [CrossRef]
- Arble, D.M.; Bass, J.; Laposky, A.D.; Vitaterna, M.H.; Turek, F.W. Circadian timing of food intake contributes to weight gain. Obesity 2009, 17, 2100–2102. [Google Scholar] [CrossRef]
- Hatori, M.; Vollmers, C.; Zarrinpar, A.; DiTacchio, L.; Bushong, E.A.; Gill, S.; Leblanc, M.; Chaix, A.; Joens, M.; Fitzpatrick, J.A.; et al. Time-restricted feeding without reducing caloric intake prevents metabolic diseases in mice fed a high-fat diet. Cell Metab. 2012, 15, 848–860. [Google Scholar] [CrossRef]
- Panda, S. Circadian physiology of metabolism. Science 2016, 354, 1008–1015. [Google Scholar] [CrossRef]
- Merikanto, I.; Kronholm, E.; Peltonen, M.; Laatikainen, T.; Lahti, T.; Partonen, T. Relation of chronotype to sleep complaints in the general Finnish population. Chronobiol. Int. 2012, 29, 311–317. [Google Scholar] [CrossRef]
- Pugliese, G.; Barrea, L.; Laudisio, D.; Salzano, C.; Aprano, S.; Colao, A.; Savastano, S.; Muscogiuri, G. Sleep Apnea, Obesity, and Disturbed Glucose Homeostasis: Epidemiologic Evidence, Biologic Insights, and Therapeutic Strategies. Curr. Obes. Rep. 2020, 9, 30–38. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Barrea, L.; Scannapieco, M.; Di Somma, C.; Scacchi, M.; Aimaretti, G.; Savastano, S.; Colao, A.; Marzullo, P. The lullaby of the sun: The role of vitamin D in sleep disturbance. Sleep Med. 2019, 54, 262–265. [Google Scholar] [CrossRef] [PubMed]
- Muscogiuri, G.; Barrea, L.; Annunziata, G.; Di Somma, C.; Laudisio, D.; Colao, A.; Savastano, S. Obesity and sleep disturbance: The chicken or the egg? Crit. Rev. Food Sci. Nutr. 2019, 59, 2158–2165. [Google Scholar] [CrossRef] [PubMed]
- Baron, K.G.; Reid, K.J.; Kern, A.S.; Zee, P.C. Role of sleep timing in caloric intake and BMI. Obesity 2011, 19, 1374–1381. [Google Scholar] [CrossRef] [PubMed]
- Mota, M.C.; Waterhouse, J.; De-Souza, D.A.; Rossato, L.T.; Silva, C.M.; Araújo, M.B.; Tufik, S.; de Mello, M.T.; Crispim, C.A. Association between chronotype, food intake and physical activity in medical residents. Chronobiol. Int. 2016, 33, 730–739. [Google Scholar] [CrossRef]
- Gontijo, C.A.; Cabral, B.B.M.; Balieiro, L.C.T.; Teixeira, G.P.; Fahmy, W.M.; Maia, Y.C.P.; Crispim, C.A. Time-related eating patterns and chronotype are associated with diet quality in pregnant women. Chronobiol. Int. 2019, 36, 75–84. [Google Scholar] [CrossRef]
- Roßbach, S.; Diederichs, T.; Nöthlings, U.; Buyken, A.E.; Alexy, U. Relevance of chronotype for eating patterns in adolescents. Chronobiol. Int. 2018, 35, 336–347. [Google Scholar] [CrossRef]
- Sato-Mito, N.; Shibata, S.; Sasaki, S.; Sato, K. Dietary intake is associated with human chronotype as assessed by both morningness-eveningness score and preferred midpoint of sleep in young Japanese women. Int. J. Food Sci. Nutr. 2011, 62, 525–532. [Google Scholar] [CrossRef]
- The OPERA Prevention Project. Int. J. Food Sci. Nutr. 2020. [CrossRef]
- Wong, P.M.; Hasler, B.P.; Kamarck, T.W.; Muldoon, M.F.; Manuck, S.B. Social Jetlag, Chronotype, and Cardiometabolic Risk. J. Clin. Endocrinol. Metab. 2015, 100, 4612–4620. [Google Scholar] [CrossRef]
- Barrea, L.; Arnone, A.; Annunziata, G.; Muscogiuri, G.; Laudisio, D.; Salzano, C.; Pugliese, G.; Colao, A.; Savastano, S. Adherence to the Mediterranean Diet, Dietary Patterns and Body Composition in Women with Polycystic Ovary Syndrome (PCOS). Nutrients 2019, 11, 2278. [Google Scholar] [CrossRef]
- Barrea, L.; Macchia, P.E.; Tarantino, G.; Di Somma, C.; Pane, E.; Balato, N.; Napolitano, M.; Colao, A.; Savastano, S. Nutrition: A key environmental dietary factor in clinical severity and cardio-metabolic risk in psoriatic male patients evaluated by 7-day food-frequency questionnaire. J. Transl. Med. 2015, 13, 303. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Annunziata, G.; Muscogiuri, G.; Laudisio, D.; Di Somma, C.; Maisto, M.; Tenore, G.C.; Colao, C.; Savastano, S. Trimethylamine N-oxide, Mediterranean diet, and nutrition in healthy, normal-weight adults: Also a matter of sex? Nutrition 2019, 62, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-item Mediterranean diet assessment tool and obesity indexes among high-risk subjects: The PREDIMED trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef] [PubMed]
- Arora, T.; Taheri, S. Associations among late chronotype, body mass index and dietary behaviors in young adolescents. Int. J. Obes. 2015, 39, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Ross, K.M.; Graham Thomas, J.; Wing, R.R. Successful weight loss maintenance associated with morning chronotype and better sleep quality. J. Behav. Med. 2016, 39, 465–471. [Google Scholar] [CrossRef]
- Soreca, I.; Fagiolini, A.; Frank, E.; Goodpaster, B.H.; Kupfer, D.J. Chronotype and Body Composition in Bipolar Disorder. Chronobiol. Int. 2009, 26, 780–788. [Google Scholar] [CrossRef]
- Ruiz-Lozano, T.; Vidal, J.; de Hollanda, A.; Canteras, M.; Garaulet, M.; Izquierdo-Pulido, M. Evening chronotype associates with obesity in severely obese subjects: Interaction with CLOCK 3111T/C. Int. J. Obes. 2016, 40, 1550–1557. [Google Scholar] [CrossRef]
- Lucassen, E.A.; Zhao, X.; Rother, K.I.; Mattingly, M.S.; Courville, A.B.; de Jonge, L.; Csako, G.; Cizza, G. Evening chronotype is associated with changes in eating behavior, more sleep apnea, and increased stress hormones in short sleeping obese individuals. PLoS ONE 2013, 8, e56519. [Google Scholar] [CrossRef]
- De Amicis, R.; Galasso, L.; Leone, A.; Vignati, L.; de Carlo, G.; Foppiani, A.; Montaruli, A.; Roveda, E.; Cè, E.; Esposito, F.; et al. Is Abdominal Fat Distribution Associated with Chronotype in Adults Independently of Lifestyle Factors? Nutrients 2020, 12, 592. [Google Scholar] [CrossRef]
- Godos, J.; Castellano, S.; Ray, S.; Grosso, G.; Galvano, F. Dietary Polyphenol Intake and Depression: Results from the Mediterranean Healthy Eating, Lifestyle and Aging (MEAL) Study. Molecules 2018, 23, 999. [Google Scholar] [CrossRef]
- Chang, S.C.; Cassidy, A.; Willett, W.C.; Rimm, E.B.; O’Reilly, E.J.; Okereke, O.I. Dietary flavonoid intake and risk of incident depression in midlife and older women123. Am. J. Clin. Nutr. 2016, 104, 704–714. [Google Scholar] [CrossRef] [PubMed]
- Potì, F.; Santi, D.; Spaggiari, G.; Zimetti, F.; Zanotti, I. Polyphenol Health Effects on Cardiovascular and Neurodegenerative Disorders: A Review and Meta-Analysis. Int. J. Mol. Sci. 2019, 20, 351. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameters | Study Population n = 172 |
|---|---|
| Age | 51.8 ± 15.7 years |
| Gender | |
| Males | 49, 28.5% |
| Females | 123, 71.5% |
| Lifestyle Habits | |
| Smoking | |
| Yes (n, %) | 146, 84.8% |
| No (n, %) | 26, 15.2% |
| Physical activity | |
| Sedentary (n, %) | 84, 48.8% |
| Moderate (n, %) | 88, 51.2% |
| Anthropometric measurements | |
| Weight (kg) | 84.6 ± 18.9 |
| Height (m) | 1.6 ± 0.09 |
| BMI (kg/m2) | 32.1 ± 6.3 |
| Normal-weight (n, %) | 18, 10.5% |
| Over-weight (n, %) | 47, 27.3% |
| Obesity I (n, %) | 58, 33.7% |
| Obesity II (n, %) | 29, 16.9% |
| Obesity III (n, %) | 20, 11.6% |
| WC (cm) | 103.0 ± 16.0 |
| Adherence to the MD | |
| PREDIMED score | 7.8 ± 2.2 |
| Low adherence to the MD | 21, 12.2% |
| Average adherence to the MD | 110, 64.0% |
| High adherence to the MD | 41, 23.8% |
| Chronotype Score | 58.4 ± 13.1 |
| Morning Chronotype | 100, 58.1% |
| Intermediate Chronotype | 50,29.1% |
| Evening Chronotype | 22,12.8% |
| Parameters | Morning Type n = 100, 58.1% | Neither Type n = 50, 29.1% | Evening Type n = 22, 12.8% | p-Value |
|---|---|---|---|---|
| Gender | ||||
| Males | 34, 34.0 | 13, 26.0 | 2, 9.1 | p = 0.18 |
| Females | 66, 66.0 | 37, 74.0 | 20, 90.9 | |
| Lifestyle Habits | ||||
| Age (years) | 55.5 ± 13.7 | 43.0 ± 17.4 a,b | 55.3 ± 11.9 | <0.001 |
| Smoking | ||||
| Yes (n, %) | 7, 7.0 | 11, 22.0 | 8, 36.4 a,c | p < 0.001 |
| No (n, %) | 93, 93.0 | 39, 78.0 | 14, 63.6 a,c | |
| Physical activity | ||||
| Sedentary (n, %) | 39, 39.0 | 26, 52.0 | 19, 86.4 a,c | p < 0.001 |
| Moderate (n, %) | 61, 61.0 | 24, 48.0 | 3, 13.6 a,c | |
| Anthropometric measurements | ||||
| Weight (kg) | 82.9 ± 19.0 | 88.1 ± 20.6 | 83.7 ± 12.5 | 0.29 |
| Height (m) | 1.6 ± 0.09 | 1.6 ± 0.08 | 1.6 ± 0.08 | 0.57 |
| BMI (kg/m2) | 31.4 ± 5.8 | 33.1 ± 7.3 | 32.6 ± 5.5 | 0.27 |
| Normal-weight (n, %) | 10, 10.0 | 7, 14.0 | 1, 4.5 | p = 0.47 |
| Over-weight (n, %) | 33, 33.0 | 9, 18.0 | 5, 22.7 | p = 0.13 |
| Obesity I (n, %) | 32, 32.0 | 15, 30.0 | 11, 50.0 | p = 0.22 |
| Obesity II (n, %) | 15, 15.0 | 11, 22.0 | 3, 13.6 | p = 0.51 |
| Obesity III (n, %) | 10, 10.0 | 8, 16.0 | 2, 9.1 | p = 0.52 |
| WC (cm) | 102.7 ± 16.4 | 102.9 ± 17.3 | 104.5 ± 11.8 | 0.89 |
| Adherence to the MD | ||||
| PREDIMED score | 8.8 ± 1.9 | 7.0 ± 1.5 a,b | 5.1 ± 1.8 a,c | <0.001 |
| Low adherence to the MD | 3, 3.0 | 6, 12.0 a,b | 12, 54.5 a,c | p < 0.001 |
| Average adherence to the MD | 58, 58.0 | 42, 84.0 a,b | 10, 45.5 a,c | p = 0.001 |
| High adherence to the MD | 39, 39.0 | 2, 4.0 a,b | 0, 0 a,c | p < 0.001 |
| Chronotype Score | ||
|---|---|---|
| Parameters | r | p-Value |
| Age (years) | 0.21 | 0.01 |
| BMI (kg/m2) | −0.18 | 0.02 |
| WC (cm) | −0.07 | 0.35 |
| Questions | OR | R2 | 95% IC | p-Value |
|---|---|---|---|---|
| Use of extra virgin olive oil (EVOO) as main culinary lipid | 1.07 | 0.07 | 1.03–1.12 | 0.001 |
| Extra virgin olive oil >4 tablespoons | 1.03 | 0.04 | 1.00–1.06 | 0.013 |
| Vegetables ≥2 servings/day | 1.05 | 0.07 | 1.02–1.07 | 0.001 |
| Fruits ≥3 servings/day | 1.07 | 0.13 | 1.04–1.10 | <0.001 |
| Red/processed meats <1/day | 1.05 | 0.08 | 1.02–1.08 | <0.001 |
| Butter, cream, margarine <1/day | 1.05 | 0.06 | 1.02–1.08 | 0.001 |
| Soda drinks <1/day | 1.04 | 0.07 | 1.01–1.07 | 0.001 |
| Wine glasses ≥7/week | 1.05 | 0.05 | 1.01–1.09 | 0.004 |
| Legumes ≥3/week | 1.02 | 0.02 | 0.99–1.05 | 0.08 |
| Fish/seafood ≥3/week | 1.03 | 0.03 | 1.00–1.06 | 0.02 |
| Commercial sweets and confectionery ≤2/week | 1.04 | 0.04 | 1.01–1.06 | 0.007 |
| Tree nuts ≥3/week | 1.03 | 0.03 | 1.00–1.06 | 0.014 |
| Poultry more than red meats | 1.05 | 0.08 | 1.03–1.08 | <0.001 |
| Use of sofrito sauce ≥2/week | 1.02 | 0.01 | 0.99–1.04 | 0.22 |
| PREDIMED categories | ||||
| Low adherence to the MD | 0.89 | 0.20 | 0.85–0.93 | <0.001 |
| Average adherence to the MD | 0.99 | 0.01 | 0.96–1.01 | 0.05 |
| High adherence to the MD | 1.15 | 0.25 | 1.09–1.21 | <0.001 |
| Chronotype Categories | OR | R2 | 95% IC | p-Value |
|---|---|---|---|---|
| Morning Type | 2.02 | 0.29 | 1.61–2.54 | <0.001 |
| Neither Type | 0.78 | 0.06 | 0.66–0.91 | 0.002 |
| Evening Type | 0.42 | 0.22 | 0.30–0.59 | <0.001 |
| Parameters | Multiple Regression Analysis | |||
|---|---|---|---|---|
| Model 1: Morning Type | R2 | β | t | p-Value |
| PREDIMED score | 0.18 | 0.43 | 4.69 | <0.001 |
| Model 2: Neither Type | ||||
| Butter, cream, margarine <1/day | 0.09 | −0.30 | −2.17 | 0.04 |
| Model 3: Evening Type | ||||
| PREDIMED score | 0.23 | 0.48 | 2.46 | 0.02 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muscogiuri, G.; Barrea, L.; Aprano, S.; Framondi, L.; Di Matteo, R.; Laudisio, D.; Pugliese, G.; Savastano, S.; Colao, A.; on behalf of the Opera Prevention Project. Chronotype and Adherence to the Mediterranean Diet in Obesity: Results from the Opera Prevention Project. Nutrients 2020, 12, 1354. https://doi.org/10.3390/nu12051354
Muscogiuri G, Barrea L, Aprano S, Framondi L, Di Matteo R, Laudisio D, Pugliese G, Savastano S, Colao A, on behalf of the Opera Prevention Project. Chronotype and Adherence to the Mediterranean Diet in Obesity: Results from the Opera Prevention Project. Nutrients. 2020; 12(5):1354. https://doi.org/10.3390/nu12051354
Chicago/Turabian StyleMuscogiuri, Giovanna, Luigi Barrea, Sara Aprano, Lydia Framondi, Rossana Di Matteo, Daniela Laudisio, Gabriella Pugliese, Silvia Savastano, Annamaria Colao, and on behalf of the Opera Prevention Project. 2020. "Chronotype and Adherence to the Mediterranean Diet in Obesity: Results from the Opera Prevention Project" Nutrients 12, no. 5: 1354. https://doi.org/10.3390/nu12051354
APA StyleMuscogiuri, G., Barrea, L., Aprano, S., Framondi, L., Di Matteo, R., Laudisio, D., Pugliese, G., Savastano, S., Colao, A., & on behalf of the Opera Prevention Project. (2020). Chronotype and Adherence to the Mediterranean Diet in Obesity: Results from the Opera Prevention Project. Nutrients, 12(5), 1354. https://doi.org/10.3390/nu12051354