Snapshots of Urban and Rural Food Environments: EPOCH-Based Mapping in a High-, Middle-, and Low-Income Country from a Non-Communicable Disease Perspective

 , ,
, ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample
2.2.1. Site Selection
2.2.2. Description of Study Sites
2.3. Data Collection and Analysis
2.3.1. Data Collection Tool
2.3.2. Data Collection Process
2.3.3. Data Analysis
2.4. Ethical Considerations
3. Results
3.1. Availability
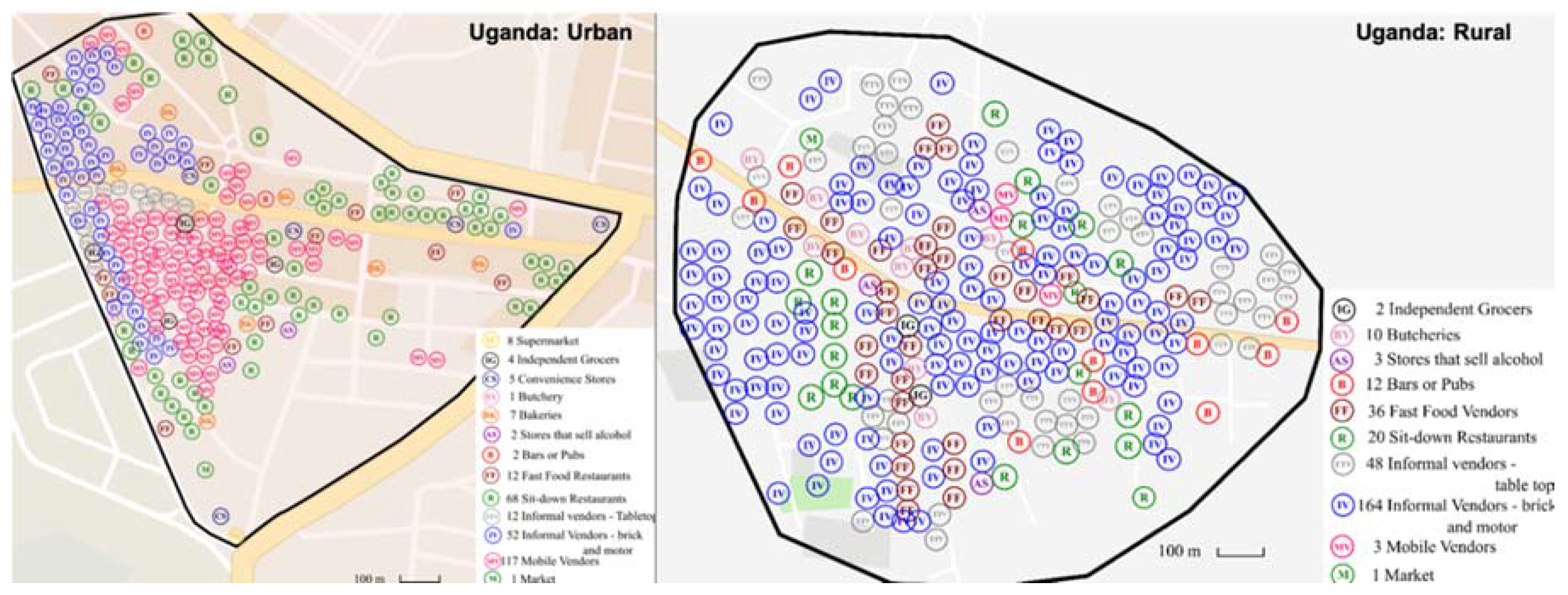
3.1.1. Presence and Distribution of Food Retail Outlets
3.1.2. Presence of Food Items in Food Retail Outlets
3.2. Vendor and Product Properties
3.2.1. Vendor Typology
3.2.2. Product and Food Quality
3.3. Price
3.4. Marketing and Regulation
3.4.1. Advertising and Promotion
3.4.2. Product Labelling
4. Discussion
4.1. Implications for NCD Prevention and Interventions
4.2. Study Strengths and Weaknesses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sweeney, G.; Hand, M.; Kaiser, M.; Clark, J.K.; Rogers, C.; Spees, C. The state of food mapping: Academic literature since 2008 and review of online GIS-based food mapping resources. J. Plan. Lit. 2015, 31, 123–219. [Google Scholar] [CrossRef]
- Beaulac, J.; Kristjansson, E.; Cummins, S. A systematic review of food deserts, 1966–2007. Prev. Chronic Dis. 2009, 6, A105. [Google Scholar]
- Turner, C.; Aggarwal, A.; Walls, H.; Herforth, A.; Drewnowski, A.; Coates, J.; Kalamatianou, S.; Kadiyala, S. Concepts and critical perspectives for food environment research: A global framework with implications for action in low-and middle-income countries. Glob. Food Secur. 2018, 18, 93–101. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC)-Africa Working Group. Trends in obesity and diabetes across Africa from 1980 to 2014: An analysis of pooled population-based studies. Int. J. Epidemiol. 2017, 46, 1421–1432. [Google Scholar] [CrossRef] [PubMed]
- Gouda, H.N.; Charlson, F.; Sorsdahl, K.; Ahmadzada, S.; Ferrari, A.J.; Erskine, H.; Leung, J.; Santamauro, D.; Lund, C.; Aminde, L.N.; et al. Burden of non-communicable diseases in sub-Saharan Africa, 1990–2017: results from the Global Burden of Disease Study 2017. The Lancet Global Health 2019, 7, e1375–e1387. [Google Scholar] [CrossRef]
- Turner, C.; Kalamatianou, S.; Drewnowski, A.; Kulkarni, B.; Kinra, S.; Kadiyala, S. Food environment research in low-and middle-income countries: A systematic scoping review. Adv. Nutr. 2019, 10, 730. [Google Scholar] [CrossRef]
- Battersby, J.; Crush, J. Africa’s urban food deserts. Urban Forum 2014, 25, 143–151. [Google Scholar] [CrossRef]
- Kelly, B.; Flood, V.M.; Yeatman, H. Measuring local food environments: An overview of available methods and measures. Health Place 2011, 17, 1284–1293. [Google Scholar] [CrossRef]
- Pitt, E.; Gallegos, D.; Comans, T.; Cameron, C.; Thornton, L. Exploring the influence of local food environments on food behaviours: A systematic review of qualitative literature. Public Health Nutr. 2017, 20, 2393–2405. [Google Scholar] [CrossRef]
- Giskes, K.; van Lenthe, F.; Avendano-Pabon, M.; Brug, J. A systematic review of environmental factors and obesogenic dietary intakes among adults: Are we getting closer to understanding obesogenic environments? Obes. Rev. 2011, 12, e95–e106. [Google Scholar] [CrossRef]
- Caspi, C.E.; Kawachi, I.; Subramanian, S.V.; Adamkiewicz, G.; Sorensen, G. The relationship between diet and perceived and objective access to supermarkets among low-income housing residents. Soc. Sci. Med. 2012, 75, 1254–1262. [Google Scholar] [CrossRef] [PubMed]
- Caspi, C.E.; Sorensen, G.; Subramanian, S.V.; Kawachi, I. The local food environment and diet: A systematic review. Health Place 2012, 18, 1172–1187. [Google Scholar] [CrossRef] [PubMed]
- Vogel, C.; Abbott, G.; Ntani, G.; Barker, M.; Cooper, C.; Moon, G.; Ball, K.; Baird, J. Examination of how food environment and psychological factors interact in their relationship with dietary behaviours: Test of a cross-sectional model. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 12. [Google Scholar] [CrossRef] [PubMed]
- Bava, C.M.; Jaeger, S.R.; Dawson, J. In-Store influences on consumers’ grocery purchasing decisions: A qualitative investigation. J. Cust. Behav. 2009, 8, 221–236. [Google Scholar] [CrossRef]
- Guwatudde, D.; Absetz, P.; Delobelle, P.; Östenson, C.-G.; Olmen Van, J.; Alvesson, H.M.; Mayega, R.W.; Ekirapa Kiracho, E.; Kiguli, J.; Sundberg, C.J.; et al. Study protocol for the SMART2D adaptive implementation trial: A cluster randomised trial comparing facility-only care with integrated facility and community care to improve type 2 diabetes outcomes in Uganda, South Africa and Sweden. BMJ Open 2018, 8, e019981. [Google Scholar] [CrossRef]
- De Man, J.; Aweko, J.; Daivadanam, M.; Alvesson, H.M.; Delobelle, P.; Mayega, R.W.; Östenson, C.-G.; Kirunda, B.; Kasujja, F.X.; Guwattude, D.; et al. Diabetes self-management in three different income settings: Cross-Learning of barriers and opportunities. PLoS ONE 2019, 14, e0213530. [Google Scholar] [CrossRef]
- van Olmen, J.; Delobelle, P.; Guwatudde, D.; Absetz, P.; Sanders, D.; Mölsted Alvesson, H.; Puoane, T.; Ostenson, C.-G.; Tomson, G.; Mayega, R.W.; et al. Using a cross-contextual reciprocal learning approach in a multisite implementation research project to improve self-management for type 2 diabetes. BMJ Glob. Health 2018, 3, e001068. [Google Scholar] [CrossRef]
- Uganda Bureau of Statistics (UBOS). National Population and Housing Census, Area-Specific Profiles: Mayuge District; Uganda Bureau of Statistics: Kampala, Uganda, 2017. [Google Scholar]
- Uganda Bureau of Statistics (UBOS). National Population and Housing Census 2014, Area-Specific Profiles: Kampala Capital City Authority; Uganda Bureau of Statistics: Kampala, Uganda, 2017. [Google Scholar]
- Chiwanga, F.S.; Njelekela, M.A.; Diamond, M.B.; Bajunirwe, F.; Guwatudde, D.; Nankya-Mutyoba, J.; Kalyesubula, R.; Adebamowo, C.; Ajayi, I.; Reid, T.G.; et al. Urban and rural prevalence of diabetes and pre-diabetes and risk factors associated with diabetes in Tanzania and Uganda. Glob. Health Action 2016, 9, 31440–31448. [Google Scholar] [CrossRef]
- StatsSA. Census. 2011. Available online: http://www.statssa.gov.za/?page_id=3839 (accessed on 15 October 2019).
- International Diabetes Federation (IDF). IDF Diabetes Atlas; International Diabetes Federation: Brussels, Belgium, 2019. [Google Scholar]
- Hall, T.; Vidén, S. The Million Homes Programme: A review of the great Swedish planning project. Plan. Perspect. 2005, 20, 301–328. [Google Scholar] [CrossRef]
- Bradby, H.; Green, G.; Davison, C.; Krause, K. Is superdiversity a useful concept in European medical sociology? Front. Sociol. 2017, 1. [Google Scholar] [CrossRef]
- SCB/SWECO. Statistik Stockholm Områdesfakta. Available online: https://stad.stockholm/utredningar-statistik-och-fakta/statistik/ (accessed on 5 June 2017).
- Region Fakta. Örebro Län. Available online: http://www.regionfakta.com/orebro-lan/geografi/storre-tatorter/ (accessed on 5 July 2017).
- Ekonomifakta. Available online: https://www.ekonomifakta.se/Fakta/Regional-statistik/Din-kommun-i-siffror/Ljusnarsberg?compare=1 (accessed on 6 February 2019).
- Bennet, L.; Groop, L.; Lindblad, U.; Agardh, C.D.; Franks, P.W. Ethnicity is an independent risk indicator when estimating diabetes risk with FINDRISC scores: A cross sectional study comparing immigrants from the Middle East and native Swedes. Prim. Care Diabetes 2014, 8, 231–238. [Google Scholar] [CrossRef]
- Chow, C.K.; Lock, K.; Madhavan, M.; Corsi, D.J.; Gilmore, A.B.; Subramanian, S.V.; Li, W.; Swaminathan, S.; Lopez-Jaramillo, P.; Avezum, A.; et al. Environmental profile of a community’s health (EPOCH): An instrument to measure environmental determinants of cardiovascular health in five countries. PLoS ONE 2010, 5, e14294. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inf. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inf. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- OECD. Exchange Rates. Available online: https://www.oecd-ilibrary.org/finance-and-investment/exchange-rates/indicator/english_037ed317-en (accessed on 1 May 2018).
- The World Bank PPP Conversion Factor, GDP (LCU per International $). Available online: https://data.worldbank.org/indicator/PA.NUS.PPP?locations=UG&name_desc=false (accessed on 1 May 2018).
- Temple, N.J.; Steyn, N.P.; Fourie, J.; De Villiers, A. Price and availability of healthy food: A study in rural South Africa. Nutrition 2011, 27, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Rydén, P.J.; Hagfors, L. Diet cost, diet quality and socio-economic position: How are they related and what contributes to differences in diet costs? Public Health Nutr. 2011, 14, 1680–1692. [Google Scholar] [CrossRef]
- Omiat, G.; Shively, G. Charting the cost of nutritionally-adequate diets in Uganda, 2000–2011. Afr. J. Food Agric. Nutr. Dev. 2017, 17, 11571–11591. [Google Scholar]
- Headey, D.D.; Alderman, H.H. The relative caloric prices of healthy and unhealthy foods differ systematically across income levels and continents. J. Nutr. 2019, 149, 2020–2033. [Google Scholar] [CrossRef]
- Vaughan, C.A.; Cohen, D.A.; Ghosh-Dastidar, M.; Hunter, G.P.; Dubowitz, T. Where do food desert residents buy most of their junk food? Supermarkets. Public Health Nutr. 2016, 20, 2608–2616. [Google Scholar] [CrossRef]
- Juul, F.; Hemmingsson, E. Trends in consumption of ultra-processed foods and obesity in Sweden between 1960 and 2010. Public Health Nutr. 2015, 18, 3096–3107. [Google Scholar] [CrossRef]
- Steyn, N.P.; McHiza, Z.J. Obesity and the nutrition transition in Sub-Saharan Africa. Ann. N. Y. Acad. Sci. 2014, 1311, 88–101. [Google Scholar] [CrossRef]
- Ronquest-Ross, L.-C.; Vink, N.; Sigge, G. Food consumption changes in South Africa since 1994. S. Afr. J. Sci. 2015, 111. [Google Scholar] [CrossRef]
- Peer, N.; Steyn, K.; Lombard, C.; Lambert, E.V.; Vythilingum, B.; Levitt, N.S. Rising diabetes prevalence among urban-dwelling black South Africans. PLoS ONE 2012, 7, e43336. [Google Scholar] [CrossRef] [PubMed]
- Bixby, H.; Bentham, J.; Zhou, B.; Di Cesare, M.; Paciorek, C.J.; Bennett, J.E.; Taddei, C.; Stevens, G.A.; Rodriguez-Martinez, A.; Carrillo-Larco, R.M.; et al. Rising rural body-mass index is the main driver of the global obesity epidemic in adults. Nature 2019, 569, 260–264. [Google Scholar]
- The High Level Panel of Experts on Food Security and Nutrition (HLPE). Nutrition and Food Systems; Food and Agriculture Organization of the United Nations (FAO): Rome, Italy, 2017. [Google Scholar]
- Battersby, J.; Watson, V. Addressing food security in African cities. Nat. Sustain. 2018, 1, 153–155. [Google Scholar] [CrossRef]
- Global Entrepreneurship Monitor (GEM). Global Report; Global Entrepreneurship Monitor: London, UK, 2014. [Google Scholar]
- Carducci, B.; Oh, C.; Keats, E.C.; Gaffey, M.F.; Roth, D.E.; Bhutta, Z.A. PROTOCOL: Impact of the food environment on diet-related health outcomes in school-age children and adolescents in low-and middle-income countries: A systematic review. Campbell Syst. Rev. 2018, 14, 1–55. [Google Scholar] [CrossRef]
- Kiguli, J.; Alvesson, H.M.; Mayega, R.W.; Kasujja, F.X.; Muyingo, A.; Kirunda, B.; Ekirapa Kiracho, E.; Kayemba Nalwadda, C.; Naggayi, G.; Peterson, S.; et al. Dietary patterns and practices in rural eastern Uganda: Implications for prevention and management of type 2 diabetes. Appetite 2019, 143, 104409. [Google Scholar] [CrossRef]
- StockholmStad. Tillstånd, Regler Och Tillsyn. Available online: https://tillstand.stockholm/tillstand-regler-och-tillsyn/ (accessed on 2 June 2019).
- Reardon, T. Surprised by supermarkets: Diffusion of modern food retail in India. J. Agribus. Dev. Emerg. Econ. 2011, 1, 134–161. [Google Scholar] [CrossRef]
- Battersby, J.; Marshak, M.; Mngqibisa, N. Mapping in the Invisible: The Informal Food Economy of Cape Town, South Africa; African Food Security Urban Network (AFSUN): Rondebosch, South Africa, 2017. [Google Scholar]
- Battersby, J.; Peyton, S. The geography of supermarkets in Cape Town: Supermarket expansion and food access. Urban Forum 2014, 25, 153–164. [Google Scholar] [CrossRef]
- Alexander, E.; Yach, D.; Mensah, G.A. Major multinational food and beverage companies and informal sector contributions to global food consumption: Implications for nutrition policy. Glob. Health 2011, 7, 26. [Google Scholar] [CrossRef]
- Patel, K.; Guenther, D.; Wiebe, K.; Seburn, R.-A. Promoting food security and livelihoods for urban poor through the informal sector: A case study of street food vendors in Madurai, Tamil Nadu, India. Food Secur. 2014, 6, 861–878. [Google Scholar] [CrossRef]
- Young, G. De-Democratisation and the rights of street vendors in Kampala, Uganda. Int. J. Hum. Rights 2018, 22, 1007–1029. [Google Scholar] [CrossRef]
- Resnick, D. The politics of crackdowns on Africa’s informal vendors. Comp. Politics 2019, 52, 21–51. [Google Scholar] [CrossRef]
- Temple, N.J.; Fraser, J. Food labels: A critical assessment. Nutrition 2014, 30, 257–260. [Google Scholar] [CrossRef] [PubMed]
- Mayhew, A.J.; Lock, K.; Kelishadi, R.; Swaminathan, S.; Marcilio, C.S.; Iqbal, R.; Dehghan, M.; Yusuf, S.; Chow, C.K. Nutrition labelling, marketing techniques, nutrition claims and health claims on chip and biscuit packages from sixteen countries. Public Health Nutr. 2015, 19, 998–1007. [Google Scholar] [CrossRef] [PubMed]
- Pettigrew, S.; Talati, Z.; Miller, C.; Dixon, H.; Kelly, B.; Ball, K. The types and aspects of front-of-pack food labelling schemes preferred by adults and children. Appetite 2017, 109, 115–123. [Google Scholar] [CrossRef]
- Spagnoli, T.D.; Cesari, L.; Caputo, M.; Magliola, R.; Audenino, M. 65—Front-of-pack logo v. guideline daily amounts: What’s the better tool to promote suitable choices of packaged products in children according to health professionals? Public Health Nutr. 2012, 15, 1583. [Google Scholar]
- Watson, W.L.; Kelly, B.; Hector, D.; Hughes, C.; King, L.; Crawford, J.; Sergeant, J.; Chapman, K. Can front-of-pack labelling schemes guide healthier food choices? Australian shoppers’ responses to seven labelling formats. Appetite 2014, 72, 90–97. [Google Scholar] [CrossRef]
- Julia, C.; Péneau, S.; Buscail, C.; Gonzalez, R.; Touvier, M.; Hercberg, S.; Kesse-Guyot, E. Perception of different formats of front-of-pack nutrition labels according to sociodemographic, lifestyle and dietary factors in a French population: Cross-Sectional study among the NutriNet-Santé cohort participants. BMJ Open 2017, 7, e016108. [Google Scholar] [CrossRef]
- Daivadanam, M.; Ingram, M.; Sidney Annerstedt, K.; Parker, G.; Bobrow, K.; Dolovich, L.; Gould, G.; Riddell, M.; Vedanthan, R.; Webster, J.; et al. The role of context in implementation research for non-communicable diseases: Answering the ‘how-to’ dilemma. PLoS ONE 2019, 14, e0214454. [Google Scholar] [CrossRef]
- Brownson, R.C.; Seiler, R.; Eyler, A.A. Measuring the impact of public health policy. Prev. Chronic Dis. 2010, 7, 1–7. [Google Scholar]
- Mahesh, R.; Vandevijvere, S.; Dominick, C.; Swinburn, B. Relative contributions of recommended food environment policies to improve population nutrition: Results from a Delphi study with international food policy experts. Public Health Nutr. 2018, 21, 2142–2148. [Google Scholar] [CrossRef] [PubMed]
- Bosire, E.N.; Stacey, N.; Mukoma, G.; Tugendhaft, A.; Hofman, K.; Norris, S.A. Attitudes and perceptions among urban South Africans towards sugar-sweetened beverages and taxation. Public Health Nutr. 2019, 23, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Black, A.P.; Brimblecombe, J.; Eyles, H.; Morris, P.; Vally, H.; O’Dea, K. Food subsidy programs and the health and nutritional status of disadvantaged families in high income countries: A systematic review. BMC Public Health 2012, 12, 1099. [Google Scholar] [CrossRef]
- Eyles, H.; Ni Mhurchu, C.; Nghiem, N.; Blakely, T. Food pricing strategies, population diets, and non-communicable disease: A systematic review of simulation studies. PLoS Med. 2012, 9, e1001353. [Google Scholar] [CrossRef]
- Chen, S.E.; Florax, R.J.G.M. Zoning for health: The obesity epidemic and opportunities for local policy intervention. J. Nutr. 2010, 140, 1181S–1184S. [Google Scholar] [CrossRef]
- Young, L.; Swinburn, B. Impact of the Pick the Tick food information programme on the salt content of food in New Zealand. Health Promot. Int. 2002, 17, 13–19. [Google Scholar] [CrossRef]
- Upadhyaya, M.; Sharma, S.; Pompeii, L.A.; Sianez, M.; Morgan, R.O. Obesity prevention worksite wellness interventions for health care workers: A narrative review. Workplace Health Saf. 2019, 68, 32–49. [Google Scholar] [CrossRef]
- Appleby, L.J.; Tadesse, G.; Wuletawu, Y.; Dejene, N.G.; Grimes, J.E.T.; French, M.D.; Teklu, A.; Moreda, B.; Negussu, N.; Kebede, B.; et al. Integrated delivery of school health interventions through the school platform: Investing for the future. PLoS Negl. Trop. Dis. 2019, 13, e0006449. [Google Scholar] [CrossRef]
- Hawkes, C.; Jewell, J.; Allen, K. A food policy package for healthy diets and the prevention of obesity and diet-related non-communicable diseases: The NOURISHING framework. Obes. Rev. 2013, 14 (Suppl. 2), 159–168. [Google Scholar] [CrossRef]
- Cairns, G.; Angus, K.; Hastings, G.; Caraher, M. Systematic reviews of the evidence on the nature, extent and effects of food marketing to children. A retrospective summary. Appetite 2013, 62, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Corvalán, C.; Reyes, M.; Garmendia, M.L.; Uauy, R. Structural responses to the obesity and non-communicable diseases epidemic: The Chilean Law of Food Labeling and Advertising. Obes. Rev. 2013, 14 (Suppl. 2), 79–87. [Google Scholar] [CrossRef]
- Labonté, M.-È.; Poon, T.; Mulligan, C.; Bernstein, J.T.; Franco-Arellano, B.; L’Abbé, M.R. Comparison of global nutrient profiling systems for restricting the commercial marketing of foods and beverages of low nutritional quality to children in Canada. Am. J. Clin. Nutr. 2017, 106, 1471–1481. [Google Scholar] [CrossRef] [PubMed]
- Nestle, M. Food Marketing and Childhood Obesity—A Matter of Policy. N. Engl. J. Med. 2006, 354, 2527–2529. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Uganda | South Africa | Sweden | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Food Retail Outlet Type | Urban n | Rural n | Total n | Urban n | Rural n | Total n | Urban n | Rural n | Total n |
| Formal food retail outlets | |||||||||
| Supermarket | 3 | 0 | 3 | 2 | 11 | 13 | 3 | 2 | 5 |
| Independent grocer | 4 | 2 | 6 | 6 | 36 | 42 | 9 | 2 | 11 |
| Convenience store | 5 | 0 | 5 | 2 | 2 | 4 | 4 | 2 | 6 |
| Total | 12 | 2 | 14 | 10 | 49 | 59 | 16 | 6 | 22 |
| Stores with specialty products | |||||||||
| Butcher/meat store | 1 | 10 | 11 | 6 | 3 | 9 | 0 | 0 | 0 |
| Bakery | 7 | 0 | 7 | 0 | 0 | 0 | 1 | 0 | 1 |
| Deli/specialty food store | 0 | 0 | 0 | 1 | 1 | 2 | 5 | 2 | 7 |
| (Stores that sell alcohol) | 2 | 3 | 5 | 3 | 5 | 8 | 2 | 4 | 6 |
| Total | 10 | 13 | 23 | 10 | 9 | 19 | 8 | 6 | 14 |
| Food service outlets | |||||||||
| Pubs/Bars | 2 | 12 | 14 | 4 | 17 | 21 | 1 | 1 | 2 |
| Fast food vendors | 12 | 36 | 48 | 11 | 18 | 29 | 5 | 1 | 6 |
| Other sit-down restaurants | 68 | 20 | 88 | 3 | 11 | 14 | 6 | 4 | 10 |
| Total | 82 | 68 | 150 | 18 | 46 | 64 | 12 | 6 | 18 |
| Informal food retail outlets | |||||||||
| Informal vendor—table top | 18 | 48 | 66 | 19 | 112 | 131 | 1 | 1 | 2 |
| Informal vendor—brick and mortar | 52 | 164 | 216 | 50 | 33 | 83 | 0 | 0 | 0 |
| Mobile vendor | 117 | 3 | 120 | 5 | 1 | 6 | 0 | 0 | 0 |
| Market | 1 | 1 | 2 | 0 | 0 | 0 | 0 | 0 | 0 |
| Total | 188 | 216 | 404 | 74 | 146 | 220 | 1 | 1 | 2 |
| Overall Total † | 290 | 296 | 586 | 109 | 245 | 354 | 35 | 15 | 50 |
| Food Items | Uganda Urban 11; Rural 7; Total 18 | South Africa Urban 8; Rural 11; Total 19 | Sweden Urban 7; Rural 6; Total 13 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Urban n (%) † | Rural n (%) | Total n (%) | Urban n (%) | Rural n (%) | Total n (%) | Urban n (%) | Rural n (%) | Total n (%) | |
| Fruits | 8 (72.7) | 2 (28.6) | 10 (55.6) | 5 (62.5) | 7 (63.6) | 12 (63.2) | 4 (57.1) | 5 (83.3) | 9 (69.2) |
| Vegetables | 7 (63.6) | 3 (42.9) | 10 (55.6) | 5 (62.5) | 6 (54.5) | 11 (57.9) | 4 (57.1) | 5 (83.3) | 9 (69.2) |
| Mean n and % | 7.5 (68.2) | 2.5 (35.7) | 10 (55.6) | 5 (62.5) | 6.5 (59.1) | 11.5 (60.5) | 4 (57.1) | 5 (83.3) | 9 (69.2) |
| Other groceries: | |||||||||
| Breakfast cereal | 5 (45.5) | 1 (14.3) | 6 (33.3) | 7 (87.5) | 6 (54.5) | 13 (68.4) | 4 (57.1) | 5 (83.3) | 9 (69.2) |
| Bread | 4 (36.4) | 4 (57.1) | 8 (44.4) | 6 (75) | 5 (45.5) | 11 (57.9) | 4 (57.1) | 6 (100) | 10 (76.9) |
| Milk | 5 (45.5) | 2 (28.6) | 7 (38.9) | 7 (87.5) | 6 (54.5) | 13 (68.4) | 4 (57.1) | 4 (66.7) | 8 (61.5) |
| Yoghurt | 5 (45.5) | 2 (28.6) | 7 (38.9) | 7 (87.5) | 3 (27.3) | 10 (52.6) | 3 (42.9) | 6 (100) | 9 (69.2) |
| Mean n and % | 4.8 (43.2) | 2.3 (32.1) | 7 (38.9) | 6.8 (84.4) | 5 (45.5) | 11.8 (61.8) | 3.8 (53.6) | 5.3 (87.5) | 9 (69.2) |
| Confectionaries: | |||||||||
| Biscuits | 6 (54.5) | 3 (42.9) | 9 (50) *.‡ | 7 (87.5) | 7 (63.6) | 14 (73.7) * | 6 (85.7) | 6 (100) | 12 (92.3) * |
| Chips | 5 (45.5) | 0 (0) | 5 (27.8) * | 7 (87.5) | 8 (72.7) | 15 (78.9) * | 6 (85.7) | 6 (100) | 12 (92.3) * |
| Chocolate bar | 5 (45.5) | 1 (14.3) | 6 (33.3) * | 7 (87.5) | 5 (45.5) | 12 (63.2) * | 6 (85.7) | 5 (83.3) | 11 (84.6) * |
| Mean n and % | 5.3 (48.5) | 1.3 (19) | 6.7 (37) | 7 (87.5) | 8 (72.7) | 13.7 (71.9) | 6 (85.7) | 5.7 (94.4) | 11.7 (89.7) |
| Sweetened beverages: | |||||||||
| Non-diet soda | 6 (54.5) | 4 (57.1) | 10 (55.6) | 7 (87.5) | 6 (54.5) | 13 (68.4) | 6 (85.7) | 6 (100) | 12 (92.3) |
| Fruit drink | 7 (63.6) | 3 (42.9) | 10 (55.6) | 7 (87.5) | 6 (54.5) | 13 (68.4) | 6 (85.7) | 6 (100) | 12 (92.3) |
| Energy drink | 6 (54.5) | 4 (57.1) | 10 (55.6) | 7 (87.5) | 6 (54.5) | 13 (68.4) | 6 (85.7) | 6 (100) | 12 (92.3) |
| Mean n and % | 6.3 (57.6) | 3.7 (52.4) | 10 (55.6) | 7 (87.5) | 6 (54.5) | 13 (68.4) | 6 (85.7) | 6 (100) | 12 (92.3) |
| Overall mean n and % | 6.0 (54.4) | 2.4 (34.8) | 8.4 (46.8) | 6.4 (80.5) | 6.4 (58.0) | 12.5 (65.7) | 4.9 (70.5) | 5.5 (91.3) | 10.4 (80.1) |
| Type of Promotion | Uganda | South Africa | Sweden | |||
|---|---|---|---|---|---|---|
| Urban | Rural | Urban | Rural | Urban | Rural | |
| Diet (non-commercial) | 0 | 0 | 0 | 0 | 1 | 0 |
| Diet (commercial) | 0 | 0 | 0 | 1 | 6 | 10 |
| Physical activity (non-commercial) | 0 | 0 | 0 | 0 | 4 | 0 |
| Physical activity (commercial) | 0 | 0 | 0 | 0 | 1 | 1 |
| Signs prohibiting smoking | 0 | 0 | 0 | 0 | 2 | 1 |
| Smoking cessation | 0 | 0 | 0 | 2 | 0 | 0 |
| Alcohol cessation | 0 | 0 | 0 | 0 | 0 | 0 |
| Total | 0 | 0 | 0 | 3 | 14 | 12 |
| Country total | 0 | 3 | 26 | |||
| Type of Advertising | Uganda | South Africa | Sweden | ||||
|---|---|---|---|---|---|---|---|
| Urban | Rural | Urban | Rural | Urban | Rural | Total | |
| ‘Junk food’ | 21 | 2 | 15 | 27 | 36 | 20 | 121 |
| Sweetened beverages | 27 | 170 | 30 | 8 | 10 | 4 | 249 |
| Cigarette or tobacco product | 0 | 0 | 1 | 0 | 1 | 1 | 3 |
| Alcoholic drinks | 6 | 21 | 15 | 15 | 2 | 7 | 66 |
| Total | 54 | 193 | 61 | 50 | 49 | 32 | 439 |
| Country Total | 247 | 111 | 81 | ||||
| Back-of-Pack Label | Front-of-Pack Label | ||||||
|---|---|---|---|---|---|---|---|
| Products with a Package | Nutrition Info in Required Language † | Ingredients List | Nutrition Facts | Consumer Guidance Info | Nutrition Claim | Health Claim | |
| Urban | |||||||
| Uganda | n = 57 | 53 (92.9%) | 44 (77.2%) | 43 (75.4%) | 6 (10.5%) | 9 (15.8%) | 17 (29.8%) |
| South Africa | n = 76 | 69 (90.8%) | 61 (80.3%) | 61 (80.3%) | 18 (23.7%) | 32 (42.1%) | 18 (23.7%) |
| Sweden | n = 55 | 52 (94.5%) | 49 (89.1%) | 51 (92.7%) | 26 (47.2%) | 10 (18.2%) | 5 (9.1%) |
| Rural | |||||||
| Uganda | n = 25 | 25 (100%) | 23 (92.0%) | 17 (68%) | 2 (8%) | 5 (20.0%) | 6 (24.0%) |
| South Africa | n = 63 | 60 (95.2%) | 53 (84.1%) | 55 (87.3%) | 12 (19.0%) | 23 (36.5%) | 13 (20.6%) |
| Sweden | n = 62 | 61 (98.4%) | 56 (90.3%) | 60 (96.7%) | 28 (45.1%) | 9 (14.5%) | 3 (4.8%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spires, M.; Berggreen-Clausen, A.; Kasujja, F.X.; Delobelle, P.; Puoane, T.; Sanders, D.; Daivadanam, M. Snapshots of Urban and Rural Food Environments: EPOCH-Based Mapping in a High-, Middle-, and Low-Income Country from a Non-Communicable Disease Perspective. Nutrients 2020, 12, 484. https://doi.org/10.3390/nu12020484
Spires M, Berggreen-Clausen A, Kasujja FX, Delobelle P, Puoane T, Sanders D, Daivadanam M. Snapshots of Urban and Rural Food Environments: EPOCH-Based Mapping in a High-, Middle-, and Low-Income Country from a Non-Communicable Disease Perspective. Nutrients. 2020; 12(2):484. https://doi.org/10.3390/nu12020484
Chicago/Turabian StyleSpires, Mark, Aravinda Berggreen-Clausen, Francis Xavier Kasujja, Peter Delobelle, Thandi Puoane, David Sanders, and Meena Daivadanam. 2020. "Snapshots of Urban and Rural Food Environments: EPOCH-Based Mapping in a High-, Middle-, and Low-Income Country from a Non-Communicable Disease Perspective" Nutrients 12, no. 2: 484. https://doi.org/10.3390/nu12020484
APA StyleSpires, M., Berggreen-Clausen, A., Kasujja, F. X., Delobelle, P., Puoane, T., Sanders, D., & Daivadanam, M. (2020). Snapshots of Urban and Rural Food Environments: EPOCH-Based Mapping in a High-, Middle-, and Low-Income Country from a Non-Communicable Disease Perspective. Nutrients, 12(2), 484. https://doi.org/10.3390/nu12020484