A Systematic Review of Organic Versus Conventional Food Consumption: Is There a Measurable Benefit on Human Health?


Abstract
1. Introduction
2. Methods
2.1. Literature Search
2.2. Study Eligibility Criteria
2.2.1. Population
2.2.2. Intervention
2.2.3. Outcome
2.2.4. Study Designs
2.2.5. Exclusion Criteria
2.3. Data Extraction
2.4. Assessment of Risk of Bias
3. Results
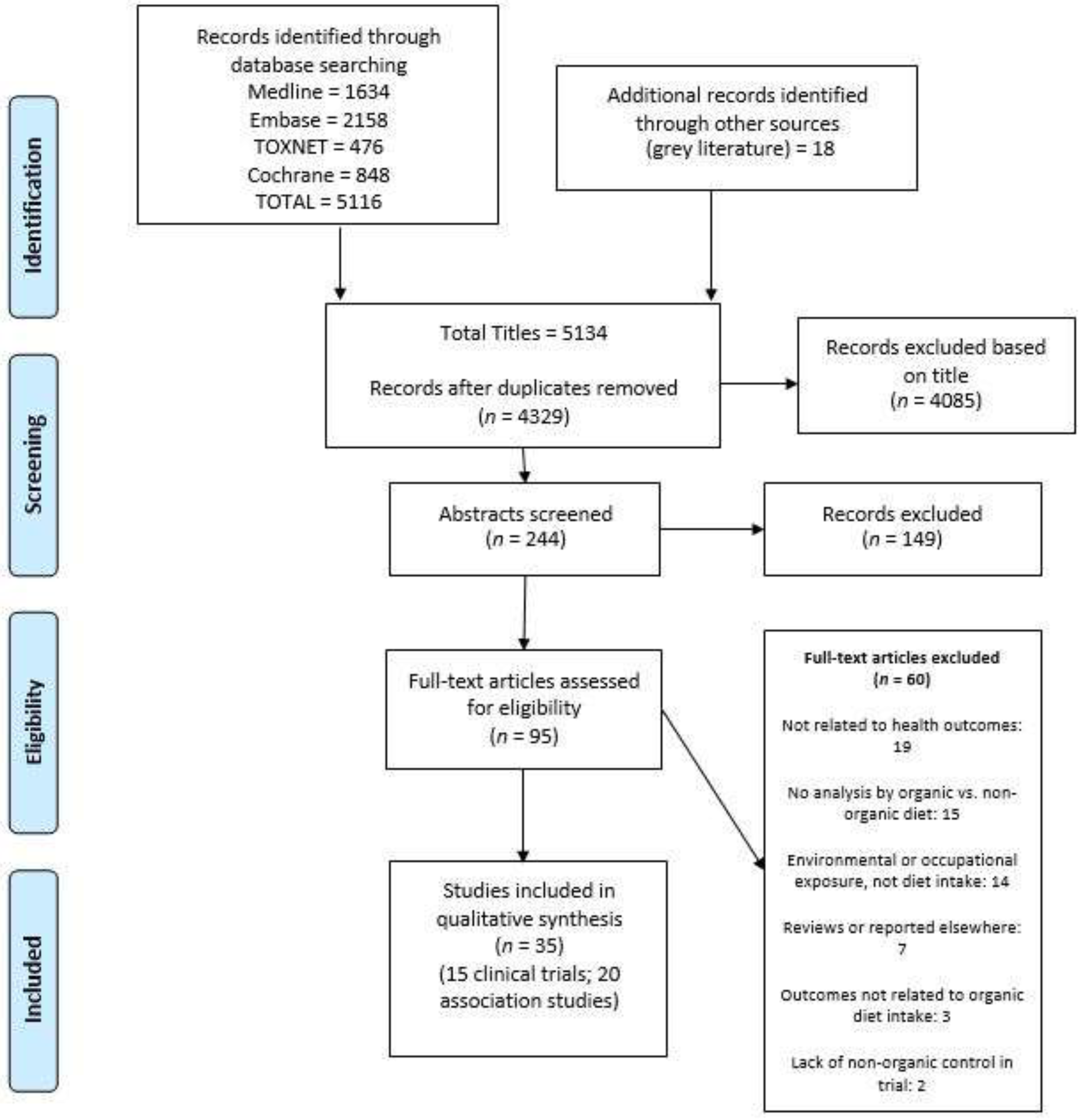
3.1. Study Selection and Characteristics
3.2. Clinical Trials (Single Food/Drink Item Substitution)
3.3. Clinical Trials (Whole Diet Substitution)
3.4. Observational cohort studies
3.4.1. Sperm and Fertility
3.4.2. Mother–Child cohorts
3.4.3. Early Childhood
3.4.4. Adult Research
3.5. Bias Assessments
3.6. Quality of included Reviews
4. Discussion
4.1. Clinical Trials
4.2. Observational Research
4.3. Pesticide Excretion
4.4. Confounders of Results
4.5. Limitations
5. Conclusions
Recommendations for Future Research
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- IFOAM. Consolidated Annual Report of IFOAM-Organics International; IFOAM: Bonn, Germany, 2018. [Google Scholar]
- Willer, H.; Lernoud, J. The World of Organic Agriculture. Statistics and Emerging Trends; Research Institute of Organic Agriculture (FiBL) & IFOAM-Organics International: Frick, Switzerland, 2017. [Google Scholar]
- USDA. U.S. Organic Food Sales by Category: 2005-14E. Available online: https://www.ers.usda.gov/topics/natural-resources-environment/organic-agriculture/organic-market-overview/ (accessed on 31 July 2018).
- Apaolaza, V.; Hartmann, P.; D’Souza, C.; López, C.M. Eat organic–Feel good? The relationship between organic food consumption, health concern and subjective wellbeing. Food Qual. Prefer. 2018, 63, 51–62. [Google Scholar] [CrossRef]
- Hoefkens, C.; Verbeke, W.; Aertsens, J.; Mondelaers, K.; Van Camp, J. The nutritional and toxicological value of organic vegetables. Br. Food. J. 2009, 111, 1062–1077. [Google Scholar] [CrossRef]
- van de Vijver, L.P.L.; van Vliet, M.E.T. Health effects of an organic diet-Consumer experiences in the Netherlands. J. Sci. Food Agric. 2012, 92, 2923–2927. [Google Scholar] [CrossRef] [PubMed]
- Baudry, J.; Méjean, C.; Péneau, S.; Galan, P.; Hercberg, S.; Lairon, D.; Kesse-Guyot, E. Health and dietary traits of organic food consumers: Results from the NutriNet-Santé study. Br. J. Nutr. 2015, 114, 2064–2073. [Google Scholar] [CrossRef]
- Eisinger-Watzl, M.; Wittig, F.; Heuer, T.; Hoffmann, I. Customers purchasing organic food-Do they live healthier? Results of the German National Nutrition Survey II. Eur. J. Nutr. Food Saf. 2015, 5, 59–71. [Google Scholar] [CrossRef]
- Simões-Wüst, A.P.; Moltó-Puigmartí, C.; van Dongen, M.C.; Dagnelie, P.C.; Thijs, C. Organic food consumption during pregnancy is associated with different consumer profiles, food patterns and intake: The KOALA Birth Cohort Study. Public Health Nutr. 2017, 20, 2134–2144. [Google Scholar] [CrossRef]
- Barański, M.; Średnicka-Tober, D.; Volakakis, N.; Seal, C.; Sanderson, R.; Stewart, G.B.; Benbrook, C.; Biavati, B.; Markellou, E.; Giotis, C.; et al. Higher antioxidant and lower cadmium concentrations and lower incidence of pesticide residues in organically grown crops: A systematic literature review and meta-analyses. Br. J. Nutr. 2014, 112, 794–811. [Google Scholar] [CrossRef]
- Benbrook, C.M.; Butler, G.; Latif, M.A.; Leifert, C.; Davis, D.R. Organic Production Enhances Milk Nutritional Quality by Shifting Fatty Acid Composition: A United States–Wide, 18-Month Study. PLoS ONE 2013, 8, e82429. [Google Scholar] [CrossRef]
- Palupi, E.; Jayanegara, A.; Ploeger, A.; Kahl, J. Comparison of nutritional quality between conventional and organic dairy products: A meta-analysis. J. Sci. Food Agric. 2012, 92, 2774–2781. [Google Scholar] [CrossRef]
- Srednicka-Tober, D.; Baranski, M.; Seal, C.; Sanderson, R.; Benbrook, C.; Steinshamn, H.; Gromadzka-Ostrowska, J.; Rembialkowska, E.; Skwarlo-Sonìta, K.; Eyre, M.; et al. Higher PUFA and n-3 PUFA, conjugated linoleic acid, [...]-tocopherol and iron, but lower iodine and selenium concentrations in organic milk: A systematic literature review and meta- and redundancy analyses. Br. J. Nutr. 2016, 115, 1043–1060. [Google Scholar] [CrossRef]
- Ribas-Agusti, A.; Diaz, I.; Sarraga, C.; Garcia-Regueiro, J.A.; Castellari, M. Nutritional properties of organic and conventional beef meat at retail. J. Sci. Food Agric. 2019, 99, 4218–4225. [Google Scholar] [CrossRef] [PubMed]
- Srednicka-Tober, D.; Baranski, M.; Seal, C.; Sanderson, R.; Benbrook, C.; Steinshamn, H.; Gromadzka-Ostrowska, J.; Rembialkowska, E.; Skwarlo-Sonìta, K.; Eyre, M.; et al. Composition differences between organic and conventional meat: A systematic literature review and meta-analysis. Br. J. Nutr. 2016, 115, 994–1011. [Google Scholar] [CrossRef] [PubMed]
- Barański, M.; Rempelos, L.; Iversen, P.O.; Leifert, C. Effects of organic food consumption on human health; the jury is still out! Food Nutr. Res. 2017, 61, 1287333. [Google Scholar] [CrossRef]
- Brantsæter, A.L.; Ydersbond, T.A.; Hoppin, J.A.; Haugen, M.; Meltzer, H.M. Organic food in the diet: Exposure and health implications. Annu. Rev. Public Health 2017, 38, 295–313. [Google Scholar] [CrossRef] [PubMed]
- Hurtado-Barroso, S.; Tresserra-Rimbau, A.; Vallverdu-Queralt, A.; Lamuela-Raventos, R.M. Organic food and the impact on human health. Crit. Rev. Food Sci. Nutr. 2017, 59, 704–714. [Google Scholar] [CrossRef] [PubMed]
- Smith-Spangler, C.; Brandeau, M.L.; Hunter, G.E.; Clay Bavinger, J.; Pearson, M.; Eschbach, P.J.; Sundaram, V.; Liu, H.; Schirmer, P.; Stave, C.; et al. Are organic foods safer or healthier than conventional alternatives?: A systematic review. Ann. Intern. Med. 2012, 157, 348–366. [Google Scholar] [CrossRef]
- Baudry, J.; Ducros, V.; Druesne-Pecollo, N.; Galan, P.; Hercberg, S.; Debrauwer, L.; Amiot, M.J.; Lairon, D.; Kesse-Guyot, E. Some Differences in Nutritional Biomarkers are Detected Between Consumers and Nonconsumers of Organic Foods: Findings from the BioNutriNet Project. Curr. Dev. Nutr. 2018, 3, nzy090. [Google Scholar] [CrossRef]
- Mie, A.; Andersen, H.R.; Gunnarsson, S.; Kahl, J.; Kesse-Guyot, E.; Rembiałkowska, E.; Quaglio, G.; Grandjean, P. Human health implications of organic food and organic agriculture: A comprehensive review. Environ. Health 2017, 16, 111. [Google Scholar] [CrossRef]
- European Environment Agency. Late Lessons from Early Warnings: Science, Precaution, Innovation; European Environment Agency: Copenhagen, Danmark, 2013. [Google Scholar]
- Mesnage, R.; Antoniou, M.N. Ignoring adjuvant toxicity falsifies the safety profile of commercial pesticides. Front. Public Health 2018, 5, 361. [Google Scholar] [CrossRef]
- EFSA. The 2016 European Union report on pesticide residues in food. EFSA J. 2018, 16, 5348. [Google Scholar]
- United States Department of Agriculture. Pesticide Data Program: Annual Summary; United States Department of Agriculture: Washington, DC, USA, 2017; pp. 1–203.
- Lydy, M.; Belden, J.; Wheelock, C.; Hammock, B.; Denton, D. Challenges in regulating pesticide mixtures. Ecol. Soc. 2004, 9, 1. [Google Scholar] [CrossRef]
- Rizzati, V.; Briand, O.; Guillou, H.; Gamet-Payrastre, L. Effects of pesticide mixtures in human and animal models: An update of the recent literature. Chem. Biol. Interact. 2016, 254, 231–246. [Google Scholar] [CrossRef]
- Mostafalou, S.; Abdollahi, M. Pesticides: An update of human exposure and toxicity. Arch. Toxicol. 2017, 91, 549–599. [Google Scholar] [CrossRef] [PubMed]
- Tago, D.; Andersson, H.; Treich, N. Pesticides and health: A review of evidence on health effects, valuation of risks, and benefit-cost analysis. Adv. Health Econ. Health Serv. Res. 2014, 24, 203–295. [Google Scholar] [PubMed]
- WHO. Pesticide Residues in Food–2016: Toxicological Evaluations. In Proceedings of the Joint Meeting of the FAO Panel of Experts on Pesticide Residues in Food and the Environment and the WHO Core Assessment Group on Pesticide Residues, Geneva, Switzerland, 9–13 May 2016. [Google Scholar]
- Bradman, A.; Quirós-Alcalá, L.; Castorina, R.; Schall, R.A.; Camacho, J.; Holland, N.T.; Barr, D.B.; Eskenazi, B. Effect of organic diet intervention on pesticide exposures in young children living in low-income urban and agricultural communities. Environ. Health Perspect. 2015, 123, 1086–1093. [Google Scholar] [CrossRef] [PubMed]
- Curl, C.L.; Beresford, S.A.A.; Fenske, R.A.; Fitzpatrick, A.L.; Lu, C.; Nettleton, J.A.; Kaufman, J.D. Estimating pesticide exposure from dietary intake and organic food choices: The Multi-Ethnic Study of Atherosclerosis (MESA). Environ. Health Perspect. 2015, 123, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Curl, C.L.; Fenske, R.A.; Elgethum, K. Organophosphorus pesticide exposure of urban and suburban preschool children with organic and conventional diets. Environ. Health Perspect. 2003, 111, 377–382. [Google Scholar] [CrossRef]
- Oates, L.; Cohen, M.; Braun, L.; Schembri, A.; Taskova, R. Reduction in urinary organophosphate pesticide metabolites in adults after a week-long organic diet. Environ. Res. 2014, 132, 105–111. [Google Scholar] [CrossRef]
- Dangour, A.D.; Lock, K.; Hayter, A.; Aikenhead, A.; Allen, E.; Uauy, R. Nutrition-related health effects of organic foods: A systematic review. Am. J. Clin. Nutr. 2010, 92, 203–210. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Caris-Veyrat, C.; Amiot, M.J.; Tyssandier, V.; Grasselly, D.; Buret, M.; Mikolajczak, M.; Guilland, J.C.; Bouteloup-Demange, C.; Borel, P. Influence of organic versus conventional agricultural practice on the antioxidant microconstituent content of tomatoes and derived purees; consequences on antioxidant plasma status in humans. J. Agric. Food Chem. 2004, 52, 6503–6509. [Google Scholar] [CrossRef] [PubMed]
- Stracke, B.A.; Rufer, C.E.; Bub, A.; Briviba, K.; Seifert, S.; Kunz, C.; Watzl, B. Bioavailability and nutritional effects of carotenoids from organically and conventionally produced carrots in healthy men. Br. J. Nutr. 2009, 101, 1664–1672. [Google Scholar] [CrossRef] [PubMed]
- Stracke, B.A.; Rufer, C.E.; Bub, A.; Seifert, S.; Weibel, F.P.; Kunz, C.; Watzl, B. No effect of the farming system (organic/conventional) on the bioavailability of apple (Malus domestica Bork, cultivar Golden Delicious) polyphenols in healthy men: A comparative study. Eur. J. Nutr. 2010, 49, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Briviba, K.; Stracke, B.A.; Rufer, C.E.; Watzl, B.; Weibel, F.P.; Bub, A. Effect of consumption of organically and conventionally produced apples on antioxidant activity and DNA damage in humans. J. Agric. Food Chem. 2007, 55, 7716–7721. [Google Scholar] [CrossRef] [PubMed]
- Grinder-Pedersen, L.; Rasmussen, S.E.; Bugel, S.; Jorgensen, L.V.; Dragsted, L.O.; Gundersen, V.; Sandstrom, B. Effect of diets based on foods from conventional versus organic production on intake and excretion of flavonoids and markers of antioxidative defense in humans. J. Agric. Food Chem. 2003, 51, 5671–5676. [Google Scholar] [CrossRef] [PubMed]
- Akçay, Y.D.; Yıldırım, H.K.; Güvenç, U.; Sözmen, E.Y. The effects of consumption of organic and nonorganic red wine on low-density lipoprotein oxidation and antioxidant capacity in humans. Nutr. Res. 2004, 24, 541–554. [Google Scholar] [CrossRef]
- Lu, C.; Toepel, K.; Irish, R.; Fenske, R.A.; Barr, D.B.; Bravo, R. Organic diets significantly lower children’s dietary exposure to organophosphorus pesticides. Environ. Health Perspect. 2006, 114, 260–263. [Google Scholar] [CrossRef]
- Lu, C.; Barr, D.B.; Pearson, M.A.; Waller, L.A. Dietary intake and its contribution to longitudinal organophosphorus pesticide exposure in urban/suburban children. Environ. Health Perspect. 2008, 116, 537–542. [Google Scholar] [CrossRef]
- Di Renzo, L.; Di Pierro, D.; Bigioni, M.; Sodi, V.; Galvano, F.; Cianci, R.; La Fauci, L.; De Lorenzo, A. Is antioxidant plasma status in humans a consequence of the antioxidant food content influence? Eur. Rev. Med. Pharmacol. Sci. 2007, 11, 185–192. [Google Scholar]
- De Lorenzo, A.; Noce, A.; Bigioni, M.; Calabrese, V.; Della Rocca, D.G.; Di Daniele, N.; Tozzo, C.; Di Renzo, L. The effects of Italian Mediterranean organic diet (IMOD) on health status. Curr. Pharm. Des. 2010, 16, 814–824. [Google Scholar] [CrossRef]
- Søltoft, M.; Bysted, A.; Madsen, K.H.; Mark, A.B.; Bügel, S.G.; Nielsen, J.; Knuthsen, P. Effects of organic and conventional growth systems on the content of carotenoids in carrot roots, and on intake and plasma status of carotenoids in humans. J. Sci. Food Agric. 2011, 91, 767–775. [Google Scholar] [CrossRef] [PubMed]
- Toaldo, I.M.; Cruz, F.A.; da Silva, E.L.; Bordignon-Luiz, M.T. Acute consumption of organic and conventional tropical grape juices (Vitis labrusca L.) increases antioxidants in plasma and erythrocytes, but not glucose and uric acid levels, in healthy individuals. Nutr. Res. 2016, 36, 808–817. [Google Scholar] [CrossRef] [PubMed]
- Goen, T.; Schmidt, L.; Lichtensteiger, W.; Schlumpf, M. Efficiency control of dietary pesticide intake reduction by human biomonitoring. Int. J. Hyg. Environ. Health 2017, 220, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Jensen, T.K.; Giwercman, A.; Carlsen, E.; Scheike, T.; Skakkebaek, N.E. Semen quality among members of organic food associations in Zealand, Denmark. Lancet 1996, 347, 1844. [Google Scholar] [CrossRef]
- Juhler, R.K.; Larsen, S.B.; Meyer, O.; Jensen, N.D.; Spano, M.; Giwercman, A.; Bonde, J.P. Human semen quality in relation to dietary pesticide exposure and organic diet. Arch. Environ. Contam. Toxicol. 1999, 37, 415–423. [Google Scholar] [CrossRef]
- Chiu, Y.H.; Williams, P.L.; Gillman, M.W.; Gaskins, A.J.; Minguez-Alarcon, L.; Souter, I.; Toth, T.L.; Ford, J.B.; Hauser, R.; Chavarro, J.E.; et al. Association between pesticide residue intake from consumption of fruits and vegetables and pregnancy outcomes among women undergoing infertility treatment with assisted reproductive technology. JAMA Intern. Med. 2018, 178, 17–26. [Google Scholar] [CrossRef]
- Baudry, J.; Assmann, K.E.; Touvier, M.; Allès, B.; Seconda, L.; Latino-Martel, P.; Ezzedine, K.; Galan, P.; Hercberg, S.; Lairon, D.; et al. Association of frequency of organic food consumption with cancer risk: Findings from the nutrinet-santé prospective cohort study. JAMA Intern. Med. 2018, 178, 1597–1606. [Google Scholar] [CrossRef]
- Baudry, J.; Debrauwer, L.; Durand, G.; Limon, G.; Delcambre, A.; Vidal, R.; Taupier-Letage, B.; Druesne-Pecollo, N.; Galan, P.; Hercberg, S.; et al. Urinary pesticide concentrations in French adults with low and high organic food consumption: Results from the general population-based NutriNet-Santé. J. Expo. Sci. Environ. Epidemiol. 2019, 29, 366–378. [Google Scholar] [CrossRef]
- Brantsæter, A.L.; Torjusen, H.; Meltzer, H.M.; Papadopoulou, E.; Hoppin, J.A.; Alexander, J.; Lieblein, G.; Roos, G.; Holten, J.M.; Swartz, J.; et al. Organic food consumption during pregnancy and hypospadias and cryptorchidism at birth: The Norwegian Mother and Child Cohort Study (MoBa). Environ. Health Perspect. 2016, 124, 357–364. [Google Scholar] [CrossRef]
- Torjusen, H.; Brantsæter, A.L.; Haugen, M.; Alexander, J.; Bakketeig, L.S.; Lieblein, G.; Stigum, H.; Næs, T.; Swartz, J.; Holmboe-Ottesen, G.; et al. Reduced risk of pre-eclampsia with organic vegetable consumption: Results from the prospective Norwegian Mother and Child Cohort Study. BMJ Open 2014, 4, 6143. [Google Scholar] [CrossRef]
- Christensen, J.S.; Asklund, C.; Skakkebaek, N.E.; Jorgensen, N.; Andersen, H.R.; Jorgensen, T.M.; Olsen, L.H.; Hoyer, A.P.; Moesgaard, J.; Thorup, J.; et al. Association between organic dietary choice during pregnancy and hypospadias in offspring: A study of mothers of 306 boys operated on for hypospadias. J. Urol. 2013, 189, 1077–1082. [Google Scholar] [CrossRef] [PubMed]
- Rist, L.; Mueller, A.; Barthel, C.; Snijders, B.; Jansen, M.; Simões-Wüst, A.P.; Huber, M.; Kummeling, I.; von Mandach, U.; Steinhart, H.; et al. Influence of organic diet on the amount of conjugated linoleic acids in breast milk of lactating women in the Netherlands. Br. J. Nutr. 2007, 97, 735–743. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Mueller, A.; Steinhart, H.; Thijs, C.; Rist, L.; Simoes-Wust, A.P.; Huber, M. Trans fatty acids in human milk are an indicator of different maternal dietary sources containing trans fatty acids. Lipids 2010, 45, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Kummeling, I.; Thijs, C.; Huber, M.; van de Vijver, L.P.L.; Snijders, B.E.P.; Penders, J.; Stelma, F.; van Ree, R.; van den Brandt, P.A.; Dagnelie, P.C. Consumption of organic foods and risk of atopic disease during the first 2 years of life in the Netherlands. Br. J. Nutr. 2008, 99, 598–605. [Google Scholar] [CrossRef] [PubMed]
- Stenius, F.; Swartz, J.; Lilja, G.; Borres, M.; Bottai, M.; Pershagen, G.; Scheynius, A.; Alm, J. Lifestyle factors and sensitization in children-the ALADDIN birth cohort. Allergy 2011, 66, 1330–1338. [Google Scholar] [CrossRef]
- Buscail, C.; Chevrier, C.; Serrano, T.; Pele, F.; Monfort, C.; Cordier, S.; Viel, J.F. Prenatal pesticide exposure and otitis media during early childhood in the PELAGIE mother-child cohort. Occup. Environ. Med. 2015, 72, 837–844. [Google Scholar] [CrossRef]
- Kesse-Guyot, E.; Baudry, J.; Assmann, K.E.; Galan, P.; Hercberg, S.; Lairon, D. Prospective association between consumption frequency of organic food and body weight change, risk of overweight or obesity: Results from the NutriNet-Santé Study. Br. J. Nutr. 2017, 117, 325–334. [Google Scholar] [CrossRef]
- Baudry, J.; Lelong, H.; Adriouch, S.; Julia, C.; Allès, B.; Hercberg, S.; Touvier, M.; Lairon, D.; Galan, P.; Kesse-Guyot, E. Association between organic food consumption and metabolic syndrome: Cross-sectional results from the NutriNet-Santé study. Eur. J. Nutr. 2017, 57, 2477–2488. [Google Scholar] [CrossRef]
- Bradbury, K.E.; Balkwill, A.; Spencer, E.A.; Roddam, A.W.; Reeves, G.K.; Green, J.; Key, T.J.; Beral, V.; Pirie, K. Organic food consumption and the incidence of cancer in a large prospective study of women in the United Kingdom. Br. J. Cancer 2014, 110, 2321–2326. [Google Scholar] [CrossRef]
- McGuire, M.K.; McGuire, M.A.; Price, W.J.; Shafii, B.; Carrothers, J.M.; Lackey, K.A.; Goldstein, D.A.; Jensen, P.K.; Vicini, J.L. Glyphosate and aminomethylphosphonic acid are not detectable in human milk. Am. J. Clin. Nutr. 2016, 103, 1285–1290. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Specialist Unit for Review Evidence (SURE). Questions to Assist with the Critical Appraisal of Cross-Sectional Studies. Available online: https://www.cardiff.ac.uk/specialist-unit-for-review-evidence/resources/critical-appraisal-checklists (accessed on 23 January 2019).
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 22 March 2019).
- Scheepers, L.E.J.M.; Penders, J.; Mbakwa, C.A.; Thijs, C.; Mommers, M.; Arts, I.C.W. The intestinal microbiota composition and weight development in children: The KOALA Birth Cohort Study. Int. J. Obes. 2015, 39, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Simoes-Wust, A.P.; Ischa, K.; Monique, M.; Machteld, H.; Lukas, R.; Van De Vijver, L.; Dagnelie, P.C.; Carel, T. Influence of alternative lifestyles on health status and health risk factors in pregnancy and maternity. Eur. J. Integr. Med. 2012, 4, 182–183. [Google Scholar]
- Lu, C.; Barr, D.B.; Pearson, M.; Bartell, S.; Bravo, R. A longitudinal approach to assessing urban and suburban children’s exposure to pyrethroid pesticides. Environ. Health Perspect. 2006, 114, 1419–1423. [Google Scholar] [CrossRef] [PubMed]
- Larsen, S.B.; Spano, M.; Giwercman, A.; Bonde, J.P. Semen quality and sex hormones among organic and traditional Danish farmers. ASCLEPIOS Study Group. Occup. Environ. Med. 1999, 56, 139–144. [Google Scholar] [CrossRef]
- Skakkebaek, N.E.; Jørgensen, N.; Andersson, A.-M.; Juul, A.; Main, K.M.; Jensen, T.K.; Toppari, J. Populations, decreasing fertility, and reproductive health. Lancet 2019, 393, 1500–1501. [Google Scholar] [CrossRef]
- Alfven, T.; Braun-Fahrlander, C.; Brunekreef, B.; von Mutius, E.; Riedler, J.; Scheynius, A.; van Hage, M.; Wickman, M.; Benz, M.R.; Budde, J.; et al. Allergic diseases and atopic sensitization in children related to farming and anthroposophic lifestyle: The PARSIFAL study. Allergy 2006, 61, 414–421. [Google Scholar] [CrossRef]
- Alm, J.; Swartz, J.; Lilja, G.; Scheynius, A.; Pershagen, G. Atopy in children of families with an anthroposophic lifestyle. Lancet 1999, 353, 1485. [Google Scholar] [CrossRef]
- Flöistrup, H.; Swartz, J.; Bergström, A.; Alm, J.S.; Scheynius, A.; van Hage, M.; Waser, M.; Braun-Fahrländer, C.; Schram-Bijkerk, D.; Huber, M.; et al. Allergic disease and sensitization in Steiner school children. J. Allergy Clin. Immunol. 2006, 117, 59–66. [Google Scholar] [CrossRef]
- Lee, D.H.; Lee, I.K.; Porta, M.; Steffes, M.; Jacobs, D.R. Relationship between serum concentrations of persistent organic pollutants and the prevalence of metabolic syndrome among non-diabetic adults: Results from the National Health and Nutrition Examination Survey 1999–2002. Diabetologia 2007, 50, 1841–1851. [Google Scholar] [CrossRef]
- Lee, D.-H.; Steffes, M.W.; Sjödin, A.; Jones, R.S.; Needham, L.L.; Jacobs, D.R., Jr. Low dose organochlorine pesticides and polychlorinated biphenyls predict obesity, dyslipidemia, and insulin resistance among people free of diabetes. PLoS ONE 2011, 6, e15977. [Google Scholar] [CrossRef] [PubMed]
- Guyton, K.Z.; Loomis, D.; Grosse, Y.; El Ghissassi, F.; Benbrahim-Tallaa, L.; Guha, N.; Scoccianti, C.; Mattock, H.; Straif, K. Carcinogenicity of tetrachlorvinphos, parathion, malathion, diazinon, and glyphosate. Lancet Oncol. 2015, 16, 490–491. [Google Scholar] [CrossRef]
- Kaushik, G.; Satya, S.; Naik, S.N. Food processing a tool to pesticide residue dissipation–A review. Food Res. Int. 2009, 42, 26–40. [Google Scholar] [CrossRef]
- Conlon, M.A.; Bird, A.R. The impact of diet and lifestyle on gut microbiota and human health. Nutrients 2014, 7, 17–44. [Google Scholar] [CrossRef] [PubMed]
- De Filippo, C.; Cavalieri, D.; Di Paola, M.; Ramazzotti, M.; Poullet, J.B.; Massart, S.; Collini, S.; Pieraccini, G.; Lionetti, P. Impact of diet in shaping gut microbiota revealed by a comparative study in children from Europe and rural Africa. Proc. Natl. Acad. Sci. USA 2010, 107, 14691–14696. [Google Scholar] [CrossRef]
- Hercberg, S.; Castetbon, K.; Czernichow, S.; Malon, A.; Mejean, C.; Kesse, E.; Touvier, M.; Galan, P. The Nutrinet-Santé Study: A web-based prospective study on the relationship between nutrition and health and determinants of dietary patterns and nutritional status. BMC Public Health 2010, 10, 242. [Google Scholar] [CrossRef]
- Ronningen, K.S.; Paltiel, L.; Meltzer, H.M.; Nordhagen, R.; Lie, K.K.; Hovengen, R.; Haugen, M.; Nystad, W.; Magnus, P.; Hoppin, J.A. The biobank of the Norwegian Mother and Child Cohort Study: A resource for the next 100 years. Eur. J. Epidemiol. 2006, 21, 619–625. [Google Scholar] [CrossRef]


{kind=link}
| Ref. | Study population | n | Design and Duration | Exposure/treatment | Outcome measures | Results | Definition of organic |
|---|---|---|---|---|---|---|---|
| Caris-Veyrant (2004) [37] | France Age: 21–39 years 100% female Healthy | 24 | Parallel RCT. Single-blind. 2-arm, 3 week dietary intervention. | 100 g of conventional tomato puree (NO), or organic tomato puree (O) added to lunch or dinner once daily. | Plasma Vit C, β-carotene and lycopene. | Tomato puree increased plasma β-carotene and lycopene in both groups. There were no significant between-group differences in any outcome. The two purees had similar lycopene and beta-carotene contents. | Describes growing conditions of both crops. They were both experimental crops for the study. |
| Stracke (2009) [38] | Germany Age: 19–54 years 100% male Healthy | 36 | Parallel RCT. Double-blind. 3-arm, 14 day intervention, with 4-week low carotenoid diet prior to baseline. | 200 g of conventional blanched carrots (NO) or organic blanched carrots (O) consumed with main meal and minimum 10 g fat. Control (C) followed carotenoid restricted diet. | Plasma carotenoid concentration (α- and β-carotene, lycopene, lutein, zeaxanthin and b-cryptoxanthin), Vit E, Vit C, antioxidant activity (FRAP, ORAC, TEAC), and LDL oxidation; cytokine quantity, NK cell quantity and activity, DNA damage, plasma glucose, uric acid, TAG, cholesterol. | No significant difference in any outcome measure. There was no significant difference in carotenoid concentration of O and NO carrots. | The fertilisation, harvest and distribution of the carrots were monitored by the Institute of Organic Farming of the Johann Heinrich von Thünen Institute, Federal Research Institute for Rural Areas, Forestry and Fisheries at Westerau. |
| Stracke (2010) a) [39] | Germany Study 1: Age: 23–32 years 100% male Healthy | 6 | Crossover. Double-blind RCT. 2 phases, single consumption after overnight fast. | 1000 g of conventional apples (NO) or organic apples (O) | Apple polyphenols and their metabolites, total antioxidant status (FRAP, TEAC, and ORAC). | There were no significant differences between the O and NO intake in any of the analysed polyphenols. Apple consumption had no effect on TEAC, ORAC or FRAP. | Cultivated according to the requirements of “Bio Suisse” (predominant label organisation for certified organic production in Switzerland). |
| Stracke (2010) b) [39] | Germany Study 2: Age: (22–40yrs) 100% male Healthy | 43 | Parallel RCT Double-blind. 3-arm, 5-week study (1-week depletion period /4-week intervention). | 500 g of conventional apples (NO) or organic apples (O). The third group served as control group (C), and maintained an apple- and polyphenol restricted diet. | Apple polyphenols and their metabolites, glucose, TAG, cholesterol, WBC, and uric acid; total antioxidant status (FRAP, TEAC, and ORAC); Vit C, Vit E, carotenoids. | No between group differences between O and NO groups in plasma glucose, uric acid, TAG, cholesterol, Vit C, Vit E, carotenoids, WBC, polyphenol concentrations, or antioxidant markers. | Cultivated according to the requirements of “Bio Suisse” (predominant label organisation for certified organic production in Switzerland). |
| Briviba (2007) [40] | Germany Age: 23–32 years 100% male Healthy | 6 | Crossover. Double-blind RCT. 2 phases. 3-day polyphenol depletion prior to single consumption (after overnight fast), 1-week washout. | Single consumption of 1000 g of conventional apples (NO) or organic apples (O). | Antioxidant activity, LDL oxidation, DNA damage (comet assay). | There were no statistically significant differences between groups on DNA damage, antioxidant activity or LDL oxidation. | Cultivated according to the requirements of “Bio Suisse” (predominant label organisation for certified organic production in Switzerland). |
| Grinder-Pedersen (2003) [41] | Denmark Age: 21–35 years 6 males + 10 females Healthy | 16 | Crossover. Double-blind RCT. 2 phases. 1 week run-in (excluding flavonoid-containing foods), 22 days each intervention with 3-week washout. | Whole diet intervention. Two intervention diets: conventional (NO) and organic (O); consisted of 4 different menus with identical meals and quantities. | SOD, Gpx, GR, Cat, TEAC, FRAP, malondialdehyde, 22-AAS. 24hr urine samples (Days 0 and 22): measured flavonoids (quercetin, kaempferol, and isorhamnetin) and flavonones (naringenin and hesperitin). | Quercetin (p < 0.01) and 2-AAS (p < 0.05) were significantly higher, as was urinary excretion of quercetin and kaempferol (p < 0.05) in O phase. TEAC was significantly increased (p < 0.05) after intake of NO compared to O. No significant difference was seen for isorhamnetin (p = 0.07) or kaempferol (p = 0.10). | No organic certification defined. The study used local, known conventional and organic growers (pork - from same litter, dairy, eggs, fruit and vegetables sowed and harvested within same week and from similar geographic location). |
| Akcay (2004) [42] | Turkey Age: 24–54 years 6 male + 2 female Healthy | 8 | Crossover trial. 2 phases. 6-week washout. | Single dose of conventional wine (NO), or organic wine (O). Men drank 200 mL (alcohol content 24 g) and women drank 100 mL (alcohol content 12 g) over 15 minutes. | Blood samples at 0, 60 and 360 minutes, measured total phenol content, SOD, Cat, TBARS, LDL-TBARS. | Very poorly reported results. SOD increased at 1 hour (p = 0.046) and 6 hours (p = 0.028) in O group compared to baseline (no group comparison). SOD at 6 hour increased in NO group compared to baseline (no values given). No significant difference in TBARS. | No organic certification defined. "The organic wine Cabernet Sauvignon (CS) was obtained by defined standards (certificated grapes of Vitis vinifera origin..” |
| Lu (2006) [43] | United States Age: 3–11 years 13 male + 10 female School children | 23 | Crossover trial. 3 phases: conventional diet (NO) days 1–3 and days 9–15, organic diet (O) days 4–8. | Food items were substituted for most of children’s conventional diet, including fruits, vegetables and grains for 5 days. Urine samples (first and last of the day) collected for whole 15 day period. | Metabolites for selected OP pesticides, pyrethroid insecticides, and herbicides. | Immediately after beginning O diet, median urinary MDA and TCPY decreased to non-detectable levels, where they remained until conventional diets were reintroduced (p < 0.01). No effect of diets on other metabolites. | No organic certification defined. "All organic food items were purchased by the research staff from a single grocery store.” |
| Lu (2008) [44] | United States Age: 3–11 years 13 male + 10 female School children | 23 | Crossover trial. 3 phases: conventional diet (NO) days 1–3 and days 9–15, organic diet (O) days 4–8. | Details as above, including testing for 15- or 12-consecutive-days in the summer (July–August) and fall (October–November), respectively, and a 7-consecutive-day sampling period in both the winter (January–February) and spring (April–May). | Metabolites for selected OP pesticides, pyrethroid insecticides, and herbicides. | Authors observed a seasonal effect on organophosphorus urinary biomarker levels in this cohort, and this seasonality corresponds to the consumption of fresh produce among the children throughout the year. This study is extended seasonal data for the same study detailed in Lu 2006. | No organic certification defined. "All organic food items were purchased by the research staff from a single grocery store.” |
| Di Renzo (2007) [45] | Italy Age: 30–65 years 100% male Healthy | 10 | Crossover trial. 2 phases. 14 days diet 1, then 14 days diet 2 - no washout. | Conventional Mediterranean diet intervention (NO), followed by organic Mediterranean diet intervention (O). | Plasma antioxidant (ORAC) capacity. | ORAC after NO Mediterranean diet was 2.25 mM TE, and 2.75 mM TE after O Mediterranean diet. This was a significant increase (21%) after the consumption of O diet. | No organic certification defined. Described as an "exclusively organic" diet for the organic treatment arm. |
| De Lorenzo (2010) [46] | Italy Age: 30–65 years 100% male n=100 healthy; n=50 stable chronic kidney disease (CKD) | 150 | Crossover trial. 2 phases. 14 days diet 1, then 14 days diet 2 - no washout. | Organic Mediterranean diet intervention (NO), followed by organic Mediterranean diet intervention (O). | BMI, DXA, Hcy, serum phosphorus, blood glucose concentrations, lipid profile, inflammatory markers, microalbuminuria. | DXA showed significant differences between NO Mediterranean diet and O Mediterranean diet for fat mass (p < 0.001), average loss of 6.1 kg. Significant decrease in cholesterol (p = 0.04), calcium and microalbuminuria (p = 0.003) after O diet only in CKD patients. Inflammatory parameters decreased in both groups after the O diet. | No organic certification defined. Described as an "exclusively organic" diet for the organic treatment arm. |
| Soltoft (2011) [47] | Denmark Age: 18–40 years 100% male Healthy | 18 | Crossover. Double-blind RCT. 3 phases. 12 days each intervention with 2 week wash-out. | 3 x treatment arms. (OA: organic based on livestock manure, OB: organic based on green manure and NO: conventional with mineral fertilizers) grown in two consecutive years (year 1 and 2). Diets fully controlled. | Fasting blood samples (day 1 and day 13 of each treatment arm) analysed for carotenoid content. | There was no significant difference in the plasma carotenoid content from the three different diets. There was very little difference between the concentrations of carotenoids in the carrots across growth systems, or across year to year of crops. | The organic growth systems were managed in compliance with the Danish guidelines for organic farming administered by the Danish Plant Directorate. |
| Toaldo (2016) [48] | Brazil Age: 20–55 years 15 male + 28 female Healthy | 24 | Crossover. Single-blind RCT. 3 phases. 14-day washout. 3 days polyphenol depletion prior to acute dose. | 3 x treatment arms. Single dose of 400 mL of conventional juice (NO), organic juice (O), or water. Blood samples were collected at 0 and 60 minutes. | GSH, Cat, SOD, Gpx, TAC, glucose, and uric acid. | GSH increased by 8.2% (p < 0.001) and 7.0% (p < 0.05) after NO and O, respectively, with no significant difference between juices. CAT increased 22% after O (p < 0.001). SOD increased 12.9% and 16.3% after NO and O, respectively (p < 0.001). GPx increased 6.9% and 7.3%, respectively, after NO and O (p < 0.05). | No organic certification defined. "Two red grape juices were used in this study: an organic juice prepared with organic Bordo grapes and a conventional juice prepared with conventional grapes.." |
| Goen (2017) [49] | Switzerland Age: 46–49 years 1 male + 1 female Healthy | 2 | Crossover trial. 2 phases. 11 days on conventional diet, followed by 18 days organic diet, no washout. | Conventional diet (NO) or organic diet (O). Participants purchased/ prepared all food. Urine samples taken for last 4 days of each intervention. | Urinary pesticide excretion, including DAP, pyrethroid metabolites, chlorinated phenoxycarboxylic acids, glyphosate, AMPA. | This very small study (n = 2) shows some small but statistically significant reduction in some components of pesticide exposure with O diet. NO shows organophosphate pesticides and some chlorinated phenoxy carboxylic acids as main exposure components. | Not defined. "participants switched to exclusively organic food intake" |
| Bradman (2015) [31] | United States Age: 3–6 years 19 male + 21 female Pre-school children | 40 | Crossover trial. 3-phases: conventional diet (NO) days 1–4, organic diet (O) days 5–11, conventional diet (NO) days 12–16. | Prior to study children enrolled primarily consumed conventional diet. Urine samples collected over 16 consecutive days. Food diaries kept during study phases. | Urinary concentrations of pesticides (23 pesticide metabolites including specific and nonspecific metabolites for OP, pyrethrin, and pyrethroid insecticides and select herbicides). | Most metabolites were below LOD, mean concentrations of 6 were lower during O for all children, and were significant for total DAPs and dimethyl DAPs and 2,4-D (2,4-dichlorophenoxyacetic acid, a herbicide), with reductions of 40%, 49%, and 25%, respectively (p < 0.01). | No organic certification defined. Food for the organic phase was provided by the researchers according to the families shopping list request (to maintain diet similarity). |
| Oates (2014) [34] | Australia Age: mean 42 years 4 male + 9 female Healthy | 13 | Crossover. RCT. 2 phases: conventional diet (NO) or ≥80% organic diet (O). 7 days per intervention, no washout. | Participants maintained usual dietary choices and sourced own food. Spot morning urine sample analysed on day 8 of each diet. | Urinary concentrations of pesticides, including six DAP metabolites of OP pesticides (DMP, DMTP, DMDTP, DEP, DETP and DEDTP). | Statistically significant lower levels of urinary DMP and DMTP (p < 0.05), with a trend for DMDTP during O phase. No significant difference for DEP, DETP, and DEDTP. Overall pesticide results in the O phase were 89% lower than in NO phase (p = 0.013). | Not defined. "Participants were asked to consume as close to 100% conventional or organic food as possible during each 7 day dietary period." |
| Ref | Study Population | n | Design and Duration | Exposure/Treatment | Outcome Measures | Results | Definition of Organic |
|---|---|---|---|---|---|---|---|
| Jensen (1996) [50] | Denmark Age: mean 33 years 100% male Members of organic farming organisations (n = 55) / airline company (n = 141) | 196 | Cross-sectional study. Analysis of semen samples for sperm quality in male organic farmers and airline workers. | Diet, working conditions, health, and lifestyle were assessed with questionnaire. Those with >25% organic diet defined as organic group. Self-reported FFQ. | Comparison of sperm concentration, seminal volume, total sperm count, and sperm morphology. | Sperm concentration was 43.1% (95%CI 3.2%–98.8%, p = 0.033) higher among men eating organically produced food. Seminal volume, total sperm count, and sperm morphology were not different between groups. This was a short report and missing detail on organic diet definitions between groups. | No specific definition of organic. |
| Juhler (1999) [51] | Denmark Age: mean 38 years 100% male Organic farmers (n = 85) / conventional farmers (n = 171) | 256 | Cross-sectional study. Analysis of semen samples for sperm quality in organic vs. conventional farmers. | Farmers divided into three groups, according to organic production/proportion of organic food consumption: none (N, 0%), medium (M, 1–49%), or a high (H, 50–100%) proportion FV consumed. Self-reported FFQ. | Correlation between estimated dietary pesticide intakes and semen parameters (including sperm concentration, seminal volume, total sperm count, and sperm morphology). | Group N showed a significantly lower proportion of morphologically normal spermatozoa, but no difference in 14 other semen parameters. A higher intake of five specific pesticides equated with a lower percentage of dead spermatozoa. No other significant differences were found. | No specific definition of organic. |
| Chiu (2018) [52] | United States; Environment and Reproductive Health (EARTH) Study Age: mean 35 years 100% female Women attending fertility clinic | 325 | Prospective cohort. Artificially assisted reproduction (AAR) outcomes in women, including pregnancy/birth outcomes associated with high and low dietary pesticide exposure. | Self-reported FFQ, prior to starting AAR. A total Pesticide Residue Burden Score (PRBS) was calculated (based on pesticide residue data and organic FV intake). Classifications were organic >3 times/week, or non-organic <3 times/week. | Clinical outcomes included implantation, clinical pregnancy, live birth. Early ART end points included markers of ovarian responses to stimulation (peak estradiol levels, endometrial thickness, oocyte development, total oocytes), fertilization rate, and embryo quality. | High PRBS was inversely associated with probability of clinical pregnancy and live birth per initiated cycle. Compared with women in the lowest quartile of high-pesticide residue FV intake (<1 serving/day), women in the highest quartile (≥2.3 servings/d) had 18% (95%CI, 5%–30%) lower probability of clinical pregnancy and 26% (95%CI, 13%–37%) lower probability of live birth. No association was found between quartiles and early ART end points. The adjusted probabilities of total pregnancy loss were 7% (95%CI, 3%–15%), 23% (95%CI, 16%–33%), 24% (95% CI, 15%–36%), and 34% (95% CI, 20%–51%) for women in increasing quartiles of high–pesticide residue FV intake. | No specific definition of organic. Volunteers were asked to provide information on frequency of organic FV consumption (<3 vs ≥3 times/week). |
| Baudry (2018) [53] | France; Nutri-Net Santé Cohort study Age: mean 44 years 78% female General population | 68,946 | Prospective observational cohort study (internet-based). Followed for up to 7 years, looking at all first primary cancers diagnosed between study inclusion and November 2016. | FFQ and cancer data (self-reported, but verified with medical records in >90% of cases). Estimated intake of 16 organic food/beverage items recorded to determine an organic score. Organic quartiles: Q4 = highest organic food intake, Q1 = lowest organic food intake. | All first primary cancers diagnosed between study inclusion and November 2016. All cancer types considered cases except for basal cell skin carcinoma, which was not considered cancer. | High organic food scores were linearly and negatively associated with the overall risk of cancer (HR for Q4 vs Q1, 0.75; 95%CI, 0.63–0.88; P for trend = .001; absolute risk reduction, 0.6%; HR for a 5-point increase, 0.92; 95% CI, 0.88–0.96). Within individual cancer types, a significantly reduced HR was seen for those with Q4 intake vs. Q1 for all lymphomas, non-Hodgkin lymphoma and post-menopausal breast cancer. | No specific definition of organic. Consumption frequency of 264 food and drink items used to calculate organic score. |
| Baudry (2018) [20] | France; Nutri-Net Santé Cohort study Age: mean 58 years 70% female General population | 300 | Nested matched case-control study of 300 participants (150 low and 150 high organic food consumers), with available fasting blood samples for analysis. | Self-reported FFQ used to estimate organic food intake. Low and high organic food consumers were grouped according to proportion of organic food below 10% or above 50%. The average proportions of organic food in the diet were 3% (± 3) and 67% (± 13) in the conventional and organic groups, respectively. | Plasma concentrations of vitamins A and E as well as 6 carotenoids (α-carotene, β-carotene, β-cryptoxanthin, lutein, zeaxanthin, and lycopene), copper, cadmium, magnesium, iron, transferrin and ferritin, fatty acid composition. | No significant differences were found between the 2 groups for α-tocopherol and retinol, cadmium, copper, ferritin or transferrin. Organic consumers exhibited higher plasma concentrations of α-carotene, β-carotene, lutein, and zeaxanthin with no differences for other carotenoids. Organic consumers had higher magnesium, lower iron, lower palmitoleic acid, γ-linolenic acid, and docosapentaenoic acid, and higher linoleic acid. | No specific definition of organic. Consumption frequency of 264 food and drink items used to calculate organic score. |
| Baudry (2019) [54] | France; Nutri-Net Santé Cohort study Age: mean 58 years 70% female General population | 300 | Nested matched case-control study of 300 participants (150 low and 150 high organic food consumers), with available urine samples for analysis. | Self-reported FFQ used to estimate organic food intake. Low and high organic food consumers were grouped according to proportion of organic food below 10% or above 50%. The average proportions of organic food in the diet were 3% (± 3) and 67% (± 13) in the conventional and organic groups, respectively. | Urinary pesticide and metabolite concentrations (organophosphorus, pyrethroid, and azole compounds). | Pesticide concentrations were mostly below LOD. For pesticide metabolites, significantly higher levels of DETP, DMTP, total DAPs (organophosphorus metabolites) and free 3-PBA (a pyrethroid metabolite) were found among conventional consumers compared to organic consumers, with median concentration levels of diethylphosphate (0.196 versus 0.297), dimethylphosphate (0.620 versus 1.382), and total dialkylphosphates (0.12 versus 0.16), p < 0.05. | No specific definition of organic. Consumption frequency of 264 food and drink items used to calculate organic score. |
| Brantsæter (2016) [55] | Norway; The Norwegian Mother and Child Cohort Study (MoBa). 100% female Pregnant women who delivered a singleton male infant. | 35,107 | Prospective cohort. Pregnant women at gestational week 22 surveyed for organic food consumption with results correlated to prevalence of male infants born with hypospadias or cryptorchidism. | Self-reported FFQ collected information about average dietary intake since start of pregnancy over six groups of organically produced food (vegetables, fruit, bread/cereal, milk/dairy products, eggs, and meat). | Association between non-organic/organic food consumption (never/seldom vs sometimes/often/mostly) and development of hypospadias or cryptorchidism in male newborns. | Seventy-four male newborns were diagnosed with hypospadias (0.2%), and 151 with cryptorchidism (0.4%). Women who consumed any organic food during pregnancy were less likely to give birth to a boy with hypospadias (OR = 0.42; 95% CI: 0.25, 0.70, based on 21 exposed cases) than women who reported they never or seldom consumed organic food. Associations with specific organic foods were strongest for vegetable (OR = 0.36; 95% CI: 0.15, 0.85; 10 exposed cases) and milk/dairy (OR = 0.43; 95% CI: 0.17, 1.07; 7 exposed cases) consumption. No association was observed for consumption of organic food and cryptorchidism. | All food sold as organic in Norway must be certified by Debio. Debio is accredited organic by Norwegian Accreditation and by IFOAM. |
| Torjusen (2016) [56] | Norway; The Norwegian Mother and Child Cohort Study (MoBa) Age: mean 28 years 100% female Nulliparous pregnant females. | 28,192 | Prospective cohort. Pregnant women at gestational week 22 surveyed for organic food consumption with results correlated to prevalence of pre-eclampsia. | Among the 28,192 women in this study, the majority reported never/rarely eating organic food; 39.8% ate at least one organic food ‘sometimes’; 7% ate at least one organic food ‘often’; and 1.8% reported use of any organic food ‘mostly’. | Pre-eclampsia in pregnant women. | The prevalence of pre-eclampsia in the study sample was 5.3% (n = 1,491). Women who reported eating organic ‘often’ or ‘mostly’ (n = 2,493, 8.8%) had lower risk of pre-eclampsia than those who reported ‘never/rarely’ or ‘sometimes’ (crude OR = 0.76, 95%CI 0.61, 0.96; adjusted OR = 0.79, 95%CI 0.62, 0.99). The lower risk was evident also when adjusting for overall dietary quality. | No specific definition of organic. Frequent organic consumption was defined as eating organic food ‘often’ for at least one of the six food categories. |
| Christensen (2013) [57] | Denmark 100% female Mothers of boys operated on for hypospadias (n = 306) and matching control group (n = 306) | 612 | Retrospective case-control study. Retrospective interviews of organic dietary habits in mothers with male infant born with hypospadias and matched controls. | FFQ listed choice of organic food items in the first trimester for milk, other dairy, eggs, meat, FV. Responses consisted of often, sometimes, rarely and never. Current dietary habits (up to several years post-pregnancy) were taken as proxy for pregnancy diet. | Association between organic food consumption of specified food groups during pregnancy and prevalence of hypospadias in infant sons. | Higher OR for hypospadias was found with rare or no consumption of organic non-milk dairy products, however, the association was not statistically significant after adjustment (OR = 1.36, 95%CI 0.95, 1.94). A similar association was observed for mothers rarely or never choosing organic eggs (OR = 1.28, 95%CI 0.92, 1.79). Total organic intake showed no statistically significant association, however, mothers who never or rarely chose any organic products had nonsignificant increased odds of giving birth to a boy with hypospadias (adjusted OR = 1.31, 95%CI 0.78, 2.21). | No specific definition of organic. |
| Rist (2007) [58] | Netherlands; KOALA Birth Cohort Age: mean 33 years 100% female Breastfeeding mothers with conventional (NO) or alternative (O) lifestyle | 312 | Cross-sectional study. Analysis of breast milk for fatty acid content from lactating women with predominantly organic or non-organic food consumption. | FFQ at gestational week 34. Classification into four groups based on the origin of meat/dairy products only. Organic = >90% organic Moderate = 50-90% organic Conventional = <50% organic | Amount of conjugated linoleic acids in breast milk of lactating women, measured as trans-vaccenic acid (TVA) and cis-9,trans-11-octadecadienoic acid (Rumenic). | Rumenic acid increased in a statistically significant way moving from a conventional diet (n = 186) to a moderately organic diet (n = 33), to a strict organic diet (n = 37). TVA levels were higher in the two mostly organic quartiles than in the conventional or minimal groups. | No specific definition of organic. Food origin specified as conventional or organic and % of food group as <50 %, 50–90% or >90%. |
| Mueller (2010) [59] | Netherlands; KOALA Birth Cohort Age: mean 33 years 100% female Breastfeeding mothers with conventional (NO) or alternative (O) lifestyle | 310 | Cross-sectional study. Analysis of breast milk for trans fatty acid content from lactating women with predominantly organic or non-organic food consumption. | FFQ at gestational week 34. Classification into four groups based on the origin of meat/dairy products only. Organic = >90% organic Moderate = 50-90% organic Conventional = <50% organic | Amount of trans fatty acids (TFA) in breast milk of lactating women, measured as different trans fatty acid isomers. | Total TFA content of mothers’ milk in the compared groups ranged between 3 and 3.3% of total fatty acids. There were no significant differences in the total TFA content between groups of organic vs. non-organic intake or amount of dairy fat intake reported. | No specific definition of organic. Food origin specified as conventional or organic and % of food group as <50 %, 50–90% or >90%. |
| Kummeling (2008) [60] | Netherlands; KOALA birth Cohort Age: 2 years Infants with non-organic (NO) (n = 2,135), or organic diet (O) (n = 463) | 2598 | Prospective cohort. Mothers of infants surveyed about child’s organic food consumption and allergy symptoms at 3, 7, 12 and 24 months of age. | Parents completed FFQ at each time-point. Infants diet classified as: ‘conventional’ (<50% organic); ‘moderately organic’ (50–90% organic); ‘strictly organic’ (>90% organic). | Association between allergic symptoms reported by parents (including eczema, wheeze occurrence, rash) and intake of organic vs. conventional foods; IgE antibodies measured in a subset of children (n = 815). | Consumption of organic dairy products was associated with lower eczema risk (OR = 0·64, 95%CI 0·44, 0·93), but there was no association for development of eczema, wheeze or atopic sensitisation. No statistically significant associations were observed between organic food consumption and recurrent wheeze (OR = 0·51, 95%CI 0·26, 0·99) during the first 2 years of life. | In the Netherlands ‘organic’ products include biodynamic production, which carry the registered ‘EKO’ certification. |
| Stenius (2011) [61] | Sweden; ALLADIN Study Age: foetal period (2nd trimester of mother) – 24 months | 330 | Prospective cohort. Anthroposophic or non-anthroposophic families followed for development of allergic sensitisation in children, correlated with lifestyle factors (including organic food choice). | FFQ completed by pregnant women in 2nd trimester. Child followed for allergic sensitisation to 24 months. Organic food consumption in AL group was 80% and 5% in CL group. | IgE in cord blood and sensitisation to common allergens and total IgE at 6, 12, and 24 months of age. | Children of families with AL had a markedly decreased risk of sensitisation during the first 2 years of life compared with children of CL families with adjusted OR = 0.25 (95%CI 0.10, 0.64), p = 0.004. Children from families with a partly anthroposophic lifestyle had similar result with adjusted OR = 0.31 (95%CI 0.15, 0.54), p = 0.002. | No specific definition of organic. Organic/biodynamic diet evaluated as one of many lifestyle questions, with no detail of how this was quantified. |
| Buscail (2015) [62] | France; PELAIGE mother-child cohort Age: foetal period (from gestation) – 24 months | 1505 | Prospective observational cohort study. Mothers consumption of organic food mid-pregnancy and when infant is 2 years, correlated to episodes of otitis media. | Pregnant women completed questionnaires reporting domestic use of pesticides and consumption of organic diet during pregnancy at 19 weeks of gestation and again at age 2 of infant. Children were assessed for otitis media during early childhood. | Episodes of otitis media (OM) and recurrent OM in children. Urinary samples to measure pesticides (n = 248). Associations between pesticide measurements and OM. | Children whose mothers reported an organic diet during pregnancy had a reduced risk of OM (at least one episode, p trend = 0.01). No association was found between any outcome and residential proximity to crops. The presence in maternal urine of dealkylated triazine metabolites (herbicide) was positively associated with recurrent OM (OR = 2.12 (1.01 to 4.47)). | No specific definition of organic. Fruit, vegetables and cereals from a non-organic diet were selected as proxies for insecticide exposure. |
| Kesse-Guyot (2017) [63] | France; Nutri-Net Santé Cohort study Age: mean 45 years 78% Female General population | 62,224 | Prospective cohort (internet-based). Followed for up to 10 years, looking at body weight change, risk of overweight or obesity and consumption of organic food. | Self-reported FFQ and anthropometric data completed annually (average 3.1 year follow-up). Estimated intake of 16 organic food/beverage items recorded to determine an organic score (OS). Organic diet quartiles: Q4 = highest rate of organic food consumption, Q1 = lowest rate of organic food consumption. | Correlation between the OS and change in BMI during follow-up and risk of overweight and obesity. | Lower BMI increase was observed across quartiles of the OS (mean difference Q4 v.Q1 = −0.16 (95%CI −0.32, −0.01). An increase in the OS was associated with a lower risk of overweight and obesity (among non-overweight and non-obese participants at inclusion): OR for Q4 v. Q1 were 0.77 (95%CI 0.68, 0.86) and 0.69 (95%CI 0.58, 0.82), respectively. The association remained strong and highly significant, with a reduction in the risk of obesity of 37% at follow-up. A similar association was observed for overweight, although the strength of the association was smaller. | No specific definition of organic. Consumption frequency of 264 food and drink items used to calculate organic score. |
| Baudry (2017) [64] | France; Nutri-Net Santé Cohort study Age: mean 45 years 78% Female General population | 8174 | Cross-sectional analysis of proportion of organic food in the diet (overall and by food group) and prevalence of metabolic syndrome. | Participants filled out a self-administered FFQ, including 264 food and beverage items. Separated into tertiles of organic food consumption. | Correlation between level of organic food intake and prevalence of metabolic syndrome. | Higher organic food consumption was associated with a lower probability of metabolic syndrome, being negatively associated with prevalence, 0.69 (95%CI 0.61, 0.78) when comparing the third tertile of proportion of organic food in the diet with the first one (p < 0.0001). | No specific definition of organic. Consumption frequency of 264 food and drink items used to calculate organic score. |
| Bradbury (2014) [65] | United Kingdom; The Million Women Study Age: mean 59 years 100% Female General population | 623,080 | Prospective cohort. Study correlates frequency of organic food intake to cancer incidence in women, followed on average for 9.3 years. | Women without cancer at baseline completed a questionnaire asking ‘Do you eat organic food?’ with four possible responses: ‘never, sometimes, usually, and always.’ Repeated at follow-up (on average 9.3 yr). | Association of organic diet with cancer, including all cancers combined (except non-melanoma skin cancer), oral, oesophageal, stomach, colorectum, pancreas, lung, malignant melanoma, breast, endometrium, ovary, kidney, bladder, brain, non-Hodgkin lymphoma, multiple myeloma, and leukaemia. | At baseline, 30%, 63% and 7% of women reported never, sometimes, or usually/always eating organic food, respectively. Consumption of organic food was not associated with a reduction in the incidence of all cancer (n = 53,769 cases in total) (RR for usually/always vs never = 1.03, 95%CI 0.99, 1.07), soft tissue sarcoma (RR = 1.37, 95%CI 0.82, 2.27), or breast cancer (RR = 1.09, 95%CI 1.02, 1.15), but was associated with reduced risk for non-Hodgkin lymphoma (RR = 0.79, 95%CI 0.65, 0.96). | No specific definition of organic. |
| McGuire (2016) [66] | United States Age: mean 29 years 100% female Breastfeeding women 1–3 months postpartum | 41 | Cross-sectional study. Single milk and urine sample from each woman to assess level of pesticides. | 5 question survey that documented potential glyphosate exposure from environment and diet. 42% of the women identified as having "strictly or mainly organic food choices" | Glyphosate and AMPA concentrations in human milk, correlated with pesticide excretion in urine samples. | Glyphosate and AMPA were not detectable in milk samples. There were no significant effects of consuming organic over conventional foods or living on/near a farm compared with living in an urban/suburban region on concentrations of glyphosate (p = 0.1870 and 0.8773, respectively), or AMPA in urine (p = 0.1414 and 0.2525, respectively). | No specific definition of organic. Food intake was self-reported as either mainly organic or mainly conventional. |
| Curl (2003) [33] | United States Age: 2–5 years 56% Male Children | 39 | Cross-sectional study. Level of organic food (%) in diet correlated to pesticide excretion in urine. Food frequency data and urine samples were collected. | Parents of children interviewed about diet, health information and pesticide use, with 2 day food diary completed on day of child's urine sampling. Diet reported as mostly organic or mostly conventional. | 24-hour urine samples measured for urinary DAP or DMP concentrations. | The median total DMP concentration was approximately six times higher for children with conventional diets than for children with organic diets (0.17 and 0.03 µmol/L; p = 0.0003); mean concentrations differed by a factor of nine (0.34 and 0.04 µmol/L). | No specific definition of organic. >75% of dietary intake as organic or conventionally separated the two groups. |
| Curl (2015) [32] | United States Age: 45–84 years 50% Female Adults with subclinical cardiovascular disease | 6814 | Cross-sectional study. Food frequency data and urine samples were collected, correlating organic intake to urinary excretion of pesticides. | Diet was reported as mostly organic or conventional. Participants were asked about their “usual” intake of specific foods and beverages “over the past year.” Average pesticide intake was then calculated. | Correlation between pesticide intake and excretion of pesticides in urine. Sub-group analysis of urine samples for pesticides (n = 240). | Among conventional consumers, increasing tertile of estimated dietary organophosphate exposure was associated with higher DAP concentrations (p < 0.05). DAP concentrations were also significantly lower in groups reporting more frequent consumption of organic produce (p < 0.02). | No specific definition of organic. Foods eaten are correlated to US Dept Agriculture data on pesticide residues and a pesticide exposure number assigned. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vigar, V.; Myers, S.; Oliver, C.; Arellano, J.; Robinson, S.; Leifert, C. A Systematic Review of Organic Versus Conventional Food Consumption: Is There a Measurable Benefit on Human Health? Nutrients 2020, 12, 7. https://doi.org/10.3390/nu12010007
Vigar V, Myers S, Oliver C, Arellano J, Robinson S, Leifert C. A Systematic Review of Organic Versus Conventional Food Consumption: Is There a Measurable Benefit on Human Health? Nutrients. 2020; 12(1):7. https://doi.org/10.3390/nu12010007
Chicago/Turabian StyleVigar, Vanessa, Stephen Myers, Christopher Oliver, Jacinta Arellano, Shelley Robinson, and Carlo Leifert. 2020. "A Systematic Review of Organic Versus Conventional Food Consumption: Is There a Measurable Benefit on Human Health?" Nutrients 12, no. 1: 7. https://doi.org/10.3390/nu12010007
APA StyleVigar, V., Myers, S., Oliver, C., Arellano, J., Robinson, S., & Leifert, C. (2020). A Systematic Review of Organic Versus Conventional Food Consumption: Is There a Measurable Benefit on Human Health? Nutrients, 12(1), 7. https://doi.org/10.3390/nu12010007