A Randomized, Placebo-Controlled Study on the Safety and Efficacy of Daily Ingestion of Green Tea (Camellia sinensis L.) cv. “Yabukita” and “Sunrouge” on Eyestrain and Blood Pressure in Healthy Adults

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
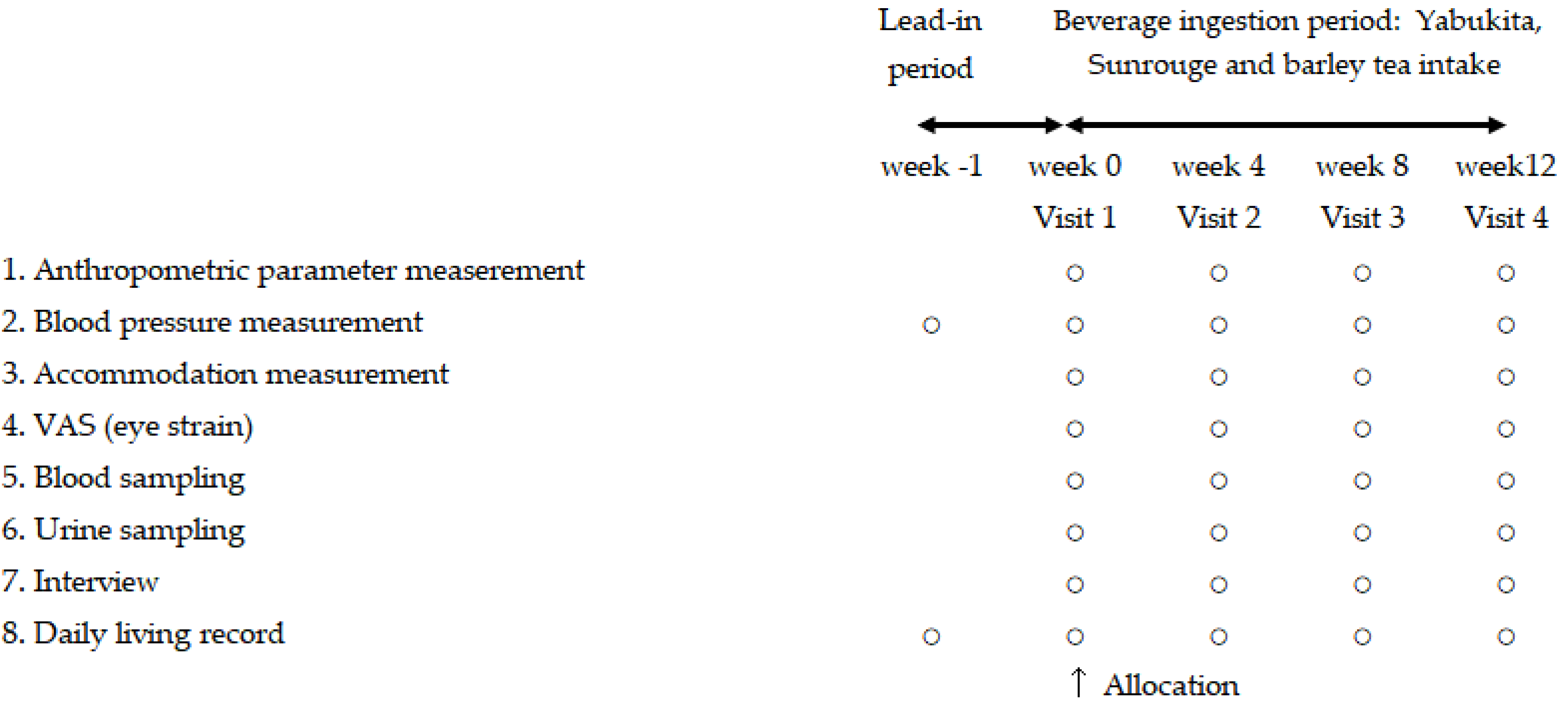
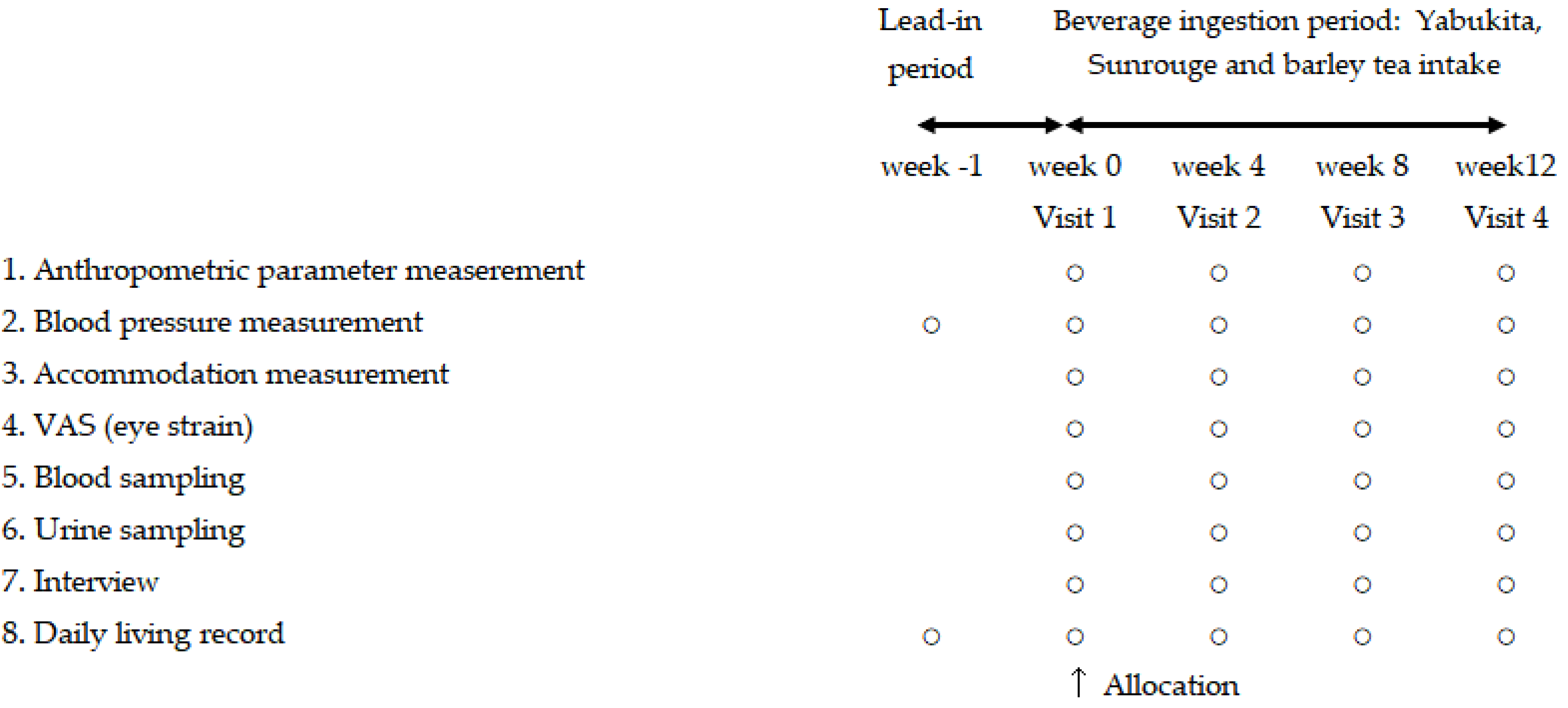
2.1. Study Design
2.2. Subjects
2.3. Test Samples
2.4. Study Outcomes
2.5. Measurement of Blood Pressure
2.6. Measurement of Accommodation after VDT Work Load
2.7. Measurement of Eyestrain Symptoms
2.8. Adverse Events
2.9. Ethics Committee
2.10. Statistical Analysis
3. Results and Discussion
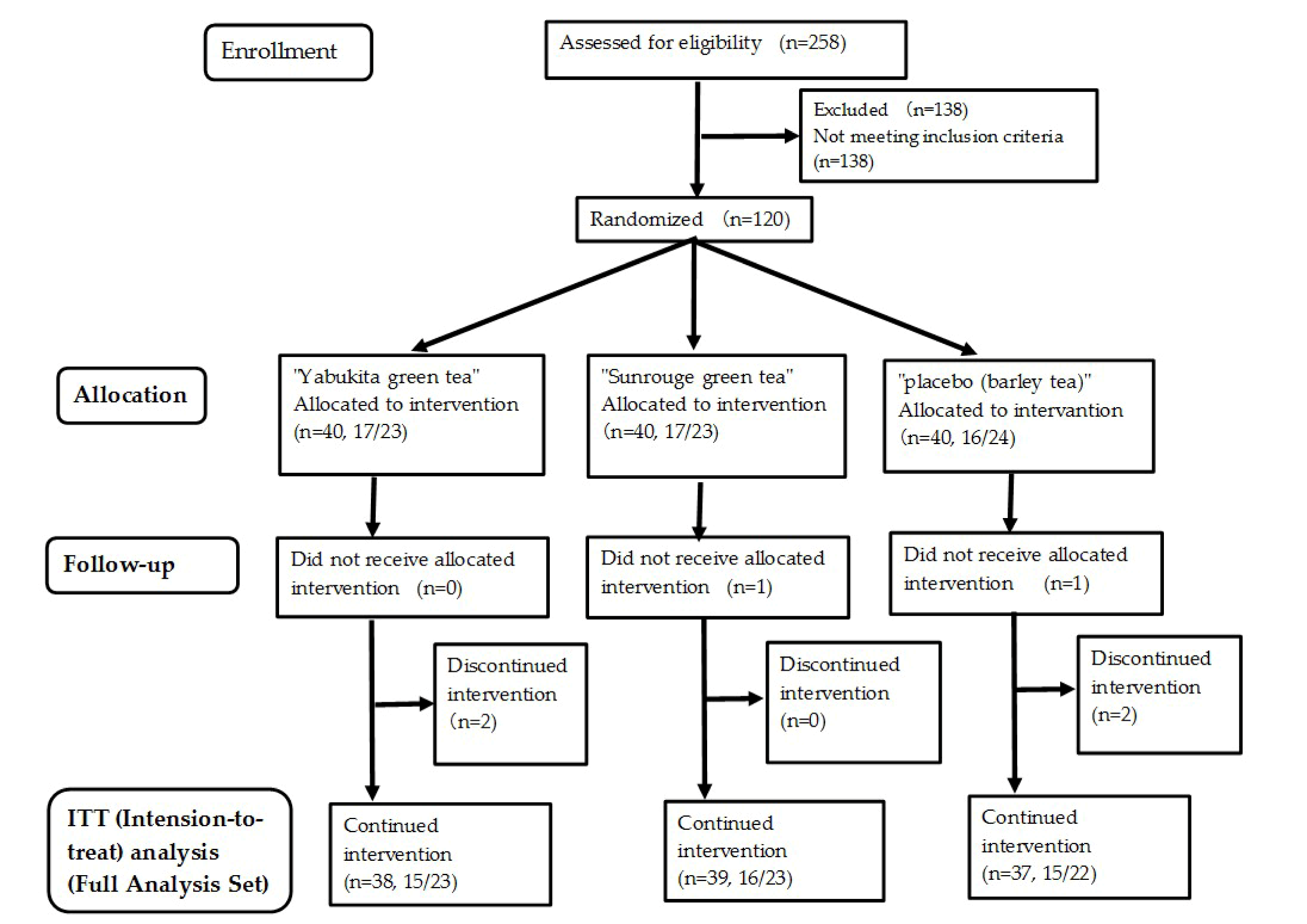
3.1. Number of Subjects and Intake Rate of Test Teas
3.2. Physical Characteristics
3.3. Primary Outcomes
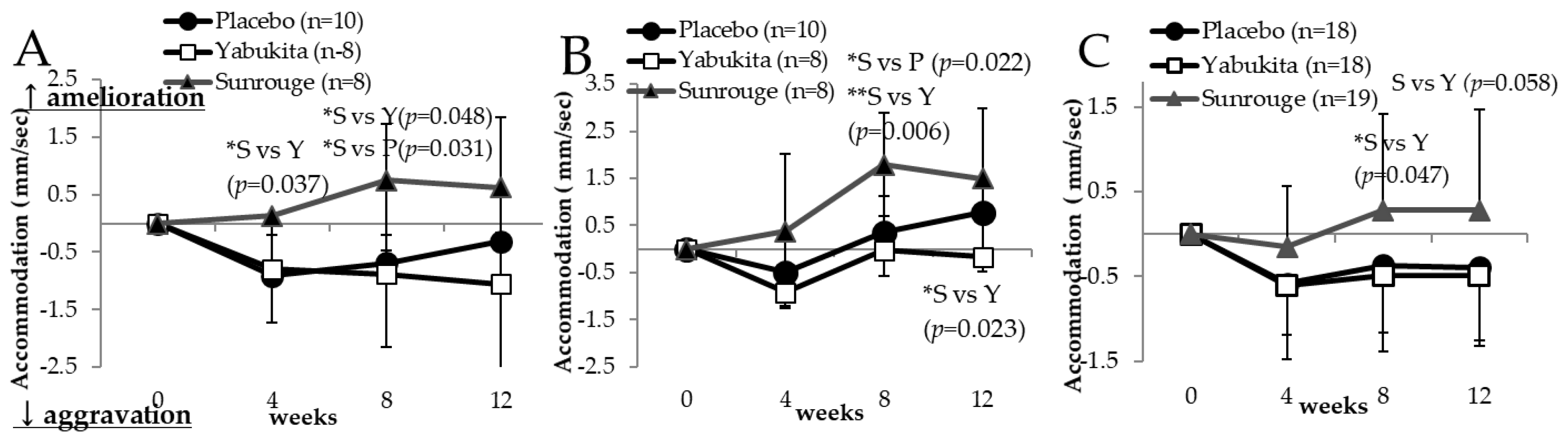
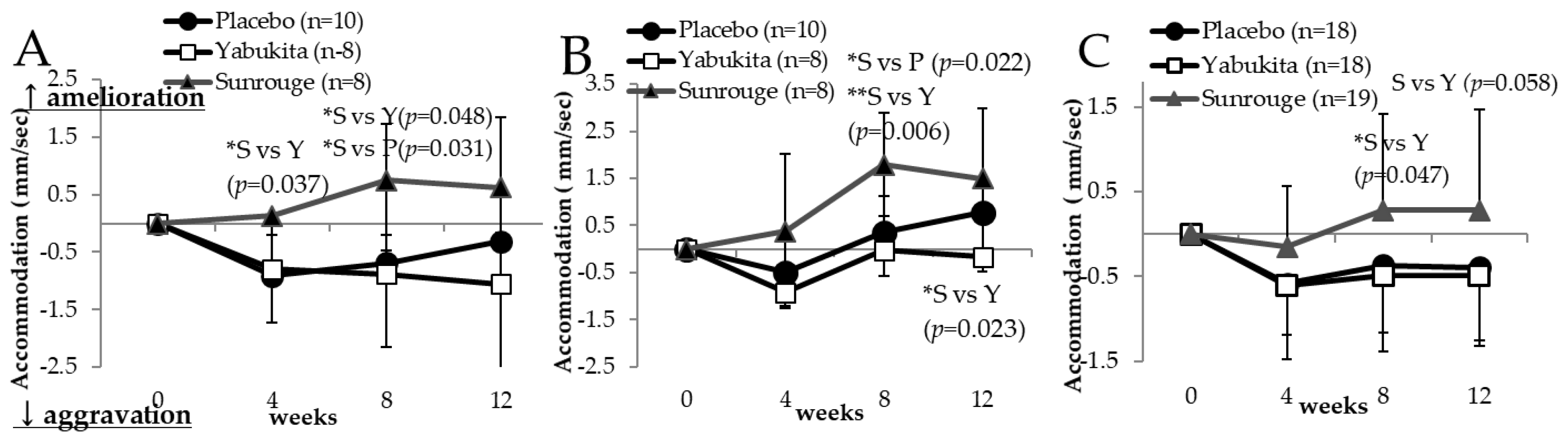
3.3.1. Accommodation Ability (AA)
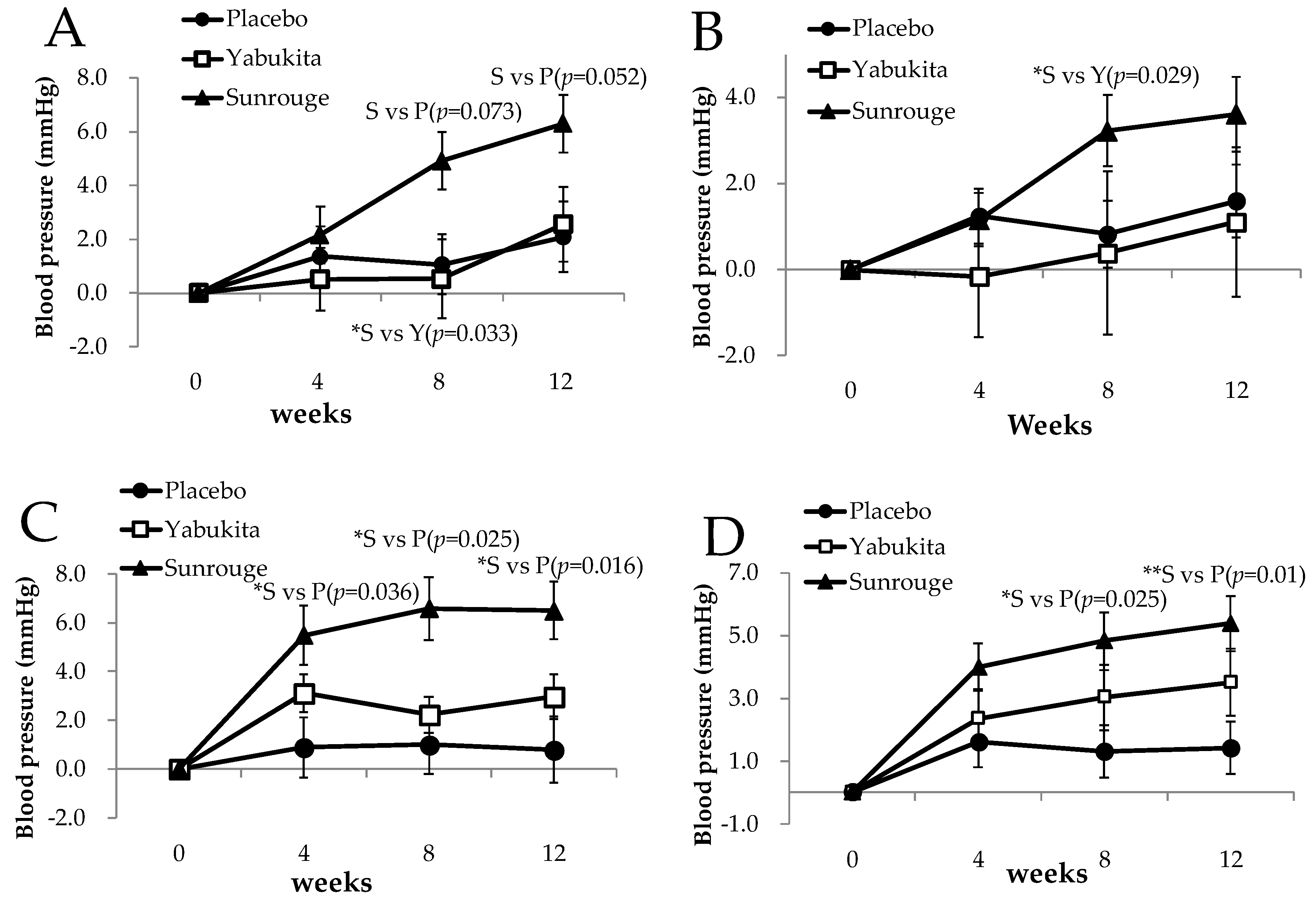
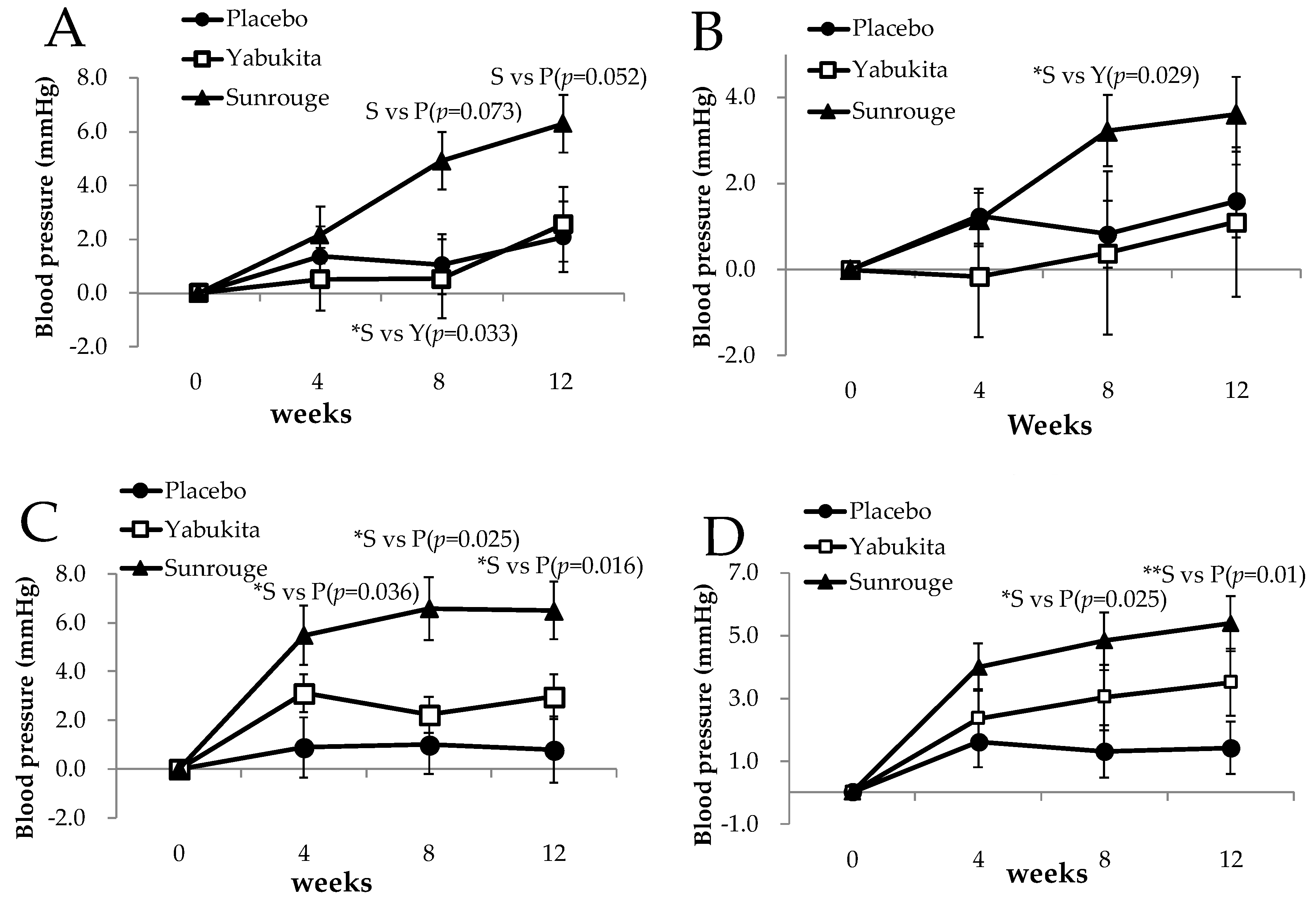
3.3.2. Home Blood Pressure
3.4. Secondary Outcomes
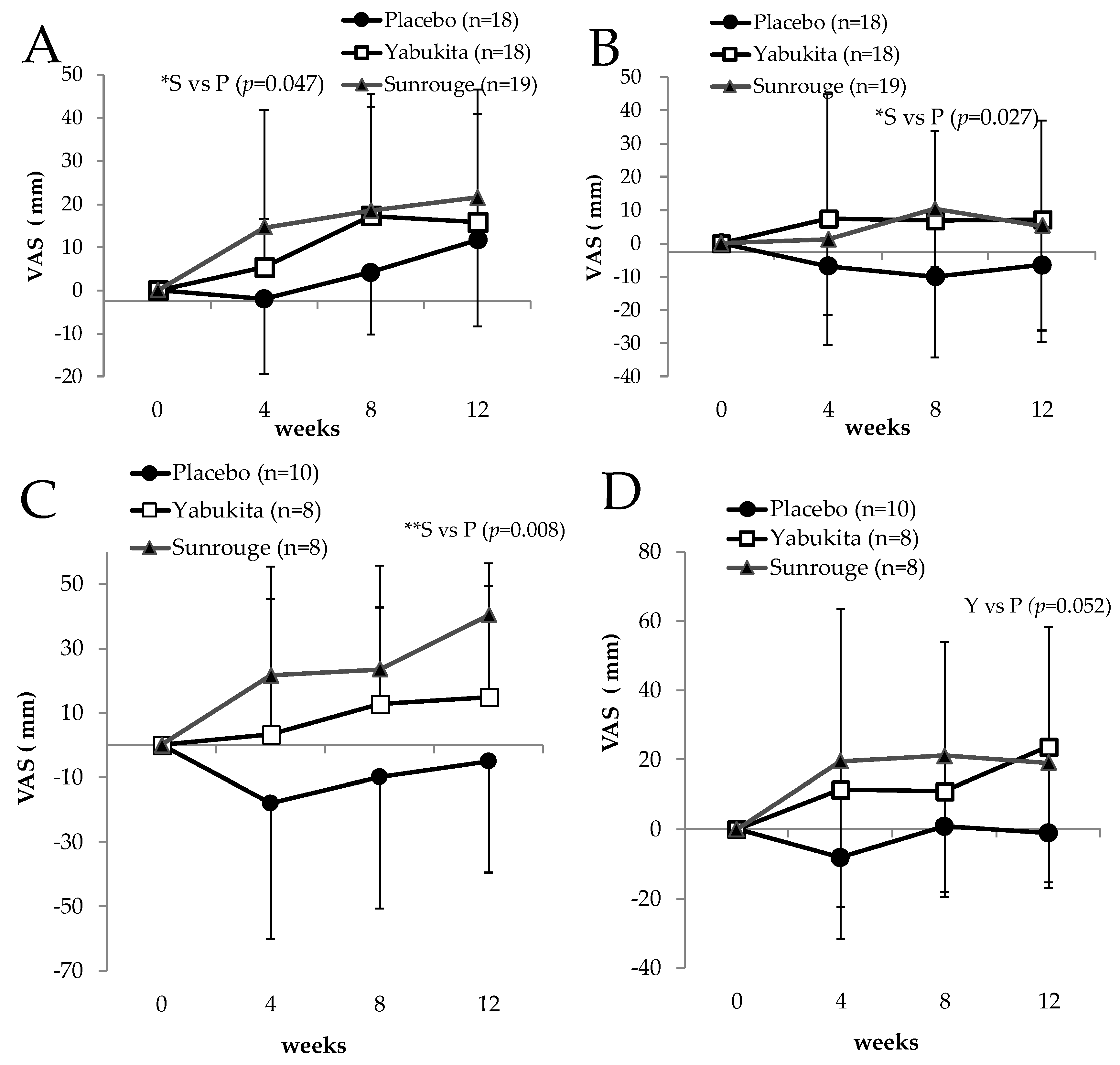
3.5. Eyestrain Symptoms
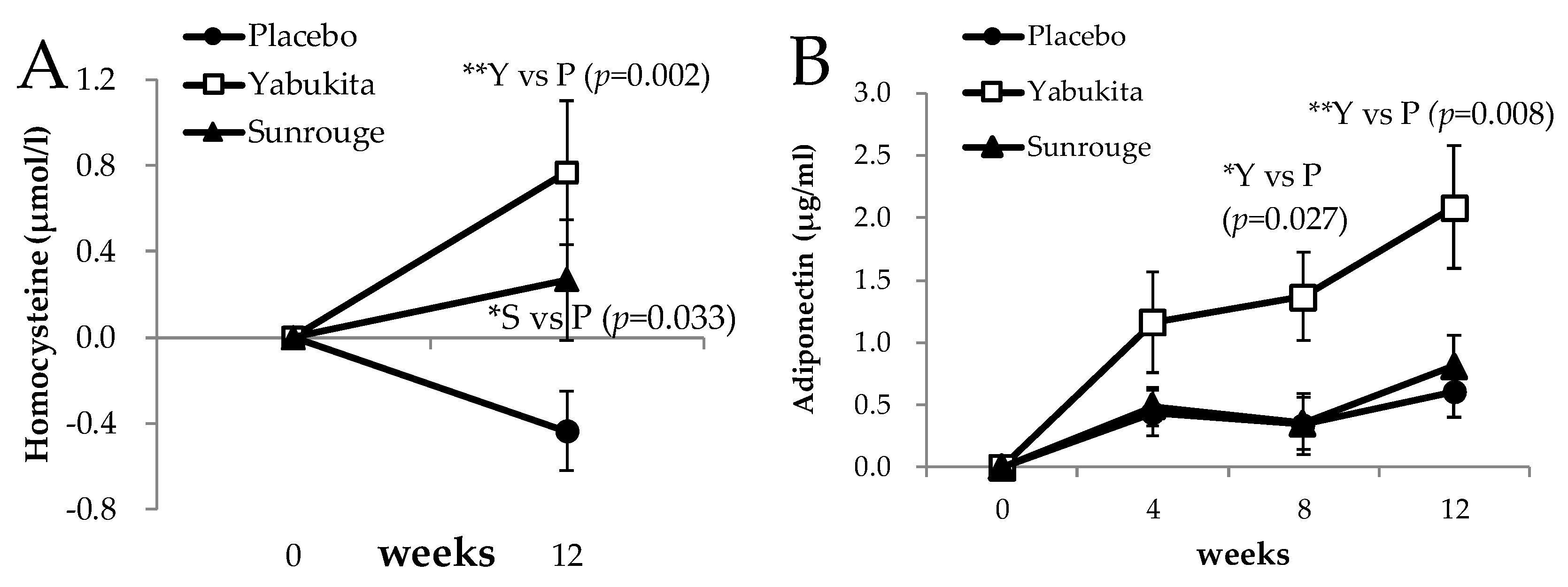
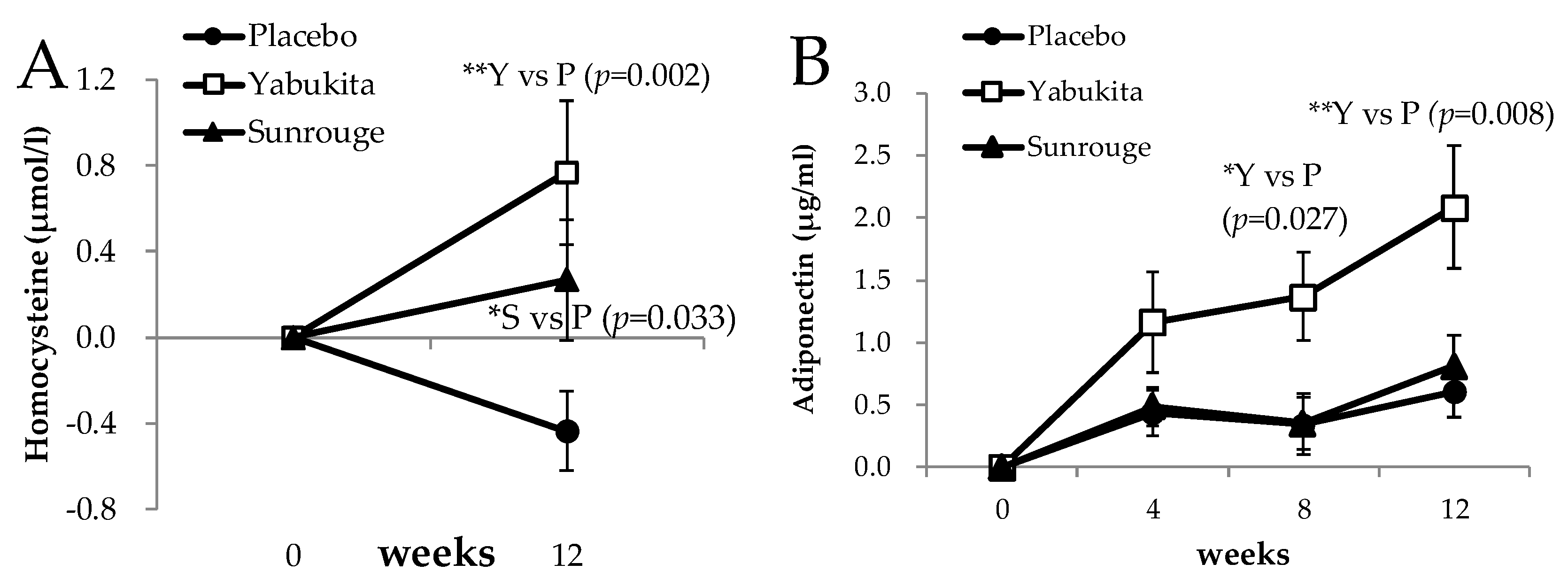
3.6. Endothelial Markers
3.7. Safety and Hospitalization
4. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Penetration of Internet, Japanese Ministry of Internal Affairs and Communications. Available online: http://www.soumu.go.jp/johotsusintokei/whitepaper/ja/h28/html/nc252110.html (accessed on 11 March 2018).
- Data about the Number of the Telecommunications Service the Contracts and the Share, Japanese Ministry of Internal Affairs and Communications. Available online: http://www.soumu.go.jp/menu_news/s-news/01kiban04_02000123.html (accessed on 11 March 2018).
- Ichikawa, H.; Honda, K.; Ohashi, M. Relation between Computer Screen Brightness in the Negative Display Mode and Work Efficiency and Fatigue. Joho Shakai Gakkaishi 2006, 1, 64–72. [Google Scholar]
- Khan, N.; Siddiqui, I.A.; Adhami, V.A.; Mukhtar, H. Green tea polyphenols for cancer risk reduction. In Green Tea polyphenols, Nutraceuticals of Modern Life; Juneja, L.R., Kapoor, M.P., Okubo, T., Rao, T.P., Eds.; CRC Press; Taylor & Francis Group: Boca Raton, FL, USA, 2013; pp. 57–82. ISBN 9781138199378. [Google Scholar]
- Sakuma, T.; Takase, H.; Hase, T.; Tokimutsu, I. Green tea polyphenols in weight management (Obesity) and diabetes. In Green Tea Polyphenols, Nutraceuticals of Modern Life; Juneja, L.R., Kapoor, M.P., Okubo, T., Rao, T.P., Eds.; CRC Press; Taylor & Francis Group: Boca Raton, FL, USA, 2013; pp. 157–176. ISBN 9781138199378. [Google Scholar]
- Keske, M.A.; Ng, H.L.; Premilovac, D.; Rattigan, S.; Kim, J.A.; Munir, K.; Yang, P.; Quon, M.J. Vascular and metabolic actions of the green tea polyphenol epigallocatechin gallate. Curr. Med. Chem. 2015, 22, 59–69. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.; Chiu, A.; Barone, M.K.; Avino, D.; Wang, F.; Coleman, C.I.; Phung, O.J. Green tea catechins decrease total and low-density lipoprotein cholesterol: A systematic review and meta-analysis. J. Am. Diet. Assoc. 2011, 111, 1720–1729. [Google Scholar] [CrossRef] [PubMed]
- Momose, Y.; Maeda-Yamamoto, M.; Nabetani, H. Systematic review of green tea epigallocatechin gallate in reducing low-density lipoprotein cholesterol levels of humans. Int. J. Food Sci. Nutr. 2016, 20, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Yokozawa, T.; Noh, J.S.; Park, C.H.; Park, J.C. Green tea polyphenols for protection of internal organs-focus on renal damage caused by oxidative stress. In Green Tea Polyphenols, Nutraceuticals of Modern Life; Juneja, L.R., Kapoor, M.P., Okubo, T., Rao, T.P., Eds.; CRC Press; Taylor & Francis Group: Boca Raton, FL, USA, 2013; pp. 177–204. ISBN 9781138199378. [Google Scholar]
- Khan, N.; Mukhtar, H. Tea and health: Studies in humans. Curr. Pharm. Des. 2013, 19, 6141–6147. [Google Scholar] [CrossRef] [PubMed]
- Maeda-Yamamoto, M. Human Clinical Studies of Tea Polyphenols in Allergy or Life Style-related Diseases. Curr. Pharm. Des. 2013, 19, 6148–6155. [Google Scholar] [CrossRef]
- Nejabat, M.; Reza, S.A.; Zadmehr, M.; Yasemi, M.; Sobhani, Z. Efficacy of green tea extract for treatment of dry eye and meibomian gland dysfunction; A double-blind randomized controlled clinical trial study. J. Clin. Diagn. Res. 2017, 11, NC05–NC08. [Google Scholar] [CrossRef] [PubMed]
- Nesumi, A.; Ogino, A.; Yoshida, K.; Taniguchi, F.; Maeda-Yamamoto, M.J.; Tanaka, J.; Murakami, A. ‘Sunrouge’, a new tea cultivar with high anthocyanin. Jpn. Agric. Res. Q. 2012, 46, 321–328. [Google Scholar] [CrossRef]
- Saito, T.; Honma, D.; Tagashira, M.; Kanda, T.; Maeda-Yamamoto, M. Anthocyanins from New Red Leaf Tea ‘Sunrouge’. J. Agric. Food Chem. 2011, 59, 4779–4782. [Google Scholar] [CrossRef] [PubMed]
- Maeda-Yamamoto, M.; Saito, T.; Nesumi, A.; Tokuda, Y.; Ema, K.; Honma, D.; Ogino, A.; Monobe, M.; Murakami, A.; Murakami, A.; et al. Chemical analysis and acetylcholinesterase inhibitory effect of anthocyanin-rich red leaf tea (cv. Sunrouge). J. Sci. Food Agric. 2012, 92, 2379–2386. [Google Scholar] [CrossRef] [PubMed]
- Khoo, H.E.; Azlan, A.; Tang, S.T.; Lim, S.M. Anthocyanidins and anthocyanins: Colored pigments as food, pharmaceutical ingredients, and the potential health benefits. Food Nutr. Res. 2017, 61, 1361779. [Google Scholar] [CrossRef] [PubMed]
- Kurita, I.; Maeda-Yamamoto, M.; Tachibana, H.; Kamei, M. Antihypertensive Effect of Benifuuki Tea Containing O-methylated EGCG. J. Agric. Food Chem. 2010, 58, 1903–1908. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.L.; Lane, J.; Coverly, J.; Stocks, J.; Jackson, S.; Stephen, A.; Bluck, L.; Coward, A.; Hendrickx, H. Effects of dietary supplementation with the green tea polyphenol epigallocatechin-3-gallate on insulin resistance and associated metabolic risk factors: Randomized controlled trial. Br. J. Nutr. 2009, 101, 886–894. [Google Scholar] [CrossRef] [PubMed]
- Nakaishi, H.; Matsumoto, H.; Tominaga, S.; Hirayama, M. Effects of black current anthocyanoside intake on dark adaptation and VDT work-induced transient refractive alteration in healthy humans. Altern. Med. Rev. 2000, 5, 553–562. [Google Scholar] [PubMed]
- Lee, J.; Lee, H.K.; Kim, C.Y.; Hong, Y.J.; Choe, C.M.; You, T.W. Purified high-dose anthocyanoside oligomer administration improves nocturnal vision and clinical symptoms in myopia subjects. Br J. Nutr. 2005, 93, 895–899. [Google Scholar] [CrossRef] [PubMed]
- Nair, A.G.; Patil-Chhablani, P.; Venkatramani, D.V.; Gandh, R.A. Ocular myasthenia gravis: A review. Indian J. Ophthalmol. 2014, 62, 985–991. [Google Scholar] [PubMed]
- Monobe, M.; Nomura, S.; Ema, K.; Matsunaga, A.; Nesumi, A.; Yoshida, K.; Maeda-Yamamoto, M.; Horie, H. Quercetin Glycosides-rich Tea Cultivars (Camellia sinensis L.) in Japan. Food Sci. Technol. Res. 2015, 21, 333–340. [Google Scholar] [CrossRef]
- Naruszewicz, M.; Łaniewska, I.; Millo, B.; Dłużniewski, M. Combination therapy of statin with flavonoids rich extract from chokeberry fruits enhanced reduction in cardiovascular risk markers in patients after myocardial infraction (MI). Atherosclerosis 2007, 194, e179–e184. [Google Scholar] [CrossRef] [PubMed]
- Wallace, T.C.; Slavin, M.; Frankenfeld, C.L. Systematic Review of Anthocyanins and Markers of Cardiovascular Disease. Nutrients 2016, 8, 32. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.Y.; Wu, H.; Li, D.J.; Song, J.F.; Xiao, Y.D.; Liu, C.Q.; Zhou, J.Z.; Sui, Z.Q. Protective Effects of Blueberry Anthocyanins against H2O2-Induced Oxidative Injuries in Human Retinal Pigment Epithelial Cells. J. Agric. Food Chem. 2018, 66, 1638–1648. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, H.; Nakamura, Y.; Tachibanaki, S.; Kawamura, S.; Hirayama, M. Stimulatory effect of cyanidin 3-glycosides on the regeneration of rhodopsin. J. Agric. Food Chem. 2003, 51, 3560–3563. [Google Scholar] [CrossRef] [PubMed]
- Shimada, M.; Mochizuki, K.; Sakurai, N.; Goda, T. Dietary supplementation with epigallocatechin gallate elevates levels of circulating adiponectin in non-obese type-2 diabetic Goto-Kakizaki rats. Biosci. Biotechnol. Biochem. 2007, 71, 2079–2082. [Google Scholar] [CrossRef] [PubMed]
- Shimada, K.; Kawarabayashi, T.; Tanaka, A.; Fukuda, D.; Nakamura, Y.; Yoshiyama, M.; Takeuchi, K.; Sawaki, T.; Hosoda, K.; Yoshikawa, J. Oolong tea increases plasma adiponectin levels and low-density lipoprotein particle size in patients with coronary artery disease. Diabetes Res. Clin. Pract. 2004, 65, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.; Zhao, Y.; Zhao, B. Green tea catechins prevent obesity through modulation of peroxisome proliferator-activated receptors. Sci. China Life Sci. 2013, 56, 804–810. [Google Scholar] [CrossRef] [PubMed]
- Risk and Alerts. Green Tea Weight Management. Available online: http://healthycanadians.gc.ca/recall-alert-rappel-avis/hc-sc/2006/9538r-eng.php?_ga=2.19965181.456035033.1523512048-1311801335.1523512048 (accessed on 12 April 2018).
- Hu, J.; Webster, D.; Cao, J.; Shao, A. The safety of green tea and green tea extracts consumption in adults-Results of a systematic review. Regul. Toxicol. Pharmacol. 2018. pii:02732 S–S300(18)30092-8. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| “Yabukita” Green Tea | “Sunrouge” Green Tea | Placebo Barley Tea | |
|---|---|---|---|
| Anthocyanins | 0.0 | 11.2 * | 0.0 |
| EGCG 2 | 322.2 | 323.6 | 0.0 |
| EGC 3 | 413.1 | 85.7 | 0.0 |
| EGCG3”Me 4 | 0.0 | 12.3 | 0.0 |
| Flavonols | 54.8 5 | 40.4 6 | 0.0 |
| Caffeine | 202.5 | 184.8 | 0.0 |
| Baseline Characteristics | “Yabukita” | “Sunrouge” | Placebo |
|---|---|---|---|
| Gender(male/female) (n) | 38 (15/23) | 39 (16/23) | 37 (15/22) |
| Age (years) | 49.8 ± 6.7 | 49.5 ± 6.2 | 48.5 ± 7.5 |
| Body weight (kg) | 64.3 ± 9.7 | 61.4 ± 11.7 | 62.1 ± 10.0 |
| Body mass index (kg/m2) | 23.9 ± 3.3 | 23.3 ± 3.4 | 23.3 ± 2.4 |
| Body fat ratio (%) | 28.9 ± 6.9 | 27.9 ± 6.3 | 28.7 ± 6.7 |
| Home SBP at waking up (mmHg) | 126.8 ± 11.9 | 126.6 ± 14.2 | 124.6 ± 10.1 |
| Home DBP at waking up (mmHg) | 80.5 ± 9.8 | 81.8 ± 9.8 * | 77.3 ± 7.4 |
| Home SBP at bedtime (mmHg) | 123.7 ± 11.9 | 123.3 ± 12.9 | 123.7 ± 11.0 |
| Home DBP at bedtime (mmHg) | 75.3 ± 10.0 | 77.1 ± 8.5 | 74.8 ± 7.0 |
| Pulse (bpm) | 74.6 ± 9.9 | 75.8 ± 11.1 | 74.4 ± 10.7 |
| Interventions | Week 0 | Week 4 | Week 8 | Week 12 | |
|---|---|---|---|---|---|
| Home SBP at waking up | “Yabukita” | 126.8 ± 11.9 | 127.3 ± 11.9 | 127.3 ± 13.8 | 129.3 ± 14.4 |
| (mmHg) | “Sunrouge” | 126.6 ± 14.2 | 128.8 ± 13.5 # | 131.5 ± 13.4 *## | 132.9 ± 14.3 *## |
| Placebo | 124.6 ± 10.1 | 125.2 ± 9.4 | 125.6 ± 9.2 | 126.7 ± 10.5 | |
| Home DBP at waking up | “Yabukita” | 80.5 ± 9.8 | 80.3 ± 8.7 | 80.8 ± 9.7 | 81.6 ± 1.6 |
| (mmHg) | “Sunrouge” | 81.8 ± 9.8 * | 83.0 ± 8.7 * | 85.1 ± 8.8 **## | 85.5 ± 1.5 **## |
| Placebo | 77.3 ± 7.4 | 78.4 ± 7.0 | 78.1 ± 7.7 | 78.9 ± 1.4 | |
| Home SBP at bedtime | “Yabukita” | 123.7 ± 11.9 | 126.8 ± 13.5 | 125.9 ± 15.6 | 126.3 ± 14.7 |
| (mmHg) | “Sunrouge” | 123.3 ± 12.9 | 128.8 ± 13.8 ## | 129.9 ± 13.7 ## | 129.8 ± 12.7 ## |
| Placebo | 123.7 ± 11.0 | 123.8 ± 13.8 | 124.7 ± 10.5 | 124.5± 12.6 | |
| Home DBP at bedtime | “Yabukita” | 75.3 ± 10.0 | 77.7± 10.3 | 78.4 ± 10.9 | 78.8 ± 11.1 |
| (mmHg) | “Sunrouge” | 77.1 ± 8.5 | 81.0 ± 8.9 *## | 81.9 ± 8.5 **## | 82.4 ± 8.2 **## |
| Placebo | 74.8 ± 7.0 | 76.3 ± 7.3 | 76.1 ± 8.7 | 76.2 ± 9.0 |
| Interventions | Week 0 | Week 4 | Week 8 | Week 12 | |
|---|---|---|---|---|---|
| Oxidation marker | |||||
| TBARS (mM) | “Yabukita” | 13.7 ± 3.5 | 16.2 ± 5.4 *# | 9.9 ± 3.3 ## | 12.8 ± 3.8 |
| “Sunrouge” | 13.0 ± 3.3 | 13.9 ± 5.3 | 9.1 ± 3.5 ## | 12,0 ± 4.0 | |
| Placebo | 13.8 ± 3.7 | 14.2 ± 3.9 | 8.5 ± 3.0 ## | 11.9 ± 3.5 # | |
| SOD (U/L) | “Yabukita” | 3.2 ± 1.8 | 2.7 ± 1.8 *# | 2.9 ± 1.9 *## | 2.7 ± 2.2 ## |
| “Sunrouge” | 3.0 ± 1.6 | 2.4 ± 1.6 ## | 2.9 ± 2.2 | 2.6 ± 2.1 ## | |
| Placebo | 2.6 ± 0.8 | 2.0 ± 0.8 ## | 2.3 ± 1.2 # | 2.1 ± 1.3 ## |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maeda-Yamamoto, M.; Nishimura, M.; Kitaichi, N.; Nesumi, A.; Monobe, M.; Nomura, S.; Horie, Y.; Tachibana, H.; Nishihira, J. A Randomized, Placebo-Controlled Study on the Safety and Efficacy of Daily Ingestion of Green Tea (Camellia sinensis L.) cv. “Yabukita” and “Sunrouge” on Eyestrain and Blood Pressure in Healthy Adults. Nutrients 2018, 10, 569. https://doi.org/10.3390/nu10050569
Maeda-Yamamoto M, Nishimura M, Kitaichi N, Nesumi A, Monobe M, Nomura S, Horie Y, Tachibana H, Nishihira J. A Randomized, Placebo-Controlled Study on the Safety and Efficacy of Daily Ingestion of Green Tea (Camellia sinensis L.) cv. “Yabukita” and “Sunrouge” on Eyestrain and Blood Pressure in Healthy Adults. Nutrients. 2018; 10(5):569. https://doi.org/10.3390/nu10050569
Chicago/Turabian StyleMaeda-Yamamoto, Mari, Mie Nishimura, Nobuyoshi Kitaichi, Atsushi Nesumi, Manami Monobe, Sachiko Nomura, Yukihiro Horie, Hirofumi Tachibana, and Jun Nishihira. 2018. "A Randomized, Placebo-Controlled Study on the Safety and Efficacy of Daily Ingestion of Green Tea (Camellia sinensis L.) cv. “Yabukita” and “Sunrouge” on Eyestrain and Blood Pressure in Healthy Adults" Nutrients 10, no. 5: 569. https://doi.org/10.3390/nu10050569
APA StyleMaeda-Yamamoto, M., Nishimura, M., Kitaichi, N., Nesumi, A., Monobe, M., Nomura, S., Horie, Y., Tachibana, H., & Nishihira, J. (2018). A Randomized, Placebo-Controlled Study on the Safety and Efficacy of Daily Ingestion of Green Tea (Camellia sinensis L.) cv. “Yabukita” and “Sunrouge” on Eyestrain and Blood Pressure in Healthy Adults. Nutrients, 10(5), 569. https://doi.org/10.3390/nu10050569