

Pathophysiology and Treatment of Psoriasis: From Clinical Practice to Basic Research

 and
and
Abstract
1. Introduction
2. Clinical Types of Psoriasis
3. Pathogenesis of Psoriasis
3.1. Histological Features
3.2. Etiology
3.3. Cell Signaling Pathways Related to Psoriasis
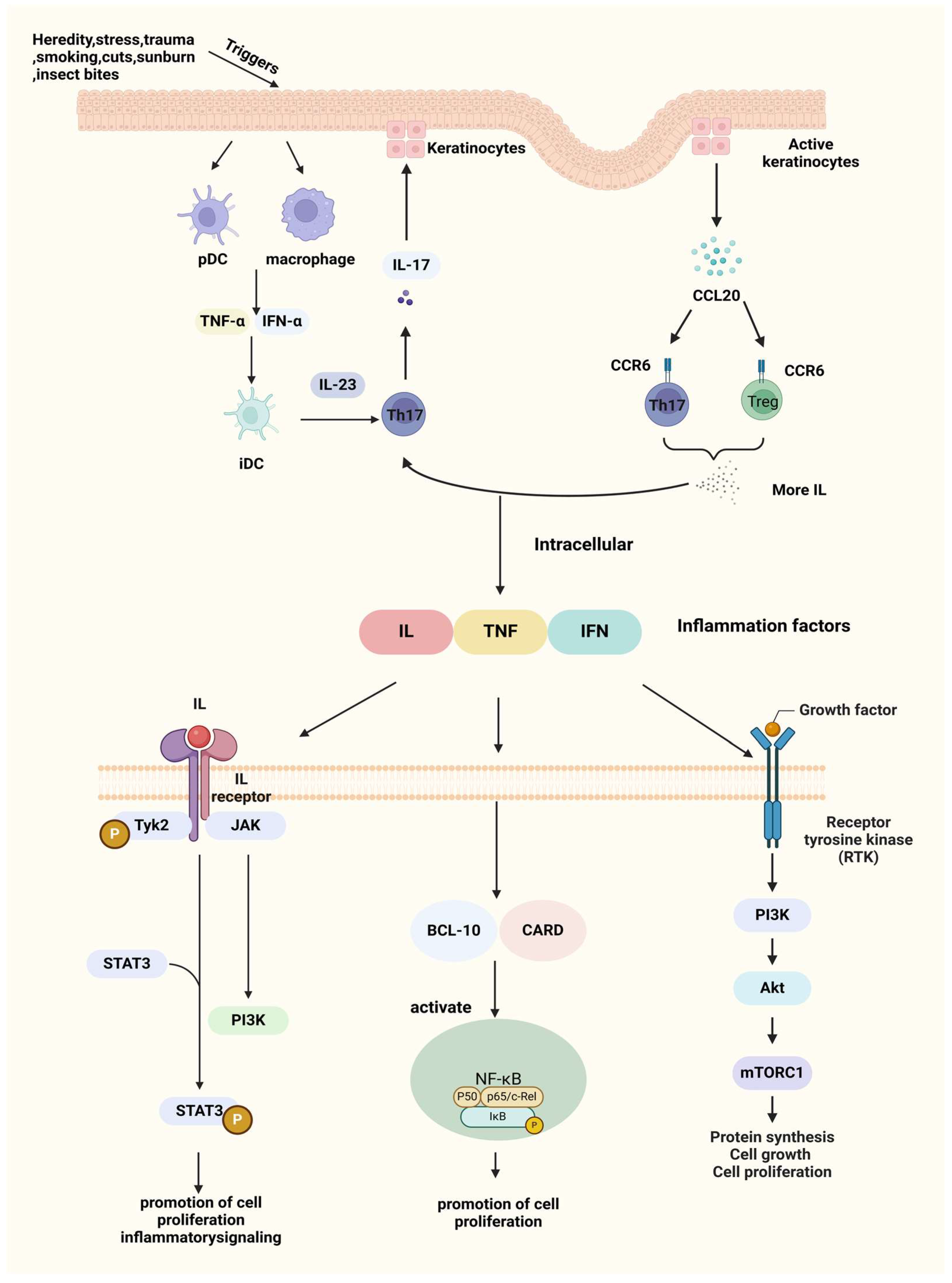
3.3.1. Interleukin-23/T Helper Cell (IL-23/Th17) Axis
3.3.2. Macrophage Inflammatory Protein 3 Alpha/Chemokine (C-C Motif) Ligand 20-C-C Chemokine Receptor 6(MIP-3α/CCL20-CCR6) Pathway
3.3.3. Nuclear Factor Kappa-B (NF-κB) Signaling Pathway
3.3.4. JAK (Janus Kinase)/STAT (Signal Transducer and Activator of Transcription) Signaling Pathway
3.3.5. Phosphatidylinositol 3 Kinase (PI3K)/Protein Kinase B (AKT) Signaling Pathway
4. Diagnosis and Clinical Treatment of Psoriasis
4.1. Diagnosis of Psoriasis
4.2. Clinical Treatment of Psoriasis
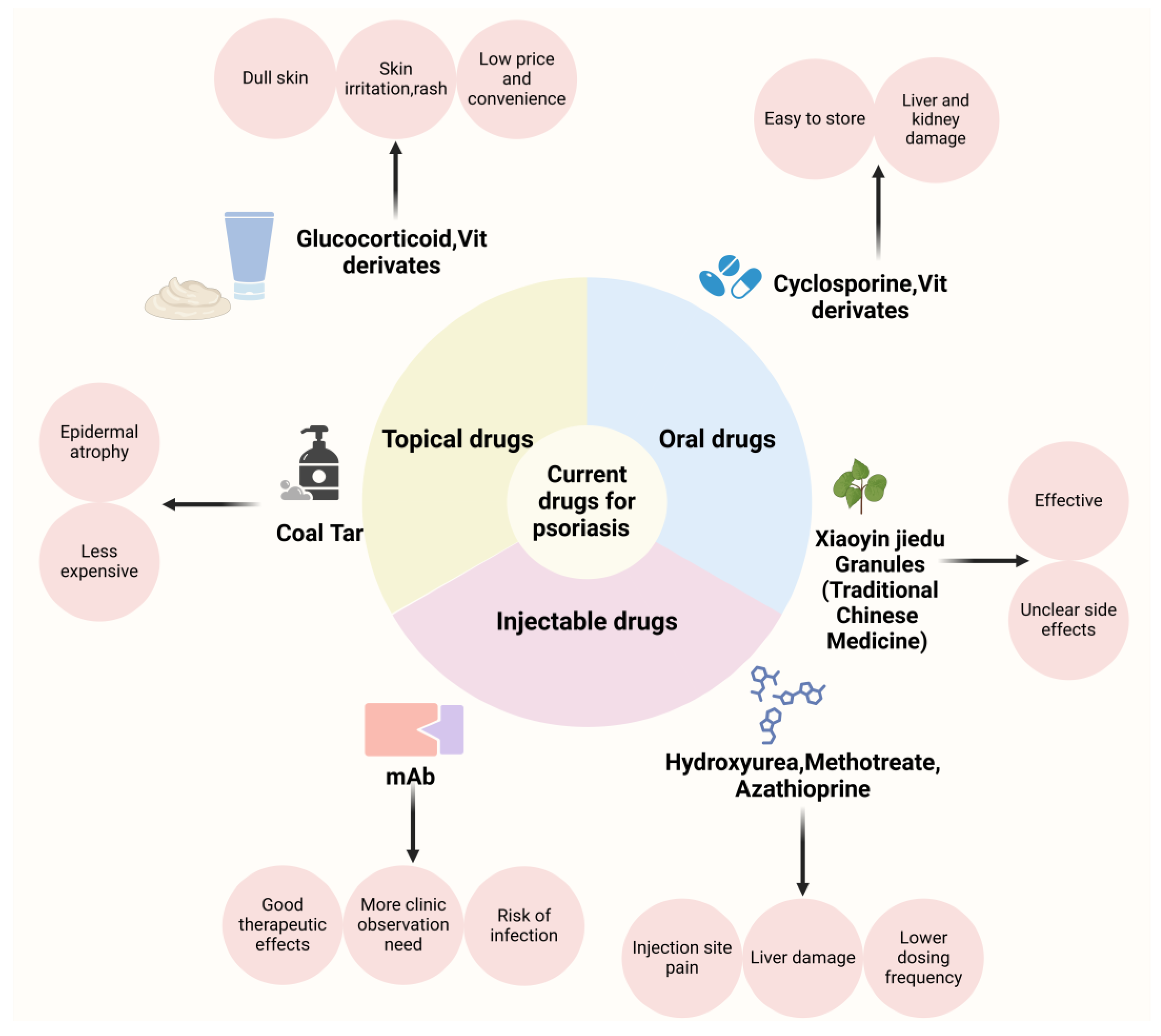
4.2.1. Oral Medicines for Psoriasis
4.2.2. Injectable Medications for Psoriasis
4.2.3. Topical Therapies for Psoriasis
5. Challenges and Innovations in Transdermal Drug Delivery System for Psoriasis Treatment
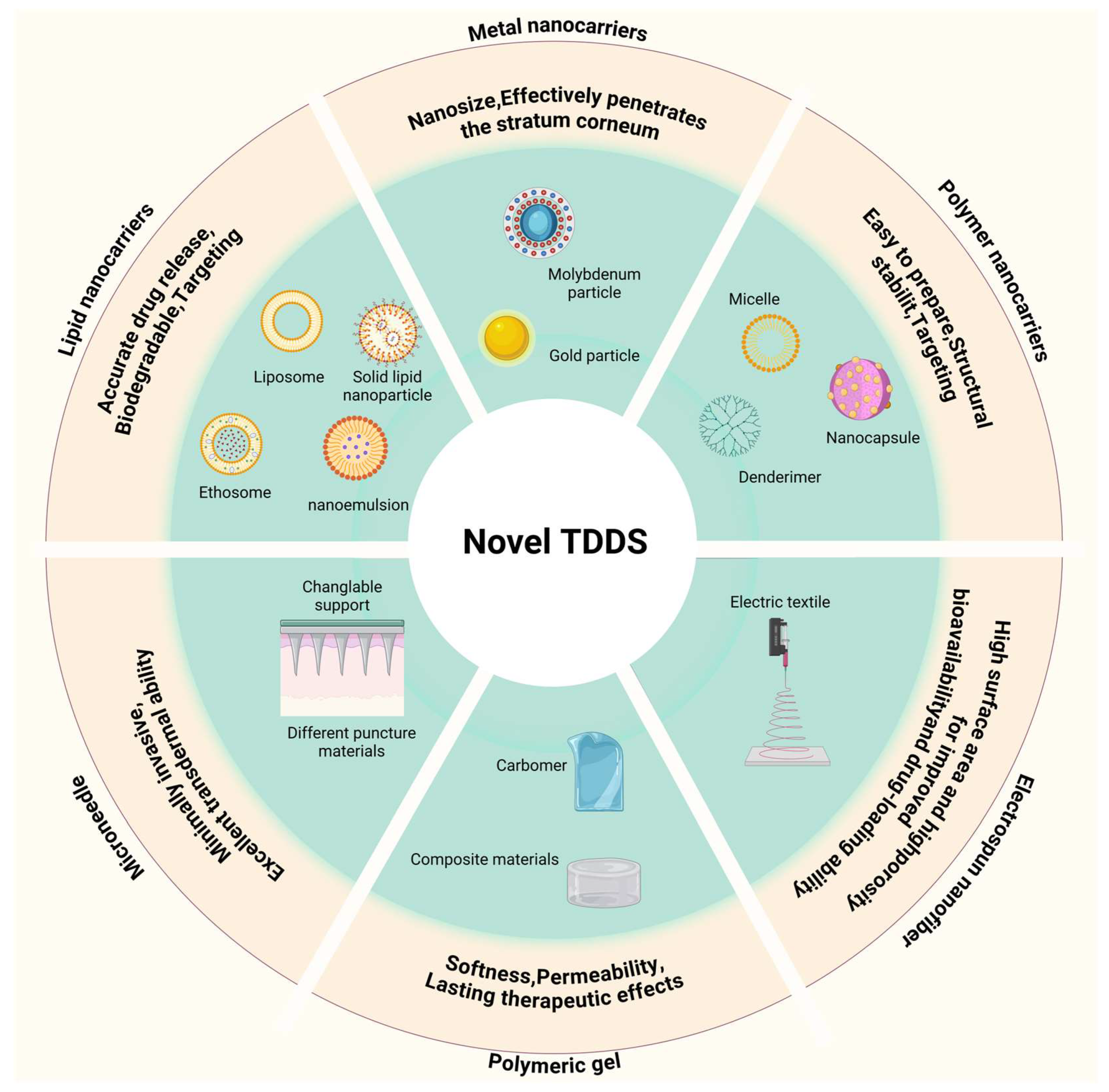
5.1. Nanotechnology-Based Transdermal Delivery for Psoriasis Treatment
5.1.1. Metal Nanocarriers for Psoriasis Treatment
5.1.2. Polymer Nanocarriers for Psoriasis Treatment
5.1.3. Lipid Nanocarriers for Psoriasis Treatment
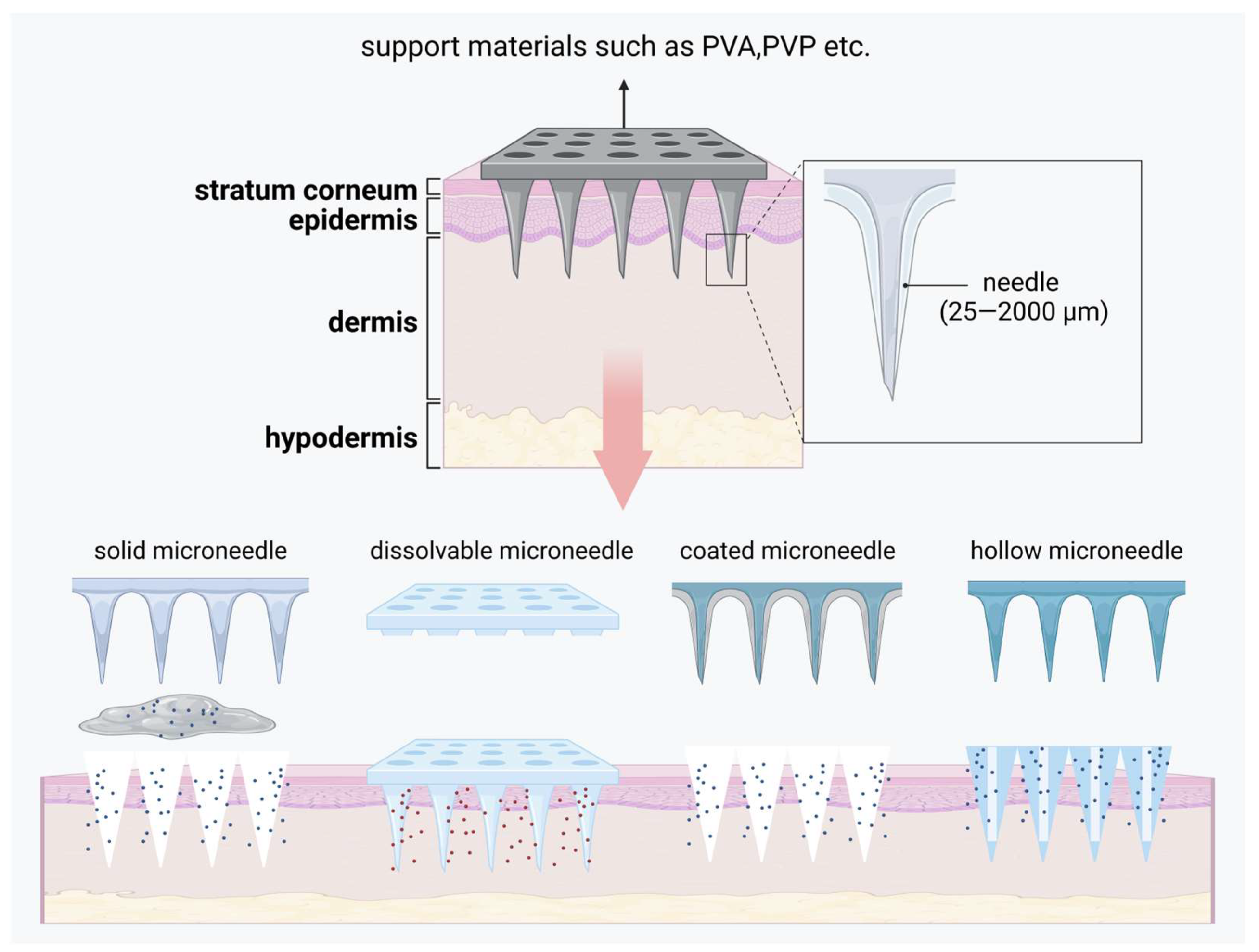
5.2. Microneedle-Based Transdermal Delivery for Psoriasis Treatment
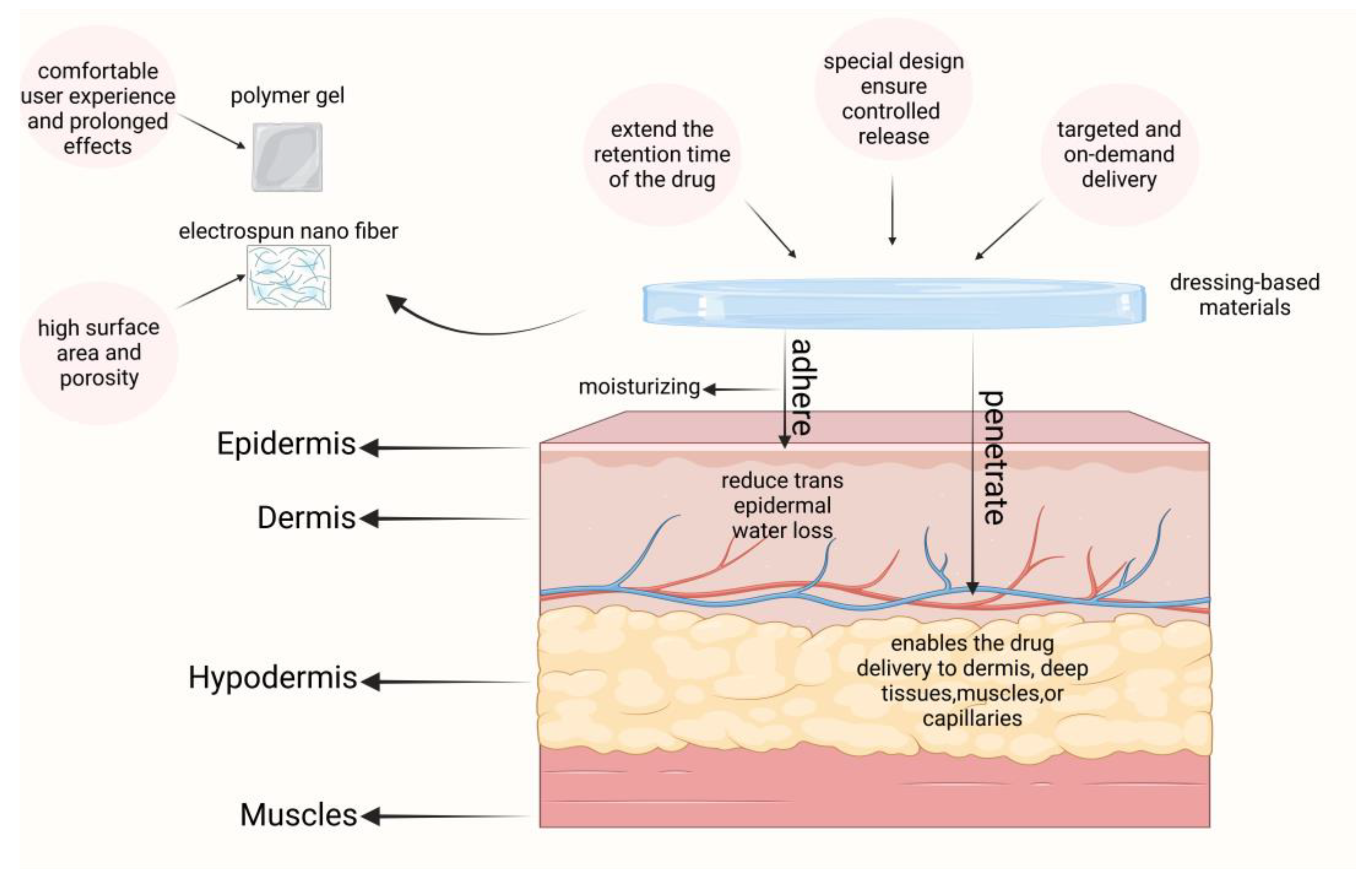
5.3. Dressing-Based Transdermal Delivery for Psoriasis Treatment
5.3.1. Polymeric Gels for Psoriasis Treatment
5.3.2. Electrospun Nanofiber Materials
6. Recent Patents and Clinical Trials
7. Future Perspectives and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brezinski, E.A.; Dhillon, J.S.; Armstrong, A.W. Economic burden of psoriasis in the United States: A systematic review. JAMA Dermatol. 2015, 151, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Zhao, Y.; Cao, X. Global burden and future trends in psoriasis epidemiology: Insights from the global burden of disease study 2019 and predictions to 2030. Arch. Dermatol. Res. 2024, 316, 114. [Google Scholar] [CrossRef] [PubMed]
- Parisi, R.; Iskandar, I.Y.; Kontopantelis, E.; Augustin, M.; Griffiths, C.E.; Ashcroft, D.M. National, regional, and worldwide epidemiology of psoriasis: Systematic analysis and modelling study. BMJ 2020, 369, m1590. [Google Scholar] [CrossRef] [PubMed]
- AlQassimi, S.; AlBrashdi, S.; Galadari, H.; Hashim, M.J. Global burden of psoriasis–comparison of regional and global epidemiology, 1990 to 2017. Int. J. Dermatol. 2020, 59, 566–571. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.W.; Bohannan, B.; Mburu, S.; Coates, L.C.; Ogdie, A.; Alarcon, I.; Kasparek, T.; Frade, S.; Barrio, S.F.; Augustin, M. Patient Perspectives on Psoriatic Disease Burden: Results from the Global Psoriasis and Beyond Survey. Dermatology 2023, 239, 621–634. [Google Scholar] [CrossRef] [PubMed]
- Mahmutović, E.; Dolićanin, Z.; Todorović, S.T.; Milićević, S.; Doder, R.; Bošković, K. Psoriasis and Psoriatic Arthritis. Arch. Phys. Med. Rehabil. 2018, 99, e211. [Google Scholar] [CrossRef]
- Nowowiejska, J.; Baran, A.; Grabowska, P.; Lewoc, M.; Kaminski, T.W.; Flisiak, I. Assessment of life quality, stress and physical activity among patients with psoriasis. Dermatol. Ther. 2022, 12, 395–406. [Google Scholar] [CrossRef]
- Segaert, S.; Calzavara-Pinton, P.; de la Cueva, P.; Jalili, A.; Lons Danic, D.; Pink, A.E.; Thaçi, D.; Gooderham, M. Long-term topical management of psoriasis: The road ahead. J. Dermatol. Treat. 2022, 33, 111–120. [Google Scholar] [CrossRef]
- Reich, K.; Sorbe, C.; Griese, L.; Reich, J.; Augustin, M. The value of subcutaneous vs. oral methotrexate: Real-world data from the German psoriasis registry PsoBest. Br. J. Dermatol. 2021, 184, 765–767. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Sharma, G.; Singh, B.; Dhiman, V.; Bhadada, S.K.; Katare, O. Holistic development of coal tar lotion by embedding design of experiments (DoE) technique: Preclinical investigations. Expert Opin. Drug Deliv. 2020, 17, 255–273. [Google Scholar] [CrossRef] [PubMed]
- Green, L.; Sadoff, W. A clinical evaluation of tazarotene 0.1% gel, with and without a high-or mid-high-potency corticosteroid, in patients with stable plaque psoriasis. J. Cutan. Med. Surg. 2002, 6, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.; Luo, Y.; Xu, J.; Guan, X.; He, H.; Xuan, X.; Wu, J. Latest on biomaterial-based therapies for topical treatment of psoriasis. J. Mater. Chem. B 2022, 10, 7397–7417. [Google Scholar] [CrossRef] [PubMed]
- Yao, Q.; Zhai, Y.; He, Z.; Wang, Q.; Sun, L.; Sun, T.; Lv, L.; Li, Y.; Yang, J.; Lv, D. Water-responsive gel extends drug retention and facilitates skin penetration for curcumin topical delivery against psoriasis. Asian J. Pharm. Sci. 2023, 18, 100782. [Google Scholar] [CrossRef] [PubMed]
- Van de Kerkhof, P.; Hoefnagels, W.; Van Haelst, U.; Mali, J. Methotrexate maintenance therapy and liver damage in psoriasis. Clin. Exp. Dermatol. 1985, 10, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Corden, E.; Higgins, E.; Smith, C. Hypercalcaemia-induced kidney injury caused by the vitamin D analogue calcitriol for psoriasis: A note of caution when prescribing topical treatment. Clin. Exp. Dermatol. 2016, 41, 899–901. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Naisbitt, D.J.; Sun, Y.; Zhang, F. Pathomechanism of Adverse Reactions to Biological Treatment of Inflammatory Skin Conditions. Clin. Exp. Allergy 2024. [Google Scholar] [CrossRef] [PubMed]
- Morita, A.; Choon, S.E.; Bachelez, H.; Anadkat, M.J.; Marrakchi, S.; Zheng, M.; Tsai, T.-F.; Turki, H.; Hua, H.; Rajeswari, S. Design of Effisayil™ 2: A randomized, double-blind, placebo-controlled study of spesolimab in preventing flares in patients with generalized pustular psoriasis. Dermatol. Ther. 2023, 13, 347–359. [Google Scholar] [CrossRef]
- Hoy, S.M. Deucravacitinib: First approval. Drugs 2022, 82, 1671–1679. [Google Scholar] [CrossRef]
- Singh, V.; Bansal, K.; Bhati, H.; Bajpai, M. New insights into pharmaceutical nanocrystals for the improved topical delivery of therapeutics in various skin disorders. Curr. Pharm. Biotechnol. 2024, 25, 1182–1198. [Google Scholar] [CrossRef] [PubMed]
- Safta, D.A.; Bogdan, C.; Moldovan, M.-L. SLNs and NLCs for Skin Applications: Enhancing the Bioavailability of Natural Bioactives. Pharmaceutics 2024, 16, 1270. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.H.; Rho, J.G.; Yang, Y.; Lee, S.; Kweon, S.; Kim, H.-M.; Yoon, J.; Choi, H.; Lee, E.; Kim, S.H. Hyaluronic acid nanoparticles as a topical agent for treating psoriasis. ACS Nano 2022, 16, 20057–20074. [Google Scholar] [CrossRef]
- Sun, H.; Zhao, Y.; Zhang, P.; Zhai, S.; Li, W.; Cui, J. Transcutaneous delivery of mung bean-derived nanoparticles for amelioration of psoriasis-like skin inflammation. Nanoscale 2022, 14, 3040–3048. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, C.E.; Armstrong, A.W.; Gudjonsson, J.E.; Barker, J.N. Psoriasis. Lancet 2021, 397, 1301–1315. [Google Scholar] [CrossRef]
- Bartholomew, E.; Chung, B.-Y.; Davis, M.; Yeroushalmi, S.; Chung, M.; Hakimi, M.; Bhutani, T.; Liao, W. Rapid Remission of Sunburn-Induced Guttate Psoriasis with Guselkumab. Dermatol. Ther. 2023, 13, 2473–2478. [Google Scholar] [CrossRef]
- Gaspari, V.; Orioni, G.; Peron, I.; Misciali, C.; Bardazzi, F. A case of guttate psoriasis after primary herpetic gingivostomatitis. Int. J. STD AIDS 2024, 35, 739–741. [Google Scholar] [CrossRef] [PubMed]
- Bachelez, H. Pustular psoriasis: The dawn of a new era. Acta Derm.-Venereol. 2020, 100, 5651. [Google Scholar] [CrossRef] [PubMed]
- Prajapati, V.H.; Lynde, C.W.; Gooderham, M.J.; Hong, H.C.h.; Kirchhof, M.G.; Lansang, P.; Ringuet, J.; Turchin, I.; Vender, R.; Yeung, J. Considerations for defining and diagnosing generalized pustular psoriasis. J. Eur. Acad. Dermatol. Venereol. 2024. Epub ahead of print. [Google Scholar] [CrossRef]
- Gisondi, P.; Bellinato, F.; Girolomoni, G. Clinical characteristics of patients with pustular psoriasis: A single-center retrospective observational study. Vaccines 2022, 10, 1171. [Google Scholar] [CrossRef] [PubMed]
- Han, G.-M.; Yang, W.-S.; Yang, B. Inhibition of progression of acrodermatitis continua of Hallopeau with Baricitinib. JAMA Dermatol. 2021, 157, 466–468. [Google Scholar] [CrossRef]
- Trovato, E.; Orsini, C.; Russo, F.; Cortonesi, G.; Rubegni, P. Ixekizumab as treatment of erythrodermic psoriasis. Dermatol. Ther. 2021, 34, e14868. [Google Scholar] [CrossRef]
- Megna, M.; Ruggiero, A.; Salsano, A.; Lauletta, G.; Portarapillo, A.; Torta, G.; Martora, F.; Potestio, L. A case of erythrodermic psoriasis successfully treated with risankizumab. Clin. Cosmet. Investig. Dermatol. 2023, 16, 3503–3507. [Google Scholar] [CrossRef] [PubMed]
- Umezawa, Y. Psoriatic arthritis. J. Dermatol. 2021, 48, 741–749. [Google Scholar] [CrossRef]
- Uribe-Herranz, M.; Lian, L.-H.; Hooper, K.M.; Milora, K.A.; Jensen, L.E. IL-1R1 signaling facilitates Munro’s microabscess formation in psoriasiform imiquimod-induced skin inflammation. J. Investig. Dermatol. 2013, 133, 1541–1549. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-H.; Park, Y.J.; Kim, S.K.; Kwon, J.E.; Kang, H.Y.; Lee, E.-S.; Choi, J.H.; Kim, Y.C. Histopathological differential diagnosis of psoriasis and seborrheic dermatitis of the scalp. Ann. Dermatol. 2016, 28, 427–432. [Google Scholar] [CrossRef]
- Li, J.; Hou, H.; Zhou, L.; Wang, J.; Liang, J.; Li, J.; Hou, R.; Niu, X.; Yin, G.; Li, X. Increased angiogenesis and migration of dermal microvascular endothelial cells from patients with psoriasis. Exp. Dermatol. 2021, 30, 973–981. [Google Scholar] [CrossRef]
- Mateu-Arrom, L.; Puig, L. Genetic and Epigenetic Mechanisms of Psoriasis. Genes 2023, 14, 1619. [Google Scholar] [CrossRef]
- Capon, F. The genetic basis of psoriasis. Int. J. Mol. Sci. 2017, 18, 2526. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Ito, T.; Gilhar, A.; Tokura, Y.; Reich, K.; Paus, R. The hair follicle-psoriasis axis: Shared regulatory mechanisms and therapeutic targets. Exp. Dermatol. 2022, 31, 266–279. [Google Scholar] [CrossRef]
- Gazel, U.; Ayan, G.; Solmaz, D.; Akar, S.; Aydin, S.Z. The impact of smoking on prevalence of psoriasis and psoriatic arthritis. Rheumatology 2020, 59, 2695–2710. [Google Scholar] [CrossRef] [PubMed]
- Tseng, J.-C.; Chang, Y.-C.; Huang, C.-M.; Hsu, L.-C.; Chuang, T.-H. Therapeutic development based on the immunopathogenic mechanisms of psoriasis. Pharmaceutics 2021, 13, 1064. [Google Scholar] [CrossRef]
- Kamata, M.; Tada, Y. Dendritic cells and macrophages in the pathogenesis of psoriasis. Front. Immunol. 2022, 13, 941071. [Google Scholar] [CrossRef]
- Potestio, L.; Martora, F.; Lauletta, G.; Vallone, Y.; Battista, T.; Megna, M. The Role of Interleukin 23/17 Axis in Psoriasis Management: A Comprehensive Review of Clinical Trials. Clin. Cosmet. Investig. Dermatol. 2024, 829–842. [Google Scholar] [CrossRef]
- Sondermann, W.; Körber, A. IL-17-Blockade in der Psoriasis-Therapie. Kompass Dermatol. 2018, 6, 69–78. [Google Scholar] [CrossRef]
- Shi, Z.; Wu, X.; Wu, C.-Y.; Singh, S.P.; Law, T.; Yamada, D.; Huynh, M.; Liakos, W.; Yang, G.; Farber, J.M. Bile acids improve psoriasiform dermatitis through inhibition of IL-17A expression and CCL20-CCR6–mediated trafficking of T cells. J. Investig. Dermatol. 2022, 142, 1381–1390. e1311. [Google Scholar] [CrossRef]
- Hedrick, M.N.; Lonsdorf, A.S.; Shirakawa, A.-K.; Lee, C.-C.R.; Liao, F.; Singh, S.P.; Zhang, H.H.; Grinberg, A.; Love, P.E.; Hwang, S.T. CCR6 is required for IL-23–induced psoriasis-like inflammation in mice. J. Clin. Investig. 2009, 119, 2317–2329. [Google Scholar] [CrossRef]
- Howes, A.; O’Sullivan, P.A.; Breyer, F.; Ghose, A.; Cao, L.; Krappmann, D.; Bowcock, A.M.; Ley, S.C. Psoriasis mutations disrupt CARD14 autoinhibition promoting BCL10-MALT1-dependent NF-κB activation. Biochem. J. 2016, 473, 1759–1768. [Google Scholar] [CrossRef] [PubMed]
- Furtunescu, A.R.; Georgescu, S.R.; Tampa, M.; Matei, C. Inhibition of the JAK-STAT Pathway in the Treatment of Psoriasis: A Review of the Literature. Int. J. Mol. Sci. 2024, 25, 4681. [Google Scholar] [CrossRef] [PubMed]
- Fathi, N.; Rashidi, G.; Khodadadi, A.; Shahi, S.; Sharifi, S. STAT3 and apoptosis challenges in cancer. Int. J. Biol. Macromol. 2018, 117, 993–1001. [Google Scholar] [CrossRef]
- Xie, X.; Zhang, L.; Lin, Y.; Liu, X.; Wang, N.; Li, P. IL-17A exacerbates psoriasis in a STAT3 overexpressing mouse model. PeerJ 2023, 11, e15727. [Google Scholar] [CrossRef]
- Abduelmula, A.; Gooderham, M.J. TYK2 inhibition: Changing the treatment landscape for psoriasis? Expert Rev. Clin. Immunol. 2022, 18, 185–187. [Google Scholar] [CrossRef]
- Locke, G.A.; Muckelbauer, J.; Tokarski, J.S.; Barbieri, C.M.; Belić, S.; Falk, B.; Tredup, J.; Wang, Y.-K. Identification and characterization of TYK2 pseudokinase domain stabilizers that allosterically inhibit TYK2 signaling. In Methods in Enzymology; Academic Press: Cambridge, MA, USA, 2022; Volume 667, pp. 685–727. [Google Scholar]
- Ren, Y.; Dong, H.; Jin, R.; Jiang, J.; Zhang, X. TRIM22 actives PI3K/Akt/mTOR pathway to promote psoriasis through enhancing cell proliferation and inflammation and inhibiting autophagy. Cutan. Ocul. Toxicol. 2022, 41, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Aldabbas, R.; Shaker, O.G.; Ismail, M.F.; Fathy, N. miRNA-559 and MTDH as possible diagnostic markers of psoriasis: Role of PTEN/AKT/FOXO pathway in disease pathogenesis. Mol. Cell. Biochem. 2023, 478, 1427–1438. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Liu, X.; Huang, M.; Wang, R.; Zhu, W.; Li, Y.; Shen, L.; Li, C. Metformin inhibits haCaT cell proliferation under hyperlipidemia through reducing reactive oxygen species via FOXO3 activation. Clin. Cosmet. Investig. Dermatol. 2022, 1403–1413. [Google Scholar] [CrossRef] [PubMed]
- Brandon, A.; Mufti, A.; Sibbald, R.G. Diagnosis and management of cutaneous psoriasis: A review. Adv. Ski. Wound Care 2019, 32, 58–69. [Google Scholar] [CrossRef] [PubMed]
- Morariu, S.-H.; Cotoi, O.S.; Tiucă, O.M.; Baican, A.; Gheucă-Solovăstru, L.; Decean, H.; Brihan, I.; Silaghi, K.; Biro, V.; Șerban-Pescar, D. Blood-Count-Derived Inflammatory Markers as Predictors of Response to Biologics and Small-Molecule Inhibitors in Psoriasis: A Multicenter Study. J. Clin. Med. 2024, 13, 3992. [Google Scholar] [CrossRef] [PubMed]
- Kayaçetin, S.; Öcalan, D.T.; Gül, Ü. Comparison of Histopathological Findings in Psoriasis According to the Lesion Location From Biopsy. Am. J. Dermatopathol. 2024, 46, 353–357. [Google Scholar] [CrossRef] [PubMed]
- Makhecha, M.; Singh, T.; Khatib, Y. Dermoscopy differentiates guttate psoriasis from a mimicker—Pityriasis rosea. Dermatol. Pract. Concept. 2021, 11, e2021138. [Google Scholar] [CrossRef]
- Sobolev, V.V.; Denisova, E.V.; Korsunskaia, I.M.; Lavrov, A.A.; Krivoshchapov, L.G. A new approach to combined therapy of psoriasis. Russ. J. Clin. Dermatol. Venereol. 2015, 14, 82–86. [Google Scholar] [CrossRef]
- Lacouture, M.E.; Goleva, E.; Shah, N.; Rotemberg, V.; Kraehenbuehl, L.; Ketosugbo, K.F.; Merghoub, T.; Maier, T.; Bang, A.; Gu, S. Immunologic Profiling of Immune-Related Cutaneous Adverse Events with Checkpoint Inhibitors Reveals Polarized Actionable Pathways. Clin. Cancer Res. 2024, OF1–OF13. [Google Scholar] [CrossRef]
- Mizukawa, I.; Kamata, M.; Yamamoto, A.; Tada, Y. Prevalence of subclinical axial involvement in patients diagnosed with peripheral psoriatic arthritis on X-rays: A single-centre retrospective study. Exp. Dermatol. 2023, 32, 2180–2182. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, T.; Umezawa, Y.; Tojo, S.; Yonenaga, T.; Asahina, A.; Nakagawa, H.; Fukuda, K. OP0126 Dual Energy CT with Iodine Map Is Promising New Imaging Modality in The Evaluation of Hand Psoriatic Arthritis; BMJ Publishing Group Ltd.: London, UK, 2016. [Google Scholar]
- Coates, L.C.; Hodgson, R.; Conaghan, P.G.; Freeston, J.E. MRI and ultrasonography for diagnosis and monitoring of psoriatic arthritis. Best Pract. Res. Clin. Rheumatol. 2012, 26, 805–822. [Google Scholar] [CrossRef] [PubMed]
- Yiu, Z.Z.; Warren, R.B. Raising standards for the evaluation of future psoriasis therapeutics: A critical checklist. Clin. Pharmacol. Ther. 2017, 102, 642–648. [Google Scholar] [CrossRef]
- Wu, A.G.; Conway, J.; Barazani, L.; Roy, B.; Cline, A.; Pereira, F. Is clear always clear? Comparison of Psoriasis Area and Severity Index (PASI) and the Physician’s Global Assessment (PGA) in psoriasis clearance. Dermatol. Ther. 2020, 10, 1155–1163. [Google Scholar] [CrossRef]
- Dar, A.; Fehaid, A.; Alkhatani, S.; Alarifi, S.; Alqahtani, W.; Albasher, G.; Almeer, R.; Alfarraj, S.; Moneim, A.A. The protective role of luteolin against the methotrexate-induced hepato-renal toxicity via its antioxidative, anti-inflammatory, and anti-apoptotic effects in rats. Hum. Exp. Toxicol. 2021, 40, 1194–1207. [Google Scholar] [CrossRef]
- Sandhu, V.K.; Eder, L.; Yeung, J. Apremilast and its role in psoriatic arthritis. G. Ital. Di Dermatol. E Venereol. Organo Uff. Soc. Ital. Di Dermatol. E Sifilogr. 2020, 155, 386–399. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K.; Goldfarb, M.T.; Ellis, C.N.; Voorhees, J.J. Side-effect profile of acitretin therapy in psoriasis. J. Am. Acad. Dermatol. 1989, 20, 1088–1093. [Google Scholar] [CrossRef] [PubMed]
- Zkib, J.; Sattout, R.; Faour, S.; Haddad, S.; Bassut, R.; Swed, W.; Hritani, S.; Mansouer, M.; Ghabally, M. Corticosteroid-induced bradycardia following high-dose methylprednisolone administration: A case report. Ann. Med. Surg. 2024, 86, 6300–6302. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, K.; Kono, T.; Ishii, M.; Taniguchi, S.; Saito, S. Lupus Erythematosus Panniculitis in a Patient with Autoimmune Hepatitis. Acta Derm.-Venereol. 2000, 80, 373. [Google Scholar] [CrossRef]
- Chen, Y.; Xu, D.; Xia, X.; Chen, G.; Xiao, H.; Chen, L.; Wang, H. Sex difference in adrenal developmental toxicity induced by dexamethasone and its intrauterine programming mechanism. Pharmacol. Res. 2021, 174, 105942. [Google Scholar] [CrossRef] [PubMed]
- Xi, C.; Runtian, Z.; Xingwu, D.; Ming, X.; Tiange, Q.; Lingling, L. Effectiveness of Xiaoyin Jiedu granules in the treatment of psoriasis vulgaris in patients with blood-heat symptom patterns in terms of Traditional Chinese Medicine. J. Tradit. Chin. Med. 2020, 40, 863. [Google Scholar]
- González-Moure, C.; Figueroa-Silva, O.; Álvarez-García, O.; Gil-Pallares, P.; Peña-López, S.; Usero-Bárcena, T.; Campo-Cerecedo, F.; Vázquez-Rodríguez, T.R.; Monteagudo-Sánchez, B. Injection site reaction with subcutaneous methotrexate. Dermatol. Ther. 2022, 35, 1. [Google Scholar] [CrossRef] [PubMed]
- Bulte, C.A.; Hoegler, K.M.; Kutlu, Ö.; Khachemoune, A. Hydroxyurea: A reappraisal of its cutaneous side effects and their management. Int. J. Dermatol. 2021, 60, 810–817. [Google Scholar] [CrossRef]
- Arun Kumar, A.; Elsayed, M.E.; Alghali, A.; Ali, A.A.; Mohamed, H.; Hussein, W.; Hackett, C.; Leonard, N.; Stack, A.G. Sweet syndrome: A rare feature of ANCA-associated vasculitis or unusual consequence of azathioprine-induced treatment. Allergy Asthma Clin. Immunol. 2018, 14, 46. [Google Scholar] [CrossRef] [PubMed]
- Huntoon, M.A. Etanercept: An epidural steroid alternative for minimally invasive treatment of radiculitis. J. Am. Soc. Anesthesiol. 2009, 110, 967–969. [Google Scholar] [CrossRef]
- Verea, M.M.; Pozo, J.D.; Yebra-Pimentel, M.T.; Porta, A.; Fonseca, E. Psoriasiform eruption induced by infliximab. Ann. Pharmacother. 2004, 38, 54–57. [Google Scholar] [CrossRef]
- Mohammed, R.H.A.; Essam, M.; Anwar, I.; Shehab, H.; Komy, M.E. Psoriasis paradox—Infliximab-induced psoriasis in a patient with Crohn’s disease: A case report and mini-review. J. Int. Med. Res. 2023, 51, 1–7. [Google Scholar] [CrossRef]
- Scheinfeld, N. Adalimumab: A review of side effects. Expert Opin. Drug Saf. 2005, 4, 637–641. [Google Scholar] [CrossRef]
- Deeks, E.D. Certolizumab pegol: A review in inflammatory autoimmune diseases. BioDrugs 2016, 30, 607–617. [Google Scholar] [CrossRef] [PubMed]
- Tada, Y.; Sugiura, Y.; Kamishima, M.; Tanaka, Y.; Tsuchiya, H.; Masuda, J.; Yamanaka, K. Safety and effectiveness of guselkumab in Japanese patients with psoriasis: 20-week interim analysis of a postmarketing surveillance study. J. Dermatol. 2024, 51, 779–790. [Google Scholar] [CrossRef]
- Lin, J.; Chen, X.; Luo, M.; Zhuo, Q.; Zhang, H.; Chen, N.; Zhuo, Y.; Han, Y. Safety of tildrakizumab: A disproportionality analysis based on the FDA adverse event reporting system (FAERS) database from 2018–2023. Front. Pharmacol. 2024, 15, 1420478. [Google Scholar] [CrossRef] [PubMed]
- Shu, Y.; Chen, J.; Ding, Y.; Zhang, Q. Adverse events with risankizumab in the real world: Postmarketing pharmacovigilance assessment of the FDA adverse event reporting system. Front. Immunol. 2023, 14, 1169735. [Google Scholar] [CrossRef] [PubMed]
- Peigottu, M.; Montesu, M. Adverse skin reaction to Secukinumab. J. Eur. Acad. Dermatol. Venereol. 2017, 31, e432. [Google Scholar] [CrossRef] [PubMed]
- Deodhar, A.; van der Heijde, D.; Gensler, L.S.; Kim, T.-H.; Maksymowych, W.P.; Østergaard, M.; Poddubnyy, D.; Marzo-Ortega, H.; Bessette, L.; Tomita, T. Ixekizumab for patients with non-radiographic axial spondyloarthritis (COAST-X): A randomised, placebo-controlled trial. Lancet 2020, 395, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Lebwohl, M.G.; Papp, K.A.; Marangell, L.B.; Koo, J.; Blauvelt, A.; Gooderham, M.; Wu, J.J.; Rastogi, S.; Harris, S.; Pillai, R. Psychiatric adverse events during treatment with brodalumab: Analysis of psoriasis clinical trials. J. Am. Acad. Dermatol. 2018, 78, 81–89.e85. [Google Scholar] [CrossRef] [PubMed]
- Galluzzo, M.; D’adamio, S.; Bianchi, L.; Talamonti, M. Brodalumab for the treatment of psoriasis. Expert Rev. Clin. Immunol. 2016, 12, 1255–1271. [Google Scholar] [CrossRef] [PubMed]
- Pathak, G.N.; Wang, E.; Dhillon, J.; Parikh, P.N.; Esseghir, R.; Rao, B.K.; Feldman, S.R. Spesolimab: A Review of the First IL-36 Blocker Approved for Generalized Pustular Psoriasis. Ann. Pharmacother. 2024. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- López-Ferrer, A.; Laiz, A.; Puig, L. The safety of ustekinumab for the treatment of psoriatic arthritis. Expert Opin. Drug Saf. 2017, 16, 733–742. [Google Scholar] [CrossRef] [PubMed]
- Nie, T.; Shirley, M. Bimekizumab: A Review in Psoriatic Arthritis. Drugs 2024, 84, 587–598. [Google Scholar] [CrossRef]
- Ren, J.; Zhu, Q.; Wang, S.; Li, X.; Sun, Z.; Li, N.; Feng, J.; Ding, H.; Dong, S.; Wang, H. Clinical efficacy and safety of using calcipotriol–betamethasone compounding agent for psoriasis treatment: A systematic review and meta-analysis. Arch. Dermatol. Res. 2022, 314, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Moustafa, G.A.; Xanthopoulou, E.; Riza, E.; Linos, A. Skin disease after occupational dermal exposure to coal tar: A review of the scientific literature. Int. J. Dermatol. 2015, 54, 868–879. [Google Scholar] [CrossRef]
- Spencer, C.M.; Wiseman, L.R. Topical fluticasone propionate: A review of its pharmacological properties and therapeutic use in the treatment of dermatological disorders. BioDrugs 1997, 7, 318–334. [Google Scholar] [CrossRef]
- Kelly, J.W.; Cains, G.D.; Rallings, M.; Gilmore, S.J. Safety and efficacy of mometasone furoate cream in the treatment of steroid responsive dermatoses. Australas. J. Dermatol. 1991, 32, 85–91. [Google Scholar] [CrossRef]
- Zimath, P.L.; Almeida, M.S.; Bruxel, M.A.; Rafacho, A. Oral mometasone furoate administration preserves anti-inflammatory action with fewer metabolic adverse effects in rats. Biochem. Pharmacol. 2023, 210, 115486. [Google Scholar] [CrossRef] [PubMed]
- Lebwohl, M.; Freeman, A.K.; Chapman, M.S.; Feldman, S.R.; Hartle, J.E.; Henning, A. Tacrolimus ointment is effective for facial and intertriginous psoriasis. J. Am. Acad. Dermatol. 2004, 51, 723–730. [Google Scholar] [CrossRef]
- Arab, H.H.; Abd El-Aal, S.A.; Eid, A.H.; Arafa, E.-S.A.; Mahmoud, A.M.; Ashour, A.M. Targeting inflammation, autophagy, and apoptosis by troxerutin attenuates methotrexate-induced renal injury in rats. Int. Immunopharmacol. 2022, 103, 108284. [Google Scholar] [CrossRef]
- Pandey, S.; Tripathi, P.; Gupta, A.; Yadav, J.S. A comprehensive review on possibilities of treating psoriasis using dermal cyclosporine. Drug Deliv. Transl. Res. 2022, 12, 1541–1555. [Google Scholar] [CrossRef] [PubMed]
- Katz, H.I.; Waalen, J.; Leach, E.E. Acitretin in psoriasis: An overview of adverse effects. J. Am. Acad. Dermatol. 1999, 41, S7–S12. [Google Scholar] [CrossRef]
- Hengge, U.R.; Ruzicka, T.; Schwartz, R.A.; Cork, M.J. Adverse effects of topical glucocorticosteroids. J. Am. Acad. Dermatol. 2006, 54, 1–15. [Google Scholar] [CrossRef]
- Zhang, W. Learning History to Develop Traditional Chinese Medicine. Planta Medica 2010, 76, S35. [Google Scholar] [CrossRef]
- Wang, Z.; Zhang, G.; Zhang, H.; Li, L. Xiaoyin Jiedu Granules may alleviate psoriasis-like skin diseases in mice by regulating sphingosine 1-phosphate receptor expression and reducing Th17 cells. Heliyon 2023, 9, e19109. [Google Scholar] [CrossRef] [PubMed]
- Hazari, S.A.; Kaur, H.; Karwasra, R.; Abourehab, M.A.; Khan, A.A.; Kesharwani, P. An overview of topical lipid-based and polymer-based nanocarriers for treatment of psoriasis. Int. J. Pharm. 2023, 638, 122938. [Google Scholar] [CrossRef] [PubMed]
- Turner, K.B.; Alves, N.J.; Medintz, I.L.; Walper, S.A. Improving the targeting of therapeutics with single-domain antibodies. Expert Opin. Drug Deliv. 2016, 13, 561–570. [Google Scholar] [CrossRef] [PubMed]
- Megna, M.; Ocampo-Garza, S.S.; Potestio, L.; Fontanella, G.; Gallo, L.; Cacciapuoti, S.; Ruggiero, A.; Fabbrocini, G. New-onset psoriatic arthritis under biologics in psoriasis patients: An increasing challenge? Biomedicines 2021, 9, 1482. [Google Scholar] [CrossRef] [PubMed]
- Pasadyn, S.R.; Knabel, D.; Fernandez, A.P.; Warren, C.B. Cutaneous adverse effects of biologic medications. Clevel. Clin. J. Med. 2020, 87, 288–299. [Google Scholar] [CrossRef]
- Pender, E.K.; Kirby, B. An update on topical therapies for psoriasis. Curr. Opin. Rheumatol. 2024, 36, 289–294. [Google Scholar] [CrossRef]
- Zhang, M.; Hong, S.; Sun, X.; Zhou, Y.; Luo, Y.; Liu, L.; Wang, J.; Wang, C.; Lin, N.; Li, X. Exploration of and insights into advanced topical nanocarrier systems for the treatment of psoriasis. Front. Med. 2022, 9, 1017126. [Google Scholar] [CrossRef]
- Singh, T.; Arora, A.; Sahu, K.K.; Patel, P.; Kaur, S.; Thakur, S.; Gupta, G.D.; Singh, D.; Kurmi, B.D. A complete sojourn of recent advancements and applications in transdermal drug delivery systems. J. Drug Deliv. Sci. Technol. 2024, 106328. [Google Scholar] [CrossRef]
- Kang, Y.; Zhang, S.; Wang, G.; Yan, Z.; Wu, G.; Tang, L.; Wang, W. Nanocarrier-Based Transdermal Drug Delivery Systems for Dermatological Therapy. Pharmaceutics 2024, 16, 1384. [Google Scholar] [CrossRef] [PubMed]
- Melo-Guímaro, S.; Cardoso, R.; Lobo, C.S.; Pereira, D.A.; Varela, C.; Santos, J.; João, C.P.; Serpa, C.; Arnaut, L.G. Delivery of minoxidil encapsulated in cyclodextrins with photoacoustic waves enhances hair growth. Eur. J. Pharm. Biopharm. 2024, 202, 114390. [Google Scholar] [CrossRef] [PubMed]
- Men, Z.; Su, T.; Tang, Z.; Liang, J.; Shen, T. Tacrolimus nanocrystals microneedle patch for plaque psoriasis. Int. J. Pharm. 2022, 627, 122207. [Google Scholar] [CrossRef]
- Blauvelt, A. In This Issue--Full Court Press on Psoriasis. J. Investig. Dermatol. 2004, 123, vii–viii. [Google Scholar] [CrossRef]
- Ahmad, M.Z.; Mohammed, A.A.; Algahtani, M.S.; Mishra, A.; Ahmad, J. Nanoscale topical pharmacotherapy in management of psoriasis: Contemporary Research and scope. J. Funct. Biomater. 2022, 14, 19. [Google Scholar] [CrossRef]
- Feng, S.; Yang, L.; Wen, D.; Zheng, Z.; Luo, Z.; Zheng, B.; Lei, S.; Cai, Y.; Liao, W.; Zeng, K. A transdermal delivery system using microneedle patches containing poly (lactic-co-glycolic)-encapsulated acitretin nanoparticles for topical and extended treatment. Int. Biodeterior. Biodegrad. 2024, 195, 105906. [Google Scholar] [CrossRef]
- Nirmal, G.; Liao, C.-C.; Lin, Z.-C.; Alshetaili, A.; Hwang, E.; Yang, S.-C.; Fang, J.-Y. Topically applied pH-responsive nanogels for alkyl radical-based therapy against psoriasiform hyperplasia. Drug Deliv. 2023, 30, 2245169. [Google Scholar] [CrossRef]
- Ramanunny, A.K.; Wadhwa, S.; Thakur, D.; Singh, S.K.; Kumar, R. Treatment modalities of psoriasis: A focus on requisite for topical nanocarrier. Endocr. Metab. Immune Disord.-Drug Targets (Former. Curr. Drug Targets-Immune Endocr. Metab. Disord.) 2021, 21, 418–433. [Google Scholar] [CrossRef]
- Fratoddi, I.; Benassi, L.; Botti, E.; Vaschieri, C.; Venditti, I.; Bessar, H.; Samir, M.A.; Azzoni, P.; Magnoni, C.; Costanzo, A. Effects of topical methotrexate loaded gold nanoparticle in cutaneous inflammatory mouse model. Nanomed. Nanotechnol. Biol. Med. 2019, 17, 276–286. [Google Scholar] [CrossRef]
- Nemati, H.; Ghahramani, M.-H.; Faridi-Majidi, R.; Izadi, B.; Bahrami, G.; Madani, S.-H.; Tavoosidana, G. Using siRNA-based spherical nucleic acid nanoparticle conjugates for gene regulation in psoriasis. J. Control. Release 2017, 268, 259–268. [Google Scholar] [CrossRef]
- Yao, L.; Tian, F.; Meng, Q.; Guo, L.; Ma, Z.; Hu, T.; Liang, Q.; Li, Z. Reactive oxygen species-responsive supramolecular deucravacitinib self-assembly polymer micelles alleviate psoriatic skin inflammation by reducing mitochondrial oxidative stress. Front. Immunol. 2024, 15, 1407782. [Google Scholar] [CrossRef] [PubMed]
- Su, J.; Lin, N.; You, X.; Dai, H.; Rao, M.; Ye, L.; Ye, F.; Cai, L.; Chen, Y.; Zhou, G. Phenylboronic acid-functionalized gelatin–oleic acid nanoparticles for high loading and efficient transdermal delivery of Celastrol towards the treatment of psoriasis. Macromol. Res. 2023, 31, 1029–1042. [Google Scholar] [CrossRef]
- Hua, Y.; Chang, T.; Jiang, K.; Wang, J.; Cui, X.; Cheng, M.; Yan, F.; Song, B.; Wang, Y. ROS-sensitive calcipotriol nano-micelles prepared by methoxypolyethylene glycol (mPEG)–modified polymer for the treatment of psoriasis. Drug Deliv. 2022, 29, 1903–1913. [Google Scholar] [CrossRef] [PubMed]
- Fereig, S.A.; El-Zaafarany, G.M.; Arafa, M.G.; Abdel-Mottaleb, M.M. Tacrolimus-loaded chitosan nanoparticles for enhanced skin deposition and management of plaque psoriasis. Carbohydr. Polym. 2021, 268, 118238. [Google Scholar] [CrossRef] [PubMed]
- Fereig, S.A.; El-Zaafarany, G.M.; Arafa, M.G.; Abdel-Mottaleb, M.M. Self-assembled tacrolimus-loaded lecithin-chitosan hybrid nanoparticles for in vivo management of psoriasis. Int. J. Pharm. 2021, 608, 121114. [Google Scholar] [CrossRef]
- Sheikh, A.; Hazari, S.A.; Molugulu, N.; Alshehri, S.A.; Wahab, S.; Sahebkar, A.; Kesharwani, P. Hyaluronic acid engineered gallic acid embedded chitosan nanoparticle as an effective delivery system for treatment of psoriasis. Environ. Res. 2023, 238, 117086. [Google Scholar] [CrossRef]
- Supasena, W.; Muangnoi, C.; Thaweesest, W.; Songkram, C.; Ueda, K.; Higashi, K.; Moribe, K.; Tanasupawat, S.; Rojsitthisak, P. Enhanced antipsoriatic activity of mycophenolic acid against the TNF-α-induced HaCaT cell proliferation by conjugated poloxamer micelles. J. Pharm. Sci. 2020, 109, 1153–1160. [Google Scholar] [CrossRef] [PubMed]
- Khurana, B.; Arora, D.; Narang, R.K. QbD based exploration of resveratrol loaded polymeric micelles based carbomer gel for topical treatment of plaque psoriasis: In vitro, ex vivo and in vivo studies. J. Drug Deliv. Sci. Technol. 2020, 59, 101901. [Google Scholar] [CrossRef]
- Yan, Y.; Liang, H.; Liu, X.; Liu, L.; Chen, Y. Topical cationic hairy particles targeting cell free DNA in dermis enhance treatment of psoriasis. Biomaterials 2021, 276, 121027. [Google Scholar] [CrossRef]
- Ramanunny, A.K.; Wadhwa, S.; Singh, S.K.; Kumar, B.; Gulati, M.; Kumar, A.; Almawash, S.; Al Saqr, A.; Gowthamarajan, K.; Dua, K. Topical non-aqueous nanoemulsion of Alpinia galanga extract for effective treatment in psoriasis: In vitro and in vivo evaluation. Int. J. Pharm. 2022, 624, 121882. [Google Scholar] [CrossRef] [PubMed]
- Algahtani, M.S.; Ahmad, M.Z.; Ahmad, J. Nanoemulsion loaded polymeric hydrogel for topical delivery of curcumin in psoriasis. J. Drug Deliv. Sci. Technol. 2020, 59, 101847. [Google Scholar] [CrossRef]
- Yu, F.; Zhang, Y.; Yang, C.; Li, F.; Qiu, B.; Ding, W. Enhanced transdermal efficiency of curcumin-loaded peptide-modified liposomes for highly effective antipsoriatic therapy. J. Mater. Chem. B 2021, 9, 4846–4856. [Google Scholar] [CrossRef]
- Xi, L.; Lin, Z.; Qiu, F.; Chen, S.; Li, P.; Chen, X.; Wang, Z.; Zheng, Y. Enhanced uptake and anti-maturation effect of celastrol-loaded mannosylated liposomes on dendritic cells for psoriasis treatment. Acta Pharm. Sin. B 2022, 12, 339–352. [Google Scholar] [CrossRef] [PubMed]
- Sohail, S.; Arshad, S.; Khalid, S.; Dar, M.J.; Iqbal, K.; Sohail, H. Development and Evaluation of Methotrexate and Baicalin-Loaded Nanolipid Carriers for Psoriasis Treatment. Development 2024, 21, 327–339. [Google Scholar]
- Saka, R.; Jain, H.; Kommineni, N.; Chella, N.; Khan, W. Enhanced penetration and improved therapeutic efficacy of bexarotene via topical liposomal gel in imiquimod induced psoriatic plaque model in BALB/c mice. J. Drug Deliv. Sci. Technol. 2020, 58, 101691. [Google Scholar] [CrossRef]
- Elhabal, S.F.; Abdelaal, N.; Al-Zuhairy, S.A.; Mohamed Elrefai, M.F.; Khalifa, M.M.; Khasawneh, M.A.; Elsaid Hamdan, A.M.; Mohie, P.M.; Gad, R.A.; Kabil, S.L. Revolutionizing Psoriasis Topical Treatment: Enhanced Efficacy Through Ceramide/Phospholipid Composite Cerosomes Co-Delivery of Cyclosporine and Dithranol: In-Vitro, Ex-Vivo, and In-Vivo Studies. Int. J. Nanomed. 2024, 1163–1187. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.-T.; Shen, L.-N.; Wu, Z.-H.; Zhao, J.-H.; Feng, N.-P. Comparison of ethosomes and liposomes for skin delivery of psoralen for psoriasis therapy. Int. J. Pharm. 2014, 471, 449–452. [Google Scholar] [CrossRef]
- Guo, J.; Xiao, Q.; Lu, Y.; Gao, J.; Ning, P.; Jia, C.; Cai, Y.; Gong, C.; Yao, W.; Huang, M. Molybdenum Nanoparticles Ameliorate Psoriatic Lesions by Inhibiting the ROS/NF-κb Signaling Axis. ACS Appl. Nano Mater. 2024, 7, 12839–12847. [Google Scholar] [CrossRef]
- Han, R.; Ho, L.W.C.; Bai, Q.; Chan, C.K.W.; Lee, L.K.C.; Choi, P.C.-L.; Choi, C.H.J. Alkyl-terminated gold nanoparticles as a self-therapeutic treatment for psoriasis. Nano Lett. 2021, 21, 8723–8733. [Google Scholar] [CrossRef]
- Sontakke, A.; Dighe, S.; Sharma, R.; Yadav, V.; Jain, S. Harnessing the potential of fatty Acid-Surfactant-Based micellar gel for enhanced topical delivery of Apremilast in psoriasis treatment. Int. J. Pharm. 2024, 655, 124026. [Google Scholar] [CrossRef]
- Wang, H.; Su, D.; Huang, R.; Shu, F.; Cheng, F.; Zheng, G. Cellular nanovesicles with bioorthogonal targeting enhance photodynamic/photothermal therapy in psoriasis. Acta Biomater. 2021, 134, 674–685. [Google Scholar] [CrossRef]
- Yu, H.; Liu, Y.; Zheng, F.; Chen, W.; Wei, K. Erianin-loaded photo-responsive dendrimer mesoporous silica nanoparticles: Exploration of a psoriasis treatment method. Molecules 2022, 27, 6328. [Google Scholar] [CrossRef]
- Ashraf, M.; El-Sawy, H.S.; El Zaafarany, G.M.; Abdel-Mottaleb, M.M. Eucalyptus oil nanoemulsion for enhanced skin deposition of fluticasone propionate in psoriatic plaques: A combinatorial anti-inflammatory effect to suppress implicated cytokines. Arch. Der Pharm. 2024, e2400557. [Google Scholar] [CrossRef] [PubMed]
- Wan, T.; Pan, J.; Long, Y.; Yu, K.; Wang, Y.; Pan, W.; Ruan, W.; Qin, M.; Wu, C.; Xu, Y. Dual roles of TPGS based microemulsion for tacrolimus: Enhancing the percutaneous delivery and anti-psoriatic efficacy. Int. J. Pharm. 2017, 528, 511–523. [Google Scholar] [CrossRef] [PubMed]
- Doppalapudi, S.; Jain, A.; Chopra, D.K.; Khan, W. Psoralen loaded liposomal nanocarriers for improved skin penetration and efficacy of topical PUVA in psoriasis. Eur. J. Pharm. Sci. 2017, 96, 515–529. [Google Scholar] [CrossRef] [PubMed]
- Guo, T.; Lu, J.; Fan, Y.; Zhang, Y.; Yin, S.; Sha, X.; Feng, N. TPGS assists the percutaneous administration of curcumin and glycyrrhetinic acid coloaded functionalized ethosomes for the synergistic treatment of psoriasis. Int. J. Pharm. 2021, 604, 120762. [Google Scholar] [CrossRef]
- Ren, G.; Zhao, Y. Preparation methods and thermal stability of calcipotriol solid lipid nanoparticles and efficacy in plaque psoriasis treatment. J. Therm. Anal. Calorim. 2021, 144, 2091–2098. [Google Scholar] [CrossRef]
- Lim, D.-J.; Kim, H.-J. Microneedles in action: Microneedling and microneedles-assisted transdermal delivery. Polymers 2022, 14, 1608. [Google Scholar] [CrossRef]
- Luo, X.; Yang, L.; Cui, Y. Microneedles: Materials, fabrication, and biomedical applications. Biomed. Microdevices 2023, 25, 20. [Google Scholar] [CrossRef]
- Ali, R.; Mehta, P.; Arshad, M.; Kucuk, I.; Chang, M.; Ahmad, Z. Transdermal microneedles—A materials perspective. Aaps Pharmscitech 2020, 21, 12. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Guo, R.; Wang, S.; Yang, X.; Ling, G.; Zhang, P. Fabrication, evaluation and applications of dissolving microneedles. Int. J. Pharm. 2021, 604, 120749. [Google Scholar] [CrossRef] [PubMed]
- Dai, X.; Permana, A.D.; Li, M.; Habibie; Nur Amir, M.; Peng, K.; Zhang, C.; Dai, H.; Paredes, A.J.; Vora, L.K. Calcipotriol Nanosuspension-Loaded Trilayer Dissolving Microneedle Patches for the Treatment of Psoriasis: In Vitro Delivery and In Vivo Antipsoriatic Activity Studies. Mol. Pharm. 2024, 21, 2813–2827. [Google Scholar] [CrossRef] [PubMed]
- Bi, D.; Qu, F.; Xiao, W.; Wu, J.; Liu, P.; Du, H.; Xie, Y.; Liu, H.; Zhang, L.; Tao, J. Reactive oxygen species-responsive gel-based microneedle patches for prolonged and intelligent psoriasis management. ACS Nano 2023, 17, 4346–4357. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Hao, R.; Peng, B.; Chang, J.; Chen, S.; Chen, Y.; Yin, X.; Que, Y.; Fan, C.; Xu, Y. Dissolvable hyaluronic acid microneedles loaded with β-Elemene for the treatment of psoriasis. Front. Pharmacol. 2022, 13, 1067051. [Google Scholar] [CrossRef]
- Su, H.; Liu, Z.; Zhang, Z.; Jing, X.; Meng, L. Development of a Deep Eutectic Solvent-Assisted Kaempferol Hydrogel: A Promising Therapeutic Approach for Psoriasis-like Skin Inflammation. Mol. Pharm. 2023, 20, 6319–6329. [Google Scholar] [CrossRef] [PubMed]
- Telange, D.R.; Mahajan, N.M.; Mandale, T.; More, S.; Warokar, A. P ongamia pinnata seed extract-mediated green synthesis of silver nanoparticle loaded nanogel for estimation of their antipsoriatic properties. Bioprocess Biosyst. Eng. 2024, 47, 1409–1431. [Google Scholar] [CrossRef]
- Ghosal, K.; Augustine, R.; Zaszczynska, A.; Barman, M.; Jain, A.; Hasan, A.; Kalarikkal, N.; Sajkiewicz, P.; Thomas, S. Novel drug delivery systems based on triaxial electrospinning based nanofibers. React. Funct. Polym. 2021, 163, 104895. [Google Scholar] [CrossRef]
- Hemati Azandaryani, A.; Derakhshandeh, K.; Arkan, E. Electrospun nanobandage for hydrocortisone topical delivery as an antipsoriasis candidate. Int. J. Polym. Mater. Polym. Biomater. 2018, 67, 677–685. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnostic Methods | Inspection Items | Diagnostic Criteria | Precautions | Ref. |
|---|---|---|---|---|
| Blood Routine Test | White blood cell count, erythrocyte sedimentation rate, and platelet count in blood | Elevated white blood cell count, increased erythrocyte sedimentation rate, and elevated platelet count, among other things | Maintain an empty stomach to avoid compromising diagnostic results | [56] |
| Histopathology | Skin tissue samples for microscopic examination | Thickening of the stratum corneum, hyperkeratosis, hypertrophy of the stratum spinosum, and vasodilatation of the papillary layer of the dermis | Ensure representative sampling of skin tissue from lesions and take care to avoid topical medications from affecting results | [57] |
| Dermoscopy | Patient’s area of skin damage | Bright red background, regularly or circumferentially distributed punctate blood vessels, and diffusely distributed white scales | Dermoscopic test results should only be used as a reference, and pathologic biopsies are also performed when necessary to prevent misdiagnosis | [58] |
| Biochemical Test | Liver function, kidney function, and blood lipids | Abnormal liver function, hypertriglyceridemia, low HDL, etc. | Maintain a fasting state to avoid the influence of food on the test results | [59] |
| Immunological Test | Immunoglobulins, complement and cytokines, etc. | Elevated immunoglobulins, decreased complement, and abnormal cytokine levels | Maintain a fasting state to avoid the influence of food on the test results | [60] |
| Digital X-ray photography | Patients with symptoms such as joint pain or swelling | Evaluate joints for lesions such as narrowing of the joint space, osteoporosis, osteophytes, or other changes in joint structure | Some radiation to the human body, metal inserts in the body need to be notified | [61] |
| Computed Tomography (CT) | Patients with suspected or diagnosed arthropathic psoriasis | Signs of bone erosion, osteophytes, and narrowing of the joint space at the margins and center of the joints | Remove all metal objects from the body; inform the body of the presence of metal implants; pregnant women should minimize CT examinations to avoid affecting the development of the fetus | [62] |
| Magnetic Resonance Imaging (MRI) | Patients with suspected or diagnosed arthropathic psoriasis | Ancillary X-rays to assess the extent of inflammation, joint cavity effusion, synovial thickening, bone marrow edema, inflammation of tendons and ligaments, and bone destruction | MRI is poorly reported in the literature, and there is no consensus on the criteria for examining to evaluate activity and bone structure changes in psoriatic arthritis | [63] |
| Treatment | Types of Drugs | Used Drugs | Advantages | Disadvantages | Ref. |
|---|---|---|---|---|---|
| Oral medicines | Immunosuppressants | Methotrexate | Convenient, easy to store, relatively inexpensive | liver and kidney damage | [66] |
| Apremilast | Short-term gastrointestinal side effects | [67] | |||
| Vitamins derivatives | Acitretin | Elevated serum triglycerides and, to a lesser extent, elevated serum cholesterol and liver transaminase levels | [68] | ||
| Glucocorticosteroid | Methylprednisolone | Hyperglycemia, hypertension, osteoporosis, immunosuppression, weight gain, and bradycardia and cardiac arrhythmias | [69] | ||
| Prednisone | Possible skin atrophy | [70] | |||
| Dexamethasone | Adrenal function effects | [71] | |||
| TCM | Xiaoyin jiedu granules | Less researched, unknown side effects | [72] | ||
| Injectable medications | Immunosuppressant | Methotrexate | Effective, lower dosing frequency, more economical | Injection site edema, pimples, erythema, etc. | [73] |
| Hydroxyurea | Hyperpigmentation, dryness, and skin atrophy | [74] | |||
| Azathioprine | Pemphigus erythematosus rash and fever | [75] | |||
| Biological agents: TNF-α inhibitor | Etanercept | Outstanding therapeutic effect, good specificity | Allergic reactions, immunodeficiencies, sepsis, tuberculosis (reactivated or novel infections), and rare lymphoma risks | [76] | |
| Infliximab | Itching, erythema, rash, and other rare side effects such as induced psoriasis in Crohn’s patients | [77,78] | |||
| Adalimumab | Injection site reactions, rare side effects include congestive heart failure, lupus-like syndrome, lymphoma promotion, neurological disorders | [79] | |||
| Certolizumab Pegol | Upper respiratory tract infections, skin rashes, and urinary tract infections | [80] | |||
| Biological agents: IL-23 inhibitor | Guselkumab | Infections, nasopharyngitis, etc. | [81] | ||
| Tildrakizumab | Nasopharyngitis, headaches, upper respiratory infections, and worsening psoriasis | [82] | |||
| Biological agents: IL-23 inhibitor | Risankizumab | Pneumonia, cerebrovascular accidents, cataracts, loss of consciousness, heart disease, cirrhosis of the liver and thrombosis | [83] | ||
| Biological agents: IL-17A inhibitor | Secukinumab | Nasopharyngitis, diarrhea, upper respiratory infections, itching and headaches | [84] | ||
| Ixekizumab | Nasopharyngitis and injection site reactions | [85] | |||
| Brodalumab | Suicidal ideation and behavior, Nasopharyngitis, headaches, upper respiratory infections and joint pains | [86,87] | |||
| Biological agents: IL-36 receptor inhibitor | Spesolimab | Drug reactions such as eosinophilia and systemic symptoms (DRESS), cholelithiasis, and breast cancer | [88] | ||
| Biological agents: IL-12/23 inhibitor | Ustekinumab | Inhalation tract infections, nasopharyngitis, headache and injection site reactions, and a small number of serious infections or cardiovascular adverse events | [89] | ||
| Biological agents: IL-17A/F inhibitor | Bimekizumab | Nasopharyngitis, upper respiratory tract infections, oral candidiasis, headaches and diarrhea | [90] | ||
| Topical medicines | Vitamin derivatives | Calcipotriol | Lower side effects than systemic administration, protects the skin barrier, less expensive | Possible transient hypercalcemia, prolonged use of calcipotriol may cause local skin reactions, which may lead to non-compliance; approximately 20% of patients do not respond to calcipotriol treatment | [91] |
| Tar preparations | Coal tar detergent | Allergic dermatitis, folliculitis, occupational acne, epidermal atrophy and hyperpigmentation | [92] | ||
| Glucocorticosteroid | Fluticasone propionate, Mometasone furoate | Itching, burning, dryness, stinging, folliculitis, irritation or worsening of skin conditions Possible diabetes, skin atrophy | [93,94,95] | ||
| Calcineurin inhibitors | Tacrolimus | Poor penetration appears to be relatively ineffective in the treatment of plaque psoriasis | [96] |
| Delivery Carrier | Materials | Drug | Size and Zeta Potential | Mechanism and Efficacy | Ref. |
|---|---|---|---|---|---|
| Metal nanocarriers | Gold nanoparticles functionalized with 3-mercapto-1-propansulfonate | Methotrexate | 5 nm, −32 ± 1 mV | Reduction of induced keratinocyte hyperproliferation, epidermal thickness, and inflammatory infiltrate in a psoriasis-like mouse model | [118] |
| Spherical nucleic acid nanoparticle conjugates | - | 12.38 ± 1.59 nm, −28 mV | Stable and non-toxic. Significantly reduces gene expression in cells, and in vivo experiments show that S significantly inhibits cell proliferation | [119] | |
| Polymer nanocarriers | Diblock copolymer of polyethylene glycol and polypropylene sulfide | Deucravacitinib | 105 nm | Longer retention time in the dermis inhibits the STAT3 signaling cascade, with corresponding reductions in the levels of the differentiation and proliferation markers Keratin 17 and Cyclin D1, respectively | [120] |
| Polymer nanocarrier | Gelatin-oleic acid coupling modified with 4-(3-boronophenylamino)-4-oxobutanoic acid | Celastrol | 200–300 nm, −6.00 ± 0.10 mV | Improved cellular and skin penetration and enhanced antipsoriasis activity in a mouse model | [121] |
| Methoxypolyethyleneglycol-thioether-thiols | Calcipotriol | 283 ± 13.1 nm, −14.9 mV | ROS sensitivity, good biocompatibility, safe routes of administration, short treatment cycles, etc. | [122] | |
| Solvent-free ion-gelation of chitosan | Tacrolimus | 140.8 ± 50.0 nm, 17–33 mV | Successful, repeatable, and simple. It eliminates the use of any harmful organic solvents and is superior to Talmos® Ointment in its efficacy in the treatment of plaque psoriasis | [123] | |
| Lecithin–chitosan hybrid | Tacrolimus | 160.9 ± 15.9 nm/118.7 ± 13.3 nm, 11–42 mV | Successfully doped with hydrophobic drugs; the addition of suitable co-solvents maximized the drug-carrying capacity of the above hybrid particles for hydrophobic drugs, and the efficiency of the treatment of psoriasis was superior to that of commercially available tacrolimus ointment | [124] | |
| Hyaluronic acid-modified chitosan | Gallic acid | 220.1 ± 0.18 nm, −2.104 ± 0.34 mV | Reduces epidermal hyperproliferation and associated inflammation and exhibits negligible systemic toxicity | [125] | |
| Kolliphor® 407 Coupling | Mycophenolic acid | Around 20 nm | Higher critical micelle concentration. Improved antiproliferative effect on TNF alpha-induced HaCaT cell proliferation | [126] | |
| Polymer nanocarrier | Polaxomer F127 and P123 designed by the Quality by Design (QbD) methodology. | Resveratrol | 142.67 ± 6.98 nm, −35.65 mV | Better skin penetration and enhanced resveratrol deposition in deeper skin layers enhanced the expected therapeutic effect of topical treatment of plaque-like psoriasis-like skin disease | [127] |
| Poly(2-(dimethylamino)ethyl methacrylate) (PDMA) grafted hairy silica particles (cSPs) with tunable PDMA length and particle size | - | 700 nm, +53.1 mV | enhance drug accumulation and prolong retention time in psoriatic lesions, leading to excellent treatment results. Ability to target cell free DNA | [128] | |
| Capryol 90/MCT oil, glycerin, Absolute ethanol | Alpinia galanga extract | 60.81 ± 18.88 nm, −7.99 ± 4.14 mV | Useful for restoring radiant skin texture and effectively treating psoriasis in a mouse model | [129] | |
| Propylene glycol dicaprylocaprate, Diethylene glycol monoethyl ether, Polyoxyethylene sorbitan monolaurate | Curcumin | 10.57 nm, −18.7 mV | It is possible to improve the topical efficacy of poorly penetrating Curcumin for the long-term management of psoriasis | [130] | |
| Lipid nanocarriers | Peptide TD-coupled liposomes | Curcumin | Around 100 nm | Increased transdermal efficiency of curcumin | [131] |
| Mannosylated liposomes | Celastrol | 85.5 ± 0.7 nm, −6.0 ± 0.3 mV | Enhancement of DC uptake and induction of DC tolerance | [132] | |
| Transfersomes | Methotrexate and Baicalin | 150.20 ± 3.57 nm, +38.6 mV | Better permeability | [133] | |
| DOTAP liposome | Bexarotene | 67.8.2 ± 7.15 nm, 46.4 ± 2.8 mV | Increased drug penetration and effective reversal of psoriasis | [134] | |
| Ceramide/Phospholipid Composite Cerosomes | Cyclosporine and Dithranol | 222.36 ± 0.36 nm, 29.36 ± 0.38 mV | Increased skin permeability and anti-proliferation | [135] | |
| Lipoid S 100, ethanol, and Phosphatidylcholine | Psoralen | 120.77 ± 22.43 nm | Good biocompatibility, low cytotoxicity | [136] |
| Type | Drug Name | Controlled Substance | Research Target | Clinical Trials Status | Country or Region | Item No. |
|---|---|---|---|---|---|---|
| Topical therapies | SGX302 (topical hypericin ointment and gel) | placebo | Patients with Mild to Moderate Psoriasis | Phase 2 Study Evaluating | USA | NCT05442190 |
| Sericin extract and turmeric extract cream | Triamcinolone acetonide 1% Cream | Patients over 18 years of age with psoriasis | / | Thailand | NCT06482398 | |
| Tapinarof cream | / | Plaque Psoriasis in Pediatric Subjects | Phase 3 | USA, Canada | NCT05172726 | |
| Chitosan Nanocrystalline Qinteng Huoxue Runji Ointment | placebo | Psoriasis with Blood Stasis Syndrome | / | China | NCT06396013 | |
| ZL-1102 Topical gel | Chronic Plaque Psoriasis | Phase 2 | Australia | NCT06380907 | ||
| Oral medicines | GM-XANTHO | placebo | Mild to Moderate Psoriasis | Phase IIa clinical trial | / | NCT06620692 |
| TAK-279 | / | Generalized Pustular Psoriasis or Erythrodermic Psoriasis | Phase 3 | Japan | NCT06323356 | |
| Piclidenoson | Placebo | Moderate-to-Severe Plaque Psoriasis | Phase 3 | / | NCT06643260 | |
| Shuiniujiao Dihuang Decoction | Placebo | Mild to moderate plaque Psoriasis | Hong Kong | NCT05815797 | ||
| LY4100511 | Placebo | Moderate-to-severe plaque Psoriasis | Phase 2 | USA | NCT06602219 | |
| Jiuweihuaban Pill | Placebo | Moderate to Severe Plaque Psoriasis (Syndrome of Blood-heat) | Phase II | China | NCT06058546 | |
| Oral medicines | ESK-001 | Apremilast, placebo | Moderate to Severe Plaque Psoriasis | / | USA, Canada | NCT06586112 |
| Injectable medications | Enoxaparin | / | Plaque Psoriasis | / | / | NCT06416566 |
| Tildrakizumab (biological agent) | / | Psoriasis in specific areas such as scalp, nails, genital area, and palmoplantar localization | / | France | NCT05938361 | |
| HB0017 (biological agent) | placebo | Moderate to Severe Plaque Psoriasis in adults | phase III clinical study | China | NCT06477237 | |
| CMAB015 (biological agent) | Secukinumab | Moderate to Severe Plaque Psoriasis in adults | / | China | NCT06398652 | |
| Tildrakizumab (biological agent) | / | Genital Psoriasis | / | Austria | NCT06029257 | |
| Netakimab (biological agent) | Placebo, Adalimumab | Children with Moderate to Severe Plaque Psoriasis | / | Russia | NCT06640517 | |
| Botulinum Toxin-A | / | Psoriasis Vulgaris | / | / | NCT06203470 |
| Type | Drug | Use | Country or Region | No. |
|---|---|---|---|---|
| / | New peptide from the alpha1 adrenergic receptor | Peptides (I) from the alpha 1-adrenergic receptor (AR), or their mutants or variants, form an epitope that can bind to autoantibodies (AAb) present in patients with psoriasis | German | DE10041560A1 |
| / | CDK4/6 inhibitor | Inhibitor for the suppression of the cellular IκBζ expression | German | EP3797776A1; US2022280511A1; WO2021063734A1 |
| Oral medicines | Dimethyl fumarate | Psoriasis treatment | Spanish | WO2020053218A1 |
| Topical therapies | FLUVOXAMINE | Psoriasis treatment | Portugal | EP4469032A1; PT117765A; WO2023146426A1 |
| / | SIALIC ACID | Psoriasis treatment | Norway | CN114450026A; EP4003365A1; US2022288095A1; WO2021019295A1 |
| / | CGRP receptor antagonists and/or pharmaceutical compositions | Methods are useful for treating, ameliorating, alleviating, providing for prophylaxis or prevention of, halting the progression of, and/or reducing the risk of psoriasis in a mammalian subject, such as a human | Ireland | AR126954A1; WO2023034466A1 |
| Injectable medications | IL-17 antagonists (biological agent) | Modifying the psoriasis disease course in particular patients having chronic plaque-type psoriasis and inhibiting the progression to PsA in these patients, as well as medicaments, dosing regimens, pharmaceutical formulations, dosage forms, and kits for use in the disclosed uses and methods. | Switzerland | WO2018158741A1 |
| / | Oligonucleotide complementary to the sequence of human miR-203b-3p microRNA | Psoriasis-induced itching | Italy | EP4437105A1 |
| Topical therapies | Composition comprising calcipotriol and betamethasone as active ingredients, petrolatum, and a propellant | Use in maintenance treatment of patients with psoriasis who are in remission. | Denmark | EP4041186A1 |
| Oral medicines | Small molecule inhibitors of tumor necrosis factor-alpha | Psoriasis treatment | France | WO2024223740A1 |
| Topical therapies | Medicament formed of a hydrogel and coal tar and/or coal tar extract is held | The dressings may be adapted for use in conjunction with phototherapy from UV light sources | USA | US10058711B2 |
| / | Comprising PPAR agonists and Nrf2 activators and methods of using combinations of PPAR agonists and Nrf2 activators | Psoriasis treatment | Australia | AU2021201390B2 |
| Topical therapies | An active agent comprising at least one steroid in the form of topical sprays that are propellant-free, and/or substantially non-foaming, and/or alcohol-free | Psoriasis treatment | USA | US20210386758A1 |
| / | Anti-interleukin antibodies | Psoriasis treatment | Japan | JP7558326B2 |
| / | Anti-IL-12 antibody | Production of antibodies or portions for treating and/or diagnosing IL-12-related conditions, diseases, and disorders | USA | US9409984B2 |
| Topical therapies | Psoriasis nanoemulsion tincture | Ppina gleditsiae and radix platycodonis nanoemulsion tincture; radix et rhizoma cynanchi paniculati and cortex dictamni meridian freeing, blood activating, heat-clearing, dampness drying, parasite removing, wind dispelling, and itching arresting relieving nanoemulsion tincture | China | CN106668689A |
| Topical therapies | Tripterine analog pristimerin-loaded exosome composite nanohydrogels for targeted therapy | The hydrogel delivers the drug to the psoriasis site in a targeted manner through PD-1/PD-L1 specificity to play a role in psoriasis, thus realizing targeted treatment of psoriasis, improving the microenvironment of the disease, lowering the toxicity and side effects of the drug, and improving the therapeutic effect | China | CN116059158A |
| Topical therapies | Long-acting gel preparation containing arsenic trioxide nano-liposome | After transdermal administration, arsenic trioxide can slowly penetrate and accumulate in the diseased area at a stable concentration. The long-acting gel preparation prepared by the present invention promotes efficient transdermal absorption of the drug, increases the retention of arsenic trioxide in the skin, improves the local concentration of the drug, and enhances the therapeutic effect on psoriasis | China | CN116270425A |
| Topical therapies | TCM micro-nano fiber film | Topical Chinese medicine micro-nano-fiber film for psoriasis treatment has the advantages of low cost, convenience, direct action on the affected area, fast onset of action, short course of treatment, not easy to recur, no toxic side effects and so on | China | CN114960028A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, Y.; Xu, T.; Wang, Y.; Hu, Y.; Yin, S.; Qin, Z.; Yu, H. Pathophysiology and Treatment of Psoriasis: From Clinical Practice to Basic Research. Pharmaceutics 2025, 17, 56. https://doi.org/10.3390/pharmaceutics17010056
Gao Y, Xu T, Wang Y, Hu Y, Yin S, Qin Z, Yu H. Pathophysiology and Treatment of Psoriasis: From Clinical Practice to Basic Research. Pharmaceutics. 2025; 17(1):56. https://doi.org/10.3390/pharmaceutics17010056
Chicago/Turabian StyleGao, Yujie, Tianqi Xu, Yu Wang, Yanjinhui Hu, Shaoping Yin, Zhiguo Qin, and Hua Yu. 2025. "Pathophysiology and Treatment of Psoriasis: From Clinical Practice to Basic Research" Pharmaceutics 17, no. 1: 56. https://doi.org/10.3390/pharmaceutics17010056
APA StyleGao, Y., Xu, T., Wang, Y., Hu, Y., Yin, S., Qin, Z., & Yu, H. (2025). Pathophysiology and Treatment of Psoriasis: From Clinical Practice to Basic Research. Pharmaceutics, 17(1), 56. https://doi.org/10.3390/pharmaceutics17010056