
Prevalence and Genetic Characterisation of Human Sapovirus from Children with Diarrhoea in the Rural Areas of Vhembe District, South Africa, 2017–2020


Abstract
1. Introduction
2. Results
2.1. Study Population
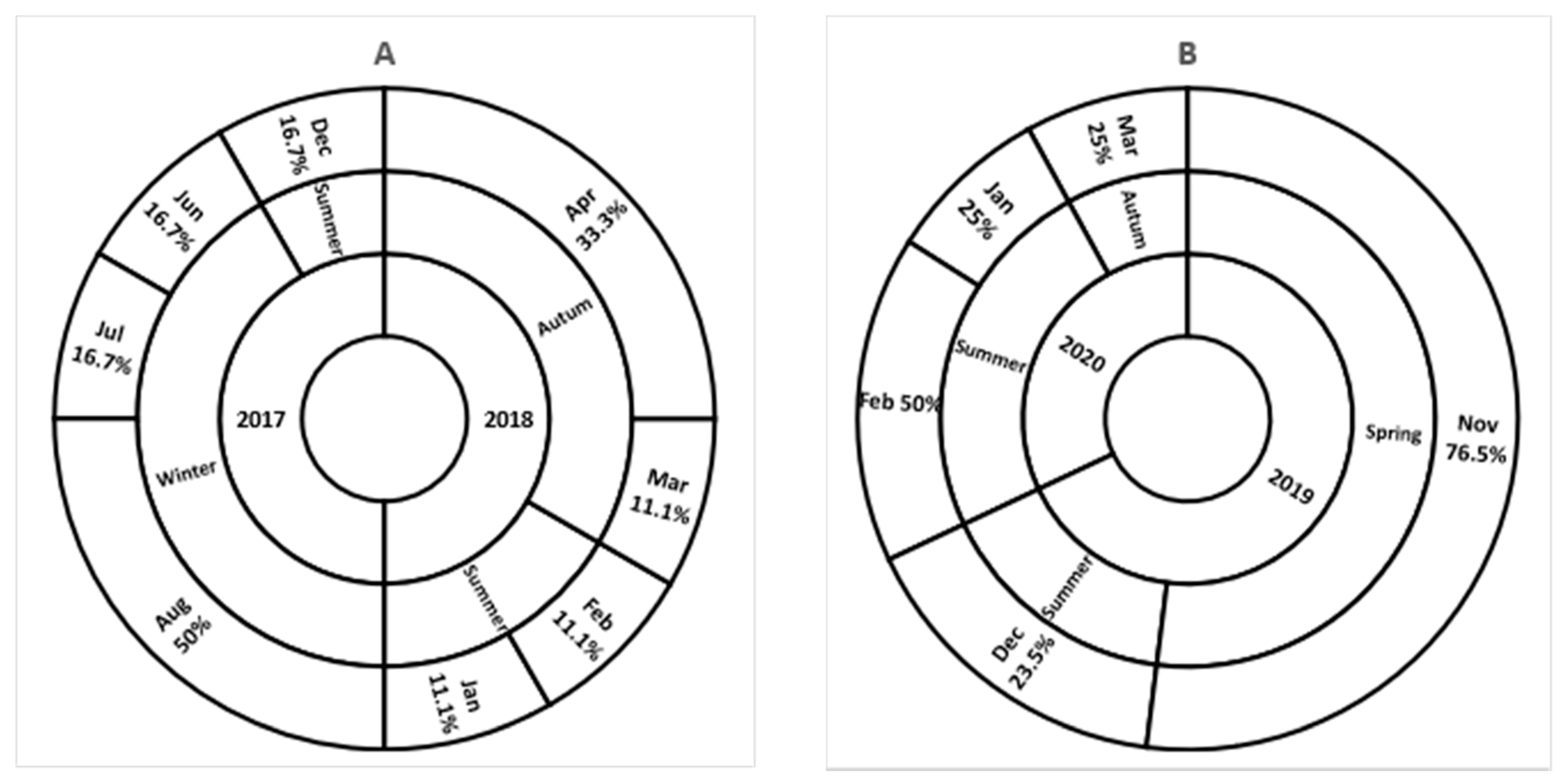
2.2. Sapovirus Detection
2.3. Clinical Manifestation
2.4. Household Setting and SV Distribution
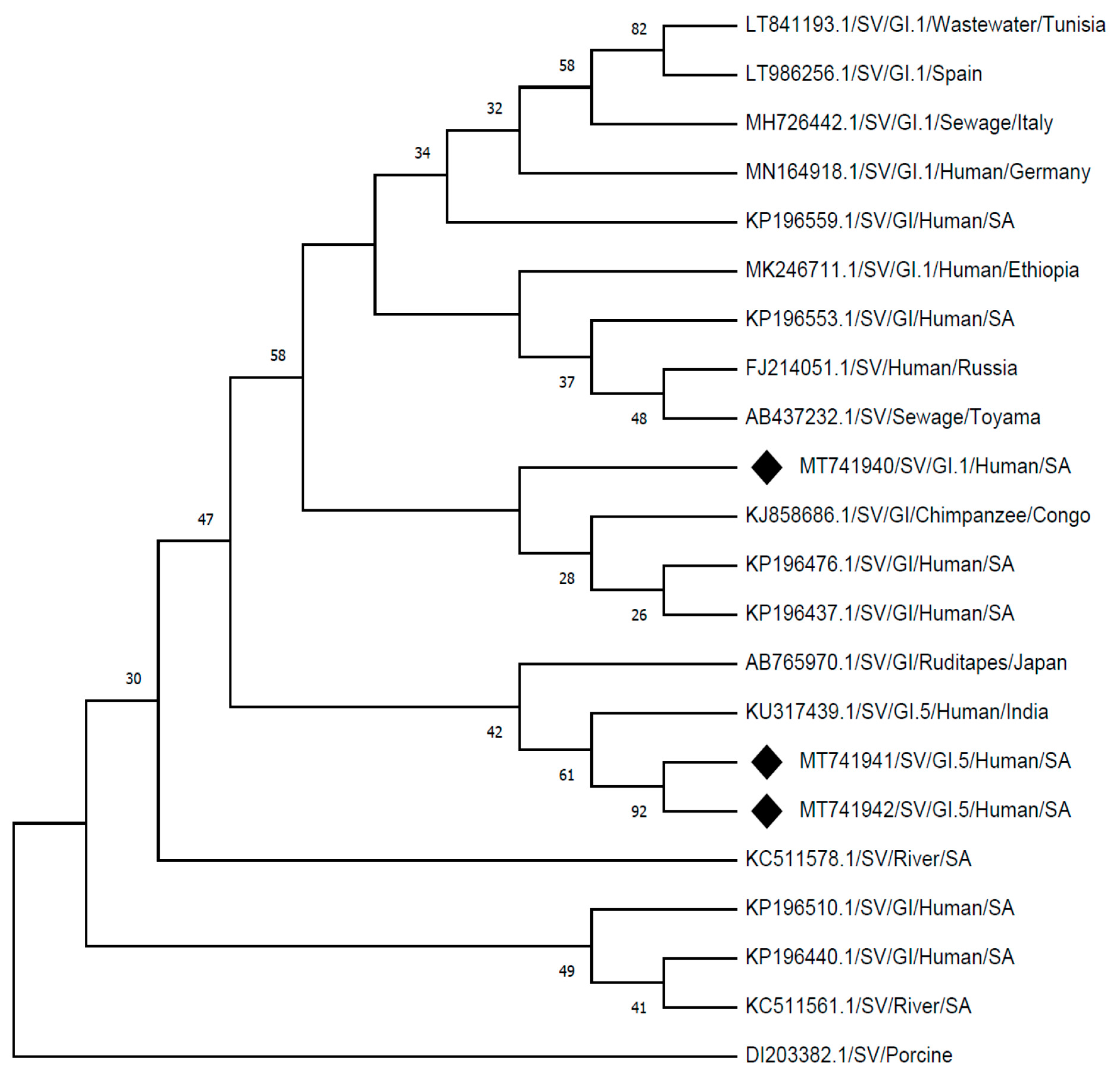
2.5. Molecular Characterization
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Sample Collection
4.3. Quality Control
4.4. Molecular Detection and Genogrouping of Sapovirus
4.4.1. Nucleic Acid Extraction
4.4.2. mPCR Detection of Sapoviruses from Stools
4.4.3. Sapovirus Genogrouping and Sequencing
4.5. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kapwata, T.; Mathee, A.; Le Roux, W.J.; Wright, C.Y. Diarrhoeal Disease in Relation to Possible Household Risk Factors in South African Villages. Int. J. Environ. Res. Public Health 2018, 15, 1665. [Google Scholar] [CrossRef]
- Awotiwon, O.F.; Wyk, V.P.; Dhansay, A.; Day, C.; Bradshaw, D. Diarrhoea in children under five years of age in South Africa (1997–2014). Trop. Med. Int. Health 2016, 21, 1060–1070. [Google Scholar] [CrossRef]
- Magwalivha, M.; Kabue, J.-P.; Traore, A.N.; Potgieter, N. Prevalence of Human Sapovirus in Low and Middle Income Countries. Adv. Virol. 2018, 2018, 1–12. [Google Scholar] [CrossRef]
- GBD Diarrhoeal Diseases Collaborators. Estimates of global, regional, and national morbidity, mortality, and aetiologies of diarrhoeal diseases: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Infect. Dis. 2015, 17, 909–948. [Google Scholar]
- Willey, J.M.; Sherwood, L.M.; Woolverton, C.J. Human Diseases Caused by Viruses and Prions, Prescott’s Microbiology, 8th ed.; McGraw-Hill: New York, NY, USA, 2011; pp. 922–923. [Google Scholar]
- Oka, T.; Wang, Q.; Katayama, K.; Saif, L.J. Comprehensive Review of Human Sapoviruses. Clin. Microbiol. Rev. 2015, 28, 32–53. [Google Scholar] [CrossRef]
- Yan, Y.; Li, Y.; Shi, W.; Kong, X.; Li, H.; Zhang, Q.; Pang, L.; Jiang, L.; Liu, J.; Jin, M.; et al. An outbreak of gastroenteritis associated with a novel GII.8 sapovirus variant-transmitted by vomit in Shenzhen, China, 2019. BMC Infect. Dis. 2020, 20, 1–9. [Google Scholar] [CrossRef]
- Iritani, N.; Yamamoto, S.P.; Abe, N.; Kubo, H.; Oka, T.; Kaida, A. Epidemics of GI.2 sapovirus in gastroenteritis outbreaks during 2012−2013 in Osaka City, Japan. J. Med. Virol. 2016, 88, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Jahuira, H.; Gilman, R.H.; Alva, A.; Cabrera, L.; Okamoto, M.; Xu, H.; Windle, H.J.; Kelleher, D.; Varela, M.; et al. Etiological Role and Repeated Infections of Sapovirus among Children Aged Less than 2 Years in a Cohort Study in a Peri-urban Community of Peru. J. Clin. Microbiol. 2016, 54, 1598–1604. [Google Scholar] [CrossRef]
- Platts-Mills, J.A.; Liu, J.; Rogawski, E.T.; Kabir, F.; Lertsethtakarn, P.; Siguas, M.; Khan, S.S.; Praharaj, I.; Murei, A.; Nshama, R.; et al. Use of quantitative molecular diagnostic methods to assess the aetiology, burden, and clinical characteristics of diarrhoea in children in low-resource settings: A reanalysis of the MAL-ED cohort study. Lancet Glob. Health 2018, 6, e1309–e1318. [Google Scholar] [CrossRef]
- Oka, T.; Lu, Z.; Phan, T.; Delwart, E.L.; Saif, L.J.; Wang, Q. Genetic Characterization and Classification of Human and Animal Sapoviruses. PLoS ONE 2016, 11, e0156373. [Google Scholar] [CrossRef]
- Ishida, S.; Yoshizumi, S.; Miyoshi, M.; Ikeda, T.; Okui, T.; Katayama, K.; Takeda, N.; Oka, T. Characterization of sapoviruses detected in Hokkaido, Japan. Jpn. J. Infect. Dis. 2008, 61, 504–506. [Google Scholar]
- Chang, K.-O.; Sosnovtsev, S.S.; Belliot, G.; Wang, Q.; Saif, L.J.; Green, K.Y. Reverse Genetics System for Porcine Enteric Calicivirus, a Prototype Sapovirus in the Caliciviridae. J. Virol. 2005, 79, 1409–1416. [Google Scholar] [CrossRef]
- Chiba, S.; Nakata, S.; Numata-Kinoshita, K.; Honma, S. Sapporo Virus: History and Recent Findings. J. Infect. Dis. 2000, 181, S303–S308. [Google Scholar] [CrossRef]
- Nakata, S.; Honma, S.; Numata, K.; Kogawa, K.; Ukae, S.; Morita, Y.; Adachi, N.; Chiba, S. Members of the Family Caliciviridae (Norwalk Virus and Sapporo Virus) Are the Most Prevalent Cause of Gastroenteritis Outbreaks among Infants in Japan. J. Infect. Dis. 2000, 181, 2029–2032. [Google Scholar] [CrossRef]
- Kobayashi, S.; Fujiwara, N.; Yasui, Y.; Yamashita, T.; Hiramatsu, R.; Minagawa, H. A foodborne outbreak of sapovirus linked to catered box lunches in Japan. Arch. Virol. 2012, 157, 1995–1997. [Google Scholar] [CrossRef]
- Lee, L.E.; Cebelinski, E.A.; Fuller, C.; Keene, W.E.; Smith, K.; Vinjé, J.; Besser, J.M. Sapovirus Outbreaks in Long-Term Care Facilities, Oregon and Minnesota, USA, 2002–2009. Emerg. Infect. Dis. 2012, 18, 873–876. [Google Scholar] [CrossRef] [PubMed]
- Kitajima, M.; Haramoto, E.; Phanuwan, C.; Katayama, H. Genotype Distribution of Human Sapoviruses in Wastewater in Japan. Appl. Environ. Microbiol. 2011, 77, 4226–4229. [Google Scholar] [CrossRef]
- Iizuka, S.; Oka, T.; Tabara, K.; Omura, T.; Katayama, K.; Takeda, N.; Noda, M. Detection of sapoviruses and noroviruses in an outbreak of gastroenteritis linked genetically to shellfish. J. Med. Virol. 2010, 82, 1247–1254. [Google Scholar] [CrossRef]
- Rasanen, S.; Lappalainen, S.; Kaikkonen, S.; Hämäläinen, M.; Salminen, M.; Vesikari, T. Mixed viral infections causing acute gastroenteritis in children in a waterborne outbreak. Epidemiol. Infect. 2010, 138, 1227–1234. [Google Scholar] [CrossRef]
- Hansman, G.S.; Saito, H.; Shibata, C.; Ishizuka, S.; Oseto, M.; Oka, T.; Takeda, N. Outbreak of Gastroenteritis Due to Sapovirus. J. Clin. Microbiol. 2007, 45, 1347–1349. [Google Scholar] [CrossRef]
- Murray, T.Y.; Nadan, S.; Page, N.A.; Taylor, M.B. Diverse sapovirus genotypes identified in children hospitalised with gastroenteritis in selected regions of South Africa. J. Clin. Virol. 2016, 76, 24–29. [Google Scholar] [CrossRef]
- Murray, T.Y.; Taylor, M.B. Quantification and molecular characterisation of human sapoviruses in water sources impacted by highly polluted discharged wastewater in South Africa. J. Water Health 2015, 13, 1055–1059. [Google Scholar] [CrossRef]
- Murray, T.Y.; Mans, J.; Van Zyl, W.B.; Taylor, M.B. Application of a Competitive Internal Amplification Control for the Detection of Sapoviruses in Wastewater. Food Environ. Virol. 2012, 5, 61–68. [Google Scholar] [CrossRef][Green Version]
- Noronet Typing Tool, Version 2.0. Available online: http://www.rivm.nlm/norovirus/typingtool (accessed on 28 February 2021).
- Kumar, S.; Stecher, G.; Li, M.; Knyaz, C.; Tamura, K. MEGA X: Molecular evolutionary genetics analysis across computing platforms. Mol. Biol. Evol. 2018, 35, 1547–1549. [Google Scholar] [CrossRef]
- Page, N.; Groome, M.J.; Murray, T.Y.; Nadan, S.; Netshikweta, R.; Keddy, K.H.; Poonsamy, B.; Moyes, J.; Walaza, S.; Kahn, K.; et al. Sapovirus prevalence in children less than five years of age hospitalised for diarrhoeal disease in South Africa, 2009–2013. J. Clin. Virol. 2016, 78, 82–88. [Google Scholar] [CrossRef]
- Costa, L.C.P.D.N.; Siqueira, J.A.M.; Portal, T.M.; Júnior, E.C.S.; Linhares, A.D.C.; Gabbay, Y.B.; Resque, H.R. Detection and genotyping of human adenovirus and sapovirus in children with acute gastroenteritis in Belém, Pará, between 1990 and 1992: First detection of GI.7 and GV.2 sapoviruses in Brazil. Rev. Soc. Bras. Med. Trop. 2017, 50, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Aragão, G.C.; Mascarenhas, J.D.P.; Kaiano, J.H.L.; de Lucena, M.S.S.; Siqueira, J.A.M.; Fumian, T.M.; Hernandez, J.M.; de Oliveira, C.S.; Oliveira, D.S.; Araujo, E.C. Norovirus diversity in diarrheic children from an African descendant settlement in Belem, Northern Brazil. PLoS ONE 2013, 8, e56608. [Google Scholar] [CrossRef]
- Phan, T.G.; Okame, M.; Nguyen, T.A.; Maneekarn, N.; Nishio, O.; Okitsu, S.; Ushijima, H. Human astrovirus, norovirus (GI, GII), and sapovirus infections in Pakistani children with diarrhoea. J. Med. Virol. 2004, 73, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Ouédraogo, N.; Kaplon, J.; Bonkoungou, I.J.O.; Traoré, A.S.; Pothier, P.; Barro, N.; Ambert-Balay, K. Prevalence and genetic diversity of enteric viruses in children with diarrhoea in Ouagadougou, Burkina Faso. PLoS ONE 2016, 11, e0153652. [Google Scholar] [CrossRef] [PubMed]
- Binder, H.J.; Brown, I.; Ramakrishna, B.S.; Young, G.P. Oral Rehydration Therapy in the Second Decade of the Twenty-first Century. Curr. Gastroenterol. Rep. 2014, 16, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kotloff, K.L.; Nataro, J.P.; Blackwelder, W.C.; Nasrin, D.; Farag, T.H.; Panchalingam, S.; Wu, Y.; Sow, S.O.; Sur, D.; Breiman, R.F.; et al. Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the Global Enteric Multicenter Study, GEMS): A prospective, case-control study. Lancet 2013, 382, 209–222. [Google Scholar] [CrossRef]
- Matussek, A.; Dienus, O.; Djeneba, O.; Simpore, J.; Nitiema, L.; Nordgren, J. Molecular characterization and genetic susceptibility of sapovirus in children with diarrhoea in Burkina Faso. Infect. Genet. Evol. 2015, 32, 396–400. [Google Scholar] [CrossRef] [PubMed]
- Bucardo, F.; Reyes, Y.; Svensson, L.; Nordgren, J. Predominance of Norovirus and Sapovirus in Nicaragua after Implementation of Universal Rotavirus Vaccination. PLoS ONE 2014, 9, e98201. [Google Scholar] [CrossRef] [PubMed]
- Department of Water and Sanitation (DWS). Directorate: Water Macro Planning. In Strategic Overview of the Water Services Sector in South Africa 2015, 4th ed.; Department of Water and Sanitation (DWS) Directorate: Pretoria, South Africa, 2015; pp. 1–71. [Google Scholar]
- Potgieter, N.; Becker, P.; Ehlers, M. Evaluation of the CDC safe water-storage intervention to improve the microbiological quality of point-of-use drinking water in rural communities in South Africa. Water SA 2009, 35, 505–516. [Google Scholar] [CrossRef]
- Cláudia, B.; Helena, A.; Joana, S.; Paula, T. Role of flies as vectors of foodborne pathogens in rural areas. ISRN Microbiol. 2013, 2013, 1–7. [Google Scholar]
- Woldu, W.; Bitwe, B.D.; Gizaw, Z. Socioeconomic factors associated with diarrhoeal diseases among under-five children of the nomadic population in Northeast Ethiopia. Trop. Med. Health 2016, 44, 40. [Google Scholar] [CrossRef] [PubMed]
- Bessong, P.O.; Odiyo, J.O.; Musekene, J.N.; Tessema, A. Spatial Distribution of Diarrhoea and Microbial Quality of Domestic Water during an Outbreak of Diarrhoea in the Tshikuwi Community in Venda, South Africa. J. Health Popul. Nutr. 2009, 27, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Kabue, J.P.; Meader, E.; Hunter, P.R.; Potgieter, N. Norovirus prevalence and estimated viral load in symptomatic and asymptomatic children from rural communities of Vhembe district, South Africa. J. Clin. Virol. 2016, 84, 12–18. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Treatment of Diarrhoea: A Manual for Physicians and Senior Health Workers. 2005. Available online: http://whqlibdoc.who.int/publications (accessed on 30 December 2019).
- Boom, R.; Sol, C.J.; Salimans, M.M.; Jansen, C.L.; Dillen, P.M.W.-V.; Van Der Noordaa, J. Rapid and simple method for purification of nucleic acids. J. Clin. Microbiol. 1990, 28, 495–503. [Google Scholar] [CrossRef] [PubMed]
- NCBI GenBAnk, Blast Tool. Available online: http://www.ncbi.nlm.nih.gov/blast (accessed on 28 February 2021).



{kind=link}
{kind=link}
| Clinical Samples Collected | Outpatients from Clinics | Inpatients from Hospitals | Total Overall | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Age (Months) | Gender | n | Age (Months) | Gender | n | |||||
| M | F | M | F | ||||||||
| Children with diarrhoea (symptomatic) | 137 (71%) | 0–12 | 64(46.7%) | 31 | 34 | 91 (100%) | 0–12 | 46(50.5%) | 28 | 18 | 228 |
| 13–24 | 42(30.7%) | 23 | 19 | 13–24 | 29(31.9%) | 12 | 17 | ||||
| 25–36 | 14(10.2%) | 7 | 7 | 25–36 | 12(13.2%) | 7 | 5 | ||||
| 37–48 | 12(8.8%) | 3 | 9 | 37–48 | – | – | – | ||||
| 49–60 | 2(1.5%) | 0 | 2 | 49–60 | – | – | – | ||||
| Unknown | 3(2.2%) | 1 | 2 | Unknown | 4(4.4%) | 2 | 2 | ||||
| Children without diarrhoea (asymptomatic) | 56 (29%) | 0–12 | 38(67.9%) | 15 | 23 | 0 (0%) | 0–12 | – | N/A | N/A | 56 |
| 13–24 | 13(23.2%) | 5 | 8 | 13–24 | – | ||||||
| 25–36 | 4(7.1%) | 2 | 2 | 25–36 | – | ||||||
| 37–48 | – | – | – | 37–48 | – | ||||||
| 49–60 | – | – | – | 49–60 | – | ||||||
| Unknown | 1(1.8%) | 0 | 1 | Unknown | – | ||||||
| Total | n = 193 (100%) | n = 91 (100%) | 284 | ||||||||
| Case Patients (n = 228) | Controls (n = 56) | |||
|---|---|---|---|---|
| Parameters | SV Positives (%) n = 38 (16.7%) | SV Negatives (%) n = 190 (83.3%) | SV Positives (%) n = 2 (3.6%) | SV Negatives (%) n = 54 (96.8%) |
| Symptoms | None | |||
| Diarrhoea only | 22 (57.9%) | 68 (35.8%) | ||
| Diarrhoea with other symptoms | 16 (42.1%) | 121 (63.7%) | ||
| Unknown | – | 1 (0.5%) | ||
| Other symptoms | N/A | |||
| Vomiting | 11 (29.7%) | 91 (47.6%) | ||
| Fever | 8 (21.6%) | 60 (31.4%) | ||
| Abdominal pain | 4 (10.8%) | 27 (14.1%) | ||
| Dehydration | 3 (8.1%) | 24 (12.6%) | ||
| Interval * | N/A | |||
| ≤3 days | 22 (57.9%) | 122 (64.2%) | ||
| ≥3 days | 16 (42.1%) | 67 (35.3%) | ||
| Not defined | – | 1 (0.5%) | ||
| Case Patients (n = 228) | ||
|---|---|---|
| Parameters | Clinics (n = 137) (Positives/No. of Cases (%)) | Hospitals (n = 91) (Positives/No. of Cases (%)) |
| Diarrhoea only | 17/69 (24.6%) | 5/21 (23.8%) |
| Diarrhoea with other symptoms | 9/68 (13.2%) | 7/69 (10.1%) |
| Unknown | None | 1 (Neg) |
| Other symptoms | ||
| Vomiting | 7/45 (15.6%) | 4/55 (7.3%) |
| Fever | 4/22 (18.2%) | 2/32 (6.3%) |
| Abdominal pain | 2/13 (15.4%) | 4/28 (14.3%) |
| Dehydration | 0 | 3/27 (11.1%) |
| Household Settings | SV Positives v/s Enrolled Cases (%) | Patients Age Group (Month) and SV Positive Cases | |||||
|---|---|---|---|---|---|---|---|
| 0–12 Months | 13–24 Months | 25–36 Months | 37–48 Months | 49–60 Months | Unknown | ||
| 19 pos | 14 pos | 4 pos | 3 pos | 0 | 0 | ||
| Latrine | |||||||
| Used | 21/187 (11.2%) | 9/96 | 7/53 | 2/24 | 3/10 | 0/2 | 0/2 |
| Not used | 19/95 (20%) | 10/51 | 7/32 | 2/7 | 0/1 | 0 | 0/4 |
| Unknown | 0/2 (0%) | 0 | 0 | 0/2 | 0 | 0 | 0 |
| Water sources | |||||||
| Tap | 31/244 (12.7%) | 14/125 | 11/72 | 4/30 | 2/10 | 0/1 | 0/6 |
| Borehole | 5/26 (19.2%) | 3/16 | 1/6 | 0/2 | 1/1 | 0/1 | 0 |
| River | 2/2 (100%) | 1/1 | 1/1 | 0 | 0 | 0 | 0 |
| Spring | 2/9 (22.2%) | 1/5 | 1/4 | 0 | 0 | 0 | 0 |
| Unknown | 0/3 (0%) | 0 | 0/3 | 0 | 0 | 0 | 0 |
| Breastfeeding | |||||||
| Yes | 25/185 (13.5%) | 16/119 | 6/45 | 2/9 | 1/7 | 0/1 | 0/4 |
| No | 14/92 (15.2%) | 3/28 | 8/37 | 2/21 | 1/3 | 0/1 | 0/2 |
| Unknown | 1/7 (14.3%) | 0/1 | 0/3 | 0/2 | 1/1 | 0 | 0 |
| Livestock | |||||||
| Present | 9/88 (10.2%) | 4/39 | 3/32 | 1/10 | 1/3 | 0 | 0/4 |
| Absent | 31/196 (15.8%) | 15/106 | 11/56 | 3/22 | 2/8 | 0/2 | 0/2 |
| Unknown | 0/1 (0%) | 0/1 | 0 | 0 | 0 | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magwalivha, M.; Ngandu, J.-P.K.; Traore, A.N.; Potgieter, N. Prevalence and Genetic Characterisation of Human Sapovirus from Children with Diarrhoea in the Rural Areas of Vhembe District, South Africa, 2017–2020. Viruses 2021, 13, 393. https://doi.org/10.3390/v13030393
Magwalivha M, Ngandu J-PK, Traore AN, Potgieter N. Prevalence and Genetic Characterisation of Human Sapovirus from Children with Diarrhoea in the Rural Areas of Vhembe District, South Africa, 2017–2020. Viruses. 2021; 13(3):393. https://doi.org/10.3390/v13030393
Chicago/Turabian StyleMagwalivha, Mpho, Jean-Pierre Kabue Ngandu, Afsatou Ndama Traore, and Natasha Potgieter. 2021. "Prevalence and Genetic Characterisation of Human Sapovirus from Children with Diarrhoea in the Rural Areas of Vhembe District, South Africa, 2017–2020" Viruses 13, no. 3: 393. https://doi.org/10.3390/v13030393
APA StyleMagwalivha, M., Ngandu, J.-P. K., Traore, A. N., & Potgieter, N. (2021). Prevalence and Genetic Characterisation of Human Sapovirus from Children with Diarrhoea in the Rural Areas of Vhembe District, South Africa, 2017–2020. Viruses, 13(3), 393. https://doi.org/10.3390/v13030393