


Early Detection of Alzheimer’s Disease Using Generative Models: A Review of GANs and Diffusion Models in Medical Imaging

Abstract

1. Introduction
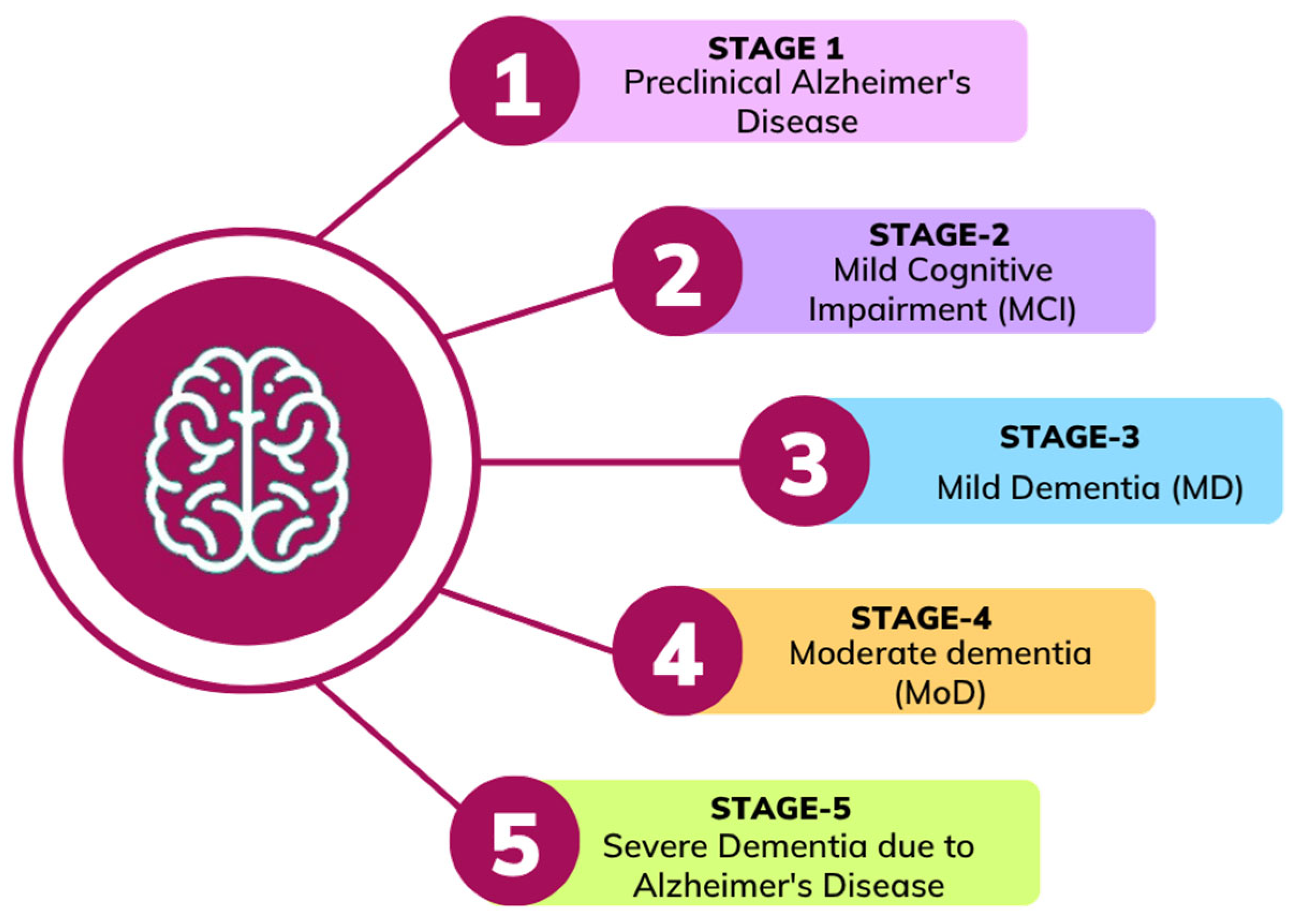
2. Alzheimer’s Disease Stages
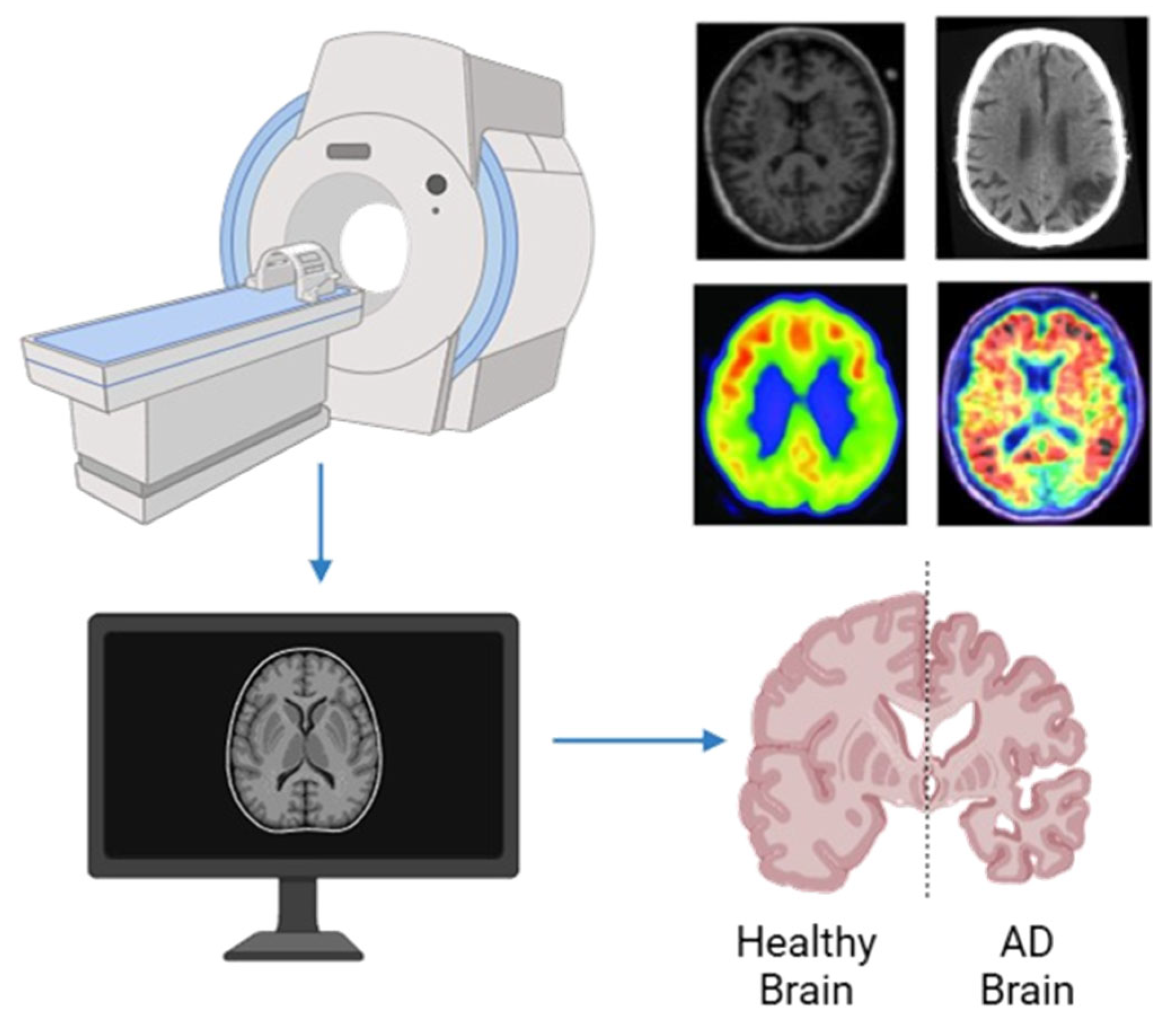
3. Neuroimaging Modalities
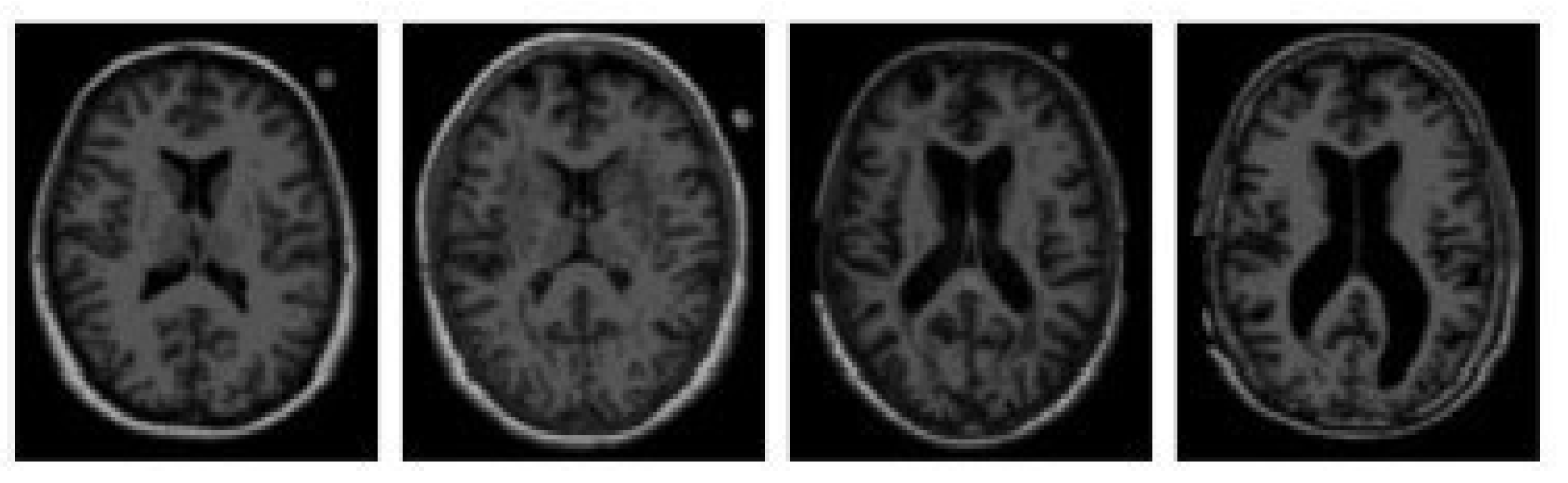
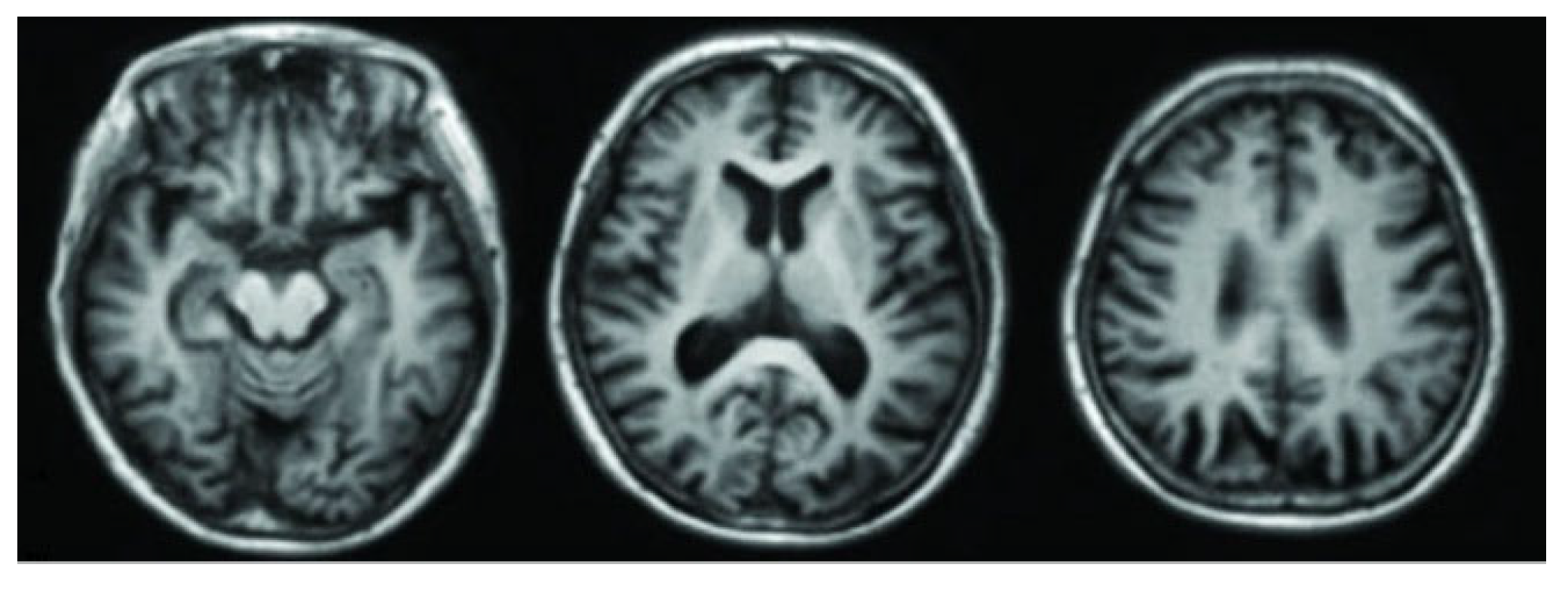
3.1. Magnetic Resonance Imaging (MRI)
3.2. Functional Magnetic Resonance Imaging (fMRI)
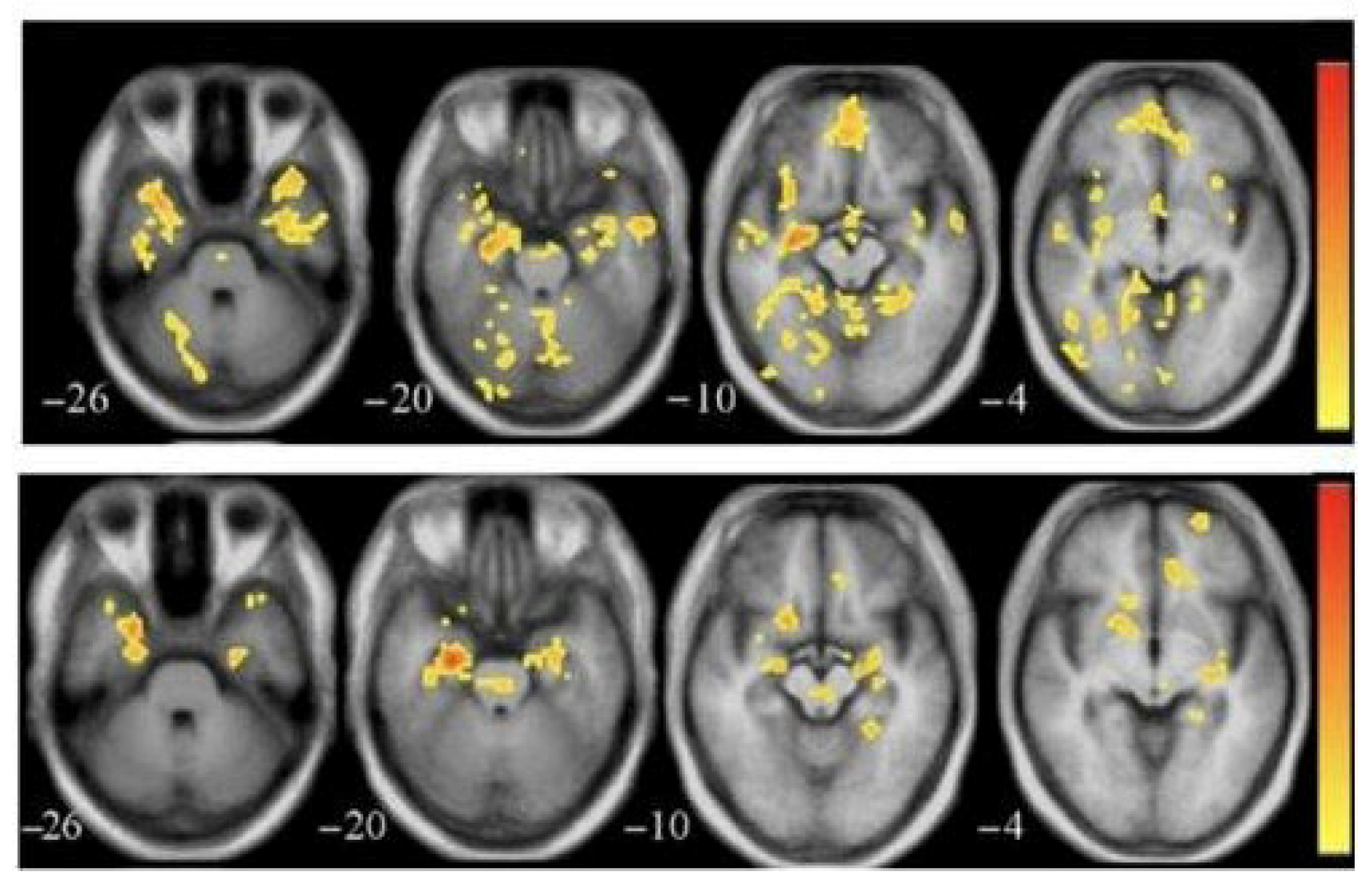
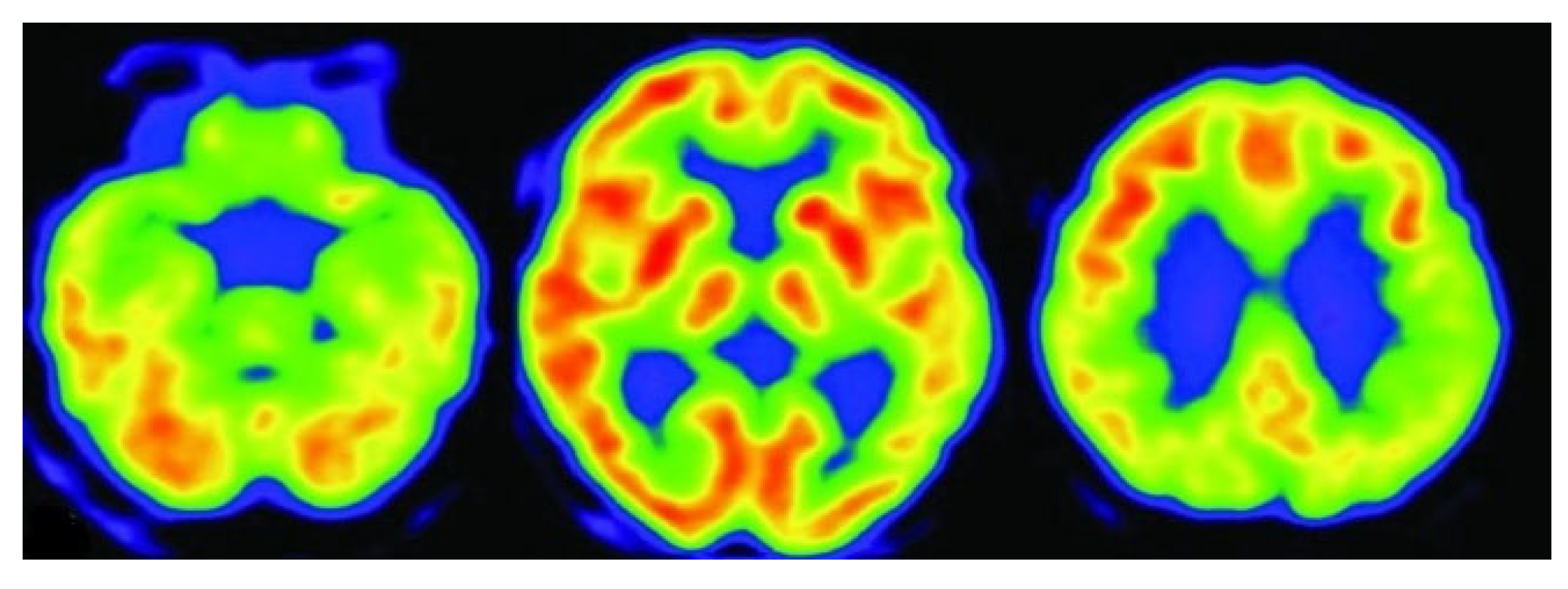
3.3. Positron Emission Tomography (PET)
3.4. Fluorodeoxyglucose Positron Emission Tomography (FDG-PET)
3.5. Computed Tomography (CT)
3.6. Diffusion Tensor Imaging (DTI)
4. Background Study
4.1. Paper Selection Strategy
4.2. Literature Review

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Dataset | Modality | Total Number of Participants |
|---|---|---|---|
| [21] | ADNI-like MRI data (T1w), Diffusion MRI of healthy subjects | Structural MRI | 18 AD, 18 bvFTD, 19 control: 14 healthy for connectome |
| [23] | ADNI-1 and ADNI-2 | MRI, PET | ADNI-1: 821; ADNI-2: 636 |
| [24] | OASIS-3 | MRI | Training: 408 subjects; Test: 113 healthy, 99 (CDR 0.5), 61 (CDR 1), 4 (CDR 2) |
| [25] | ADNI | MRI, PET | 1033 (722 train, 104 val, 207 test) |
| [26] | ADNI | PET | 411 PET scans (98 AD, 105 NC, 208 MCI) |
| [27] | ADNI | MRI, PET | 680 subjects |
| [28] | ADNI-1, ADNI-2 | MRI, PET | ADNI-1 (PET AD only), ADNI-2 (100 NC, 20 AD, 80 AD MRI-only) |
| [29] | ADNI-GO, ADNI-2, OASIS | 3D MRI | 210 (mi-GAN), 603 (classifier), 48 (validation) |
| [30] | OASIS-3, Internal dataset | T1, T1c MRI | 408 (T1), 135 (T1c healthy) |
| [31] | ADNI, AIBL, NACC | MRI (1.5-T and 3-T) | ADNI: 151 (training), AIBL: 107, NACC: 565 |
| [32] | ADNI-1, ADNI-2 | MRI + PET | ADNI-1: 821; ADNI-2: 534 |
| [33] | ADNI-1 | T1 MRI | 833 (221 AD, 297 MCI, 315 NC) |
| [34] | ADNI (268 subjects) | rs-fMRI + DTI | 268 |
| [35] | ADNI (13,500 3D MRI images after augmentation) | 3D Structural MRI | 138 (original), 13,500 (augmented scans) |
| [36] | ADNI (1732 scan-pairs, 873 subjects) | MRI → Synthesized PET | 873 |
| [37] | ADNI | T1-weighted MRI | 632 participants |
| [38] | ADNI2 | T1-weighted MRI | 169 participants, 27,600 image pairs |
| [39] | Custom MRI dataset (Kaggle) | T1-weighted Brain MRI | 6400 images (approx.) |
| [40] | ADNI2, NIFD (in-domain), NACC (external) | T1-weighted MRI | 3319 MRI scans |
| [41] | ADNI | MRI and PET (multimodal) | ~2400 (14,800 imaging sessions) |
| [42] | ADNI (Discovery), SMC (Practice) | T1-weighted MRI, Demographics, Cognitive scores | 538 (ADNI) + 343 (SMC) |
| [43] | ADNI | T1-weighted MRI | 362 (CN: 87, MCI: 211, AD: 64) |
| [44] | ADNI1, ADNI3, AIBL | 1.5 T & 3 T MRI | ~168 for SR cohort, ~1517 for classification |
| [45] | ADNI | T1-weighted MRI | 6400 images across 4 stages (Non-Demented, Very Mild, Mild, Moderate Demented) |
| [46] | ADNI | Cognitive Features | 819 participants (5013 records) |
| [47] | ADNI, OASIS-3, Centiloid | Low-res PET + MRI → High-res PET | ADNI: 334; OASIS-3: 113; Centiloid: 46 |
| [48] | ADNI | MRI T1WI, FDG PET (Synth.) | 332 subjects, 1035 paired scans |
| [49] | ADNI, OASIS, UK Biobank | 3D T1-weighted MRI | ADNI: 1188, OASIS: 600, UKB: 38,703 |
| [50] | Alzheimer MRI (6400 images) | T1-weighted MRI | Alzheimer: 6400 images |
| [51] | OASIS-3 | T1-weighted MRI | 300 (100 AD, 100 MCI, 100 NC) |
| [52] | ADNI-3, In-house | Siemens ASL MRI (T1, M0, CBF) | ADNI Siemens: 122; GE: 52; In-house: 58 |
| [53] | ADNI | MRI + Biospecimen (Aβ, t-tau, p-tau) | 50 subjects |
| [54] | OASIS | MRI | 300 subjects (100 AD, 100 MCI, 100 NC) |
| [55] | ADNI | MRI | 311 (AD: 65, MCI: 67, NC: 102, cMCI: 77) |
| [56] | ADNI | Structural MRI → Aβ-PET, Tau-PET (synthetic) | 1274 |
| [57] | Kaggle | MRI | 6400 images (4 AD classes) |
| [58] | ADNI | sMRI, DTI, fMRI (multimodal) | 5 AD stages (NC, SMC, EMCI, LMCI, AD) |
| Reference | Technique/Method | Model | Results |
|---|---|---|---|
| [21] | Network Diffusion Model | Network eigenmode diffusion model | Strong correlation between predicted and actual atrophy maps; eigenmodes accurately classified AD/bvFTD; ROC AUC higher than PCA |
| [23] | 3D CycleGAN + LM3IL | Two-stage: PET synthesis (3D-cGAN) + classification (LM3IL) | AD vs. HC—Accuracy: 92.5%, Sensitivity: 89.94%, Specificity: 94.53%; PSNR: 24.49 ± 3.46 |
| [24] | WGAN-GP + L1 loss (MRI slice reconstruction) | WGAN-GP-based unsupervised reconstruction + anomaly detection using L2 loss | AUC: 0.780 (CDR 0.5), 0.833 (CDR 1), 0.917 (CDR 2) |
| [25] | GANDALF: GAN with discriminator-adaptive loss for MRI-to-PET synthesis and AD classification | GAN + Classifier | Binary (AD/CN): 85.2% Acc3-class: 78.7% Acc, F2: 0.69, Prec: 0.83, Rec: 0.664-class: 37.0% Acc |
| [26] | DCGAN to generate PET images for NC, MCI, and AD | DCGAN | PSNR: 32.83, SSIM: 77.48, CNN classification accuracy improved to 71.45% with synthetic data |
| [27] | Bidirectional GAN with ResU-Net generator, ResNet-34 encoder, PatchGAN discriminator | Bidirectional GAN | PSNR: 27.36, SSIM: 0.88; AD vs. CN classification accuracy: 87.82% with synthetic PET |
| [28] | DCGAN for PET synthesis from noise; DenseNet classifier for AD vs. NC | DCGAN + DenseNet | Accuracy improved from 67% to 74%; MMD: 1.78, SSIM: 0.53 |
| [29] | 3D patch-based mi-GAN with baseline MRI + metadata; 3D DenseNet with focal loss for classification | mi-GAN + DenseNet | SSIM: 0.943, Multi-class Accuracy: 76.67%, pMCI vs. sMCI Accuracy: 78.45% |
| [30] | MADGAN: GAN with multiple adjacent slice reconstruction using WGAN-GP + ℓ1 loss and self-attention | 7-SA MADGAN | AUC for AD: 0.727 (MCI), 0.894 (late AD); AUC for brain metastases: 0.921 |
| [31] | Generative Adversarial Network (GAN), Fully Convolutional Network (FCN) | GAN + FCN | Improved AD classification with accuracy increases up to 5.5%. SNR, BRISQUE, and NIQE metrics showed significant image quality improvements. |
| [32] | TPA-GAN for PET imputation, PT-DCN for classification | TPA-GAN + PT-DCN | AD vs. CN: ACC 90.7%, SEN 91.2%, SPE 90.3%, F1 90.9%, AUC 0.95; pMCI vs. sMCI: ACC 85.2%, AUC 0.89 |
| [33] | THS-GAN: Tensor-train semi-supervised GAN with high-order pooling and 3D-DenseNet | THS-GAN | AD vs. NC: AUC 95.92%, Acc 95.92%; MCI vs. NC: AUC 88.72%, Acc 89.29%; AD vs. MCI: AUC 85.35%, Acc 85.71% |
| [34] | CT-GAN with Cross-Modal Transformer and Bi-Attention | GAN + Transformer with Bi-Attention | AD vs. NC: Acc = 94.44%, Sen = 93.33%, Spe = 95.24%LMCI vs. NC: Acc = 93.55%, Sen = 90.0%, Spe = 95.24%EMCI vs. NC: Acc = 92.68%, Sen = 90.48%, Spe = 95.0% |
| [35] | WGANGP-DTL (Wasserstein GAN with Gradient Penalty + Deep Transfer Learning using Inception v3 and DBN) | WGANGP + Inception v3 + DBN | Accuracy: 99.70% Sensitivity: 99.09% Specificity: 99.82% F1-score: >99% |
| [36] | BPGAN (3D BicycleGAN with Multiple Convolution U-Net, Hybrid Loss) | 3D BicycleGAN (BPGAN) with MCU Generator | Dataset-A: MAE = 0.0318, PSNR = 26.92, SSIM = 0.7294Dataset-B: MAE = 0.0396, PSNR = 25.08, SSIM = 0.6646 Diagnosis Acc = 85.03% (multi-class, MRI + Synth. PET) |
| [37] | ReMiND (Diffusion-based MRI Imputation) | Denoising Diffusion Probabilistic Model (DDPM) with modified U-Net | SSIM: 0.895, PSNR: 28.96; no classification metrics reported |
| [38] | Wavelet-guided Denoising Diffusion Probabilistic Model (Wavelet Diffusion) | Wavelet Diffusion with Wavelet U-Net | SSIM: 0.8201, PSNR: 27.15, FID: 13.15 (×4 scale); Recall ~90% (AD vs. NC); improved classification performance overall |
| [39] | CNN + GAN (DCGAN to augment data; CNN for classification) | CNN + DCGAN (data augmentation) | Accuracy: 96% (with GAN), 69% (without GAN); classification across 4 AD stages |
| [40] | Deep Grading + Multi-layer Perceptron + SVM Ensemble (Structure Grading + Atrophy) | 125 3D U-Nets + Ensemble (MLP + SVM) | In-domain (3-class): Accuracy: 86.0%, BACC: 84.7%, AUC: 93.8%, Sensitivity (CN/AD/FTD): 89.6/83.2/81.3; Out-of-domain: Accuracy: 87.1%, BACC: 81.6%, AUC: 91.6%, Sensitivity (CN/AD/FTD): 89.6/76.9/78.4 |
| [41] | GAN for synthetic MRI generation + Ensemble deep learning classifiers | GAN + CNN, LSTM, Ensemble Networks | GAN results: Precision: 0.84, Recall: 0.76, F1-score: 0.80, AUC-ROC: 0.91, Proposed Ensemble: Precision: 0.85, Recall: 0.79, F1-score: 0.82, AUC-ROC: 0.93 |
| [42] | Modified HexaGAN (Deep Generative Framework) | Modified HexaGAN (GAN + Semi-supervised + Imputation) | ADNI: AUROC 0.8609, Accuracy 0.8244, F1-score 0.7596, Sensitivity 0.8415, Specificity 0.8178; SMC: AUROC 0.9143, Accuracy 0.8528, Sensitivity 0.9667, Specificity 0.8286. |
| [43] | Conditional Diffusion Model for Data Augmentation | Conditional DDPM + U-Net | Best result (Combine 900): Accuracy: 74.73%, Precision: 77.28%, Recall (Sensitivity): 66.52%, F1-score: 0.6968, AUC: 0.8590; Specificity: not reported |
| [44] | Latent Diffusion Model (d3T*) for MRI super-resolution + DenseNet Siamese Network for AD/MCI/NC classification | Latent Diffusion-based SR + Siamese DenseNet | AD classification: Accuracy 92.3%, AUROC 93.1%, F1-score 91.9%; Significant improvement over 1.5 T and c3T*; Comparable to real 3 T MRI |
| [45] | GAN-based data augmentation + hybrid CNN-InceptionV3 model for multiclass AD classification | GAN + Transfer Learning (CNN + InceptionV3) | Accuracy: 90.91%; metrics like precision, recall, and F1-score also reported high performance |
| [46] | DeepCGAN (GAN + BiGRU with Wasserstein Loss) | Encoder–Decoder GAN with BiGRU layers | Accuracy: 97.32%, Recall (Sensitivity): 95.43%, Precision: 95.31%, F1-Score: 95.61%, AUC: 99.51% |
| [47] | Latent Diffusion Model for Resolution Recovery (LDM-RR) | Latent Diffusion Model (LDM-RR) | Recovery coefficient: 0.96; Longitudinal p-value: 1.3 × 10−10; Cross-tracer correlation: r = 0.9411; Harmonization p = 0.0421 |
| [48] | Diffusion-based multi-view learning (one-way and two-way synthesis) | U-NET-based Diffusion Model with MLP Classifier | Accuracy: 82.19%, SSIM: 0.9380, PSNR: 26.47, Sensitivity: 95.19%, Specificity: 92.98%, Recall: 82.19% |
| [49] | Conditional DDPM and LDM with counterfactual generation and DenseNet121 classifier | LDM + 3D DenseNet121 CNN | AUC: 0.870, F1-score: 0.760, Sensitivity: 0.889, Specificity: 0.837 (ADNI test set after fine-tuning) |
| [50] | GANs, VAEs, Diffusion (DDIM) models for MRI generation + DenseNet/ResNet classifiers | DDIM (Diffusion Model) + DenseNet | Accuracy: 80.84%, Precision: 86.06%, Recall: 78.14%, F1-Score: 80.98% (Alzheimer’s, DenseNet + DDIM) |
| [51] | GAN-based data generation + EfficientNet for multistage classification | GAN for data augmentation + EfficientNet CNN | Accuracy: 88.67% (1:0), 87.17% (9:1), 82.50% (8:2), 80.17% (7:3); Recall/Sensitivity/Specificity not separately reported |
| [52] | Conditional Latent Diffusion Model (LDM) for M0 image synthesis from Siemens PASL | Conditional LDM + ML classifier | SSIM: 0.924, PSNR: 33.35, CBF error: 1.07 ± 2.12 mL/100 g/min; AUC: 0.75 (Siemens), 0.90 (GE) in AD vs. CN classification |
| [53] | Multi-modal conditional diffusion model for image-to-image translation (prognosis prediction) | Conditional Diffusion Model + U-Net | PSNR: 31.99 dB, SSIM: 0.75, FID: 11.43 |
| [54] | GAN for synthetic MRI image generation + EfficientNet for multi-stage classification | GAN + EfficientNet | Validation accuracy improved from 78.48% to 85.11%, training accuracy from 90.16% to 98.68% with GAN data |
| [55] | Dual GAN + Pyramid Attention + CNN | Dual GAN with Pyramid Attention and CNN | Accuracy: 98.87%, Recall/Sensitivity: 95.67%, Specificity: 98.78%, Precision: 99.78%, F1-score: 99.67% |
| [56] | Prior-information-guided residual diffusion model with CLIP module and intra-domain difference loss | Residual Diffusion Model with CLIP guidance | SSIM: 92.49% (Aβ), 91.44% (Tau); PSNR: 26.38 dB (Aβ), 27.78 dB (Tau); AUC: 90.74%, F1: 82.74% (Aβ); AUC: 90.02%, F1: 76.67% (Tau) |
| [57] | Hybrid of Deep Super-Resolution GAN (DSR-GAN) for image enhancement + CNN for classification | DSR-GAN + CNN | Accuracy: 99.22%, Precision: 99.01%, Recall: 99.01%, F1-score: 99.01%, AUC: 100%, PSNR: 29.30 dB, SSIM: 0.847, MS-SSIM: 96.39% |
| [58] | Bidirectional Graph GAN (BG-GAN) + Inner Graph Convolution Network + Balancer for stable multimodal connectivity generation | BG-GAN + InnerGCN | Accuracy > 96%, Precision/Recall/F1 ≈ 0.98–1.00, synthetic data outperformed real in classification |
| Reference | Dataset | Model | Challenges and Limitations |
|---|---|---|---|
| [21] | ADNI-like MRI data (T1w), Diffusion MRI of healthy subjects | Network eigenmode diffusion model | Small sample size; no conventional ML metrics (accuracy, F1); assumes static connectivity; limited resolution in tractography; noise in MRI volumetrics. |
| [23] | ADNI-1 & ADNI-2 | Two-stage: PET synthesis (3D-cGAN) + classification (LM3IL) | Requires accurate MRI–PET alignment; patch-based learning may limit generalization. |
| [24] | OASIS-3 | WGAN-GP-based unsupervised reconstruction + anomaly detection using L2 loss | Region-limited detection (hippocampus/amygdala); may miss anomalies outside selected areas. |
| [25] | ADNI | GAN + Classifier | Binary classification was not better than CNN-only models; requires more tuning and architectural exploration. |
| [26] | ADNI | DCGAN | Trained separate GANs per class; used 2D slices only; lacks unified 3D modeling approach. |
| [27] | ADNI | Bidirectional GAN | Limited fine detail in some outputs; latent vector injection mechanism could be improved for better synthesis. |
| [28] | ADNI-1, ADNI-2 | DCGAN + DenseNet | Used 2D image generation; manual filtering of outputs; lacks 3D modeling and automation. |
| [29] | ADNI-GO, ADNI-2, OASIS | mi-GAN + DenseNet | Lower performance on gray matter prediction; limited short-term progression prediction; improvement possible with better feature modeling. |
| [30] | OASIS-3, Internal dataset | 7-SA MADGAN | Reconstruction instability on T1c scans; limited generalization; fewer healthy T1c scans; needs optimized attention modules. |
| [31] | ADNI, AIBL, NACC | GAN + FCN | Small sample size for GAN training (151 participants). Limited to AD vs. normal cognition (no MCI). |
| [32] | ADNI-1, ADNI-2 | TPA-GAN + PT-DCN | Requires paired modalities; model trained/tested on ADNI-1/2 independently; limited generalization. |
| [33] | ADNI-1 | THS-GAN | Requires careful TT-rank tuning; performance varies with GSP block position; validation limited to ADNI dataset. |
| [34] | ADNI (268 subjects) | GAN + Transformer with Bi-Attention | Limited dataset size, dependency on predefined ROIs, potential overfitting; lacks validation on other neurodegenerative disorders. |
| [35] | ADNI (13,500 3D MRI images after augmentation) | WGANGP + Inception v3 + DBN | Heavy reliance on data augmentation, complex pipeline requiring multiple preprocessing and tuning steps. |
| [36] | ADNI (1732 scan-pairs, 873 subjects) | 3D BicycleGAN (BPGAN) with MCU Generator | High preprocessing complexity, marginal diagnostic gains, requires broader validation and adaptive ROI exploration. |
| [37] | ADNI | Denoising Diffusion Probabilistic Model (DDPM) with modified U-Net | Uses only adjacent timepoints; assumes fixed intervals; no classification; no sensitivity/specificity; computationally intensive. |
| [38] | ADNI2 | Wavelet Diffusion with Wavelet U-Net | High computational cost; limited to T1 MRI; does not incorporate multi-modal data or longitudinal timepoints. |
| [39] | Custom MRI dataset (Kaggle) | CNN + DCGAN (data augmentation) | Risk of overfitting due to small original dataset; no reporting of sensitivity/specificity; limited to image data. |
| [40] | ADNI2, NIFD (in-domain), NACC (external) | 125 3D U-Nets + Ensemble (MLP + SVM) | High computational cost (393 M parameters, 25.9 TFLOPs); inference time ~1.6 s; only baseline MRI used; limited by class imbalance and absence of multimodal or longitudinal data. |
| [41] | ADNI | GAN + CNN, LSTM, Ensemble Networks | Limited real Alzheimer’s samples; reliance on synthetic augmentation; needs more external validation and data diversity. |
| [42] | ADNI (Discovery), SMC (Practice) | Modified HexaGAN (GAN + Semi-supervised + Imputation) | High model complexity; requires fine-tuning across datasets; limited to MRI and tabular inputs. |
| [43] | ADNI | Conditional DDPM + U-Net | Small dataset, imbalanced classes; specificity not reported; limited to static MRI slices; no multi-modal or longitudinal data. |
| [44] | DNI1, ADNI3, AIBL | Latent Diffusion-based SR + Siamese DenseNet | High computational cost; needs advanced infrastructure for training; diffusion SR takes longer than CNN-based methods. |
| [45] | ADNI | GAN + Transfer Learning (CNN + InceptionV3) | Class imbalance still impacts performance slightly; more detailed metrics (sensitivity/specificity) not reported. |
| [46] | ADNI | Encoder–Decoder GAN with BiGRU layers | Computational complexity, GAN training instability, underutilization of multimodal data (e.g., neuroimaging). |
| [47] | ADNI, OASIS-3, Centiloid | Latent Diffusion Model (LDM-RR) | High computational cost; trained on synthetic data; limited interpretability; real-time deployment needs optimization. |
| [48] | ADNI | U-NET-based Diffusion Model with MLP Classifier | One-way synthesis introduces variability; computational intensity; requires improvement in generalization and speed. |
| [49] | ADNI, OASIS, UK Biobank | LDM + 3D DenseNet121 CNN | High computational cost, requires careful fine-tuning, limited by resolution/memory constraints. |
| [50] | Alzheimer MRI (6400 images) | DDIM (Diffusion Model) + DenseNet | Diffusion models are computationally intensive; VAE had low image quality; fine-tuning reduced accuracy in some cases; computational cost vs. performance tradeoff. |
| [51] | OASIS-3 | GAN for data augmentation + EfficientNet CNN | GAN training instability; performance drop when synthetic data exceeds real data; no separate sensitivity/specificity metrics reported. |
| [52] | ADNI-3, In-house | Conditional LDM + ML classifier | No ground truth M0 for Siemens data; SNR difference between PASL/pCASL; class imbalance; vendor variability. |
| [53] | ADNI | Conditional Diffusion Model + U-Net | Small sample size; no classification metrics reported; requires broader validation with more diverse data. |
| [54] | OASIS | GAN + EfficientNet | GAN training instability; overfitting in CNN; limited dataset size; scope to explore alternate GAN models for robustness. |
| [55] | ADNI | Dual GAN with Pyramid Attention and CNN | Dependent on ADNI dataset quality; generalization affected by population diversity; limited interpretability; reliance on image features for AD detection. |
| [56] | ADNI | Residual Diffusion Model with CLIP guidance | Dependent on accurate prior info (e.g., age, gender); high computational cost; needs optimization for broader demographic generalization. |
| [57] | Kaggle | DSR-GAN + CNN | High computational complexity; SR trained on only 1700 images; generalizability and real-time scalability remain open challenges. |
| [58] | ADNI | BG-GAN + InnerGCN | Difficulty in precise structure-function mapping due to fMRI variability; biological coordination model can be improved. |
5. Dataset
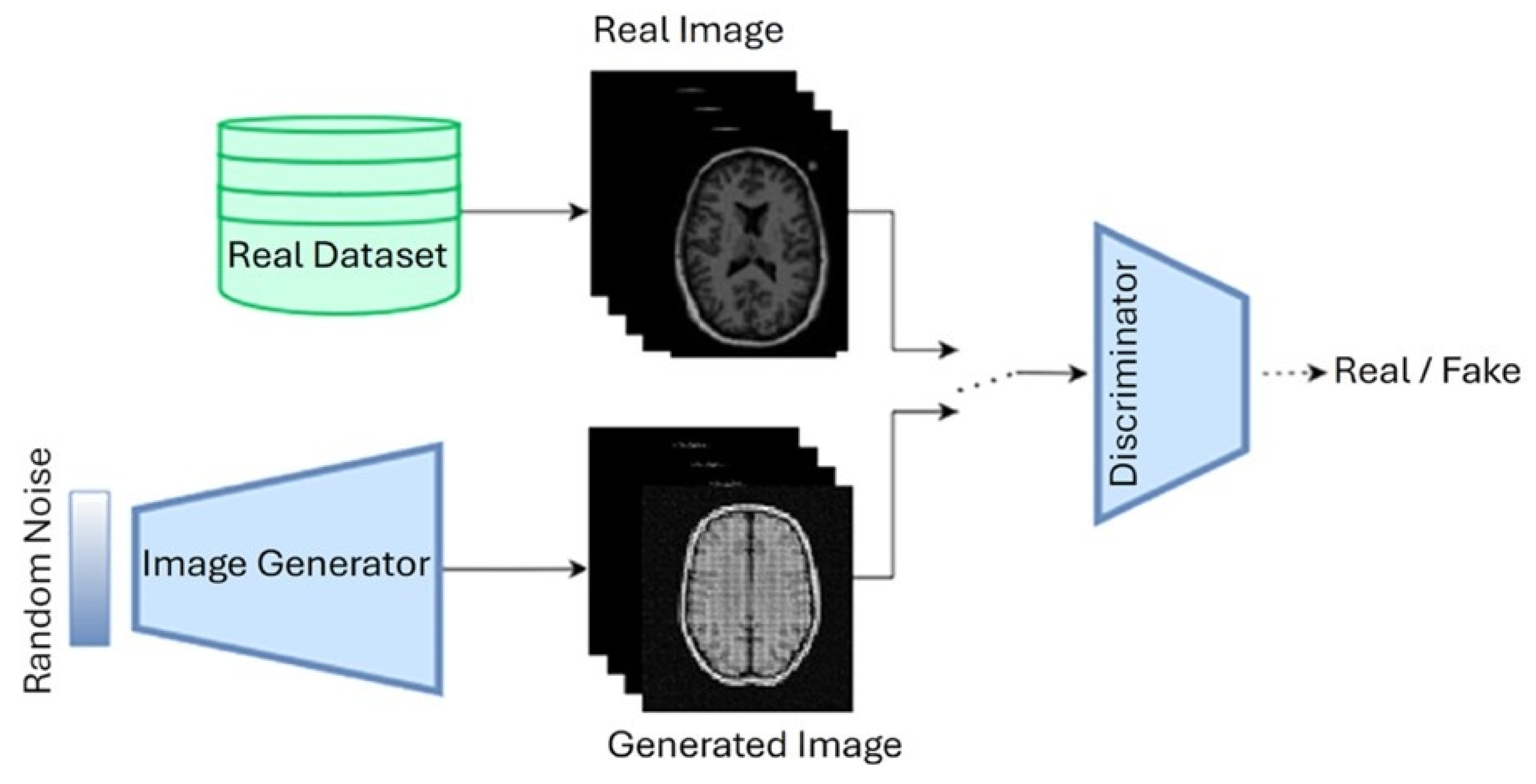
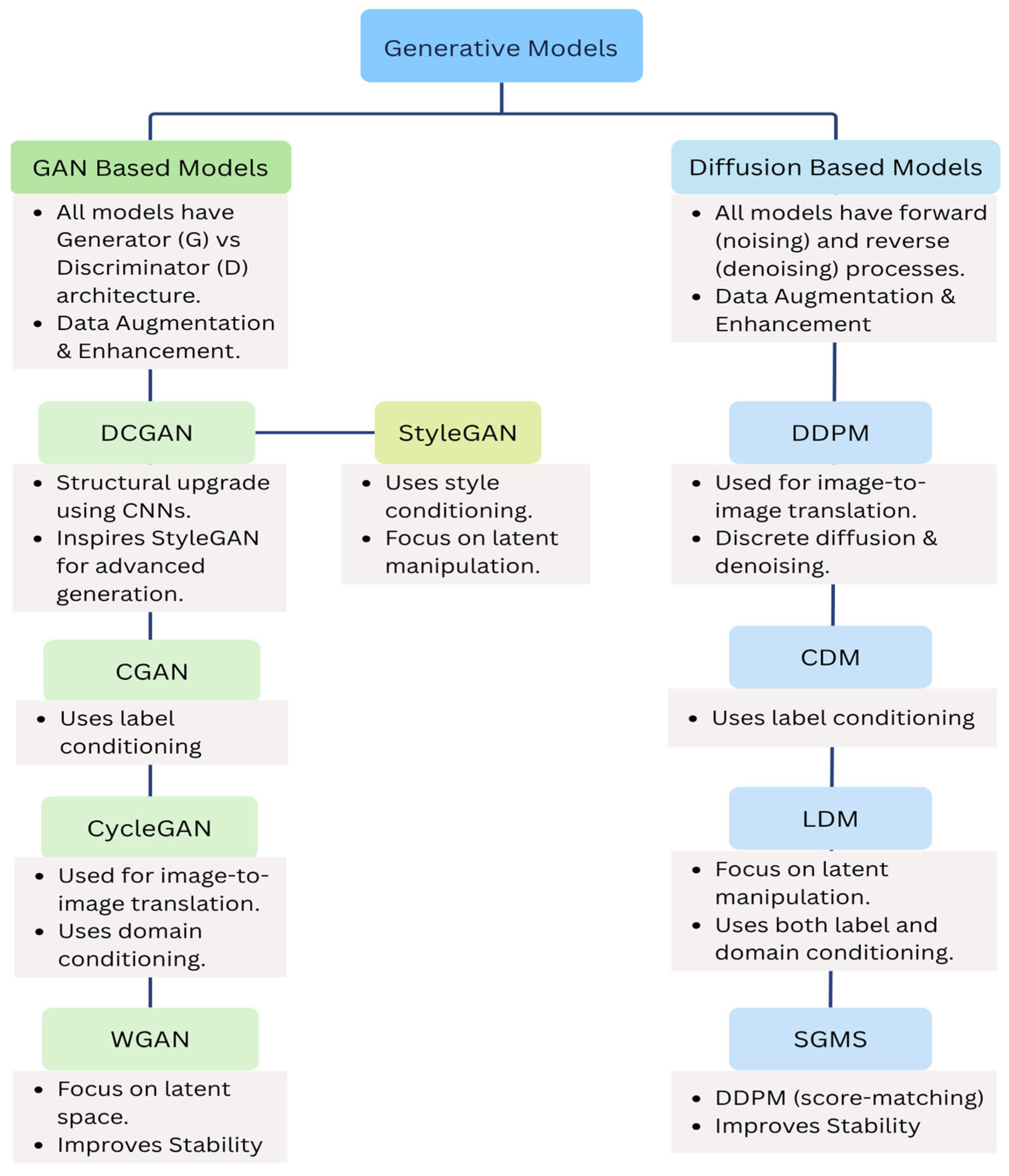
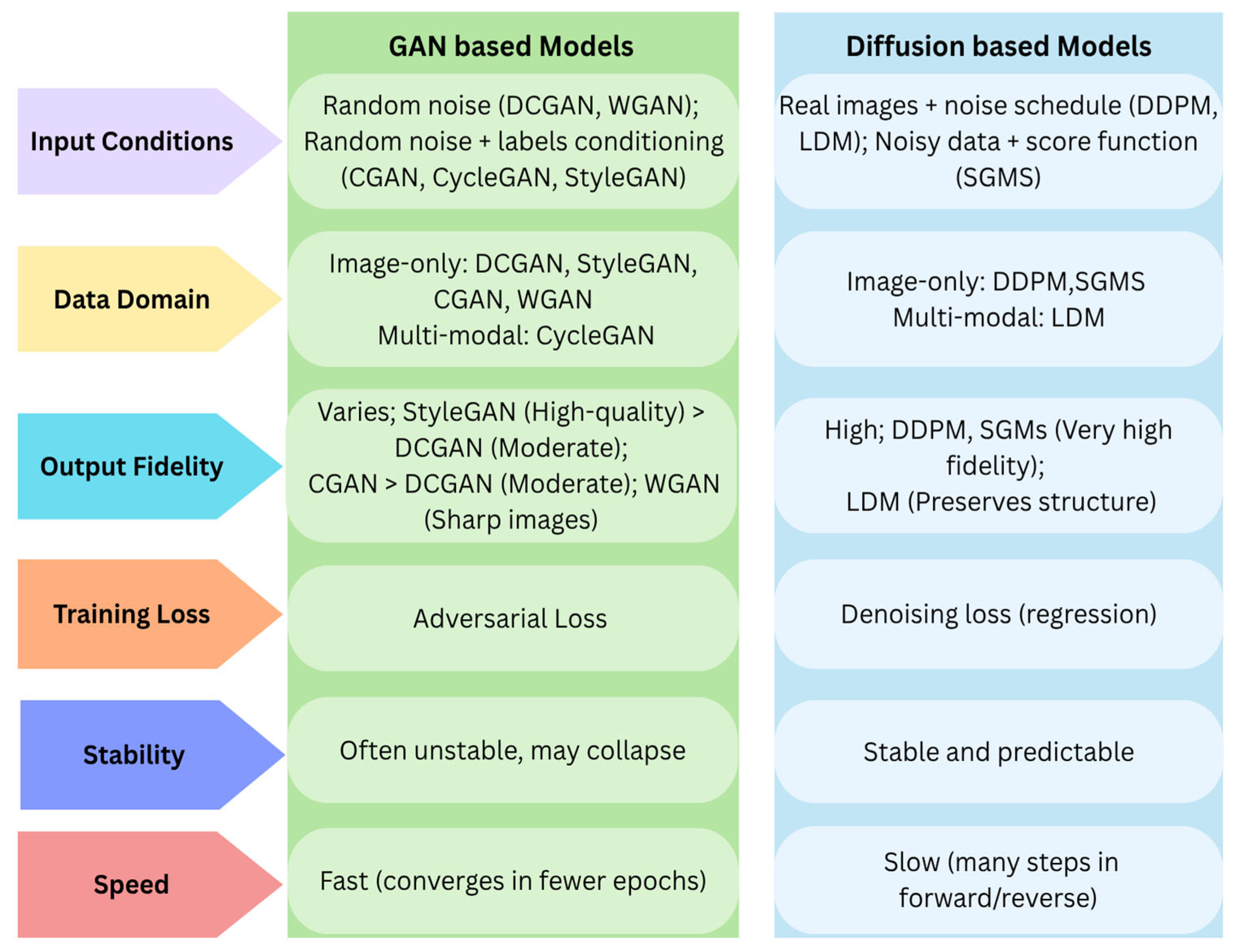
6. Generative Adversarial Networks (GANs)
6.1. Deep Convolutional Gan (DCGAN)
6.2. Conditional Gan (CGAN)
6.3. CycleGAN
6.4. StyleGAN
6.5. Wasserstein GAN (WGAN)
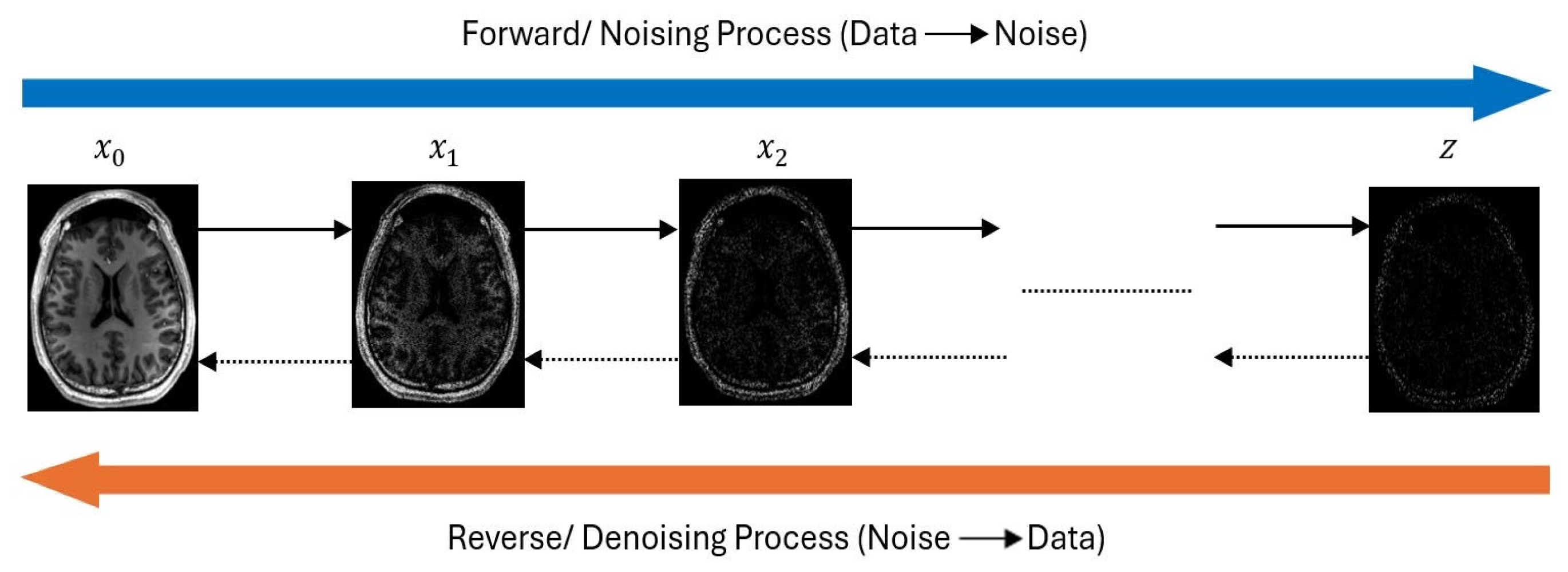
7. Diffusion Models
7.1. Denoising Diffusion Probabilistic Models (DDPM)
7.2. Convolutional Diffusion Models (CDM)
7.3. Latentl Diffusion Models (LDM)
7.4. Score-Based Generative Models (SGMS)
8. Discussion and Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| GAN | Generative Adversarial Network |
| MRI | Magnetic Resonance Imaging |
| MCI | Mild Cognitive Impairment |
| AD | Alzheimer’s Disease |
References
- World Health Organization. Ageing and Health; WHO (World Health Organization): Geneva, Switzerland, 2024. [Google Scholar]
- Bronzuoli, M.R.; Iacomino, A.; Steardo, L.; Scuderi, C. Targeting neuroinflammation in Alzheimer’s disease. J. Inflamm. Res. 2016, 9, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Alzheimer’s Disease International. Alzheimer’s Disease International; Alzheimer’s Disease International: London, UK, 2024. [Google Scholar]
- Alzheimer and Association. American Perspectives on Early Detection of Alzheimer’s Disease in the Era of Treatment; Alzheimer’s Association: Chicago, IL, USA, 2025. [Google Scholar]
- Uddin, J.; Shumi, S.S.; Khandoker, F.; Fariha, T. Factors Contributing to Alzheimer’s disease in Older Adult Populations: A Narrative Review. Int. J. Sci. Res. Multidiscip. Stud. 2024, 10, 76–82. [Google Scholar]
- Braak, H.; Braak, E. Neuropathological stageing of Alzheimer-related changes. Acta Neuropathol. 1991, 82, 239–259. [Google Scholar] [CrossRef] [PubMed]
- Ávila-Villanueva, M.; Dolado, A.M.; Gómez-Ramírez, J.; Fernández-Blázquez, M. Brain Structural and Functional Changes in Cognitive Impairment Due to Alzheimer’s Disease. Front. Psychol. 2022, 13, 886619. [Google Scholar] [CrossRef] [PubMed]
- Jack, C.R., Jr.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimer’s Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef] [PubMed]
- Goodfellow, I.J.; Pouget-Abadie, J.; Mirza, M.; Xu, B.; Warde-Farley, D.; Ozair, S.; Courville, A.; Bengio, Y. Generative Adversarial Networks. arXiv 2014, arXiv:1406.2661. [Google Scholar] [CrossRef]
- Bowles, C.; Chen, L.; Guerrero, R.; Bentley, P.; Gunn, R.; Hammers, A.; Dickie, D.A.; Hernández, M.V.; Wardlaw, J.; Rueckert, D. GAN Augmentation: Augmenting Training Data using Generative Adversarial Networks. arXiv 2018, arXiv:1810.10863. [Google Scholar] [CrossRef]
- Chartsias, A.; Joyce, T.; Giuffrida, M.V.; Tsaftaris, S.A. Multimodal MR Synthesis via Modality-Invariant Latent Representation. IEEE Trans. Med. Imaging 2018, 37, 803–814. [Google Scholar] [CrossRef] [PubMed]
- You, C.; Li, G.; Zhang, Y.; Zhang, X.; Shan, H.; Ju, S.; Zhao, Z.; Zhang, Z.; Cong, W.; Vannier, M.W.; et al. CT Super-Resolution GAN Constrained by the Identical, Residual, and Cycle Learning Ensemble (GAN-CIRCLE). IEEE Trans. Med. Imaging 2020, 39, 188–203. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.; Jain, A.; Abbeel, P. Denoising Diffusion Probabilistic Models. arXiv 2020, arXiv:2006.11239. [Google Scholar] [CrossRef]
- Khandoker, F.; Uddin, J.; Fariha, T.; Shumi, S.S. Importance of Psychological Well-being after disasters in Bangladesh: A Narrative Review. Int. J. Sci. Res. Multidiscip. Stud. 2024, 10, 1–6. [Google Scholar]
- Clinic, M. Alzheimer’s Stages: How the Disease Progresses. Available online: https://www.mayoclinic.org/diseases-conditions/alzheimers-disease/in-depth/alzheimers-stages/art-20048448 (accessed on 4 July 2025).
- Ahmed, M.R.; Zhang, Y.; Feng, Z.; Lo, B.; Inan, O.T.; Liao, H. Neuroimaging and Machine Learning for Dementia Diagnosis: Recent Advancements and Future Prospects. IEEE Rev. Biomed. Eng. 2019, 12, 19–33. [Google Scholar] [CrossRef] [PubMed]
- Scheltens, P.; Fox, N.; Barkhof, F.; De Carli, C. Structural magnetic resonance imaging in the practical assessment of dementia: Beyond exclusion. Lancet Neurol. 2002, 1, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Jeong, M.; Stiles, W.R.; Choi, H.S. Neuroimaging Modalities in Alzheimer’s Disease: Diagnosis and Clinical Features. Int. J. Mol. Sci. 2022, 23, 6079. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.; Shan, Y.; Ding, J. A literature review of MRI techniques used to detect amyloid-beta plaques in Alzheimer’s disease patients. Ann. Palliat. Med. 2021, 10, 10062–10074. [Google Scholar] [CrossRef] [PubMed]
- Alves, G.S.; Knöchel, V.O.; Knöchel, C.; Carvalho, A.F.; Pantel, J.; Engelhardt, E.; Laks, J. Integrating Retrogenesis Theory to Alzheimer’s Disease Pathology: Insight from DTI-TBSS Investigation of the White Matter Microstructural Integrity. Biomed. Res. Int. 2015, 2015, 291658. [Google Scholar] [CrossRef] [PubMed]
- Raj, A.; Kuceyeski, A.; Weiner, M. A Network Diffusion Model of Disease Progression in Dementia. Neuron 2012, 73, 1204–1215. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.; Park, B.; Han, K. Classification of diffusion tensor images for the early detection of Alzheimer’s disease. Comput. Biol. Med. 2013, 43, 1313–1320. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Liu, M.; Lian, C.; Zhou, T.; Xia, Y.; Shen, D. Synthesizing missing PET from MRI with cycle-consistent generative adversarial networks for Alzheimer’s disease diagnosis. In Medical Image Computing and Computer Assisted Intervention–MICCAI 2018, Proceedings of the 21st International Conference, Granada, Spain, 16–20 September 2018; Lecture Notes in Computer Science (Including Subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics); Springer: Cham, Switzerland, 2018; pp. 455–463. [Google Scholar] [CrossRef]
- Han, C.; Rundo, L.; Murao, K.; Milacski, Z.Á.; Umemoto, K.; Sala, E.; Nakayama, H.; Satoh, S. GAN-based Multiple Adjacent Brain MRI Slice Reconstruction for Unsupervised Alzheimer’s Disease Diagnosis. arXiv 2019, arXiv:1906.06114. [Google Scholar]
- Shin, H.-C.; Ihsani, A.; Xu, Z.; Mandava, S.; Sreenivas, S.T.; Forster, C.; Cha, J.; Alzheimer’s Disease Neuroimaging Initiative. GANDALF: Generative Adversarial Networks with Discriminator-Adaptive Loss Fine-Tuning for Alzheimer’s Disease Diagnosis from MRI. In Medical Image Computing and Computer Assisted Intervention–MICCAI 2020, Proceedings of the 23rd International Conference, Lima, Peru, 4–8 October 2020; Lecture Notes in Computer Science (Including Subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics); Springer Science and Business Media Deutschland GmbH: Berlin, Germany, 2020; pp. 688–697. [Google Scholar] [CrossRef]
- Islam, J.; Zhang, Y. GAN-based synthetic brain PET image generation. Brain Inf. 2020, 7, 3. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.; Shen, Y.; Wang, S.; Lei, B. Brain MR to PET Synthesis via Bidirectional Generative Adversarial Network. In Medical Image Computing and Computer Assisted Intervention–MICCAI 2020, Proceedings of the 23rd International Conference, Lima, Peru, 4–8 October 2020; Lecture Notes in Computer Science (Including Subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics); Springer Science and Business Media Deutschland GmbH: Berlin, Germany, 2020; pp. 698–707. [Google Scholar] [CrossRef]
- Hu, S.; Yu, W.; Chen, Z.; Wang, S. Medical Image Reconstruction Using Generative Adversarial Network for Alzheimer Disease Assessment with Class-Imbalance Problem. In Proceedings of the 2020 IEEE 6th International Conference on Computer and Communications, ICCC 2020, Chengdu, China, 11–14 December 2020; pp. 1323–1327. [Google Scholar] [CrossRef]
- Zhao, Y.; Ma, B.; Jiang, P.; Zeng, D.; Wang, X.; Li, S. Prediction of Alzheimer’s Disease Progression with Multi-Information Generative Adversarial Network. IEEE J. Biomed. Health Inform. 2021, 25, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Han, C.; Rundo, L.; Murao, K.; Noguchi, T.; Shimahara, Y.; Milacski, Z.A.; Koshino, S.; Sala, E.; Nakayama, H.; Satoh, S. MADGAN: Unsupervised medical anomaly detection GAN using multiple adjacent brain MRI slice reconstruction. BMC Bioinform. 2021, 22, 31. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Qiu, S.; Joshi, P.S.; Xue, C.; Killiany, R.J.; Mian, A.Z.; Chin, S.P.; Au, R. Enhancing magnetic resonance imaging-driven Alzheimer’s disease classification performance using generative adversarial learning. Alzheimer’s Res. Ther. 2021, 13, 60. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Shi, F.; Shen, D.; Liu, M.; Disease, T.A. Task-Induced Pyramid and Attention GAN for Multimodal Brain Image Imputation and Classification in Alzheimer’s Disease. IEEE J. Biomed. Health Inform. 2022, 26, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.; Lei, B.; Ng, M.K.; Cheung, A.C.; Shen, Y.; Wang, S. Tensorizing GAN with High-Order Pooling for Alzheimer’s Disease Assessment. arXiv 2020, arXiv:2008.00748. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Wang, S. Cross-Modal Transformer GAN: A Brain Structure-Function Deep Fusing Framework for Alzheimer’s Disease. arXiv 2022, arXiv:2206.13393. [Google Scholar]
- Thota, N.R.; Vasumathi, D. Wasserstein Gan-Gradient Penalty with Deep Transfer Learning Based Alzheimer Disease Classification on 3D Mri Scans. I-Manag. J. Image Process. 2022, 9, 9–20. [Google Scholar]
- Zhang, J.; He, X.; Qing, L.; Gao, F.; Wang, B. BPGAN: Brain PET synthesis from MRI using generative adversarial network for multi-modal Alzheimer’s disease diagnosis. Comput. Methods Programs Biomed. 2022, 217, 106676. [Google Scholar] [CrossRef] [PubMed]
- Yuan, C.; Duan, J.; Tustison, N.J.; Xu, K.; Hubbard, R.A.; Linn, K.A. ReMiND: Recovery of Missing Neuroimaging using Diffusion Models with Application to Alzheimer’s Disease. medRxiv 2023. [Google Scholar] [CrossRef]
- Huang, G.; Chen, X.; Shen, Y.; Wang, S. MR Image Super-Resolution Using Wavelet Diffusion for Predicting Alzheimer’s Disease. In Brain Informatics, Proceedings of the 16th International Conference, BI 2023, Hoboken, NJ, USA, 1–3 August 2023; Lecture Notes in Computer Science (Including Subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics); Springer Science and Business Media Deutschland GmbH: Berlin, Germany, 2023; pp. 146–157. [Google Scholar] [CrossRef]
- Boyapati, N.; Tej, M.B.; Darshitha, M.; Shreya, P.; Naveen, S.N.; Gandhi, C.R.; Amrutha, V. Alzheimer’s Disease Prediction using Convolutional Neural Network (CNN) with Generative Adversarial Network (GAN). In Proceedings of the 2023 International Conference on Data Science, Agents and Artificial Intelligence, ICDSAAI 2023, Chennai, India, 21–23 December 2023. [Google Scholar] [CrossRef]
- Nguyen, H.D.; Clément, M.; Planche, V.; Mansencal, B.; Coupé, P. Deep grading for MRI-based differential diagnosis of Alzheimer’s disease and Frontotemporal dementia. Artif. Intell. Med. 2023, 144, 102636. [Google Scholar] [CrossRef] [PubMed]
- Sekhar, U.S.; Vyas, N.; Dutt, V.; Kumar, A. Multimodal Neuroimaging Data in Early Detection of Alzheimer’s Disease: Exploring the Role of Ensemble Models and GAN Algorithm. In Proceedings of the International Conference on Circuit Power and Computing Technologies, ICCPCT 2023, Kollam, India, 10–11 August 2023; pp. 1664–1669. [Google Scholar] [CrossRef]
- Hwang, U.; Kim, S.-W.; Jung, D.; Kim, S.; Seo, S.W.; Seong, J.-K.; Yoon, S.; Alzheimer’s Disease Neuroimaging Initiative. Real-world prediction of preclinical Alzheimer’s disease with a deep generative model. Artif. Intell. Med. 2023, 144, 102654. [Google Scholar] [CrossRef] [PubMed]
- Yao, W.; Shen, Y.; Nicolls, F.; Wang, S.Q. Conditional Diffusion Model-Based Data Augmentation for Alzheimer’s Prediction. In Communications in Computer and Information Science; Springer Science and Business Media Deutschland GmbH: Berlin, Germany, 2023; pp. 33–46. [Google Scholar] [CrossRef]
- Yoon, D.; Myong, Y.; Kim, Y.G.; Sim, Y.; Cho, M.; Oh, B.-M.; Kim, S. Latent diffusion model-based MRI superresolution enhances mild cognitive impairment prognostication and Alzheimer’s disease classification. Neuroimage 2024, 296, 120663. [Google Scholar] [CrossRef] [PubMed]
- Tufail, H.; Ahad, A.; Puspitasari, I.; Shayea, I.; Coelho, P.J.; Pires, I.M. Deep Learning in Smart Healthcare: A GAN-based Approach for Imbalanced Alzheimer’s Disease Classification. Procedia Comput. Sci. 2024, 241, 146–153. [Google Scholar] [CrossRef]
- Ali, I.; Saleem, N.; Alhussein, M.; Zohra, B.; Aurangzeb, K.; Haq, Q.M.U. DeepCGAN: Early Alzheimer’s detection with deep convolutional generative adversarial networks. Front. Med. 2024, 11, 1443151. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.; Che, Y.; Sohankar, J.; Luo, J.; Li, B.; Su, Y.; Wu, T.; For the Alzheimer’s Disease Neuroimaging Initiative. Enhancing Amyloid PET Quantification: MRI-Guided Super-Resolution Using Latent Diffusion Models. Life 2024, 14, 1580. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Weng, Y.; Huang, Y.; Zhang, Y.; Dening, T.; Hosseini, A.A.; Xiao, W. A multi-view learning approach with diffusion model to synthesize FDG PET from MRI T1WI for diagnosis of Alzheimer’s disease. Alzheimer’s Dement. 2024, 21, e14421. [Google Scholar] [CrossRef] [PubMed]
- Dhinagar, N.J.; Thomopoulos, S.I.; Laltoo, E.; Thompson, P.M. Counterfactual MRI Generation with Denoising Diffusion Models for Interpretable Alzheimer’s Disease Effect Detection. In Proceedings of the 2024 46th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 15–19 July 2024; pp. 1–6. [Google Scholar] [CrossRef]
- Gajjar, P.; Garg, M.; Desai, S.; Chhinkaniwala, H.; Sanghvi, H.A.; Patel, R.H.; Gupta, S.; Pandya, A.S. An Empirical Analysis of Diffusion, Autoencoders, and Adversarial Deep Learning Models for Predicting Dementia Using High-Fidelity MRI. IEEE Access 2024, 12, 131231–131243. [Google Scholar] [CrossRef]
- Wong, P.C.; Abdullah, S.S.; Shapiai, M.I. Exceptional performance with minimal data using a generative adversarial network for alzheimer’s disease classification. Sci. Rep. 2024, 14, 17037. [Google Scholar] [CrossRef] [PubMed]
- Shou, Q.; Cen, S.; Chen, N.-K.; Ringman, J.M.; Wen, J.; Kim, H.; Wang, D.J.; Alzheimer’s Disease Neuroimaging Initiative. Diffusion model enables quantitative CBF analysis of Alzheimer’s Disease. medRxiv 2024. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.; Shin, J. Prognosis Prediction of Alzheimer’s Disease Based on Multi-Modal Diffusion Model. In Proceedings of the 2024 18th International Conference on Ubiquitous Information Management and Communication, IMCOM 2024, Kuala Lumpur, Malaysia, 3–5 January 2024. [Google Scholar] [CrossRef]
- Ching, W.P.; Abdullah, S.S.; Shapiai, M.I.; Islam, A.K.M.M. Performance Enhancement of Alzheimer’s Disease Diagnosis Using Generative Adversarial Network. J. Adv. Res. Appl. Sci. Eng. Technol. 2025, 45, 191–201. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, L. Early Diagnosis of Alzheimer’s Disease Using Dual GAN Model with Pyramid Attention Networks; Taylor and Francis Ltd.: Oxfordshire, UK, 2024. [Google Scholar] [CrossRef]
- Ou, Z.; Jiang, C.; Pan, Y.; Zhang, Y.; Cui, Z.; Shen, D. A Prior-information-guided Residual Diffusion Model for Multi-modal PET Synthesis from MRI. In Proceedings of the Thirty-Third International Joint Conference on Artificial Intelligence Main Track, Jeju-si, Republic of Korea, 3–9 August 2024. [Google Scholar]
- Oraby, S.; Emran, A.; El-Saghir, B.; Mohsen, S. Hybrid of DSR-GAN and CNN for Alzheimer disease detection based on MRI images. Sci. Rep. 2025, 15, 12727. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.; Ding, C.; Jing, C.; Liu, F.; Hung, K.; Pham, H.; Mahmud, M.; Lyu, Z.; Qiao, S.; Wang, S.; et al. BG-GAN: Generative AI Enable Representing Brain Structure-Function Connections for Alzheimer’s Disease. IEEE Trans. Consum. Electron. 2025. [Google Scholar] [CrossRef]
- Gavidia-Bovadilla, G.; Kanaan-Izquierdo, S.; Mataroa-Serrat, M.; Perera-Lluna, A. Early prediction of Alzheimer’s disease using null longitudinal model-based classifiers. PLoS ONE 2017, 12, e0168011. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Zhang, J.; Adeli, E.; Shen, D. Landmark-based deep multi-instance learning for brain disease diagnosis. Med. Image Anal. 2018, 43, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Radford, A.; Metz, L.; Chintala, S. Unsupervised Representation Learning with Deep Convolutional Generative Adversarial Networks. arXiv 2015, arXiv:1511.06434. [Google Scholar]
- Mirza, M.; Osindero, S. Conditional Generative Adversarial Nets. arXiv 2014, arXiv:1411.1784. [Google Scholar] [CrossRef]
- Kazeminia, S.; Baur, C.; Kuijper, A.; Van Ginneken, B.; Navab, N.; Albarqouni, S.; Mukhopadhyay, A. GANs for medical image analysis. Artif. Intell. Med. 2020, 109, 101938. [Google Scholar] [CrossRef] [PubMed]
- Karras, T.; Laine, S.; Aila, T. A Style-Based Generator Architecture for Generative Adversarial Networks. In Proceedings of the 2019 IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR), Long Beach, CA, USA, 15–20 June 2019; pp. 4396–4405. [Google Scholar] [CrossRef]
- Arjovsky, M.; Chintala, S.; Bottou, L. Wasserstein Generative Adversarial Networks. In Proceedings of the 34th International Conference on Machine Learning, Sydney, Australia, 6–11 August 2017. [Google Scholar]
- Song, Y.; Ermon, S. Generative Modeling by Estimating Gradients of the Data Distribution. arXiv 2019, arXiv:1907.05600. [Google Scholar]

| Modality | Type | What It Detects | Strengths | Limitations |
|---|---|---|---|---|
| MRI | Structural | Brain atrophy, hippocampal and cortical shrinkage | Non-invasive, high-resolution, and widely available. | Limited functional insight, relatively expensive |
| fMRI | Functional | Brain activity and connectivity between regions. | Real-time brain function | Sensitive to motion and requires complex analysis |
| PET | Molecular /Functional | Amyloid plaques, tau proteins, glucose metabolism | Identifies biochemical changes early, aids in staging | High cost, uses radioactive tracers |
| FDG-PET | Metabolic Imaging | Glucose metabolism, hypometabolic regions in AD | Detects early metabolic dysfunction in AD-affected areas | Radiation exposure, lower spatial resolution than MRI |
| CT | Structural | Structural abnormalities, bleeding or lesions | Fast, accessible in emergency settings | Lower soft tissue contrast than MRI, less specific for AD |
| DTI | Microstructural | White matter integrity, neural pathway disruptions | Subtle white matter changes, supports early diagnosis | Requires complex processing, susceptible to motion and noise. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alam, M.M.; Latifi, S. Early Detection of Alzheimer’s Disease Using Generative Models: A Review of GANs and Diffusion Models in Medical Imaging. Algorithms 2025, 18, 434. https://doi.org/10.3390/a18070434
Alam MM, Latifi S. Early Detection of Alzheimer’s Disease Using Generative Models: A Review of GANs and Diffusion Models in Medical Imaging. Algorithms. 2025; 18(7):434. https://doi.org/10.3390/a18070434
Chicago/Turabian StyleAlam, Md Minul, and Shahram Latifi. 2025. "Early Detection of Alzheimer’s Disease Using Generative Models: A Review of GANs and Diffusion Models in Medical Imaging" Algorithms 18, no. 7: 434. https://doi.org/10.3390/a18070434
APA StyleAlam, M. M., & Latifi, S. (2025). Early Detection of Alzheimer’s Disease Using Generative Models: A Review of GANs and Diffusion Models in Medical Imaging. Algorithms, 18(7), 434. https://doi.org/10.3390/a18070434