

FEA Comparison of the Mechanical Behavior of Three Dental Crown Materials: Enamel, Ceramic, and Zirconia


Abstract
1. Introduction
2. Materials and Methods
2.1. CAD Model
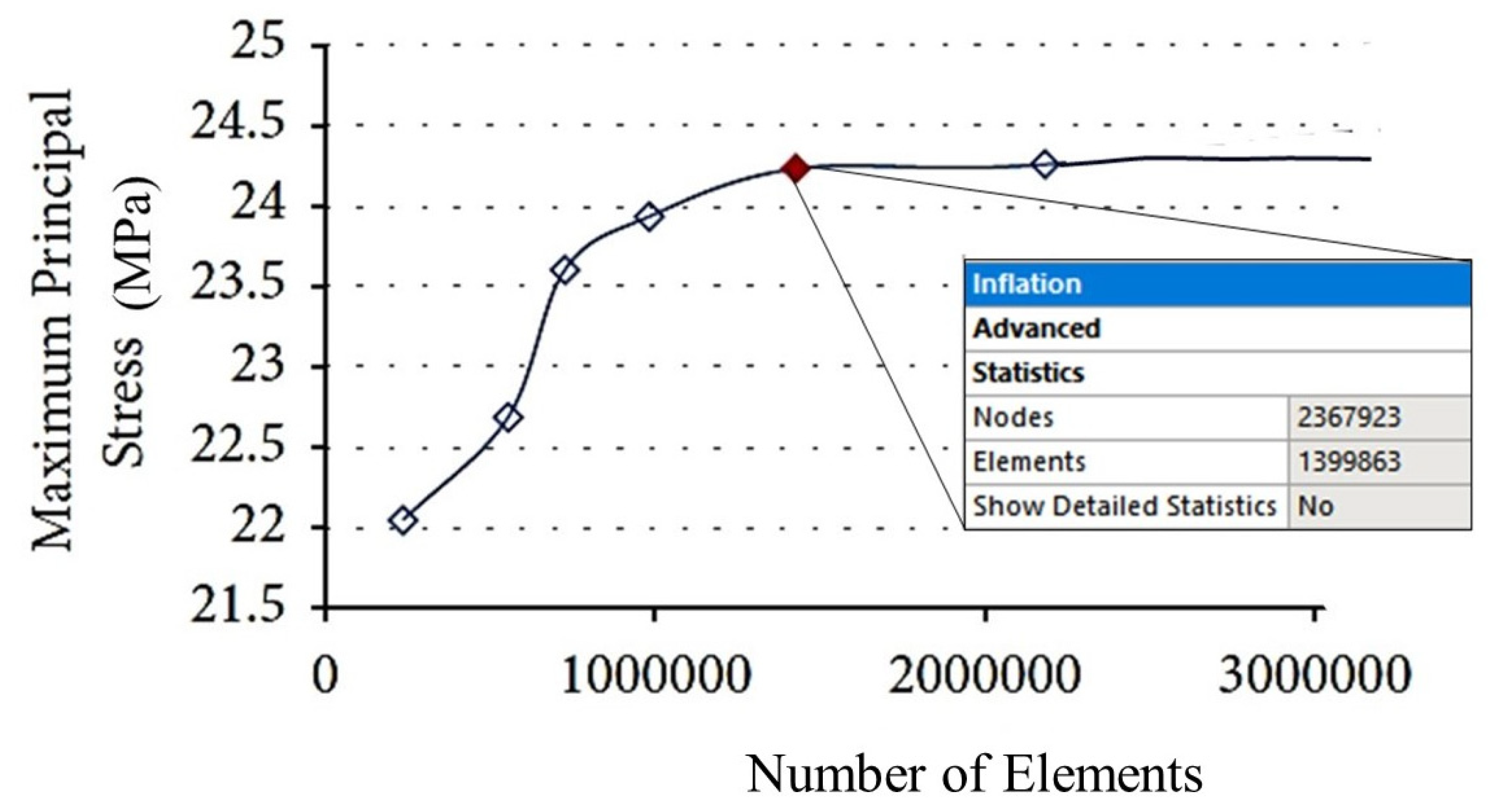
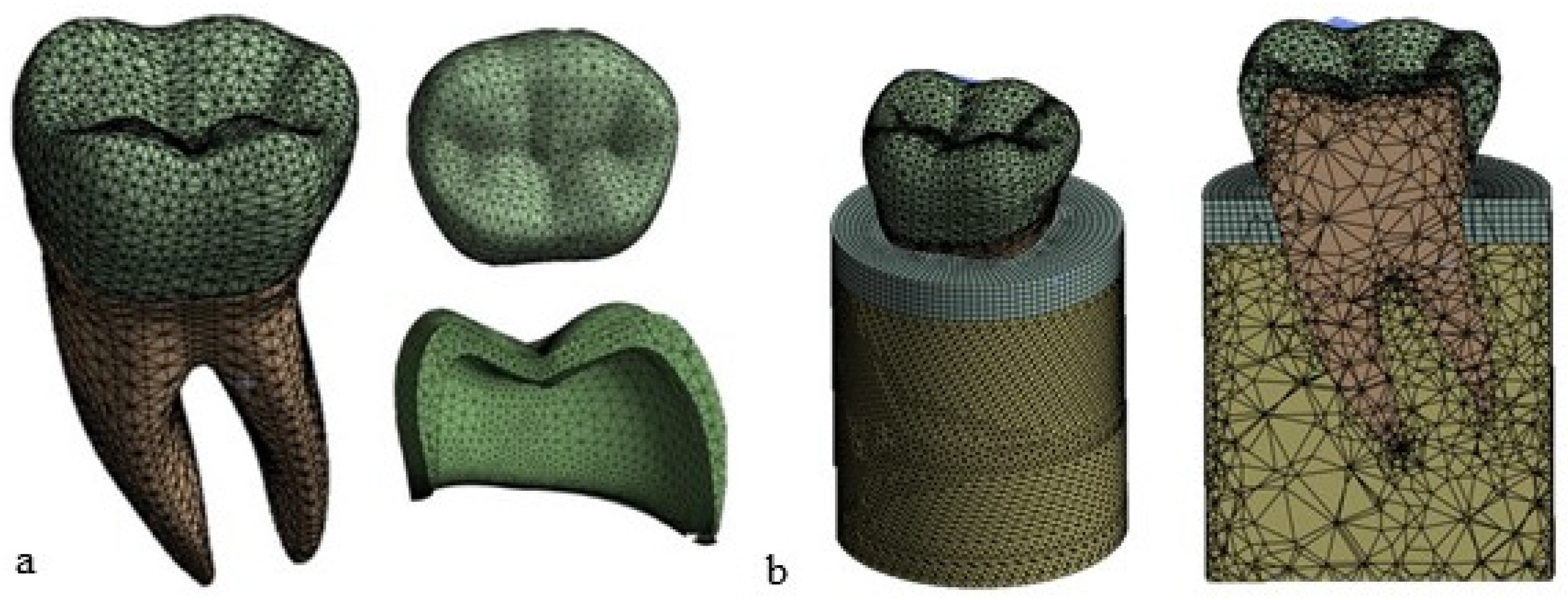
2.2. Finite Element Modeling
2.3. Material Properties
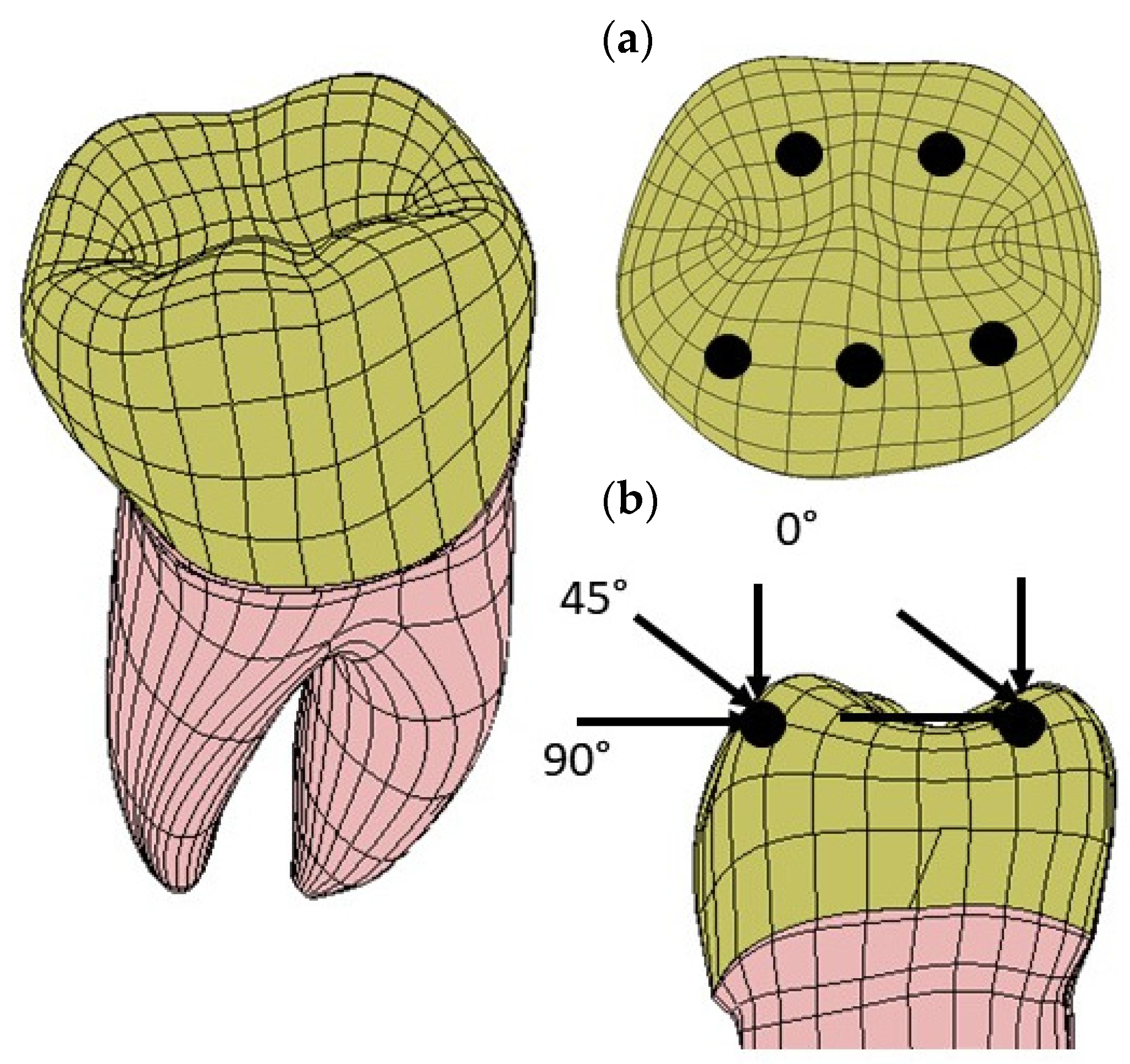
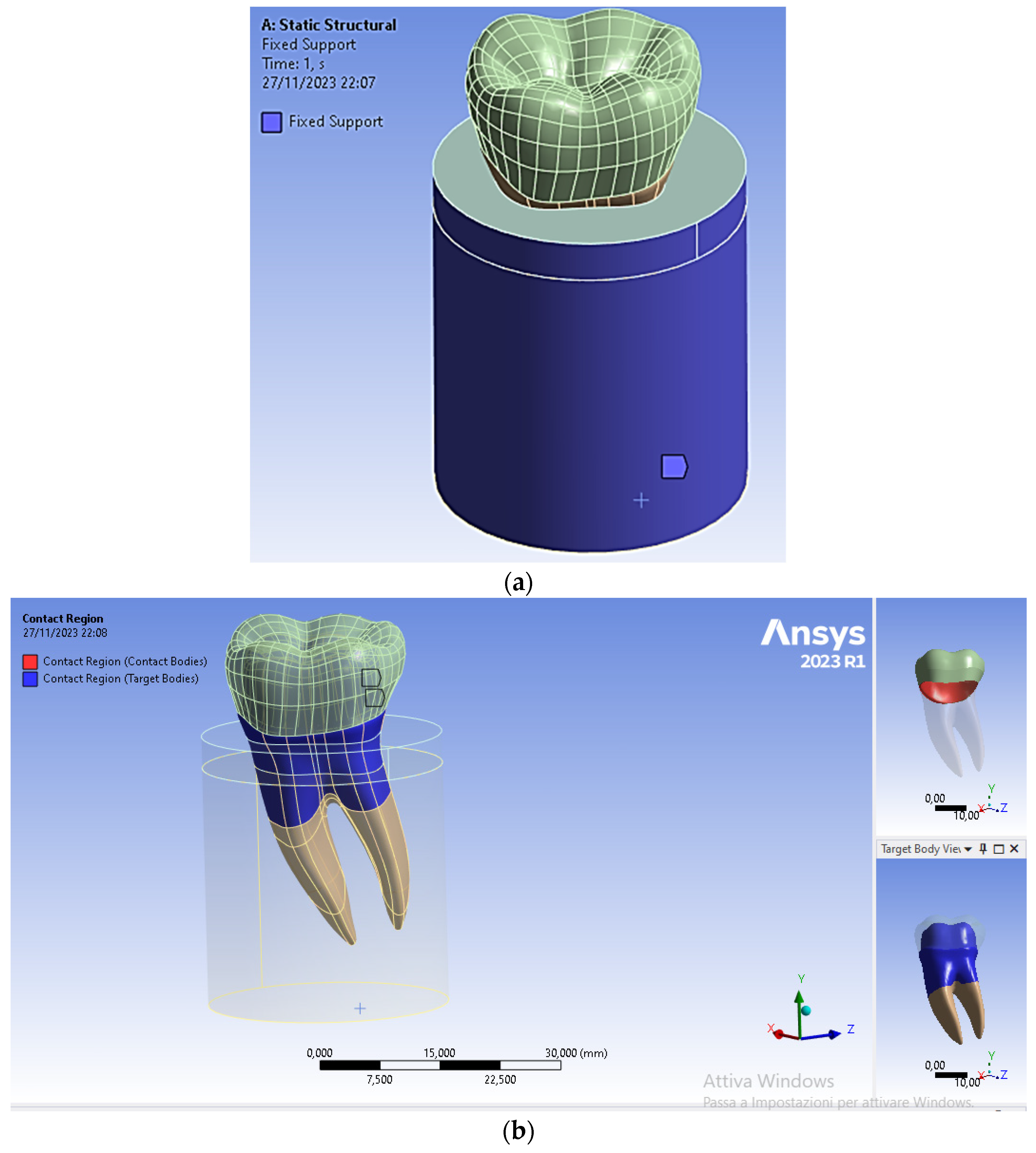
2.4. Loads and Constraints
2.5. Kinematic Constraint Conditions
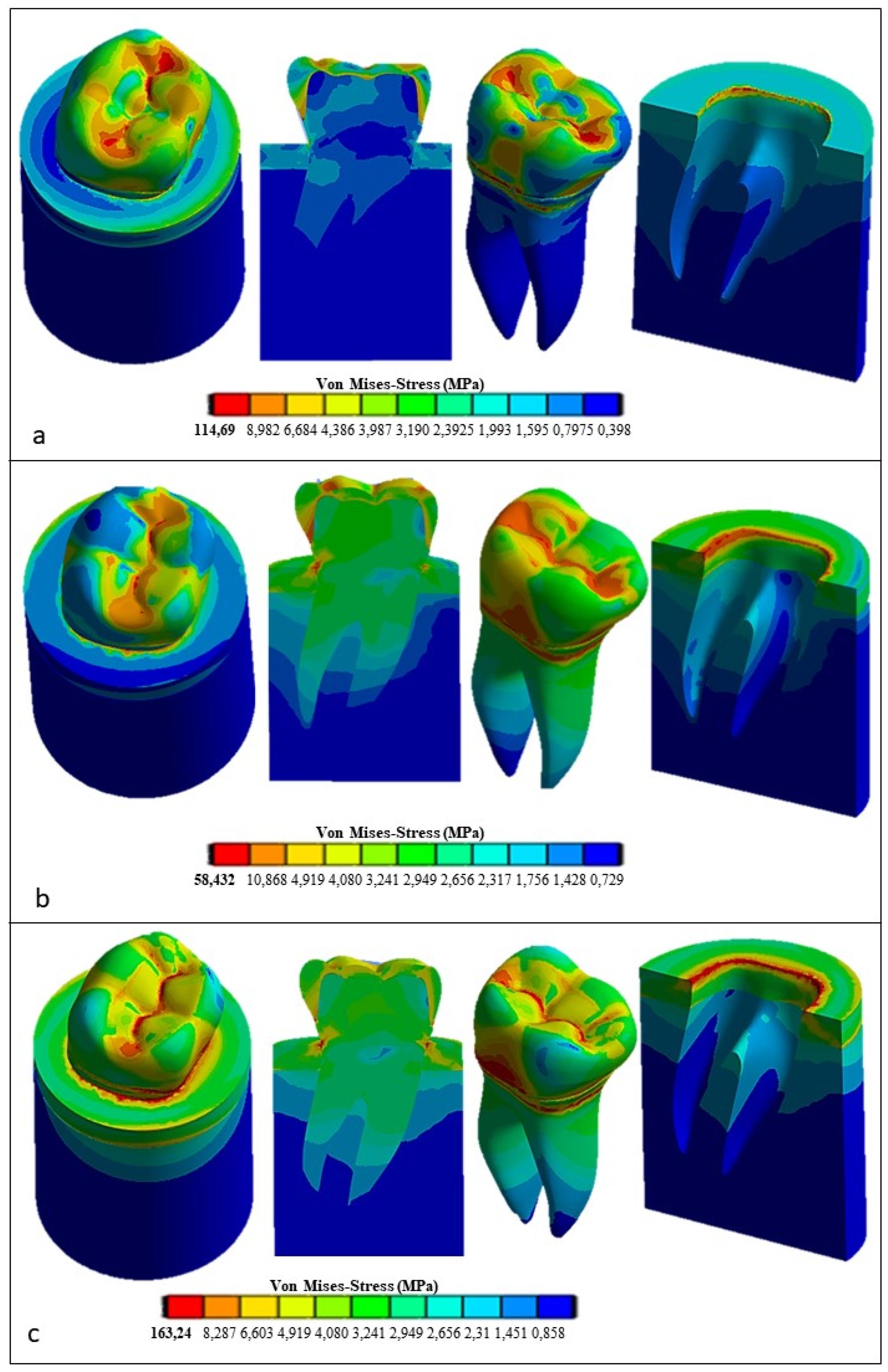
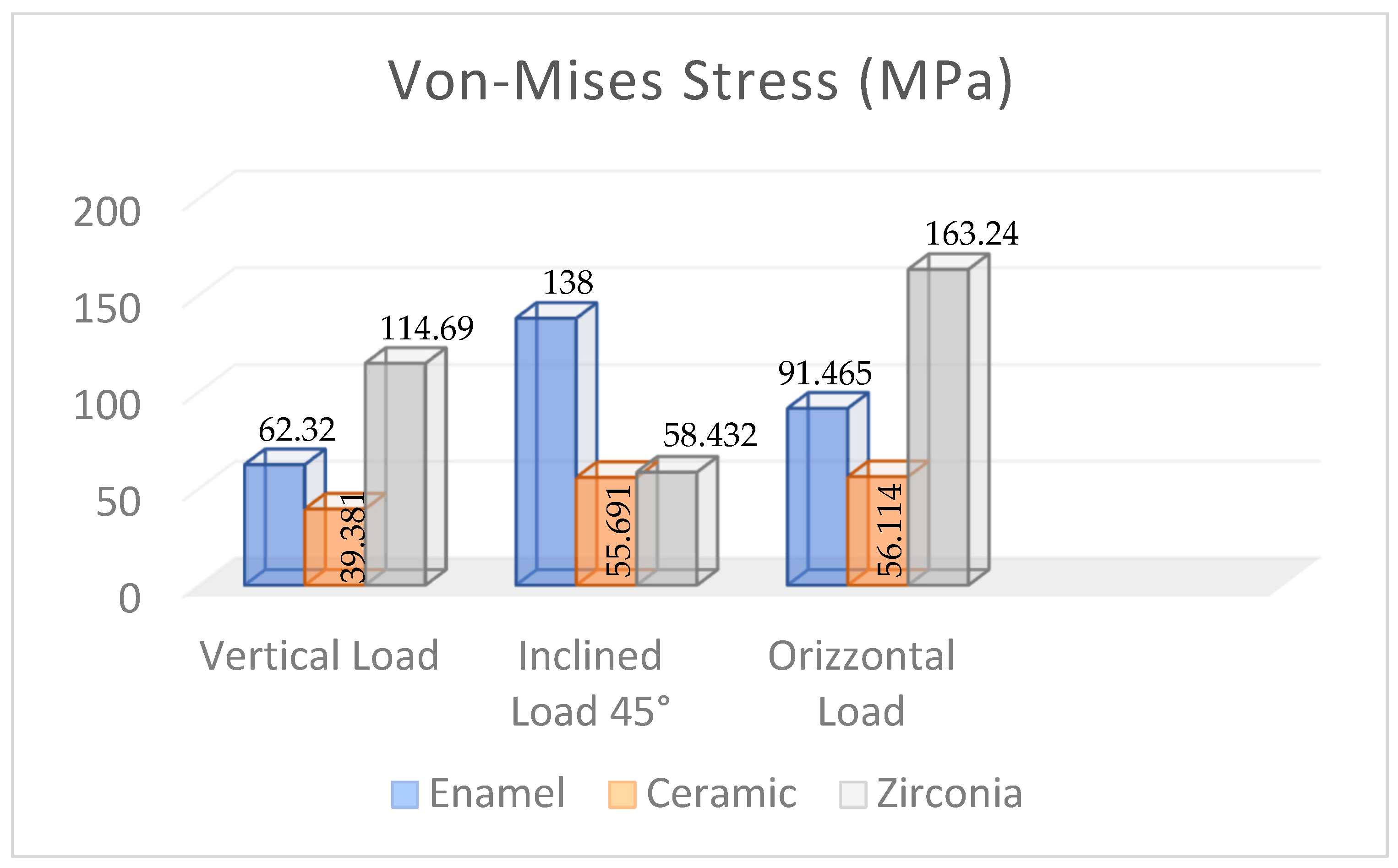
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alhasanyah, A.; Vaidyanathan, T.K.; Flinton, R.J. Effect of core thickness differences on post-fatigue indentation fracture resistance of veneered zirconia crowns. J. Prosthodont. 2013, 22, 383–390. [Google Scholar] [CrossRef]
- Christensen, G.J. Porcelain-fused-to-metal versus zirconia based ceramic restorations. J. Am. Dent. Assoc. 2009, 140, 1036–1039. [Google Scholar] [CrossRef] [PubMed]
- Kharouf, N.; Mancino, D.; Naji-Amrani, A.; Eid, A.; Haikel, Y.; Hemmerle, J. Effectiveness of etching by three acids on the morphological and chemical features of dentin tissue. J. Contemp. Dent. Pract. 2019, 20, 915–919. [Google Scholar]
- Ogata, M.; Okuda, M.; Nakajima, M.; Pereira, P.N.; Sano, H.; Tagami, J. Influence of the direction of tubules on bond strength to dentin. Oper. Dent. 2001, 26, 27–35. [Google Scholar]
- Kinney, J.H.; Balooch, M.; Marshall, S.J.; Marshall, W.J.R.; Weih, T.P. Hardness and Young’s modulus of human peritubular and intertubular dentine. Arch. Oral Biol. 1996, 41, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Wentrup-Byrne, E.; Armstrong, C.A.; Armstrong, R.S.; Collins, M. Fourier transform Raman microscopic mapping of the molecular components in a human tooth. J. Raman Spectrosc. 1997, 28, 151–158. [Google Scholar] [CrossRef]
- Huo, B.; Zheng, Q.S. Effect of dentin tubules to the mechanical properties of dentin. Part I: Stress–strain relations and strength criterion. Acta Mech. Sin. (Engl. Ser.) 1999, 15, 355–364. [Google Scholar]
- Lertchirakarn, V.; Palamara, E.A.; Messer, H.H. Anisotropy of tensile strength of root dentin. J. Dent. Res. 2001, 80, 453–456. [Google Scholar] [CrossRef] [PubMed]
- Huo, B.; Zheng, Q.S.; Zhang, Q.; Wang, J.D. Effect of dentin tubules to the mechanical properties of dentin. Part II: Experimental study. Acta Mech. Sin. (Engl. Ser.) 2000, 16, 75–82. [Google Scholar]
- Wang, R.Z.; Weiner, S. Strain–structure relations in human teeth using moiré fringes. J. Biomech. 1998, 31, 135–141. [Google Scholar] [CrossRef]
- Kinney, J.H.; Balooch, M.; Marshall, G.W.; Marshall, S.J. A micromechanics model of the elastic properties of human dentine. Arch. Oral Biol. 1999, 44, 813–822. [Google Scholar] [CrossRef]
- Pol-Christian, W.P.; Kalk, W. A systematic review of ceramic inlays in posterior teeth: An update. Int. J. Prosthodont. 2011, 24, 566–575. [Google Scholar]
- Asgar, K. Casting metals in dentistry: Past present future. Adv. Dent. Res. 1988, 23, 3–43. [Google Scholar] [CrossRef]
- Jiang, L.; Zhao, Y.-Q.; Zhang, J.-C.; Liao, Y.-M.; Li, W. Zhonghua kou qiang yi xue za zhi = Zhonghua kouqiang yixue zazhi. Chin. J. Stomatol. 2010, 45, 376–380. [Google Scholar]
- Kosmac, T.; Oblak, C.; Jevnikar, P.; Funduk, N.; Marion, L. The effect of surface grinding and sandblasting on flexural strength and reliability of Y-TZP zirconia ceramic. Dent. Mater. 1999, 15, 426–433. [Google Scholar] [CrossRef]
- Blatz, M.B.; Sadan, A.; Arch, G.H., Jr.; Lang, B.R. In vitro evaluation of long-term bonding of ProceraAllCeram alumina restorations with a modified resin luting agent. J. Prosthet. Dent. 2003, 89, 381–387. [Google Scholar] [CrossRef]
- Mori, T.; Tanaka, K. Average stress in matrix and average elastic energy of materials with misfitting inclusions. Acta Metall. 1973, 21, 571–574. [Google Scholar] [CrossRef]
- Gommers, B.; Verpoest, I.; Van Houtte, P. The Mori-Tanaka method applied to textile composite materials. Acta Mater. 1998, 46, 2223–2235. [Google Scholar] [CrossRef]
- Grzebieluch, W.; Będziński, R.; Czapliński, T.; Kaczmarek, U. The mechanical properties of human dentin for 3-D finite element modeling: Numerical and analytical evaluation. Adv. Clin. Exp. Med. 2017, 26, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Shinno, Y.; Ishimoto, T.; Saito, M.; Uemura, R.; Arino, M.; Marumo, K.; Nakano, T.; Hayashi, M. Comprehensive analyses of how tubule occlusion and advanced glycation end-products diminish strength of aged dentin. Sci. Rep. 2016, 6, 19849. [Google Scholar] [CrossRef]
- Reddy, M.K.; Vandana, K.L. Three-dimensional finite element analysis of stress in the periodontium. J. Int. Acad. Periodontol. 2005, 7, 102–107. [Google Scholar]
- Bramanti, E.; Cervino, G.; Lauritano, F.; Fiorillo, L.; D’amico, C.; Sambataro, S.; Denaro, D.; Famà, F.; Ierardo, G.; Polimeni, A.; et al. FEM and Von Mises analysis on prosthetic crowns structural elements: Evaluation of different applied materials. Sci. World J. 2017, 2017, 1029574. [Google Scholar] [CrossRef] [PubMed]
- Kanat, B.; Cömlekoğlu, E.M.; Dündar-Çömlekoğlu, M.; Hakan Sen, B.; Özcan, M.; Güngör, M.A. Effect of various veneering techniques on mechanical strength of computer-controlled zirconia framework designs. J. Prosthodont. 2014, 23, 445–455. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.; Lee, M.-J.; Kang, I.; Oh, S. Evaluation of Biomechanical Stability of Teeth Tissue According to Crown Materials: A Three-Dimensional Finite Element Analysis. Materials 2023, 16, 4756. [Google Scholar] [CrossRef]
- Shahmoradi, M.; Wan, B.; Zhang, Z.; Wilson, T.; Swain, M.; Li, Q. Monolithic crowns fracture analysis: The effect of material properties, cusp angle and crown thickness. Dent. Mater. 2020, 36, 1038–1051. [Google Scholar] [CrossRef]
- Ha, S.R. Biomechanical three-dimensional finite element analysis of monolithic zirconia crown with different cement type. J. Adv. Prosthodont. 2015, 7, 475–483. [Google Scholar] [CrossRef]
- Di Pietro, N.; Ceddia, M.; Romasco, T.; De Bortoli Junior, N.; Mello, B.F.; Tumedei, M.; Specchiulli, A.; Piattelli, A.; Trentadue, B. Finite element analysis (FEA) of the stress and strain distribution in cone-morse implant–abutment connection implants placed equicrestally and subcrestally. Appl. Sci. 2023, 13, 8147. [Google Scholar] [CrossRef]
- Ceddia, M.; Comuzzi, L.; Di Pietro, N.; Romasco, T.; Specchiulli, A.; Piattelli, A.; Trentadue, B. Finite Element Analysis (FEA) for the evaluation of retention in a Conometric Connection for Implant and Prosthesis. Osteology 2023, 3, 140–156. [Google Scholar] [CrossRef]
- Li, P.; Shen, L.; Li, J.; Liang, R.; Tian, W.; Tang, W. Optimal design of an individual endoprosthesis for the reconstruction of extensive mandibular defects with finite element analysis. J. Cranio-Maxillofac. Surg. 2014, 42, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Van Eijden, T.M. Biomechanics of the mandible. Crit. Rev. Oral Biol. Med. 2000, 11, 123–136. [Google Scholar] [CrossRef]
- Cansiz, E.; Dogru, S.C.; Arslan, Y.Z. Evaluation of different fixation materials for mandibular condyle fractures. In Proceedings of the XIX International Conference on Mechanics in Medicine and Biology, Bologna, Italy, 3–5 September 2014. [Google Scholar]
- Wirtz, D.C.; Schiffers, N.; Pandorf, T.; Radermacher, K.; Weichert, D.; Forst, R. Critical evaluation of known bone material properties to realize anisotropic FE-simulation of the proximal femur. J. Biomech. 2000, 33, 1325–1330. [Google Scholar] [CrossRef]
- Schileo, E.; Dall’Ara, E.; Taddei, F.; Malandrino, A.; Schotkamp, T.; Baleani, M.; Viceconti, M. An accurate estimation of bone density improves the accuracy of subject-specific finite element models. J. Biomech. 2008, 41, 2483–2491. [Google Scholar] [CrossRef]
- Helgason, B.; Perilli, E.; Schileo, E.; Taddei, F.; Brynjólfsson, S.; Viceconti, M. Mathematical relationships between bone density and mechanical properties: A literature review. Clin. Biomech. 2008, 23, 135–146. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, A.M.; Williams, J.L.; Spencer, P. Anisotropic elasticity of cortical and cancellous bone in the posterior mandible increases peri-implant stress and strain under oblique loading. Clin. Oral. Implant. Res. 2001, 12, 648–657. [Google Scholar] [CrossRef] [PubMed]
- Silva, G.C.; Cornacchia, T.M.; De Magalhaes, C.S.; Bueno, A.C.; Moreira, A.N. Biomechanical evaluation of screw- and cement-retained implant-supported prostheses: A nonlinear finite element analysis. J. Prosthet. Dent. 2014, 112, 1479–1488. [Google Scholar] [CrossRef] [PubMed]
- Miura, J.; Maeda, Y.; Nakai, H.; Zako, M. Multiscale analysis of stress distribution in teeth under applied forces. Dent. Mater. 2009, 25, 67–73. [Google Scholar] [CrossRef]
- Munari, L.S.; Cornacchia, T.P.; Moreira, A.N.; Gonçalves, J.B.; Casas, E.B.D.L.; Magalhães, C.S. Stress distribution in a premolar 3D model with anisotropic and isotropic enamel. Med. Biol. Eng. Comput. 2015, 53, 751–758. [Google Scholar] [CrossRef]
- Su, K.C.; Chuang, S.F.; Ng, E.Y.K.; Chang, C.H. An investigation of dentinal fluid flow in dental pulp during food mastication: Simulation of fluid–structure interaction. Biomech. Model. Mechanobiol. 2014, 13, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.-R.; Kim, S.-H.; Lee, J.-B.; Han, J.-S.; Yeo, I.-S.; Yoo, S.-H.; Kim, H.-K. Biomechanical three dimensional finite element analysis of monolithic zirconia crown with different cement thickness. Ceram. Int. 2016, 42, 14928–14936. [Google Scholar] [CrossRef]
- Rocha, E.P.; Anchieta, R.B.; Almeida, E.O.; Freitas, A.C.F., Jr.; Martini, A.P.; Sotto-Maior, B.S.; Luersen, M.A.; Ko, C.C. Zirconia-based dental crown to support a removable partial denture: A three-dimensional finite element analysis using contact elements and micro-CT data. Comput. Methods Biomech. Biomed. Eng. 2015, 18, 1744–1752. [Google Scholar] [CrossRef]
- Jithendra Babu, P.; Alla, R.K.; Alluri, V.R.; Datla, S.R.; Konakanchi, A. Dental ceramics: Part I—An overview of composition, structure and properties. Am. J. Mater. Eng. Technol. 2015, 3, 13–18. [Google Scholar]
- Dejak, B.; Młotkowski, A.; Langot, C. Three-dimensional finite element analysis of molars with thin-walled prosthetic crowns made of various materials. Dent. Mater. 2012, 28, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E.; Qu, Z.; Bidez, M.W. Mechanical properties of trabecular bone in the human mandible: Implications for dental implant treatment planning and surgical placement. J. Oral Maxillofac. Surg. 1999, 57, 700–706; discussion 706–708. [Google Scholar] [CrossRef]
- Morgan, E.F.; Unnikrisnan, G.U.; Hussein, A.I. Bone mechanical properties in healthy and diseased states. Annu. Rev. Biomed. Eng. 2018, 20, 119–143. [Google Scholar] [CrossRef]
- Shimizu, K.; Oka, M.; Kumar, P.; Kotoura, Y.; Yamamuro, T.; Makinouchi, K.; Nakamura, T. Time-dependent changes in the mechanical properties of zirconia ceramic. J. Biomed. Mater. Res. 1993, 27, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Luthardt, R.G.; Holzhuter, M.; Sandkuhl, O.; Herold, V.; Schnapp, J.D.; Kuhlisch, E.; Walter, M. Reliability and properties of ground Y-TZP-zirconia ceramics. J. Dent. Res. 2002, 81, 487–491. [Google Scholar] [CrossRef]
- Blatz, M.B.; Sadan, A.; Martin, J.; Lang, B. In vitro evaluation of shear bond strengths of resin to densely sintered high-purity zirconium-oxide ceramic after long-term storage and thermal cycling. J. Prosthet. Dent. 2004, 91, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Omur, C.; Gozneli, T.R.; Ozkan, Y. Effects of silica coating by physical vapor deposition and repeated firing on the low temperature degradation and flexural strength of a zirconia ceramic. J. Prosthodont. 2019, 28, e186–e194. [Google Scholar]
- Goff, J.P.; Hayes, W.; Hull, S.; Hutchings, M.T.; Clausen, K.N. Defect structure of yttria stabilized zirconia and its influence on the ionic conductivity at elevated temperatures. Phys. Rev. B 1999, 59, 14202–14218. [Google Scholar] [CrossRef]
- Alsadon, O.; Patrick, D.; Johnson, A.; Pollington, S.; Wood, D. Fracture resistance of zirconia-composite veneered crowns in comparison with zirconia-porcelain crowns. Dent. Mater. J. 2017, 36, 289–295. [Google Scholar] [CrossRef]
- Sailer, B.; Pjetursson, E.; Zwahlen, Z.; Hammerle, C.H. A systematic review of the survival and complication rates of all ceramic and metal–ceramic reconstructions after an observation period of at least 3 years. Part II: Fixed dental prostheses. Clin. Oral Implant. Res. 2007, 18, 86–96. [Google Scholar] [CrossRef]
- Larsson, C.; Von Steyern, P.V. Five-year follow-up of implant-supported Y-TZP and ZTA fixed dental prostheses. A randomized, prospective clinical trial comparing two different material systems. Int. J. Prosthodont. 2010, 23, 555–561. [Google Scholar]
- Schwarz, S.; Schröder, C.; Hassel, A.; Bömicke, W.; Rammelsberg, P. Survival and chipping of zirconia based and metal–ceramic implant supported single crowns. Clin. Implant. Dent. Relat. Res. 2012, 14, e119–e125. [Google Scholar] [CrossRef]
- Moraguez, O.D.; Wiskott, H.A.; Scherrer, S.S. Three-to nine-year survival estimates and fracture mechanisms of zirconia-and alumina-based restorations using standardized criteria to distinguish the severity of ceramic fractures. Clin. Oral Investig. 2015, 19, 2295–2307. [Google Scholar] [CrossRef]
- Güncü, M.B.; Cakan, U.; Muhtarogullari, M.; Canay, S. Zirconia-based crowns up to 5 years in function: A retrospective clinical study and evaluation of prosthetic restorations and failures. Int. J. Prosthodont. 2015, 28, 152–157. [Google Scholar] [CrossRef]
- Lin, M.T.; Sy-Munoz, J.; Munoz, C.A.; Goodacre, C.J.; Naylor, W.P. The effect of tooth preparation form on the fit of Procera copings. Int. J. Prosthodont. 1998, 11, 580–590. [Google Scholar]
- Reich, S.; Wichmann, M.; Nkenke, E.; Proeschel, P. Clinical fit of all-ceramic three-unit fixed partial dentures, generated with three different CAD/CAM systems. Eur. J. Oral Sci. 2005, 113, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Pilo, R.; Cardash, H.S. In vivo retrospective study of cement thickness under crowns. J. Prosthet. Dent. 1998, 79, 621–625. [Google Scholar] [CrossRef] [PubMed]
- Aboushelib, M.N.; De Jager, N.; Kleverlaan, C.J.; Feilzer, A.J. Effect of loading method on the fracture mechanics of two layered all-ceramic restorative systems. Dent. Mater. 2007, 23, 952–959. [Google Scholar] [CrossRef] [PubMed]
- Casson, A.M.; Glyn Jones, J.C.; Youngson, C.C.; Wood, D.J. The effect of luting media on the fracture resistance of a flame sprayed all-ceramic crown. J. Dent. 2001, 29, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Sorrentino, R.; Triulzio, C.; Tricarico, M.G.; Bonadeo, G.; Gherlone, E.F.; Ferrari, M. In vitro analysis of the fracture resistance of CAD-CAM monolithic zirconia molar crowns with different occlusal thickness. J. Mech. Behav. Biomed. Mater. 2016, 61, 328–333. [Google Scholar] [CrossRef]
- Magne, P. Efficient 3D finite element analysis of dental restorative procedures using micro-CT data. Dent. Mater. 2007, 23, 539–548. [Google Scholar] [CrossRef] [PubMed]
- Himmlova, L.; Dostalova, T.; Kacovsky, A.; Konvickova, S. Influence of implant length and diameter on stress distribution: A finite element analysis. J. Prosthet. Dent. 2004, 91, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Geng, J.P.; Tan, K.B.; Liu, G.R. Application of finite element analysis in implant dentistry: A review of the literature. J. Prosthet. Dent. 2001, 85, 585–598. [Google Scholar] [CrossRef] [PubMed]
- Heydecke, G.; Butz, F.; Binder, J.; Strub, J. Material characteristics of a novel shrinkage-free ZrSiO4 ceramic for the fabrication of posterior crowns. Dent. Mater. 2007, 23, 785–791. [Google Scholar] [CrossRef]
- Fathy, S.M.; Anwar, M.I.E.; Fallal, A.A.E.; El-Negoly, S.A. Three-dimensional finite element analysis of lower molar tooth restored with fully milled and layered zirconia crowns. J. Dent. Health Oral Disord. Ther. 2014, 1, 89–95. [Google Scholar] [CrossRef][Green Version]
- Rocha, E.P.; Anchieta, R.B.; Freitas, A.C., Jr.; de Almeida, E.O.; Cattaneo, P.M.; Ko, C.C. Mechanical behavior of ceramic veneer in zirconia-based restorations: A 3-dimensional finite element analysis using microcomputed tomography data. J. Prosthet. Dent. 2011, 105, 14–20. [Google Scholar] [CrossRef]
- Taskonak, B.; Yan, J.; Mecholsky, J.J., Jr.; Sertqoz, A.; Koçak, A. Fractographic analyses of zirconia-based fixed partial dentures. Dent. Mater. 2008, 24, 1077–1082. [Google Scholar] [CrossRef]
- De Jager, N.; Pallav, P.; Feilzer, A.J. The apparent increase of the Young’s modulus in thin cement layers. Dent. Mater. 2004, 20, 457–462. [Google Scholar] [CrossRef]
- Son, Y.H.; Han, C.H.; Kim, S. Influence of internal-gap width and cement type on the retentive force of zirconia copings in pullout testing. J. Dent. 2012, 40, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Toms, S.R.; Eberhardt, A.W. A nonlinear finite element analysis of the periodontal ligament under orthodontic tooth loading. Am. J. Orthod. Dentofac. Orthop. 2003, 123, 657–665. [Google Scholar] [CrossRef] [PubMed]
- Ovy, E.G.; Romanyk, D.L.; Flores Mir, C.; Westover, L. Modelling and evaluating periodontal ligament mechanical behaviour and properties: A scoping review of current approaches and limitations. Orthod. Craniofac. Res. 2022, 25, 199–211. [Google Scholar] [CrossRef]
- Karimi, A.; Razaghi, R.; Biglari, H.; Rahmati, S.M.; Sandbothe, A.; Hasani, M. Finite element modeling of the periodontal ligament under a realistic kinetic loading of the jaw system. Saudi Dent. J. 2020, 32, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, P.M.; Cornelis, M.A. Orthodontic tooth movement studied by finite element analysis: An update. What can we learn from these simulations? Curr. Osteoporos. Rep. 2021, 19, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Field, C.; Ichim, I.; Swain, M.V.; Chan, E.; Darendeliler, M.A.; Li, W.; Li, Q. Mechanical responses to orthodontic loading: A 3-dimensional finite element multi-tooth model. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 174–181. [Google Scholar] [CrossRef]
- Viecilli, R.F.; Katona, T.R.; Chen, J.; Hartsfield, J.K.; Roberts, W.E. Three-dimensional mechanical environment of orthodontic tooth movement and root resorption. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 791.e11–791.e26. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Ez (GPa) | Ey (GPa) | Ex (GPa) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Cortical bone | 17.9 | 12.5 | 26.6 | 0.28 | 0.18 | 0.31 | 7.1 | 4.5 | 5.3 |
| Cancellous bone | 0.21 | 1.148 | 1.148 | 0.055 | 0.322 | 0.055 | 0.068 | 0.434 | 0.068 |
| Material | Ez (GPa) | Ey (GPa) | Ex (GPa) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Dentin | 17.07 | 5.61 | 5.61 | 0.30 | 0.33 | 0.30 | 1.7 | 6 | 1.7 |
| Material | E (GPa) | |
|---|---|---|
| Enamel | 72.7 | 0.30 |
| Material | E (GPa) | |
|---|---|---|
| Zirconia | 205 | 0.22 |
| Porcelain | 68.9 | 0.28 |
| Material | Tensile Strength (MPa) | Compressive Strength (MPa) |
|---|---|---|
| Enamel | 11.5 | 384.0 |
| Dentin | 105.5 | 297.0 |
| Zirconia | 745.0 | 2000.0 |
| Ceramic | 330 | |
| Cortical bone | 135 | 205 |
| Trabecular bone | 10.44 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ceddia, M.; Lamberti, L.; Trentadue, B. FEA Comparison of the Mechanical Behavior of Three Dental Crown Materials: Enamel, Ceramic, and Zirconia. Materials 2024, 17, 673. https://doi.org/10.3390/ma17030673
Ceddia M, Lamberti L, Trentadue B. FEA Comparison of the Mechanical Behavior of Three Dental Crown Materials: Enamel, Ceramic, and Zirconia. Materials. 2024; 17(3):673. https://doi.org/10.3390/ma17030673
Chicago/Turabian StyleCeddia, Mario, Luciano Lamberti, and Bartolomeo Trentadue. 2024. "FEA Comparison of the Mechanical Behavior of Three Dental Crown Materials: Enamel, Ceramic, and Zirconia" Materials 17, no. 3: 673. https://doi.org/10.3390/ma17030673
APA StyleCeddia, M., Lamberti, L., & Trentadue, B. (2024). FEA Comparison of the Mechanical Behavior of Three Dental Crown Materials: Enamel, Ceramic, and Zirconia. Materials, 17(3), 673. https://doi.org/10.3390/ma17030673