Long-Term Results of a Second-Generation, Small-Diameter, Metal-On-Metal Bearing in Primary Total Hip Arthroplasty at 14-Year Follow-Up

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
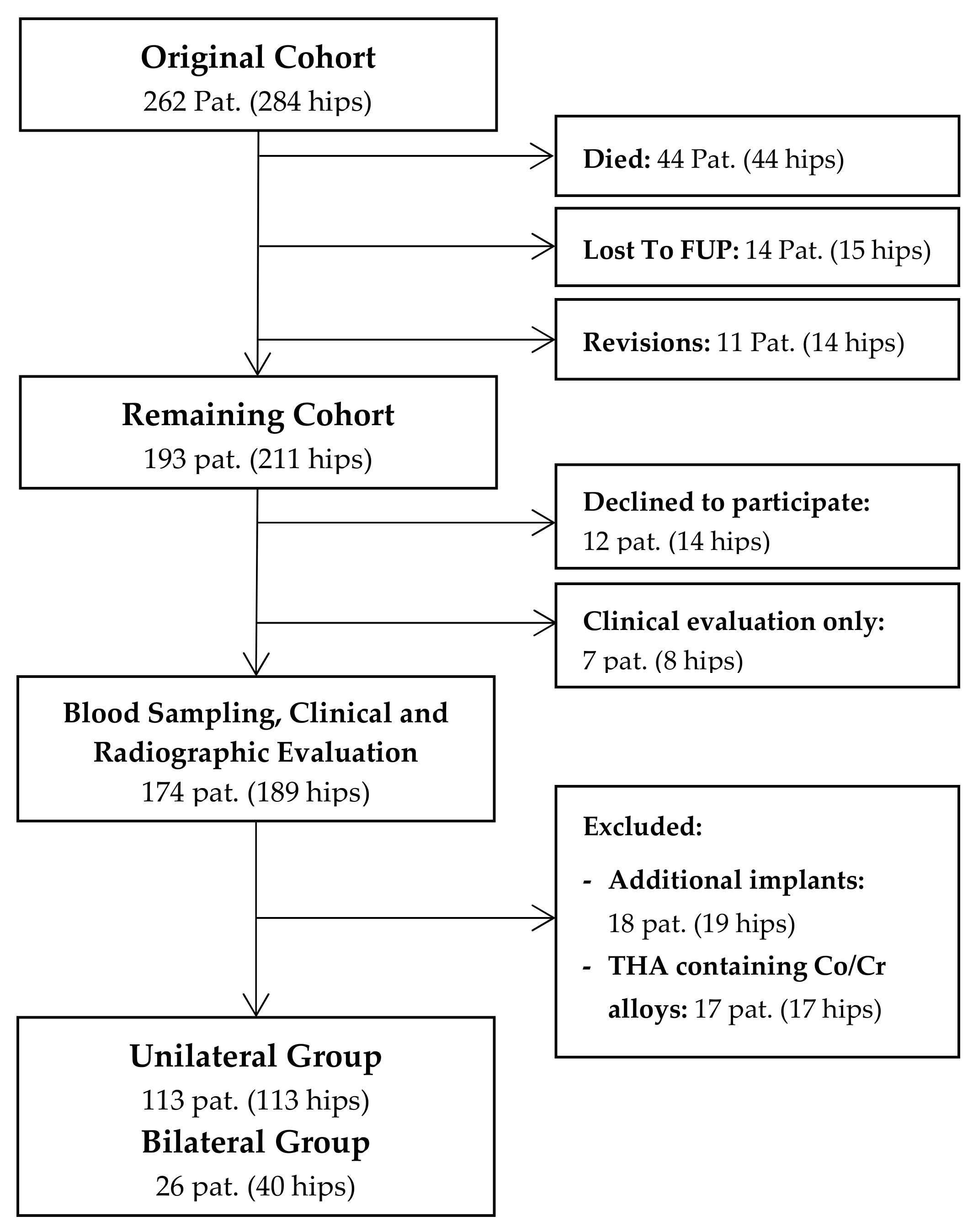
2.1. Study Design and Patients
2.2. Clinical and Radiographic Follow-up
2.3. Metal Ion Analysis
2.4. Statistical Methods
3. Results
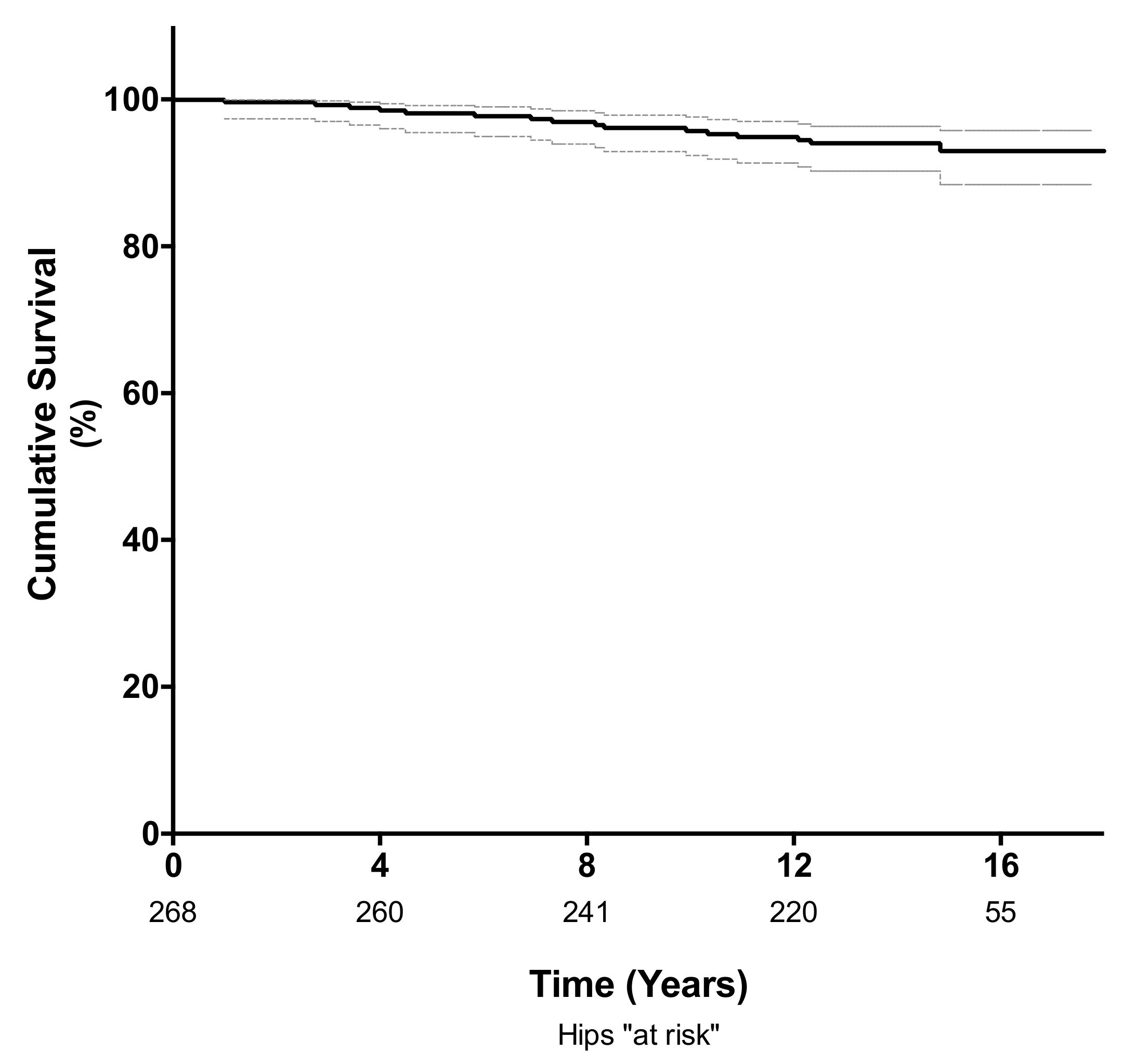
3.1. Survival Analysis
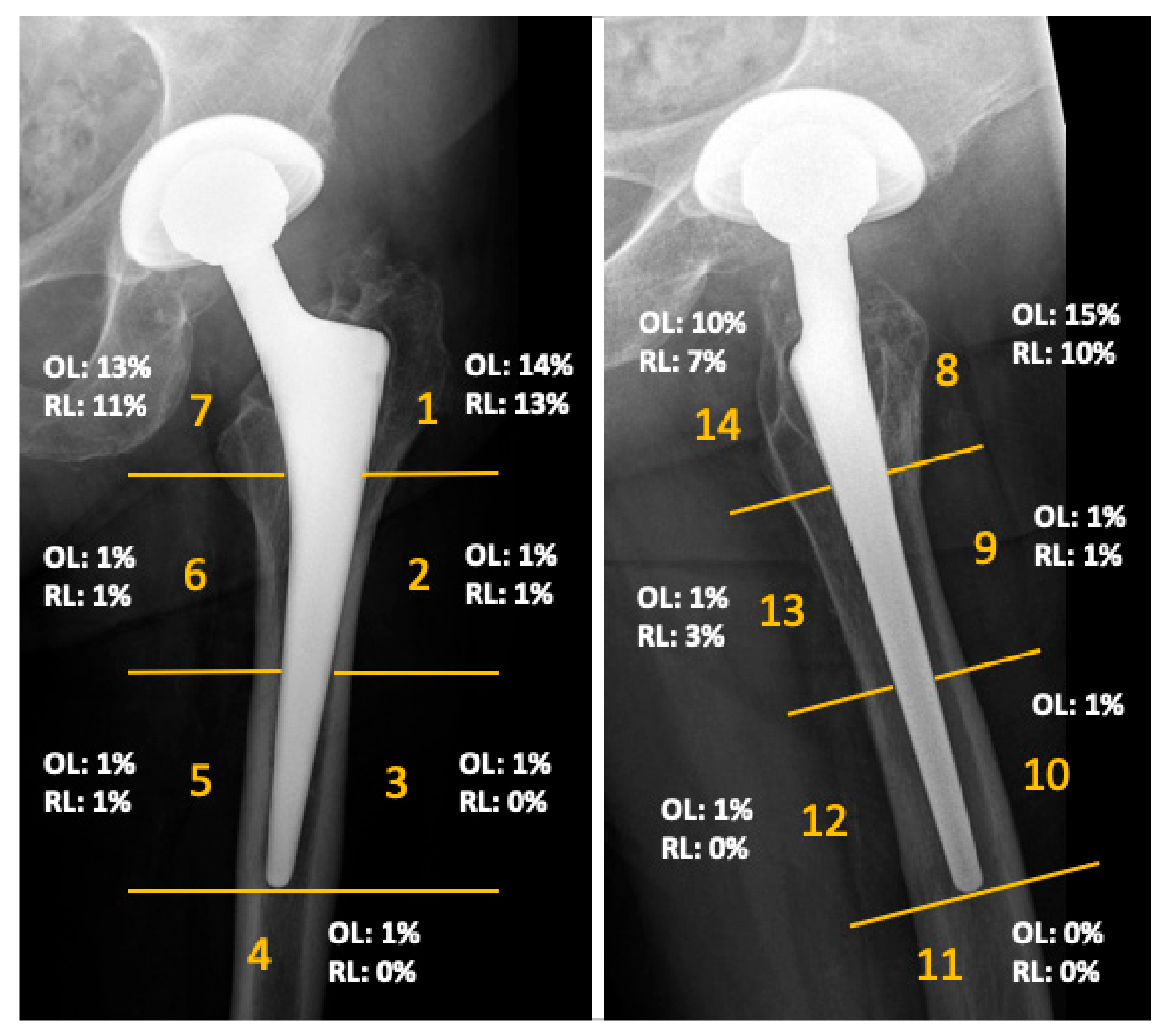
3.2. Clinical and Radiographic Evaluation
3.3. Metal Ion Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Weber, B.G. Experience with the Metasul total hip bearing system. Clin. Orthop. Relat. Res. 1996, 329, S69–S77. [Google Scholar] [CrossRef] [PubMed]
- Bozic, K.J.; Kurtz, S.; Lau, E.; Ong, K.; Chiu, V.; Vail, T.P.; Rubash, H.E.; Berry, D.J. The epidemiology of bearing surface usage in total hip arthroplasty in the United States. J. Bone Joint Surg. Am. 2009, 91, 1614–1620. [Google Scholar] [CrossRef] [PubMed]
- Hart, A.J.; Sabah, S.; Henckel, J.; Lewis, A.; Cobb, J.; Sampson, B.; Mitchell, A.; Skinner, J.A. The painful metal-on-metal hip resurfacing. J. Bone Joint Surg. Br. 2009, 91, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Pandit, H.; Glyn-Jones, S.; McLardy-Smith, P.; Gundle, R.; Whitwell, D.; Gibbons, C.L.; Ostlere, S.; Athanasou, N.; Gill, H.S.; Murray, D.W. Pseudotumours associated with metal-on-metal hip resurfacings. J. Bone Joint Surg. Br. 2008, 90, 847–851. [Google Scholar] [CrossRef]
- Smith, A.J.; Dieppe, P.; Vernon, K.; Porter, M.; Blom, A.W.; National Joint Registry of, England and Wales. Failure rates of stemmed metal-on-metal hip replacements: Analysis of data from the National Joint Registry of England and Wales. Lancet 2012, 379, 1199–1204. [Google Scholar] [CrossRef]
- Campbell, P.; Ebramzadeh, E.; Nelson, S.; Takamura, K.; De Smet, K.; Amstutz, H.C. Histological features of pseudotumor-like tissues from metal-on-metal hips. Clin. Orthop. Relat. Res. 2010, 468, 2321–2327. [Google Scholar] [CrossRef]
- Lombardi, A.V., Jr.; Barrack, R.L.; Berend, K.R.; Cuckler, J.M.; Jacobs, J.J.; Mont, M.A.; Schmalzried, T.P. The Hip Society: Algorithmic approach to diagnosis and management of metal-on-metal arthroplasty. J. Bone Joint Surg. Br. 2012, 94, 14–18. [Google Scholar] [CrossRef]
- Medical and Healthcare Products Regulatory Agency (MHRA). Medical Device Alert: All Metal-on-metal (MoM) Hip Replacements: Updated Advice for Follow-up of Patients; MDA/2017/018; Medicines and Healthcare products Regulatory Agency: London, UK, 2017. Available online: http://www.mhra.gov.uk/ (accessed on 21 January 2020).
- Medical Devices. Metal-on-metal Hip Implants. Information for Orthopaedic Surgeons. Available online: http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/ImplantsandProsthetics/MetalonMetalHipImplants/ucm241667.htm (accessed on 21 January 2020).
- Hannemann, F.; Hartmann, A.; Schmitt, J.; Lutzner, J.; Seidler, A.; Campbell, P.; Delaunay, C.P.; Drexler, H.; Ettema, H.B.; Garcia-Cimbrelo, E.; et al. European multidisciplinary consensus statement on the use and monitoring of metal-on-metal bearings for total hip replacement and hip resurfacing. Orthop. Traumatol. Surg. Res. 2013, 99, 263–271. [Google Scholar] [CrossRef]
- Hwang, K.T.; Kim, Y.H.; Kim, Y.S.; Ryu, J.A. Prevalence of a soft-tissue lesion after small head metal-on-metal total hip replacement: 13- to 19-year follow-up study. Bone Joint J. 2014, 96, 1594–1599. [Google Scholar] [CrossRef]
- Lombardi, A.V., Jr.; Berend, K.R.; Adams, J.B.; Satterwhite, K.L. Adverse Reactions to Metal on Metal Are Not Exclusive to Large Heads in Total Hip Arthroplasty. Clin. Orthop. Relat. Res. 2016, 474, 432–440. [Google Scholar] [CrossRef]
- Reiner, T.; Do, T.D.; Klotz, M.C.; Hertzsch, F.; Seelmann, K.; Gaida, M.M.; Weber, M.A.; Gotterbarm, T. MRI Findings in Patients After Small-Head Metal-on-Metal Total Hip Arthroplasty with a Minimum Follow-up of 10 Years. J. Bone Joint Surg. Am. 2017, 99, 1540–1546. [Google Scholar] [CrossRef] [PubMed]
- Lons, A.; Putman, S.; Pasquier, G.; Migaud, H.; Drumez, E.; Girard, J. Metallic ion release after knee prosthesis implantation: A prospective study. Int. Orthop. 2017, 41, 2503–2508. [Google Scholar] [CrossRef] [PubMed]
- Innmann, M.M.; Gotterbarm, T.; Kretzer, J.P.; Merle, C.; Ewerbeck, V.; Weiss, S.; Aldinger, P.R.; Streit, M.R. Minimum ten-year results of a 28-mm metal-on-metal bearing in cementless total hip arthroplasty in patients fifty years of age and younger. Int. Orthop. 2014, 38, 929–934. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Gruen, T.A.; McNeice, G.M.; Amstutz, H.C. "Modes of failure" of cemented stem-type femoral components: A radiographic analysis of loosening. Clin. Orthop. Relat. Res. 1979, 141, 17–27. [Google Scholar] [CrossRef]
- DeLee, J.G.; Charnley, J. Radiological demarcation of cemented sockets in total hip replacement. Clin. Orthop. Relat. Res. 1976, 121, 20–32. [Google Scholar] [CrossRef]
- Streit, M.R.; Schroder, K.; Korber, M.; Merle, C.; Gotterbarm, T.; Ewerbeck, V.; Aldinger, P.R. High survival in young patients using a second generation uncemented total hip replacement. Int. Orthop. 2012, 36, 1129–1136. [Google Scholar] [CrossRef] [PubMed]
- Krachler M, H.C.; Kretzer, J.P. Validation of ultratrace analysis of Co, Cr, Ni and Mo in whole blood, serum and urine using ICP-SMS. J. Anal. Spectrom. 2009, 24, 605–610. [Google Scholar] [CrossRef]
- Engh, C.A.; MacDonald, S.J.; Sritulanondha, S.; Korczak, A.; Naudie, D.; Engh, C. Metal ion levels after metal-on-metal total hip arthroplasty: A five-year, prospective randomized trial. J. Bone Joint Surg. Am. 2014, 96, 448–455. [Google Scholar] [CrossRef]
- Migaud, H.; Putman, S.; Krantz, N.; Vasseur, L.; Girard, J. Cementless metal-on-metal versus ceramic-on-polyethylene hip arthroplasty in patients less than fifty years of age: a comparative study with twelve to fourteen-year follow-up. J. Bone Joint Surg. Am. 2011, 93, 137–142. [Google Scholar] [CrossRef]
- Ayoub, B.; Putman, S.; Cholewinski, P.; Paris, A.; Migaud, H.; Girard, J. Incidence of Adverse Reactions to Metal Debris From 28-mm Metal-on-Metal Total Hip Arthroplasties With Minimum 10 Years of Follow-Up: Clinical, Laboratory, and Ultrasound Assessment of 44 Cases. J. Arthroplasty. 2017, 32, 1206–1210. [Google Scholar] [CrossRef]
- De Haan, R.; Pattyn, C.; Gill, H.S.; Murray, D.W.; Campbell, P.A.; De Smet, K. Correlation between inclination of the acetabular component and metal ion levels in metal-on-metal hip resurfacing replacement. J. Bone Joint Surg. Br. 2008, 90, 1291–1297. [Google Scholar] [CrossRef] [PubMed]
- Langton, D.J.; Joyce, T.J.; Jameson, S.S.; Lord, J.; Van Orsouw, M.; Holland, J.P.; Nargol, A.V.; De Smet, K.A. Adverse reaction to metal debris following hip resurfacing: The influence of component type, orientation and volumetric wear. J. Bone Joint Surg. Br. 2011, 93, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Sidaginamale, R.P.; Joyce, T.J.; Lord, J.K.; Jefferson, R.; Blain, P.G.; Nargol, A.V.; Langton, D.J. Blood metal ion testing is an effectivescreening tool to identify poorly performing metal-on-metal bearingsurfaces. J. Bone Joint. Res. 2013, 2, 84–95. [Google Scholar] [CrossRef] [PubMed]
- Hart, A.J.; Sabah, S.A.; Sampson, B.; Skinner, J.A.; Powell, J.J.; Palla, L.; Pajamaki, K.J.; Puolakka, T.; Reito, A.; Eskelinen, A. Surveillance of Patients with Metal-on-Metal Hip Resurfacing and Total Hip Prostheses: A Prospective Cohort Study to Investigate the Relationship Between Blood Metal Ion Levels and Implant Failure. J. Bone Joint Surg. Am. 2014, 96, 1091–1099. [Google Scholar] [CrossRef] [PubMed]
- Lass, R.; Grubl, A.; Kolb, A.; Domayer, S.; Csuk, C.; Kubista, B.; Giurea, A.; Windhager, R. Primary cementless total hip arthroplasty with second-generation metal-on-metal bearings: a concise follow-up, at a minimum of seventeen years, of a previous report. J. Bone Joint Surg. Am. 2014, 96, e37. [Google Scholar] [CrossRef] [PubMed]
- Dastane, M.; Wan, Z.; Deshmane, P.; Long, W.T.; Dorr, L.D. Primary hip arthroplasty with 28-mm Metasul articulation. J. Arthroplasty. 2011, 26, 662–664. [Google Scholar] [CrossRef]
- Malik, A.; Dorr, L.D.; Long, W.T. Impingement as a mechanism of dissociation of a metasul metal-on-metal liner. J. Arthroplasty. 2009, 24, 323.e13–3323.e16. [Google Scholar] [CrossRef]
- National Institute for Health and Clinical Excellence (NICE). Guidance on the Selection of Prostheses for Primary Total Hip Replacement; National Institute for Health and Clinical Excellence (NICE): London, UK, 2000. Available online: https://www.nice.org.uk/guidance/ta304 (accessed on 21 January 2020).
- Hwang, K.T.; Kim, Y.H.; Kim, Y.S.; Choi, I.Y. Is second generation metal-on-metal primary total hip arthroplasty with a 28 mm head a worthy option?: A 12- to 18-year follow-up study. J. Arthroplasty. 2013, 28, 1828–1833. [Google Scholar] [CrossRef]
- Brodner, W.; Bitzan, P.; Meisinger, V.; Kaider, A.; Gottsauner-Wolf, F.; Kotz, R. Serum cobalt levels after metal-on-metal total hip arthroplasty. J. Bone Joint Surg. Am. 2003, 85, 2168–2173. [Google Scholar] [CrossRef]
- Lazennec, J.Y.; Boyer, P.; Poupon, J.; Rousseau, M.A.; Roy, C.; Ravaud, P.; Catonne, Y. Outcome and serum ion determination up to 11 years after implantation of a cemented metal-on-metal hip prosthesis. Acta Orthop. 2009, 80, 168–173. [Google Scholar] [CrossRef]
- Savarino, L.; Padovani, G.; Ferretti, M.; Greco, M.; Cenni, E.; Perrone, G.; Greco, F.; Baldini, N.; Giunti, A. Serum ion levels after ceramic-on-ceramic and metal-on-metal total hip arthroplasty: 8-year minimum follow-up. J. Orthop. Res. 2008, 26, 1569–1576. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Unilateral Group (n = 113) | Bilateral Group (n = 26) | p-Value | |
|---|---|---|---|
| Mean (Range) | Mean (Range) | ||
| Age at follow-up (years) | 67 (34–86) | 64 (48–79) | 0.117 |
| Female gender (%) | 35 | 50 | 0.167 |
| Body mass index (kg/m2) | 26 (17–40) | 27 (18–39) | 0.887 |
| Time of follow-up (years) | 14.3 (10.2–18.8) | 14.4 (11.9–17.7) | 0.960 |
| GFR (ml/min) | 72 (31–116) | 81 (54–106) | 0.021* |
| Cup Inclination (°) | 43 (25–62) | 45 (27–62) | 0.064 |
| Harris Hip Score | 91 (40–100) | 90 (46–100) | 0.765 |
| Unilateral Group (n = 113) µg/L | Bilateral Group (n = 26) µg/L | p-Value | ||
|---|---|---|---|---|
| Cobalt | Mean (SD) | 0.82 (0.78) | 2.59 (4.81) | 0.082 |
| Median | 0.55 | 1.30 | ||
| Range | 0.22–4.45 | 0.43–24.75 | ||
| Chromium | Mean (SD) | 1.51 (2.47) | 2.50 (3.22) | 0.092 |
| Median | 0.85 | 1.38 | ||
| Range | 0.04–22.69 | 0.26–16.75 | ||
| Titanium | Mean (SD) | 2.68 (2.50) | 3.76 (3.70) | 0.079 |
| Median | 2.01 | 2.71 | ||
| Range | 0.26–19.56 | 0.67–19.77 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reiner, T.; Klotz, M.C.; Seelmann, K.; Hertzsch, F.; Innmann, M.M.; Streit, M.R.; Nees, T.A.; Moradi, B.; Merle, C.; Kretzer, J.P.; et al. Long-Term Results of a Second-Generation, Small-Diameter, Metal-On-Metal Bearing in Primary Total Hip Arthroplasty at 14-Year Follow-Up. Materials 2020, 13, 557. https://doi.org/10.3390/ma13030557
Reiner T, Klotz MC, Seelmann K, Hertzsch F, Innmann MM, Streit MR, Nees TA, Moradi B, Merle C, Kretzer JP, et al. Long-Term Results of a Second-Generation, Small-Diameter, Metal-On-Metal Bearing in Primary Total Hip Arthroplasty at 14-Year Follow-Up. Materials. 2020; 13(3):557. https://doi.org/10.3390/ma13030557
Chicago/Turabian StyleReiner, Tobias, Matthias C. Klotz, Kirsten Seelmann, Fabian Hertzsch, Moritz M. Innmann, Marcus R. Streit, Timo A. Nees, Babak Moradi, Christian Merle, Jan Philippe Kretzer, and et al. 2020. "Long-Term Results of a Second-Generation, Small-Diameter, Metal-On-Metal Bearing in Primary Total Hip Arthroplasty at 14-Year Follow-Up" Materials 13, no. 3: 557. https://doi.org/10.3390/ma13030557
APA StyleReiner, T., Klotz, M. C., Seelmann, K., Hertzsch, F., Innmann, M. M., Streit, M. R., Nees, T. A., Moradi, B., Merle, C., Kretzer, J. P., & Gotterbarm, T. (2020). Long-Term Results of a Second-Generation, Small-Diameter, Metal-On-Metal Bearing in Primary Total Hip Arthroplasty at 14-Year Follow-Up. Materials, 13(3), 557. https://doi.org/10.3390/ma13030557