Abstract
We present a modified technique to close anterior open bite as well as to correct anterior and vertical macrogenia without sacrificing the lowermost symphyseal segment, in comparison with conventional Kole’s osteotomy, which can alter the symmetric bone architecture of the chin and jeopardize the blood supply of the sandwich segments
Kole in 1959 published his series on subapical osteotomy for the correction of anterior open bite deformity [1]. This procedure can be used for the correction of localized deformities such as mild to severe open bites and similar major asymmetric segmental deformities [2].
A patient who has a cleft with an anterior open bite with class III mandibular incisor relationship may present with prognathic mandible, increased vertical mentum, anterior open bite, and increased chin prominence (Figure 3 and Figure 4). Conventional maxillary advancement osteotomy with posterior impaction or distraction osteogenesis will be the treatment option if maxillary hypoplasia exists along with open bite.

Figure 3.
Preoperative profile view.

Figure 4.
Preoperative intraoral view.
We have developed a technique where anterior open bite and macrogenia can be corrected simultaneously via an intraoral subapical osteotomy. Instead of using a lower chin segment [3] as a bone graft for filling the bone lacunae underneath the subapical segment, we used a separate osteotomized bone segment above the symphyseal component as a donor graft.
Surgical Method
The subapical osteotomy cuts were made between the first and second premolar (no extraction) as in diagram (Figure 1). The subapical osteotomy segment was repositioned superiorly as in standard Kole’s technique to correct the open bite. After a low-level genioplasty, a 5-mm wedge of bicortical bone was removed above the level of genioplasty cut as in the picture (Figure 2). This bone wedge was used to fill the defect below the subapical bone defect (subapical sandwich with vertical and anterior genial correction; Figure 2). Because the pogonion had soft tissue excess, an intraoral symmetrical soft tissue excision also was done to improve the chin’s soft tissue profile.
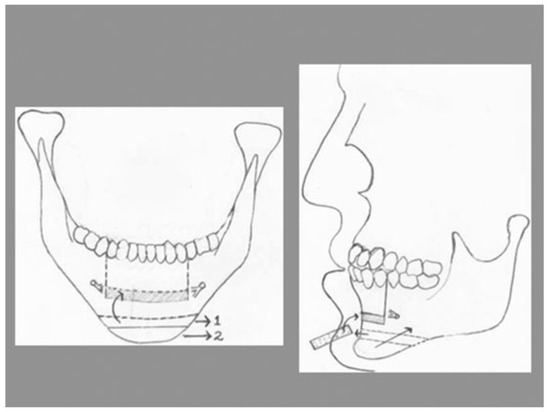
Figure 1.
Diagrammatic presentation of surgical procedure.
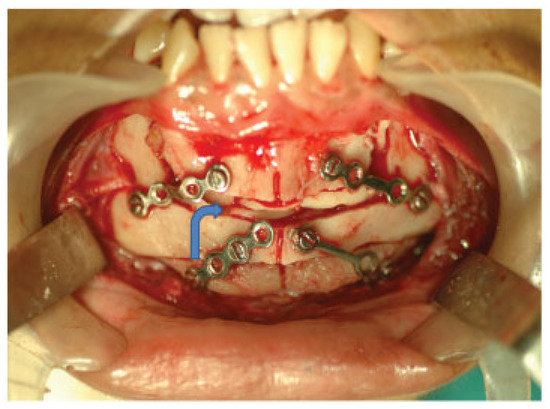
Figure 2.
Intraoperative view. Arrow shows the sandwich of bone below the subapical segment.
This modified technique is done to close anterior open bite as well to correct anterior and vertical macrogenia without sacrificing the lowermost symphyseal segment, in comparison with conventional Kole’s osteotomy, which can alter the symmetric bone architecture of the chin and jeopardize the blood supply of the sandwich segments (Figure 5 and Figure 6).

Figure 5.
Postoperative profile view.

Figure 6.
Postoperative intraoral view.
Conflicts of Interest
None.
References
- Kole, H. Chirurgische kieferorthopadie am alveolarkamm. Ost. Z. Stomato 1959, 56, 427. [Google Scholar]
- Lachard, J.; Blanc, J.L.; Lagier, J.P.; Cheynet, F.; Le Retraite, C.; Saban, Y. [Köle’s operation]. Rev Stomatol Chir Maxillofac 1987, 88, 306–310. [Google Scholar] [PubMed]
- Meyer, R.A. Mandibular symphysis as donor site in bone grafting for surgical correction of open bite: Report of case. J Oral Surg 1972, 30, 125–130. [Google Scholar] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2013 by the author. The Author(s) 2013.