Increased Pre-Operative Lung Immune Prognostic Index Score Is a Prognostic Factor in Cases of Pathological T3 Renal Cell Carcinoma

 , ,
, ,
Abstract

1. Introduction
2. Methods
2.1. Patients
2.2. Ethical Considerations
2.3. Endpoints
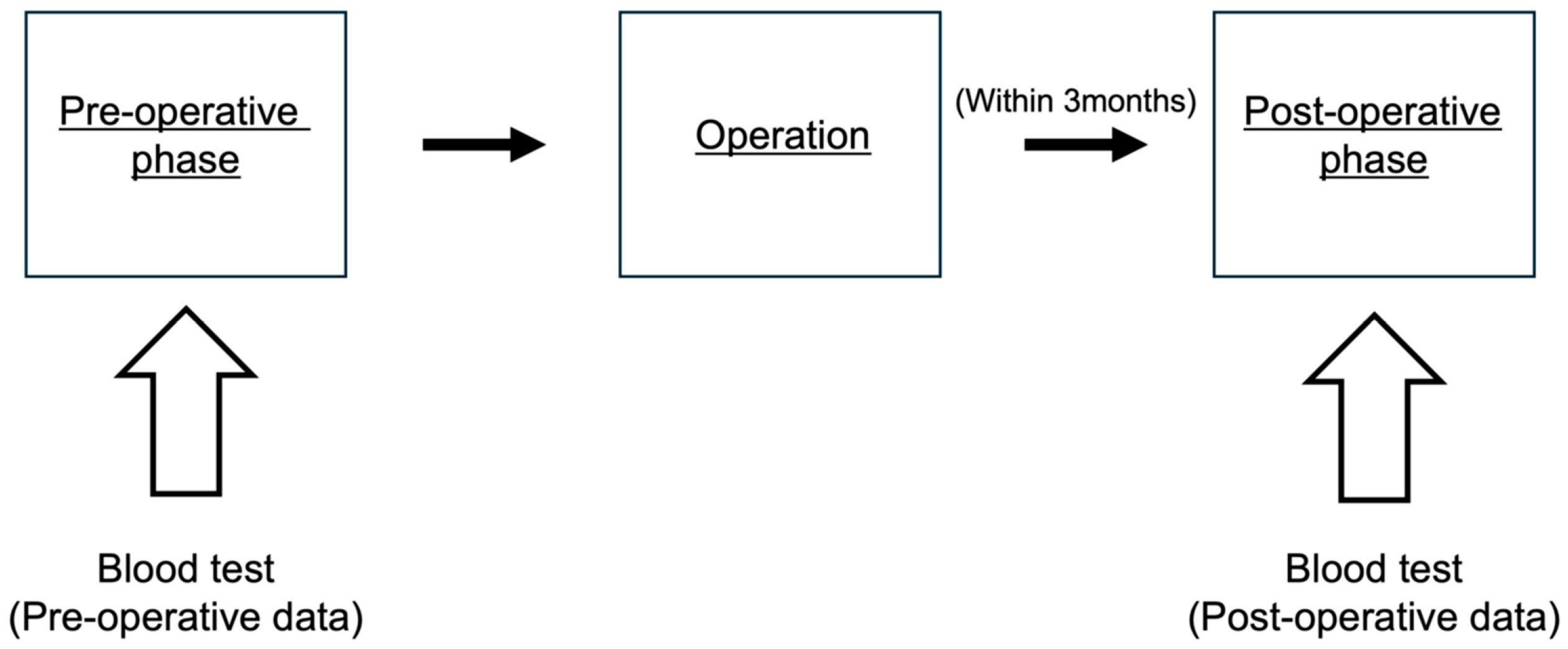
2.4. Calculation of LIPI Score
2.5. Data Collection
2.6. Statistical Analysis
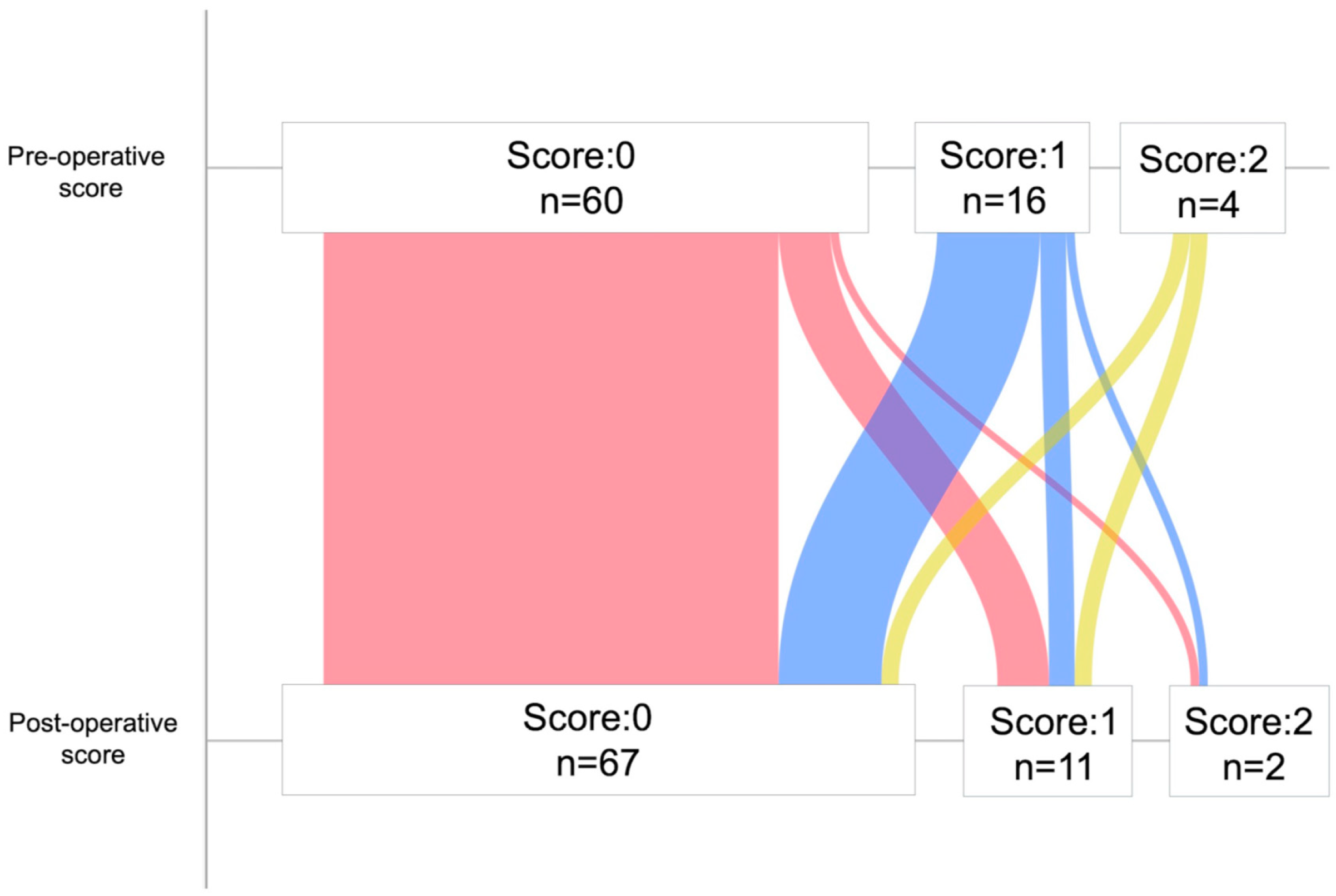
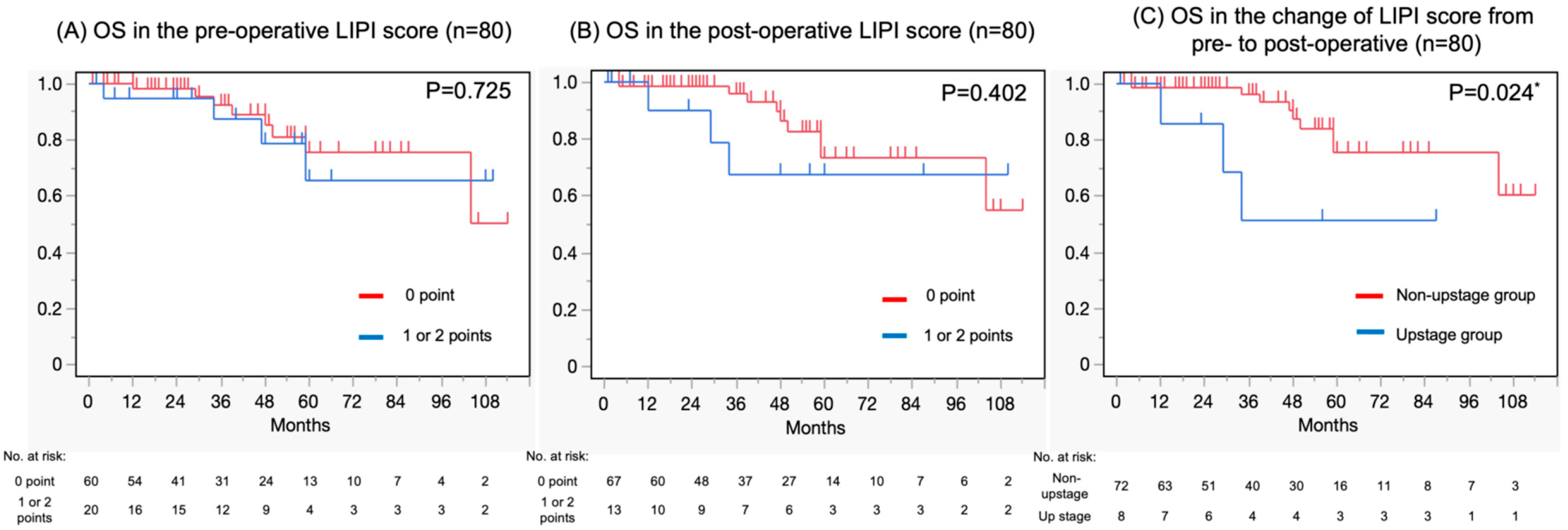
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ICIs | Immune checkpoint inhibitors |
| LIPI | Lung Immune Prognostic Index |
| RCC | Renal cell carcinoma |
| OS | Overall survival |
| pT3 | Pathological T3 |
| dNLR | Derived neutrophil-to-leukocyte ratio |
| NLR | Neutrophil-to-leukocyte ratio |
| LDH | Lactate dehydrogenase |
| ISUP | International Society of Urological Pathology |
| CRP | C-reactive protein |
| CI | Confidence interval |
| NR | Not reached |
| HR | Hazard ratio |
References
- Mezquita, L.; Auclin, E.; Ferrara, R.; Charrier, M.; Remon, J.; Planchard, D.; Ponce, S.; Ares, L.P.; Leroy, L.; Audigier-Valette, C.; et al. Association of the lung immune prognostic index with immune checkpoint inhibitor outcomes in patients with advanced non-small cell lung cancer. JAMA Oncol. 2018, 4, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Zhang, A. Correlation of Lung Immune Prognostic Index with Efficacy of PD-1/PD-L1 Inhibitor Combined with Chemotherapy and Prognosis in Patients with Advanced Non-Small Cell Lung Cancer. Am. J. Clin. Oncol. 2023, 46, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Auclin, E.; Roulleaux Dugage, M.; Gorria, T.; Vauchier, C.; Laguna, J.; Lupinacci, L.; Crous, C.; Naigeon, M.; Oudard, S.; Besse, B.; et al. Validation of the Lung Immune Prognostic Index in patients with untreated advanced non-small cell lung cancer: Post hoc analysis of the IMpower 130, 131 and 150 trials. Lung Cancer 2025, 199, 108039. [Google Scholar] [CrossRef] [PubMed]
- Liao, S.; Sun, S.; Lu, H.; Wu, J.; Wu, J.; Wu, Z.; Xi, J.; Liao, W.; Wang, Y. Neutrophil-to-lymphocyte ratio-based prognostic score can predict outcomes in patients with advanced non-small cell lung cancer treated with immunotherapy plus chemotherapy. BMC Cancer 2025, 25, 697. [Google Scholar] [CrossRef]
- Herranz-Bayo, E.; Chara-Velarde, L.; Cassinello-Espinosa, J.; Gimeno-Ballester, V.; Artal-Cortés, A.; Moratiel-Pellitero, A.; Alcácera-López, A.; Navarro-Expósito, F.; Riesco-Montes, B.; Clemente-Andujar, M. Lung immune prognostic index (LIPI) as a prognostic factor in patients with extensive-stage small cell lung cancer treated with first-line chemoimmunotherapy. Clin. Transl. Oncol. 2025, 27, 1484–1492. [Google Scholar] [CrossRef]
- Meyers, D.E.; Stukalin, I.; Vallerand, I.A.; Lewinson, R.T.; Suo, A.; Dean, M.; North, S.; Pabani, A.; Cheng, T.; Heng, D.Y.C.; et al. The Lung Immune Prognostic Index Discriminates Survival Outcomes in Patients with Solid Tumors Treated with Immune Checkpoint Inhibitors. Cancers 2019, 11, 1713. [Google Scholar] [CrossRef]
- Pierro, M.; Baldini, C.; Auclin, E.; Vincent, H.; Varga, A.; Martin Romano, P.; Vuagnat, P.; Besse, B.; Planchard, D.; Hollebecque, A.; et al. Predicting Immunotherapy Outcomes in Older Patients with Solid Tumors Using the LIPI Score. Cancers 2022, 14, 5078. [Google Scholar] [CrossRef]
- Sun, T.; Guo, Y.; Sun, B.; Chen, L.; Ren, Y.; Zhu, L.; Zhang, L.; Liu, Y.; Zheng, C. Association of the pretreatment lung immune prognostic index with immune checkpoint inhibitor outcomes in patients with advanced hepatocellular carcinoma. Eur. J. Med. Res. 2023, 28, 225. [Google Scholar] [CrossRef]
- Carril, L.; Colomba, E.; Romero-Ferreiro, C.; Cerbone, L.; Ratta, R.; Barthélémy, P.; Vindry, C.; Cherifi, F.; Boughalem, E.; Linassier, C.; et al. Efficacy of first-line combination therapy in metastatic renal cell carcinoma (mRCC) patients (pts) with poor performance status (PS). J. Clin. Oncol. 2022, 40 (Suppl. 6), 320. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Tomczak, P.; Park, S.H.; Venugopal, B.; Ferguson, T.; Chang, Y.H.; Hajek, J.; Symeonides, S.N.; Lee, J.L.; Sarwar, N.; et al. Adjuvant pembrolizumab after nephrectomy in renal-cell carcinoma. N. Engl. J. Med. 2021, 385, 683–694. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Tomczak, P.; Park, S.H.; Venugopal, B.; Ferguson, T.; Symeonides, S.N.; Hajek, J.; Chang, Y.H.; Lee, J.L.; Sarwar, N.; et al. Overall survival with adjuvant pembrolizumab in renal-cell carcinoma. N. Engl. J. Med. 2024, 390, 1359–1371. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Tomczak, P.; Park, S.H.; Venugopal, B.; Ferguson, T.; Symeonides, S.N.; Hajek, J.; Gurney, H.; Chang, Y.H.; Lee, J.L.; et al. Pembrolizumab versus placebo as post-nephrectomy adjuvant therapy for clear cell renal cell carcinoma (KEYNOTE-564): 30-month follow-up analysis of a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2022, 23, 1133–1144. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.W.; Chen, Y.; Wang, L.; Panian, J.; Dhanji, S.; Derweesh, I.; Rose, B.; Bagrodia, A.; McKay, R. Treatment Landscape of Renal Cell Carcinoma. Curr. Treat. Options Oncol. 2023, 24, 1889–1916. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Tomczak, P.; Park, S.H.; Venugopal, B.; Ferguson, T.; Chang, Y.H.; Hajek, J.; Symeonides, S.N.; Lee, J.L.; Sarwar, N.; et al. Pembrolizumab as post nephrectomy adjuvant therapy for patients with renal cell carcinoma: Results from 30-month follow-up of KEYNOTE-564. J. Clin. Oncol. 2022, 40 (Suppl. 6), 290. [Google Scholar] [CrossRef]
- Ding, K.; Yang, Z.; Zhang, D.; Sun, L. Efficacy Assessment of Post-nephrectomy Adjuvant Therapies in Patients with Renal Cell Carcinoma. Ann. Surg. Oncol. 2024, 31, 3894–3905. [Google Scholar] [CrossRef]
- Patel, S.H.; Uzzo, R.; Larcher, A.; Peyronnet, B.; Lane, B.; Pruthi, D.; Reddy, M.; Capitanio, U.; Joshi, S.; Noyes, S.; et al. Oncologic and Functional Outcomes of Radical and Partial Nephrectomy in pT3a Pathologically Upstaged Renal Cell Carcinoma: A Multi-institutional Analysis. Clin. Genitourin. Cancer 2020, 18, e723–e729. [Google Scholar] [CrossRef]
- Ferrucci, P.F.; Ascierto, P.A.; Pigozzo, J.; Del Vecchio, M.; Maio, M.; Antonini Cappellini, G.C.; Guidoboni, M.; Queirolo, P.; Savoia, P.; Mandalà, M.; et al. Baseline neutrophils and derived neutrophil-to-lymphocyte ratio: Prognostic relevance in metastatic melanoma patients receiving ipilimumab. Ann. Oncol. 2016, 27, 732–738. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Wang, Y.; Ye, Q.; Wang, Y.; Min, L.; Luo, Y.; Zhou, Y.; Tu, C. Lung immune prognostic index could predict metastasis in patients with osteosarcoma. Front. Surg. 2022, 9, 923427. [Google Scholar] [CrossRef]
- Carril-Ajuria, L.; Lavaud, P.; Dalban, C.; Negrier, S.; Gravis, G.; Motzer, R.J.; Chevreau, C.; Tannir, N.M.; Oudard, S.; McDermott, D.F.; et al. Validation of the Lung Immune Prognostic Index (LIPI) as a prognostic biomarker in metastatic renal cell carcinoma. Eur. J. Cancer 2024, 204, 114048. [Google Scholar] [CrossRef]
- Obayashi, K.; Miki, J.; Fukuokaya, W.; Yanagisawa, T.; Kimura, S.; Tsuzuki, S.; Kimura, T.; Egawa, S. The prognostic value of the preoperative lung immune prognostic index in patients with urothelial bladder cancer undergoing radical cystectomy. Int. J. Clin. Oncol. 2022, 27, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Albiges, L.; Tannir, N.M.; Burotto, M.; McDermott, D.; Plimack, E.R.; Barthélémy, P.; Porta, C.; Powles, T.; Donskov, F.; George, S.; et al. Nivolumab plus ipilimumab versus sunitinib for first-line treatment of advanced renal cell carcinoma: Extended 4-year follow-up of the phase III CheckMate 214 trial. ESMO Open 2020, 5, e001079. [Google Scholar] [CrossRef]
- Carril-Ajuria, L.; Motzer, R.J.; Tannir, N.M.; McDermott, D.F.; Hammers, H.J.; Plimack, E.R.; Donskov, F.; Rini, B.I.; Jiang, R.; Lee, C.W.; et al. Prognostic value of the lung immune prognostic index in patients with untreated advanced renal cell carcinoma (aRCC) receiving nivolumab plus ipilimumab (N+I) or sunitinib (SUN) in the CheckMate 214 trial. J. Clin. Oncol. 2022, 40, 4538. [Google Scholar] [CrossRef]
- Silva, C.A.C.; Zoppi, S.; Reni, A.; Piccinno, G.; Lahmar, I.; Cerbone, L.; Carril-Ajuria, L.; Colomba, E.; Flippot, R.; Sow, C.; et al. The Lung Immune Prognostic Index (LIPI) stratifies prognostic groups and correlates with gut microbiota (GM) in patients with advanced renal cell carcinoma (RCC). J. Clin. Oncol. 2023, 41, 719. [Google Scholar] [CrossRef]
- Paramanathan, A.; Saxena, A.; Morris, D.L. A systematic review and meta-analysis on the impact of pre-operative neutrophil lymphocyte ratio on long term outcomes after curative intent resection of solid tumours. Surg. Oncol. 2014, 23, 31–39. [Google Scholar] [CrossRef]
- Gu, X.B.; Tian, T.; Tian, X.J.; Zhang, X.J. Prognostic significance of neutrophil-to-lymphocyte ratio in non-small cell lung cancer: A meta-analysis. Sci. Rep. 2015, 5, 12493. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, R.; Takagi, T.; Hikichi, T.; Konno, N.; Sugimoto, M.; Watanabe, K.O.; Nakamura, J.; Waragai, Y.; Kikuchi, H.; Takasumi, M.; et al. Derived neutrophil/lymphocyte ratio predicts gemcitabine therapy outcome in unresectable pancreatic cancer. Oncol. Lett. 2016, 11, 3441–3445. [Google Scholar] [CrossRef]
- Amato, R.J.; Flaherty, A.; Zhang, Y.; Ouyang, F.; Mohlere, V. Clinical prognostic factors associated with outcome in patients with renal cell cancer with prior tyrosine kinase inhibitors or immunotherapy treated with everolimus. Urol. Oncol. 2014, 32, 345–354. [Google Scholar] [CrossRef]
- van Kessel, K.E.M.; de Haan, L.M.; Fransen van de Putte, E.E.; van Rhijn, B.W.; de Wit, R.; van der Heijden, M.S.; Zwarthoff, E.C.; Boormans, J.L. Elevated derived neutrophil-to-lymphocyte ratio corresponds with poor outcome in patients undergoing pre-operative chemotherapy in muscle-invasive bladder cancer. Bladder Cancer 2016, 2, 351–360. [Google Scholar] [CrossRef]
- Ishiyama, Y.; Kondo, T.; Yoshida, K.; Iizuka, J.; Takagi, T. Prognostic value of the lung immune prognostic index on recurrence after radical surgery for high-risk renal cell carcinoma. Cancers 2024, 16, 776. [Google Scholar] [CrossRef]
- Veccia, A.; Falagario, U.; Martini, A.; Marchioni, M.; Antonelli, A.; Simeone, C.; Cormio, L.; Capitanio, U.; Mir, M.C.; Derweesh, I.; et al. Upstaging to pT3a in patients undergoing partial or radical nephrectomy for cT1 renal tumors: A systematic review and meta-analysis of outcomes and predictive factors. Eur. Urol. Focus. 2021, 7, 574–581. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, Z.A.; Capitanio, U.; Pruthi, D.; Ghali, F.; Larcher, A.; Patel, D.N.; Eldefrawy, A.; Patel, S.; Cotta, B.H.; Bradshaw, A.W.; et al. Risk factors for upstaging, recurrence, and mortality in clinical T1-2 renal cell carcinoma patients upstage to pT3a disease: An international analysis utilizing the 8th edition of the tumor-node-metastasis staging criteria. Urology 2020, 138, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Russell, C.M.; Lebastchi, A.H.; Chipollini, J.; Niemann, A.; Mehra, R.; Morgan, T.M.; Miller, D.C.; Palapattu, G.S.; Hafez, K.S.; Sexton, W.; et al. Multi-institutional survival analysis of incidental pathologic T3a upstaging in clinical T1 renal cell carcinoma following partial nephrectomy. Urology 2018, 117, 95–100. [Google Scholar] [CrossRef]
- Komai, Y.; Saito, K.; Sakai, K.; Morimoto, S. Increased preoperative serum C-reactive protein level predicts a poor prognosis in patients with localized renal cell carcinoma. BJU Int. 2007, 99, 77–80. [Google Scholar] [CrossRef]
- De Martino, M.; Klatte, T.; Seemann, C.; Waldert, M.; Haitel, A.; Schatzl, G.; Remzi, M.; Weibl, P. Validation of serum C-reactive protein (CRP) as an independent prognostic factor for disease-free survival in patients with localised renal cell carcinoma (RCC). BJU Int. 2013, 111, E348–E353. [Google Scholar] [CrossRef] [PubMed]
- Ishiyama, Y.; Kondo, T.; Ishihara, H.; Yoshida, K.; Iizuka, J.; Tanabe, K.; Takagi, T. C-reactive protein kinetics to predict recurrence of high-risk renal cell carcinoma after radical surgery. Int. J. Clin. Oncol. 2022, 27, 969–976. [Google Scholar] [CrossRef]
- Zhang, B.Y.; Cheville, J.C.; Thompson, R.H.; Lohse, C.M.; Boorjian, S.A.; Leibovich, B.C.; Costello, B.A. Impact of rhabdoid differentiation on prognosis for patients with Grade 4 renal cell carcinoma. Eur. Urol. 2015, 68, 5–7. [Google Scholar] [CrossRef]
- Kim, H.; Inomoto, C.; Uchida, T.; Furuya, H.; Komiyama, T.; Kajiwara, H.; Kobayashi, H.; Nakamura, N.; Miyajima, A. Verification of the International Society of Urological Pathology recommendations in Japanese patients with clear cell renal cell carcinoma. Int. J. Oncol. 2018, 52, 1139–1148. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value (%) or Median (IQR) |
|---|---|
| Age, years | 68 (60–75) |
| Sex: | |
| Male | 59 (73.8) |
| Female | 21 (26.2) |
| Surgical Technique: | |
| Open | 39 (48.8) |
| Laparoscopic | 30 (37.5) |
| RAPN | 6 (7.5) |
| RARN | 5 (6.2) |
| Tumor side, left | 47 (58.8) |
| Pathological stage: | |
| pT3a | 78 (97.5) |
| pT3b | 2 (2.5) |
| Pathology: | |
| Clear cell | 74 (92.5) |
| Non-clear cell | 6 (7.5) |
| Fuhrman, or WHO/ISUP grade: | |
| 1 | 7 (8.8) |
| 2 | 43 (53.8) |
| 3 | 19 (23.7) |
| 4 | 8 (10) |
| Unclassified | 3 (3.7) |
| Lymphatic vessel invasion | 66 (82.5) |
| Sarcomatoid change | 8 (10) |
| Pre-operative metastasis | 9 (11.3) |
| CRP > 0.5 | |
| Pre-operative | 25 (31.3) |
| Post-operative | 15 (18.8) |
| Parameter | Cutoff | Univariable | Multivariable | ||
|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | ||
| Sex | Male | 2.78 (0.35–21.59) | 0.328 | ||
| Female | Reference | ||||
| Age | >70 years | 1.51 (0.46–5.00) | 0.492 | ||
| ≤70 | Reference | ||||
| Fuhrman WHO/ISUP | Grades 3/4 | 1.15 (0.33–3.99) | 0.814 | ||
| Grade 1/2/unclassified | Reference | ||||
| Sarcomatoid change | Yes | 7.81 (1.56–39.12) | 0.012 * | 8.71 (1.64–46.19) | 0.010 * |
| No | Reference | Reference | |||
| Lymphatic vessel invasion | Yes | 1.03 (0.22–4.70) | 0.969 | ||
| No | Reference | ||||
| Pre-operative LIPI | 1 or 2 points | 1.23 (0.37–4.13) | 0.728 | ||
| 0 points | Reference | ||||
| Post-operative LIPI | 1 or 2 points | 1.73 (0.46–6.40) | 0.411 | ||
| 0 points | Reference | ||||
| Pre-operative CRP | >0.5 | 1.29 (0.40–4.14) | 0.662 | ||
| ≤0.5 | Reference | ||||
| Post-operative CRP | >0.5 | 1.26 (0.34–4.71) | 0.722 | ||
LIPI score change (pre- to post-operative) | ≤0.5 Upstage Non-upstage | Reference 4.10 (1.07–15.61) Reference | 0.038 * | 4.38 (1.13–16.89) Reference | 0.031 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoshina, H.; Sugihara, T.; Kurokawa, M.; Takaoka, E.-i.; Ando, S.; Kume, H.; Fujimura, T. Increased Pre-Operative Lung Immune Prognostic Index Score Is a Prognostic Factor in Cases of Pathological T3 Renal Cell Carcinoma. Curr. Oncol. 2025, 32, 335. https://doi.org/10.3390/curroncol32060335
Hoshina H, Sugihara T, Kurokawa M, Takaoka E-i, Ando S, Kume H, Fujimura T. Increased Pre-Operative Lung Immune Prognostic Index Score Is a Prognostic Factor in Cases of Pathological T3 Renal Cell Carcinoma. Current Oncology. 2025; 32(6):335. https://doi.org/10.3390/curroncol32060335
Chicago/Turabian StyleHoshina, Hayato, Toru Sugihara, Masayuki Kurokawa, Ei-ichiro Takaoka, Satoshi Ando, Haruki Kume, and Tetsuya Fujimura. 2025. "Increased Pre-Operative Lung Immune Prognostic Index Score Is a Prognostic Factor in Cases of Pathological T3 Renal Cell Carcinoma" Current Oncology 32, no. 6: 335. https://doi.org/10.3390/curroncol32060335
APA StyleHoshina, H., Sugihara, T., Kurokawa, M., Takaoka, E.-i., Ando, S., Kume, H., & Fujimura, T. (2025). Increased Pre-Operative Lung Immune Prognostic Index Score Is a Prognostic Factor in Cases of Pathological T3 Renal Cell Carcinoma. Current Oncology, 32(6), 335. https://doi.org/10.3390/curroncol32060335