Effects of Symptom Burden on Quality of Life in Patients with Lung Cancer

Abstract
1. Introduction
2. Methods
2.1. Design and Sample
2.2. Patient Demographics and Database
2.3. EORTC Quality of Life Questionnaire C-30 (EORTC-QLQ-C30)
2.4. EORTC Quality of Life Questionnaire in Lung Cancer (EORTC-QLQ-LC13)
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Cancer Fact Sheet. 2023. Available online: https://www.who.int/mediacentre/factsheets/fs297/en/ (accessed on 1 June 2023).
- Morrison, E.J.; Novotny, P.J.; Sloan, J.A.; Yang, P.; Patten, C.A.; Ruddy, K.J.; Clark, M.M. Emotional Problems, Quality of Life, and Symptom Burden in Patients With Lung Cancer. Clin. Lung Cancer 2017, 18, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Ryu, E. Effects of symptom clusters and depression on the quality of life in patients with advanced lung cancer. Eur. J. Cancer Care 2018, 27, e12508. [Google Scholar] [CrossRef] [PubMed]
- Iyer, S.; Taylor-Stokes, G.; Roughley, A. Symptom burden and quality of life in advanced non-small cell lung cancer patients in France and Germany. Lung Cancer 2013, 81, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Chen, Y.; Yang, L.; Zhou, J. Pain, fatigue, disturbed sleep and distress comprised a symptom cluster that related to quality of life and functional status of lung cancer surgery patients. J. Clin. Nurs. 2013, 22, 1281–1290. [Google Scholar] [CrossRef]
- Barsevick, A.M. The elusive concept of the symptom cluster. Oncol. Nurs. Forum 2007, 34, 971–980. [Google Scholar] [CrossRef]
- Hung, H.Y.; Wu, L.M.; Chen, K.P. Determinants of Quality of Life in Lung Cancer Patients. J. Nurs. Scholarsh. 2018, 50, 257–264. [Google Scholar] [CrossRef]
- Machingura, A.; Taye, M.; Musoro, J.; Ringash, J.; Pe, M.; Coens, C.; Martinelli, F.; Tu, D.; Basch, E.; Brandberg, Y.; et al. Clustering of EORTC QLQ-C30 health-related quality of life scales across several cancer types: Validation study. Eur. J. Cancer 2022, 170, 1–9. [Google Scholar] [CrossRef]
- Trejo, M.J.; Bell, M.L.; Dhillon, H.M.; Vardy, J.L. Baseline quality of life is associated with survival among people with advanced lung cancer. J. Psychosoc. Oncol. 2020, 38, 635–641. [Google Scholar] [CrossRef]
- Plunkett, T.A.; Chrystal, K.F.; Harper, P.G. Quality of life and the treatment of advanced lung cancer. Clin. Lung Cancer 2003, 5, 28–32. [Google Scholar] [CrossRef]
- Quinten, C.; Martinelli, F.; Coens, C.; Sprangers, M.A.G.; Ringash, J.; Gotay, C.; Bjordal, K.; Greimel, E.; Reeve, B.B.; Maringwa, J.; et al. A global analysis of multitrial data investigating quality of life and symptoms as prognostic factors for survival in different tumor sites. Cancer 2014, 120, 302–311. [Google Scholar] [CrossRef]
- Iyer, S.; Roughley, A.; Rider, A.; Taylor-Stokes, G. The symptom burden of non-small cell lung cancer in the USA: A real-world cross-sectional study. Support. Care Cancer 2014, 22, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Mohan, A.; Singh, P.; Singh, S.; Goyal, A.; Pathak, A.; Mohan, C.; Guleria, R. Quality of life in lung cancer patients: Impact of baseline clinical profile and respiratory status. Eur. J. Cancer Care 2007, 16, 268–276. [Google Scholar] [CrossRef] [PubMed]
- Xará, S.; Amaral, T.F.; Parente, B. Undernutrition and quality of life in non small cell lung cancer patients. Rev. Port. De Pneumol. 2011, 17, 153–158. [Google Scholar] [CrossRef] [PubMed]
- John, L.D. Self-care strategies used by patients with lung cancer to promote quality of life. Oncol. Nurs. Forum 2010, 37, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Hammer, M.J.; Cooper, B.; Paul, S.M.; Kober, K.M.; Cartwright, F.; Conley, Y.P.; Wright, F.; Levine, J.D.; Miaskowski, C. Identification of Distinct Symptom Profiles in Cancer Patients Using a Pre-Specified Symptom Cluster. J. Pain Symptom Manag. 2022, 64, 17–27. [Google Scholar] [CrossRef]
- Liao, C.H.; Yu, S.; Lin, K.C.; Wu, Y.C.; Wang, T.J.; Wang, K.Y. The determinants of health-related quality of life among patients with newly diagnosed lung cancer in Taiwan: A cross-sectional study. J. Chin. Med. Assoc. 2023, 86, 338–344. [Google Scholar] [CrossRef]
- Vedadi, A.; Shakik, S.; Brown, M.C.; Lok, B.H.; Shepherd, F.A.; Leighl, N.B.; Sacher, A.; Bradbury, P.A.; Xu, W.; Liu, G.; et al. The impact of symptoms and comorbidity on health utility scores and health-related quality of life in small cell lung cancer using real world data. Qual Life Res. 2021, 30, 445–454. [Google Scholar] [CrossRef]
- Chie, W.C.; Yang, C.H.; Hsu, C.; Yang, P.C. Quality of life of lung cancer patients: Validation of the Taiwan Chinese version of the EORTC QLQ-C30 and QLQ-LC13. Qual Life Res. 2004, 13, 257–262. [Google Scholar] [CrossRef]
- Mols, F.; Husson, O.; Oudejans, M.; Vlooswijk, C.; Horevoorts, N.; van de Poll-Franse, L.V. Reference data of the EORTC QLQ-C30 questionnaire: Five consecutive annual assessments of approximately 2000 representative Dutch men and women. Acta Oncol. 2018, 57, 1381–1391. [Google Scholar] [CrossRef]
- Miret, C.; Orive, M.; Sala, M.; García-Gutiérrez, S.; Sarasqueta, C.; Legarreta, M.J.; Redondo, M.; Rivero, A.; Castells, X.; Quintana, J.M.; et al. Reference values of EORTC QLQ-C30, EORTC QLQ-BR23, and EQ-5D-5L for women with non-metastatic breast cancer at diagnosis and 2 years after. Qual. Life Res. 2023, 32, 989–1003. [Google Scholar] [CrossRef]
- Coon, C.D.; Schlichting, M.; Zhang, X. Interpreting Within-Patient Changes on the EORTC QLQ-C30 and EORTC QLQ-LC13. Patient 2022, 15, 691–702. [Google Scholar] [CrossRef] [PubMed]
- Levy, J.; Gupta, V.; Amirazodi, E.; Allen-Ayodabo, C.; Jivraj, N.; Jeong, Y.; Davis, L.E.; Mahar, A.L.; De Mestral, C.; Saarela, O.; et al. Textbook Outcome and Survival in Patients With Gastric Cancer: An Analysis of the Population Registry of Esophageal and Stomach Tumours in Ontario (PRESTO). Ann. Surg. 2022, 275, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.C.; Shun, S.C.; Liao, W.Y.; Yu, C.J.; Yang, P.C.; Lai, Y.H. Quality of life and related factors in patients with newly diagnosed advanced lung cancer: A longitudinal study. Oncol. Nurs. Forum 2014, 41, E44–E55. [Google Scholar] [CrossRef] [PubMed]
- Montazeri, A.; Milroy, R.; Hole, D.; McEwen, J.; Gillis, C.R. How quality of life data contribute to our understanding of cancer patients’ experiences? A study of patients with lung cancer. Qual. Life Res. 2003, 12, 157–166. [Google Scholar] [CrossRef]
- Brown, J.K.; Cooley, M.E.; Chernecky, C.; Sarna, L. A symptom cluster and sentinel symptom experienced by women with lung cancer. Oncol. Nurs. Forum 2011, 38, E425–E435. [Google Scholar] [CrossRef] [PubMed]
- Larsson, M.; Ljung, L.; Johansson, B.B. Health-related quality of life in advanced non-small cell lung cancer: Correlates and comparisons to normative data. Eur. J. Cancer Care 2012, 21, 642–649. [Google Scholar] [CrossRef]
- Miura, S.; Naito, T.; Mitsunaga, S.; Omae, K.; Mori, K.; Inano, T.; Yamaguchi, T.; Tatematsu, N.; Okayama, T.; Morikawa, A.; et al. A randomized phase II study of nutritional and exercise treatment for elderly patients with advanced non-small cell lung or pancreatic cancer: The NEXTAC-TWO study protocol. BMC Cancer 2019, 19, 528. [Google Scholar] [CrossRef]
- Dhillon, H.M.; van der Ploeg, H.P.; Bell, M.L.; Boyer, M.; Clarke, S.; Vardy, J. The impact of physical activity on fatigue and quality of life in lung cancer patients: A randomised controlled trial protocol. BMC Cancer 2012, 12, 572. [Google Scholar] [CrossRef]
- Rowntree, R.A.; Hosseinzadeh, H. Lung Cancer and Self-Management Interventions: A Systematic Review of Randomised Controlled Trials. Int. J. Environ. Res. Public Health 2022, 19, 536. [Google Scholar] [CrossRef]
- Liu, X.; Wang, Y.Q.; Xie, J. Effects of Breathing Exercises on Patients With Lung Cancer. Oncol. Nurs. Forum 2019, 46, 303–317. [Google Scholar]
- Chouaid, C.; Agulnik, J.; Goker, E.; Herder, G.J.; Lester, J.F.; Vansteenkiste, J.; Finnern, H.W.; Lungershausen, J.; Eriksson, J.; Kim, K.; et al. Health-related quality of life and utility in patients with advanced non-small-cell lung cancer: A prospective cross-sectional patient survey in a real-world setting. J. Thorac. Oncol. 2013, 8, 997–1003. [Google Scholar] [CrossRef] [PubMed]
- Chang, G.-C.; Chiu, C.-H.; Yu, C.-J.; Chang, Y.-C.; Chang, Y.-H.; Hsu, K.-H.; Wu, Y.-C.; Chen, C.-Y.; Hsu, H.-H.; Wu, M.-T.; et al. Low-dose CT screening among never-smokers with or without a family history of lung cancer in Taiwan: A prospective cohort study. Lancet Respir. Med. 2024, 12, 141–152. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristic | n | % | Global QOL | Cohen’s d | |
|---|---|---|---|---|---|
| Age, mean ± SD (range) | 63.12 ± 11.4 (37–88) | ||||
| Sex | |||||
| Male | 56 | 35.2 | 68.60 ± 21.73 | 0.05 | |
| Female | 103 | 64.8 | 67.48 ± 22.61 | ||
| Marital status | |||||
| Married | 122 | 76.7 | 67.14 ± 22.79 | 0.14 | |
| Single or widowed | 37 | 23.3 | 70.27 ± 20.46 | ||
| Education level | |||||
| College or higher | 61 | 38.4 | 68.44 ± 21.79 | 0.04 | |
| High school or lower | 98 | 61.6 | 67.52 ± 22.62 | ||
| Live with family | |||||
| Yes | 136 | 85.5 | 67.28 ± 22.28 | 0.18 | |
| No | 23 | 14.5 | 71.38 ± 22.17 | ||
| Duration of postdiagnosis | |||||
| Diagnosed more than five years (before 2016) | 50 | 31.5 | 67.33 ± 23.86 | 0.03 | |
| Diagnosed within five years (2017–2021) | 109 | 68.6 | 68.12 ± 21.57 | ||
| Smoking status | |||||
| Never | 124 | 78.0 | 68.01 ± 23.39 | 0.03 | |
| Former or current | 35 | 22.0 | 67.38 ± 17.89 | ||
| Family history | |||||
| No | 117 | 73.6 | 66.52 ± 23.39 | 0.24 | |
| Yes | 42 | 26.4 | 71.63 ± 18.41 | ||
| Secondhand smoke status | |||||
| No | 116 | 73.0 | 68.32 ± 22.82 | 0.08 | |
| Yes | 43 | 27.0 | 66.67 ± 20.81 | ||
| Stage | |||||
| I–III | 50 | 31.5 | 73.67 ± 17.44 | 0.41 | |
| IV | 109 | 68.5 | 65.21 ± 23.73 | ||
| Monthly income level | |||||
| ≥US$645 | 95 | 59.8 | 69.82 ± 21.06 | 0.22 | |
| ≤US$645 | 64 | 40.2 | 64.97 ± 23.76 | ||
| Occupational status | |||||
| Yes | 33 | 20.8 | 68.69 ± 19.88 | 0.05 | |
| No | 126 | 79.2 | 67.66 ± 22.89 | ||
| Treatment | |||||
| Nil a | 59 | 37.1 | 71.05 ± 22.18 | 0.02 b | |
| Chemotherapy or radiotherapy | 67 | 42.1 | 67.29 ± 20.38 | ||
| Chemotherapy and radiotherapy | 33 | 20.8 | 63.38 ± 25.60 | ||
| Treatment line | |||||
| First Line | 52 | 32.7 | 71.79 ± 20.22 | 0.04 b | |
| Second Line | 55 | 34.6 | 69.85 ± 21.49 | ||
| Third to fifth Line | 52 | 32.7 | 61.86 ± 24.05 | ||
| Characteristic | Mean a | SD | |
|---|---|---|---|
| Quality of life (QLQ-C30) | |||
| Global QOL | 67.87 | 22.24 | |
| Physical function | 82.14 | 20.28 | |
| Role function | 82.29 | 27.98 | |
| Emotional function | 86.69 | 21.26 | |
| Cognitive function | 84.28 | 21.24 | |
| Social function | 80.29 | 27.55 | |
| Symptom burden | |||
| QLQ-C30 | |||
| Fatigue | 23.27 | 27.04 | |
| Nausea and vomiting | 6.60 | 18.85 | |
| Pain | 16.25 | 26.65 | |
| Dyspnea | 24.53 | 31.48 | |
| Insomnia | 32.08 | 36.72 | |
| Appetite loss | 18.03 | 30.87 | |
| Constipation | 13.42 | 27.07 | |
| Diarrhea | 14.47 | 26.13 | |
| Financial difficulties | 9.64 | 24.40 | |
| QLQ-LC13 | |||
| Dyspnea | 19.92 | 27.28 | |
| Coughing | 23.06 | 29.04 | |
| Haemoptysis | 2.10 | 10.40 | |
| Sore mouth | 11.11 | 25.62 | |
| Dysphagia | 5.24 | 16.58 | |
| Peripheral neuropathy | 14.05 | 24.42 | |
| Alopecia | 17.61 | 31.56 | |
| Pain in chest | 10.90 | 22.66 | |
| Pain in arm or shoulder | 10.06 | 22.74 | |
| Pain in other parts | 13.42 | 27.07 | |
| Global QOL | Physical Function | Role Function | Emotional Function | Cognitive Function | Social Function | ||
|---|---|---|---|---|---|---|---|
| QLQ-C30 | |||||||
| Fatigue | −0.49 ** | −0.56 ** | −0.66 ** | −0.29 ** | −0.24 ** | −0.52 ** | |
| Nausea and vomiting | −0.29 ** | −0.19 * | −0.35 ** | −0.19 * | −0.02 | −0.21 ** | |
| Pain | −0.36 ** | −0.31 ** | −0.41 ** | −0.17 * | −0.29 ** | −0.34 ** | |
| Dyspnea | −0.34 ** | −0.48 ** | −0.40 ** | −0.07 | −0.27 ** | −0.38 ** | |
| Insomnia | −0.05 | −0.11 | −0.15 | −0.25 ** | −0.22 ** | −0.12 | |
| Appetite loss | −0.52 ** | −0.42 ** | −0.52 ** | −0.22 ** | −0.33 ** | −0.46 ** | |
| Constipation | −0.28 ** | −0.31 ** | −0.29 ** | −0.05 | −0.17 * | −0.25 ** | |
| Diarrhea | −0.25 ** | −0.18 * | −0.22 ** | −0.09 | −0.16 * | −0.11 | |
| QLQ-LC13 | |||||||
| Dyspnea | −0.44 ** | −0.65 ** | −0.61 ** | −0.15 | −0.27 ** | −0.51 ** | |
| Coughing | −0.14 | −0.23 ** | −0.13 | −0.11 | −0.01 | −0.21 ** | |
| Hemoptysis | −0.03 | −0.08 | 0.01 | 0.04 | 0.02 | −0.09 | |
| Sore mouth | −0.12 | −0.19 * | −0.18 * | −0.06 | −0.10 | −0.22 ** | |
| Dysphagia | −0.01 | −0.11 | −0.16 * | −0.02 | −0.10 | −0.20 * | |
| Peripheral neuropathy | −0.09 | −0.06 | −0.14 | 0.08 | −0.08 | −0.26 ** | |
| Alopecia | −0.17 * | −0.06 | −0.05 | 0.07 | −0.09 | −0.14 | |
| Pain in chest | −0.37 ** | −0.31 ** | −0.29 ** | −0.22 ** | −0.26 ** | −0.30 ** | |
| Pain in arm or shoulder | −0.17 * | −0.09 | −0.14 | −0.02 | −0.180 * | −0.16 * | |
| Pain in other parts | −0.20 * | −0.17 * | −0.31 ** | −0.06 | −0.27 ** | −0.30 ** | |
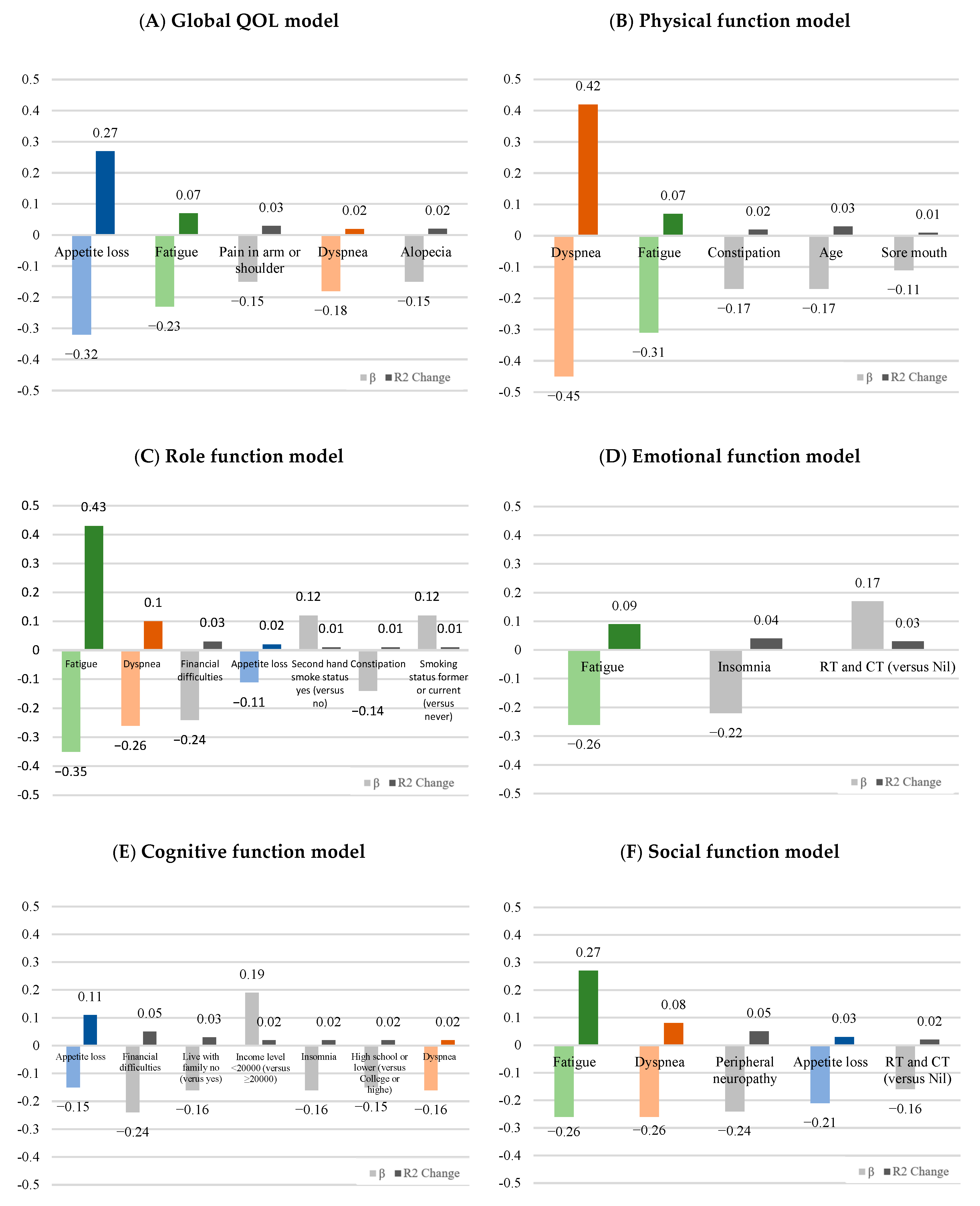
| Quality of Life Model | B | SE | β | t | p | Adjusted R2 | R2 Change | |
|---|---|---|---|---|---|---|---|---|
| Global QOL model | ||||||||
| Appetite loss | −0.23 | 0.05 | −0.32 | −4.38 | <0.001 | 0.27 | 0.27 | |
| Fatigue | −0.19 | 0.06 | −0.23 | −2.95 | 0.004 | 0.34 | 0.07 | |
| Pain in arm or shoulder | −0.15 | 0.06 | −0.15 | −2.45 | 0.016 | 0.36 | 0.03 | |
| Dyspnea | −0.15 | 0.06 | −0.18 | −2.50 | 0.013 | 0.38 | 0.02 | |
| Alopecia | −0.11 | 0.04 | −0.15 | −2.42 | 0.017 | 0.40 | 0.02 | |
| Physical function model | ||||||||
| Dyspnea | −0.33 | 0.05 | −0.45 | −6.94 | <0.001 | 0.42 | 0.42 | |
| Fatigue | −0.23 | 0.05 | −0.31 | −4.74 | <0.001 | 0.49 | 0.07 | |
| Constipation | −0.13 | 0.04 | −0.17 | −3.11 | 0.002 | 0.51 | 0.02 | |
| Age | −0.30 | 0.10 | −0.17 | −3.05 | 0.003 | 0.53 | 0.03 | |
| Sore mouth | −0.09 | 0.04 | −0.11 | −1.98 | 0.049 | 0.54 | 0.01 | |
| Role function model | ||||||||
| Fatigue | −0.36 | 0.07 | −0.35 | −5.33 | <0.001 | 0.43 | 0.43 | |
| Dyspnea | −0.26 | 0.06 | −0.26 | −4.05 | <0.001 | 0.52 | 0.10 | |
| Financial difficulties | −0.27 | 0.07 | −0.24 | −3.92 | <0.001 | 0.55 | 0.03 | |
| Appetite loss | −0.10 | 0.06 | −0.11 | −1.67 | 0.097 | 0.57 | 0.02 | |
| Secondhand smoke status yes (versus no) | 7.47 | 3.25 | 0.12 | 2.30 | 0.023 | 0.58 | 0.01 | |
| Constipation | −0.14 | 0.06 | −0.14 | −2.49 | 0.014 | 0.59 | 0.01 | |
| Smoking status former or current (versus never) | 8.08 | 3.50 | 0.12 | 2.31 | 0.022 | 0.60 | 0.01 | |
| Emotional function model | ||||||||
| Fatigue | −0.21 | 0.06 | −0.26 | −3.46 | 0.001 | 0.08 | 0.09 | |
| Insomnia | −0.13 | 0.04 | −0.22 | −2.84 | 0.005 | 0.11 | 0.04 | |
| RT and CT (versus nil) | 8.76 | 3.93 | 0.17 | 2.23 | 0.027 | 0.13 | 0.03 | |
| Cognitive function model | ||||||||
| Appetite loss | −0.11 | 0.06 | −0.15 | −1.90 | 0.059 | 0.10 | 0.11 | |
| Financial difficulties | −0.21 | 0.07 | −0.24 | −3.06 | 0.003 | 0.14 | 0.05 | |
| Live with family no (versus yes) | −9.91 | 4.31 | −0.16 | −2.30 | 0.023 | 0.16 | 0.03 | |
| Income level < 20,000 (versus ≥ 20,000) | 8.15 | 3.18 | 0.19 | 2.56 | 0.011 | 0.18 | 0.02 | |
| Insomnia | −0.09 | 0.04 | −0.16 | −2.26 | 0.025 | 0.20 | 0.02 | |
| High school or lower (versus college or higher) | −6.50 | 3.19 | −0.15 | −2.04 | 0.043 | 0.22 | 0.02 | |
| Dyspnea | −0.11 | 0.05 | −0.16 | −2.04 | 0.043 | 0.23 | 0.02 | |
| Social function model | ||||||||
| Fatigue | −0.27 | 0.08 | −0.26 | −3.52 | 0.001 | 0.27 | 0.27 | |
| Dyspnea | −0.27 | 0.07 | −0.26 | −3.73 | <0.001 | 0.35 | 0.08 | |
| Peripheral neuropathy | −0.27 | 0.07 | −0.24 | −3.99 | <0.001 | 0.39 | 0.05 | |
| Appetite loss | −0.19 | 0.06 | −0.21 | −3.07 | 0.003 | 0.42 | 0.03 | |
| RT and CT (versus nil) | −10.53 | 4.03 | −0.16 | −2.61 | 0.010 | 0.45 | 0.02 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiou, L.-J.; Lin, Y.-Y.; Lang, H.-C. Effects of Symptom Burden on Quality of Life in Patients with Lung Cancer. Curr. Oncol. 2024, 31, 6144-6154. https://doi.org/10.3390/curroncol31100458
Chiou L-J, Lin Y-Y, Lang H-C. Effects of Symptom Burden on Quality of Life in Patients with Lung Cancer. Current Oncology. 2024; 31(10):6144-6154. https://doi.org/10.3390/curroncol31100458
Chicago/Turabian StyleChiou, Ling-Jan, Yun-Yen Lin, and Hui-Chu Lang. 2024. "Effects of Symptom Burden on Quality of Life in Patients with Lung Cancer" Current Oncology 31, no. 10: 6144-6154. https://doi.org/10.3390/curroncol31100458
APA StyleChiou, L.-J., Lin, Y.-Y., & Lang, H.-C. (2024). Effects of Symptom Burden on Quality of Life in Patients with Lung Cancer. Current Oncology, 31(10), 6144-6154. https://doi.org/10.3390/curroncol31100458