Primary Signet Ring Cell/Histiocytoid Carcinoma of the Eyelid: Somatic Mutations in CDH1 and Other Clinically Actionable Mutations Imply Early Use of Targeted Agents

 ,
, 
 and
and
Abstract
1. Introduction
2. Materials and Methods
3. Results
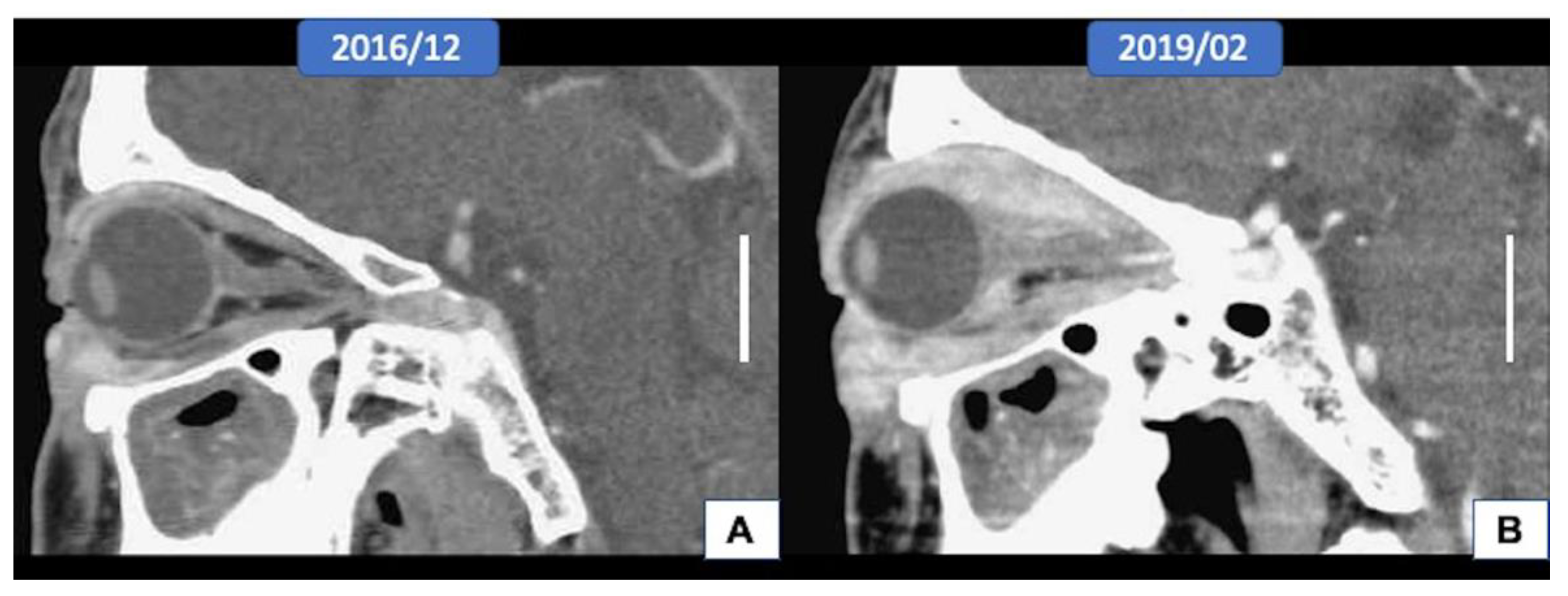
3.1. Clinical Features
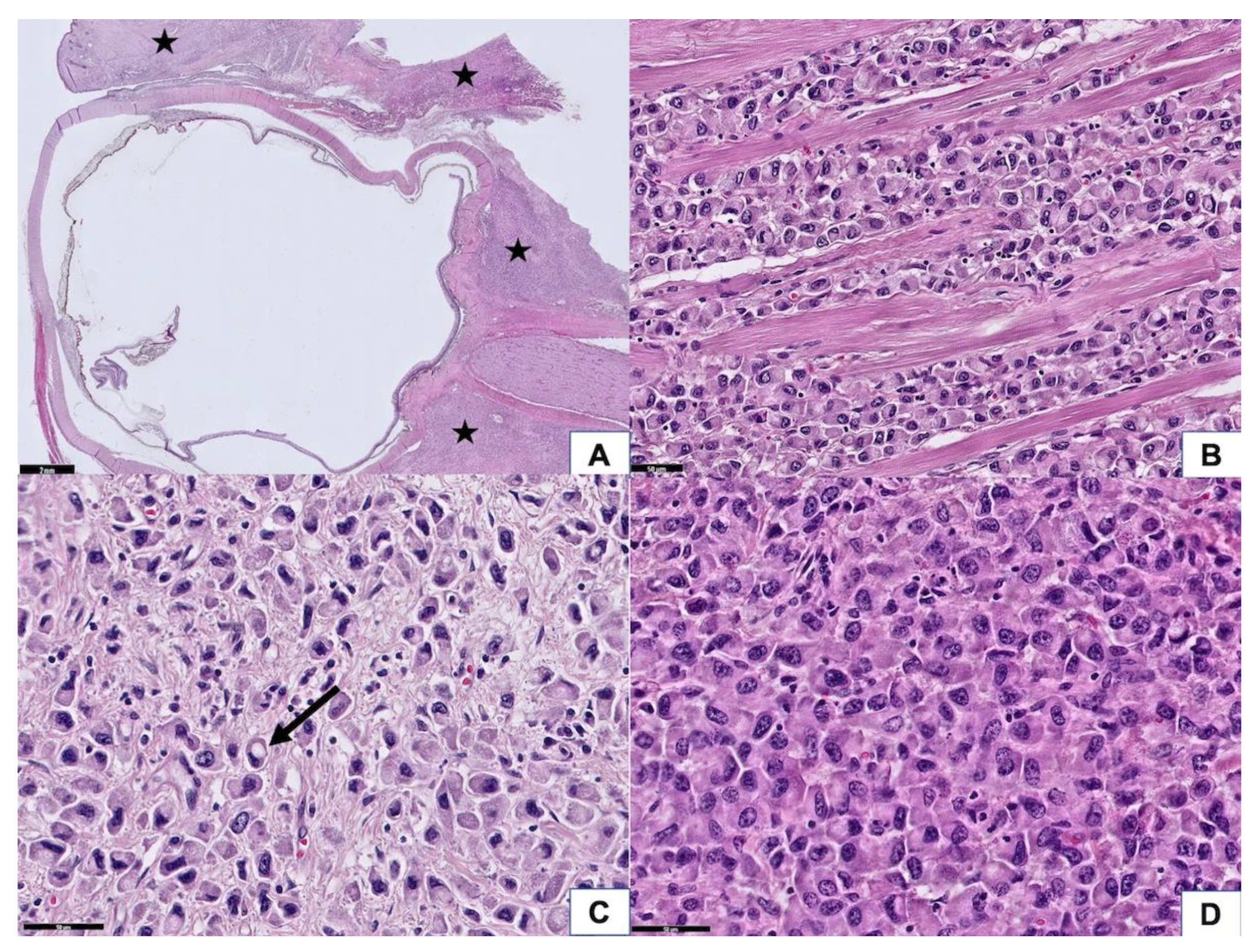
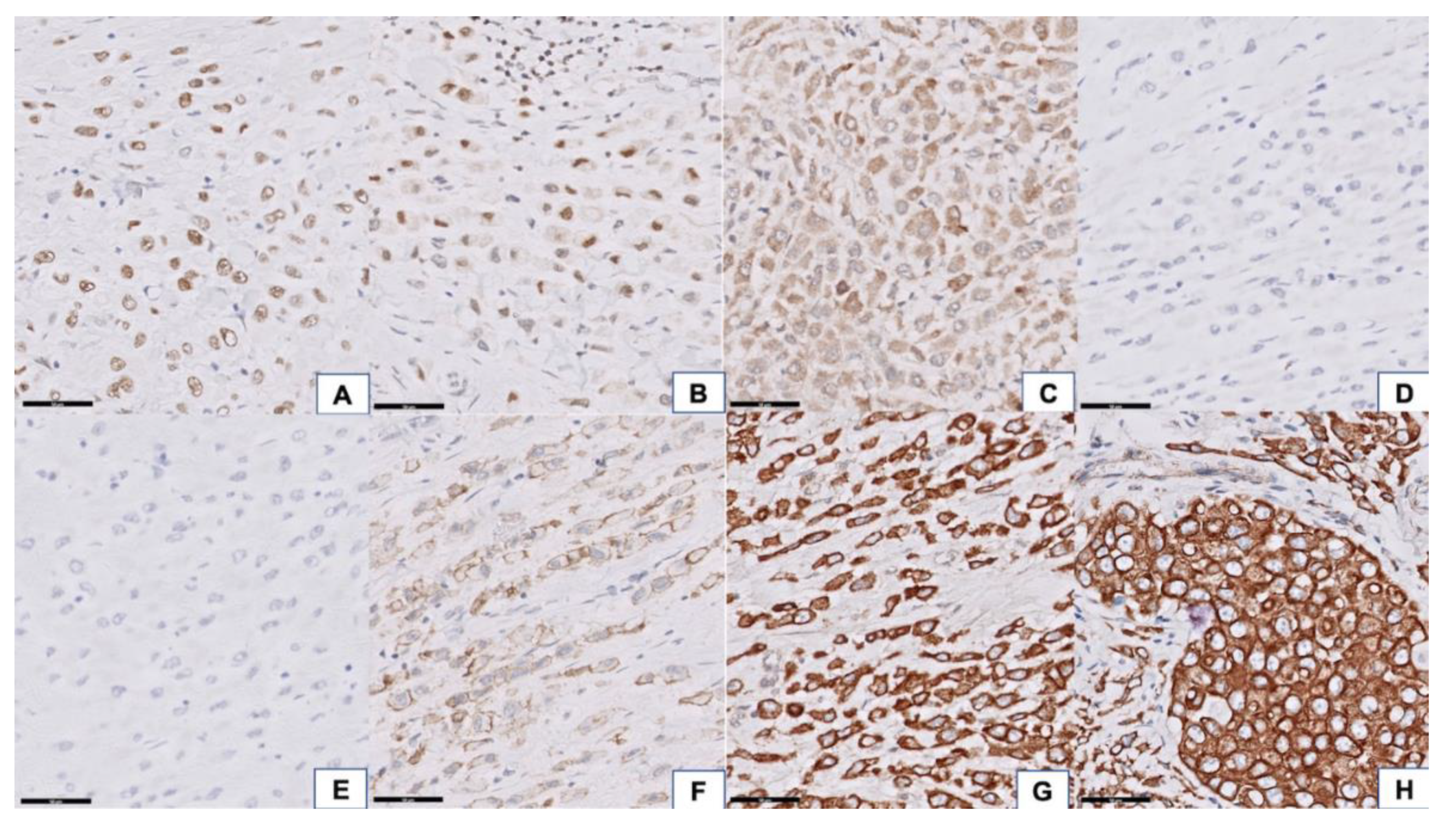
3.2. Histopathologic Findings
3.3. Next-Generation Sequencing
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kramer, T.R.; E Grossniklaus, H.; McLean, I.W.; Orcutt, J.; Green, W.R.; Iliff, N.T.; Tressera, F. Histiocytoid variant of eccrine sweat gland carcinoma of the eyelid and orbit: Report of five cases. Ophthalmology 2002, 109, 553–559. [Google Scholar] [CrossRef]
- Requena, L.; Prieto, V.G.; Requena, C.; Requena, C.; Sarasa, J.L.; Manzano, R.; Seco, M.; Rütten, A.; Kazakov, D.V.; Cerroni, L.; et al. Primary signet-ring cell/histiocytoid carcinoma of the eyelid: A clinicopathologic study of 5 cases and review of the literature. Am. J. Surg. Pathol. 2011, 35, 378–391. [Google Scholar] [CrossRef] [PubMed]
- Iwaya, M.; Uehara, T.; Yoshizawa, A.; Kobayashi, Y.; Momose, M.; Honda, T.; Ota, H. A case of primary signet-ring cell/histiocytoid carcinoma of the eyelid: Immunohistochemical comparison with the normal sweat gland and review of the literature. Am. J. Dermatopathol. 2012, 34, e139–e145. [Google Scholar] [CrossRef]
- Bernárdez, C.; Macías del Toro, E.; Ramírez Bellver, J.L.; Martinez Menchón, T.; Martinez Barba, E.; Molina-Ruiz, A.M.; Requena, L. Primary Signet-Ring Cell/Histiocytoid Carcinoma of the Eyelid: A “Binocle” Presentation of the “Monocle Tumor”. Am. J. Dermatopathol. 2016, 38, 623–627. [Google Scholar] [CrossRef]
- Auw-Haedrich, C.; Boehm, N.; Weissenberger, C. Signet ring carcinoma of the eccrine sweat gland in the eyelid, treated by radiotherapy alone. Br. J. Ophthalmol. 2001, 85, 112–113. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bellman, B.; Gregory, N.A.; Silvers, D.; Fountain, K.S. Sweat gland carcinoma with metastases to the skin: Response to 5-fluorouracil chemotherapy. Cutis 1995, 55, 221–224. [Google Scholar] [PubMed]
- Fb, F.B.; Hofman, V.; Lagier, J.; Gastaud, P.; Santini, J.; Hofman, P. Primary signet ring cell carcinoma of the eccrine sweat gland in the eyelid. Immunohistochemical and ultrastructural study of a case. J. Fr. Ophtalmol. 2002, 25, 547–551. [Google Scholar]
- Bhargava, R.; Beriwal, S.; Dabbs, D.J. Mammaglobin vs GCDFP-15: An immunohistologic validation survey for sensitivity and specificity. Am. J. Clin. Pathol. 2007, 127, 103–113. [Google Scholar] [CrossRef]
- González-Lois, C.; Rodríguez-Peralto, J.L.; Serrano-Pardo, R.; Martínez-González, M.A.; López-Ríos, F. Cutaneous signet ring cell carcinoma: A report of a case and review of the literature. Am. J. Dermatopathol. 2001, 23, 325–328. [Google Scholar] [CrossRef]
- Bouza Gonzalo, E.; Luezas Morcuende, J.; Martínez Montero, J.C.; Cuesta Gil, M.; Fernández De Castro Pombo, J. Eccrine gland adenocarcinoma of the eyelid. Arch. Soc. Esp. Oftalmol. 2001, 76, 739–742. [Google Scholar]
- Grizzard, W.S.; Torezynski, E.; Edwards, W.C. Adenocarcinoma of eccrine sweat glands. Arch Ophthalmol. 1976, 94, 2119–2123. [Google Scholar] [CrossRef]
- Jakobiec, F.A.; Austin, P.; Iwamoto, T.; Trokel, S.L.; Marquardt, M.D.; Harrison, W. Primary infiltrating signet ring carcinoma of the eyelids. Ophthalmology 1983, 90, 291–299. [Google Scholar] [CrossRef]
- Kiyohara, T.; Kumakiri, M.; Kouraba, S.; Tokuriki, A.; Ansai, S. Primary cutaneous signet ring cell carcinoma expressing cytokeratin 20 immunoreactivity. J. Am. Acad. Dermatol. 2006, 54, 532–536. [Google Scholar] [CrossRef][Green Version]
- Langel, D.J.; Yeatts, R.P.; White, W.L. Primary signet ring cell carcinoma of the eyelid: Report of a case demonstrating further analogy to lobular carcinoma of the breast with a literature review. Am. J. Dermatopathol. 2001, 23, 444–449. [Google Scholar] [CrossRef] [PubMed]
- Mortensen, A.L.; Heegaard, S.; Clemmensen, O.; Prause, J.U. Signet ring cell carcinoma of the eyelid—The monocle tumour. Apmis 2008, 116, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Rosen, Y.; Kim, B.; Yermakov, V.A. Eccrine sweat gland tumor of clear cell origin involving the eyelids. Cancer 1975, 36, 1034–1041. [Google Scholar] [CrossRef]
- Swinson, B.; Ryan, F.; Barrett, A.W.; Jerjes, W.; Landon, G.; Calonje, E.; Kalavrezos, N. Histiocytoid eccrine sweat gland carcinoma of the eyelid: Report of a case. Clin. Exp. Dermatol. 2006, 31, 786–789. [Google Scholar] [CrossRef]
- Thomas, J.W.; Fu, Y.S.; Levine, M.R. Primary mucinous sweat gland carcinoma of the eyelid simulating metastatic carcinoma. Am. J. Ophthalmol. 1979, 87, 29–33. [Google Scholar] [CrossRef]
- Wollensak, G.; Witschel, H.; Böhm, N. Signet ring cell carcinoma of the eccrine sweat glands in the eyelid. Ophthalmology 1996, 103, 1788–1793. [Google Scholar] [CrossRef]
- Palakkamanil, M.M.; Mahmood, M.N.; Chan, A. Diagnostic and treatment challenges of a case of primary cutaneous signet-ring cell/histiocytoid carcinoma of the eyelid. BMC Ophthalmol. 2020, 20, 410. [Google Scholar] [CrossRef] [PubMed]
- Tanboon, J.; Uiprasertkul, M.; Luemsamran, P. Signet-ring cell/histiocytoid carcinoma of the eyelid: A case report and review of the literature. Am. J. Dermatopathol. 2013, 35, e1–e5. [Google Scholar] [CrossRef]
- Stewart, S.; Houghton, J.; Kamalarajah, S.; Curragh, D. Primary Adnexal Signet-Ring Cell/Histiocytoid Carcinoma. Ophthalmic. Plast Reconstr. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Sayan, A.; Mitchell, O.; Taibjee, S.; Ilankovan, V. Unusual case of primary cutaneous signet-ring cell (histocytoid) carcinoma. Br. J. Oral. Maxillofac. Surg. 2020, 58, 475–477. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, K.; Ito, T.; Tanioka, F.; Fukamizu, H.; Tokura, Y. Primary signet-ring cell/histiocytoid carcinoma of the eyelid expressing androgen receptors and treated with bicalutamide. J. Dermatol. 2017, 44, e230–e231. [Google Scholar] [CrossRef] [PubMed]
- Droubi, D.; Zeitouni, N.C.; Skitzki, J.; Bogner, P.N. Primary signet-ring cell carcinoma of the axilla. J. Cutan. Pathol. 2013, 40, 269–273. [Google Scholar] [CrossRef]
- Tan, J.S.; McKelvie, P.A.; Hardy, T.G. Primary signet ring cell carcinoma of the eyelid. Orbit 2013, 32, 399–401. [Google Scholar] [CrossRef]
- Cameselle-Teijeiro, J.; Alfonsín-Barreiro, N.; Allegue, F.; Caeiro, M. Apocrine carcinoma with signet ring cells and histiocytoid features. A potentially confusing axillary tumor. Pathol. Res. Pract. 1997, 193, 713–720; discussion 721–722. [Google Scholar] [CrossRef]
- Kuno, Y.; Numata, T.; Kanzaki, T. Adenocarcinoma with signet ring cells of the axilla showing apocrine features: A case report. Am. J. Dermatopathol. 1999, 21, 37–41. [Google Scholar] [CrossRef]
- Misago, N.; Shinoda, Y.; Okawa, T.; Aoki, S.; Toda, S.; Koike, K.; Narisawa, Y. Histiocytoid and signet-ring cell carcinoma of the axilla: A type of cutaneous apocrine carcinoma equivalent to histiocytoid lobular carcinoma of the breast? Clin. Exp. Dermatol. 2011, 36, 874–877. [Google Scholar] [CrossRef]
- Raghavan, S.S.; Clark, M.; Louie, C.Y.; Jensen, K.C.; Dietrich, B.; Beadle, B.M.; El-Sawy, T.; Baik, F.; Kunder, C.A.; Brown, R.A. Molecular profiling of a primary cutaneous signet-ring cell/histiocytoid carcinoma of the eyelid. J. Cutan. Pathol. 2020, 47, 860–864. [Google Scholar] [CrossRef]
- Oliveira, C.; Pinheiro, H.; Figueiredo, J.; Seruca, R.; Carneiro, F. E-cadherin alterations in hereditary disorders with emphasis on hereditary diffuse gastric cancer. Prog. Mol. Biol. Transl. Sci. 2013, 116, 337–359. [Google Scholar]
- Da Silva, L.; Parry, S.; Reid, L.; Keith, P.; Waddell, N.; Kossai, M.; Clarke, C.; Lakhani, S.R.; Simpson, P.T. Aberrant expression of E-cadherin in lobular carcinomas of the breast. Am. J. Surg. Pathol. 2008, 32, 773–783. [Google Scholar] [CrossRef] [PubMed]
- Berx, G.; Cleton-Jansen, A.M.; Strumane, K.; Keith, P.; Waddell, N.; Kossai, M.; Catherine, C.; Sunil, R.L.; Peter, T.S.; Simpson, P.T.; et al. E-cadherin is inactivated in a majority of invasive human lobular breast cancers by truncation mutations throughout its extracellular domain. Oncogene 1996, 13, 1919–1925. [Google Scholar]
- Harigopal, M.; Shin, S.J.; Murray, M.P.; Tickoo, S.K.; Brogi, E.; Rosen, P.P. Aberrant E-cadherin staining patterns in invasive mammary carcinoma. World J. Surg. Oncol. 2005, 3, 73. [Google Scholar] [CrossRef] [PubMed]
- Ohshiro, K.; Zaidi, S.; Korkut, A.; Chen, J.; Rao, S.; Gu, S.; Jogunoori, W.; Mishra, B.; Akbani, R.; Mishra, L. A Pan-Cancer Analysis Reveals High-Frequency Genetic Alterations in Mediators of Signaling by the TGF-β Superfamily. Cell Syst. 2018, 7, 422–437.e427. [Google Scholar]
- Al-Ahmadie, H.A.; Iyer, G.; Lee, B.H.; Scott, S.N.; Mehra, R.; Bagrodia, A.; Jordan, E.J.; Gao, S.P.; Ramirez, R.; Cha, E.K.; et al. Frequent somatic CDH1 loss-of-function mutations in plasmacytoid variant bladder cancer. Nat. Genet. 2016, 48, 356–358. [Google Scholar] [CrossRef] [PubMed]
- Meric-Bernstam, F.; Johnson, A.M.; Dumbrava, E.E.I.; Raghav, K.; Balaji, K.; Bhatt, M.; Murthy, R.K.; Rodon, J.; Piha-Paul, S.A. Advances in HER2-Targeted Therapy: Novel Agents and Opportunities Beyond Breast and Gastric Cancer. Clin. Cancer Res. 2019, 25, 2033–2041. [Google Scholar] [CrossRef] [PubMed]
- Bose, R.; Kavuri, S.M.; Searleman, A.C.; Shen, W.; Shen, D.; Koboldt, D.C.; Monsey, J.; Goel, N.; Aronson, A.B.; Li, S.; et al. Activating HER2 mutations in HER2 gene amplification negative breast cancer. Cancer Discov. 2013, 3, 224–237. [Google Scholar] [CrossRef]
- Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/208051s004lbl.pdf (accessed on 15 February 2021).
- Volinia, S.; Hiles, I.; Ormondroyd, E.; Nizetic, D.; Antonacci, R.; Rocchi, M.; Waterfield, M.O. Molecular cloning, cDNA sequence, and chromosomal localization of the human phosphatidylinositol 3-kinase p110 alpha (PIK3CA) gene. Genomics 1994, 24, 472–477. [Google Scholar] [CrossRef]
- Weinstein, J.N.; The Cancer Genome Atlas Research Network; Collisson, E.A.; Mills, G.B.; Shaw, K.R.M.; Ozenberger, B.A.; Ellrott, K.; Shmulevich, I.; Sander, C.; Stuart, J.M. The Cancer Genome Atlas Pan-Cancer analysis project. Nat. Genet. 2013, 45, 1113–1120. [Google Scholar] [CrossRef]
- Cerami, E.; Gao, J.; Dogrusoz, U.; Gross, B.E.; Sumer, S.O.; Aksoy, B.A.; Jacobsen, A.; Byrne, C.J.; Heuer, M.L.; Larsson, E.; et al. The cBio cancer genomics portal: An open platform for exploring multidimensional cancer genomics data. Cancer Discov. 2012, 2, 401–404. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Antibody | Clone | Source | Dilution | Case |
|---|---|---|---|---|
| E-cadherin | HECD1 | Invitrogen | 1:300 | +++ |
| β-catenin | D10A8 | Cell Signaling | 1:50 | +++ (membrane and cytoplasm) |
| Estrogen receptor | 6F11 | Leica | 1:100 | - |
| Progesterone receptor | 16 | Leica | 1:200 | - |
| Her2-Neu | A0485 | DAKO | 1:900 | ++ |
| Cytokeratin | AE1/AE3 | Leica | 1:200 | +++ |
| Cytokeratin 7 | RN7 | Leica | 1:100 | +++ |
| GCDFP15 | 23A3 | Novocastra | 1:150 | ++ |
| GATA3 | L50-823 | ZETA | 1:250 | ++ |
| AR | SP107 | ZETA | 1:100 | ++ |
| Gene | Amino Acid Change | Coding | Locus | Variant Effect | Allele Frequency |
|---|---|---|---|---|---|
| TPR | p.(D1348H) | c.4042G>C | chr1:186308883 | missense | 16.82% |
| LRP1B | p.(D41N) | c.121G>A | chr2:142567932 | missense | 4.41% |
| NFE2L2 | p.(F246S) | c.737T>C | chr2:178096594 | missense | 53.28% |
| LTF | p.(R23dup) | c.68_69insAAG | chr3:46501284 | Inframe insertion | 99.95% |
| PIK3CA | p.(K111_L113del) | c.333_341delGATCCTCAA | chr3:178916943 | Inframe deletion | 24.73% |
| TET2 | p.(H863Y) | c.2587C>T | chr4:106157686 | missense | 13.31% |
| WRN | p.(P982S) | c.2944C>T | chr8:30989999 | missense | 45.58% |
| CDKN2B | p.(A38T) | c.112G>A | chr9:22008841 | missense | 4.00% |
| TAF1L | p.(M155I) | c.465G>A | chr9:32635113 | missense | 15.25% |
| RALGDS | p.(T883I) | c.2648C>T | chr9:135974068 | missense | 8.05% |
| SUFU | p.(P18S) | c.52C>T | chr10:104263961 | missense | 5.56% |
| EP400 | p.(P35S) | c.103C>T | chr12:132445267 | missense | 4.97% |
| ERCC5 | p.(D703G) | c.2108A>G | chr13:103518170 | missense | 46.35% |
| CDH1 | unknown | c.687+1G>T | chr16:68842752 | splice donor variant | 27.08% |
| FANCA | p.(R591Q) | c.1772G>A | chr16:89845355 | missense | 89.43% |
| NLRP1 | p.(V1241L) | c.3721G>C | chr17:5424906 | missense | 55.09% |
| NLRP1 | p.(M1119V) | c.3355A>G | chr17:5433966 | missense | 51.70% |
| NLRP1 | p.(T995I) | c.2984C>T | chr17:5437285 | missense | 48.10% |
| NLRP1 | p.(T878M) | c.2633C>T | chr17:5445243 | missense | 47.70% |
| NLRP1 | p.(T782S) | c.2345C>G | chr17:5461671 | missense | 52.24% |
| NLRP1 | p.(T246S) | c.737C>G | chr17:5463279 | missense | 47.73% |
| ERBB2 | p.(V777L) | c.2329G>T | chr17:37881000 | missense | 13.26% |
| RNF213 | p.(A5021V) | c.15062C>T | chr17:78363034 | missense | 49.92% |
| CDH2 | p.(E38K) | c.112G>A | chr18:25727697 | missense | 7.50% |
| STK11 | p.(H168Y) | c.502C>T | chr19:1220409 | missense | 4.72% |
| JAK3 | p.(G936V) | c.2807G>T | chr19:17942208 | missense | 9.55% |
| AXL | p.(I252V) | c.754A>G | chr19:41737174 | missense | 51.61% |
| TAF1 | p.(V803I) | c.2407G>A | chrX:70607231 | missense | 7.46% |
| TAF1 | p.(G804S) | c.2410G>A | chrX:70607234 | missense | 5.97% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, L.-C.; Lin, T.-C.; Yeh, Y.-C.; Ho, H.-L.; Tsai, C.-C.; Chou, T.-Y. Primary Signet Ring Cell/Histiocytoid Carcinoma of the Eyelid: Somatic Mutations in CDH1 and Other Clinically Actionable Mutations Imply Early Use of Targeted Agents. Curr. Oncol. 2021, 28, 918-927. https://doi.org/10.3390/curroncol28010090
Wang L-C, Lin T-C, Yeh Y-C, Ho H-L, Tsai C-C, Chou T-Y. Primary Signet Ring Cell/Histiocytoid Carcinoma of the Eyelid: Somatic Mutations in CDH1 and Other Clinically Actionable Mutations Imply Early Use of Targeted Agents. Current Oncology. 2021; 28(1):918-927. https://doi.org/10.3390/curroncol28010090
Chicago/Turabian StyleWang, Lei-Chi, Tai-Chi Lin, Yi-Chen Yeh, Hsiang-Ling Ho, Chieh-Chih Tsai, and Teh-Ying Chou. 2021. "Primary Signet Ring Cell/Histiocytoid Carcinoma of the Eyelid: Somatic Mutations in CDH1 and Other Clinically Actionable Mutations Imply Early Use of Targeted Agents" Current Oncology 28, no. 1: 918-927. https://doi.org/10.3390/curroncol28010090
APA StyleWang, L.-C., Lin, T.-C., Yeh, Y.-C., Ho, H.-L., Tsai, C.-C., & Chou, T.-Y. (2021). Primary Signet Ring Cell/Histiocytoid Carcinoma of the Eyelid: Somatic Mutations in CDH1 and Other Clinically Actionable Mutations Imply Early Use of Targeted Agents. Current Oncology, 28(1), 918-927. https://doi.org/10.3390/curroncol28010090