Abstract
Caseous calcification of the mitral annu-lus (CCMA) is a rare variant of mitral annular calcification, which can be difficult to diagnose and can be misdiag-nosed as a cardiac tumour or abscess. Multimodality imaging is important for the diagnosis of this entity and to avoid unnecessary surgical treatment. We present the case of a 77-year-old female patient with initially asymp-tomatic CCMA who later developed third degree atrioven-tricular heart block. Four years after the initial diagnosis, she was admitted to hospital for acute heart failure due to mitral stenosis. Multimodality imaging including transthoracic and transoesophageal echocardiography, and computed tomography showed an increase in the size of the caseous calcification with symptomatic mitral stenosis.
Introduction
Caseous calcification of the mitral annulus is a rare finding [1,2]. It is commonly misdiagnosed as an abscess or a tumour of the mitral valve annulus [1]. As it is a benign process, an accurate diagnosis is important to avoid erroneous management and potentially unnecessary surgery in asymptomatic patients.
Case report
A 77-year-old female patient presented to the emergency department with several days of worsening dyspnoea. Her past medical history was significant for hypertension, dyslipidaemia, obesity, type II diabetes, cognitive impairment and mobility difficulties due to a polyradiculopathy.
A routine transthoracic echocardiogram (TTE) performed 4 years previously, with a view to orthopaedic surgery, had revealed a cardiac mass attached to the posterior mitral annulus with a mitral mean gradient of 6 mm Hg (at a heart rate of 80 beats per minute). At that time cardiac magnetic resonance imaging (cMRI) and computed tomography (CT) were performed and the diagnosis of caseous calcification of the mitral annulus was established (Figure 1). Two years after the initial diagnosis, the patient developed third degree atrioventricular block for which a dual-chamber pacemaker was implanted. The patient was asymptomatic for a further 2 years until she developed an episode of acute severe dyspnoea.
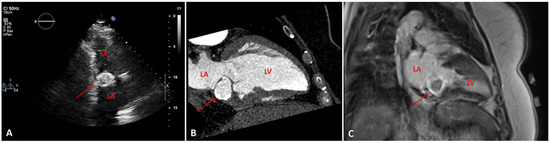
Figure 1.
A. transthoracic echocardiogram, two-chamber view showing a posterior mitral annulus caseous calcification (arrow), which appears as a well-defined brightened edge corresponding to an echodense periphery, and a central echolucent area corresponding to the central liquefaction. B. Computed tomography scan, showing a well-defined oval or crescent-shaped hyperdense mass with peripheral calcification (arrow). C. Late gadolinium enhancement-magnetic resonance imaging sequence, showing caseous calcification of the mitral annulus as a hypointense zone without late gadolinium enhancement (arrow). LV: left ventricle; LA: left atrium
In the emergency department the patient’s vital signs (oxygen saturation 88%), clinical examination (tachypnoea, orthopnoea, bilateral lung crackles), laboratory tests (elevated N-terminal pro-B-type natriuretic peptide [NT-proBNP]) and chest X-ray (lung congestion) confirmed the diagnosis of acute heart failure, albeit of unclear aetiology: her blood pressure was only mildly increased, mild troponin elevation argued against an acute coronary syndrome, haemoglobin levels and heart rate were stable (Table 1). The patient was admitted for oxygen supplementation and intravenous diuretics with rapid recovery ensuing in a few days. A TTE documented normal heart function but an increase in the size of the cardiac mass ( 46 mm × 31 mm compared with 36 mm × 27 mm 4 years before), the mean gradient across the mitral valve was unchanged at 6–7 mm Hg at a heart rate of 65 bpm (Figure 2) The mitral valve area obtained by two-dimensional planimetry from the parasternal short axis view was 1.2 cm2 (Figure 3B). No other significant valve disease was found. Transoesophageal echocardiography (TOE) showed moderate mitral stenosis. The mitral valve orifice measured by three-dimensional planimetry was 1.4 cm2 (Figure 3A). Remarkably, there was an increase in the mean diastolic mitral gradient from 6 mm Hg at the time of the TTE to 13 mm Hg on TOE, probably due to a higher heart rate of 85 bpm (Figure 5). A CT scan showed an increased size of the mass (Figure 4). Due to the frailty of the patient and in accordance with her wish not to undergo any invasive treatment, surgery was not proposed. The patient was discharged before being admitted 2 months later for another episode of acute heart failure treated with intravenous diuretics. The therapeutic attitude was altered and at this time the patient was again discharged for ambulatory follow up for treatment adjustment and only symptomatic management if acute heart failure happens again.

Table 1.
Principal clinical and biological values which could contribute to the acute heart failure or which may affect echocardiographic measures, showing no changes overtime.
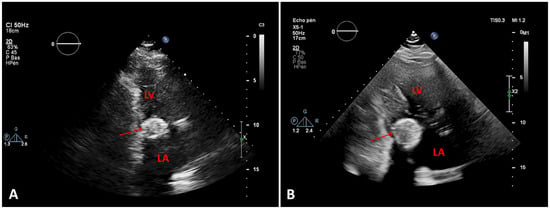
Figure 2.
A. First transthoracic echocardiogram (TTE), two-chamber view, at the time of diagnosis B. TTE 4 years later, showing the increasing size of the caseous calcification of the mitral annulus (arrows). LV: left ventricle; LA: left atrium
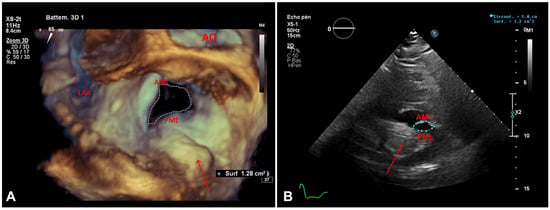
Figure 3.
A. Transoesophageal echocardiogram, three-dimensional planimetry of the mitral valve orifice (surgical view) and the (arrow). PML: posterior mitral leaflet; AML: anterior mitral leaflet, AO: aortic valve, LAA: left atrial appendage. B. Transthoracic echocardiogram, two-dimensional planimetry of the mitral valve orifice on parsternal short axis view and the c(arrow). PML: posterior mitral leaflet: AM anterior mitral leaflet.
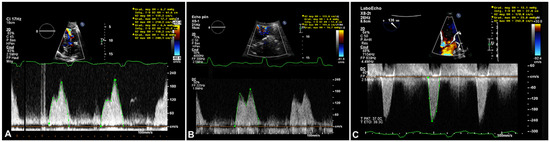
Figure 5.
A. Transthoracic echocardiogram (TTE), continuous Doppler transmitral mean gradient (6 mm Hg at 80 bpm) on initial presentation in 2016 B. TTE, continuous Doppler transmitral mean gradient (6–7 mm Hg at 65 bpm) 4years later in 2020. C. Transoesophageal echocardiogram, continuous Doppler transmitral mean gradient (6–13 mm Hg at 85 bpm) in 2020.
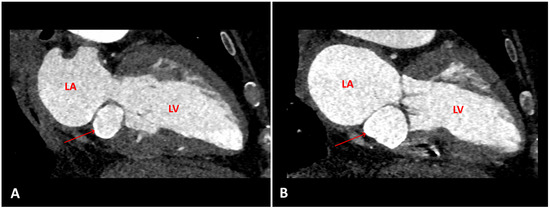
Figure 4.
A. Computed tomography (CT) scan, two chambers, at the time of diagnosis. B. CT scan, same view, 4 years later, showing the increasing size of the (arrows). LV = left ventricle, LA = left atrium
Discussion
- Pathogenesis and prevalence
Mitral annular calcification is a relatively common degenerative condition of the mitral valve, usually involving the posterior annulus, in some series affecting 8.5% of the general population [2].
Caseous calcification of the mitral annulus is a rare variant of mitral annular calcificationand occurs when there is liquefaction and caseous degeneration (caseous typically refers to a category of necrosis, which is encountered in tuberculosis) of the calcified annulus, but the exact mechanism is unknown [1]. It tends to occur more often in elderly women and is associated with hypertension and patients with chronic renal failure or altered calcium-phosphate metabolism [3,5]. Macroscopically, caseous calcification of the mitral annulus appears like a calcified envelope that surrounds caseous materiel inside (described as a toothpaste-like, milky, material) [1]. This contrasts with classical mitral annular calcification, which usually lacks central hypoechoic area, tends to be less rounded in shape and extend to a greater portion of the posterior mitral annulus. Less frequently, the differential diagnosis includes radiation-induced mitral annulus calcification (usually involving the aorto-mitral curtain) or, rarely, cardiac tumours. The true prevalence of caseous calcification of the mitral annulus is unknown. Based on several series it may vary between 0.63 and 0.64% of the 10.6% of patients with MAC found on echocardiography [3,4]. A higher prevalence of casesous calcification of 2.7% was found in a necropsy series of mitral annular calcification[1].
Clinical manifestation
The most common symptoms are palpitations and dyspnoea, but rarely patients may present syncope secondary to atrioventricular blocks, as did our patient. This is possibly due to direct extension of calcific deposits to the area of the atrioventricular node and the bundle of His. Less often, systemic embolisation can occur [1,3,6,11]. Moreover, the presence of mitral annular calcification is associated with increased cardiovascular events and mortality, as well as with significant obstructive coronary artery disease. Possible reasons for these results are that mitral annular calcification may be a marker for atherosclerotic disease burden, or that other unmeasured influences, such as metabolic, inflammatory and haemostatic risk factors, might be responsible for the increased risk of cardiovascular disease and mortality in these patients [11].
Multimodal imaging
On transthoracic echocardiography (TEE), appears as a round calcification, with well-defined brightened edges corresponding to an echodense periphery, and a central echolucent area corresponding to the central liquefaction area. Colour Doppler shows a lack of flow inside the central zone [1,7]. Differences between mitral annular calcification and caseous calcification on TEE are summarised on Table 2 and illustrated in Figure 6.
Table 2.
Differences between mitral annular calcification (MAC) and caseous calcification of the mitral annulus (CCMA) on transthoracic echocardiography.
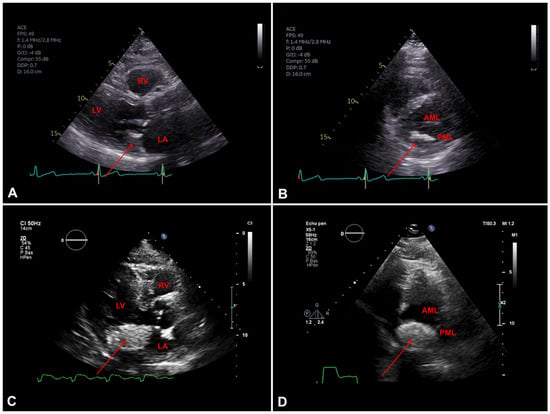
Figure 6.
A. Transothoracic echocardiography (TTE) parasternal long axis view showing mitral annular calcification (MAC) (arrow), LV: left ventricle; LA: left atrium; RV: right ventricule. B. TTE parasternal short axis view showing mitral valve with MAC (arrow), PML: posterior mitral leaflet; AML: anterior mitral leaflet. C. TTE parasternal long axis view showing (arrow), LV:left ventricle LA: left atrium;RV: right ventricule. D. TTE parasternal short axis view showing mitral valve with caseous calcification (arrow), PML: posterior mitral leaflet; AML: anterior mitral leaflet.
Transoesophageal echography (TOE) can be performed to better characterise the mass in patients with poor echographic windows, to better quantify mitral regurgitation, if present, and better delineate its anatomic boundaries
On CT scan, appears as a well-defined oval or crescentshaped hyperdense mass with peripheral calcification, with high Hounsfield units and lack of contrast enhancement [1,7,8].
Cardiac MRI may be helpful in equivocal cases. CCMA is seen as a hypointense zone both in T1- and T2-weighted sequences. In postcontrast studies, contrast enhancement on first-pass sequences is not found; however, there may be peripheral enhancement during delayed postcontrast sequences [7,9,10].
Treatment
Caseous calcification of the mitral annulus is considered as a benign tumour and conservative medical treatment (follow up, diuretics) is indicated for asymptomatic patients. Surgical treatment is considered when mitral valvular dysfunction is present (regurgitation or stenosis), when embolic events occur or when it is not possible to exclude a malignant tumour with noninvasive diagnostic tools.
Conclusion
Caseous calcification of the mitral annulus is a rare benign finding, likely underreported and may be confused with tumours or abscess. Clinical manifestations vary from lack of symptoms to acute heart failure due to mitral valve dysfunction (stenosis or regurgitation) and may include syncope secondary to atrioventricular block, and stroke. Multimodality imaging is often necessary to establish the diagnosis, to decide on the best treatment and avoid often times unnecessary surgery.
Disclosure statement
No financial support and no other potential conflict of interest relevant to this article was reported.
Guarantor of submission
The corresponding author is the guarantor of submission.
Funding information
The authors have no funding to report
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analysed during the current study
References
- Elgendy, I.Y.; Conti, C.R. Caseous calcification of the mitral annulus: a review. Clin Cardiol. 2013, 36, E27–E31. [Google Scholar] [CrossRef] [PubMed]
- Pomerance, A. Pathological and clinical study of calcification of the mitral valve ring. J Clin Pathol. 1970, 23, 354–361. [Google Scholar] [CrossRef] [PubMed]
- Deluca, G.; Correale, M.; Ieva, R.; Del Salvatore, B.; Gramenzi, S.; Di Biase, M. The incidence and clinical course of caseous calcification of the mitral annulus: a prospective echocardiographic study. J Am Soc Echocardiogr. 2008, 21, 828–833. [Google Scholar] [CrossRef] [PubMed]
- Harpaz, D.; Auerbach, I.; Vered, Z.; Motro, M.; Tobar, A.; Rosenblatt, S. Caseous calcification of the mitral annulus: a neglected, unrecognized diagnosis. J Am Soc Echocardiogr. 2001, 14, 825–831. [Google Scholar] [CrossRef] [PubMed]
- Akram, M.; Hasanin, A.M. Caseous mitral annular calcification: is it a benign condition? J Saudi Heart Assoc. 2012, 24, 205–208. [Google Scholar] [CrossRef] [PubMed]
- Gulati, A.; Chan, C.; Duncan, A.; Raza, S.; Kilner, P.J.; Pepper, J. Multimodality cardiac imaging in the evaluation of mitral annular caseous calcification. Circulation. 2011, 123, e1–e2. [Google Scholar] [CrossRef] [PubMed]
- Hamdi, I.; Chourabi, C.; Arous, Y.; Ghommidh, M.; Houissa, K.; Haggui, A.; et al. Multimodality imaging assessment of a caseous calcification of the mitral valve annulus. J Saudi Heart Assoc. 2018, 30, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Biteker, M.; Duran, N.E.; Ozkan, M. Caseous calcification of the mitral annulus imaged with 64-slice multidetector CT. Echocardiography. 2009, 26, 744–745. [Google Scholar] [CrossRef] [PubMed]
- Monti, L.; Renifilo, E.; Profili, M.; Balzarini, L. Cardiovascular magnetic resonance features of caseous calcification of the mitral annulus. J Cardiovasc Magn Reson. 2008, 10, 25. [Google Scholar] [CrossRef] [PubMed]
- Balci, S.; Akkaya, S.; Ardali, S.; Hazirolan, T. Caseous necrosis of mitral annulus. Case Rep Radiol. 2015, 2015, 561329, Edifix has not found an issue number in the journal reference. Please check the volume/issue information. (Ref. 10 "Balci, Akkaya, Ardali, Hazirolan, 2015"). [Google Scholar] [CrossRef] [PubMed]
- Abramowitz, Y.; Jilaihawi, H.; Chakravarty, T.; Mack, M.J.; Makkar, R.R. Mitral Annulus Calcification. J Am Coll Cardiol. 2015, 66, 1934–1941. [Google Scholar] [CrossRef] [PubMed]
© 2021 by the author. Attribution Non-Commercial NoDerivatives 4.0.