Case Report
A 49-year-old man with a history of sarcoidosis and associated severe pulmonary hypertension was referred for myocardial perfusion imaging (MPI) because of preoperative workup (planed lung transplant). A recent right heart catheterisation had revealed a mean pulmonary artery pressure of 62 mm Hg.
The ECG at rest showed sinus rhythm with right-axis deviation, P-pulmonale, incomplete right-bundle-branch-block, and strain in lead V1 to V3 (Figure 1). Due to severe dyspnoea und muscle weakness pharmacologic MPI was performed. During the test, the patient did not experience any symptoms apart from flushing, and the ECG did not demonstrate any ischaemic changes. Rest 201Tl/stress (adenosine) 99mTc sestamibi single-photon emission computed tomography (SPECT; Figure 2) revealed a markedly dilated and hypertrophied right ventricle with flattened interventricular septum during both systole and diastole, thus resulting in the picture of a “D-shaped” left ventricle. Tracer uptake in the interventricular septum was decreased both at rest and during stress. Otherwise, tracer up-take in the left ventricular myocardium was normal. Transthoracic echocardiography confirmed the presence of a dilated and hypertrophied right ventricle. Right ventricular function was moderately impaired, and there was moderate tricuspid regurgitation. A systolic right ventricular pressure of 65 mm Hg plus right atrial pressure (which was significantly elevated as indicated by marked dilation of the inferior vena cava and the hepatic veins) was calculated from the tricuspid regurgitation jet velocity. The left ventricle was normal-sized and non-hypertrophied but had an obvious “D-shaped” morphology (Figure 3).
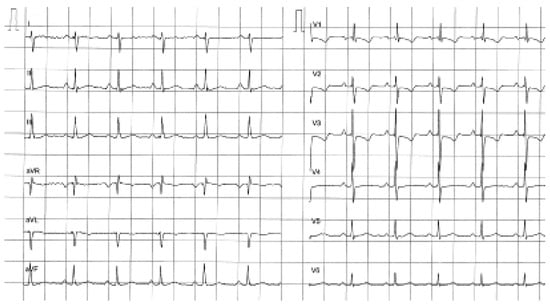
Figure 1.
ECG at rest showing sinus rhythm with right-axis deviation, P-pulmonale, incomplete right-bundlebranch-block, and strain in lead V1 to V3.
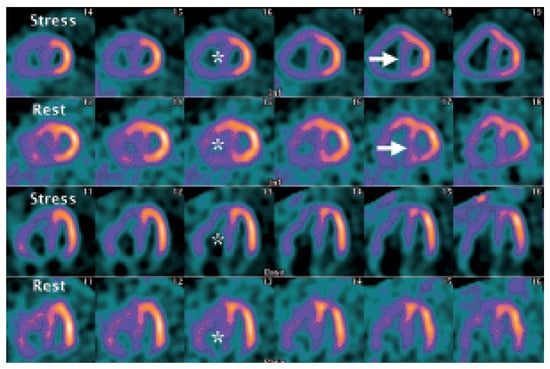
Figure 2.
Rest 201Tl/stress (adenosine) 99mTc sestamibi SPECT (short axis view and horizontal long axis view) showing a dilated and hypertrophied right ventricle with flattened interventricular septum (arrows) and decreased tracer uptake in the interventricular septum both at rest and during stress (*).
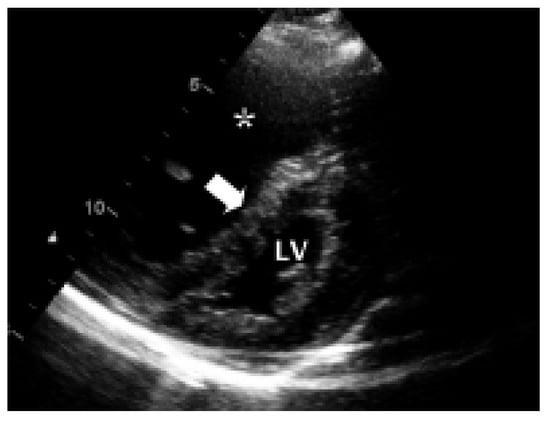
Figure 3.
Transthoracic echocardiogram (parasternal short axis view) showing a large right ventricle (uncompletely shown, *) and small left ventricle (LV) with marked systolic flattening of the interventricular septum (arrow), leading to the aspect of a “D-shaped” left ventricle.
Discussion
During myocardial perfusion SPECT studies, the right ventricle most often is only faintly and incompletely visualised. The presence of right ventricular uptake which allows good delineation of the ventricle may be suggestive for right ventricular hypertrophy due to pressure or volume overload [1]. However, other SPECT signs of right ventricular pathologies are not well defined. The present case demonstrates that apart from right ventricular hypertrophy, flattening of the interventricular septum is a feature of significant pulmonary artery hypertension also during myocardial perfusion SPECT studies. This phenomenon of the “Dshaped” left ventricle, ie flattening of the interventricular septum during both systole and diastole in right ventricular pressure overload (or only during diastole in right ventricular volume overload) as seen during echocardiographic studies has been known for a long time. However, the analogous phenomenon has only very recently been described during SPECT [2]. Among eight patients with flattened interventricular septum, seven had an elevated systolic pulmonary artery pressure as estimated by echocardiographic measurements [2].
A surprising finding in the present patient was the abnormal tracer up-take in the septum both at rest and during rest, thus mimicking a fixed defect formally most likely consistent with a scar. This finding is not entirely clear, and we are not aware of similar reports. Data from a canine model suggest that acute right ventricular pressure overload (induced by pulmonary artery banding) significantly compromises septal coronary blood flow [3], which led to the speculation that angina-like chest pain in patients with pulmonary hypertension but normal epicardial coronary arteries might reflect ischaemia due to septal compression [3].
In conclusion, the presence of a hypertrophied right ventricle and a “D-shaped” left ventricle are important features of pulmonary artery hypertension not only during echocardiography but also MPI studies. The impact of a decreased tracer up-take in the interventricular septum remains to be evaluated.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Khaja, F.; Alam, M.; Goldstein, S.; Anbe, D.T.; Marks, D.S. Diagnostic value of visualization of the right ventricle using thallium-201 myocardial imaging. Circulation 1979, 59, 182–188. [Google Scholar] [CrossRef]
- Movahed, M.R.; Hepner, A.; Lizotte, P.; Milne, N. Flattening of the interventricular septum (D-shaped left ventricle) in addition to high right ventricular tracer uptake and increased right ventricular volume found on gated SPECT studies strongly correlates with right ventricular overload. J. Nucl. Cardiol. 2005, 12, 428–434. [Google Scholar] [CrossRef] [PubMed]
- Gibbons Kroeker, C.A.; Adeeb, S.; Shrive, N.G.; Tyberg, J.V. Compression induced by RV pressure overload decreases regional coronary blood flow in anaesthetised dogs. Am. J. Physiol. Heart Circ. Physiol. 2006, 290, H2432–H2438. [Google Scholar] [CrossRef] [PubMed]



© 2007 by the author. Attribution - Non-Commercial - NoDerivatives 4.0.