

Creating Family-Centred Support for Preschoolers with Developmental Disabilities in Low-Income Countries: A Rapid Review to Guide Practitioners


Abstract
1. Introduction
2. The Art of the Possible
- There has been an accumulation of knowledge and skills over the past 20 years as to how preschoolers with disabilities—those aged 0 to 6 years—can be helped [4,5]. These have come from within and across nations, especially in richer countries but also countries with fewer resources. We can confidently claim that the development of all preschoolers can be enhanced, and we can specify practical ways of doing this.
- Families are the main caregivers and educators of preschoolers all over the world. In low-income countries, often they are the only ones available to assist boys and girls with disabilities. Hence, parents are the bedrock for creating better lives for disabled preschoolers. Most mothers and grandmothers rise willingly to the challenge, as will many but not all fathers. Hence, support for the child needs to be delivered through support for their family carers and it has been shown to be effective [6].
- Even within the most impoverished communities, families have found ways of coping with adversity while demonstrating remarkable resilience. Moreover, they can draw upon their indigenous knowledge and cultural heritage in rearing their children, allied with the support of their relatives and local community [7]. Discovering ways of mobilising family and community supports creates an essential asset.
- People of good intent are present in every community. Their motivation to assist others in need, allied with knowledge of what practical steps they can take, is a powerful contributor to success. Among those who might instigate support for families who have a preschooler with disabilities within local communities could be parents of older children with disabilities, unpaid and paid community workers, community and religious leaders, professionals such as therapists, teachers, social workers, and local politicians and government officials. In truth though, it could be anyone with a heart to help their fellow citizens and the confidence to approach others for the cause. Identifying likely and available leaders of new support services is a key ingredient of creating change [8].
- Admittedly, the impetus for creating community-based services and supports for persons with disabilities has mostly come from outside the local community, albeit with the intention of sharing ownership of the project with leaders from that community. This external form of leadership has tended to come from national and international Non-Governmental Organisations (NGOs), Disabled Persons Organisations, or Parent-led Associations, but also from front-line health and social services and educational professionals [9]. Arguably, some of these external supports are or could be present in nearly all communities in all countries. Supports for families of preschoolers with developmental disabilities may not feature at all in their current workload and few may be currently motivated to include them, but some will be prepared to do so. This article may also serve to challenge and inform practitioners in these external organisations as to how they might instigate and support local community responses for this marginalised group of families.
3. An International Imperative
- International statements on rights of children and of persons with disabilities have been mostly incorporated into national laws and policies. They emphasise that discrimination based on disability is unacceptable if not unlawful. For example, Article 23.3 of the Convention on the Rights of the Child states: “Recognizing the special needs of a disabled child, assistance … shall be designed to ensure that the disabled child has effective access to and receives education, training, health care services, rehabilitation services, preparation for employment and recreation opportunities in a manner conducive to the child’s achieving the fullest possible social integration and individual development, including his or her cultural and spiritual development”. (last accessed on February 2024).
- There has been a shameful lack of progress in responding to the needs of preschoolers with disabilities. A recent review undertaken by the Collaboration for Global Research on Developmental Disabilities [10] noted that over 53 million preschoolers globally have a developmental disability with an overall prevalence rate of 7.5% among under fives. Yet, an analysis of the funding provided by Development Assistance for Health to low- and middle-income countries [11] which totalled USD 76.3 billion during 2009 to 2016 found only USD 0.7 billion (2% of the total) was for disability. Moreover, this funding declined over that period despite an increasing prevalence rate [12]. Consequently, governments seemingly have neither requested nor been given or found the financial resources to address the needs of these preschoolers. This neglect is unjust.
- These preschoolers and their families experience multiple disadvantages, chief of which is poverty allied with poor physical infrastructures, such as housing, sanitation, and transport [13,14]. Responding to these needs arguably could bring benefits to other households experiencing similar difficulties in the community, especially as the empowerment of local people is a central response in meeting these needs, as will become apparent in later sections. Strategies to help a few can result in many benefitting.
- Creating educational systems that are inclusive of pupils with disabilities is an international imperative to achieve the sustainable development goals agreed by the world’s nations. For example, Sustainable Development Target 4.2 requires that by 2030, “all girls and boys have access to quality early childhood development, care, and pre-primary education so that they are ready for primary education”. (http://www.un.org/sustainabledevelopment/sustainable-development-goals: accessed on 1 February 2024). The foundations need to be laid in the preschool years both in terms of boosting parental engagement in the child’s education and through the provision of early childhood education centres. Yet, fewer than 30% of preschoolers in many African countries, for example, attend such centres [15].
Common Causes of Inaction
- The stigma around disability persists in many communities which has created shame in families and an unwillingness to request assistance. Likewise, parents have been shunned and faced ridicule even from their own relatives. Well-tested strategies have been identified for reducing stigma [16], most notably through the building of personal relationships among the affected families and in turn with their community neighbours. More positive attitudes result in increases in the child’s social inclusion [17].
- The lack of knowledge within families and community services on how best to help the child manifests in feelings of helplessness and hopelessness, and ultimately in the exclusion of the child from health services and preschool education. A necessary response is the provision of learning opportunities to families and to community personnel, allied with their personal experience of seeing the children progress [11].
- Preschoolers with disabilities are not a priority in low-income countries when so many other groups also have unmet needs [18]. Nevertheless, new or extra resources are not necessarily required by these families or the children. Rather, supports provided to other groups should be made inclusive of their needs, be it for income generation, improved housing, and transport [19]. But for this to happen, the above two points need to be addressed.
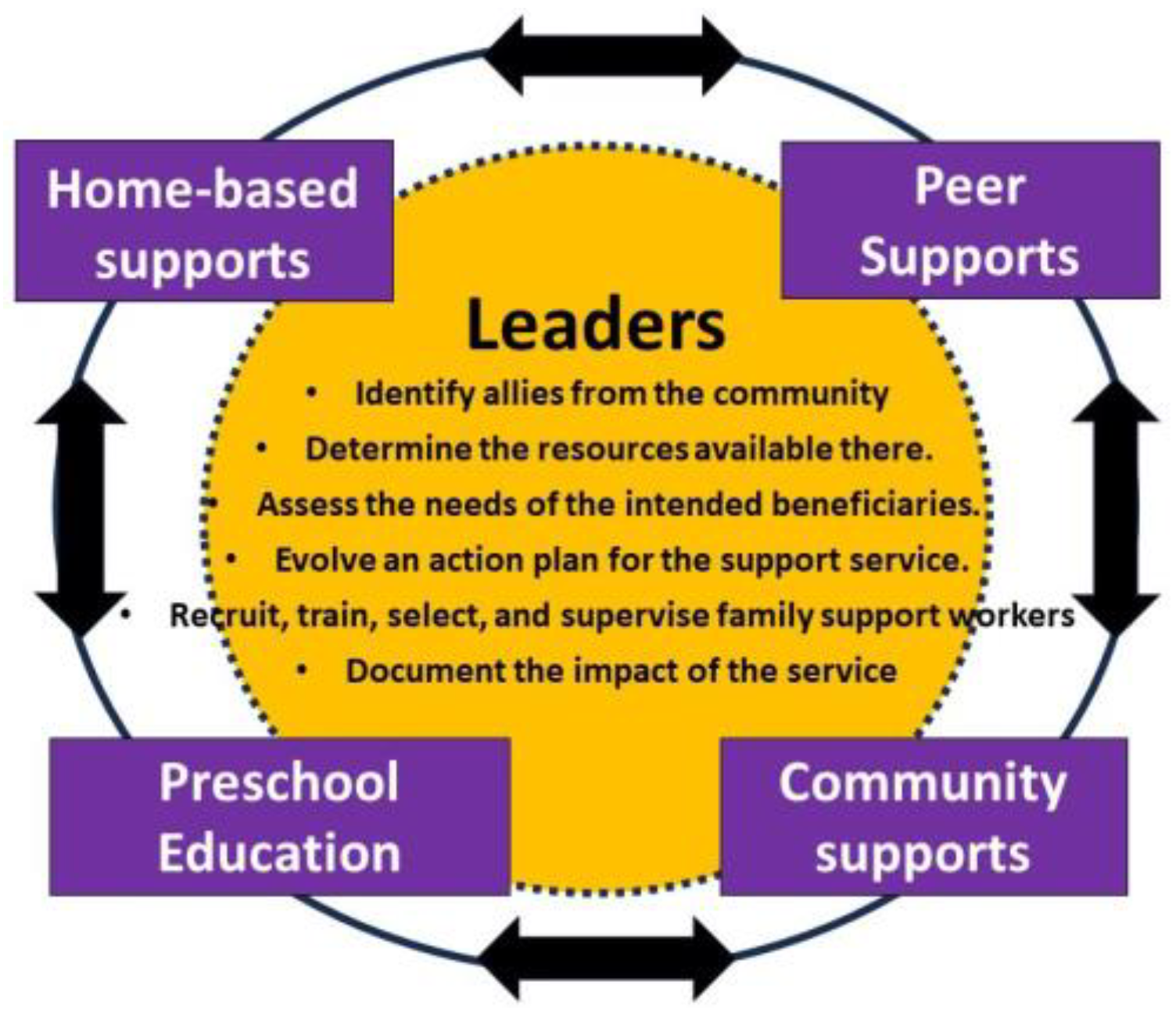
4. Making a Start—The Role of Service Leaders
4.1. Leadership
4.1.1. Identify Allies from Within the Community
4.1.2. Determine the Resources Available in the Community
4.1.3. Assess the Needs of the Intended Beneficiaries
4.1.4. Evolve an Action Plan for the Support Service
5. What Is Meant by Family-Centred Supports?
- Sharing knowledge and information with parents so that families can make informed decisions.
- Respect for families’ culture, beliefs, and values.
- Recognising and building on family members’ strengths and resources, and active participation by family members in assessments of the child’s needs and developmental interventions.
- Psycho-social supports to enhance mothers’ emotional wellbeing and increase their feelings of self-advocacy.
- Encouraging advocacy by families in support of their rights.
- Providing or mobilising supports and resources in response to family concerns and priorities.
6. Creating Family-Centred Support Services
6.1. Recruiting Family Support Workers
6.2. Basic Training and Selection
6.3. Ongoing Training and Support
7. Home Visits
7.1. Identifying the Child’s Strengths and Needs
7.2. Children’s Health and Nutrition
7.3. Identifying the Needs of the Main Caregiver
7.4. Individual Family Plans
8. Mobilising Peer Support for Families
8.1. Sharing Information and Experiences
8.2. Joint Advocacy
8.3. Income Generation
9. Mobilising Community Support
9.1. Traditional Healers and Faith Communities
9.2. Health and Social Services
9.3. Poverty Alleviation
9.4. Approaching Community Groups
- Engage the target community in conversations based around stories of the children and their progress: how they and their families have been helped. Give them the opportunity to meet some of the children and their caregivers. Pose the question: what could you do to help?
- Offer your assistance to them and assure them that you envisage a partnership that will be mutually beneficial.
- Identify the potential change leaders in the community and build a trusted relationship with them.
- Positively affirm their efforts to include the children and give them the credit for their achievements.
10. Preschool Education
10.1. Partnering with Existing Centres
10.2. Creating Preschool Educational Opportunities
11. Documenting and Sharing the Impact of the Service
- Creating a database that collates the pertinent details. of the children and families who avail of the service.
- Documenting the various supports availed of by families: the number of home visits, attendance at group meetings, training events provided, and so forth.
- Providing a computer-based pro forma for documenting individual family plans that can be updated in terms of goals achieved for both the child and the caregiver.
- Maintaining a diary of meetings held and the outcomes from them, especially with respect to mobilising communities.
- Obtaining feedback from families about the supports they have been given. This can be achieved through interviews with a sample of families and/or in group meetings.
- Organising celebrations of significant achievements—such as parties and concerts—for families, support staff, and volunteers.
- Keeping financial accounts of income and expenditure. This will assist in making estimates of the cost benefits arising from the supports provided.
- The above information can be brought together into an annual report accompanied by photographs and infographics highlighting the main outcomes from the support service. The report can be shared with print and broadcast media to inform local communities and provide positive news stories to counter the stigma around disability. The report can be used to lobby decision-makers in local and national government for resources to further develop community supports.
Planning for Sustainability
12. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. How the Review Was Conducted

{kind=link}
| Reference Number | Topic (Year Published) | Type of Review | Number of Studies | Total Cases 1 |
|---|---|---|---|---|
| [3] | Asset-based approaches to promote health in communities (2020) | Scoping review | 50 | Not given |
| [5] | Strategies for addressing the needs of children with or at risk of developmental disabilities in early childhood (2024) | Systematic umbrella review of reviews | 18 reviews of 251 studies | 1.2 million children |
| [6] | Parenting interventions to promote early child development (2021) | Systematic review and meta-analysis | 111 | >20,000 |
| [14] | Poverty and disability in low- and middle-income countries (2017) | Systematic review | 150 | Not given |
| [16] | Reducing stigma experienced by children with disabilities and their families (2020) | Systematic review | 20 | @14,600 |
| [17] | Family support and outcomes (2020) | Scoping Review | 13 | 1295 |
| [20] | Community Conversations (2018) | Unspecified review | 10 | 3100 |
| [24] | A universal model of family centered care (2019) | Scoping Review—thematic analysis | 55 | Not given |
| [25] | Stigma, Acceptance and Belonging for People with IDD Across Cultures (2020) | Literature review | 74 | Not given |
| [26] | Parenting interventions and self-efficacy (2018) | Systematic review | 25 | 1697 |
| [27] | Parental engagement in early intervention (2022) | Realist synthesis | 17 | 289 |
| [28] | Rehabilitation services for children with disabilities in LMICs (2019) | Scoping Review | 81 | Not given |
| [30] | Family-centred care in early intervention (2022) | Systematic review—narrative analysis | 42 | @4800 |
| [33] | Community support for persons with disabilities in LMICs (2022) | Scoping Review—thematic analysis | 424 | Not given |
| [41] | Healthcare access for children with disabilities (2020) | Scoping Review | 15 | @1400 |
| [43] | Healthcare-Based Interventions to Improve Parenting Outcomes in LMICs: (2022) | Systematic Review and Meta-Analysis | 8 | 6408 |
| [44] | Family quality of life in Africa (2022) | Scoping Review | 53 | Not given |
| [45] | Depression and anxiety in parents of children with intellectual and developmental disabilities (2019) | Systematic review and meta-analysis | 19 | 3303 |
| [47] | Family and parenting interventions in LMICs: child and youth mental health outcomes (2019) | Systematic Review | 32 | 6781 |
| [49] | Improving livelihood outcomes for people with disabilities in LMICs (2022) | Systematic Review | 9 | 5570 |
| [50] | The Impact of Cash Transfers (2019) | Review | 165 | Not given |
| [51] | African families’ and caregivers’ experiences of raising a child with intellectual disability (2021) | Narrative Synthesis | 9 | Not given |
| [52] | psychosocial interventions for parents and their children with intellectual disabilities in LMICs (2021) | Systematic Review | 13 | 684 |
| [56] | Barriers and facilitators to education in LMICs | Systematic review and thematic analysis | 13 | Not given |
References
- McConkey, R.; Allan, S.; Mlambo, C.; Kambarami, P.; Martin, K. Creating Family-Centred Support for Children with Developmental Disabilities in Africa. Examples of Local Community Interventions. (Paper under Review). 2024. Available online: https://www.researchgate.net/publication/380478268_Creating_Family-Centred_Support_for_Children_with_Developmental_Disabilities_in_Africa_Examples_of_Local_Community_Interventions (accessed on 13 May 2024).
- World Health Organization. World Report on Disability, 2011. WHO. Available online: https://www.who.int/publications/i/item/9789241564182 (accessed on 29 February 2024).
- Cassetti, V.; Powell, K.; Barnes, A.; Sanders, T. A systematic scoping review of asset-based approaches to promote health in communities: Development of a framework. Glob. Health Promot. 2020, 27, 15–23. [Google Scholar] [CrossRef]
- Vargas-Baron, E.; Small, J.; Wertlieb, D.; Hix-Small, H.; Gomez Botero, R.; Diehl, K.; Vergara, P.; Lynch, P. Global Survey of Inclusive Early Childhood Development and Early Childhood Intervention Programs; RISE Institute: Washington, DC, USA, 2019; Available online: https://www.unicef.org/media/126046/file/Global-Survey-of-IECD-and-ECI-Programs-2019.pdf (accessed on 29 February 2024).
- Smythe, T.; Scherer, N.; Nanyunja, C.; Tann, C.J.; Olusanya, B.O. Strategies for addressing the needs of children with or at risk of developmental disabilities in early childhood by 2030: A systematic umbrella review. BMC Med. 2024, 22, 51. [Google Scholar] [CrossRef]
- Jeong, J.; Franchett, E.E.; Ramos de Oliveira, C.V.; Rehmani, K.; Yousafzai, A.K. Parenting interventions to promote early child development in the first three years of life: A global systematic review and meta-analysis. PLoS Med. 2021, 18, e1003602. [Google Scholar] [CrossRef]
- Singal, N.; Muthukrishna, N. Education, childhood and disability in countries of the South–Re-positioning the debates. Childhood 2014, 21, 293–307. [Google Scholar] [CrossRef]
- Green, D. How Change Happens; Oxford University Press: Oxford, UK, 2016; Available online: https://library.oapen.org/bitstream/id/a2d96f5a-5189-4cf8-a876-d44eda71545f/618650.pdf (accessed on 29 February 2024).
- UNICEF. Inclusive Interventions for Children with Disabilities: An Evidence and Gap Map from Low- and Middle-Income Countries; UNICEF Innocenti—Global Office of Research and Foresight: Rome, Italy, 2022; Available online: https://www.unicef-irc.org/publications/1537-inclusive-interventions-for-children-with-disabilities-in-low-and-middle-income-countries-an-evidence-gap-map.html (accessed on 29 February 2024).
- Olusanya, B.O.; Boo, N.Y.; Nair, M.K.; Samms-Vaughan, M.E.; Hadders-Algra, M.; Wright, S.M.; Breinbauer, C.; Almasri, N.; Moreno-Angarita, M.; Arabloo, J.; et al. Accelerating progress on early childhood development for children under 5 years with disabilities by 2030. Lancet Glob. Health 2022, 10, e438–e444. [Google Scholar] [CrossRef]
- Institute for Health Metrics and Evaluation. Financing Global Health Visualization; IHME; University of Washington: Seattle, WA, USA, 2020; Available online: http://vizhub.healthdata.org/fgh/ (accessed on 29 February 2024).
- Olusanya, B.O.; Davis, A.C.; Wertlieb, D.; Boo, N.Y.; Nair, M.K.C.; Halpern, R.; Kuper, H.; Breinbauer, C.; De Vries, P.J.; Gladstone, M.; et al. Developmental disabilities among children younger than 5 years in 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Glob. Health 2018, 6, e1100–e1121. [Google Scholar] [CrossRef]
- Emerson, E.; Llewellyn, G. The circumstances of children with and without disabilities or significant cognitive delay living in ordinary households in 30 middle-and low-income countries. Disabilities 2021, 1, 174–186. [Google Scholar] [CrossRef]
- Banks, L.M.; Kuper, H.; Polack, S. Poverty and disability in low-and middle-income countries: A systematic review. PLoS ONE 2017, 12, e0189996. [Google Scholar] [CrossRef]
- Lu, C.; Cuartas, J.; Fink, G.; McCoy, D.; Liu, K.; Li, Z.; Daelmans, B.; Richter, L. Inequalities in early childhood care and development in low/middle-income countries: 2010–2018. BMJ Glob. Health 2020, 5, e002314. [Google Scholar] [CrossRef]
- Smythe, T.; Adelson, J.D.; Polack, S. Systematic review of interventions for reducing stigma experienced by children with disabilities and their families in low-and middle-income countries: State of the evidence. Trop. Med. Int. Health 2020, 25, 508–524. [Google Scholar] [CrossRef]
- Nuri, R.P.; Batorowicz, B.; Aldersey, H.M. Family support and family and child-related outcomes among families impacted by disability in low-and middle-income countries: A scoping review. J. Child Health Care 2020, 24, 637–654. [Google Scholar] [CrossRef]
- ACPF. The African Report on Children with Disabilities: Promising Starts and Persisting Challenges; The African Child Policy Forum (ACPF): Addis Ababa, Ethiopia, 2014; Available online: https://africanchildforum.org/index.php/en/sobipro?sid=175 (accessed on 29 February 2024).
- World Health Organization; UNICEF. Global Report on Children with Developmental Disabilities: From the Margins to the Mainstream; World Health Organization: Geneva, Switzerland; United Nations Children’s Fund (UNICEF): New York City, NY, USA, 2023; Available online: https://www.who.int/publications/i/item/9789240080539 (accessed on 29 February 2024).
- Carter, E.W.; Bumble, J.L. The promise and possibilities of community conversations: Expanding opportunities for people with disabilities. J. Disabil. Policy Stud. 2018, 28, 195–202. [Google Scholar] [CrossRef]
- Kuper, H.; Hameed, S.; Reichenberger, V.; Scherer, N.; Wilbur, J.; Zuurmond, M.; Mactaggart, I.; Bright, T.; Shakespeare, T. Participatory Research in Disability in Low- and Middle-Income Countries: What have we Learnt and what Should we Do? Scand. J. Disabil. Res. 2021, 23, 328–337. [Google Scholar] [CrossRef]
- Bailey, D.B., Jr.; Bruder, M.B.; Hebbeler, K.; Carta, J.; Defosset, M.; Greenwood, C.; Kahn, L.; Mallik, S.; Markowitz, J.; Spiker, D.; et al. Recommended outcomes for families of young children with disabilities. J. Early Interv. 2006, 28, 227–251. [Google Scholar] [CrossRef]
- Dunst, C.J.; Espe-Sherwindt, M. Family-Centered Practices in Early Childhood Intervention. In Handbook of Early Childhood Special Education; Springer: Cham, Switzerland, 2016; pp. 37–55. Available online: https://link.springer.com/chapter/10.1007/978-3-319-28492-7_3 (accessed on 29 February 2024).
- Kokorelias, K.M.; Gignac, M.A.; Naglie, G.; Cameron, J.I. Towards a universal model of family centered care: A scoping review. BMC Health Serv. Res. 2019, 19, 564. [Google Scholar] [CrossRef] [PubMed]
- Jansen-van Vuuren, J.; Aldersey, H.M. Stigma, Acceptance and Belonging for People with IDD Across Cultures. Curr. Dev. Disord. Rep. 2020, 7, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Hohlfeld, A.S.; Harty, M.; Engel, M.E. Parents of children with disabilities: A systematic review of parenting interventions and self-efficacy. Afr. J. Disabil. 2018, 7, 1–2. Available online: https://hdl.handle.net/10520/EJC-11ef255b7e (accessed on 29 February 2024). [CrossRef] [PubMed]
- Harniess, P.A.; Gibbs, D.; Bezemer, J.; Purna Basu, A. Parental engagement in early intervention for infants with cerebral palsy—A realist synthesis. Child Care Health Dev. 2022, 48, 359–377. [Google Scholar] [CrossRef] [PubMed]
- Magnusson, D.; Sweeney, F.; Landry, M. Provision of rehabilitation services for children with disabilities living in low-and middle-income countries: A scoping review. Disabil. Rehabil. 2019, 41, 861–868. [Google Scholar] [CrossRef]
- Woodside, J.M.; Rosenbaum, P.L.; King, S.M.; King, G.A. Family-centered service: Developing and validating a self-assessment tool for pediatric service providers. Child. Health Care 2001, 30, 237–252. [Google Scholar] [CrossRef]
- McCarthy, E.; Guerin, S. Family-centred care in early intervention: A systematic review of the processes and outcomes of family-centred care and impacting factors. Child Care Health Dev. 2022, 48, 1–32. [Google Scholar] [CrossRef]
- Smythe, T.; Zuurmond, M.; Tann, C.J.; Gladstone, M.; Kuper, H. Early intervention for children with developmental or disabilities in low and middle-income countries–the case for action. Int. Health 2021, 13, 222–231. [Google Scholar] [CrossRef]
- Ned, L.; Tiwari, R.; Hess-April, L.; Lorenzo, T.; Chikte, U. A situational mapping overview of training programmes for community-based rehabilitation workers in Southern Africa: Strategies for strengthening accessible rural rehabilitation practice. Front. Public Health 2020, 8, 569279. [Google Scholar] [CrossRef]
- Hunt, X.; Bradshaw, M.; Vogel, S.L.; Encalada, A.V.; Eksteen, S.; Schneider, M.; Chunga, K.; Swartz, L. Community support for persons with disabilities in low-and middle-income countries: A scoping review. Int. J. Environ. Res. Public Health 2022, 19, 8269. [Google Scholar] [CrossRef]
- World Health Organization. Caregiver Skills Training for Families of Children with Developmental Delays or Disabilities—Introduction. Available online: https://www.who.int/publications/i/item/9789240048836 (accessed on 29 February 2024).
- Neocleous, M.; Hepworth, K.; Cavallera, V.; Gladstone, M. Training packages for the use of child development tools in low/middle-income countries: A review. Arch. Dis. Child. 2023, 108, 103–107. [Google Scholar] [CrossRef]
- UNICEF. Early Childhood Development Index 2030. Available online: https://data.unicef.org/resources/early-childhood-development-index-2030-ecdi2030/ (accessed on 29 February 2024).
- Sabanathan, S.; Wills, B.; Gladstone, M. Child development assessment tools in low-income and middle-income countries: How can we use them more appropriately? Arch. Dis. Child. 2015, 100, 482–488. [Google Scholar] [CrossRef]
- Ozturk Ertem, I.; Krishnamurthy, V.; Mulaudzi, M.C.; Sguassero, Y.; Bilik, B.; Srinivasan, R.; Balta, H.; Gulumser, O.; Gan, G.; Calvocoressi, L.; et al. Validation of the International Guide for Monitoring Child Development demonstrates good sensitivity and specificity in four diverse countries. Acta Paediatr. 2019, 108, 1074–1086. [Google Scholar] [CrossRef]
- Salomone, E.; Pacione, L.; Shire, S.; Brown, F.L.; Reichow, B.; Servili, C. Development of the WHO caregiver skills training program for developmental disorders or delays. Front. Psychiatry 2019, 10, 769. [Google Scholar] [CrossRef]
- Tekola, B.; Girma, F.; Kinfe, M.; Abdurahman, R.; Tesfaye, M.; Yenus, Z.; WHO CST Team; Salomone, E.; Pacione, L.; Fekadu, A.; et al. Adapting and pre-testing the World Health Organization’s Caregiver Skills Training programme for autism and other developmental disorders in a very low-resource setting: Findings from Ethiopia. Autism 2020, 24, 51–63. [Google Scholar] [CrossRef]
- Adugna, M.B.; Nabbouh, F.; Shehata, S.; Ghahari, S. Barriers and facilitators to healthcare access for children with disabilities in low and middle income sub-Saharan African countries: A scoping review. BMC Health Serv. Res. 2020, 20, 15. [Google Scholar] [CrossRef]
- World Health Organisation. Nurturing Care for Early Childhood Development: A Framework for Helping Children Survive and Thrive to Transform Health and Human Potential; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Shah, R.; Camarena, A.; Park, C.; Martin, A.; Clark, M.; Atkins, M.; Schwartz, A. Healthcare-Based Interventions to Improve Parenting Outcomes in LMICs: A Systematic Review and Meta-Analysis. Matern. Child Health J. 2022, 26, 1217–1230. [Google Scholar] [CrossRef]
- Jansen-van Vuuren, J.; Nuri, R.P.; Nega, A.; Batorowicz, B.; Lysaght, R.; Aldersey, H.M. Family quality of life for families of children with disabilities in African contexts: A scoping review. Qual. Life Res. 2022, 1289–1307. [Google Scholar] [CrossRef]
- Scherer, N.; Verhey, I.; Kuper, H. Depression and anxiety in parents of children with intellectual and developmental disabilities: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0219888. [Google Scholar] [CrossRef]
- Herba, C.M.; Glover, V.; Ramchandani, P.G.; Rondon, M.B. Maternal depression and mental health in early childhood: An examination of underlying mechanisms in low-income and middle-income countries. Lancet Psychiatry 2016, 3, 983–992. [Google Scholar] [CrossRef]
- Pedersen, G.A.; Smallegange, E.; Coetzee, A.; Hartog, K.; Turner, J.; Jordans, M.J.; Brown, F.L. A systematic review of the evidence for family and parenting interventions in low-and middle-income countries: Child and youth mental health outcomes. J. Child Fam. Stud. 2019, 28, 2036–2055. [Google Scholar] [CrossRef]
- Bunning, K.; Gona, J.K.; Newton, C.R.; Andrews, F.; Blazey, C.; Ruddock, H.; Henery, J.; Hartley, S. Empowering self-help groups for caregivers of children with disabilities in Kilifi, Kenya: Impacts and their underlying mechanisms. PLoS ONE 2020, 15, e0229851. [Google Scholar] [CrossRef]
- Hunt, X.; Saran, A.; Banks, L.M.; White, H.; Kuper, H. Effectiveness of interventions for improving livelihood outcomes for people with disabilities in low-and middle-income countries: A systematic review. Campbell Syst. Rev. 2022, 18, e1257. [Google Scholar] [CrossRef]
- Bastagli, F.; Hagen-Zanker, J.; Harman, L.; Barca, V.; Sturge, G.; Schmidt, T. The impact of cash transfers: A review of the evidence from low-and middle-income countries. J. Soc. Policy 2019, 48, 569–594. [Google Scholar] [CrossRef]
- Mkabile, S.; Garrun, K.L.; Shelton, M.; Swartz, L. African families’ and caregivers’ experiences of raising a child with intellectual disability: A narrative synthesis of qualitative studies. Afr. J. Disabil. (Online) 2021, 10, a827. [Google Scholar] [CrossRef]
- Susanty, D.; Noel, P.; Sabeh, M.S.; Jahoda, A. Benefits and cultural adaptations of psychosocial interventions for parents and their children with intellectual disabilities in low-and middle-income countries: A systematic review. J. Appl. Res. Intellect. Disabil. 2021, 34, 421–445. [Google Scholar] [CrossRef]
- Mkabile, S.; Swartz, L. Traditional healers’ explanatory models of intellectual disability in Cape Town. Transcult. Psychiatry 2022, 59, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Nair, M.K.; Radhakrishnan, R.; Olusanya, B.O. Promoting school readiness in children with developmental disabilities in LMICs. Front. Public Health 2023, 11, 993642. [Google Scholar] [CrossRef] [PubMed]
- Egan, R.; Wilson, R.; Robertson, M.; Scandiffio, J.; Ross-White, A.; Coderre-Ball, A.M. Barriers and facilitators to education experienced by students with disabilities in low-and middle-income African countries: A systematic review of qualitative evidence. JBI Evid. Synth. 2022, 20, 2475–2511. [Google Scholar] [CrossRef] [PubMed]
- Mariga, L.; McConkey, R.; Myezwa, H. Inclusive Education in Low-Income Countries: A Resource Book for Teacher Educators, Parent Trainers and Community Development. Disability Innovations Africa. 2014. Available online: https://www.eenet.org.uk/resources/docs/Inclusive_Education_in_Low_Income_Countries.pdf (accessed on 29 February 2024).
- Winthrop, R.; Barton, A.; Ershadi, M.; Ziegler, L. Collaborating to Transform and Improve Education Systems. Center for Universal Education at Brookings. Available online: https://www.brookings.edu/articles/collaborating-to-transform-and-improve-education-systems-a-playbook-for-family-school-engagement/ (accessed on 29 February 2024).
- Boyd, B.A.; Stahmer, A.C.; Odom, S.L.; Wallisch, A.; Matheis, M. It’s time to close the research to practice gap in autism: The need for implementation science. Autism 2022, 26, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Singla, D.R.; Kohrt, B.A.; Murray, L.K.; Anand, A.; Chorpita, B.F.; Patel, V. Psychological treatments for the world: Lessons from low-and middle-income countries. Annu. Rev. Clin. Psychol. 2017, 13, 149–181. [Google Scholar] [CrossRef]
- Xu, Y.; Zeng, W.; Wang, Y.; Magaña, S. Barriers to service access for immigrant families of children with developmental disabilities: A scoping review. Intellect. Dev. Disabil. 2022, 60, 382–404. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McConkey, R. Creating Family-Centred Support for Preschoolers with Developmental Disabilities in Low-Income Countries: A Rapid Review to Guide Practitioners. Int. J. Environ. Res. Public Health 2024, 21, 651. https://doi.org/10.3390/ijerph21060651
McConkey R. Creating Family-Centred Support for Preschoolers with Developmental Disabilities in Low-Income Countries: A Rapid Review to Guide Practitioners. International Journal of Environmental Research and Public Health. 2024; 21(6):651. https://doi.org/10.3390/ijerph21060651
Chicago/Turabian StyleMcConkey, Roy. 2024. "Creating Family-Centred Support for Preschoolers with Developmental Disabilities in Low-Income Countries: A Rapid Review to Guide Practitioners" International Journal of Environmental Research and Public Health 21, no. 6: 651. https://doi.org/10.3390/ijerph21060651
APA StyleMcConkey, R. (2024). Creating Family-Centred Support for Preschoolers with Developmental Disabilities in Low-Income Countries: A Rapid Review to Guide Practitioners. International Journal of Environmental Research and Public Health, 21(6), 651. https://doi.org/10.3390/ijerph21060651