
Effects of Cannabis Legalization on Road Safety: A Literature Review

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
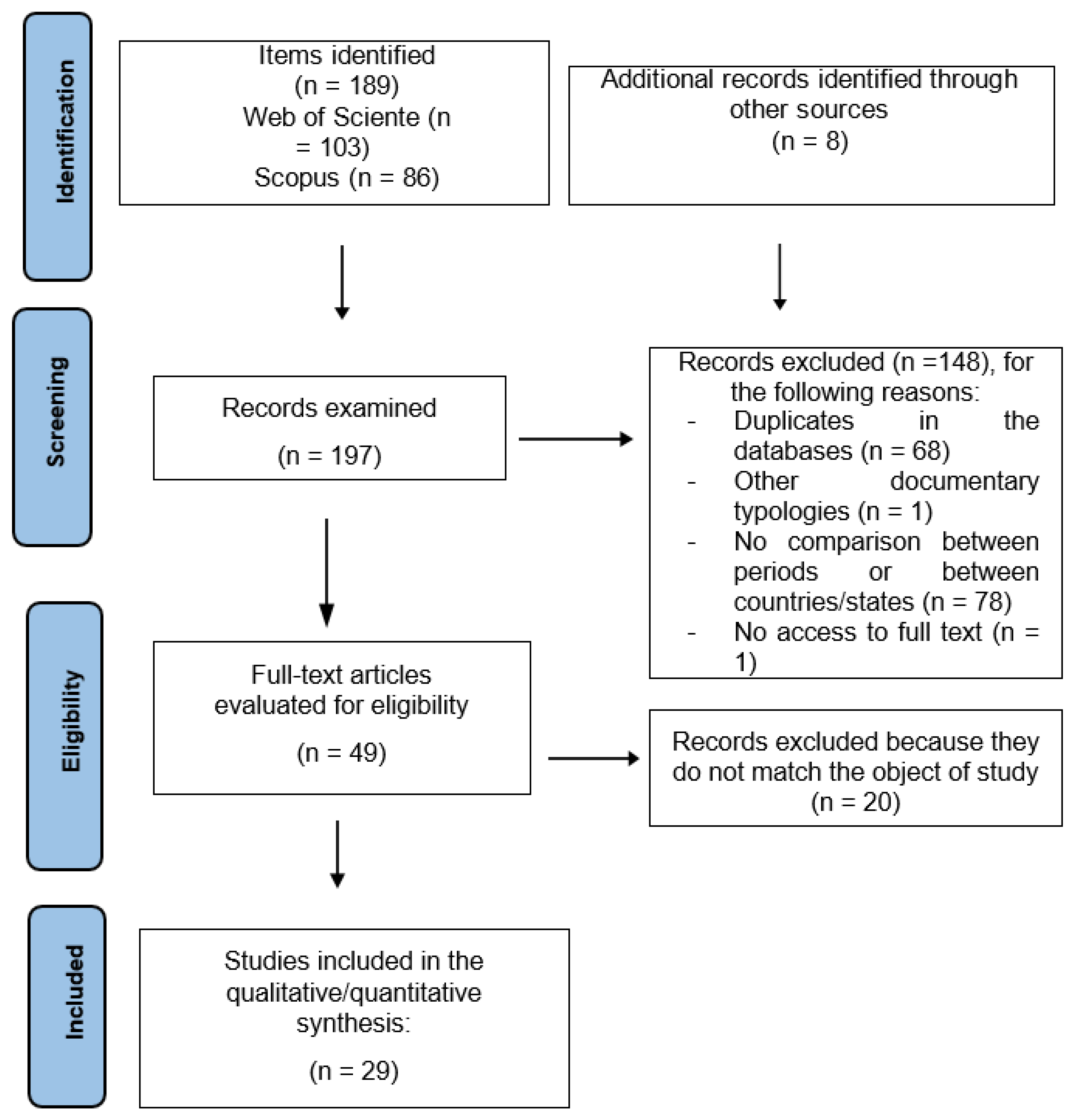
2.3. Study Selection
3. Results
3.1. Characteristics of the Studies Included in the Systematic Review
3.2. Relationship between the Legalization of Medical Cannabis and Traffic Accidents
3.3. Relationship between the Legalization of Recreational Cannabis and Traffic Accidents
3.4. Legalization and Decriminalization of Medical and Recreational Cannabis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Management of Substance Abuse: Cannabis. 2019. Available online: https://www.who.int/substance_abuse/facts/cannabis/en/ (accessed on 4 September 2022).
- Cruz, J.M.; Queirolo, R.; Boidi, M.F. Determinants of public support for marijuana legalization in Uruguay, the United States, and El Salvador. J. Drug Issues 2016, 46, 308–325. [Google Scholar] [CrossRef]
- Delling, F.N.; Vittinghoff, E.; Dewland, T.A.; Pletcher, M.J.; Olgin, J.E.; Nah, G.; Aschbacher, K.; Fang, C.D.; Lee, E.S.; Fan, S.M.; et al. Does cannabis legalization change healthcare utilization? A population-based study using the healthcare cost and utilization project in Colorado, USA. BMJ Open 2019, 9, e027432. [Google Scholar] [CrossRef]
- González-Sala, F.; San José, A.; Ciudad-Fernández, V. Effects of cannabis legalisation on physical health: A literature review. Rev. Esp. Drogodepend. 2020, 45, 74–90. [Google Scholar]
- Hartman, R.L.; Huestis, M.A. Cannabis effects on driving skills. Clin. Chem. 2013, 59, 478–492. [Google Scholar] [CrossRef]
- Li, M.C.; Brady, J.E.; DiMaggio, C.J.; Lusardi, A.R.; Tzong, K.Y.; Li, G. Marijuana use and motor vehicle crashes. Epidemiol. Rev. 2012, 34, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Roffman, R. Legalization of cannabis in Washington State: How is it going? Addiction 2016, 111, 1139–1140. [Google Scholar] [CrossRef]
- Woo, Y.; Willits, D.W.; Stohr, M.K.; Hemmens, C.; Hoff, S. Wreck on the highway: Intersectionality of driver culpability, tetrahydrocannabinols, other intoxicants and fatalities in Washington State. Transp. Res. Rec. 2019, 2673, 127–140. [Google Scholar] [CrossRef]
- Kamer, R.S.; Warshafsky, S.; Kamer, G.C. Change in traffic fatality rates in the first 4 states to legalize recreational marijuana. JAMA Intern. Med. 2020, 180, 1119–1120. [Google Scholar] [CrossRef]
- National Cannabis Survey, First Quarter 2019; Statistics Canada: Ottawa, ON, Canada, 2019; Available online: https://www150.statcan.gc.ca/n1/daily-quotidien/190502/dq190502a-eng.htm (accessed on 23 September 2022).
- Romano, E.; Torres-Saavedra, P.; Voas, R.B.; Lacey, J.H. Drugs and alcohol: Their relative crash risk. J. Stud. Alcohol. Drugs 2014, 75, 56–64. [Google Scholar] [CrossRef]
- Alonso, F.; Pastor, J.C.; Montoro, L.; Esteban, C. Driving under the influence of alcohol: Frequency, reasons, perceived risk and punishment. Subst. Abus. Treat. Prev. Policy 2015, 10, 11. [Google Scholar] [CrossRef]
- Fergusson, D.M.; Horwood, L.J. Cannabis use and traffic accidents in a birth cohort of young adults. Accid. Anal. Prev. 2001, 33, 703–711. [Google Scholar] [CrossRef] [PubMed]
- Siliquini, R.; Bert, F.; Alonso, F.; Berchialla, P.; Colombo, A.; Druart, A.; Kedzia, M.; Siliquini, V.; Vankov, D.; Villerusa, A.; et al. Correlation between driving-related skill and alcohol use in young-adults from six European countries: The TEN-D by Night Project. BMC Public Health 2011, 11, 526. [Google Scholar] [CrossRef] [PubMed]
- Siliquini, R.; Piat, S.C.; Alonso, F.; Druart, A.; Kedzia, M.; Mollica, A.; Siliquini, V.; Vankov, D.; Villerusa, A.; Manzoli, L.; et al. A European study on alcohol and drug use among young drivers: The TEND by Night study design and methodology. BMC Public Health 2010, 10, 205. [Google Scholar] [CrossRef] [PubMed]
- Alonso, F.; Esteban, C.; Montoro, L.; Tortosa, F. Psychotropic drugs and driving: Prevalence and types. Ann. Gen. Psychiatry 2014, 13, 14. [Google Scholar] [CrossRef] [PubMed]
- Palamar, J.J.; Ompad, D.C.; Petkova, E. Correlates of intentions to use cannabis among US high school seniors in the case of cannabis legalization. Int. J. Drug Policy 2014, 25, 424–435. [Google Scholar] [CrossRef]
- Cavazos-Rehg, P.A.; Krauss, M.J.; Sowles, S.J.; Floyd, G.M.; Cahn, E.S.; Chaitan, V.L.; Ponton, M. Leveraging user perspectives for insight into cannabis concentrates. Am. J. Drug Alcohol Abus. 2018, 44, 628–641. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Urrútia, G.; Bonfill, X. Declaración PRISMA: Una propuesta para mejorar la publicación de revisiones sistemáticas y metaanálisis. Med. Clínica 2010, 135, 507–511. [Google Scholar] [CrossRef]
- Ogrinc, G.; Davies, L.; Goodman, D.; Batalden, P.; Davidoff, F.; Stevens, D. SQUIRE 2.0 (Standards for Quality Improvement Reporting Excellence): Revised publication guidelines from a detailed consensus process. Am. J. Med. Qual. 2015, 30, 543–549. [Google Scholar] [CrossRef]
- Jones, J.M.; Shults, R.A.; Robinson, B.; Komatsu, K.K.; Sauber-Schatz, E.K. Marijuana and alcohol use among injured drivers evaluated at level I trauma centers in Arizona, 2008–2014. Drug Alcohol Depend. 2019, 204, 107539. [Google Scholar] [CrossRef] [PubMed]
- Wadsworth, E.; Hammond, D. International differences in patterns of cannabis use among youth: Prevalence, perceptions of harm, and driving under the influence in Canada, England & United States. Addic. Behav. 2019, 90, 171–175. [Google Scholar] [CrossRef]
- Steinemann, S.; Galanis, D.; Nguyen, T.; Biffl, W. Motor vehicle crash fatalaties and undercompensated care associated with legalization of marijuana. J. Trauma Acute Care Surg. 2018, 85, 566–571. [Google Scholar] [CrossRef] [PubMed]
- Sevigny, E.L. The effects of medical marijuana laws on cannabis-involved driving. Accid. Anal. Prev. 2018, 118, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Santaella-Tenorio, J.; Mauro, C.M.; Wall, M.M.; Kim, J.H.; Cerdá, M.; Keyes, K.; Hasin, D.; Galea, S.; Martins, S. US traffic fatalities, 1985-2014, and their relationship to medical marijuana laws. Am. J. Public Health 2017, 107, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Masten, S.V.; Guenzburger, G.V. Changes in driver cannabinoid prevalence in 12 US states after implementing medical marijuana laws. J. Safety Res. 2014, 50, 35–52. [Google Scholar] [CrossRef]
- Salomonsen-Sautel, S.; Min, S.J.; Sakai, J.T.; Thurstone, C.; Hopfer, C. Trends in fatal motor vehicle crashes before and after marijuana commercialization in Colorado. Drug Alcohol Depend. 2014, 140, 137–144. [Google Scholar] [CrossRef]
- Anderson, D.M.; Hansen, B.; Rees, D.I. Medical marijuana laws, traffic fatalities, and alcohol consumption. J. Law Econ. 2013, 56, 333–369. [Google Scholar] [CrossRef]
- Callaghan, R.C.; Sanches, M.; Vander Heiden, J.; Asbridge, M.; Stockwell, T.; Macdonald, S.; Peterman, B.H.; Kish, S.J. Canada’s cannabis legalization and drivers’ traffic-injury presentations to emergency departments in Ontario and Alberta, 2015–2019. Drug Alcohol Depend. 2021, 228, 109008. [Google Scholar] [CrossRef] [PubMed]
- Tefft, B.C.; Arnold, L.S. Estimating cannabis involvement in fatal crashes in Washington State before and after the legalization of recreational cannabis consumption using multiple imputation of missing values. Am. J. Epidemiol. 2021, 190, 2582–2591. [Google Scholar] [CrossRef]
- Windle, S.B.; Eisenberg, M.J.; Reynier, P.; Cabaussel, J.; Thombs, B.D.; Grad, R.; Ells, C.; Sequeira, C.; Filion, K.B. Association between legalization of recreational cannabis and fatal motor vehicle collisions in the United States: An ecologic study. CMAJ Open 2021, 9, E233–E241. [Google Scholar] [CrossRef]
- Lensch, T.; Sloan, K.; Ausmus, J.; Pearson, J.L.; Clements-Nolle, K.; Goodman, S.; Hammond, D. Cannabis use and driving under the influence: Behaviors and attitudes by state-level legal sale of recreational cannabis. Prev. Med. 2020, 141, 106320. [Google Scholar] [CrossRef] [PubMed]
- Nazif-Munoz, J.I.; Oulhote, Y.; Ouimet, M.C. The association between legalization of cannabis use and traffic deaths in Uruguay. Addiction 2020, 115, 1697–1706. [Google Scholar] [CrossRef] [PubMed]
- Rotermann, M. What has changed since cannabis was legalized? Health Rep. 2020, 31, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Borst, J.M.; Costantini, T.W.; Reilly, L.; Smith, A.M.; Stabley, R.; Steele, J.; Wintz, D.; Bansal, V.; Biffl, W.; Godat, L.N. Driving under the influence: A multi-center evaluation of vehicular crashes in the era of cannabis legalization. Trauma Surg. Acute Care Open 2021, 6, e000736. [Google Scholar] [CrossRef] [PubMed]
- Hansen, B.; Miller, K.; Weber, C. Early evidence on recreational marijuana legalization and traffic fatalities. Econ. Inq. 2020, 58, 547–568. [Google Scholar] [CrossRef]
- Santaella-Tenorio, J.; Wheeler-Martin, K.; DiMaggio, C.; Castillo-Carniglia, A.; Keyes, K.; Hasin, D.; Cerdá, M. Association of recreational cannabis laws in Colorado and Washington State with changes in traffic fatalities, 2005–2017. JAMA Intern. Med. 2020, 180, 1061–1068. [Google Scholar] [CrossRef]
- Aydelotte, J.D.; Brown, L.H.; Luftman, K.M.; Mardock, A.L.; Teixeira, P.G.; Coopwood, B.; Brown, C.V. Crash fatality rates after recreational marijuana legalization in Washington and Colorado. Am. J. Public Health 2017, 107, 1329–1331. [Google Scholar] [CrossRef]
- Aydelotte, J.D.; Mardock, A.L.; Mancheski, C.A.; Quamar, S.M.; Teixeira, P.G.; Brown, C.V.; Brown, L.H. Fatal crashes in the 5 years after recreational marijuana legalization in Colorado and Washington. Accid. Anal. Prev. 2019, 132, 105284. [Google Scholar] [CrossRef]
- Lane, T.J.; Hall, W. Traffic fatalities within US states that have legalized recreational cannabis sales and their neighbours. Addiction 2019, 114, 847–856. [Google Scholar] [CrossRef]
- Benedetti, M.H.; Li, L.; Neuroth, L.M.; Humphries, K.D.; Brooks-Russell, A.; Zhu, M. Self-reported driving after marijuana use in association with medical and recreational marijuana policies. Int. J. Drug Policy 2021, 92, 102944. [Google Scholar] [CrossRef]
- Lee, J.; Abdel-Aty, A.; Park, J. Investigation of associations between marijuana law changes and marijuana-involved fatal traffic crashes: A state-level analysis. J. Transp. Health 2018, 10, 194–202. [Google Scholar] [CrossRef]
- Kruse, M.; Perez, M.; Blatt, M.; Zielonka, T.; Dolich, D.; Keric, N.; Schreiber, M.; Bini, J.; Hofmann, L.; Cohn, S.M. Marijuana legalization and rates of crashing under the influence of tetrahydrocannabinol and alcohol. Am. Surg. 2021, 0003134821995053. [Google Scholar] [CrossRef] [PubMed]
- Keric, N.; Hofmann, L.J.; Babbitt-Jonas, R.; Michalek, J.; Dolich, M.; Khoury, L.; Perez, J.M.; Cohn, S.M. The impact of marijuana legalization on vehicular trauma. Cureus 2018, 10, e3671. [Google Scholar] [CrossRef]
- Hamzeie, R.; Thompson, I.; Roy, S.; Savolainen, P.T. State-level comparison of traffic fatality data in consideration of marijuana laws. Transp. Res. Rec. 2017, 2660, 78–85. [Google Scholar] [CrossRef]
- Pollini, R.A.; Romano, E.; Johnson, M.B.; Lacey, J.H. The impact of marijuana decriminalization on California drivers. Drug Alcohol Depend. 2015, 150, 135–140. [Google Scholar] [CrossRef]
- Couper, F.J.; Peterson, B.L. The prevalence of marijuana in suspected impaired driving cases in Washington state. J. Anal. Toxicol. 2014, 38, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Faus, M.; Alonso, F.; Fernández, C.; Useche, S.A. Are traffic announcements really effective? A systematic review of evaluations of crash-prevention communication campaigns. Safety 2021, 7, 66. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]


{kind=link}
| Article | Country (States)/Years | Sample Size | Study Group | Variables | Data Collected/Detection Method |
|---|---|---|---|---|---|
| Jones et al. (2019) [22] | U.S. (Arizona) (2008–2014) | THC+: N = 2590 Alcohol+: N = 5266 THC+ and alcohol: N = 1086 | Injured driver | Use of cannabis, alcohol, or both substances after a traffic accident. Pre-legalization: January 2008–April 2011; Post-legalization: April 2011–December 2014. | Urine drug screens for cannabis metabolites and BAC. |
| Wadsworth and Hammond (2019) [23] | Canada, England, and U.S. July, 2017 | Canada: N = 4008 England: N = 3970 U.S.: N = 4086 | Youth | Use, access, perceptions of harm and driving after cannabis and/or alcohol use. Sociodemographic variables. | Self-report completed using web-based surveys. |
| Steinemann et al. (2018) [24] | U.S. (Hawaii) (1993–2015) | Pre-legalization (1993–2000): N = 560; THC+ 31 (6%). Post-legalization (2001–2015): N = 1018. THC+ 151(15%). | Drivers killed | THC+ and alcohol in drivers. Pre- and post-legalization. | FARS. Urine toxicology and blood drug test. |
| Sevigny (2018) [25] | U.S. (1993–2014) | Nearly 1.2 million drivers involved in fatal traffic accidents. THC+ 8.8% BAC ≥ 0.08 = 20.1%. | Drivers | Presence of THC, other illicit drugs, and alcohol. Variables related to cannabis regularization. Contextual and control variables. | FARS. Blood drug test. |
| Santaella-Tenorio et al. (2017) [26] | U.S. (50 states) (1985–2014) | N = 1,220,610. | Deaths in traffic accidents | Fatal traffic accidents. Age 14–24, 25–44, and 45< years. Date MML by State. Dispensaries. | FARS. Blood drug test. |
| Masten and Guenzburger (2014) [27] | U.S. (14 states that have legalized cannabis and 37 jurisdictions without MCL) (1992–2009) | Drivers involved in fatal crashes: THC+ N = 19,977. | Drivers | Presence of THC in drivers involved in fatal traffic accidents. | FARS. Blood and/or urine drug test. |
| Salomonsen-Sautel et al. (2014) [28] | U.S. (Colorado and 34 states without MCL) (1994–2011) | Proportions of drivers involved in fatal crashes. Colorado: THC+ between 4.5% to 10%. States without MCL: THC+ between 1.1% to 4.1% | Drivers | THC+ or alcohol BAC ≥ 0.08. Pre-commercialization, June 1994–July 2009; Post-commercialization, July 2009–2011. | FARS. Blood and/or urine drug test. |
| Anderson et al. (2013) [29] | U.S. (1990–2010) | Age: 15–60< years old. 20.48 (7.15) | Fatalities per 100,000 people | Fatal traffic accidents. Sociodemographic variables. Control states and MCL states. | FARS. Blood drug test. |
| Article | Statistical Analysis | Main Result | Limitations |
|---|---|---|---|
| Jones et al. (2019) [22] | Regression analysis of interrupted time series. | Before legalization, decreased positive drivers by 0.5%/year (95% CI: −1.0/year, 0.0/year). After legalization, a significant increase in the trend of cannabis-positive drivers of 0.6%/year (95% CI: 0.0/year, 0.8/year). | Differences between and within states in drug testing protocols. Testing positive for THC does not imply recent use. No control group. |
| Wadsworth and Hammond (2019) [23] | Chi-squared tests, nominal logistic regression, and multinomial logistic regression models. | There are differences in driving after cannabis use between countries. England: less likely to drive after drinking than Canada (p < 0.001) and the U.S. (p < 0.001). Canada: less likely than the U.S. (p < 0.001). | Self-report measures. Social desirability. Biases in a recall. General legislation of the country is taken and differences between different districts/cities are not taken into account. Non-random subject selection. |
| Steinemann et al. (2018) [24] | t-tests and Chi-squared tests. | Significant increase (p < 0.001) in the number of drivers testing positive for THC after legalization in 2000 in fatal accidents. | THC+ does not imply recent consumption. A THC level cannot be extrapolated to an accident risk level. There is no discrimination between acute, heavy, and chronic use. |
| Sevigny (2018) [25] | Generalized linear model (GLM) with a binomial distribution and logit link function. Sensitivity analyses. | There is no relationship between the MCL and the number of fatal traffic accidents OR [95% CI] 1.05 [0.93, 1.19]. The implementation of medical cannabis dispensaries does correlate with a higher number of accidents involving cannabis OR [95% CI] 1.14 [1.02, 1.29] (p < 0.01). | THC+ does not imply recent use. Differences between states in drug testing protocols, as well as changes in trends after legalization. Not all crash victims are drug tested. Levels of cannabis use are not systematically quantified. |
| Santaella-Tenorio et al. (2017) [26] | Multilevel regression models with state-level random intercepts. | States with MCL laws have lower rates of traffic fatalities than states without MCL laws (26.3% lower; 95% confidence interval [CI] = 13.9%, 36.9%). A 10.8% reduction in fatalities after MCL (95% CI = 9.0%, 12.5%; % reduction = [1 − exp(−0.114)] − 100). Following the legalization of cannabis, there was a reduction in fatal traffic accidents in 7 states. | Causal relationships cannot be established. Local aspects that may have an influence are not taken into account. Short post-legalization periods. THC tests are not performed. |
| Masten and Guenzburger (2014) [27] | Time series analyses. Auto-regressive integrated moving average analysis. | MCL is only associated with an increase in fatal traffic accidents in California, Hawaii, and Washington (out of a total of 12 states) after adjusting for the frequency of drug testing by state and the prevalence of cannabinoids in drivers in states without legalization laws. | They only study fatal traffic accidents. State differences in drug testing protocols and changes in trends after legalization. Not all crash victims are tested for drugs. THC+ does not imply recent use. |
| Salomonsen-Sautel et al. (2014) [28] | Linear regression analysis. Estimated generalized least squares (EGLS) methods. | Significant trend change (2.16 (0.45), p < 0.0001) in Colorado (not in the rest of the states) after legalization, with an increase in THC-positives among drivers involved in fatal accidents. | They only study fatal traffic accidents. THC+ does not imply recent use. Levels of marijuana use are not systematically quantified. |
| Anderson et al. (2013) [29] | Linear regression analysis by ordinary least squares (OLS) estimates | Legalization leads to a significant decrease in fatal traffic accidents, although when state-specific time trends are included, the decrease is not significant (p = 0.139). Legalization leads to a reduction in crashes where the driver tests positive for alcohol (R = −0.141, p < 0.01) and in cases where the alcohol level is above 0.10 (R = 0.168, p < 0.05). | Not specified |
| Article | Country (States)/Years | Sample Size | Study Group | Variables | Data Collected/Detection Method |
|---|---|---|---|---|---|
| Callaghan et al. (2021) [30] | Canada (Alberta and Ontario) (2015–2019). | Alberta: N = 52,752. Youth-driver N = 3265, Ontario: N = 186,921. Youth-driver N = 4565. | Injured drivers | Weekly visits to medical emergency units for injuries in traffic accidents. Young drivers and total drivers. Pre-legalization: 1 April 2015–16 October 2018. Post-legalization: 17 October 2018–31 December 2019. | National Ambulatory Care Reporting System database. |
| Tefft and Arnold (2021) [31] | U.S. (Washington). (2008–2019). | THC+: N = 735; negative: N = 3528; unknown: N = 4019 | Drivers involved in fatal crashes | THC in blood: positive (1.0 ng/mL or more). Negative no THC detected in blood. Unknown: no drug test or no confirmation. THC concentrations were 0, 1.0–4.9 ng/mL, 5.0–9.9 ng/mL, and ≥10.0 ng/mL. Pre-legalization: 1 January 2008–5 December 2012. Post-legalization: 6 December 2012–31 December 2019. Vehicle and crash characteristics. | FARS. Blood drug test. |
| Windle et al. (2021) [32] | U.S. (10 states and District of Columbia). RCD (7 states). (2007–2018). | Periods RCL: 17,116 accidents and 18,580 deaths. Periods without legalization: 56,866 accidents and 61,822 deaths. | Death from motor vehicle collision | Fatal accidents. Deaths following a collision. Recreational cannabis dispensaries (7 states). Cannabis-specific impaired driving law: zero tolerance, per se limit ≥ 2 ng/mL THC, per se limit ≥ 5 ng/mL THC, or none. | FARS. |
| Lensch et al. (2020) [33] | U.S. (2018) | N = 17,112 adults. Legal sale states: N = 5548. Non-legal sale states: N = 11,564. | Drivers and Passengers | Six legal sale states with dispensaries. Non-legal sale states where despite legalizing marijuana, there are no dispensaries. Attitudes and behaviors related to driving, consumption, and frequency of cannabis use. | Web-based surveys (Self-reported). |
| Nazif-Muñoz et al. (2020) [34] | Uruguay (Montevideo and 4 rural provinces) (2012–2017). | N = 3037 fatal accidents. | Drivers and motorcyclists | Accidents and mortality rate in traffic accidents. Urban and rural areas. Type of vehicle: automobiles and motorcycles. | National Road Safety Agency. Ministry of Transport and Public Works |
| Rotermann (2020) [35] | Canada. (2018–2019). | Pre-legalization: N = 17,683. Post-legalization: N = 21,872. | Drivers and passengers | Pre-legalization: first, second, and third quarters of 2018. Post-legalization: first, second, third, and fourth quarters of 2019. Consumption and origin of the product. Driving a vehicle 2 h after consumption. Accompanying a driver who has consumed. | National Cannabis Survey: Internet-based electronic questionnaire |
| Borst et al. (2020) [36] | U.S. (California). (2010–2018). | THC+: N = 1345. THC+ and Alcohol+: N = 578. No use: N = 7078. | Patients | Type of use: no use, cannabis only, alcohol only (>0.08%), cannabis and alcohol, and cannabis with methamphetamines or cocaine. Pre-legalization: 2010–2015. Post-legalization: 2016–2018. Data concerning injuries and protective measures. | San Diego County’s trauma center registries. Blood and urine test. |
| Hansen et al. (2020) [37] | U.S. (Colorado, Washington, and control states) (2000–2016). | Not specified | Drivers | Fatal traffic accidents, alcohol-involved accidents, and marijuana-involved accidents. | FARS. |
| Santaella et al. (2020) [38] | U.S. (Colorado, Washington, and 42 control states) (2005–2017). | Not specified | Driver and passenger deaths | Mortality rate per traffic accident and year. Vehicle miles traveled. Age adjusted fatality rates. Pre-legalization: 2007–2013. Post-legalization: 2014–2017. | FARS. |
| Delling et al. (2019) [3] | U.S. (Colorado and control states). (2010–2014). | Colorado: N = 2,088,909. New York: N = 11,726,283. Oklahoma: N = 2,334,988. | Patients | Admission to hospital due to traffic accidents. Sociodemographic and health variables and alcohol consumption. | Healthcare Cost and Utilization Project database. |
| Aydelotte et al. (2017) [39] | U.S. (Colorado, Washington, and 8 control states) (2009–2015). | N = 60,737 fatal traffic accidents. | Drivers and passengers | Number of fatal traffic accidents. Billion vehicle miles traveled. | FARS. |
| Aydelotte et al. (2019) [40] | U.S. (Colorado, Washington, and 9 control States) (2007–2017). | Fatal accidents (Pre-legalization N = 12,348; Post-legalization N = 12,865). | Driver and passenger deaths | Fatal traffic accidents. Legalization: Before November 2007–October 2012, and January 2013–December 2017. Period of commercial dipensaries available: August 2014–December 2017. Period of the opening of the first dispensary: August 2010–December 2013. Billion vehicle miles traveled. Gross domestic product. Control variables in control states. | FARS. |
| Lane and Hall (2019) [41] | U.S. (12 states) (2009–2016) | States LRC (Colorado, Washington, and Oregon) and 9 adjoining states. | Deaths in traffic accidents | Rate of fatal traffic accidents per million population. States that have legalized recreative cannabis and neighboring states. | Centers for Disease Control and Prevention’s Wide-Ranging Online Data for Epidemiologic Research and RoadSafetyBC report. |
| Article | Statistical Analysis | Main Results | Limitations |
|---|---|---|---|
| Callaghan et al. (2021) [30] | Interrupted time-series analysis. Seasonal autoregressive integrated moving average models | There is no significant effect of increased injury visits among young drivers and all drivers before and after legalization. Significant differences (95% CI −26.32; 84.19; p = 0.30) are observed for all drivers in Ontario in emergency department visits. | Data are only collected from two provinces in Canada and from cases that have resulted in moderate to severe injuries. |
| Tefft and Arnold (2021) [31] | Logistic regression and marginal standardization. | Increase in the proportion of drivers who tested positive for THC from 9.3% before and 19.1% after legalization (APR: 2.3, 95% CI: 1.3, 4.1) and in the concentration of THC (APR: 4.7, 95% CI: 1.5, 15.1). | There is a significant number of drivers for which there is no drug test. Bias in the results by not taking into account other variables. Data are not compared with other states that have not legalized RC. |
| Windle et al. (2021) [32] | Poisson regression, meta-analyzed estimates, and DerSimonian and Laird random-effects models. | Increase in fatal traffic accidents (IRR 1.15, 95% CI 1.06–1.26) and deaths (IRR 1.16, 95% CI 1.06–1.27) in the first year after legalization. | Observational study. Jurisdiction differed among states. |
| Lensch et al. (2020) [33] | Chi-square tests. APR and 95% CI. | Higher incidence of use in states that legalized cannabis in the previous 30 days (APR: 1.34; 95% CI: 1.19, 1.51) and in the previous 12 months (APR: 1.16; 95% CI: 1.06, 1.28). Higher protective behaviors in states that have legalized RC. | Cross-sectional study. Non-representative sample of the general population. |
| Nazif-Muñoz et al. (2020) [34] | Interrupted time-series analysis. Extension autoregressive integrated moving average. | Significant increase in the light motor vehicle driver fatality rate (CI = 11.6, 93.3, p = 0.012). Significant increase in automobile driver mortality in Montevideo (CI = 0.01, 0.11, p = 0.025) but not in rural areas. | Prevalence of cannabis use in traffic accidents. Accidents with injuries are not considered. Possible biases in the coding of accidents. |
| Rotermann (2020) [35] | t-test statistics. | Stability in the number of cases of driving after having consumed before and after legalization, being more frequent in men than in women (p < 0.05). In general, decrease in the number of cases of traveling in a vehicle whose driver had consumed. | Self-report data. The type of design does not allow for causal inferences. The study is limited to surveyed households only. |
| Borst et al. (2020) [36] | Multivariate logistic regression. Linear regression. Binomial logistic regressions. Pearson χ2. Time-series regression analysis | A 7.6-percentage point increase of THC+ cases in accidents after legalization. The THC+ group used fewer protective measures while driving (8.5% vs. 14.3%, p < 0.001) and suffered more serious injuries (8.4 ± 9.4 vs. 9.0 ± 9.9, p < 0.001) than the non-consumption group. | There is no legal threshold for driving under the influence of cannabis. Time in which cannabinoids are maintained in the blood. No toxicological screening of all patients. Variability in detection rates between institutions. |
| Hansen et al. (2020) [37] | Synthetic control approach. Permutation testing of the ratio of mean squared error ratios | Control states show the same increases in the number of accidents per billion vehicle miles traveled in Colorado (p = 0.361) and Washington (p = 0.404). | Levels of marijuana use not quantified and variation among states. Only fatal traffic accidents. No causality can be asserted. |
| Santaella et al. (2020) [38] | Ecological study used a synthetic control approach. Mean square prediction error. | Increase (p = 0.047) in traffic fatalities in Colorado but not in Washington following legalization of RC. | Other variables associated with legalization. Time of legalization in Washington. No data on injuries. Not included if the driver tested positive for THC at the time of the accident. |
| Delling et al. (2019) [3] | Linear, logistical, and multinomial models. | An increase (p < 0.05) in the number of traffic accidents, alcohol abuse, overdose injuries and a decrease in chronic pain admissions is observed following the legalization of RC versus control states. | The post-legalization period is short (two years). They only compare with two control states. Colorado legalized medical marijuana prior to 2012. |
| Aydelotte et al. (2017) [39] | Random effects multivariate regression for panel data. Difference-in-differences approach. | Despite an increase, there is no significant association between legalization and changes in the rate of fatal traffic accidents (ADDC = +0.2 fatalities/billion vehicle miles traveled; 95% CI = –0.4, +0.9) in the first 3 years of legalization. | They only analyze two states in which the substance has been legalized. They do not study adjacent control states. They study fatal traffic crashes as a whole, not those in which cannabis is involved. |
| Aydelotte et al. (2019) [40] | Retrospective longitudinal cohort study. Difference–indifference analyses. | Significant increase in the number of fatal traffic accidents in states that legalized RC after opening dispensaries to buy recreational marijuana (CI: +0.4 to +3.7, p = 0.020) compared to control states. This increase was not significant before the dispensaries opened (CI: −0.6 to 2.1, p = 0.087). | Do not make any statistical adjustments for multiple analyses. Biases in the selection of control states. Missing more states where recreational marijuana use has been legalized. Only study fatal traffic accidents. |
| Lane and Hall (2019) [41] | Interrupted time-series design. Generalized least squares regression models. | The general trend is an increase in the mortality rate both in states with legalization laws and in neighboring states. There is a trend of increased mortality (p < 0.001) at the beginning and a decrease in the subsequent months (p < 0.001). At 6 months these effects are greater (step: 1.36, p = 0.006; trend: −0.07, p < 0.001). | They do not differentiate between fatal traffic accidents in which marijuana is involved and those in which it is not. They do not consider other types of accidents. They do not analyze economic factors or current policies of neighboring states regarding cannabis. |
| Article | Country (State)/Years | Sample Size | Study Group | Variables | Data Collected/Detection Method |
|---|---|---|---|---|---|
| Benedetti et al. (2021) [42] | U.S. (2013–2017). | CR illegal: N = 10,294 drivers; CR legal: N = 876 drivers. MC illegal: N = 5782 drivers; MC legal: N = 5388 drivers. | Drivers | Marijuana use while driving in the last year. States with the legalization of MM, MM, and MR or no legalization of both. Marijuana policy. Sociodemographic variables. TSCI is a nationally representative annual survey. | Self-reported. |
| Kruse et al. (2021) [44] | U.S. (Arizona, California, Ohio, Oregon, New Jersey, and Texas) Pre-legalization: 2006–2012. Post-legalization: 2013–2018. | Not specified | Patients with trauma | Vehicle collisions. THC-positive patients and alcohol-positive patients > 0.08 g/dL). | Data from different universities. Urine and blood analysis. |
| Woo et al. (2019) [8] | U.S. (Washington) (2008–2016). | N = 10,155 accidents and 5931 drivers. THC > 5.00 = 4.2%, THC <5 = 3.1%, Clean 92.6%. BAC > 0.08 = 19.2%, BAC <0.08 = 3.5%, Clean 77.3%. | Drivers | Fatal accidents. Speeding and driver error. THC (<5 ng/mL in blood or >5 ng/mL). Carboxy-THC. Alcohol (0.08 less or more). Control variables. Environmental Contexts. | FARS. Blood tested. |
| Keric et al. (2018) [45] | U.S. (Texas and California) (2006–2012). | N = 127 Surgeons. UTHSCSA center: patients traffic accidents N = 7171. Alcohol+ 21%, THC+ 4%, alcohol and THC+ 3%. Center in California: N = 16,084, alcohol+ 50%, THC+ 23%, alcohol and THC+ 7%. | Surgeons and patients | Alcohol (>0.08 g/dL). Marijuana (>50 ng/mL in Texas and >100 ng/mL in California). Injuries related to traffic accidents. Decriminalization in CA in 2010. Electronic survey completed by the members of the American Association for the Surgery of Trauma. | Trauma center registries at The University of California Irvine and UTHSCSA. |
| Lee et al. (2018) [43] | U.S. (16 states) (2008–2015). | Number of accidents involving cannabis in states with law changes. Before, N = 1458. After, N = 938. | Drivers | Types of states according to cannabis legalization and decriminalization laws. | FARS. |
| Hamzeie et al. (2017) [46] | U.S. (50 states and District of Columbia) (2010–2014). | THC+: N = 9301 drivers THC−: N = 65,332 drivers | Drivers | States with legalization and decriminalization laws and states with no such laws. Driver, accident, and vehicle characteristics. THC+ and THC−. | FARS. |
| Pollini et al. (2015) [47] | U.S. (California). (2008–2012). | (2008–2010): N = 1718; THC+ N = 203 (2011–2012): N = 1142; THC+ N = 175 | Drivers | Detection of cannabis use in drivers involved in traffic accidents. Decriminalization period: 2011–2012. No decriminalization period: 2008–2010. | FARS. |
| Couper and Peterson (2014) [48] | U.S. (Washington, D.C.) (2009–2013) | N = 25,179, age 14–85 years old. Median age 25 years pre-legalization and 26 years post-legalization. | Drivers | Detection of THC consumption. (Pre-legalization THC+ 0.2 ng/mL, carboxy-THC of 0.10 ng/mL). Pre-legalization: 2009–2012. Post-legalization: 2013. | Blood tested |
| Article | Statistical Analysis | Main Results | Limitations |
|---|---|---|---|
| Benedetti et al. (2021) [42] | Multiple logistic regression model. | States with MCL have a higher number of drivers who have driven under the influence of marijuana versus states that have not legalized MC and/or RC (OR 1.29; 95% CI 0.98, 1.70; p = 0.075). THC threshold laws: less likely to drive after consumption (OR 0.74; 95% CI 0.57, 0.95; p = 0.018). | Biases associated with self-reports. Quasi-experimental design that does not allow inferring causal relationships between marijuana use among drivers and states’ policies on marijuana use. |
| Kruse et al. (2021) [44] | Retrospective analysis of data. Percentages. | There seems to be no relationship between legalization and the probability of finding THC in patients admitted after an accident. | Discrepancies in urine THC detection limits by institution. A lack of standardized laws by the state does not allow the detection of real THC prevalence. |
| Woo et al. (2019) [8] | Series of logistic regressions. | Being a young man, driving a motorcycle, and testing positive for alcohol, delta 9-THC, or carboxy-THC and other drugs (p < 0.001) are risk factors for speeding. Cannabis predicts risky driving behavior. | Only fatal accidents are examined. Washington State data only. Not all crashes tested for drugs. Measurement errors in drug rates. |
| Keric et al. (2018) [45] | Time frame. Percentages. | A total of 90% of surgeons report no increase in cases of traumatic injuries in traffic accidents after cannabis legalization. | Not specified. |
| Lee et al. (2018) [43] | Series estimation of crash modification factors. | Increase in fatal accidents in which the driver tests positive for cannabis, mainly with decriminalization (p < 0.001) and/or legalization of RC but not MC (p < 0.001) Other effects are between decriminalization and decriminalization and MCL (p = 0.020) and between MCL and full legalization (p = 0.010). | Short post-legalization periods. Differences between states in drug testing protocols and trends after legalization. Difficulties in selecting a control group. Cannot assert causality. |
| Hamzeie et al. (2017) [46] | Logistic regression models | Higher probability of testing positive for THC in an accident in states with cannabis decriminalization (17%) and/or legalization laws (48%) (p < 0.001). Being young, male, positive for alcohol, and exhibiting more risky driving behaviors increased the probability of THC+ (p < 0.001). | They only test for CRL in two states and for a short period of time. Not all drivers take the drug test. Differences between states in drug testing protocols and trends after legalization. |
| Pollini et al. (2015) [47] | Multiple logistic regression analyses | Significant increase in the prevalence of cannabis positives among drivers involved in fatal crashes after decriminalization (17.8%; 95% CI: 14.6, 20.9). No change in THC positives among weekend nighttime drivers after decriminalization (9.2%; 95% CI: 6.3, 12.2). | Differences in drug testing protocols. Changes in consumption trends after legalization. Small and restricted sample. THC+ does not imply recent use. |
| Couper and Peterson (2014) [48] | Chi-squared tests | After a stable trend, there is a significant increase in the percentage of positive cases of THC consumption in drivers after legalization (p < 0.05). | THC concentration can be altered causing problems in the cut-off point for considering a subject positive. Delays in blood collection can influence the concentration of metabolites. |
| Effect of Legalization/Decriminalization on Traffic Accidents | States/Countries | Periods Pre- and Post-Legalization |
|---|---|---|
| YES | [3,23,25,26,27,28,33,40,41,42,43,46] | [3,8,22,24,28,31,32,34,36,38,40,41,43,47,48] |
| NO | [29,37,39] | [30,35,39,44,45] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Sala, F.; Tortosa-Pérez, M.; Peñaranda-Ortega, M.; Tortosa, F. Effects of Cannabis Legalization on Road Safety: A Literature Review. Int. J. Environ. Res. Public Health 2023, 20, 4655. https://doi.org/10.3390/ijerph20054655
González-Sala F, Tortosa-Pérez M, Peñaranda-Ortega M, Tortosa F. Effects of Cannabis Legalization on Road Safety: A Literature Review. International Journal of Environmental Research and Public Health. 2023; 20(5):4655. https://doi.org/10.3390/ijerph20054655
Chicago/Turabian StyleGonzález-Sala, Francisco, Macarena Tortosa-Pérez, María Peñaranda-Ortega, and Francisco Tortosa. 2023. "Effects of Cannabis Legalization on Road Safety: A Literature Review" International Journal of Environmental Research and Public Health 20, no. 5: 4655. https://doi.org/10.3390/ijerph20054655
APA StyleGonzález-Sala, F., Tortosa-Pérez, M., Peñaranda-Ortega, M., & Tortosa, F. (2023). Effects of Cannabis Legalization on Road Safety: A Literature Review. International Journal of Environmental Research and Public Health, 20(5), 4655. https://doi.org/10.3390/ijerph20054655