Abstract
During the start of the COVID-19 pandemic, shortages of personal protective equipment (PPE) necessitated unprecedented and non-validated approaches to conserve PPE at healthcare facilities, especially in high income countries where single-use disposable PPE was ubiquitous. Our team conducted a systematic literature review to evaluate historic approaches for conserving single-use PPE, expecting that lower-income countries or developing contexts may already be uniquely conserving PPE. However, of the 50 included studies, only 3 originated from middle-income countries and none originated from low-income countries. Data from the included studies suggest PPE remained effective with extended use and with multiple or repeated use in clinical settings, as long as donning and doffing were performed in a standard manner. Multiple decontamination techniques were effective in disinfecting single use PPE for repeated use. These findings can inform healthcare facilities and providers in establishing protocols for safe conservation of PPE supplies and updating existing protocols to improve sustainability and overall resilience. Future studies should evaluate conservation practices in low-resource settings during non-pandemic times to develop strategies for more sustainable and resilient healthcare worldwide.
1. Introduction
The emergence of SARS-CoV-2 (COVID-19) strained healthcare resources worldwide. Healthcare facilities and hospitals across the world reported severe shortages of supplies, particularly personal protective equipment (PPE) including masks and respirators, gowns, gloves, and eye protection. These shortages were driven by an unprecedented increase in consumption, compounded by factory closures along the global supply chain [1]. As a result, many hospitals and medical centers worldwide developed individual approaches to manage limited supplies based on guidance from the World Health Organization and data from previous outbreaks [2,3,4,5,6,7]. Hospitals and other health facilities enacted conservation practices such as limiting access to PPE stocks and rationing supplies. Novel, often non-validated, techniques emerged early in the pandemic to prolong the lifespans of single-use PPE, including prolonged use, multiple use, and reprocessing of single-use PPE [8].
Given the likelihood of continued supply disruptions in the recovery from the pandemic and the onslaught of climate change [9,10,11], it is imperative to better understand PPE conservation practices that can be safely employed in times of shortage. These practices must not reduce PPE efficacy to levels that increase risk of pathogen exposure [12]. Systematic reviews of PPE conservation that have been published since the emergence of COVID-19 have been narrowly focused on one type of PPE, mainly N95 respirators [13,14,15,16,17,18], and have not commented on practices in developing contexts. Here, we assess the body of knowledge at the start of the pandemic on various PPE conservation and reuse practices.
We hypothesized that low- and middle-income countries may have validated methods for conserving PPE due to regular shortages in supplies. Ideally, all countries should be enabled to meet their supply chain needs, but existing consumption practices from high-income countries could be improved by drawing from the experiences of countries with fewer resources, as has been suggested in the example of cataract surgeries [19,20,21]. We sought to analyze existing literature to assess effective means of conserving and reusing PPE, with implications for the ongoing pandemic and beyond. We anticipate that our analyses will help bolster healthcare system preparedness for future supply challenges, as well as support efforts to promote long-term environmental sustainability [22].
2. Methods
2.1. Systematic Review
On 9 June 2020, following PRISMA guidelines for systematic reviews [23], a medical librarian (TR) performed searches for studies without language or date restrictions in the LitCOVID, PubMed, Embase, HealthStar, and CINAHL databases. The search included studies describing the efficacy of methods used to conserve or reuse PPE within healthcare settings and comparisons of single-use and reusable PPE. A full description of search terms and inclusion and exclusion criteria can be found in the Supplemental Materials (SM). The citation lists of relevant systematic reviews were screened for additional studies.
Title, abstract, and full text screenings were completed by 2 researchers (GA, PL) using Covidence software [24]. The entire research team iteratively built and tested a data extraction form (see SM for further details). Data extraction from each of the included studies was carried out by four authors (GS, PS, MS, HG), with two randomized to each study; of those two, one was assigned to consolidate the two versions of extracted data into one dataset for each selected study. If needed, consolidators returned to the original study to resolve a discrepancy.
2.2. Quality Analysis
Two authors (PS, MS) independently evaluated the quality of each study to determine the validity of its recommendations. The Cochrane collaboration tool was used to assess risk of bias for randomized controlled trials [25,26,27], while the Newcastle–Ottawa quality assessment scale was used to assess risk of bias in cohort and case–control studies [28]. Discrepancies between scores were reconciled by a third author (SH). Due to the lack of a standardized quality assessment tool, the validity of studies that were lab-based, cross-sectional, or descriptive were evaluated by one author (PS), who compiled the limitations listed in each study from the latter study designs as described by the study’s authors.
2.3. Data Analysis
Included studies were stratified into three primary analytic domains: (1) the reuse and extended use of PPE manufactured as single-use, (2) methods for disinfecting PPE, and (3) efficacy of PPE by type and mode of pathogen transmission (droplets, aerosols, and fomites) (Figure 1). Reuse was defined as the repeated donning and doffing of the same pieces of PPE; extended use was defined as the practice of wearing the equipment throughout a shift or prolonged period without donning or doffing. Summary statistics were used to evaluate the types of PPE, modes of pathogen transmission, and settings under study, as well as the type of study, metrics used, and outcomes evaluated.
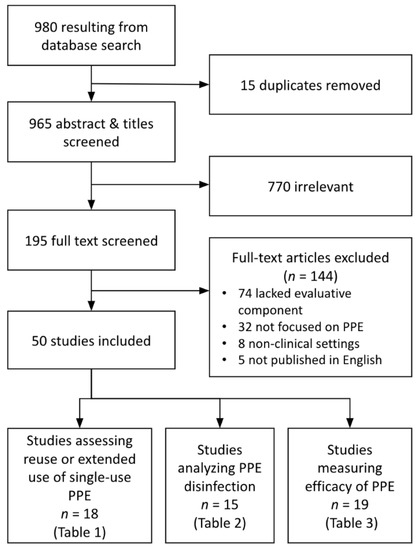
Figure 1.
PRISMA Diagram showing literature screening process and initial sorting for analysis.
Because this review sought to evaluate conservation methods for resource-limited settings, the human development index (HDI) was used to estimate the relative accessibility of each publication. In order to compare the applicability and global relevance of findings, we used the 2019 United Nations human development index to stratify study settings by relative country development level [29]. The HDI is a summary measure of achievement in health, education, and standard of living. Countries are considered to have a “very high” level of development with HDI of 0.800 or greater; “high” development with HDI of 0.700–0.799; “medium” development with HDI 0.550–0.699; and “low” with HDI < 0.550.
3. Results
3.1. Included Studies
After removing duplicates, the initial search yielded 980 studies (Figure 1). After screening, 50 articles met all inclusion criteria and were included for analysis. Eighteen studies assessed reuse or extended use of single-use PPE, 15 studies analyzed PPE disinfection methods, and 19 studies measured the efficacy of PPE, with 2 of the included studies meeting criteria for two categories. These studies were published in 27 different academic journals, with a plurality published by the American Journal of Infection Control (n = 10 papers) and the Journal of Occupational and Environmental Hygiene (n = 5). The publication dates ranged from 2008 to 2020, with 30% of included papers published in 2020 (prior to June) and 58% published in 2015 or later.
3.1.1. Geographic Distribution and Funding Sources
The 50 included studies spanned 14 countries, with some studies assessing multiple locations. The United States (45%) and China (20%) were the two most common settings. Forty-nine of the 50 studies originated in countries considered to have “high” or “very high” HDI, and 38 of these were conducted in countries ranked at a “very high” HDI. Three studies included countries with “medium” HDI, and no study was conducted in countries with “low” HDI. The average HDI of all included studies’ national setting was 0.905, more than the worldwide average HDI of 0.713.
Twenty-nine of the 50 studies were federally funded; four received university funding; three credited both federal and university funding; and 14 did not specify funding sources. Of the 23 studies from the United States, 18 were federally funded and five did not specify.
3.1.2. PPE Type, Study Setting, and Primary Outcome
The type of PPE evaluated varied across studies. N95 or elastomeric respirators were the most common type of masks evaluated (n = 35, or 70%), followed by surgical masks (n = 15, 30%) and cloth masks (n = 4, 8%). Four studies discussed improvised masks, and one studied only melt-blown fabric (a component of masks) due to a shortage of PPE. Aside from masks, five studies examined protective eyewear, two studied gloves, and five studied gowns. Two of the gown studies evaluated gown material rather than complete suits.
Seventeen studies (34%) took place in an in situ or clinical setting, while the remaining 33 were laboratory-based studies (defined as artificially replicating conditions of disease or PPE use, rather than examining an intervention or disease transmission in a clinical setting). Half of the studies included PPE disinfection (n = 25), measuring the impact of disinfection on PPE efficacy, PPE degradation, ability to reuse, and ability to effectively disinfect against specific pathogens.
Fourteen studies (28%) focused on fit testing or filtration efficacy of filtering face piece respirators (FFRs) for aerosols, and three papers studied protection from noninfectious contaminants such as chemicals. Seventeen remaining studies examined the use of PPE to protect against one or more infectious diseases, defined as a pathogen in a clinical setting or a (potentially surrogate) virus or bacteria used in a laboratory. Twelve studies measured degradation of PPE, four focused on degradation related to reuse of single-use PPE and nine studies measured the impact of disinfection on degradation of PPE. Of the 15 studies that measured the impact of PPE disinfection on reduction in contamination, eleven measured the effect of disinfection on viruses found on PPE surfaces and four studies focused on the impact of disinfection on bacteria or bacterial spores. Among all included studies, three specifically studied SARS-CoV-2, the virus causing COVID-19 [30,31,32]. The breadth of studies dedicated exclusively to COVID-19 has notably burgeoned as the pandemic has progressed.
3.2. Reuse and Extended Use of Disposable PPE
Of the 18 studies examining reuse or extended use of single-use PPE, five focused on in-situ, clinical settings and 13 were lab-based, as shown in Table 1. Overall, studies concluded that reuse can be done safely with some carefully implemented disinfection methodologies (see Supplemental Materials, SM, for description of all disinfection methods tested in the literature).

Table 1.
Extended use or multiple use of single-use PPE.
Many studies concluded that the extended use of eye protection and N95 respirators could be practiced safely with strict adherence to environmental and hand hygiene. For example, in a study evaluating surface contamination of N95 respirators and eye protection, no SARS-CoV-2 was detected by RT-PCR (reverse transcription polymerase chain reaction) from any surface of PPE worn by healthcare providers exiting hospital rooms of patients with COVID-19. No contamination was discovered on healthcare workers’ goggles, N95 respirators, or shoes worn for extended use while interacting with a series of COVID-19 patients for up to 25 min each [30].
A cross-sectional survey of infection control coordinators at hospitals in Vietnam, Pakistan, and China (medium HDI countries potentially more prone to supply shortages), demonstrated that extended use and reuse of cloth masks, surgical masks, and respirators were common practice. Examination of sample masks from participating sites revealed high penetration of particles through reused cloth and surgical masks compared with N95 respirators. This study proposed that respirators remain the most effective option compared with surgical or cloth masks, and that respirators can be reused as long as they are not visibly soiled or damaged [33].
A cluster-randomized trial conducted by MacIntyre et al. [49] found that hospital staff who wore N95 respirators throughout work shifts had fewer cases of clinical respiratory illness compared with staff who wore N95s only for high-risk procedures or when providing direct patient care under infection isolation precautions. Studies also found that N95 respirators were still effective barriers after donning and doffing. A study based in an infectious disease hospital in Brazil found that N95 respirators could be used by healthcare workers during shifts up to 12 hours and reused for up to five days [35]. A separate study found that N95 respirators could safely undergo five uses with repeated donning and doffing while maintaining filtration factors greater than 100 (considered to be effective protection); some respirator models could undergo 20 uses without fit test failure or a drop in filtration factor [37]. In contrast, a pilot study found that tethering devices such as elastic straps from some N95 respirator models could not withstand more than three donning and doffing repetitions before breaking or losing elasticity [41].
3.3. PPE Disinfection Methods
Fifteen studies focused on the disinfection of PPE through a variety of techniques (Table 2). Five studies focused on disinfecting bacterial pathogens in lab-based settings. Of the 10 studies focused on viral pathogens, two were in situ studies and eight were lab-based. In studies examining the reduction of contaminants, a 3 log10 or 5 log10 reduction in viable microorganisms was considered effective disinfection [50,51,52,53,54,55,56,57,58,59]. Overall, safe reuse depended on the specific mask material, with differences in contamination risk based on hydrophobicity or permeability; the type of contamination (bacterial, viral, non-disease-specific); the mode of application of disinfectant; and a range of other factors.
Table 2.
PPE disinfection methods against pathogens.
Viscusi et al. [59] demonstrated that moist heat incubation and microwave-generated steam decontamination—methods that can be used in a variety of settings—did not adversely affect efficacy or comfort with N95 respirators. Additionally, studies comparing multiple methods of disinfection found that ultraviolet germicidal irradiation (UVGI), ethylene oxide, vaporized hydrogen peroxide, and bleach did not adversely affect the efficacy of N95 and elastomeric respirators [42]. However, none of these studies assessed the effect of multiple rounds of decontamination on respirator function. In a separate study, higher intensities of UVGI used for decontamination led to a loss of strength and reduced efficacy of N95 respirator material [43]. Salter et al. [44] measured the deposition of toxic residues on filtering facepiece respirators after decontamination and found that the majority of decontamination methods tested did not leave significant residues on respirators. However, decontamination with ethylene oxide left behind toxic residues, and bleach caused discoloration and a lingering odor.
While many of the decontamination methods mentioned above, such as UVGI, ethylene oxide and vaporized hydrogen peroxide, require significant infrastructure and resources, several studies found that heat sterilization, which can be performed using fewer resources, was effective and could be repeated without detrimental effect to PPE. Steam or dry heat sterilization, repeated up to five times, effectively disinfected single-use N95 respirators without degrading the pressure drop, permeability, filtration factor, or penetrance of bacterial spray [45]. A separate study by Liao et al. found that heat sterilization could be repeated up to 50 times without adversely affecting filtration efficacy of the melt-blown fabric used in N95 respirators [46].
In addition to measuring the effect of disinfection on PPE efficacy and degradation, several studies evaluated disinfection methods against specific pathogens. Many of these disinfection methods, such as steam sterilization and chlorine-based disinfectants, can be used in a variety of settings without significant investment of infrastructure. Steam sterilization, either in the form of microwave-generated steam or steam from a household rice cooker, was effective in killing bacteria (Staphylococcus aureus) and influenza virus [39,43,44]. In addition, diluted chlorine solution effectively killed bacterial spores on gown material [57].
3.4. PPE Efficacy
PPE efficacy was measured most commonly through infection rate (n = 11) or filtration factor (n = 4). All other methods were grouped into a third category, “other metric” (n = 4). The infection rate studies were all conducted in clinical settings whereas the filtration factor and “other metric” studies were conducted in lab-based settings. Overall, N95 respirators were found to be superior to surgical masks in preventing infection from viruses transmited by aerosols but not more effective than surgical masks for pathogens transmitted through bacteria or fomites. Cloth masks were generally less effective than both surgical masks and N95 respirators. Finally, the one study that compared reusable gowns to disposable gowns found disposable gowns more impermeable to respiratory fluid.
3.4.1. Surgical Masks and N95 Respirators
Studies comparing infection transmission using either N95 respirators or surgical masks yielded varied results, summarized in Table 3. Overall, N95 respirators were more effective than surgical masks in preventing transmission or infection with viruses transmitted via aerosols. Wang et al. [32] evaluated the effect of N95 respirator use on SARS-CoV-2 transmission and found that N95 respirators were more effective than no mask use to prevent infection from SARS-CoV-2. Surgical masks were not evaluated in this study. With respect to prevention of infection with pathogens spread primarily via droplets or fomites (such as influenza or bacteria), N95s were not consistently more effective than surgical masks. Two randomized controlled studies in China found lower rates of clinical respiratory illness among healthcare workers who wore N95 respirators during work shifts compared with workers who wore surgical masks [49,63]. However, these studies found no difference in influenza-like illness or laboratory-confirmed respiratory viruses among groups and did not take into account infection exposure outside of the work environment.
Table 3.
Efficacy evaluations of PPE.
3.4.2. Cloth, Homemade, and Novel Masks
Studies evaluating the efficacy of cloth or homemade masks in preventing the spread of respiratory viruses are also shown in Table 3. In general, cloth or other homemade masks were less effective than surgical masks or N95s in blocking pathogens that are spread via aerosols. There was significant heterogeneity among studies and paucity of data related to droplet or fomite transmission. In an experimental model of respiratory virus transmission, cloth masks were half as effective as surgical masks and 50 times less effective than filtering facepiece respirators (FFP2, an equivalent to N95s) [76]. A randomized study of healthcare workers in Vietnam found that staff wearing surgical masks had lower rates of influenza-like illness and laboratory-confirmed respiratory virus compared with staff wearing cloth masks [64]. Conversely, a more recent study used aerosolized avian influenza virus and found that homemade cloth masks with internal layers of kitchen paper blocked 95% of aerosolized avian influenza virus, similar to the blocking effect of surgical masks and N95 respirators [61]. Overall, studies of novel or homemade masks yielded inferior results to N95s when evaluating aerosol transmission of pathogens. Our review found a lack of studies evaluating the effectiveness of novel PPE for protection from respiratory pathogens spread through respiratory droplets or fomites [72,74,77].
3.4.3. Other, Non-Mask PPE
Only one study evaluated the efficacy of reusable gowns, which could reduce reliance on disposable gowns during shortages and reduce environmental burdens [78]. In this simulation, all participants wearing reusable surgical gowns had evidence of respiratory fluid permeation onto their underlying scrubs (Table 3). After multiple washes, the reusable gowns lost their protection from permeation, while the control participant wearing a disposable gown had no permeation of respiratory fluid [38].
3.5. Quality of Included Studies
Results of our quality and bias assessment are shown in SM Figure S1 for included RCT studies and SM Table S1 for included cohort and case–control studies. Of the 50 studies reviewed, 36 did not fall into the categories of RCT, cohort, or case–control and thus were not able to be assessed for bias through either the Newcastle–Ottawa or Cochrane tools. Instead, we conducted a qualitative analysis of bias through comparison of the limitations listed in each paper. The majority of these studies took place in a lab setting and tested the efficacy of various decontamination methods.
For these 36 studies, the most commonly mentioned limitations included small sample size, evaluation of decontamination method for only one type of filtering facepiece respirator, absence of assessing fit and filtration efficiency after decontamination, lack of decontamination effect assessment on mask straps or nose pieces, and only evaluating decontamination efficacy against one microorganism. Overall concerns in many of the lab studies were that decontamination processes were not tested in a true healthcare setting, suggesting further research would be needed before implementing changes in medical facilities. Thirteen of these studies (26%) did not list limitations [31,33,34,35,38,39,53,57,60,61,73,75,77].
4. Discussion
This literature review was motivated by the COVID-19 pandemic, which overwhelmed healthcare facilities, disrupted supply chains, and caused shortages of single-use PPE in the U.S. and worldwide [79]. We are also concerned about the sustainability of medical systems, including the waste generation from single-use PPE [12,80] and the impact of climate change on medical supply chains [22]. Understanding the state of the literature on the efficacy of various types of PPE and conservation practices in healthcare settings at the early stages of the COVID-19 pandemic can help contextualize how systems’ responses have since developed, thus informing future supply chain management and resilience strategies. Prioritizing effective, reusable PPE practices could reduce excess waste in highly-resourced settings, allow redistribution of supplies to resource-limited settings, and help prepare for future infectious outbreaks.
We found that there are safe and effective ways to reuse N95s in circumstances when protection from aerosols is necessary. However, any reuse inevitably carries the risk of contamination or reduced efficacy. Many factors contribute to the safe reuse of respirators, such as a standardized process for donning and doffing and stable storage conditions. Improper doffing can enable the transfer of contaminants [40], and storage conditions with limited humidity prevent the survival of contaminating microorganisms [39]. When facing a low quantity of available PPE, extended use can limit waste [30,35] and can be done safely with standardized extended use practices that include proper donning and doffing [30,35,40,49]. Further research should focus on developing low-cost, widely accessible PPE for repeated use.
Some of the included studies developed effective disinfection methods that may not be financially or logistically feasible during outbreaks of infection or in low-resource settings, as they may require significant resource investment [31,57,60]. Disinfection methods that required significant infrastructure or cost include vaporized hydrogen peroxide and pulsed xenon ultraviolet light. On the other hand, effective disinfectants using common and inexpensive methods, such as microwave steam bags and steam sterilization using a kitchen rice cooker, are available to healthcare settings with limited resources [36,42,47,52,54,58,61].
Overall, included studies suggest that N95 respirators are superior to surgical masks with respect to preventing spread and acquisition of pathogens that are spread by aerosols. For pathogens that are spread through respiratory droplets and fomites, surgical masks can be as effective as N95 respirators. Several studies found surgical masks to be more effective than cloth masks. There are several potential reasons for this, including the mode of transmission studied (aerosol vs droplet) and variability in materials or fit of cloth and novel masks [61,64,65,66,76]. This suggests that the cost of surgical masks, rather than use or reuse of cloth masks, is worth prioritizing despite limited resources. The additional cost of N95s can be reserved for aerosol-generating procedures, direct care of patients with respiratory pathogens that are transmitted via aerosols, and during seasons with high transmission of respiratory viruses.
Our findings are consistent with those of Rowan and Laffey’s recent rapid review of SARS-CoV-2-related PPE use and reuse, which found varied global techniques for PPE reuse and reprocessing in the setting of the COVID-19 pandemic [8]. They suggest that appropriate disinfection and reuse of face coverings are important public health measures and that uptake of reusable PPE should increase. Similarly, literature reviews of N95s by Rodriguez-Martinez et. al, Seresirikachorn et. al, O’Hearn et. al, Toomey et. al, Paul et. al., and Gnatta et al. [13,14,15,16,18,81] conclude multiple decontamination approaches are appropriate for N95s, most notably ultraviolet germicidal irradiation and vaporized hydrogen peroxide; however, all studies note a lack of strong research.
Our review spanned 14 countries and included analyses conducted both during times of disease outbreak and otherwise. It also captured multiple unconventional and innovative study methodologies. The variety of conclusions in the literature illustrates that responses to infectious disease outbreaks are highly context- and microbe-specific, requiring robust but sustainable supply chains. Standardizing the metrics of PPE efficacy could enable more accurate comparison and determination of best practices for conservation.
Limitations
Given the variety of study settings and approaches in the included literature, we were unable to quantitatively compare equivalent outcome metrics or variables across all studies. Instead, we qualitatively compared the main findings and recommendations. In addition, our review did not include publications after June 2020. Thus, we intentionally focus on the literature that existed during the early stages of the COVID-19 pandemic, when healthcare settings made emergency response decisions about PPE.
Contrary to our initial hypothesis, the average HDI of study locations included in this review was higher than the worldwide average. Only two included studies attempted to summarize the diverse field of PPE use and conservation practices in low-resource settings [33,64]. Off-label reuse practices frequently occur in settings without strict regulations [33], but the safety and efficacy of these practices have not been studied. Further research on these practices would illuminate both safer approaches to resource conservation in resource-limited settings and safe PPE conservation practices that can be employed broadly for greater environmental sustainability and resilience [19].
The methods deemed successful by this body of research cannot be generalized to low- and middle-income countries, which might have different resource and cost constraints [82]. Future literature reviews are needed to address dimensions of PPE use and reuse that were not evaluated in our systematic review, such as cost and comfort.
5. Conclusions
This review identified multiple methods for safe and effective reuse and disinfection of single-use PPE such as N95 respirators, which can be viable options for conserving PPE in different healthcare settings and for use by the public. It also highlights that surgical masks, which are lower in cost compared with N95 respirators, are effective in reducing the risk of infection from pathogens spread via respiratory droplets and fomites.
Future research should prioritize (i) assessing the type and effectiveness of PPE conservation practices in developing contexts, (ii) the development of low-cost PPE that can be disinfected and reused, (iii) the creation of protocols for healthcare systems to safely reuse and disinfect existing single-use PPE during times of extreme shortage, and (iv) the standardization of updated criteria for the use of surgical masks vs N95 respirators for specific infectious diseases. Such interventions would both bolster our preparedness for future supply shortages in times of healthcare overutilization, as well as reduce the environmentally harmful volume of waste generated by healthcare systems.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ijerph20032575/s1, File S1: Inclusion and Exclusion Criteria, HDI Calculations, Extraction Form, a Summary of Each Disinfection Method in Included Disinfection Studies, and Risk of Bias and Quality Assessments.
Author Contributions
Conceptualization, C.L.T., R.V., O.E.-S. and S.E.H.; methodology, T.R., C.L.T., R.V., O.E.-S., S.E.H., P.H.L. and G.A.; software, T.R.; validation, all team members; formal analysis, P.H.L., G.A., P.S., G.S.S., M.S., H.C.G. and M.D.; writing—original draft preparation, P.S., G.S.S., H.C.G., M.S., S.E.H., C.L.T. and T.R.; writing—review and editing, entire study team; visualization, P.S., G.S.S., H.C.G., M.S., M.D., P.H.L. and G.A.; supervision, C.L.T., S.E.H., O.E.-S. and R.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was exempt from ethical review and approval by the NYU Grossman School of Medicine Institutional Review Board because it did not directly involve human subjects research.
Informed Consent Statement
Not applicable. This study did not involve human subjects.
Data Availability Statement
A spreadsheet of included articles and extracted data is available upon request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Haren, P.; Simchi-Levi, D. Operations Management: How Coronavirus Could Impact the Global Supply Chain by Mid-March. Harv. Bus. Rev. 2020, 1–4. [Google Scholar]
- Patel, A.; D’Alessandro, M.M.; Ireland, K.J.; Burel, W.G.; Wencil, E.B.; Rasmussen, S.A. Personal protective equipment supply chain: Lessons learned from recent public health emergency responses. Health Secur. 2017, 15, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Daugherty, E.L. Health care worker protection in mass casualty respiratory failure: Infection control, decontamination, and personal protective equipment. Respir. Care 2008, 53, 201–214. [Google Scholar] [PubMed]
- Rebmann, T.; Citarella, B.; Alexander, S.; Russell, B.; Volkman, J.C. Personal protective equipment use and allocation in home health during disasters. Am. J. Infect. Control 2011, 39, 823–831. [Google Scholar] [CrossRef]
- Rebmann, T.; Wilson, R.; Bartley, J.; Stricof, R. Update on infection prevention in disaster planning: New resources and policies. Am. J. Infect. Control 2009, 37, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Beckman, S.; Materna, B.; Goldmacher, S.; Zipprich, J.; D’Alessandro, M.; Novak, D.; Harrison, R. Evaluation of respiratory protection programs and practices in California hospitals during the 2009–2010 H1N1 influenza pandemic. Am. J. Infect. Control 2013, 41, 1024–1031. [Google Scholar] [CrossRef] [PubMed]
- WHO. Rational Use of Personal Protective Equipment for Coronavirus Disease 2019 (COVID-19); The World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Rowan, N.J.; Laffey, J.G. Unlocking the surge in demand for personal and protective equipment (PPE) and improvised face coverings arising from coronavirus disease (COVID-19) pandemic—Implications for efficacy, re-use and sustainable waste management. Sci. Total Environ. 2021, 752, 142259. [Google Scholar] [CrossRef]
- Suran, M. HHS Initiative to Reduce Health Risks of Climate-Related Hazards. JAMA 2022, 327, 2385. [Google Scholar] [CrossRef]
- Marazziti, D.; Cianconi, P.; Mucci, F.; Foresi, L.; Chiarantini, C.; Della Vecchia, A. Climate change, environment pollution, COVID-19 pandemic and mental health. Sci. Total Environ. 2021, 773, 145182. [Google Scholar] [CrossRef]
- Watts, N.; Amann, M.; Arnell, N.; Ayeb-Karlsson, S.; Beagley, J.; Belesova, K.; Boykoff, M.; Byass, P.; Cai, W.; Campbell-Lendrum, D.; et al. The 2020 report of The Lancet Countdown on health and climate change: Responding to converging crises. Lancet 2021, 397, 129–170. [Google Scholar] [CrossRef]
- Hicks, A.; Temizel-Sekeryan, S.; Kontar, W.; Ghamkhar, R.; Rodríguez Morris, M. Personal respiratory protection and resiliency in a pandemic, the evolving disposable versus reusable debate and its effect on waste generation. Resour. Conserv. Recycl. 2021, 168, 105262. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Martinez, C.E.; Sossa-Briceño, M.P.; Cortés, J.A. Decontamination and reuse of N95 filtering facemask respirators: A systematic review of the literature. Am. J. Infect. Control 2020, 48, 1520–1532. [Google Scholar] [CrossRef] [PubMed]
- Seresirikachorn, K.; Phoophiboon, V.; Chobarporn, T.; Tiankanon, K.; Aeumjaturapat, S.; Chusakul, S.; Snidvongs, K. Decontamination and reuse of surgical masks and N95 filtering facepiece respirators during the COVID-19 pandemic: A systematic review. Infect. Control Hosp. Epidemiol. 2021, 42, 25–30. [Google Scholar] [CrossRef] [PubMed]
- O’Hearn, K.; Gertsman, S.; Sampson, M.; Webster, R.J.; Tsampalieros, A.; Ng, R.; Gibson, J.; Lobos, A.-T.; Acharya, N.; Agarwal, A. Decontaminating N95 masks with Ultraviolet Germicidal Irradiation (UVGI) does not impair mask efficacy and safety: A Systematic Review. OSF Preprints 2020, 31. [Google Scholar] [CrossRef]
- Gnatta, J.R.; de Souza, R.Q.; Lemos, C.D.S.; Oliveira, R.A.; Martins, L.R.; Moriya, G.A.D.A.; Poveda, V.D.B. Safety in the practice of decontaminating filtering facepiece respirators: A systematic review. Am. J. Infect. Control 2021, 49, 825–835. [Google Scholar] [CrossRef]
- Peters, A.; Lotfinejad, N.; Palomo, R.; Zingg, W.; Parneix, P.; Ney, H.; Pittet, D. Decontaminating N95/FFP2 masks for reuse during the COVID-19 epidemic: A systematic review. Antimicrob Resist Infect Control 2021, 10, 144. [Google Scholar] [CrossRef]
- Paul, D.; Gupta, A.; Maurya, A.K. Exploring options for reprocessing of N95 Filtering Facepiece Respirators (N95-FFRs) amidst COVID-19 pandemic: A systematic review. PLoS ONE 2020, 15, e0242474. [Google Scholar] [CrossRef]
- Steyn, A.; Cassels-Brown, A.; Chang, D.; Faal, H.; Vedanthan, R.; Venkatesh, R.; Thiel, C. Frugal innovation for global surgery: Leveraging lessons from low- and middle-income countries to optimise resource use and promote value-based care. Bull. R. Coll. Surg. Engl. 2020, 102, 198–200. [Google Scholar] [CrossRef]
- Goel, H.; Wemyss, T.A.; Harris, T.; Steinbach, I.; Stancliffe, R.; Cassels-Brown, A.; Thomas, P.B.M.; Thiel, C.L. Improving productivity, costs and environmental impact in International Eye Health Services: Using the ‘Eyefficiency’ cataract surgical services auditing tool to assess the value of cataract surgical services. BMJ Open Ophthalmol. 2021, 6, e000642. [Google Scholar] [CrossRef]
- Thiel, C.L.; Schehlein, E.; Ravilla, T.; Ravindran, R.D.; Robin, A.L.; Saeedi, O.J.; Schuman, J.S.; Venkatesh, R. Cataract surgery and environmental sustainability: Waste and lifecycle assessment of phacoemulsification at a private healthcare facility. J. Cataract. Refract. Surg. 2017, 43, 1391–1398. [Google Scholar] [CrossRef]
- Dzau, V.J.; Levine, R.; Barrett, G.; Witty, A. Decarbonizing the US Health Sector—A Call to Action. N. Engl. J. Med. 2021, 385, 2117–2119. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Veritas Health Innovation. Covidence Systematic Review Software; Veritas Health Innovation: Melbourne, Australia, 2021. [Google Scholar]
- Saunders-Hastings, P.; Crispo, J.A.; Sikora, L.; Krewski, D. Effectiveness of personal protective measures in reducing pandemic influenza transmission: A systematic review and meta-analysis. Epidemics 2017, 20, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A. Assessing risk of bias in a randomized trial. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Chichester, UK, 2019; pp. 205–228. [Google Scholar]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2011; pp. 1–12. [Google Scholar]
- United Nations Development Programme. Human Development Report 2020: Reader’s Guide; United Nations Development Programme: New York, NY, USA, 2020. [Google Scholar]
- Ong, S.W.X.; Tan, Y.K.; Sutjipto, S.; Chia, P.Y.; Young, B.E.; Gum, M.; Lau, S.K.; Chan, M.; Vasoo, S.; Mendis, S. Absence of contamination of personal protective equipment (PPE) by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Infect. Control Hosp. Epidemiol. 2020, 41, 614–616. [Google Scholar] [CrossRef]
- Grossman, J.; Pierce, A.; Mody, J.; Gagne, J.; Sykora, C.; Sayood, S.; Cook, S.; Shomer, N.; Liang, S.Y.; Eckhouse, S.R. Institution of a novel process for N95 respirator disinfection with vaporized hydrogen peroxide in the setting of the COVID-19 pandemic at a large academic medical center. J. Am. Coll. Surg. 2020, 231, 275–280. [Google Scholar] [CrossRef]
- Wang, X.; Pan, Z.; Cheng, Z. Association between 2019-nCoV transmission and N95 respirator use. MedRxiv 2020, 105, 104–105. [Google Scholar] [CrossRef]
- Chughtai, A.A.; MacIntyre, C.R.; Ashraf, M.O.; Zheng, Y.; Yang, P.; Wang, Q.; Dung, T.C. Practices around the use of masks and respirators among hospital health care workers in 3 diverse populations. Am. J. Infect. Control 2015, 43, 1116–1118. [Google Scholar] [CrossRef]
- Mathias, J.M. Reusable protective eyewear tied to greater risk of contamination. OR Manag. 2015, 31, 16–17. [Google Scholar]
- Duarte, L.R.P.; Miola, C.E.; Cavalcante, N.J.F.; Bammann, R.H. Maintenance status of N95 respirator masks after use in a health care setting. Rev. Esc. Enferm. USP 2010, 44, 1011–1016. [Google Scholar] [CrossRef]
- Bessesen, M.T.; Adams, J.C.; Radonovich, L.; Anderson, J. Disinfection of reusable elastomeric respirators by health care workers: A feasibility study and development of standard operating procedures. Am. J. Infect. Control 2015, 43, 629–634. [Google Scholar] [CrossRef]
- Bergman, M.S.; Viscusi, D.J.; Zhuang, Z.Z.; Palmiero, A.J.; Powell, J.B.; Shaffer, R.E. Impact of multiple consecutive donnings on filtering facepiece respirator fit. Am. J. Infect. Control 2011, 40, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Lockhart, S.; Naidu, J.J.; Badh, C.S.; Duggan, L.V. Simulation as a tool for assessing and evolving your current personal protective equipment: Lessons learned during the coronavirus disease (COVID-19) pandemic. Can. J. Anesth. 2020, 67, 895–896. [Google Scholar] [CrossRef] [PubMed]
- Majchrzycka, K.; Okrasa, M.; Skóra, J.; Gutarowska, B. Evaluation of the survivability of microorganisms deposited on filtering respiratory protective devices under varying conditions of humidity. Int. J. Environ. Res. Public Health 2016, 13, 98. [Google Scholar] [CrossRef] [PubMed]
- Brady, T.M.; Strauch, A.L.; Almaguer, C.M.; Niezgoda, G.; Shaffer, R.E.; Yorio, P.L.; Fisher, E.M. Transfer of bacteriophage MS2 and fluorescein from N95 filtering facepiece respirators to hands: Measuring fomite potential. J. Occup. Environ. Hyg. 2017, 14, 898–906. [Google Scholar] [CrossRef]
- Roberge, R.; Niezgoda, G.; Benson, S. Analysis of forces generated by N95 filtering facepiece respirator tethering devices: A pilot study. J. Occup. Environ. Hyg. 2012, 9, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Viscusi, D.J.; Bergman, M.S.; Eimer, B.C.; Shaffer, R.E. Evaluation of five decontamination methods for filtering facepiece respirators. Ann. Occup. Hyg. 2009, 53, 815–827. [Google Scholar] [CrossRef]
- Lindsley, W.G.; Martin Jr, S.B.; Thewlis, R.E.; Sarkisian, K.; Nwoko, J.O.; Mead, K.R.; Noti, J.D. Effects of ultraviolet germicidal irradiation (UVGI) on N95 respirator filtration performance and structural integrity. J. Occup. Environ. Hyg. 2015, 12, 509–517. [Google Scholar] [CrossRef]
- Salter, W.; Kinney, K.; Wallace, W.; Lumley, A.; Heimbuch, B.; Wander, J. Analysis of residual chemicals on filtering facepiece respirators after decontamination. J. Occup. Environ. Hyg. 2010, 7, 437–445. [Google Scholar] [CrossRef]
- De Man, P.; Van Straten, B.; Van den Dobbelsteen, J.; Van Der Eijk, A.; Horeman, T.; Koeleman, H. Sterilization of disposable face masks by means of standardized dry and steam sterilization processes; an alternative in the fight against mask shortages due to COVID-19. J. Hosp. Infect. 2020, 105, 356–357. [Google Scholar] [CrossRef]
- Liao, L.; Xiao, W.; Zhao, M.; Yu, X.; Wang, H.; Wang, Q.; Chu, S.; Cui, Y. Can N95 respirators be reused after disinfection? How many times? ACS Nano 2020, 14, 6348–6356. [Google Scholar] [CrossRef] [PubMed]
- Fisher, E.M.; Williams, J.L.; Shaffer, R.E. Evaluation of microwave steam bags for the decontamination of filtering facepiece respirators. PLoS ONE 2011, 6, e18585. [Google Scholar] [CrossRef] [PubMed]
- Zhong, H.; Zhu, Z.; Lin, J.; Cheung, C.F.; Lu, V.L.; Yan, F.; Chan, C.Y.; Li, G. Reusable and Recyclable Graphene Masks with Outstanding Superhydrophobic and Photothermal Performances. ACS Nano. 2020, 14, 6213–6221. [Google Scholar] [CrossRef] [PubMed]
- MacIntyre, C.R.; Wang, Q.; Seale, H. A randomized clinical trial of three options for N95 respirators and medical masks in health workers. Am. J. Respir. Crit. Care Med. 2013, 187, 960–966. [Google Scholar] [CrossRef]
- Heimbuch, B.K.; Wallace, W.H.; Kinney, K.R.; Lumley, A.E.; Wu, C.-Y.; Woo, M.-H.; Wander, J.D. A pandemic influenza preparedness study: Use of energetic methods to decontaminate filtering facepiece respirators contaminated with H1N1 aerosols and droplets. Am. J. Infect. Control 2012, 39, e1–e9. [Google Scholar] [CrossRef] [PubMed]
- Jinadatha, C.; Simmons, S.; Dale, C.; Ganachari-Mallappa, N.; Villamaria, F.C.; Goulding, N.; Tanner, B. Disinfecting personal protective equipment with pulsed xenon ultraviolet as a risk mitigation strategy for health care workers. Am. J. Infect. Control 2015, 43, 412–414. [Google Scholar] [CrossRef]
- Lawrence, C.; Harnish, D.A.; Sandoval-Powers, M.; Mills, D.; Bergman, M.; Heimbuch, B.K. Assessment of half-mask elastomeric respirator and powered air-purifying respirator reprocessing for an influenza pandemic. Am. J. Infect. Control 2017, 45, 1324–1330. [Google Scholar] [CrossRef]
- Lemmer, K.; Howaldt, S.; Heinrich, R.; Roder, A.; Pauli, G.; Dorner, B.G.; Pauly, D. Test methods for estimating the efficacy of the fast-acting disinfectant peracetic acid on surfaces of personal protective equipment. J. Appl. Microbiol. 2017, 123, 1168–1183. [Google Scholar] [CrossRef]
- Li, D.F.; Cadnum, J.L.; Redmond, S.N.; Jones, L.D.; Donskey, C.J. It’s not the heat, it’s the humidity: Effectiveness of a rice cooker-steamer for decontamination of cloth and surgical face masks and N95 respirators. Am. J. Infect. Control 2020, 48, 854–855. [Google Scholar] [CrossRef]
- Lore, M.B.; Heimbuch, B.K.; Brown, T.L.; Wander, J.D.; Hinrichs, S.H. Effectiveness of three decontamination treatments against influenza virus applied to filtering facepiece respirators. Ann. Occup. Hyg. 2012, 56, 92–101. [Google Scholar] [CrossRef]
- Mills, D.; Harnish, D.A.; Lawrence, C.; Sandoval-Powers, M.; Heimbuch, B.K. Ultraviolet germicidal irradiation of influenza-contaminated N95 filtering facepiece respirators. Am. J. Infect. Control 2018, 46, e49–e55. [Google Scholar] [CrossRef]
- Papp, S.; Kimmerl, K.; Gatz, J.; Laue, M.; Grunow, R.; Kaspari, O. Evaluation of sporicidal disinfectants for the disinfection of personal protective equipment during biological hazards. Health Secur. 2020, 18, 36–48. [Google Scholar] [CrossRef]
- Robinson, G.L.; Hitchcock, S.; Kpadeh-Rogers, Z.; Karikari, N.; Johnson, J.K.; Blanco, N.; Morgan, D.J. Preventing Viral Contamination: Effects of Wipe and Spray-based Decontamination of Gloves and Gowns. Clin. Infect. Dis. 2019, 69, S228–S230. [Google Scholar] [CrossRef] [PubMed]
- Viscusi, D.J.; Bergman, M.S.; Novak, D.A.; Faulker, K.A.; Palmiero, A.; Powell, J.; Shaffer, R.E. Impact of three biological decontamination methods on filtering facepiece respirator fit, odor, comfort, and donning ease. J. Occup. Environ. Hyg. 2011, 8, 426–436. [Google Scholar] [CrossRef] [PubMed]
- Cheng, V.; Wong, S.; Kwan, G.; Hui, W.; Yuen, K. Disinfection of N95 respirators by ionized hydrogen peroxide during pandemic coronavirus disease 2019 (COVID-19) due to SARS-CoV-2. J. Hosp. Infect. 2020, 105, 358–359. [Google Scholar] [CrossRef]
- Ma, Q.X.; Shan, H.; Zhang, H.L.; Li, G.M.; Yang, R.M.; Chen, J.M. Potential utilities of mask-wearing and instant hand hygiene for fighting SARS-CoV-2. J Med Virol. 2020, 92, 1567–1571. [Google Scholar] [CrossRef]
- Subhash, S.S.; Cavaiuolo, M.; Radonovich, L.J.; Eagan, A.; Lee, M.L.; Campbell, S.; Martinello, R.A. Effectiveness of Common Healthcare Disinfectants against H1N1 Influenza Virus on Reusable Elastomeric Respirators. Infect Control Hosp Epidemiol. 2014, 35, 894–897. [Google Scholar] [CrossRef]
- MacIntyre, C.R.; Wang, Q.; Cauchemez, S. A cluster randomized clinical trial comparing fit-tested and non-fit-tested N95 respirators to medical masks to prevent respiratory virus infection in health care workers. Influenza Other Respir. Viruses 2011, 5, 170–179. [Google Scholar] [CrossRef] [PubMed]
- MacIntyre, C.R.; Seale, H.; Tham, D.C.; Hien, N.D.; Nga, P.T.; Chughtai, A.A.; Rahman, M.B. A cluster randomised trial of cloth masks compared with medical masks in healthcare workers. BMJ Open 2015, 5, e006577. [Google Scholar] [CrossRef]
- Mukerji, S.; MacIntyre, C.R.; Seale, H.; Wang, Q.; Yang, P.; Wang, X.; Newall, A.T. Cost-effectiveness analysis of N95 respirators and medical masks to protect healthcare workers in China from respiratory infections. BMC Infect. Dis. 2017, 17, 464. [Google Scholar] [CrossRef]
- Loeb, M.; Dafoe, N.; Mahony, J.; John, M.; Sarabia, A.; Glavin, V.; Webby, R. Surgical mask vs N95 respirator for preventing influenza among health care workers: A randomized trial. JAMA J. Am. Med. Assoc. 2009, 302, 1865–1871. [Google Scholar] [CrossRef]
- Jacobs, J.L.; Ohde, S.; Takahashi, O.; Tokuda, Y.; Omata, F.; Fukui, T. Use of surgical face masks to reduce the incidence of the common cold among health care workers in Japan: A randomized controlled trial. Am J Infect Control. 2009, 37, 417–419. [Google Scholar] [CrossRef] [PubMed]
- Cowling, B.J.; Fung, R.O.P.; Cheng, C.K.Y.; Fang, V.J.; Chan, K.H.; Seto, W.H.; Yung, R.; Chiu, B.; Lee, P.; Uyeki, T.M.; et al. Preliminary Findings of a Randomized Trial of Non-Pharmaceutical Interventions to Prevent Influenza Transmission in Households. PLoS ONE 2008, 3, e2101. [Google Scholar] [CrossRef] [PubMed]
- Ang, B.; Poh, B.F.; Win, M.K.; Chow, A. Surgical masks for protection of health care personnel against pandemic novel swine-origin influenza A (H1N1)-2009: Results from an observational study. Clin Infect Dis. 2010, 50, 1011–1014. [Google Scholar] [CrossRef] [PubMed]
- Radonovich, L.J.; Simberkoff, M.S.; Bessesen, M.T.; Brown, A.C.; Cummings, D.A.T.; Gaydos, C.A.; Los, J.G.; Krosche, A.E.; Gibert, C.L.; Gorse, G.J.; et al. N95 Respirators vs Medical Masks for Preventing Influenza Among Health Care Personnel: A Randomized Clinical Trial. JAMA 2019, 322, 824–833. [Google Scholar] [CrossRef] [PubMed]
- MacIntyre, C.R.; Wang, Q.; Rahman, B.; Seale, H.; Ridda, I.; Gao, Z.; Yang, P.; Shi, W.; Pang, X.; Zhang, Y.; et al. Efficacy of face masks and respirators in preventing upper respiratory tract bacterial colonization and co-infection in hospital healthcare workers. Prev Med. 2014, 62, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Majchrzycka, K.; Gutarowska, B.; Brochocka, A. Aspects of tests and assessment of filtering materials used for respiratory protection against bioaerosols. Part II: Sweat in the environment, microorganisms in the form of a bioaerosol. Int. J. Occup. Saf. Ergon. 2010, 16, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Carnino, J.M.; Ryu, S.; Ni, K.; Jin, Y. Pretreated household materials carry similar filtration protection against pathogens when compared with surgical masks. Am. J. Infect. Control 2020, 48, 883–889. [Google Scholar] [CrossRef]
- Au, S.S.; Gomersall, C.D.; Leung, P.; Li, P.T. A randomised controlled pilot study to compare filtration factor of a novel non-fit-tested high-efficiency particulate air (HEPA) filtering facemask with a fit-tested N95 mask. J Hosp Infect. 2010, 76, 23–25. [Google Scholar] [CrossRef] [PubMed]
- Quan, F.S.; Rubino, I.; Lee, S.-H.; Koch, B.; Choi, H.-J. Universal and reusable virus deactivation system for respiratory protection. Sci. Rep. 2017, 7, 39956. [Google Scholar] [CrossRef] [PubMed]
- Van der Sande, M.; Teunis, P.; Sabel, R. Professional and home-made face masks reduce exposure to respiratory infections among the general population. PLoS ONE 2008, 3, e2618. [Google Scholar] [CrossRef] [PubMed]
- Greig, P.; Carvalho, C.; El-Boghdadly, K.; Ramessur, S. Safety testing improvised COVID-19 personal protective equipment based on a modified full-face snorkel mask. Anaesthesia 2020, 75, 970–971. [Google Scholar] [CrossRef] [PubMed]
- Baker, N.; Bromley-Dulfano, R.; Chan, J.; Gupta, A.; Herman, L.; Jain, N.; Taylor, A.L.; Lu, J.; Pannu, J.; Patel, L.; et al. COVID-19 Solutions Are Climate Solutions: Lessons From Reusable Gowns. Front. Public Health 2020, 8, 590275. [Google Scholar] [CrossRef] [PubMed]
- Ranney, M.L.; Griffeth, V.; Jha, A.K. Critical Supply Shortages—The Need for Ventilators and Personal Protective Equipment during the Covid-19 Pandemic. N. Engl. J. Med. 2020, 382, e41. [Google Scholar] [CrossRef]
- Benson, N.U.; Bassey, D.E.; Palanisami, T. COVID pollution: Impact of COVID-19 pandemic on global plastic waste footprint. Heliyon 2021, 7, e06343. [Google Scholar] [CrossRef] [PubMed]
- Toomey, E.; Conway, Y.; Burton, C.; Smith, S.; Smalle, M.; Chan, X.; Adisesh, A.; Tanveer, S.; Ross, L.; Thomson, I.; et al. Extended use or re-use of single-use surgical masks and filtering facepiece respirators: A rapid evidence review. medRxiv 2020, 42, 75–83. [Google Scholar] [CrossRef]
- Boutayeb, A. The burden of communicable and non-communicable diseases in developing countries. Handbook of Disease Burdens and Quality of Life Measures; Springer: New York, NY, USA, 2010; pp. 531–546. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).