
Physical Activity and Exercise Experience in Spanish and US Men with Fibromyalgia: A Qualitative Cross-Cultural Study

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants and Setting
2.3. Data Collection
2.3.1. Spain
2.3.2. United States
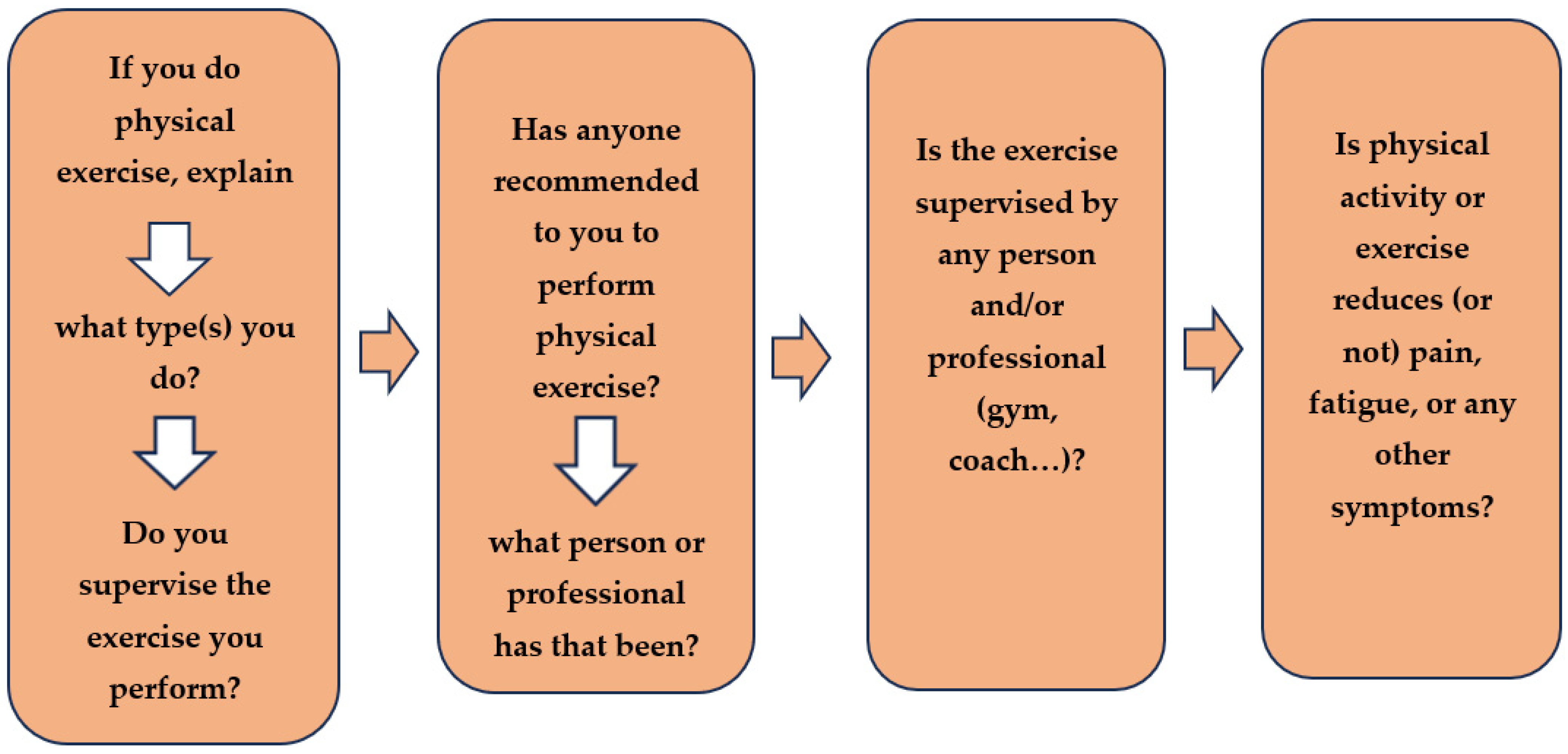
- If you do physical activity or exercise, explain what type(s) you do and if you supervise the exercise you perform.
- If anyone has recommended to you to perform physical exercise, what person or professional has that been?
- If the exercise you perform is supervised by any person and/or professional (gym, coach…).
- If physical activity or exercise reduces (or not) pain, fatigue, or any other symptoms. Describe the benefits or harmful effects in detail.
2.4. Data Analysis
2.5. Rigor
- Credibility: The first and third researchers were involved in data collection, analysis, and reporting of the findings; both were experts in qualitative methodology. Each of these researchers was assisted by a Ph.D. student in Spain and a nursing student in the US. All authors contributed to the writing of the manuscript and read, reviewed, and approved the final draft of the manuscript.
- Transferability: The transferability of the study is derived from a detailed description of the context of the study which were specialized units of fibromyalgia and confirmed diagnosis in all the volunteers. All those who agreed to participate did not drop out. The unification of the categorization and analysis process by the research team brought to light the experiences of these men with FMS that may resonate with other men with FMS.
- Reliability: The codification and categorization were carried out by the four researchers, working in pairs. Each pair of researchers in the US and Spain coded each transcript together to ensure consistent coding. Together, the four researchers built code definitions and reviewed coding decisions with each other in frequent meetings throughout the analysis. In addition, the different and multiple meetings via Skype by the three first members finished defining the final themes, categories, and subcategories. These were approved by the consensus of the whole group. The terms “physical exercise” and “physical activity” were analyzed in depth by 7 researchers, one of them a physiotherapist and Ph.D. in Anthropology, the rheumatologist, the second author professor, Ph.D. in Psychology, and the two authors in senior position, specialists in internal medicine and Ph.D. in Medicine.
- Confirmability: The original data, including draft and data analysis records, were safely stored for future reference. In addition, to observe the similarity and differences between the two countries, the US researchers translated the text into English and the Spanish into English?
2.6. Ethical Considerations
3. Results
3.1. Sample Characteristics
3.2. The Exercise Experience of Men
3.2.1. Theme 1: Understanding What Constitutes Physical Activity or Exercise
Associate the Meaning of the Term Physical Activity as Physical Exercise (a Sport or Planned Activity with the Objective of Improved Health)
Associate the Exercise with Physical Activity
3.2.2. Theme 2: Facilitating or Discouraging the Performance of Physical Exercise
Recommendation of Physical Exercise by a Specialist
Opiates Affect Exercise Performance
3.2.3. Theme 3: Effects of Physical Activity or Exercise in Symptom, Psychological, and Social Aspects
Harmful Effects
Beneficial Effects
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vincent, A.; Benzo, R.P.; Whipple, M.O.; McAllister, S.J.; Erwin, P.J.; Saligan, L.N. Beyond pain in fibromyalgia: Insights into the symptom of fatigue. Arthritis Res. Ther. 2013, 15, 221. [Google Scholar] [CrossRef] [PubMed]
- Häuser, W.; Thieme, K.; Turk, D.C. Guidelines on the management of fibromyalgia syndrome—A systematic review. Eur. J. Pain 2010, 14, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Turk, D.C.; Adams, L.M. Using a biopsychosocial perspective in the treatment of fibromyalgia patients. Pain Manag. 2016, 6, 357–369. [Google Scholar] [CrossRef] [PubMed]
- Castel, A.; Fontova, R.; Montull, S.; Periñán, R.; Poveda, M.J.; Miralles, I.; Cascón-Pereira, R.; Hernández, P.; Aragonés, N.; Salvat, I.; et al. Efficacy of a multidisciplinary fibromyalgia treatment adapted for women with low educational levels: A randomized controlled trial. Arthritis Care Res. 2013, 65, 421–431. [Google Scholar] [CrossRef]
- Menzies, V. CE: Fibromyalgia Syndrome: Current Considerations in Symptom Management. Am. J. Nurs. 2016, 116, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Ellingson, L.; Stegner, A.; Schwabacher, I.; Koltyn, K.; Cook, D. Exercise Strengthens Central Nervous System Modulation of Pain in Fibromyalgia. Brain Sci. 2016, 6, 8. [Google Scholar] [CrossRef] [PubMed]
- Ambrose, K.R.; Golightly, Y.M. Physical exercise as non-pharmacological treatment of chronic pain: Why and when. Best Pract. Res. Clin. Rheumatol. 2015, 29, 120–130. [Google Scholar] [CrossRef] [PubMed]
- National Fibromyalgia Association. It’s a Guy Thing: Men with Fibromyalgia. 2017. Available online: https://www.fmaware.org/about-fibromyalgia/prevalence/men-fibro/its-a-guy-thing-men-with-fibromyalgia/ (accessed on 3 September 2023).
- Paulson, M.; Norberg, A.; Danielson, E. Men living with fibromyalgia-type pain: Experiences as patients in the Swedish health care system. J. Adv. Nurs. 2002, 40, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Bidonde, J.; Busch, A.J.; Schachter, C.L.; Webber, S.C.; Musselman, K.E.; Overend, T.J.; Góes, S.M.; Dal Bello-Haas, V.; Boden, C. Mixed exercise training for adults with fibromyalgia. Cochrane Database Syst. Rev. 2019, 5, CD013340. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Gallardo, I.C.; Carbonell-Baeza, A.; Segura-Jiménez, V.; Soriano-Maldonado, A.; Intemann, T.; Aparicio, V.A.; Estévez-López, F.; Camiletti-Moirón, D.; Herrador-Colmenero, M.; Ruiz, J.R.; et al. Physical fitness reference standards in fibromyalgia: The al-Ándalus project. Scand. J. Med. Sci. Sports 2017, 27, 1477–1488. [Google Scholar] [CrossRef] [PubMed]
- Heredia-Jimenez, J.M.; Soto-Hermoso, V.M. Kinematics gait disorder in men with fibromyalgia. Rheumatol. Int. 2014, 34, 63–65. [Google Scholar] [CrossRef] [PubMed]
- Hooten, W.M.; Townsend, C.O.; Decker, P.A. Gender Differences Among Patients with Fibromyalgia Undergoing Multidisciplinary Pain Rehabilitation. Pain Med. 2007, 8, 624–632. [Google Scholar] [CrossRef] [PubMed]
- WHO. Physical Activity Guidelines Advisory Committee Scientific Report; WHO: Washington, DC, USA, 2018. Available online: https://health.gov/sites/default/files/2019-09/PAG_Advisory_Committee_Report.pdf (accessed on 3 September 2023).
- American College of Sports Medicine. ACSM’s Health-Related Physical Fitness Assessment Manual, 4th ed.; Baltimore, Lippincott Williams & Wilkins: Baltimore, MD, USA, 2013; Available online: https://www.amazon.com/ACSM-Guidelines-Health-Related-Package/dp/1469832429 (accessed on 3 September 2023).
- American College of Rheumatology. Fibromyalgia. 2019. Available online: https://www.rheumatology.org/I-Am-A/Patient-Caregiver/Diseases-Conditions/Fibromyalgia (accessed on 3 September 2023).
- Brosseau, L.; Wells, G.A.; Tugwell, P.; Egan, M.; Wilson, K.G.; Dubouloz, C.J.; Casimiro, L.; Robinson, V.A.; McGowan, J.; Busch, A.; et al. Ottawa panel evidence-based clinical practice guidelines for aerobic fitness exercises in the management of fibromyalgia: Part 1. Phys. Ther. 2008, 88, 857–871. [Google Scholar] [CrossRef]
- Sanz-Baños, Y.; Pastor, M.Á.; Velasco, L.; López-Roig, S.; Peñacoba, C.; Lledo, A.; Rodríguez, C. To walk or not to walk: Insights from a qualitative description study with women suffering from fibromyalgia. Rheumatol. Int. 2016, 36, 1135–1143. [Google Scholar] [CrossRef]
- Sosa-Reina, M.D.; Nunez-Nagy, S.; Gallego-Izquierdo, T.; Pecos-Martín, D.; Monserrat, J.; Álvarez-Mon, M. Effectiveness of Therapeutic Exercise in Fibromyalgia Syndrome: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. BioMed Res. Int. 2017, 2017, 2356346. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Schmid, C.H.; Fielding, R.A.; Harvey, W.F.; Reid, K.F.; Price, L.L.; Driban, J.B.; Kalish, R.; Rones, R.; McAlindon, T. Effect of tai chi versus aerobic exercise for fibromyalgia: Comparative effectiveness randomized controlled trial. BMJ 2018, 360, k851. [Google Scholar] [CrossRef] [PubMed]
- Rivera Redondo, J.; Díaz Del Campo Fontecha, P.; Alegre de Miquel, C.; Almirall Bernabé, M.; Casanueva Fernández, B.; Castillo Ojeda, C.; Collado Cruz, A.; Montesó-Curto, P.; Palao Tarrero, Á.; Trillo Calvo, E.; et al. Recommendations by the Spanish Society of Rheumatology on Fibromyalgia. Reumatol. Clín. Engl. Ed. 2022, 18, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Rivera Redondo, J.; Díaz Del Campo Fontecha, P.; Alegre de Miquel, C.; Almirall Bernabé, M.; Casanueva Fernández, B.; Castillo Ojeda, C.; Collado Cruz, A.; Montesó-Curto, P.; Palao Tarrero, Á.; Trillo Calvo, E.; et al. Recomendaciones SER Sobre Fibromialgia (FM); Sociedad Española de Reumatologia: Madrid, Spain, 2022; Available online: https://www.ser.es/wp-content/uploads/2020/11/Recomendaciones_SER_FM_DEF.pdf/ (accessed on 3 September 2023).
- Carbonell-Baeza, A.; Romero, A.; Aparicio, V.A.; Tercedor, P.; Delgado-Fernández, M.; Ruiz, J.R. T’ai-Chi intervention in men with fibromyalgia: A multiple-patient case report. J. Altern. Complement. Med. 2011, 17, 187–189. [Google Scholar] [CrossRef] [PubMed]
- Karper, W.B. Exercise Effects on Two Men with Fibromyalgia Syndrome: An Update. Am. J. Mens Health 2013, 7, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Patton, M.Q. Qualitative Research and Evaluation Methods; SAGE Publications: Thousand Oaks, CA, USA, 2002. [Google Scholar]
- Crabtree, B.F.; Miller, W.L.; William, L. Doing Qualitative Research, 2nd ed.; SAGE Publications: London, UK, 1999. [Google Scholar]
- Powell, R.A.; Single, H.M. Focus Groups. Int. J. Qual. Health Care 1996, 8, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Medscape. Gender Identity. 2019. Available online: https://emedicine.medscape.com/article/917990-overview/ (accessed on 3 September 2023).
- Hsieh, H.F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Kondracki, N.L.; Wellman, N.S.; Amundson, D.R. Content analysis: Review of methods and their applications in nutrition education. J. Nutr. Educ. Behav. 2002, 34, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Montesó-Curto, P.; García-Martínez, M.; Gómez-Martínez, C.; Ferré-Alm, S.; Panisello-Chavarria, M.L.; Romaguera, S.; Mateu, M.L.; Cubí, M.T.; Sarrió, L.; Salvadó, T.; et al. Problems and solutions for patients with fibromyalgia: Building new helping relationships. J. Adv. Nurs. 2018, 74, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Llombart, M.P.L.; Carbó, P.A.; Mora, E. Scientific discourses on chronic pain without organic cause: Incorporating gender perspective for pain resignifyng-repoliticizing. Polit. Soc. 2015, 52, 921–948. Available online: https://portalrecerca.uab.cat/en/publications/scientific-discourses-on-chronic-pain-without-organic-cause-incor (accessed on 3 September 2023).
- Lincoln, Y.S.; Guba, E.G. Naturalistic Inquiry; SAGE Publications: Newbury Park, CA, USA, 1985. [Google Scholar]
- Gupta, A.; Scott, K.; Dukewich, M. Innovative Technology Using Virtual Reality in the Treatment of Pain: Does It Reduce Pain via Distraction, or Is There More to It? Pain Med. 2018, 9, 151–159. [Google Scholar] [CrossRef]
- Shahid, R.; Benedict, C.; Mishra, S.; Mulye, M.; Guo, R. Using iPads for distraction to reduce pain during immunizations. Clin. Pediatr. 2015, 54, 145–148. [Google Scholar] [CrossRef]
- Cunningham, J.L.; Evans, M.M.; King, S.M.; Gehin, J.M.; Loukianova, L.L. Opioid Tapering in Fibromyalgia Patients: Experience from an Interdisciplinary Pain Rehabilitation Program. Pain Med. 2016, 17, 1676–1685. [Google Scholar] [CrossRef] [PubMed]
- Dow, C.M.; Roche, P.A.; Ziebland, S. Talk of frustration in the narratives of people with chronic pain. Chronic Illn. 2012, 8, 176–191. [Google Scholar] [CrossRef] [PubMed]
- Sociedad Española de Medicina Familiar y Comunitaria (SemFYC). Documento de Consenso. La Atención al Paciente con Dolor Crónico no Farmacológico en Atención Primaria. 2018. Available online: https://www.semfyc.es/wp-content/uploads/2016/06/DOCUMENTO-CONSENSO-DOLOR-17-04-A.pdf (accessed on 3 September 2023).
- Fuster, D.; Muga, R. The opioid crisis. Med. Clin. 2018, 151, 487–488. [Google Scholar] [CrossRef] [PubMed]
- Fors, E.A.; Götestam, K.G. Patient education, guided imagery and pain related talk in fibromyalgia coping. Eur. J. Psychiat. 2000, 14, 233–240. Available online: https://search.pedro.org.au/search-results/record-detail/41172 (accessed on 3 September 2023).
- Johnson, B.; Ulberg, S.; Shivale, S.; Donaldson, J.; Milczarski, B.; Faraone, S.V. Fibromyalgia, autism, and opioid addiction as natural and induced disorders of the endogenous opioid hormonal system. Discov. Med. 2014, 18, 209–220. [Google Scholar] [PubMed]
- Ibáñez-Vera, A.J.; Alvero-Cruz, J.R.; García-Romero, J.C. Therapeutic physical exercise and supplements to treat fibromyalgia. Apunts. Med. L’esport 2018, 53, 33–41. [Google Scholar] [CrossRef]
- Poindexter, K.H.C. Nursing management of fibromyalgia syndrome. Med. Surg. Nurs. 2017, 26, 349–351. Available online: https://www.thefreelibrary.com/Nursing+Management+of+Fibromyalgia+Syndrome.-a0514512720 (accessed on 3 September 2023).
- Guest, G.; Namey, E.; Taylor, J.; Eley, N.; McKenna, K. Comparing focus groups and individual interviews: Findings from a randomized study. Int. J. Soc. Res. Methodol. 2019, 20, 693–708. Available online: https://www.tandfonline.com/doi/abs/10.1080/13645579.2017.1281601 (accessed on 3 September 2023). [CrossRef]
- Artundo, C. The Provision of Health Services in the European Union, a Space for the European Health System? 2005. Available online: https://www.elsevier.es/es-revista-revista-administracion-sanitaria-siglo-xxi-261-articulo-la-provision-servicios-sanitarios-union-13082042 (accessed on 3 September 2023).

{kind=link}
| Variable | United States (n = 7) | Spain (n = 10) |
|---|---|---|
| Civil status | ||
| Married | 6 (USP1, USP2, USP3, US P5, US P6, P7) | 5 (SP2, SP3, SP4, SP5, SP9) |
| Single | 1 (USP4) | 1 (SP7) |
| Divorced/Separated | 0 | 3 (SP1, SP6, SP8) |
| Widowed | 0 | 1 (SP10) |
| Education level | ||
| No high school | 0 | 1 (SP4) |
| High school | 3 (USP1, USP4, US P5, USP6) | 7 (SP1, SP2, SP5, SP6, SP7, SP9, SP10) |
| Four-year college | 2 (USP7) | 2 (SP3, SP8) |
| Graduate/Doctoral degree | 2 (USP2, USP3) | 0 |
| Occupational status | ||
| Active worker | 4 (USP1, USP2, USP3, USP7) | 0 |
| Unemployed | 1 (USP6) | 3 (SP1, SP5, SP7) |
| Active w/work disability | 0 | 2 (SP2, SP4) |
| Permanent disability | 2 (USP4, USP5) | 2 (SP8, SP9) |
| Retired/pensioner | 0 | 3 (SP3, SP6, SP10) |
| Number of people living in the home | ||
| One | 1 (USP4) | 2 (SP1, SP5) |
| Two to four | 6 (USP1, USP2, USP3, USP5, USP6, USP7) | 8 (SP2, SP3, SP4, SP6, SP7, SP8, SP9, SP10) |
| Notes the pain and fatigue decrease with exercise | ||
| Yes | 1 (USP5) | 0 |
| No | 6 (USP1, USP2, USP3, USP4, USP6, USP7) | 8 (SP2, SP3, SP4, SP5,S p7, SP8, SP9, SP10) |
| Depend (temperature water or exercise intensity) | 0 | 2 (SP1, SP6) |
| Types of exercise | ||
| Walking | 5 (USP1, USP2, USP3, USP4, USP7) | 7 (SP2, SP3, SP5, SP6, SP8, SP9, SP10) |
| Swimming | 0 | 2 (SP1, SP6) |
| Yard work | 4 (USP1, USP5, USP6, USP7) | 0 |
| Farm work | 1 (USP1) | 0 |
| Stretching | 2 (USP3, USP5) | 1 (SP7) |
| Elliptical | 1 (USP4) | 0 |
| Biking | 2 (USP3, USP4) | 0 |
| Shoveling | 1 (USP1) | 0 |
| Digging | 1 (USP1) | 0 |
| Stairs | 1 (USP5) | 1 (SP3) |
| Treadmill | 1 (USP3) | 0 |
| Manual labor | 2 (USP1, USP6) | 0 |
| Run | 0 | 0 |
| Pilates | 0 | 1 (SP7) |
| Aqua gym | 0 | 1 (SP6) |
| Who recommended physical exercise? | ||
| Rheumatologist | 1 (USP6) | 6 (SP1, SP2, SP3, SP6, SP8, SP9) |
| General Practitioner | 4 (USP1, USP4, USP5, USP6) | 3 (SP1, SP6, SP8) |
| Physiotherapist | 2 (USP1, USP4) | 4 (SP3, SP4, SP6, SP9) |
| Traumatologist | 0 | 1 (SP9) |
| Psychiatrist | 0 | 1 (SP9) |
| Psychologist | 0 | 1 (SP9) |
| Internal Medicine | 4 (USP1, USP2, USP3, USP7) | 0 |
| Participant | Name | Country | Age | Opiates |
|---|---|---|---|---|
| 1 | Daniel | Spain | 59 | Yes |
| 2 | Jack | Spain | 30 | Yes |
| 3 | Samuel | Spain | 46 | No |
| 4 | Alexander | Spain | 45 | Yes |
| 5 | Adam | Spain | 60 | Yes |
| 6 | James | Spain | 55 | Yes |
| 7 | Jordan | Spain | 35 | No |
| 8 | Jonathan | Spain | 55 | Yes |
| 9 | Julian | Spain | 50 | No |
| 10 | Victor | Spain | 53 | Yes |
| 1 | Stephen | US | 57 | No |
| 2 | Don | US | 51 | No |
| 3 | Andrew | US | 57 | No |
| 4 | Matthew | US | 50 | No |
| 5 | Oliver | US | 63 | No |
| 6 | Ryan | US | 60 | No |
| 7 | Henry | US | 53 | No |
| Themes | Categories | US Subcategories | Spain Subcategories |
|---|---|---|---|
| 1. Understanding what constitutes physical activity or exercise | Associate the meaning of the term physical activity as physical exercise (a sport or planned activity with the objective of improved health) | Cycling: ‘I ride a bicycle for 20 min; I take a couple of laps before and after’. (Andrew-P3, US) Stretches: ‘I do stretches… my own stretches. I learned it here (Mayo) in the program which I am going to implement’. (Oliver-P5, US) Treadmill: ‘I run on a treadmill for 20–25 min. It is a low-key exercise, so it does not intensify or contribute to more pain’. (Andrew-P3, US) Physical therapy work: ‘That was for a separate hip issue and that seemed to help quite a bit. I guess that is a potential resource for the future for sure’. (Don-P2, US) Walking: ‘I could walk for 2 h, I think. Only real strenuous activity where you’re sweating, and your heart rate is up that…I firmly believe that I need some exercise and although the Mayo Clinic told me I should walk for 10 min I believe I could do it for 2 h without any problem’. (Henry-P7, US) | Cycling: ‘I liked cycling a lot, but now with vertigo, I had to leave it’. (Julian-P9, S) Swimming: ‘I think swimming is the best but now I can’t do any exercise at all’. (Jack-P2, S) Walking: ‘In fact, I was recommended that before I get tired, I should calculate when I get fatigued, and before that I should stop. The problem is that I must stop every 15 min, but I try to force myself a little to improve and try to get to 20 min.’ (James-P6, S) |
| Associate the exercise with physical activity (daily life activities) | Take care of acreage: ‘I overdo physical exercise, try to do a little more, I push myself as much as I can. I must limit my activity to 30 min. Whatever physical things I do is whatever I do regarding taking care of our acreage. There is yard work, 15 or 20 pounds… I can do a little more than that, but I need to plan to get my legs under… it is a whole effort’. (Ryan-P6, US) Climb stairs: ‘I do not have an exercise program, but at home I have stairs… I am up and down those about 15 or 17 times a day’. (Oliver-P5 US) Walking: ‘I like to do walking and because I need to lose weight, but the more I do the more I hurt’. (Stephen-P1, US) | Walking: ‘I don’t practice exercise. I have tried to do it, but after 10 min of walking, I can’t do it anymore. But even if I do, of course, I live in the suburbs, I have 2 girls, I take them up and down, I take them up and down, I take care of them all day long. During the day I do not stop, this says (clock) that today I did 8 km more or less’. (Samuel-P3, S) | |
| 2. Facilitating or discouraging the performance of physical exercise | Recommendation of physical exercise by a specialist | Practitioner: ‘They (providers) have all done it or recommended it because of my weight’. (Steven-P1, US, and Mattew-P4, US) Rheumatologist: ‘The Dr. … did… the rheumatologist up there. I think my rheumatologist did too and my family internist back home… [they] recommended it and there was no implementation on what to do’. (Ryan-P6, US) ‘I think my rheumatologist did too and my family internist back home…’. (Oliver-P5, US) Internal Medicine: ‘What they were suggesting was that maybe you should try to walk for 10 min’. (Henry-P7, US) ’I have been recommended the exercise bike, and elliptical trainer by professionals of Internal Medicine and rheumatology. I have been visiting a chiropractor for many years’. (Don-P2, US) | Practitioner: ‘I went swimming because doctors recommended it to me for the FMS, but I do not know if I am a rare species…’. (Daniel-P1, S, and Mattew-P4, US) Rheumatologist: ‘I want to talk with the rheumatologist to see if he prescribes me a physiotherapist to see if he can fix these legs’. (Victor-P10, S) |
| Opiates affect exercise performance | Sleepiness: ‘I take the tramadol, it leaves me drowsy, and I can’t do any activity, but the next day I wake up normal and spend the day acceptable’. (James-P6, S) Limitation of the movement skills and speech: ‘I had to give up everything I was doing during all these years. I was a jumper coach, I had been in the high-performance center, I had been runner-up in Spain 2 times, third in Spain in jumps with pole-vaulting, then after 7 years without jumping, I was 3rd in Catalonia. With the medication I take, I can’t do any physical activity. At first, I was taking Palexia (tapentadol), but I was very nauseous, and they changed it to tramadol. They gave me tramadol intravenous in the hospital because the oral medication did nothing for me’. (Jack-P2, S) ‘I’ve gone to pick up the girls at a loss and could barely talk. I’ve been through 3 pain clinics, and I can assure you that there is nothing that takes away the pain. Morphine patches 100 mg. for 2 years and they don’t take away the pain. I eliminated them myself for 8 months by cutting off a tiny bit every day because otherwise I had to go to the hospital to take methadone and it didn’t make any sense’. (Samuel-P3, S) Addiction: ‘And I say yes, I am hooked on opiates. I tried to stop the medication, I told him everything and I gave up everything and I couldn’t, in 3 days I needed it and I had a withdrawal that I couldn’t with. And then, after all, you’re useless, you’re lying in bed because you’re too high to go out, to be able to talk to people… (Jonathan-P8, S) | ||
| 3. Effects of physical activity or exercise in symptom, psychological, and social aspects | Harmful effects | They get so tired doing activities of daily living: ‘I try to take 20 min into 45, then there is fatigue and brutal joint pain for the rest of the day and into the next day… More labor that I do the worse my cramps are. It hurts and when it hurts you stop’. (Ryan-P6, US). ‘This weekend I was running a chainsaw and sweating a ton and just trying to work normal…and I was working with a lawn mower for 1 h and then I was sick for two weeks’. (Henry-P7, US) Their overall strength is worse: ‘Not any improvement, usually it’s worse. ‘I force myself but usually it causes pain. During and afterward, but usually afterward’ (Mattew-P4, US). ‘My overall strength is probably down 60–70% from what it was a year ago’ (Oliver-P5, US and Ryan-P6, US) Fatigue and pain: ‘The more I do the more I hurt. Then you do not walk, and you do not do things because you are hurt. It is a big snowball effect. I could not do anything they wanted me to do (yoga). It was very hard, especially for the joints’ (Stephen-P1, US). ‘I do not think it helps with my level of fatigue. I still wake up tired’ (Andrew-P3, US). ‘Stretching is painful but it feels better after and then it comes back. I do that 5–10 times a day’ (Oliver-P5, US). ‘It actually makes the fatigue and pain worst’ (Don-P2, US) | They get so tired doing activities of daily living: ‘I park the car to take the kids to school and I’m already broken, I arrive at the car, and I feel my legs that I cannot take anymore’. (Samuel-P3, S) They get so tired doing small tasks: ‘After a shower, I need 15 min to recover from the effort that is involved’ (Jonathan-P8, S). ‘If I walk 100 m to take a coffee with a friend when I return home, I lie down in bed all day’ (Victor-P10, S). ‘You try to change a light bulb, you raise your arm and it hurts all day’ (Adam-P5, S) Their overall strength is worse: ‘I tried to do everything, but after 10 min walking, I cannot take it anymore’ (Samuel-P3, S) Fatigue and pain: ‘If I start peeling 4 potatoes, hair 2 and I have to wait to peel the other 2. ‘If you walk you have pain, but at 50 steps you have fatigue too’ (Samuel-P3, S). ‘There are moments you cannot breathe, there are times when you can walk a lot, others you cannot walk, the classic FMS pain…’ (Adam-P5, S). ‘I have the beard on purpose, so I do not have to shave myself, because it represents a great effort for me’ (James-P6, S). ‘After the minimum exercise I feel worse’ (Victor-P10, S) |
| Beneficial effects | Physically, they feel worse, but mentally better: ‘And I do get pain doing it, but the pain level doesn’t increase to a point where I can’t deal with it. The benefit is felt fresher afterward, my mind feels cleaner. That is why I continue to do it. It benefits me more cognitively’ (Andrew-P3, US). ‘The more physical labor that I do the worse my cramps are’ (Ryan-P6, US) Channel anxiety: ‘So, there was a fear of that at the time and the anxiety that I am stuck with this pain for the rest of my life. You know, what am I going to do? How am I going to deal with this stuff? …they give you exercise programs to relax your muscles, but they don’t really target fibromyalgia…If you teach them how to deal with the pain and you have some medication that can work, and you combine the two together then you can really help someone deal with it and to live a very positive lifestyle’ (Andrew-P3, US) Moderation of physical exercise is perceived as beneficial: ‘On a good day, you must watch yourself that you do not do too much with that good day. You must cut back on what you do otherwise… you pay for it 2 o 3 days down the road. ‘I realized that I had two options: to do nothing and stay at home complaining or, even if I felt tired and with pain, but living my life. A while ago, in the hospital we made a study about our heart rate and how long we could walk, for me it was a very strong rhythm, I tried to do 3 or 4 days. If I do 20 or 30 min, then I have to be resting triple’ (Ryan-P6, US). ‘You really have to taper it, moderation’ (Oliver-P5, US). ‘I go up and down steps, 15 to 17 times a day, then do my own stretching. I also do some yard work, shopping and driving the car. That’s all, I have no program’. ‘The more physical work I do, the worse my cramps become’ (Oliver-P5, US) | Physically, they feel worse, but mentally better: ‘I’m tired, but I feel better. Physically I’m worse, but mentally I’m better’ (Jonathan-P8, S). ‘One must force oneself to do something, so the mind becomes distracted’ (Samuel-P3, S). Channel anxiety: ‘Maybe swimming is what worked best to channel anxiety, but now I cannot channel it with anything’ (Jack-P2, S) Socialization: ‘The important thing is to get out of the house because I socialize, but if I walk more than 20 min, I find myself three times as tired. I have to stop every 15 min then; I try to force me’. If I leave home and I meet someone, I feel better, but then I’m sitting 2 days at home, and I do not do anything else’ (James-P6, S). ‘I have a 4-year-old dog and I leave the house 1 or 2 times a day when I am well. There are days when I can’t, but I admit that it helps me to get out of the house and to talk to some people I meet’ (Julian-P9, S) Moderation of physical exercise is perceived as beneficial: ‘In theory, you do not have to get tired, so you do not have to rest’ (James-P6, S) Distraction: ‘If you’re busy, you’re less focused on pain and you feel better’ (Alexander-P4, S) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montesó-Curto, P.; Toussaint, L.; Kueny, A.; Ruschak, I.; Lunn, S.; Rosselló, L.; Campoy, C.; Clark, S.; Luedtke, C.; Gonçalves, A.Q.; et al. Physical Activity and Exercise Experience in Spanish and US Men with Fibromyalgia: A Qualitative Cross-Cultural Study. Int. J. Environ. Res. Public Health 2023, 20, 6731. https://doi.org/10.3390/ijerph20186731
Montesó-Curto P, Toussaint L, Kueny A, Ruschak I, Lunn S, Rosselló L, Campoy C, Clark S, Luedtke C, Gonçalves AQ, et al. Physical Activity and Exercise Experience in Spanish and US Men with Fibromyalgia: A Qualitative Cross-Cultural Study. International Journal of Environmental Research and Public Health. 2023; 20(18):6731. https://doi.org/10.3390/ijerph20186731
Chicago/Turabian StyleMontesó-Curto, Pilar, Loren Toussaint, Angela Kueny, Ilga Ruschak, Shannon Lunn, Lluís Rosselló, Carme Campoy, Stephanie Clark, Connie Luedtke, Alessandra Queiroga Gonçalves, and et al. 2023. "Physical Activity and Exercise Experience in Spanish and US Men with Fibromyalgia: A Qualitative Cross-Cultural Study" International Journal of Environmental Research and Public Health 20, no. 18: 6731. https://doi.org/10.3390/ijerph20186731
APA StyleMontesó-Curto, P., Toussaint, L., Kueny, A., Ruschak, I., Lunn, S., Rosselló, L., Campoy, C., Clark, S., Luedtke, C., Gonçalves, A. Q., Martín, C. A., Vincent, A., & Mohabbat, A. B. (2023). Physical Activity and Exercise Experience in Spanish and US Men with Fibromyalgia: A Qualitative Cross-Cultural Study. International Journal of Environmental Research and Public Health, 20(18), 6731. https://doi.org/10.3390/ijerph20186731