Abstract
People with disability report social support facilitates participation in physical activity. A scoping review explored social support strategies used to facilitate exercise participation for people with disability (aged ≥ 15 years) in community gym settings. Seven electronic databases were searched. Studies were screened for eligibility based on title and abstract followed by full-text review. Data were analysed using content analysis and narrative synthesis. Forty-two articles reporting data from 35 studies were included. Eight types of social support were identified: supervision (n = 30), peer support (n = 21), specialist support (n = 19), orientation (n = 15), education (n = 7), logistical support (n = 6), motivational support (n = 5) and organised social activities (n = 4). Direct supervision was typically provided 1:1 or in small groups by staff experienced working with people with disability. Peer support typically involved support from exercise group participants or a peer mentor. Specialist support was usually provided by a health or exercise professional either directly to people with disability or to the people providing support to them (e.g., trainer). Orientation to the gym environment, equipment and exercise program was usually provided over 1 or 2 sessions. Gym staff may use these strategies to guide the implementation of social supports within their facilities to promote social connectedness and participation for people with disability.
Keywords:
physical activity; fitness; adolescents; young adults; supervision; recreation centre; peer support 1. Introduction
Participation in physical activity among adolescents and adults with disability is primarily influenced by environmental factors, particularly social support [1,2,3]. Social support relates to formal or informal understanding (emotional support), tangible assistance (instrumental support), advice (informational support) or feedback (appraisal support) [4] that contributes to the capability, opportunity and motivation of people with disability to be active [3]. Empirical studies consistently report the importance of social support as an enabler of physical activity in children, young people, and older adults with disability [1,2,5]. Social support is described as a positive influence on the beliefs, experiences and prioritisation of physical activity for people with disability, and to their sense of self [3]. Social support can be provided by anyone within a social network (e.g., family, friends, peers, staff, professionals, organisations, policymakers) however for many people with disability, social support to participate in physical activity across their lifespan is often lacking within community settings or provided primarily by their families [3].
Article 30 of the United Nations Convention on the Rights of Persons with Disabilities affirms the obligation to support the participation of young people with disability in recreational and sporting activities [6]. Facilitating participation in physical activity is a priority for adolescents and adults with disability. Most do not participate in the recommended amounts of activity [7] and many are unable to access physical recreation opportunities available within their communities. Access to community-based activities and facilities is particularly important during the transition from adolescence to young adulthood. This period coincides with a sharp decline in physical activity, reduced social participation, increased social isolation, heightened psychological vulnerability [8] and reduced access to support services [9,10]. Physical activity confers physical, mental and social health benefits and people with disability who are physically active report increased social interactions, feel socially connected and have a greater sense of independence and confidence [11]. Health behaviour change theories explain the relationship between social support and physical activity participation. Self-determination theory [12] and social cognitive theory [13] propose that health behaviours can be fostered through social interactions (‘relatedness’) and learning from others (‘modelling’), respectively. The availability of social support, together with positive social connectedness, and a suitable physical environment are essential to being physically active for people with disability [3].
Gyms are a preferred [14] and socially meaningful setting for physical activity for people with disability. A lack of social support acts as a barrier to participation in community gym settings [5], while having someone to exercise with is a key enabler [5,15]. Research shows gyms can be an intimidating space for people with disability, who describe fears of ‘standing out’, self-consciousness and ‘not-belonging’ [15,16]. Having social support in the gym can facilitate participation via provision of emotional support (e.g., enable a sense of belonging [17,18]), instrumental support (e.g., assistance navigating basic exercises, using equipment or staying focused [5]) and informational support and appraisal (e.g., education on healthy lifestyle choices and motivational feedback). There are many ways in which community gym and recreation facilities could implement social support to facilitate attendance and positive physical activity experiences. The aim of this study was to describe how social support has been implemented for people with disabilities in research studies conducted in community gyms.
2. Methods
2.1. Protocol and Registration
A scoping review was completed in accordance with recommendations from the Joanna Briggs Institute [19] and reported according to the PRISMA Extension for Scoping Reviews (PRISMA-ScR) checklist (Appendix A) [20]. Scoping reviews provide an overview of the evidence, systematically mapping the available literature on a topic [21] and examining the extent (size), range (variety) and nature (characteristics) of the evidence [20]. They also enable a broad examination of available evidence to identify knowledge gaps, to clarify key concepts related to the area of interest and to report the types of evidence that may inform health practice and practice change [22]. A review protocol was published prospectively on the Open Science Framework [22].
2.2. Eligibility Criteria
Reports of primary studies (any design) of physical activity interventions were included if they were completed in a community gym or recreation centre and used social support strategies, either alone or as an adjunct, to facilitate the participation for adolescents and adults (aged ≥15 years) with disability. For the purposes of the review, disability included childhood-onset disabilities (for example, cerebral palsy or Down syndrome), disabilities occurring in childhood or adulthood (for example, stroke or acquired or traumatic brain injury) and adult-onset conditions (for example, multiple sclerosis or Parkinson’s disease). Disabilities due to primary musculoskeletal disorders (for example, low back pain or osteoarthritis), pain and fatigue disorders, fragility, ageing (including dementia) and acute psychiatric conditions were excluded. Only full text, peer-reviewed, English-language articles were included. Systematic or narrative reviews, protocol papers, conference abstracts and theses were excluded.
A community gym or recreation centre was defined as a publicly owned and funded facility operated by either a local (municipal) government authority or by a management company on that authority’s behalf. Physical activity interventions needed to have been completed in a gym setting open to the public (including those operating on university or college campuses) that included exercise equipment (for example, stationary bikes or pin-loaded weights machines) with or without a functional exercise space. Programs that took place in a group exercise space (for example, a yoga studio) that was segregated from other public users of the gym or in a research laboratory were excluded.
2.3. Search Strategy
A systematic search (Appendix B) was completed of the following databases: CINAHL, Medline, EMBASE, PsychINFO, SPORTDiscus, PubMed (last 12 months only) and PEDro. The search strategy included keywords and MeSH headings related to the concepts of ‘disability’, ‘physical activity’ and ‘community gym’. Database searches were supplemented by citation tracking using Google Scholar and by reviewing the reference lists of included studies.
2.4. Selection of Sources of Evidence
Search yields were imported into Endnote (version 20), duplicates deleted and then exported to Covidence. Titles and abstracts were assessed against the eligibility criteria by two reviewers (RK and NS), independently. Where eligibility could not be determined from the title and abstract alone, the full text of an article was retrieved and examined before a final decision on eligibility was made. Full text articles were examined by two reviewers (RK and CH or GMc) and any disagreements were resolved by consensus. The authors of full text articles were contacted via email to clarify details about their studies, where necessary.
2.5. Data Charting Process and Data Items
Data from included articles were extracted using a data extraction sheet developed for the review in Microsoft Excel. Data were extracted by one reviewer (RK) and checked by a second reviewer (NS). Any disagreements were resolved by consensus. The following data were extracted: bibliographic information (author(s), year of publication, title, country of origin), study aim, study characteristics (sample size, participant demographics, recruitment setting, study design and/or methods), details of the physical activity intervention (including duration, setting, frequency), description of the social support strategy(ies) (including what support, the purpose, who provided, training received, and how implemented). Clinical outcomes from the included studies were not reported as social support is usually implemented as part of a complex intervention making it difficult to conclude that specific outcomes resulted from social support initiatives alone. Study quality was not formally appraised as the aim of the review was to describe how social support had been implemented.
2.6. Data Synthesis
Descriptive statistics summarised the characteristics of the included studies. Content analysis including the types and sub-types of social supports and narrative synthesis were completed to describe how social support had been implemented in community gyms. Data were managed in Microsoft Excel. First, each paper was systematically coded to identify the social support strategies implemented. Social support strategies were then grouped into themes based on similarity of purpose. Descriptive labels summarising the purpose of the supports were applied to each theme and categorised according to Berkman [4]. Lastly, each social support was mapped to the socio-ecological model. At least two authors conferred on each stage and cross-checked theme groupings and categorisation.
3. Results
The search strategy identified 1517 articles for screening, with 111 articles undergoing full text review. Forty-two articles reporting data from 35 studies published between January 2004 and July 2022 were included (Figure 1).
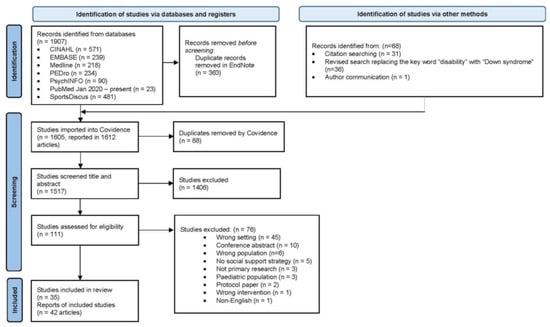
Figure 1.
PRISMA flowchart of study selection.
3.1. Characteristics of Included Studies
The studies included various congenital (for example, Down syndrome and cerebral palsy) and adult-onset disabilities (for example, multiple sclerosis and Parkinson disease) with between 3 and 163 participants of mean age from 15 and 70 years (Table 1). Studies included randomised controlled trials (n = 21) [14,17,18,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40]; pre-test post-test studies (n = 9) [41,42,43,44,45,46,47,48,49] three of which included qualitative sub-studies [15,50,51]; feasibility studies (n = 2) [52,53], a case report [54], an observational study [55] and a single-subject design [56]. Studies were conducted in developed countries, with one exception [48] (Table 1). The physical activity interventions implemented included strength, aerobic or balance training, or a combination of these (Table 2). The duration of the interventions was 3 weeks to 24 months, with most programs running for 10 to 12 weeks.

Table 1.
Characteristics of included studies grouped according to whether participants were adolescents and young adults (15–30 years) or adults (30+ years).
Table 2.
Summary of physical activity interventions, intervention duration and social support strategies.
3.2. Social Support Strategies
Social supports used in the included studies were grouped into categories according to Berkman et al. [4] (Appendix C).
3.2.1. Supervision
Direct supervision was support provided for the duration of each exercise session, usually for the purpose of providing instrumental, informational and appraisal support, and in some instances emotional support. Supervision was provided in 30 of the 35 included studies, usually by gym staff or by allied health professionals (for example, physiotherapists) however in five studies, supervision was provided by volunteers [38,44,49,54] or paid support workers [45] (Supplementary file Table S1). The supervisor to participant ratio was typically high; either 1:1 or small groups (i.e., ratio of 1:2, 1:3 or 1:4) although larger groups of 10 to 12 participants per session did occur [41,42]. Direct supervision was usually provided for the duration of the intervention, except in one study [52] where it was provided during the first exercise session only, after which participants with glioma exercised in the gym unsupervised (A. Hansen, personal communication, 10 May 2022).
Typically, direct supervision was provided by staff experienced in working with people with disability or by staff or students who had received training. Examples of the type of training completed by those providing supervision were 2- or 3 h formal education sessions [41,44,49,55,57], receipt of a training manual [14,32], attending sessions with a physiotherapist or exercise specialist [24,26,30,48,54] or a combination of these [27,37,40,56]. The content of formal training sessions included information about disability, communication strategies, managing challenging behaviour, social interaction strategies, exercise prescription and progression, motivational techniques and providing feedback.
3.2.2. Peer Support
Peer support was included in 21 of 35 studies (Table 2) and was primarily providing emotional and instrumental support. This type of support was provided by disabled peers in supervised group settings, or by non-disabled peers (mentors, usually volunteer or paid university students) who provided 1:1 support (Supplementary file Table S2). Group exercise programs used three formats: small groups of 2 to 4 participants [31,33,35,36,45,47,51,55,57,58], large groups of 10 to 15 participants [29,38,39,44,49] or a large group divided into smaller sub-groups (for example, 12 participants exercising in smaller groups of 3 or 4) [25]. During group exercise, participants either completed an individually tailored program alongside other participants [41] or participants with a similar level of independence exercised together [42].
One-to-one peer support was provided by a university student in seven studies [17,18,29,34,44,53,54]. In four of these seven studies [17,18,34,53], student mentors exercised alongside the participant with disability, unless the participant had a complex disability (usually a young person with a significant intellectual disability and/or communication impairment and/or epilepsy) [34]. In one study, participants were assigned a volunteer (university student) exercise partner during the transition (over 5 to 9 weeks) from supervised exercise in a small group area to independent exercise in the main gym [44]. Peer support was provided by high school students in two studies, who exercised in pairs (1:1) or triads (1:2) with participants with disability, as part of a larger supervised exercise program [55,57]. The roles and responsibilities of mentors included counting repetitions, motivating and providing feedback, maintaining exercise logbooks, problem solving and adapting exercises and equipment in consultation with specialists such as a physiotherapist, assisting to get on/off equipment and ensuring safe technique and equipment use.
3.2.3. Specialist Support
Specialist support was usually provided by a health professional (for example, a physiotherapist) or an exercise professional (for example, an exercise physiologist) (Supplementary file Table S3) and covered all four domains of support, that is, emotional, instrumental, appraisal and informational support. Specialist support was provided to participants with disability [23,28,29,52] or to people who provided peer support or supervision (for example fitness trainers and student mentors) [14,17,18,27,31,53,56,59] or both [26,34,37,41,44,48,60]. The type of specialist support provided included in-person gym visits [23,26,31,34,37,41,48,56,59,60], 2 to 3 h training sessions for gym staff or student mentors [14,17,18,26,27,34,41,53,56,59,60] and remote support via telephone, email or an online exercise App [14,18,23,32,34,37,49,52]. In-person visits included orientation sessions or providing gym staff and student mentors with specialist advice on motivational and behavioural management strategies [17,18,34,37,53] or adapting equipment and exercises [34,44] for participants with disability. The amount of specialist support varied and included regular scheduled support or support provided only as required [14,17,18,23,34,52,53,60]. For example, in one study, for a subset of participants with complex disability, a physiotherapist attended their first gym session and provided weekly remote monitoring thereafter for the duration of the program [34].
3.2.4. Orientation and Familiarisation Sessions
Orientation sessions for the person with disability was included in 15 of 35 studies (Supplementary file Table S4) to provide informational support. Typically, this comprised one or two sessions although up to 15 sessions [56] were reported. The intention of orientation was to familiarise the person with disability to the gym environment and to gym equipment, to ensure safety, and to make any necessary adaptations to the exercise program. Participants completed these sessions with a physiotherapist (n = 4) [26,41,43,48] or gym instructor (n = 6) [23,27,34,45,47,52], both a physiotherapist and a gym instructor (n = 1) [51] or a member of the research team (n = 4) [49,54,56,59].
3.2.5. Other Social Support Strategies
Additional types of social supports reported less commonly were ‘education’, ‘organised social activities’, ‘motivational strategies’, and ‘logistical support’.
Formal education provided informational support and was delivered to participants with disability in seven studies by staff with expertise in exercise, disability, nutrition and/or health education [26,28,29,30,49,56,59] (Supplementary file Table S5). Education was delivered using written materials, video assisted schedules delivered via electronic tablet, workshops, 1:1 consultation with participants and in-person during exercise sessions. Education included information about initiating and maintaining safe exercise and physical activity participation in the gym and healthy lifestyle choices.
Motivational strategies encompassed appraisal and emotional support and included goal setting [14,59], motivational interviewing [30], “checking in” if exercise sessions were missed [24], the use of a web-based application with the capacity to share via social media [30,61] and support from coaches of an external organisation (Special Olympics) [29].
Organised social activities were used to provide emotional support and were included in four studies of adult participants only [25,46,49,50]. These activities included socialising with other participants from the program following exercise sessions for light refreshments [25,46,50]. One study [49] provided opportunities for participants to meet at a local park for recreational sports and at a restaurant for meals during the study.
Transport to and from the gym was the most common type of logistical support provided and included instrumental and practical supports such as transport by shuttle bus, taxi or organised transport by ancillary programs attended by participants (for example, day programs) [33,35,38,54,60]. In one study, gym staff met participants in the car park to assist them into the facility [60].
3.3. Mapping Social Supports to the Socio-Ecological Model
These eight strategies map to the interpersonal and organisational levels of the socioecological model, respectively and allow an understanding of the complex interplay and range of social support strategies that young people with disability often need to successfully participate in physical activity within the gym setting (Figure 2). The identified initiatives comprise formal structured supports providing tangible instrumental assistance (supervision, peer support, specialist support and logistical support), emotional understanding (supervision, peer support, specialist support, motivational, organised socialisation), appraisal and decision making (supervision, peer support, specialist support, motivational) and informational support (supervision, specialist support, orientation, education). There were also examples of informal and unstructured supports that are less quantifiable but equally important, for example, the support offered by peers in a group exercise class. A shared element of these supports was people; the three most common social supports were person-based, that is, supervision, peer support and specialist support.
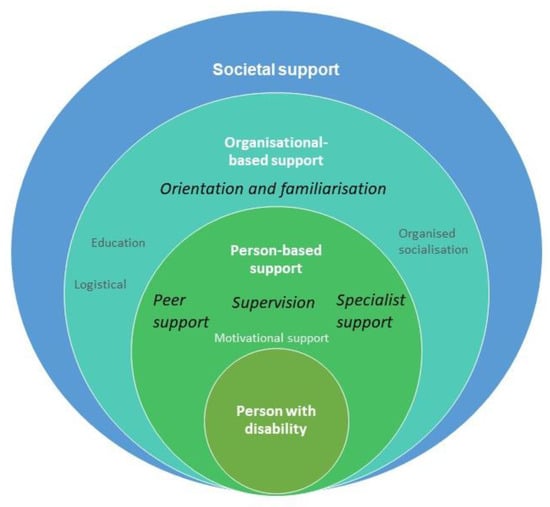
Figure 2.
Mapping social supports to the socio-ecological model. The most common person- and organisational-based supports are highlighted in italics.
4. Discussion
Of the eight identified social supports that have been used in research to facilitate exercise, person-based support appears fundamental to successful implementation and integration of people with disability in community gym settings. The person-based social supports reported most often involved direct supervision, usually by someone with disability experience, for example a gym staff member or health professional (most often a physiotherapist), working either 1:1 or in small groups. This is consistent with qualitative studies where participants with disability reported that supervision from a knowledgeable supervisor or mentor was important to them [34,37,39,41,44,48,50,51,52,53].
One-to-one support is resource intensive and differs from the common practice in gym settings of indirect supervision where a gym trainer oversees all members exercising in the gym space. The provision of social support can facilitate participation in gym settings, but it is important to consider how such support can be implemented outside of funded trials. Disability funding initiatives, such as the National Disability Insurance Scheme (NDIS) in Australia [62], may cover the costs of 1:1 support in the gym, from a support worker, personal trainer or specialist (e.g., physiotherapist or exercise physiologist). Collaboration between gym facilities, local government, funding bodies (e.g., NDIS) and available supports (e.g., specialists and carers) provide an opportunity to maximise the resources and skills of each sector to facilitate the participation of people with disability in community gym settings.
People with disability describe feeling more confident exercising with a support person when that support person has received training and understands disability and their individual needs [34]. Disability specific knowledge and skills of staff are often identified as important factors in facilitating (or not) the participation for people with disability in community gym settings. In this review, when the person providing supervision did not have disability experience, they were often provided with training about disability and supported by a specialist when adapting exercises and equipment or both. The provision of specialist support, either directly to a person with disability or indirectly via support to gym staff is therefore an important consideration for implementation of community-based physical activity programs. Provision of specialist support can bridge the gap between a rehabilitation “therapy-model” of exercise to a community-based physical activity participation model and simultaneously support the upskilling of gym staff. While specialist support within the included studies was most often provided in person, it could also be provided remotely when the infrastructure, organisation-based support and funding is in place to provide it. Providing remote specialist support facilitates access for people with disability living in regional and rural areas where specialist support might not be as readily available.
Peer support, provided by people with and without disability, was usually an adjunct to specialist support and was important to those with disability [34,39,47,50,51,53]. When a non-disabled peer exercised alongside a person with disability, their role was of a peer mentor or exercise partner rather than as an exercise instructor [17,34,53,55,57]. The non-disabled peer mentor model fostered social connection, particularly for adolescents and young adults with disability who appreciated the time taken to build rapport, making exercise more fun and being accountable to an exercise partner [15]. Peer support instils confidence in people with disability to exercise in a community gym setting, ensuring safety and as a source of social connectedness, accountability, and encouragement [3,15]. Similarly, the inclusion of caregivers and partners, usually a spouse, in group programs for older adults provided motivation to “stick” with the program [41]. Skilled strategies (such as motivational interviewing [30] and goal setting [30,40]) and practical motivational strategies (such as checking-in with participants who missed sessions [24]) were also implemented to facilitate adherence and sustained participation in the gym setting. Within the included studies, peer support was primarily facilitated by the research teams. Further implementation research is needed within gym settings to better understand how facilities might support person-based one-to-one social support initiatives as an alternative to standard gym practice.
Orientation and familiarisation were widely utilised in the included studies and mirrors standard practice, making this an appealing strategy for gym facilities given infrastructure is likely to already exist to support implementation. However, it is important the content and delivery of orientation sessions are tailored to the needs of people with disability, including how to exercise with good form, using equipment safely and with correct technique and injury prevention. It is also important to recognise a single orientation session may not be sufficient for a person with disability. In the studies included in this review, between 2 and 15 orientation sessions were implemented [56]. People with disability, particularly those with intellectual disability may need additional support so that information might be repeated, reinforced and possibly delivered in alternative formats at subsequent gym sessions. Other organisational level strategies targeted exercise participation indirectly through education, logistical support and facilitating group cohesion via organised social activities. The latter was only reported in studies involving older adults.
Although resource-intensive, person-based supports appear important in facilitating participation among people with disability in community gyms settings. All the included studies were funded research trials that provided the organisational framework and covered most, if not all, the costs of implementation including salaries, workforce training, educational resources and technology. Outside of research trials, it is unclear how the identified social supports would be implemented sustainably by gym facilities, and how the cost of social supports would be funded. Disability funding initiatives, such as the NDIS in Australia, often pay for some of the costs of community participation, such as the cost of specialists and support staff. However, the cost of entry fees or gym membership is often not covered. In some instances, philanthropic and not-for-profit organisations offer reduced, low or no-cost membership options for disadvantaged groups, including people with disability. These programs, designed to bridge the equity gap and enable access and inclusion for all to gym and recreation facilities are not, however, widespread across the industry. Cost is a known barrier to exercise participation for most people with disability [1], who are often unemployed, under-employed or in low-paying jobs. Given the physical, mental and social connection benefits of physical activity participation for people with disability [63,64], there is a need for economic evaluation from a societal perspective of social support initiatives within gym and recreation facilities to inform policy.
The social supports identified in this review primarily map within the socio-ecological model to person-based supports and organisational-based support for the individual with disability and their close social networks (Figure 2). However, no studies included in this review considered the potential impact of wider organisational, physical and social environmental or policy contexts that could facilitate or hinder the implementation of social support strategies within community gym settings. Local champions may drive practice in the provision of social support for people with disability within individual community facilities. However, the support of decision-makers within recreation organisations and the local government ultimately influences the implementation of inclusive policies and importantly, funding to support these policies. The findings of this review provide a basis for how recreation gym facilities could implement social support to increase participation among people with disability. It also provides exemplars of strategies or programs that could be supported by local government policy and funding.
A strength of this review is its size. Data from 35 exercise trials (reported in 42 articles) involving adolescents and adults with congenital, acquired and progressive disabilities, were synthesised, and eight types of social support strategies were illustrated. These strategies, applied in various forms, have been used by research programs to successfully facilitate the physical activity participation of people with disability in community gym settings. These strategies provide an ‘ideas bank’ that can be used by organisations to guide implementation within their gym facilities to promote social connection and participation of people with disability. There are limitations in this review relating to the facilities, settings and infrastructure to which the findings primarily relate (community gyms). The types of facilities in this review are more likely to be available in developed countries and may be governed by different policies and funding sources compared with privately owned gyms. Local government facilities usually exist to provide access to recreation for the whole community, including those with disability, and therefore implementing social support within these settings would align with health and inclusion policies. This scoping review is the first of a three-phase project investigating how social supports are implemented in current practice in community gyms and the perspectives and lived experience of this type of support among young adults with disability who attend community gyms [22]. The principles underpinning many of the social support strategies identified in this review may also have applications beyond community gym settings.
5. Conclusions
This review identified eight social support initiatives that can be implemented in community gym settings to facilitate the participation of people with disability in physical activity and promote social connections within their community more broadly, as part of their everyday lives, like their peers without disabilities [65]. Supervision, peer support, specialist support and orientation were the most utilised strategies. Collaboration and partnerships between researchers, rehabilitation specialists (e.g., physiotherapists), recreational organisations (e.g., gym staff and management) and government and insurance policymakers are important to better understand how these initiatives might be implemented and operationalised in practice. Transitioning exercise from a medical rehabilitation model to a community-based participation model is important in providing access to and facilitating safe, individually tailored physical activity for young people with disability.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ijerph20010699/s1, Table S1: Social support strategies in community gyms—Supervision; Table S2: Social support strategies in community gyms—Peer support; Table S3: Specialist supervision as a social support strategy in community gyms; Table S4: Orientation or familiarisation as a social support strategy in community gyms; Table S5: Education, organised social activities, technology, logistical, motivational supports used in community gyms.
Author Contributions
Conceptualization, N.S.; methodology, N.S. and R.A.K.; formal analysis, R.A.K., N.S., G.M. and C.H.; resources, N.S.; data curation, R.A.K., N.S., G.M. and C.H.; writing—original draft preparation, R.A.K.; writing—review and editing, R.A.K., N.S., G.M. and C.H.; visualization, R.A.K.; supervision, N.S.; project administration, R.A.K.; funding acquisition, N.S. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by funding received from VicHealth, through its Impact Research Grants initiative (2021). Representatives of VicHealth sit on the GYM-SPARC project’s Steering Committee and had no role in this scoping review.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Human Ethics Committee of La Trobe Univeristy (HEC21376, 30 November 2021).
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data was created.
Acknowledgments
We thank Natalie Pearce for her assistance in developing the database search strategy. We thank and acknowledge the GYM-SPARC (Getting Young adults Moving by Supporting Participation and Access to Recreation Centres) Disability Advisory Committee, for their insights and feedback on their lived experience of social support strategies within a gym setting. We also acknowledge and thank our research partners: Sport and Recreation Victoria; VICSPORT; Disability Sport and Recreation; Cerebral Palsy Support Network; Down Syndrome Victoria; CP-Achieve; YMCA Victoria; Belgravia Leisure; City of Boroondara; City of Monash.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Table A1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) Checklist [20].
Table A1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) Checklist [20].
| Section | Item | PRISMA-ScR Checklist Item | Reported on Page # |
|---|---|---|---|
| Title | |||
| Title | 1 | Identify the report as a scoping review. | Page 1 |
| Abstract | |||
| Structured summary | 2 | Provide a structured summary that includes (as applicable): background, objectives, eligibility criteria, sources of evidence, charting methods, results, and conclusions that relate to the review questions and objectives. | Page 1 |
| Introduction | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. Explain why the review questions/objectives lend themselves to a scoping review approach. | Pages 1–2 |
| Objectives | 4 | Provide an explicit statement of the questions and objectives being addressed with reference to their key elements (e.g., population or participants, concepts, and context) or other relevant key elements used to conceptualize the review questions and/or objectives. | Page 2 |
| Methods | |||
| Protocol and registration | 5 | Indicate whether a review protocol exists; state if and where it can be accessed (e.g., a Web address); and if available, provide registration information, including the registration number. | Page 2 |
| Eligibility criteria | 6 | Specify characteristics of the sources of evidence used as eligibility criteria (e.g., years considered, language, and publication status), and provide a rationale. | Pages 2–3 |
| Information sources * | 7 | Describe all information sources in the search (e.g., databases with dates of coverage and contact with authors to identify additional sources), as well as the date the most recent search was executed. | Pages 3 |
| Search | 8 | Present the full electronic search strategy for at least 1 database, including any limits used, such that it could be repeated. | Appendix B |
| Selection of sources of evidence † | 9 | State the process for selecting sources of evidence (i.e., screening and eligibility) included in the scoping review. | Pages 3 and Figure 1 |
| Data charting process ‡ | 10 | Describe the methods of charting data from the included sources of evidence (e.g., calibrated forms or forms that have been tested by the team before their use, and whether data charting was done independently or in duplicate) and any processes for obtaining and confirming data from investigators. | Page 3 |
| Data items | 11 | List and define all variables for which data were sought and any assumptions and simplifications made. | Page 3, Appendix C |
| Critical appraisal of individual sources of evidence § | 12 | If done, provide a rationale for conducting a critical appraisal of included sources of evidence; describe the methods used and how this information was used in any data synthesis (if appropriate). | N/A |
| Synthesis of results | 13 | Describe the methods of handling and summarizing the data that were charted. | Page 3–4 |
| Results | |||
| Selection of sources of evidence | 14 | Give numbers of sources of evidence screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally using a flow diagram. | Page 3 and Figure 1 |
| Characteristics of sources of evidence | 15 | For each source of evidence, present characteristics for which data were charted and provide the citations. | Page 4 and Table 1 |
| Critical appraisal within sources of evidence | 16 | If done, present data on critical appraisal of included sources of evidence (see item 12). | N/A |
| Results of individual sources of evidence | 17 | For each included source of evidence, present the relevant data that were charted that relate to the review questions and objectives. | Pages 6–9 and Table 2 and Tables S1–S5 |
| Synthesis of results | 18 | Summarize and/or present the charting results as they relate to the review questions and objectives. | Pages 6–9 and Table 2 and Tables S1–S5, Figure 2 |
| Discussion | |||
| Summary of evidence | 19 | Summarize the main results (including an overview of concepts, themes, and types of evidence available), link to the review questions and objectives, and consider the relevance to key groups. | Pages 9–11 |
| Limitations | 20 | Discuss the limitations of the scoping review process. | Page 11 |
| Conclusions | 21 | Provide a general interpretation of the results with respect to the review questions and objectives, as well as potential implications and/or next steps. | Page 11 |
| Funding | |||
| Funding | 22 | Describe sources of funding for the included sources of evidence, as well as sources of funding for the scoping review. Describe the role of the funders of the scoping review. | Page 12 |
JBI = Joanna Briggs Institute; PRISMA-ScR = Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews. * Where sources of evidence are compiled from, such as bibliographic databases, social media platforms, and Web sites. † A more inclusive/heterogeneous term used to account for the different types of evidence or data sources (e.g., quantitative and/or qualitative research, expert opinion, and policy documents) that may be eligible in a scoping review as opposed to only studies. This is not to be confused with information sources. ‡ The frameworks of processing data extraction in a scoping review are referred to as data charting. § The process of systematically examining research evidence to assess its validity, results, and relevance before using it to inform a decision. This term is used for items 12 and 19 instead of “risk of bias” (which is more applicable to systematic reviews of interventions) to include and acknowledge the various sources of evidence that may be used in a scoping review (e.g., quantitative and/or qualitative research, expert opinion, and policy documents).
Appendix B
Table A2.
Search Strategy and Example Medline Search Results.
Table A2.
Search Strategy and Example Medline Search Results.
| Research Question | ||
|---|---|---|
| Identify how social support has been provided to facilitate physical activity participation in community gym settings for adults with disability | ||
| Key Terms | ||
| Concept 1 | Concept 2 | Concept 3 |
|
|
|
| Inclusion Criteria | Exclusion Criteria | |
| ||
| Other Information | ||
Gym context important. Community gyms–focused
| ||
| Databases | ||
| ||
| Medline Search Example | ||
| # | Searches | Results |
| 1 | disabilit*.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 305,217 |
| 2 | intellectual disabilit*.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 67,883 |
| 3 | learning disabilit*.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 18,728 |
| 4 | developmental disabilit*.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 24,887 |
| 5 | physical disabilit*.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 7120 |
| 6 | Intellectual Disability/ | 56,819 |
| 7 | Learning Disabilities/ | 14,401 |
| 8 | Developmental Disabilities/ | 21,310 |
| 9 | 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 | 305,217 |
| 10 | physical activit*.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 129,700 |
| 11 | participation.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 202,081 |
| 12 | exercise.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 383,902 |
| 13 | mobility.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 180,517 |
| 14 | physical training.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 6191 |
| 15 | movement.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 445,888 |
| 16 | motor skills.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 32,232 |
| 17 | balance.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 278,798 |
| 18 | strength.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 358,126 |
| 19 | fitness.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 100,805 |
| 20 | resistance.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 959,784 |
| 21 | training.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 499,173 |
| 22 | physical fitness.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 33,548 |
| 23 | Exercise/ | 123,719 |
| 24 | 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 | 3,102,649 |
| 25 | community gym.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 5 |
| 26 | community gymnasium.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 11 |
| 27 | gym.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 1390 |
| 28 | gymnasium.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 435 |
| 29 | health facility.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 28,258 |
| 30 | wellness center.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 172 |
| 31 | fitness center.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 247 |
| 32 | health club.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 135 |
| 33 | Fitness Centers/ | 618 |
| 34 | YMCA.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 284 |
| 35 | 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 | 31,311 |
| 37 | 9 and 24 and 35 | 183 |
* Truncated search term.
Appendix C. Social Support Strategies: Types and Definitions
Social support. Support given by trusted people who provide understanding, practical help, advice or assistance to make decisions [4].
Supervision. Supervision is providing support to young people with disability to exercise in the gym but not exercising alongside that person. Supervision can be 1:1 or in a group. It can be provided by paid people, such as gym trainers and support workers, or by unpaid peoples, such as family or friends.
Peer support. Peer support involves attending the gym and exercising alongside another person. This could be someone that is known, or it could be someone that the young person with disability is paired up with as part of a program. Like supervision, peer support can be provided by paid people, such as gym trainers and support workers, or by unpaid people, such as family or friends or a volunteer. It could also be another young person with disability.
Specialist support. Is support provided by specialists in either exercise, for example an exercise physiologist or a healthcare professional, for example a physiotherapist. This support could be provided by working directly with the young person with disability, or support might be provided to the person who is supporting the young person with disability, for example the gym trainer or peer support person. Specialist support may include training in exercise, disability, behavioural management, motivation techniques and adapting exercise and equipment to the person with disability.
Orientation. This involves orientation and familiarisation to the gym space, exercises and exercise equipment. This could be provided by gym staff or health care team. It may happen on more than one occasion after starting at the gym.
Education. Formal or informal provision of information about exercise benefits and improving the health and exercise knowledge of young people with disability. This can be provided informally, through conversation, visual guides and posters; or formally through education sessions in person, online or through web-based apps.
Logistical support. Are supports to assist the young person with disability to access the facility and gym environment. It can include transport to the gym, information on a website and within the facility about disability access or allowing support person to enter the gym for free, for example recognising a companion card (a Victorian State Government initiative for people with significant disability who have a lifelong need for a high level of support to participate in community events and activities. The card allows a person’s carer free entry into participating venues and events.).
Motivation. Includes any strategies that are designed to motivate or encourage young people with disability to exercise in the gym. It may be individual, such as goal setting and documenting progress in the gym, for example via a paper program or web-based program app. Alternatively it could be checking in with the young person with disability periodically and problem solving any barriers to participation in the gym. It can also be more general, for instance an achievements/personal best/milestone board or video highlighting personal achievements that is on display in the gym.
Organised social activities Dedicated time and space for socialisation related to gym exercise, usually before or after a session. For example, this might include a snack or drink in the café after a class, or a free breakfast provided by the gym for members.
References
- Shields, N.; Synnot, A. Perceived barriers and facilitators to participation in physical activity for children with disability: A qualitative study. BMC Pediatr. 2016, 16, 9. [Google Scholar] [CrossRef] [PubMed]
- Shields, N.; Synnot, A.J.; Barr, M. Perceived barriers and facilitators to physical activity for children with disability: A systematic review. Br. J. Sport. Med. 2012, 46, 989–997. [Google Scholar] [CrossRef]
- McKenzie, G.; Willis, C.; Shields, N. Barriers and facilitators of physical activity participation for young people and adults with childhood-onset physical disability: A mixed methods systematic review. Dev. Med. Child Neurol. 2021, 63, 914–924. [Google Scholar] [CrossRef] [PubMed]
- Berkman, L.F.; Glass, T.; Brissette, I.; Seeman, T.E. From social integration to health: Durkheim in the new millennium. Soc. Sci. Med. 2000, 51, 843–857. [Google Scholar] [CrossRef] [PubMed]
- Mahy, J.; Shields, N.; Taylor, N.F.; Dodd, K.J. Identifying facilitators and barriers to physical activity for adults with down syndrome. J. Intellect. Disabil. Res. 2010, 54, 795–805. [Google Scholar] [CrossRef]
- UN General Assembly. Convention on the Rights of Persons with Disabilities; United Nations: New York, NY, USA, 2006. [Google Scholar]
- Carlon, S.L.; Taylor, N.F.; Dodd, K.J.; Shields, N. Differences in habitual physical activity levels of young people with cerebral palsy and their typically developing peers: A systematic review. Disabil. Rehabil. 2013, 35, 647–655. [Google Scholar] [CrossRef]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef]
- Ryan, J.M.; Walsh, M.; Owens, M.; Byrne, M.; Kroll, T.; Hensey, O.; Kerr, C.; Norris, M.; Walsh, A.; Lavelle, G.; et al. Transition to adult services experienced by young people with cerebral palsy: A cross-sectional study. Dev. Med. Child Neurol. 2022. [Google Scholar] [CrossRef]
- Young, N.L.; Barden, W.S.; Mills, W.A.; Burke, T.A.; Law, M.; Boydell, K. Transition to adult-oriented health care: Perspectives of youth and adults with complex physical disabilities. Phys. Occup. Ther. Pediatr. 2009, 29, 345–361. [Google Scholar] [CrossRef]
- George, C.L.; Oriel, K.N.; Blatt, P.J.; Marchese, V. Impact of a community-based exercise program on children and adolescents with disabilities. J. Allied Health 2011, 40, e55–e60. [Google Scholar]
- Deci, E.L.; Ryan, R.M. Self-determination theory: A macrotheory of human motivation, development, and health. Can. Psychol. Psychol. Can. 2008, 49, 182–185. [Google Scholar] [CrossRef]
- Bandura, A.; Walters, R.H. Social Learning Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1977; Volume 1. [Google Scholar]
- Hassett, L.M.; Moseley, A.M.; Tate, R.L.; Harmer, A.R.; Fairbairn, T.J.; Leung, J. Efficacy of a fitness centre-based exercise programme compared with a home-based exercise programme in traumatic brain injury: A randomized controlled trial. J. Rehabil. Med. 2009, 41, 247–255. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, G.; Shields, N.; Willis, C. ‘Finding what works for me’—A qualitative study of factors influencing community gym participation for young adults with cerebral palsy. Disabil. Rehabil. 2022, 1–8. [Google Scholar] [CrossRef]
- Richardson, E.V.; Smith, B.; Papathomas, A. Disability and the gym: Experiences, barriers and facilitators of gym use for individuals with physical disabilities. Disabil. Rehabil. 2017, 39, 1950–1957. [Google Scholar] [CrossRef] [PubMed]
- Shields, N.; Taylor, N.F. A student-led progressive resistance training program increases lower limb muscle strength in adolescents with Down syndrome: A randomised controlled trial. J. Physiother. 2010, 56, 187–193. [Google Scholar] [CrossRef]
- Shields, N.; Taylor, N.F.; Wee, E.; Wollersheim, D.; O’Shea, S.D.; Fernhall, B. A community-based strength training programme increases muscle strength and physical activity in young people with Down syndrome: A randomised controlled trial. Res. Dev. Disabil. 2013, 34, 4385–4394. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Grimshaw, J. A Guide to Knowledge Synthesis: A Knowledge Synthesis Chapter; Canadian Institutes of Health Research: Ottawa, ON, Canada, 2010. [Google Scholar]
- Kennedy, R.A.; Shields, N. Social Support to Facilitate Physical Activity in Community Gyms for Young Adults with Disability: A Scoping Review Protocol. Available online: https://osf.io/td7r5/ (accessed on 19 October 2022).
- Collett, J.; Franssen, M.; Meaney, A.; Wade, D.; Izadi, H.; Tims, M.; Winward, C.; Bogdanovic, M.; Farmer, A.; Dawes, H. Phase II randomised controlled trial of a 6-month self-managed community exercise programme for people with Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2017, 88, 204–211. [Google Scholar] [CrossRef]
- Corcos, D.M.; Robichaud, J.A.; David, F.J.; Leurgans, S.E.; Vaillancourt, D.E.; Poon, C.; Rafferty, M.R.; Kohrt, W.M.; Comella, C.L. A two-year randomized controlled trial of progressive resistance exercise for Parkinson’s disease. Mov. Disord. 2013, 28, 1230–1240. [Google Scholar] [CrossRef]
- Dodd, K.; Taylor, N.; Shields, N.; Prasad, D.; McDonald, E.; Gillon, A. Progressive resistance training did not improve walking but can improve muscle performance, quality of life and fatigue in adults with multiple sclerosis: A randomized controlled trial. Mult. Scler. J. 2011, 17, 1362–1374. [Google Scholar] [CrossRef] [PubMed]
- Elsworth, C.; Winward, C.; Sackley, C.; Meek, C.; Freebody, J.; Esser, P.; Izadi, H.; Soundy, A.; Barker, K.; Hilton-Jones, D.; et al. Supported community exercise in people with long-term neurological conditions: A phase II randomized controlled trial. Clin. Rehabil. 2011, 25, 588–598. [Google Scholar] [CrossRef] [PubMed]
- Fenton, S.A.M.; Veldhuijzen van Zanten, J.J.; Metsios, G.S.; Rouse, P.C.; Yu, C.A.; Ntoumanis, N.; Kitas, G.D.; Duda, J.L. Testing a self-determination theory-based process model of physical activity behavior change in rheumatoid arthritis: Results of a randomized controlled trial. Transl. Behav. Med. 2021, 11, 369–380. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J.M.; Bell, K.R.; Powell, J.M.; Behr, J.; Dunn, E.C.; Dikmen, S.; Bombardier, C.H. A randomized controlled trial of exercise to improve mood after traumatic brain injury. PM&R 2010, 2, 911–919. [Google Scholar]
- Kovacic, T.; Kovacic, M.; Ovsenik, R.; Zurc, J. The impact of multicomponent programmes on balance and fall reduction in adults with intellectual disabilities: A randomised trial. J. Intellect. Disabil. Res. 2020, 64, 381–394. [Google Scholar] [CrossRef]
- Lampousi, A.-M.; Berglind, D.; Forsell, Y. Association of changes in cardiorespiratory fitness with health-related quality of life in young adults with mobility disability: Secondary analysis of a randomized controlled trial of mobile app versus supervised training. BMC Public Health 2020, 20, 1721. [Google Scholar] [CrossRef]
- Pau, M.; Corona, F.; Coghe, G.; Marongiu, E.; Loi, A.; Crisafulli, A.; Concu, A.; Galli, M.; Marrosu, M.G.; Cocco, E. Quantitative assessment of the effects of 6 months of adapted physical activity on gait in people with multiple sclerosis: A randomized controlled trial [with consumer summary]. Disabil. Rehabil. 2018, 40, 144–151. [Google Scholar] [CrossRef]
- Shields, N.; Bennell, K.L.; Radcliffe, J.; Taylor, N.F. Is strength training feasible for young people with Prader-Willi syndrome? A phase I randomised controlled trial. Physiotherapy 2020, 106, 136–144. [Google Scholar] [CrossRef]
- Shields, N.; Taylor, N.F.; Dodd, K.J. Effects of a community-based progressive resistance training program on muscle performance and physical function in adults with Down syndrome: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2008, 89, 1215–1220. [Google Scholar] [CrossRef]
- Shields, N.; Willis, C.; Imms, C.; McKenzie, G.; van Dorsselaer, B.; Bruder, A.M.; Kennedy, R.A.; Bhowon, Y.; Southby, A.; Prendergast, L.A.; et al. Feasibility of scaling-up a community-based exercise program for young people with disability. Disabil. Rehabil. 2021, 44, 1669–1681. [Google Scholar] [CrossRef]
- Sims, J.; Galea, M.; Taylor, N.; Dodd, K.; Jespersen, S.; Joubert, L.; Joubert, J. Regenerate: Assessing the feasibility of a strength-training program to enhance the physical and mental health of chronic post stroke patients with depression. Int. J. Geriatr. Psychiatry 2009, 24, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Taylor, N.F.; Dodd, K.J.; Baker, R.J.; Willoughby, K.; Thomason, P.; Graham, H.K. Progressive resistance training and mobility-related function in young people with cerebral palsy: A randomized controlled trial. Dev. Med. Child Neurol. 2013, 55, 806–812. [Google Scholar] [CrossRef]
- Wallace, A.; Pietrusz, A.; Dewar, E.; Dudziec, M.; Jones, K.; Hennis, P.; Sterr, A.; Baio, G.; Machado, P.M.; Laurá, M.; et al. Community exercise is feasible for neuromuscular diseases and can improve aerobic capacity. Neurology 2019, 92, e1773–e1785. [Google Scholar] [CrossRef] [PubMed]
- Pett, M.; Clark, L.; Eldredge, A.; Cardell, B.; Jordan, K.; Chambless, C.; Burley, J. Effecting healthy lifestyle changes in overweight and obese young adults with intellectual disability. Am. J. Intellect. Dev. Disabil. 2013, 118, 224–243. [Google Scholar] [CrossRef]
- Poliakoff, E.; Galpin, A.J.; McDonald, K.; Kellett, M.; Dick, J.P.; Hayes, S.; Wearden, A.J. The effect of gym training on multiple outcomes in Parkinson’s disease: A pilot randomised waiting-list controlled trial. NeuroRehabilitation 2013, 32, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Obrusnikova, I.; Cavalier, A.R.; Suminski, R.R.; Blair, A.E.; Firkin, C.J.; Steinbrecher, A.M. A Resistance Training Intervention for Adults With Intellectual Disability in the Community: A Pilot Randomized Clinical Trial. Adapt. Phys. Act. Q. 2021, 38, 546–568. [Google Scholar] [CrossRef]
- Danoudis, M.; Iansek, R. A long-term community gym program for people with Parkinson’s disease: A feasibility study of the Monash Health “Health and Fitness” model. Disabil. Rehabil. 2021, 44, 7330–7338. [Google Scholar] [CrossRef]
- Duret, C.; Breuckmann, P.; Louchart, M.; Kyereme, F.; Pepin, M.; Koeppel, T. Adapted physical activity in community-dwelling adults with neurological disorders: Design and outcomes of a fitness-center based program. Disabil. Rehabil. 2020, 44, 536–541. [Google Scholar] [CrossRef]
- Morris, S.; Dodd, K.J.; Morris, M.; Matyas, T. Community-based progressive resistance strength training in traumatic brain injury: A multiple, single-system, trial. Adv. Physiother. 2009, 11, 218–226. [Google Scholar] [CrossRef]
- Ploughman, M.; Shears, J.; Harris, C.; Hogan, S.H.; Drodge, O.; Squires, S.; McCarthy, J. Effectiveness of a novel community exercise transition program for people with moderate to severe neurological disabilities. NeuroRehabilitation 2014, 35, 105–112. [Google Scholar] [CrossRef]
- Taylor, N.F.; Dodd, K.J.; Larkin, H. Adults with cerebral palsy benefit from participating in a strength training programme at a community gymnasium. Disabil. Rehabil. 2004, 26, 1128–1134. [Google Scholar] [CrossRef] [PubMed]
- Taylor, N.F.; Dodd, K.J.; Prasad, D.; Denisenko, S. Progressive resistance exercise for people with multiple sclerosis. Disabil. Rehabil. 2006, 28, 1119–1126. [Google Scholar] [CrossRef] [PubMed]
- Temple, V.A.; Stanish, H.I. The feasibility of using a peer-guided model to enhance participation in community-based physical activity for youth with intellectual disability. J. Intellect. Disabil. 2011, 15, 209–217. [Google Scholar] [CrossRef]
- Zanudin, A.; Mercer, T.; Samaan, C.; Jagadamma, K.; McKelvie, G.; van der Linden, M. A community-based exercise program for ambulant adolescents and young adults with cerebral palsy, a feasibility study. Eur. J. Adapt. Phys. Act. 2021, 14, 12. [Google Scholar] [CrossRef]
- Handlery, R.; Regan, E.; Foster Lewis, A.; Larsen, C.; Handlery, K.; Flach, A.; Fritz, S. Active Participation of Care Partners in a Physical Activity Intervention Alongside People with Stroke: A Feasibility Study. Physiother. Can. 2022, 74, 97–110. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.; Dodd, K.J.; Taylor, N.F.; McBurney, H.; Larkin, H. Strength training can be enjoyable and beneficial for adults with cerebral palsy. Disabil. Rehabil. 2004, 26, 1121–1127. [Google Scholar] [CrossRef]
- Dodd, K.J.; Taylor, N.F.; Denisenko, S.; Prasad, D. A qualitative analysis of a progressive resistance exercise programme for people with multiple sclerosis. Disabil. Rehabil. 2006, 28, 1127–1134. [Google Scholar] [CrossRef]
- Hansen, A.; Søgaard, K.; Minet, L.R.; Jarden, J.O. A 12-week interdisciplinary rehabilitation trial in patients with gliomas—A feasibility study. Disabil. Rehabil. 2018, 40, 1379–1385. [Google Scholar] [CrossRef]
- Shields, N.; van den Bos, R.; Buhlert-Smith, K.; Prendergast, L.; Taylor, N. A community-based exercise program to increase participation in physical activities among youth with disability: A feasibility study. Disabil. Rehabil. 2019, 41, 1152–1159. [Google Scholar] [CrossRef]
- Carter, M.J.; McCown, K.M.; Forest, S.; Martin, J.; Wacker, R.; Gaede, D.; Fernandez, T.A. Exercise and fitness for adults with developmental disabilities: Case report of a group intervention. Ther. Recreat. J. 2004, 38, 72–84. [Google Scholar]
- Stanish, H.I.; Temple, V.A. Exercise behaviours of youths with intellectual disability under two conditions in a community programme. World Leis. J. 2012, 54, 280–287. [Google Scholar] [CrossRef]
- Obrusnikova, I.; Novak, H.M.; Cavalier, A.R. The Effect of Systematic Prompting on the Acquisition of Five Muscle-Strengthening Exercises by Adults With Mild Intellectual Disabilities. Adapt. Phys. Act. Q. 2019, 36, 447–471. [Google Scholar] [CrossRef]
- Stanish, H.I.; Temple, V.A. Efficacy of a peer-guided exercise programme for adolescents with intellectual disability. J. Appl. Res. Intellect. Disabil. 2012, 25, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Bania, T.A.; Dodd, K.J.; Baker, R.J.; Graham, H.K.; Taylor, N.F. The effects of progressive resistance training on daily physical activity in young people with cerebral palsy: A randomised controlled trial. Disabil. Rehabil. 2016, 38, 620–626. [Google Scholar] [CrossRef] [PubMed]
- Obrusnikova, I.; Cavalier, A.R.; Novak, H.M.; Blair-McKinsey, A.E.; Suminski, R.R. Effects of a Community-Based Familiarization Intervention on Independent Performance of Resistance-Training Exercise Tasks by Adults With Intellectual Disability. Intellect. Dev. Disabil. 2021, 59, 239–255. [Google Scholar] [CrossRef]
- Winward, C.; Life Research, G. Supporting community-based exercise in long-term neurological conditions: Experience from the long-term individual fitness enablement (LIFE) project. Clin. Rehabil. 2011, 25, 579–587. [Google Scholar] [CrossRef]
- Berglind, D.; Nyberg, G.; Willmer, M.; Persson, M.; Wells, M.; Forsell, Y. An eHealth program versus a standard care supervised health program and associated health outcomes in individuals with mobility disability: Study protocol for a randomized controlled trial. Trials 2018, 19, 258. [Google Scholar] [CrossRef]
- National Disability Insurance Scheme (NDIS). Available online: https://www.ndis.gov.au/ (accessed on 20 December 2022).
- Starowicz, J.; Pratt, K.; McMorris, C.; Brunton, L. Mental Health Benefits of Physical Activity in Youth with Cerebral Palsy: A Scoping Review. Phys. Occup. Ther. Pediatr. 2022, 42, 434–450. [Google Scholar] [CrossRef]
- Verschuren, O.; Peterson, M.D.; Balemans, A.C.; Hurvitz, E.A. Exercise and physical activity recommendations for people with cerebral palsy. Dev. Med. Child Neurol. 2016, 58, 798–808. [Google Scholar] [CrossRef]
- Enright, E.; Beckman, E.M.; Connick, M.J.; Dutia, I.M.; Macaro, A.; Wilson, P.J.; O’Sullivan, J.; Lavalliere, J.-M.; Block, T.; Johnston, L.M.; et al. Competitive sport, therapy, and physical education: Voices of young people with cerebral palsy who have high support needs. Br. J. Sport. Med. 2021, 55, 524–525. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).