
Can Group Exercise Programs Improve Health Outcomes in Pregnant Women? An Updated Systematic Review

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Criteria for Considering Studies for This Review
2.1.1. Types of Studies
2.1.2. Participants
2.1.3. Type of Interventions
2.1.4. Outcomes Measures
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction
- author and year of publication;
- sample size, characteristics of participants, country and location where the study was performed, and gestational week;
- purpose of study, study design including type, frequency, and duration of intervention, exercise intensity, equipment, exercise and health specialists leading the program, and the number of participants in each session;
- maternal and fetal health and fitness outcomes measured;
- results of outcomes measured.
2.5. Quality Assessment of the Studies
2.6. The Consensus of Exercise Reporting Template (CERT)
3. Results
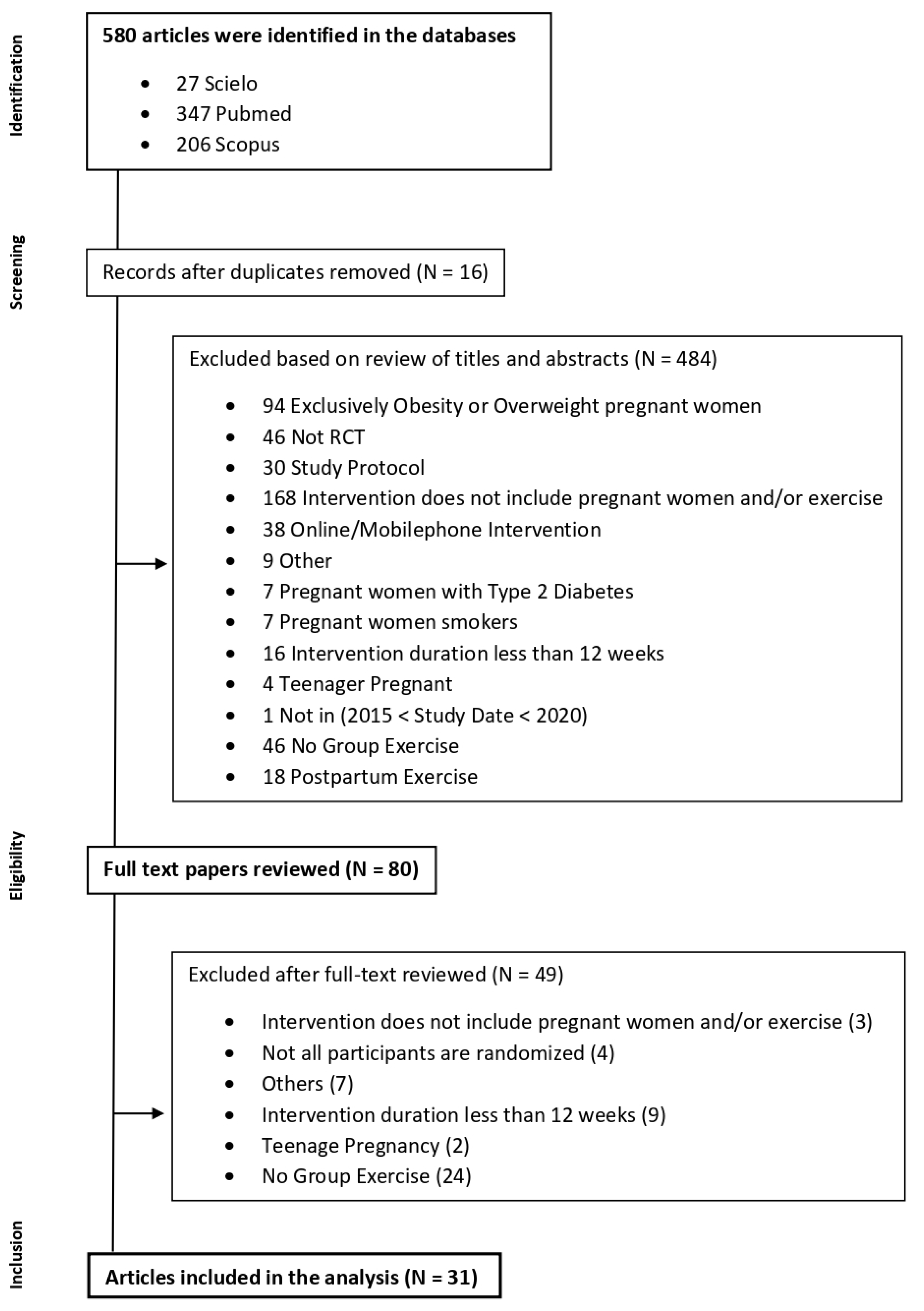
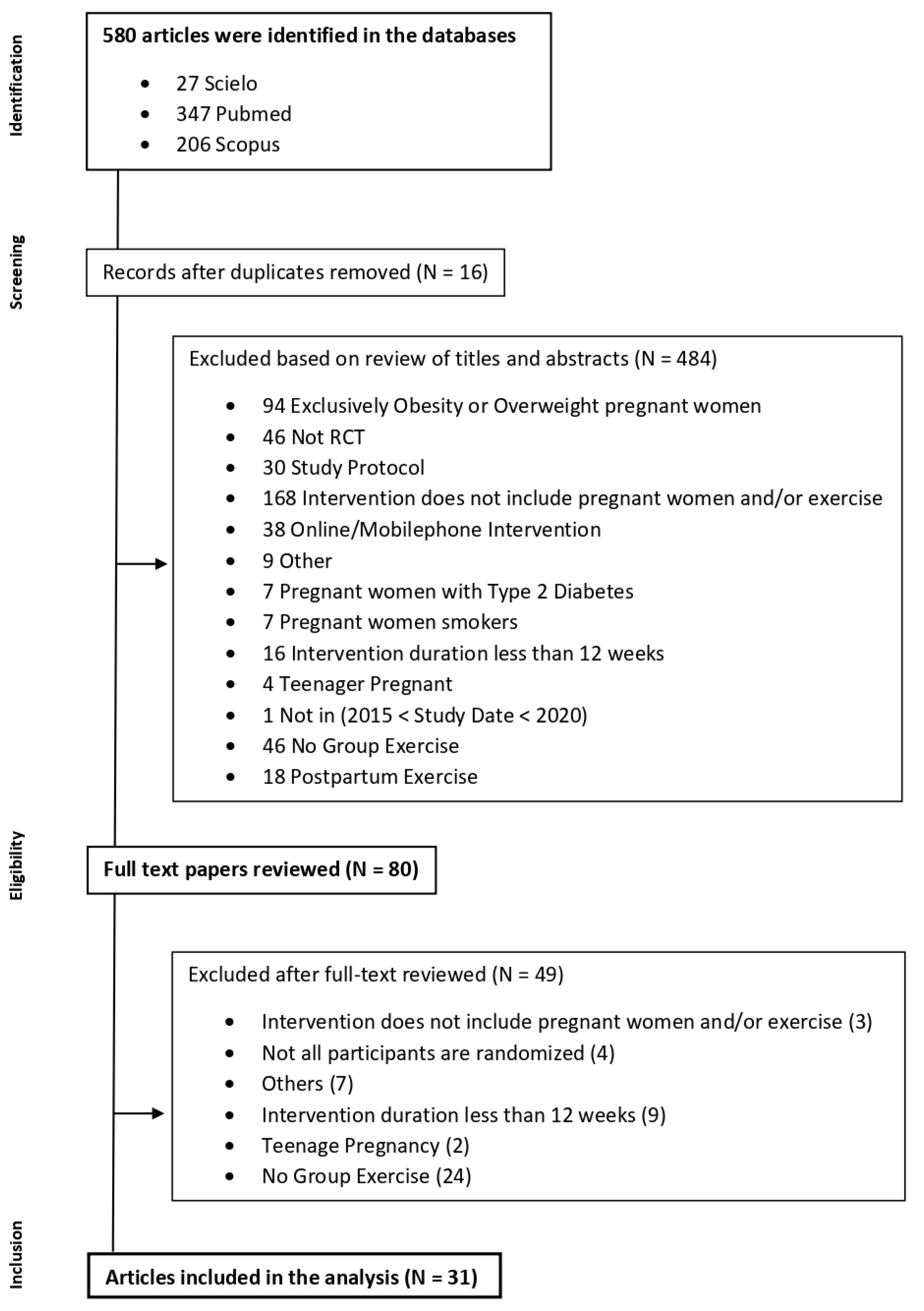
3.1. Study Selection
3.2. Characteristics of the Studies

{kind=link}
| Authors | D1 | D2 | D3 | D4 | D5 | Overall |
|---|---|---|---|---|---|---|
| Sánchez-García, J. (2019) [43] | + | + | + | + | + | + |
| Cordero, J. (2017) [17] | + | + | + | + | + | + |
| Bacchi, M. (2017) [39] | + | + | + | + | + | + |
| Haakstad, L. (2016) [7] | + | + | + | + | + | + |
| Sagedal, L.R. (2017) [18] | + | + | + | + | + | + |
| Sagedal, L.R. (2017) [19] | + | + | + | ! | + | ! |
| A-Cordero, M. (2018) [20] | + | + | + | + | + | + |
| Barakat, R. (2018) [40] | + | + | + | + | + | + |
| Sanda, B. (2018) [37] | ! | + | ! | + | + | ! |
| Terrones, M. (2018) [21] | + | + | + | + | ! | ! |
| Blanque, R. (2017) [38] | + | + | + | + | + | + |
| Dias, N. (2017) [22] | + | + | + | + | + | + |
| Haakstad, L. (2015) [23] | + | + | ! | + | + | ! |
| Gustafsson, M.K. (2015) [24] | + | + | + | + | + | + |
| Charkamyani, F. (2019) [25] | + | + | + | + | + | + |
| Perales, M. (2015) [26] | + | + | + | + | + | + |
| Palaez, M. (2019) [41] | + | + | + | + | + | + |
| Clark, E. (2019) [27] | + | + | + | + | ! | ! |
| Haakstad, L. 2020) [28] | + | + | + | + | + | + |
| Blanque, R. (2020) [29] | + | + | + | + | + | + |
| Blanque, R. (2020) [30] | + | + | + | + | + | + |
| Reoyo, O. (2019) [31] | + | + | + | + | + | + |
| Blanque, R. (2019) [32] | + | + | + | + | + | + |
| Brik, M. (2018) [33] | + | + | + | + | + | + |
| Coll, C. (2019) [12] | + | + | + | + | + | + |
| Blanque, R. (2019) [34] | + | + | + | + | + | + |
| Awad, E. (2019) [35] | + | + | - | + | ! | - |
| Barakat, R. (2017) [5] | + | + | + | + | + | + |
| Pawalia, A. (2017) [36] | − | ! | ! | + | + | − |
| Barakat, R. (2016) [4] | + | + | + | + | + | + |
| Cordero, Y. (2015) [42] | ! | + | + | + | + | ! |
| Authors and Year of Publication | Participants and Location | Objectives | Study Design | Measures | Results |
|---|---|---|---|---|---|
| Juan Carlos Sánchez-García et al. (2019) [43] | N = 129 IG = 65 + CG = 64 Healthy PW without contraindications for practice ACOG (2015). Gestational Week: 20th Location: Granada, Spain | To examine the gestational weight gain and postpartum on pregnant women who realized moderate physical exercise in an aquatic environment. | Type of Intervention: RCT (CG × IG) Description: The IG had access to a moderate intensity physical exercise program in water. The intervention was supervised by an exercise specialist. The CG received usual care and general advice on the benefits of exercise. Intensity Measurement: Borg Scale or Heart Rate Time of session: 60′ Frequency: 3x / week Duration of Intervention: 17 weeks | Primary: GWG, weight retention (16th and 18th postpartum week), and newborn weight. Secondary: The level of physical activity (GPAQ at 12th gestational week) and baseline maternal characteristics. | The study showed that the variables of GWG, weight retention (4 and 7 months), and newborn weight presented lower values on IG. |
| JAM Cordero et al. (2017) [17] | N = 140 IG = 70 + CG = 70 Healthy PW without contraindications for practice (ACOG 2015). Gestational Week: 20th Location: Granada, Spain | To examine the effect of a physical exercise program with moderate intensity during pregnancy in water on newborn weight. | Type of Intervention: RCT (CG × IG) Description: The IG had access to a moderate intensity physical exercise program in water. The intervention was supervised by an exercise specialist. The CG received usual care and general advice on the benefits of exercise. Intensity Measurement: Borg Scale or Heart Rate Time of session: 60′ Frequency: 3x / week Duration of Intervention: 17 weeks | Primary: Days of gestation and newborn weight. Secondary: maternal weight (1st and 3rd trimesters) and baseline maternal characteristics. | Lower values of newborn weight in IG. However, these differences did not represent clinical trends because both groups are in a normal state of weight. |
| Mariano Bacchi et al. (2017) [39] | N = 111 IG = 49 + CG = 62 Healthy PW without contraindications for practice (ACOG 2002). Gestational Week: 10th Location: Buenos Aires, Argentina. | To examine the influence of supervision and regular water activities program during pregnancy on maternal weight gain and birth weight. | Type of Intervention: RCT (CG × IG) Description: Moderate physical exercise intervention in water. Sessions included aerobic, strength, and aquatic activities, in standing, supine and ventral positions. Relax phase included relaxing, stretching, and breathing exercises. The intervention was supervised by an exercise specialist. The CG received usual care and did not report any physical exercise during pregnancy. Water Temperature: 28.5° to 29° Intensity Measurement: BORG Scale Time of session: 55 to 60 min Frequency: 3 per/week Duration of Intervention: 26 weeks | Primary: GWG and birth weight. Secondary: baseline maternal characteristics. | Higher percentage of women with excessive maternal weight gain in CG No differences between groups on the birth weight variable. |
| Lene A. H. Haakstad et al. (2015) [4] | N = 61 IG = 35 + CG = 26 Healthy PW without contraindications for practice (ACOG 2002). Gestational Week: 24th Location: Oslo, Norway. | To evaluate the effect of regular exercise on maternal arterial blood pressure at rest and during uphill walking. | Type of Intervention: RCT (CG × IG) Description: Moderate intensity physical exercise program. Each session included warm-up, aerobic, strength (general and pelvic), and relax phases. The participants were advised to do at least 30′ of moderate physical exercise on the rest of the days. The CG received usual care and recommendations for maintaining physical activity without receiving some incentive for physical exercise practice. Intensity Measurement: Borg Scale Time of session: 60 min Frequency: 2x/week Duration of Intervention: 12 weeks | Primary: Resting systolic and diastolic blood pressure (three times by auscultatory techniques) and walking systolic and diastolic blood pressure (during monitoring walking). This was performed before and after the intervention. | Lower values of blood pressure in rest in IG. The values of blood pressure during exercise were lower on IG. |
| Linda R. Sagedal et al. (2016) [18] | N = 591 IG = 296 + CG = 295 Healthy PW without contraindications for practice (ACOG 2002). Gestational Week: ≤20th Location: Kristiansand and Mandal, Norway. | To examine whether a lifestyle intervention on nutrition and physical exercise in pregnancy limits GWG and provides measurable health benefits for mother and newborn. | Type of Intervention: RCT (CG × IG) Description: Dietary and physical exercise intervention. The group was encouraged to engage in 30′ of moderate-intensity physical activity on three additional days per week. Counselling dietary was performed by phone. The sessions were supervised by the therapists or students in sports science, trained, and quality controlled by the team. The CG received routine prenatal care in accordance with Norwegian standards. They received a booklet with advice on prenatal nutrition and physical activity. Intensity Measurement: Borg Scale Time of session: 60 min Frequency: 2x/week Duration: 12 weeks | Primary: GWG, birthweight, the proportion of infants weighing >4000 g, and the incidence of operative deliveries. Secondary: the proportion of newborns of birthweight ≥90th percentile, the incidence of delivery complications. | Statistically significant decrease in GWG in the IG. The intervention did not decrease the incidence of pregnancy complications or operative delivery and had no effect on fetal weight or neonatal outcomes. |
| Linda R. Sagedal et al. (2017) [19] | N = 591 IG = 296 + CG = 295 Healthy PW without contraindications for practice (ACOG 2002). Gestational Week: ≤20th Location: Kristiansand and Mandal, Norway. | To examine the effect of the exercise intervention on glucose metabolism, including an assessment of the subgroups of normal-weight and overweight/obese participants | Intervention: RCT (CG × IG) Description: Dietary and physical exercise intervention. The group was encouraged to engage in 30′ of moderate-intensity physical activity on three additional days per week. Counselling dietary was performed by phone. The sessions were supervised by the therapists or students in sports science, trained, and quality controlled by the team. The CG received routine prenatal care in accordance with Norwegian standards. They received a booklet with advice on prenatal nutrition and physical activity. Intensity Measurement: Borg Scale Time of session: 60 min Frequency: 2x/week Duration: 12 weeks | Primary: GWG, birth weight of term infants, the proportion of term infants >4000 g, maternal fat percent at 36 gestational weeks, and the incidence of operative deliveries. Secondary: proportion of women with elevated 2-h glucose tolerance tests and measurement of hormones related to glucose metabolism. | Statistically significant reduction of GWG. In variables of infants, there were no differences. The levels of insulin were statistically significantly lower in IG. In the normal weight sub-group, there was a reduction in levels of insulin and leptin. In the obesity sub-group, the only difference was in fasted glucose values. |
| María José Aguilar-Cordero et al. (2019) [20] | N = 129 GI = 65 + GC = 64 Healthy PW without contraindications for practice (ACOG 2015). Gestational Week: 12th/20th Location: Granada, Spain. | To determine whether physical activity during pregnancy alleviates Postpartum Depression | Type of Intervention: RCT (CG × IG) Description: The IG had access to a moderate intensity physical exercise program in water. The intervention was supervised by an exercise specialist. The CG received usual care and general advice on the benefits of exercise. Intensity Measurement: Borg Scale or Heart Rate Time of session: 60′ Frequency: 3x/week Duration of Intervention: 17 weeks | Primary: Prevalence of PPD. Secondary: Baseline maternal characteristics and GWG. | In the normal weight category, for PPD evaluation there were statistically significant differences between groups. However, none of the groups were at high risk of postpartum depression. For overweight and obesity categories there were statistically significant differences. Contrary to a category of normal weight, the CG showed values of a high risk of postpartum depression. Lower weight gain in IG. |
| Ruben Barakat et al. (2018) [40] | N = 456 GI = 234 + GC = 222 Healthy PW without contraindications for practice (ACOG 2015). Gestational Week: 8th/10th Location: Madrid, Spain. | Examine the effects of an exercise program throughout pregnancy on maternal weight gain and the prevalence of gestational diabetes | Type of Intervention: RCT (CG × IG) Description: Moderate intensity physical exercise intervention. Each session included warm-up, aerobic, light muscle strengthening, coordination, balance, and stretching exercises. All sessions were accompanied by music and the room had appropriate conditions to practice (altitude 600 m; temperature 19–21 °C; humidity 50–60%). The CG attended regular scheduled visits to their obstetricians and midwives, usually every 4–5 weeks until the 36–38th week of gestation and then weekly until delivery. They received general nutrition and physical activity counseling from their healthcare provider. Intensity Measurement: Borg Scale (12–14) Time of session: 55 to 60 min Frequency: 3x/week Duration: 30 weeks | Primary: GWG, excessive gestational weight gain (yes/no), GDM, 1 h OGTT. Secondary: maternal gestational age at delivery, type of delivery, and birth weight | IG presented lower GWG compared with CG. The ratio of women that gained excessive weight was higher in the CG than in the IG. IG presented statistically significant lower values of OGTT results compared with CG. The ratio of women diagnosed with GDM was higher in the CG than the IG, with statistically significant differences. The results just showed that the ratio of neonate macrosomia was slightly higher in CG than in the IG. |
| Birgitte Sanda et al. (2018) [37] | N = 606 GI = 295 + GC = 294 Healthy PW without contraindications for practice (ACOG 2002). Gestational Week: 18th Location: Norway. | Examine the effect of a lifestyle intervention including group exercise classes, as well as the possible influence of physical activity level in late pregnancy, on labor outcomes. | Type of Intervention: RCT (CG × IG) Description: Dietary and physical activity intervention. The IG was encouraged to engage in 30′ of moderate-intensity physical activity on three additional days per week. Counselling dietary was performed by phone. The sessions were supervised by the therapists or students in sports science, trained, and quality controlled by the team. The CG received routine prenatal care in accordance with Norwegian standards. They also received a booklet with advice on prenatal nutrition and physical activity. Intensity Measurement: Borg Scale (12–14) Time of session: 60 min Frequency: 2 per/week Duration: 30 weeks | Primary: The duration and type of labor. Secondary: Baseline maternal characteristics, other information of labor. | IG experienced a longer 1st stage of labor with a statistically significant difference compared with CG. PW with a high level of PA levels in late pregnancy had lower odds for acute cesarean delivery compared to women with low levels. Epidural analgesia was more common among in the low active group compared to women in the high active group. |
| Marina Vargas-Terrones et al. (2018) [21] | N = 124 GI = 70 + GC = 54 Healthy PW without contraindications for practice (ACOG 2015). Gestational Week: <16th Location: Madrid, Spain. | To examine the effect of an exercise program during pregnancy on the risk of perinatal depression. | Type of Intervention: RCT (CG × IG) Description: Moderate intensity physical exercise intervention. Each session included warm-up, aerobic, strength exercises, and stretching and relaxation. The sessions were supervised by a qualified fitness specialist. Both groups received usual care from health professionals of the hospital and the general recommendations of nutrition and exercise. Intensity Measurement: Borg Scale (12–14) or heart rate (55–60%) Time of session: 60 min Frequency: 3 per/week Duration: 30 weeks | Primary: Risk of depression was measured at the beginning of the study (12–16 weeks), at gestational week 38, and the 6th week postpartum. Secondary: Baseline maternal characteristics. | The prevalence of women with depression was lower in IG. These differences were shown at gestational week 38 and week 6 postpartum. |
| R. Rodriguez Blanque et al. (2017) [38] | N = 134 GI = 67 + GC = 67 Healthy PW without contraindications for practice (ACOG 2015). Gestational Week: 12th/20th Location: Granada, Spain. | To determine whether, in pregnant women, there is an association between moderate-intensity physical activity in an aquatic environment and sleep quality. | Type of Intervention: RCT (CG × IG) Description: The IG had access to moderate intensity physical exercise program in water. The intervention was supervised by an exercise specialist. The CG received usual care and general advice on the benefits of exercise. Intensity Measurement: Borg Scale or Heart Rate Time of session: 60′ Frequency: 3x/week Duration of Intervention: 17 weeks | Primary: Sleep quality was evaluated in the 1st and 3rd trimesters. Secondary: Baseline maternal characteristics. | This study showed that IG had better results in quality, duration, latency, and regular efficiency of sleep, compared with CG. |
| Naiara T. Dias et al. (2017) [22] | N = 50 GI = 25 + GC = 25 Healthy PW without contraindications for practice (ACOG 2015). Gestational Week: 14th/16th Location: Uberlândia, Brazil. | Evaluate the effectiveness of a Pilates exercise program with PFM contraction compared to a conventional intervention in pregnant women. | Intervention: RCT (CG × IG) Description: Pilates exercise intervention. The intervention intensity increased after an adaptation period of 4 weeks. Mats, therapeutic balls, and elastic bands were used. The intervention was supervised by an exercise specialist. The CG underwent walking for 10′ and strengthening exercises of the lower libs, upper limbs, and trunk with an elastic band and body weight resistance. At the end of each session, the women performed stretching and relaxation exercises. No type of instruction or verbal command was given regarding the PFM and abdominal muscle contraction. Intensity Measurement: Borg Scale (13–14) Time of session: 60 min Frequency: 2x/week Duration: 18 weeks | Primary: PFM strength (manometer) measured at 14th and 16th weeks and, again between the 32nd and 34th weeks of gestation. Secondary: digital palpation variables—PFM strength using Oxford Scale, PFM endurance, and PFM repeatability. | There were no significant differences between groups for the PFM strength assessed by manometer. The IG presented significantly better results on PFM strength measured through the Oxford scale, PFM endurance, and PFM repeatability, compared to CG. |
| Lene A.H. Haakstad et al. (2016) [23] | N = 105 GI = 52 + GC = 53 Healthy PW without contraindications for practice (ACOG 2002). Gestational Week: <24th Location: Oslo, Norway. | To examine the effects of supervised group exercise on maternal psychological outcomes and commonly reported pregnancy complaints. | Type of Intervention: RCT (CG × IG) Description: Moderate intensity physical exercise intervention. Each session included warm-up, cardiovascular training, strength (core muscles), and stretch and relaxation phase. The intervention was supervised by an exercise specialist. The CG was asked to continue their usual physical activity habits and were neither encouraged nor discouraged from exercising. Intensity Measurement: Borg Scale (12–14) Time of session: 60 min Frequency: 2x/week Duration: At least 12 weeks | Primary: well-being, QOL, body-image, and negative mood symptoms/maternal depression (WHOQOL-bref and SF-36). Secondary: pregnancy complaints, pelvic girdle pain, and LBP. | IG presented significantly lower values in the fatigue variable compared with CG. IG presented higher values in health satisfaction compared with CG. The IG presented lower values in variables of nausea/vomiting and numbness/reduced circulation compared with CG. |
| MK Gustafsson et al. (2015) [24] | N = 761 GI = 396 + GC = 365 Healthy PW without contraindications for practice (ACOG 2002). Gestational Week: 18th/22th Location: Trondheim, Norway. | To investigate whether a customized exercise program influences pregnant women’s psychological wellbeing and general health perception reflecting HRQoL in late pregnancy. | Type of Intervention: RCT (CG × IG) Description: Moderate intensity physical exercise program. Each session included aerobic and strength phases. The participants were also encouraged to exercise three times a week. The intervention was supervised by an exercise specialist. CG received standard antenatal care and the customary information, and they were not discouraged from exercise. Women in both groups received written standardized information and recommendations on diet, pelvic floor muscle exercises, and pregnancy-related pelvic girdle pain. Intensity Measurement: Borg Scale (12–14) Time of session: Frequency: 1x/week Duration: At least 12 weeks | Primary: self-perceived general health and psychological wellbeing before and after the intervention. | The study did not show significant differences in general health perception and psychological wellbeing in the third trimester between IG and CG. |
| Forouzan Charkamyani et al. (2019) [25] | N = 170 GI = 85 + GC = 85 Healthy PW IVF with no contraindications for practice (ACOG 2002). Gestational Week: 12th/16th Location: Tehran, Iran. | The role of a structured program of exercise training in low-risk pregnancy in Iranian women undergoing in vitro fertilization (IVF) based on the reduction of gestational diabetes was examined. | Type of Intervention: RCT (CG × IG) Description: Moderate intensity physical exercise program. Each session included walking, aerobic, strength and relaxation exercises. The intervention was supervised by an exercise specialist. A similar number of classes (1 weekly session for 90 days) for both the groups were held to present routine and general care in the pregnancy period relevant to the significant impacts of physical activity on maternal and fetal health. Intensity Measurement: Borg Scale (12–14) Time of session: 60 min Frequency: 3x/week Duration: 12 weeks | Primary: GDM, OGTT at the 24–28 and 34 gestation weeks. Gestational hypertension was measured in three distinct analyses after 20 week’s gestation. | The present study showed significant differences in the suitability of physical activity after and before intervention in IG. CG did not present differences. IG had a significant reduction in GDM. The physical exercise intervention can highly decrease the risk of developing pre-eclampsia. |
| María Perales et al. (2016) [26] | N = 241 GI = 120 + GC = 121 Healthy PW without contraindications for practice (ACOG 2002). Gestational Week: <16th Location: Madrid, Spain. | Investigate the effects of pregnancy exercise on echocardiographic indicators of hemodynamics, cardiac remodeling, left ventricular function, and cardiovascular disease risk factors. | Type of Intervention: RCT (CG × IG) Description: Moderate intensity physical exercise intervention. Each session included warm-up, aerobic, strength, and stretch exercises. The intervention was supervised by an exercise specialist. The duration of the aerobic and strength training component was kept constant. During the first trimester, more importance was given to improving body awareness, in the second trimester, the priority was to improve balance, in the third trimester, more emphasis was given to improving pelvis mobility. Intensity Measurement: Borg Scale Time of session: 55 to 60 min Frequency: 3x/week Duration: 18 weeks | Secondary: Baseline maternal characteristics, hypertension was measured at 20th and 34th gestational weeks. GDM was measured at 24th to 28th gestational weeks. GWG and depression levels were measured at the end of the intervention. Pregnancy outcomes were identified at the delivery. | The proportion of women with excessive GWG at the end of pregnancy in the IG compared with the CG was significantly lower. The values of the depression scale were lower in IG compared with CG. |
| Mireia Pelaez et al. (2019) [41] | N = 345 GI = 115 + GC = 230 Healthy PW without contraindications for practice (ACOG 2002). Gestational Week: 8th/10th Location: Arroyo, Spain. | To investigate the effect of supervised moderate to vigorous exercise on gestational weight gain, its related risks (gestational diabetes), macrosomia, and type of delivery), and the preventive effects on women who exceed the weight gain recommendations. | Type of Intervention: RCT (CG × IG) Description: Moderate intensity physical exercise intervention. Each session included warm-up, core exercises, major muscles groups resistance training, and relaxation phase. The intervention was supervised by an exercise specialist. Supine position, ballistic movements, and high-impact exercises were avoided. Group dynamics were used to enhance motivation and adherence (games, exercises in pairs or groups, social networks such as Facebook and WhatsApp). The CG received standard care and physical activity counseling from health care professionals. They were not discouraged from exercising on their own. Intensity Measurement: Borg Scale (12–14) Time of session: 60 to 65 min Frequency: 3x/week Duration: 24 weeks | Primary: GWG was measured at the first and the last prenatal visit. Secondary: GDM, macrosomia, and type of delivery. | The study showed that IG gained less weight than CG with a significant difference. IG was less likely to exceed the 2009 Institute of Medicine (IoM) recommendations than CG. The values of macrosomia were lower in IG than in CG. More normal vaginal deliveries were found in the IG than in the CG. In this study, the relationship between excessive GWG and the risks mentioned existed only in the CG and not in the IG, which leads us to hypothesize that exercise provides some level of protection against the risks associated with excessive GWG. |
| Erin Clark et al. (2018) [27] | N = 36 GI = 14 + GC = 22 Healthy PW without contraindications for practice (ACSM 2010). Gestational Week: ≤ 16th Location: United States of America. | To determine the influence of exercise on maternal lipid levels and infant body size. | Type of Intervention: RCT (CG × IG) Description: Moderate intensity physical exercise intervention. Each session included warm-up, aerobic, and relaxation phases. The intervention was supervised by an exercise specialist. The CG did not receive an exercise intervention period. Intensity Measurement: Borg Scale (12–14) Time of session: 60 min Frequency: 3x/week Duration: 22 weeks | Primary: GWG, Non-fasting lipid profiles, blood samples, serum samples, total cholesterol, HDL, and triglycerides were calculated at 16th and 36th weeks gestation. Secondary: Infant measures included gestational age at birth, delivery mode, sex, Apgar score at 1 and 5 min, birth weight, birth length, head, and abdominal circumferences. | The study showed that IG presented lower values of triglycerides compared with CG. The head circumference at birth has a positive relationship with exercise during pregnancy. Improved infant outcomes are associated with lower pre-pregnancy BMI, along with increased physical exercise levels during pregnancy and late pregnancy LDL levels. Birth weight and length are associated with the amount of aerobic exercise during pregnancy and maternal lipid levels. No differences in Apgar score between groups. |
| Lene A. H Haakstad et al. (2020) [28] | N = 105 GI = 52 + GC = 53 Healthy PW without contraindications for practice (ACOG 2002). Gestational Week: ≤12th Location: Olso, Norway. | To investigate the sole effect of supervised group exercise, including pelvic floor muscle training on the course of labor and mode of delivery. | Type of Intervention: RCT (CG × IG) Description: Moderate physical exercise intervention. Each session included warm-up, cardiovascular, strength, and relaxation phases. The intervention was supervised by an exercise specialist. Intensity Measurement: Borg Scale (12–14) Time of session: 60 min Frequency: Duration: At least 12 weeks. (36 sessions) | Primary: The course of labor and mode of delivery. Secondary: Baseline maternal characteristics. | In the mode of delivery, IG had more cesarean sections compared with the CG, without significant differences. |
| Raquel Rodríguez-Blanque et al. (2020) [29] | N = 129 GI = 65 + GC = 64 Healthy PW without contraindications for practice (ACOG 2015). Gestational Week: 20th Location: Granada, Spain. | To analyze the HRQoL in pregnancy for women who complete a program of moderate physical activity in the water. | Type of Intervention: RCT (CG × IG) Description: The intervention group had access to a moderate physical exercise program in water. The intervention was supervised by an exercise specialist. The CG received usual care and general advice on the benefits of exercise. Both groups received verbal and written dietary advice during pregnancy. Intensity Measurement: Borg Scale or Heart Rate Time of session: 60′ Frequency: 3x/week Duration of Intervention: 17 weeks | Primary: HRQol at the beginning and at the end of the intervention. Secondary: Sociodemographic and anthropometric variables were measured in the first and third trimesters and parity. Body weight was measured at weeks 12 and 36 of pregnancy. Perinatal results were identified after delivery. The level of physical activity was measured with a questionnaire at the beginning of the study. | The decrease in mean HRQol scores was significantly higher in the CG compared with IG. CG presented a higher risk of depression compared with IG. |
| Raquel Rodríguez-Blanque et al. (2020) [30] | N = 129 GI = 65 + GC = 64 Healthy PW without contraindications for practice (ACOG 2015). Gestational Week: 12th/20th Location: Granada, Spain. | To evaluate the prevalence of spontaneous birth among women who participated in a water-based physical exercise program. | Type of Intervention: RCT (CG × IG) Description: The intervention group had access to a moderate physical exercise program in water. The intervention was supervised by an exercise specialist. The CG received usual care and general advice on the benefits of exercise. Both groups received verbal and written dietary advice during pregnancy. Intensity Measurement: Borg Scale or Heart Rate Time of session: 60′ Frequency: 3x/week Duration of Intervention: 17 weeks | Primary: Intrapartum and neonatal outcomes (gestational age, reason for hospital admission, birth weight, and Apgar test). Secondary: sociodemographic and anthropometric variables were measured at the beginning and at the end of the intervention. | IG presented better control of GWG and higher rate of spontaneous birth and a lower rate of instrumental deliveries and cesarean sections. GWG is related to the Apgar score. PW with BMI is in the normal-weight range had more probably to have a baby with an Apgar score of 10 at five minutes. PW whose BMI is in the normal-weight range at the start of pregnancy are more likely to give birth spontaneously than those with overweight or obesity before pregnancy. An appropriate GWG is related to a physiological birth, while PW who present a higher GWG are more likely to require instrumental birth. |
| Olga Roldan-Reoyo et al. (2019) [31] | N = 131 GI = 64 + GC = 67 Healthy PW without contraindications for practice (ACOG 2002). Gestational Week: 10th/12th Location: Madrid, Spain. | To determine if regular maternal physical activity leads to measurable adaptations of the fetal autonomic nervous system measured by FHR response recovery time. | Intervention: RCT (CG × IG) Description: Moderate intensity physical exercise intervention. Each session included warm-up, aerobic, strength, pelvic floor, and stretching exercises. The intervention was supervised by an exercise specialist. Intensity Measurement: 40–60% heart rate reserve (HRR) Time of session: 60 min Frequency: 3x/week Duration: 28 weeks | Primary: FHR recovery time was measured between 34th and 36th gestational weeks (at 40% and 60% maternal HRR). Secondary: MHR recovery time, FHR at rest, FHR after exercise, and the difference between these timepoints. | This study showed that supervised moderate intensity exercise during pregnancy is associated with quicker FHR recovery time. |
| Raquel Rodríguez-Blanque et al. (2019) [32] | N = 129 GI = 65 + GC = 64 Healthy PW without contraindications for practice (ACOG 2015). Gestational Week: 12th Location: Granada, Spain. | To determine the effect of an aquatic physical exercise program performed during pregnancy on the rate of intact perineum after childbirth. | Type of Intervention: RCT (CG × IG) Description: The intervention group had access to moderate intensity physical exercise program in water. The intervention was supervised by an exercise specialist. The CG received usual care and general advice on the benefits of exercise. Both groups received verbal and written dietary advice during pregnancy. Intensity Measurement: Borg Scale or Heart Rate Time of session: 60′ Frequency: 3x/week Duration of Intervention: 17 weeks | Primary: Reason for admission, mode of labor, integrity of the perineum (intact, lacerations, episiotomy), gestation time, birth weight, and analgesia during labor. Secondary: Baseline maternal characteristics, GWG, level of physical activity (questionnaire). | The study showed that the IG presented lower values in birth weight compared with the CG, with a significant difference. In a variable of integrity of the perineum, the IG had significantly more incidences compared with the CG. The CG had more cases of lacerations and episiotomies but without significant differences. |
| M. Brik et al. (2019) [33] | N = 120 GI = 75 + GC = 45 Healthy PW without contraindications for practice (no guidelines). Gestational Week: 9th Location: Madrid, Spain. | To evaluate the association between physical exercise during pregnancy and maternal gestational weight gain and fetal cardiac function. | Type of Intervention: RCT (CG × IG) Description: Moderate intensity physical exercise intervention. Each session included warm-up, cardiovascular, strength, coordination and balance, pelvic floor and stretching exercises. The intervention was supervised by an exercise specialist. The CG were advised not to attend during pregnancy any supervised exercise program involving exercise for more than 30′ three times per week. However, they were not discouraged from exercising on their own. Intensity Measurement: 55 to 60% of Maximum Heart Rate Time of session: 60 min Frequency: 3x/week Duration: 29 weeks | Primary: GWG, fetal cardiac function parameters. Secondary: Baseline maternal characteristics and labor outcomes. | The physical exercise intervention did not control GWG but increased maternal weight loss after delivery. The physical exercise intervention did not affect fetal cardiac function. |
| Carolina de Vargas Nunes Coll et al. (2019) [12] | N = 639 GI = 75 + GC = 45 Healthy PW without contraindications for practice (ACOG 2015). Gestational Week: 16th/20th Location: Rio Grande, Brazil. | To assess the efficacy of regular exercise during pregnancy in the prevention of postpartum depression. | Type of Intervention: RCT (CG × IG) Description: Moderate intensity physical exercise intervention. Each session included warm-up, aerobic, strength and relaxation exercises. The intensity was managed with the evolution of pregnancy. The intervention was supervised by an exercise specialist. The CG was advised to maintain their usual daily activities. Intensity Measurement: Borg Scale (12–14) Time of session: 60 min Frequency: 3x/week Duration: At least 16 weeks | Primary: Self-reported postpartum depressive symptoms (questionnaire). Secondary: Baseline maternal characteristics. | The study did not show significant differences between groups in postpartum depression. CG presented a higher risk of depression compared with IG. |
| Raquel Rodríguez-Blanque et al. (2019) [34] | N = 140 GI = 70 + GC = 70 Healthy PW without contraindications for practice (ACOG 2015). Gestational Week: 20th Location: Granada, Spain. | To determine the duration of labor in pregnant women who completed a program of moderate physical exercise in water and subsequently presented eutocic birth. | Type of Intervention: RCT (CG × IG) Description: The intervention group had access to moderate physical exercise program in water. The intervention was supervised by an exercise specialist. The CG received usual care and general advice on the benefits of exercise. Both groups received verbal and written dietary advice during pregnancy. Intensity Measurement: Borg Scale or Heart Rate Time of session: 60′ Frequency: 3x/week Duration of Intervention: 17 weeks | Primary: birthweight and duration of 1st, 2nd, and 3rd stages of labor, and the type of labor. Secondary: Baseline maternal characteristics. | The study showed that neonatal birth weight was significantly lower in IG than in CG. The study presented that the 1st and 2nd stages of labor were shorter for PW who performed intervention. The total delivery time for IG was almost 3 h less than in CG. |
| Eman Awad et al. (2019) [35] | N = 60 GI = 30 + GC = 30 Healthy PW without contraindications for practice (ACOG 2002). Gestational Week: 24th Location: Cairo, Egypt. | To determine the effect of an exercise program on the mode of delivery in gestational diabetic females | Type of Intervention: RCT (CG × IG) Description: Moderate intensity physical exercise intervention. Each session included warm-up, aerobic, strength and relaxation exercises. Both groups received the same diet with insulin therapy. Intensity Measurement: Time of session: 60 min Frequency: 3x /week Duration: 12 weeks | Primary: Mode of delivery and Apgar score. Secondary: Baseline maternal characteristics. | The study showed a significant decrease in the number of cesarean deliveries in the IG compared with the CG. The neonates of IG had Apgar score at 1st and 5th minutes after delivery better compared with CG. |
| Ruben Barakat et al. (2017) [5] | N = 65 GI = 33 + GC = 32 Healthy PW without contraindications for practice (ACOG 2015). Gestational Week: 8th/11th Location: Madrid, Spain. | To examine the influence of an aerobic exercise program throughout pregnancy on PW among healthy pregnant women. | Type of Intervention: RCT (CG × IG) Description: Moderate intensity physical exercise intervention. Each session included warm-up, aerobic dance, strength exercises, pelvic floor muscle training, and relaxation exercises. All sessions were supervised by a qualified fitness specialist and with an obstetrician’s assistance. The CG received general advice about the positive effects of physical activity. Intensity Measurement: Borg Scale (12–14) and Heart Rate (55–60% of HRR) Time of session: 55 to 60 min Frequency: 3x/week Duration: 28 weeks. (84 sessions) | Primary: The placental weight was measured during the first 30′ after delivery. Secondary: Gestational age, type of delivery, body weight, Apgar score, GDM, and hypertension. | The study did not present differences between both groups in variables. The study showed that supervised moderate exercise training during pregnancy did not affect negatively placental weight, the overall health status of the newborn, and Apgar score. |
| Now it´s corAlka Pawalia et al. (2017) [36] | N = 36 GI = 12 + GC = 12 Healthy PW without contraindications for practice (ACOG 2015). Gestational Week: 16th Location: Haryana, India. | To investigate the effect of physical activity and diet during the prenatal period and its effect on gestational weight gain (GWG), BMI, waist circumference (WC), hip circumference (HC), and postpartum weight retention (PPWR). | Type of Intervention: RCT (CG × IG x IDG) Description: Moderate intensity physical exercise intervention. Each session included warm-up, pelvic floor and Kegel’s exercises, abdominal and back care exercises, and relaxation and meditation exercises. The IG was asked to do the same exercises at home for at least 3 day/week apart from the supervised session and were also encouraged to walk daily for a minimum duration of 30 min and to do so at least 4 days/week throughout pregnancy. The IDG received timely telephonic messages emphasizing the need for adequate and healthy food choices to be followed during pregnancy. The CG was advised once at recruitment for following proper diet care and explained the importance of being physically active during pregnancy. The intervention was extended to 2 months after delivery. Intensity Measurement: Borg Scale (12–14) Time of session: 60 to 90 min Frequency: 2x/week Duration: 30 weeks | Primary: GWG, BW, fetal waist circumference, hip circumference, waist to hip ratio, and maternal weight retention at postpartum. Secondary: Baseline maternal characteristics. | The study showed birth weight was significantly lower in IG and IDG compared with CG. The IG presented lower values on the waist circumference, which has a direct relation with lifestyle diseases. There were no significant differences in GWG and Maternal weight retention at postpartum between groups. |
| Ruben Barakat et al. (2016) [4] | N = 840 GI = 420 + GC = 420 Healthy PW without contraindications for practice (ACOG 2002). Gestational Week: 9th/11th Location: Madrid, Spain. | To examine the impact of a program of supervised exercise throughout pregnancy on the incidence of pregnancy-induced hypertension. | Type of Intervention: RCT (CG × IG) Description: Moderate intensity physical exercise intervention. Each session included warm-up, strength exercises, and a relaxation phase. The CG received general advice about the positive effects of physical activity. The CG was asked by telephone about their exercise during pregnancy with a questionnaire. If they were active during pregnancy, they were excluded. Intensity Measurement: Borg Scale (12–14) and Heart rate (70% of MHR) Time of session: 50 to 55 min Frequency: 3x/week Duration: 28 weeks | Primary: Number of women who developed hypertension during pregnancy, diastolic and systolic arterial blood pressure (every visit), and BW. Secondary: Baseline maternal characteristics and GWG. | Significantly lower values on the incidence of hypertension in IG. Excessive GWG, gestational diabetes, and preeclampsia was significantly prevented in IG. Physical exercise intervention also reduced the incidence of macrosomia and protected against low-birthweight infants. |
| Yaiza Cordero et al. (2015) [42] | N = 257 GI = 101 + GC = 156 Healthy PW without contraindications for practice (no guidelines). Gestational Week: 10th/12th Location: Madrid, Spain. | To assess the effectiveness of a maternal exercise program (land/aquatic activities, both aerobic and muscular conditioning) in preventing gestational diabetes mellitus (GDM). | Type of Intervention: RCT (CG × IG) Description: Moderate intensity physical exercise intervention in and out of water. Each land session (2x) included activation, physical and psychological preparation, aerobic choreography, strength exercise, pelvic floor muscle training, and stretching. Each water session (1x) included warm-up, core and strength exercises and stretching exercises. Water Temperature: 28.5–29° Intensity Measurement: Borg Scale (12–14) Time of session: 50 to 60 min Frequency: 3x/week Duration: 10–12 weeks to the end of the pregnancy. | Primary: GDM Secondary: Baseline maternal characteristics, GWG, gestational age at delivery, type of delivery, BW, and length. | The study showed that physical exercise intervention was strongly associated with a decrease in GWG, and preserved glucose tolerance. |
3.3. Characteristics of the Interventions
CERT Model
3.4. Maternal and Fetal Physical Activity and Health Outcomes
- Non-fasting lipid profiles, blood samples, serum samples, total cholesterol, HDL, triglycerides [27]
- Gestational Hypertension and Pre-eclampsia [8]
- Resting and Walking systolic and diastolic Blood pressure [4]
- Maternal heart rate recovery [31]
- Pelvic Floor Muscle strength [22]
- Perineal status after birth [32]
- Sleep quality [38]
- Incidence of operative deliveries [18]
3.5. Effectiveness of the Interventions
- Faster maternal heart rate recovery in the intervention group [31]
- The intervention group presented lower weight retention at four and seven months of postpartum [4]
- Physical activity during pregnancy increases weight loss after delivery [33]
- Decreased quality of life was higher in the control group [29].
4. Discussion
4.1. Maternal Weight Gain
4.2. Gestational Diabetes
4.3. Pre-eclampsia and Hypertension
4.4. Depression
4.5. Type and Duration of Delivery
4.6. Quality of Life
4.7. Newborn Weight Gain and Macrosomia
4.8. Apgar Score
4.9. Fetal Heart Rate Recovery
4.10. Pelvic Floor Muscles Training (PFM)
4.11. Level of Physical Activity
4.12. Adherence of Program
4.13. Ratings of Perceived Exertion vs. Heart Rate
4.14. CERT Evaluation
- Few studies present motivation strategies. Conversely, they present a high dropout of participants
- Few studies report a final reflection of the intervention and the fulfillment of the initial planning
- Few studies have controlled the physical activity performed beyond the exercise intervention. Two problems can arise from this limitation: difficulty in evaluating the effectiveness of a program performed at home and the impossibility of evaluating its influence on the progress of pregnancy
- Few studies present the program in detail, reporting intensity monitoring, frequency, duration, and detailed description of the type of exercises, making it difficult to replicate the exercise program in future interventions
- Few studies assess the initial level of participants to adapt the intervention to each pregnant woman
- Few studies clarified the monitoring and evaluation of other components than exercise that can influence the results, such as nutrition.
5. Future Research
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mottola, M.F.; Davenport, M.H.; Ruchat, S.-M.; Davies, G.A.; Poitras, V.; Gray, C.; Garcia, A.J.; Barrowman, N.; Adamo, K.B.; Duggan, M.; et al. Canadian Guideline for Physical Activity throughout Pregnancy—2019. J. Obstet. Gynaecol. Can. 2018, 40, 1528–1537. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists. Physical Activity and Exercise During Pregnancy and the Postpartum Period: ACOG Committee Opinion, Number 804. Obstet. Gynecol. 2020, 135, e178–e188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Ma, G.; Hu, Y.; Yang, Q.; Deavila, J.M.; Zhu, M.J.; Du, M. Effects of Maternal Exercise During Pregnancy on Perinatal Growth and Childhood Obesity Outcomes: A Meta-analysis and Meta-regression. Sports Med. 2021, 51, 2329–2347. [Google Scholar] [CrossRef]
- Barakat, R.; Pelaez, M.; Cordero, Y.; Perales, M.; Lopez, C.; Coteron, J.; Mottola, M.F. Exercise during pregnancy protects against hypertension and macrosomia: Randomized clinical trial. Am. J. Obstet. Gynecol. 2016, 214, 649.e1–649.e8. [Google Scholar] [CrossRef] [PubMed]
- Barakat, R.; Vargas, M.; Brik, M.; Fernandez, I.; GIL Ares, J.; Coteron, J.; Santacruz, B. Does Exercise During Pregnancy Affect Placental Weight?: A Randomized Clinical Trial. Eval. Health Prof. 2017, 41, 400–414. [Google Scholar] [CrossRef] [PubMed]
- Mørkved, S.; Bø, K. Effect of pelvic floor muscle training during pregnancy and after childbirth on prevention and treatment of urinary incontinence: A systematic review. Br. J. Sports Med. 2014, 48, 299–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haakstad, L.A.H.; Edvardsen, E.; Bø, K. Effect of regular exercise on blood pressure in normotensive pregnant women. A randomized controlled trial. Hypertens. Pregnancy 2016, 35, 170–180. [Google Scholar] [CrossRef] [Green Version]
- Evenson, K.R.; Mottola, M.F.; Owe, K.M.; Rousham, E.K.; Brown, W.J. Summary of International Guidelines for Physical Activity After Pregnancy. Obstet. Gynecol. Surv. 2014, 69, 407–414. [Google Scholar] [CrossRef] [Green Version]
- Evenson, K.R.; Mottola, M.F.; Artal, R. Review of Recent Physical Activity Guidelines During Pregnancy to Facilitate Advice by Health Care Providers. Obstet. Gynecol. Surv. 2019, 74, 481–489. [Google Scholar] [CrossRef]
- Santos-Rocha, R. (Ed.) Exercise and Physical Activity during Pregnancy and Postpartum. Evidence-Based Guidelines, 2nd ed.; Springer International Publishing: Cham, Switzerland, 2022. [Google Scholar]
- Campos, M.D.S.B.; Buglia, S.; Colombo, C.S.S.D.S.; Buchler, R.D.D.; de Brito, A.S.X.; Mizzaci, C.C.; Feitosa, R.H.F.; Leite, D.B.; Hossri, C.A.C.; de Albuquerque, L.C.A.; et al. Position Statement on Exercise During Pregnancy and the Post-Partum Period—2021. Arq. Bras. Cardiol. 2021, 117, 160–180. [Google Scholar] [CrossRef]
- Coll, C.D.V.N.; Domingues, M.R.; Stein, A.; Da Silva, B.G.C.; Bassani, D.G.; Hartwig, F.P.; da Silva, I.C.M.; Da Silveira, M.F.; Da Silva, S.G.; Bertoldi, A.D. Efficacy of Regular Exercise During Pregnancy on the Prevention of Postpartum Depression: The PAMELA Randomized Clinical Trial. JAMA Netw. Open 2019, 2, e186861. [Google Scholar] [CrossRef] [PubMed]
- Mullins, E.; Sharma, S.; McGregor, A.H. Postnatal exercise interventions: A systematic review of adherence and effect. BMJ Open 2021, 11, e044567. [Google Scholar] [CrossRef] [PubMed]
- Haakstad, L.A.; Sanda, B.; Vistad, I.; Sagedal, L.R.; Seiler, H.L.; Torstveit, M.K. Evaluation of implementing a community-based exercise intervention during pregnancy. Midwifery 2017, 46, 45–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jorge, C.; Santos-Rocha, R.; Bento, T. Can Group Exercise Programs Improve Health Outcomes in Pregnant Women? A Systematic Review. Curr. Womens Health Rev. 2015, 11, 75–87. [Google Scholar] [CrossRef]
- Slade, S.C.; Dionne, C.E.; Underwood, M.; Buchbinder, R. Consensus on Exercise Reporting Template (CERT): Explanation and Elaboration Statement. Br. J. Sports Med. 2016, 50, 1428–1437. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Blanque, R.; Sánchez-García, J.C.; Sánchez-López, A.M.; Mur-Villar, N.; Fernández-Castillo, R.; Aguilar-Cordero, M.J. Influencia del ejercicio físico durante el embarazo sobre el peso del recién nacido: Un ensayo cliacutenico aleatorizado. Nutr. Hosp. 2017, 34, 834–840. [Google Scholar] [CrossRef] [Green Version]
- Sagedal, L.R.; Øverby, N.C.; Bere, E.; Torstveit, M.K.; Lohne-Seiler, H.; Småstuen, M.; Hillesund, E.R.; Henriksen, T.; Vistad, I. Lifestyle intervention to limit gestational weight gain: The Norwegian Fit for Delivery randomised controlled trial. BJOG Int. J. Obstet. Gynaecol. 2017, 124, 97–109. [Google Scholar] [CrossRef] [Green Version]
- Sagedal, L.R.; Vistad, I.; Øverby, N.C.; Bere, E.; Torstveit, M.K.; Lohne-Seiler, H.; Hillesund, E.R.; Pripp, A.; Henriksen, T. The effect of a prenatal lifestyle intervention on glucose metabolism: Results of the Norwegian Fit for Delivery randomized controlled trial. BMC Pregnancy Childbirth 2017, 17, 167. [Google Scholar] [CrossRef] [Green Version]
- Aguilar-Cordero, M.J.; Sánchez-García, J.C.; Rodriguez-Blanque, R.; Sánchez-López, A.M.; Mur-Villar, N. Moderate Physical Activity in an Aquatic Environment During Pregnancy (SWEP Study) and Its Influence in Preventing Postpartum Depression. J. Am. Psychiatr. Nurses Assoc. 2019, 25, 112–121. [Google Scholar] [CrossRef]
- Vargas-Terrones, M.; Barakat, R.; Santacruz, B.; Fernandez-Buihgas, I.; Mottola, M.F. Physical exercise programme during pregnancy decreases perinatal depression risk: A randomised controlled trial. Br. J. Sports Med. 2019, 53, 348–353. [Google Scholar] [CrossRef]
- Dias, N.T.; Ferreira, L.R.; Fernandes, M.G.; Resende, A.P.M.; Pereira-Baldon, V.S. A Pilates exercise program with pelvic floor muscle contraction: Is it effective for pregnant women? A randomized controlled trial. Neurourol. Urodyn. 2018, 37, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Haakstad, L.A.; Torset, B.; Bø, K. What is the effect of regular group exercise on maternal psychological outcomes and common pregnancy complaints? An assessor blinded RCT. Midwifery 2016, 32, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, M.K.; Stafne, S.N.; Romundstad, P.R.; Mørkved, S.; Salvesen, K.; Helvik, A.-S. The effects of an exercise programme during pregnancy on health-related quality of life in pregnant women: A Norwegian randomised controlled trial. BJOG Int. J. Obstet. Gynaecol. 2016, 123, 1152–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charkamyani, F.; Hosseinkhani, A.; Neisani Samani, L.; Khedmat, L. Reducing the Adverse Maternal and Fetal Outcomes in IVF Women by Exercise Interventions During Pregnancy. Res. Q. Exerc. Sport 2019, 90, 589–599. [Google Scholar] [CrossRef]
- Perales, M.; Santos-Lozano, A.; Sanchis-Gomar, F.; Luaces, M.; Pareja-Galeano, H.; Garatachea, N.; Barakat, R.; Lucia, A. Maternal Cardiac Adaptations to a Physical Exercise Program during Pregnancy. Med. Sci. Sports Exerc. 2016, 48, 896–906. [Google Scholar] [CrossRef]
- Clark, E.; Isler, C.; Strickland, D.; McMillan, A.G.; Fang, X.; Kuehn, D.; Ravisankar, S.; Strom, C.E.; May, L. Influence of aerobic exercise on maternal lipid levels and offspring morphometrics. Int. J. Obes. 2019, 43, 594–602. [Google Scholar] [CrossRef]
- Haakstad, L.A.; Bø, K. The marathon of labour—Does regular exercise training influence course of labour and mode of delivery? Secondary analysis from a randomized controlled trial. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 251, 8–13. [Google Scholar] [CrossRef]
- Rodríguez-Blanque, R.; Aguilar-Cordero, M.J.; Marín-Jiménez, A.E.; Menor-Rodríguez, M.J.; Montiel-Troya, M.; Sánchez-García, J.C. Water Exercise and Quality of Life in Pregnancy: A Randomised Clinical Trial. Int. J. Environ. Res. Public Health 2020, 17, 1288. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Blanque, R.; Aguilar-Cordero, M.J.; Marín-Jiménez, A.E.; Núñez-Negrillo, A.M.; Sánchez-López, A.M.; Sánchez-García, J.C. Influence of a Water-Based Exercise Program in the Rate of Spontaneous Birth: A Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2020, 17, 795. [Google Scholar] [CrossRef] [Green Version]
- Roldan-Reoyo, O.; Pelaez, M.; May, L.; Barakat, R. Influence of maternal physical exercise on fetal and maternal heart rate responses. Ger. J. Exerc. Sport Res. 2019, 49, 446–453. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Blanque, R.; Sanchez-Garcia, J.C.; Sanchez-López, A.M.; Expósito-Ruiz, M.; Aguilar-Cordero, M.J. Randomized Clinical Trial of an Aquatic Physical Exercise Program During Pregnancy. J. Obstet. Gynecol. Neonatal Nurs. 2019, 48, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Brik, M.; Fernández-Buhigas, I.; Martin-Arias, A.; Vargas-Terrones, M.; Barakat, R.; Santacruz, B. Does exercise during pregnancy impact on maternal weight gain and fetal cardiac function? A randomized controlled trial. Ultrasound Obstet. Gynecol. 2019, 53, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Blanque, R.; Sánchez-García, J.C.; Sánchez-López, A.M.; Aguilar-Cordero, M.J. Physical activity during pregnancy and its influence on delivery time: A randomized clinical trial. PeerJ 2019, 7, e6370. [Google Scholar] [CrossRef] [PubMed]
- Awad, E.; Ahmed, H.; Yousef, A.; Saab, I.M. Effect of antenatal exercise on mode of delivery in gestational diabetic females: A single-blind randomized controlled trial. Physiother. Q. 2019, 27, 1–5. [Google Scholar] [CrossRef]
- Pawalia, A.; Kulandaivelan, S.; Savant, S.; Yadav, V.S. Exercise in Pregnancy: Effect on Obesity Parameters in Indian Women —A Randomized Controlled Trial. Rom. J. Diabetes Nutr. Metab. Dis. 2017, 24, 315–323. [Google Scholar] [CrossRef] [Green Version]
- Sanda, B.; Vistad, I.; Sagedal, L.R.; Haakstad, L.A.H.; Lohne-Seiler, H.; Torstveit, M.K. What is the effect of physical activity on duration and mode of delivery? Secondary analysis from the Norwegian Fit for Delivery trial. Acta Obstet. Gynecol. Scand. 2018, 97, 861–871. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Blanque, R.; Sánchez-García, J.C.; Sánchez-López, A.M.; Mur-Villar, N.; Aguilar-Cordero, M. The influence of physical activity in water on sleep quality in pregnant women: A randomised trial. Women Birth 2018, 31, e51–e58. [Google Scholar] [CrossRef]
- Bacchi, M.; Mottola, M.F.; Perales, M.; Refoyo, I.; Barakat, R. Aquatic Activities During Pregnancy Prevent Excessive Maternal Weight Gain and Preserve Birth Weight: A Randomized Clinical Trial. Am. J. Health Promot. 2018, 32, 729–735. [Google Scholar] [CrossRef]
- Barakat, R.; Refoyo, I.; Coteron, J.; Franco, E. Exercise during pregnancy has a preventative effect on excessive maternal weight gain and gestational diabetes. A randomized controlled trial. Braz. J. Phys. Ther. 2019, 23, 148–155. [Google Scholar] [CrossRef]
- Pelaez, M.; Gonzalez-Cerron, S.; Montejo, R.; Barakat, R. Protective Effect of Exercise in Pregnant Women Including Those Who Exceed Weight Gain Recommendations: A Randomized Controlled Trial. Mayo Clin. Proc. 2019, 94, 1951–1959. [Google Scholar] [CrossRef]
- Cordero, Y.; Mottola, M.F.; Vargas, J.; Blanco, M.; Barakat, R. Exercise Is Associated with a Reduction in Gestational Diabetes Mellitus. Med. Sci. Sports Exerc. 2015, 47, 1328–1333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez-García, J.C.; Aguilar-Cordero, M.; Menor-Rodríguez, M.; Paucar Sánchez, A.M.; Rodríguez-Blanque, R. Influencia del ejercicio físico en la evolución del peso gestacional y posparto. Ensayo clínico aleatorizado. Nutr. Hosp. 2019, 36, 931–938. [Google Scholar] [CrossRef] [PubMed]
- ACOG. ACOG Committee on Obstetric Practice Committee opinion—Exercise during pregnancy and the postpartum period. Obstet. Gynecol. 2002, 99, 171–173. [Google Scholar] [CrossRef]
- Jaffe, S. US global health leadership hangs on election result. Lancet 2016, 388, 1969–1970. [Google Scholar] [CrossRef]
- Nascimento, S.L.; Surita, F.G.; Cecatti, J.G. Physical exercise during pregnancy. Curr. Opin. Obstet. Gynecol. 2012, 24, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Bgeginski, R.; Ribeiro, P.A.B.; Mottola, M.F.; Ramos, J.G.L. Effects of weekly supervised exercise or physi-cal activity counseling on fasting blood glucose in women diagnosed with gestational diabetes mellitus: A systematic review and meta-analysis of randomized trials. J. Diabetes 2017, 9, 1023–1032. [Google Scholar] [CrossRef] [PubMed]
- Magro-Malosso, E.R.; Saccone, G.; Di Tommaso, M.; Roman, A.; Berghella, V. Exercise during pregnancy and risk of gestational hypertensive disorders: A systematic review and meta-analysis. Acta Obstet. Gynecol. Scand. 2017, 96, 921–931. [Google Scholar] [CrossRef] [Green Version]
- Davenport, M.H.; Ruchat, S.M.; Poitras, V.J.; Jaramillo Garcia, A.; Gray, C.E.; Barrowman, N.; Skow, R.J.; Meah, V.L.; Riske, L.; Sobierajski, F.; et al. Prenatal exercise for the prevention of gestational diabetes mellitus and hypertensive disorders of pregnancy: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1367–1375. [Google Scholar] [CrossRef]
- Davenport, M.H.; McCurdy, A.P.; Mottola, M.F.; Skow, R.J.; Meah, V.L.; Poitras, V.J.; Jaramillo Garcia, A.; Gray, C.E.; Barrowman, N.; Riske, L.; et al. Impact of prenatal exercise on both prenatal and postnatal anxiety and depressive symptoms: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1376–1385. [Google Scholar] [CrossRef]
- Davenport, M.H.; Marchand, A.-A.; Mottola, M.F.; Poitras, V.J.; Gray, C.E.; Jaramillo Garcia, A.; Barrowman, N.; Sobierajski, F.; James, M.; Meah, V.L.; et al. Exercise for the prevention and treatment of low back, pelvic girdle and lumbopelvic pain during pregnancy: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 53, 90–98. [Google Scholar] [CrossRef] [Green Version]
- Dipietro, L.; Evenson, K.R.; Bloodgood, B.; Sprow, K.; Troiano, R.P.; Piercy, K.L.; Vaux-Bjerke, A.; Powell, K.E.; 2018 Physical Activity Guidelines Advisory Committee. Benefits of Physical Activity during Pregnancy and Postpartum: An Umbrella Review. Med. Sci. Sports Exerc. 2019, 51, 1292–1302. [Google Scholar] [CrossRef] [PubMed]
- Morales-Suárez-Varela, M.; Clemente-Bosch, E.; Peraita-Costa, I.; Llopis-Morales, A.; Martínez, I.; Llopis-González, A. Maternal Physical Activity During Pregnancy and the Effect on the Mother and Newborn: A Systematic Review. J. Phys. Act. Health 2020, 18, 130–147. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Burrueco, J.R.; Cano-Ibáñez, N.; Martín-Peláez, S.; Khan, K.S.; Amezcua-Prieto, C. Effects on the maternal-fetal health outcomes of various physical activity types in healthy pregnant women. A systematic review and meta-analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 262, 203–215. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, M.M.; Andrade, A.; Nunes, I. Physical exercise in pregnancy: Benefits, risks and prescription. J. Périnat. Med. 2021, 50, 4–17. [Google Scholar] [CrossRef]
- Stafne, S.N.; Salvesen, K.Å.; Romundstad, P.R.; Torjusen, I.H.; Mørkved, S. Does regular exercise including pelvic floor muscle training prevent urinary and anal incontinence during pregnancy? A randomised controlled trial. BJOG 2012, 119, 1270–1280. [Google Scholar] [CrossRef]
- Ruiz, J.R.; Perales, M.; Pelaez, M.; Lopez, C.; Lucia, A.; Barakat, R. Supervised Exercise—Based Intervention to Prevent Excessive Gestational Weight Gain: A Randomized Controlled Trial. Mayo Clin. Proc. 2013, 88, 1388–1397. [Google Scholar] [CrossRef]
- Sagedal, L.R.; Sanda, B.; Øverby, N.C.; Bere, E.; Torstveit, M.K.; Lohne-Seiler, H.; Hillesund, E.R.; Pripp, A.H.; Henriksen, T.; Vistad, I. The effect of prenatal lifestyle intervention on weight retention 12 months postpartum: Results of the Norwegian Fit for Delivery randomised controlled trial. BJOG 2016, 124, 111–121. [Google Scholar] [CrossRef] [Green Version]
- Di Lorito, C.; Long, A.; Byrne, A.; Harwood, R.H.; Gladman, J.R.F.; Schneider, S.; Logan, P.; Bosco, A.; van der Wardt, V. Exercise interventions for older adults: A systematic review of meta-analyses. J. Sport Health Sci. 2021, 10, 29–47. [Google Scholar] [CrossRef]
- Voerman, E.; Santos, S.; Inskip, H.; Amiano, P.; Barros, H.; Charles, M.A.; Chatzi, L.; Chrousos, G.P.; Corpeleijn, E.; Crozier, S.; et al. Association of Gestational Weight Gain With Adverse Maternal and Infant Outcomes. JAMA 2019, 321, 1702–1715. [Google Scholar] [CrossRef] [Green Version]
- Peggie, L. Williamson. Exercise for Special Populations, 2nd ed.; Wolters Kluwer: Killeen, TX, USA, 2019. [Google Scholar]
- Spaight, C.; Gross, J.; Horsch, A.; Puder, J.J. Gestational Diabetes Mellitus. Endocr Dev. 2016, 31, 163–178. [Google Scholar] [CrossRef]
- Gregg, V.H.; Ferguson, J.E. Exercise in Pregnancy. Clin. Sports Med. 2017, 36, 741–752. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.H.; Ruchat, S.-M.; Sobierajski, F.; Poitras, V.J.; Gray, C.E.; Yoo, C.; Skow, R.J.; Jaramillo; Garcia, A.; Barrowman, N.; et al. Impact of prenatal exercise on maternal harms, labour and delivery outcomes: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 53, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, D.P.; Hillier, V.F. A scaled version of the General Health Questionnaire. Psychol. Med. 1979, 9, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Jenkinson, C.; Coulter, A.; Wright, L. Short form 36 (SF 36) health survey questionnaire: Normative data for adults of working age. Br. Med. J. 1993, 306, 1437–1440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundgren-Nilsson, Å.; Jonsdottir, I.H.; Ahlborg, G.; Tennant, A. Construct validity of the psychological general well being index (PGWBI) in a sample of patients undergoing treatment for stress-related exhaustion: A rasch analysis. Health Qual. Life Outcomes 2013, 11, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davenport, M.H.; Meah, V.L.; Ruchat, S.M.; Davies, G.A.; Skow, R.J.; Barrowman, N.; Adamo, K.B.; Poitras, V.J.; Gray, C.E.; Jaramillo Garcia, A.; et al. Impact of prenatal exercise on neonatal and childhood outcomes: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1386–1396. [Google Scholar] [CrossRef] [PubMed]
- Watterberg, K.L.; Aucott, S.; Benitz, W.E.; Cummings, J.J.; Eichenwald, E.C.; Goldsmith, J.; Poindexter, B.B.; Puopolo, K.; Stewart, D.L.; Wang, K.S.; et al. The Apgar Score. Am. Acad. Pediatr. 2015, 136, 819–822. [Google Scholar] [CrossRef] [Green Version]
- Pires, T.F.; Pires, P.M.; Costa, R.; Viana, R. Effects of pelvic floor muscle training in pregnant women. Porto Biomed. J. 2020, 5, e077. [Google Scholar] [CrossRef]
- Woodley, S.J.; Lawrenson, P.; Boyle, R.; Cody, J.D.; Mørkved, S.; Kernohan, A.; Hay-Smith, E.J.C. Pelvic floor muscle training for preventing and treating urinary and faecal incontinence in antenatal and postnatal women. Cochrane Database Syst. Rev. 2020, 2021, CD007471. [Google Scholar] [CrossRef]
- Cai, C.; Ruchat, S.-M.; Sivak, A.; Davenport, M.H. Prenatal Exercise and Cardiorespiratory Health and Fitness: A Meta-analysis. Med. Sci. Sports Exerc. 2020, 52, 1538–1548. [Google Scholar] [CrossRef]
- Thompson, W.R. Worldwide Survey of Fitness Trends for 2022. ACSM’S Health Fit. J. 2022, 26, 11–20. [Google Scholar] [CrossRef]
- Zheng, Y.D.; Li, H.; Gao, K.; Gallo, P.M. Developing a Home-Based Body Weight Physical Activity/Exercise Program. ACSM’s Health Fit. J. 2022, 26, 20–28. [Google Scholar] [CrossRef]
- Chan, C.W.H.; Au Yeung, E.; Law, B.M.H. Effectiveness of Physical Activity Interventions on Pregnancy-Related Outcomes among Pregnant Women: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 1840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Möhler, R.; Köpke, S.; Meyer, G. Criteria for Reporting the Development and Evaluation of Complex Interventions in healthcare: Revised guideline (CReDECI 2). Trials 2015, 16, 204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| Authors | Total | Authors | Total | Authors | Total |
|---|---|---|---|---|---|
| Sánchez-García, J. (2019) [43] | 14 | Dias, N. (2017) [22] | 7 | Blanque, R. (2019) [32] | 15 |
| Cordero, R. (2017) [17] | 14 | Haakstad, L. (2015) [23] | 8 | Brik, M. (2018) [33] | 5 |
| Bacchi, M. (2017) [39] | 8 | Gustafsson, M.K. (2015) [24] | 10 | Coll, C. (2019) [12] | 10 |
| Haakstad, L. (2016) [4] | 9 | Charkamyani, F. (2019) [25] | 5 | Blanque, R. (2019) [34] | 13 |
| Sagedal, L.R. (2017) [18] | 10 | Perales, M. (2015) [26] | 9 | Awad, E. (2019) [35] | 10 |
| Sagedal, L.R. (2017) [19] | 10 | Palaez, M. (2019) [41] | 8 | Barakat, R. (2017) [5] | 9 |
| A-Cordero, M. (2018) [20] | 15 | Clark, E. (2019) [27] | 8 | Pawalia, A. (2017) [36] | 7 |
| Barakat, R. (2018) [40] | 9 | Haakstad, L. 2020) [28] | 7 | Barakat, R. (2016) [4] | 9 |
| Sanda, B. (2018) [37] | 6 | Blanque, R. (2020) [29] | 15 | Cordero, Y. (2015) [42] | 9 |
| Terrones, M. (2018) [21] | 11 | Blanque, R. (2020) [30] | 15 | ||
| Blanque, R. (2017) [38] | 14 | Reoyo, O. (2019) [31] | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Castro, R.; Antunes, R.; Mendes, D.; Szumilewicz, A.; Santos-Rocha, R. Can Group Exercise Programs Improve Health Outcomes in Pregnant Women? An Updated Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 4875. https://doi.org/10.3390/ijerph19084875
de Castro R, Antunes R, Mendes D, Szumilewicz A, Santos-Rocha R. Can Group Exercise Programs Improve Health Outcomes in Pregnant Women? An Updated Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(8):4875. https://doi.org/10.3390/ijerph19084875
Chicago/Turabian Stylede Castro, Rebeca, Raul Antunes, Diogo Mendes, Anna Szumilewicz, and Rita Santos-Rocha. 2022. "Can Group Exercise Programs Improve Health Outcomes in Pregnant Women? An Updated Systematic Review" International Journal of Environmental Research and Public Health 19, no. 8: 4875. https://doi.org/10.3390/ijerph19084875
APA Stylede Castro, R., Antunes, R., Mendes, D., Szumilewicz, A., & Santos-Rocha, R. (2022). Can Group Exercise Programs Improve Health Outcomes in Pregnant Women? An Updated Systematic Review. International Journal of Environmental Research and Public Health, 19(8), 4875. https://doi.org/10.3390/ijerph19084875