
Effectiveness of Mantra-Based Meditation on Mental Health: A Systematic Review and Meta-Analysis

 , , , , ,
, , , , ,  , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search and Study Selection
2.2. Inclusion Criteria
2.3. Data Extraction and Assessment of Methodological Quality
2.4. Analysis
3. Results
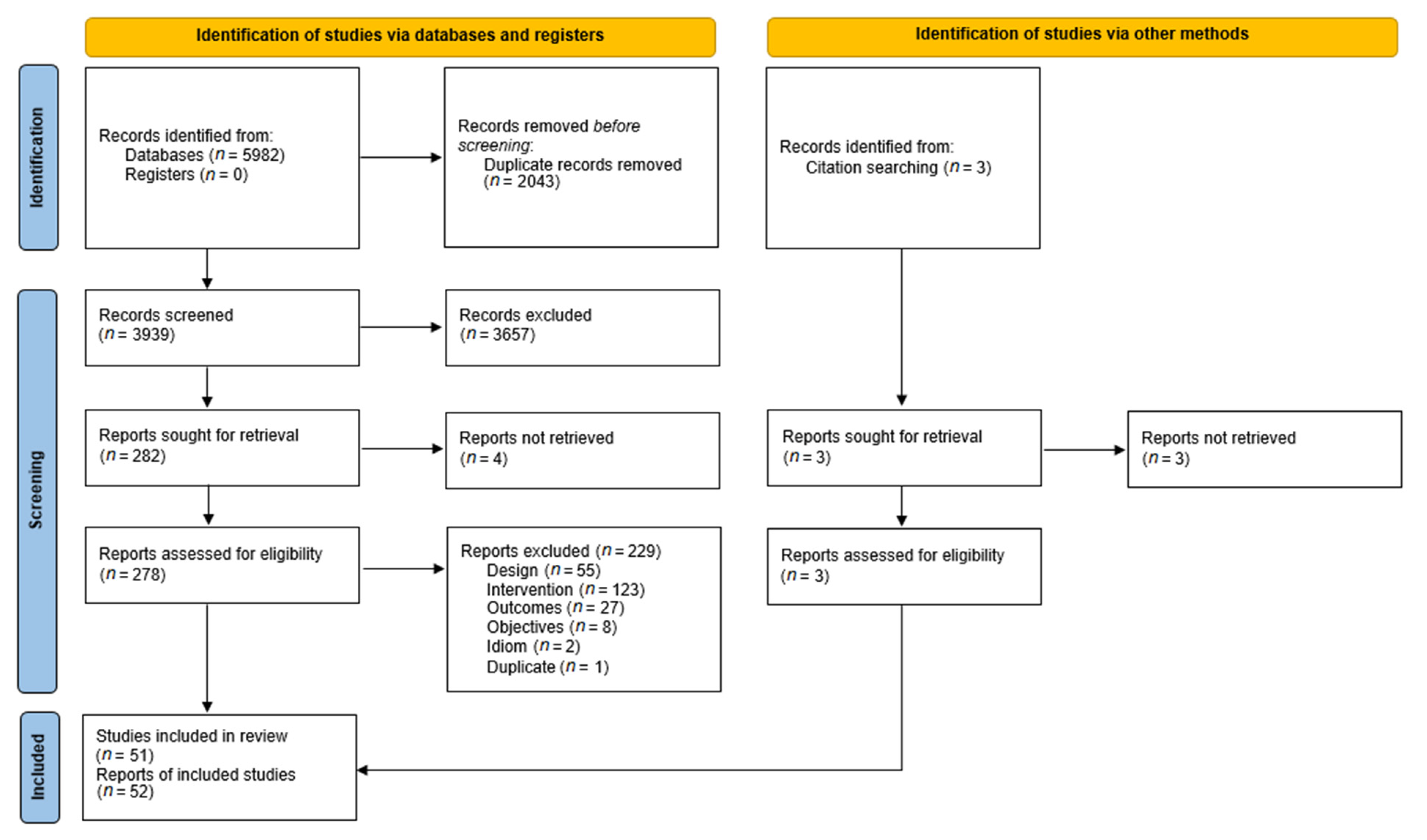
3.1. Results of the Search
3.2. Characteristics of Included Studies
3.3. Methodological Quality
3.4. Effects of the Intervention
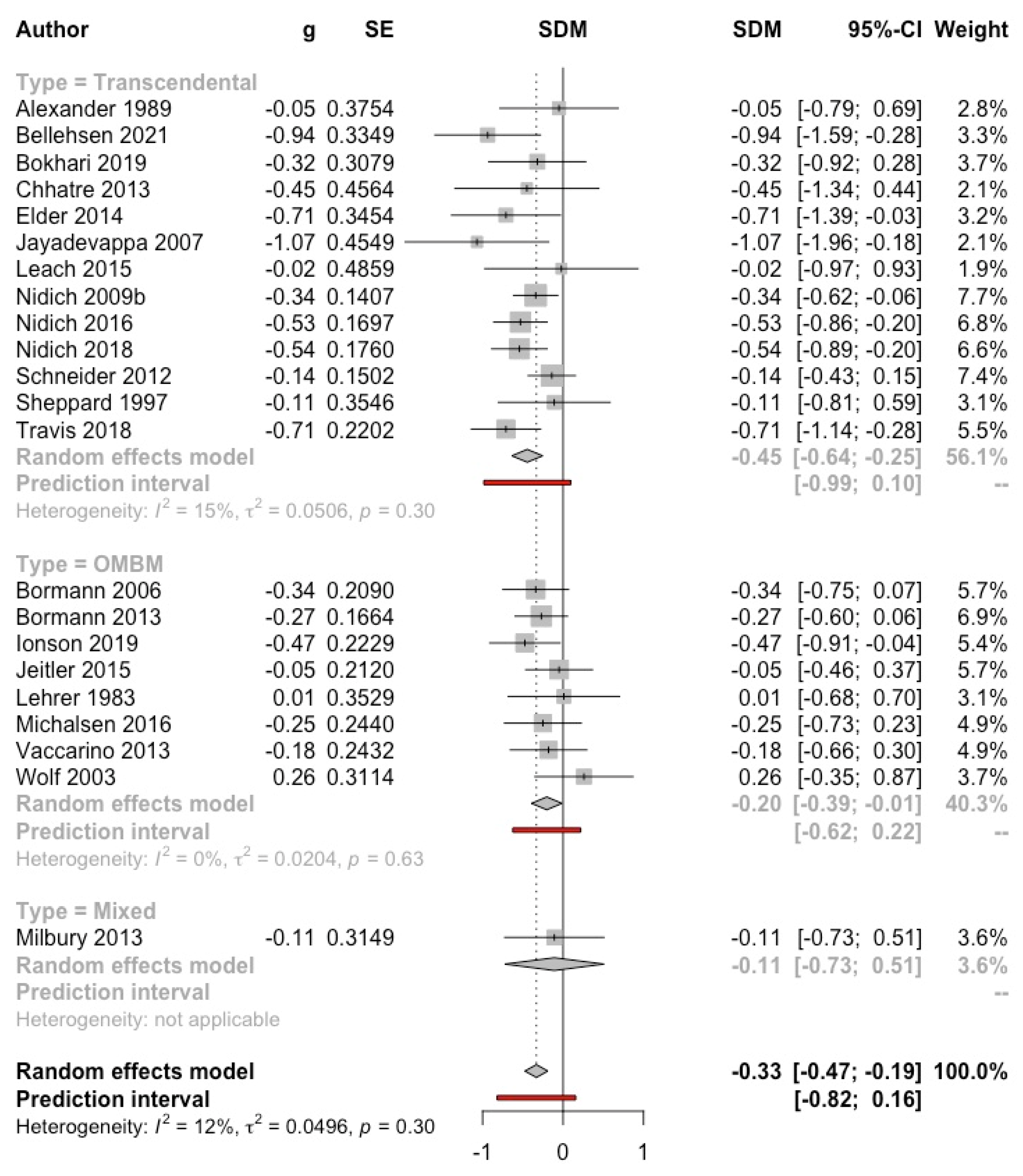
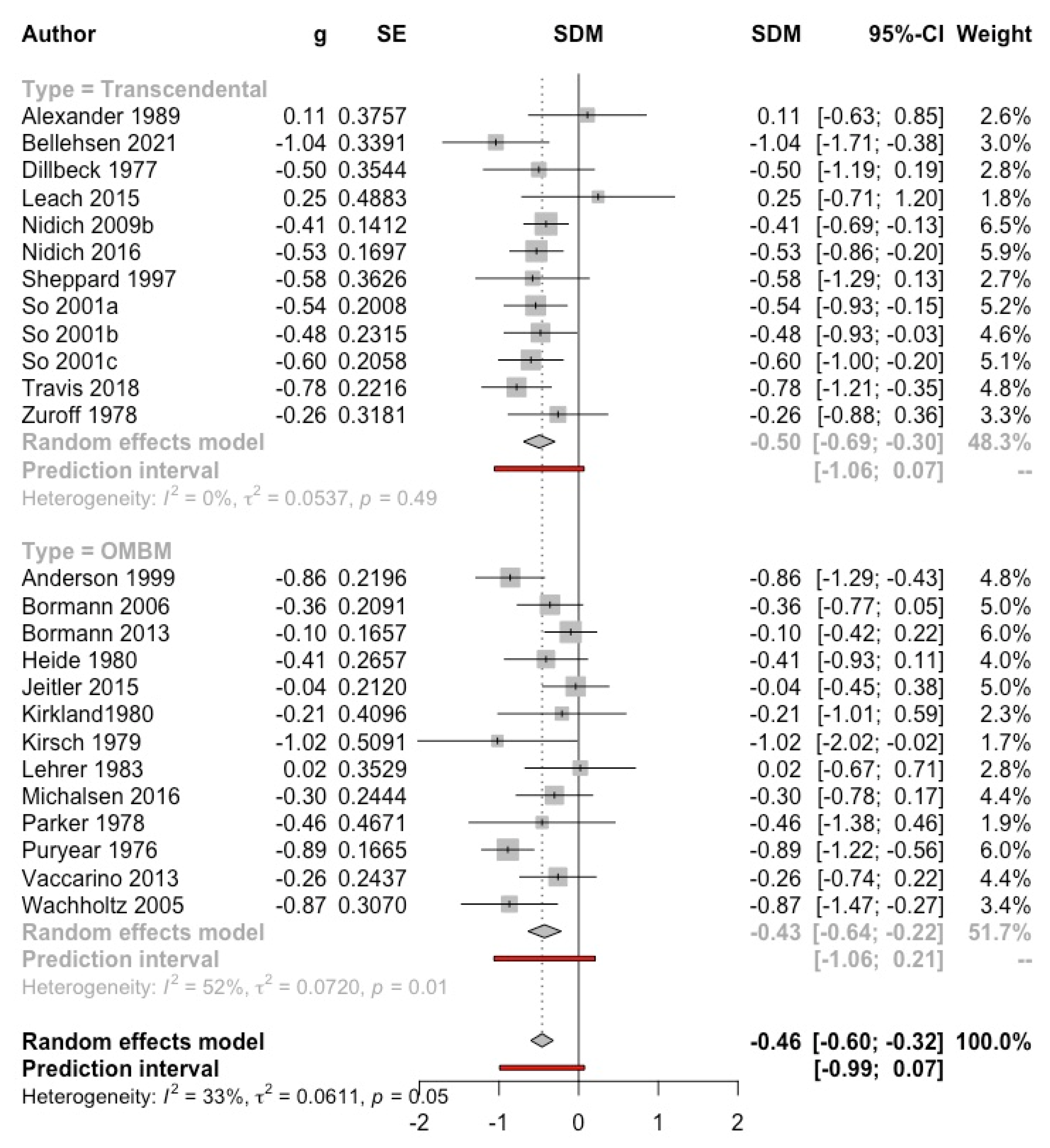
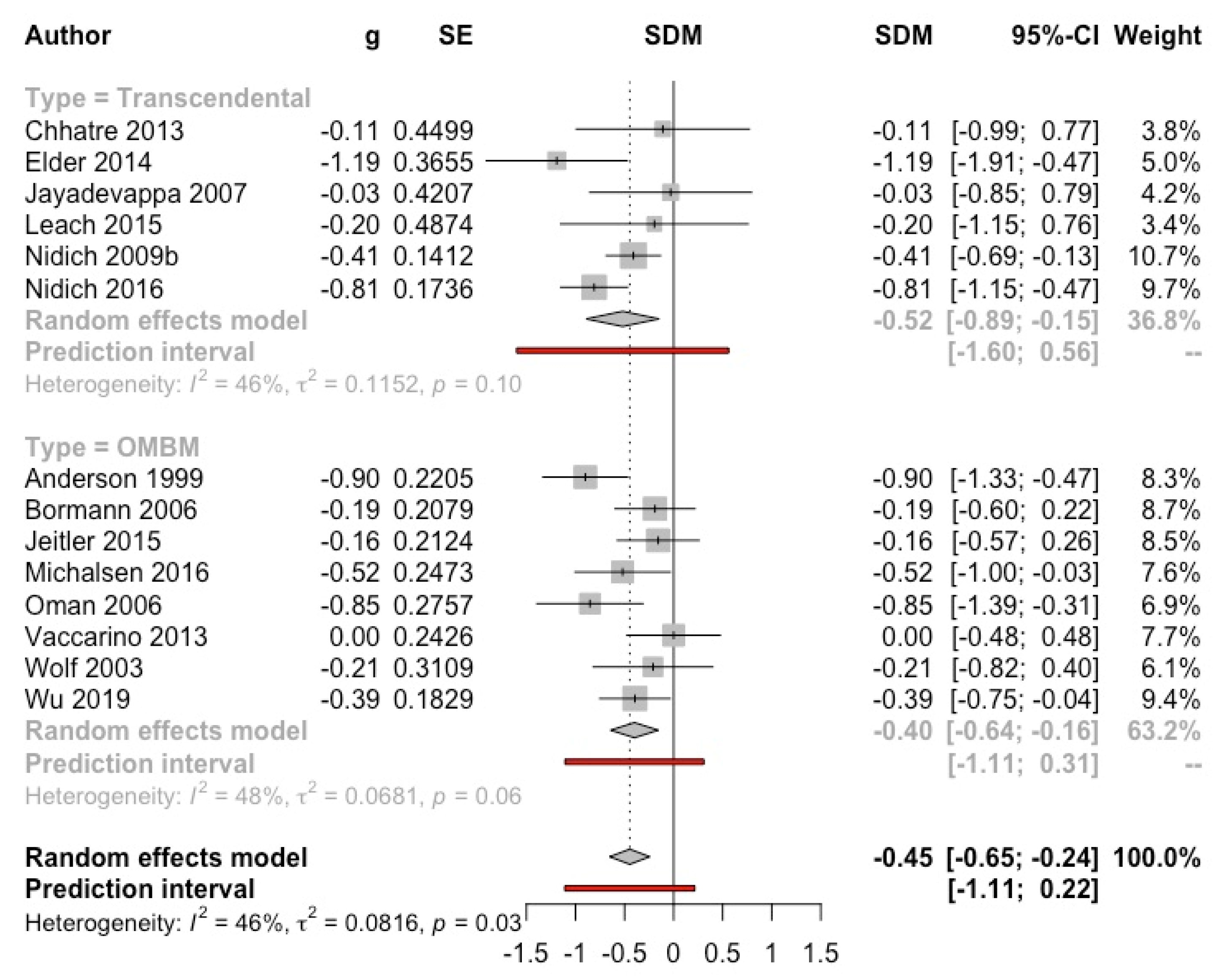
3.4.1. Anxiety
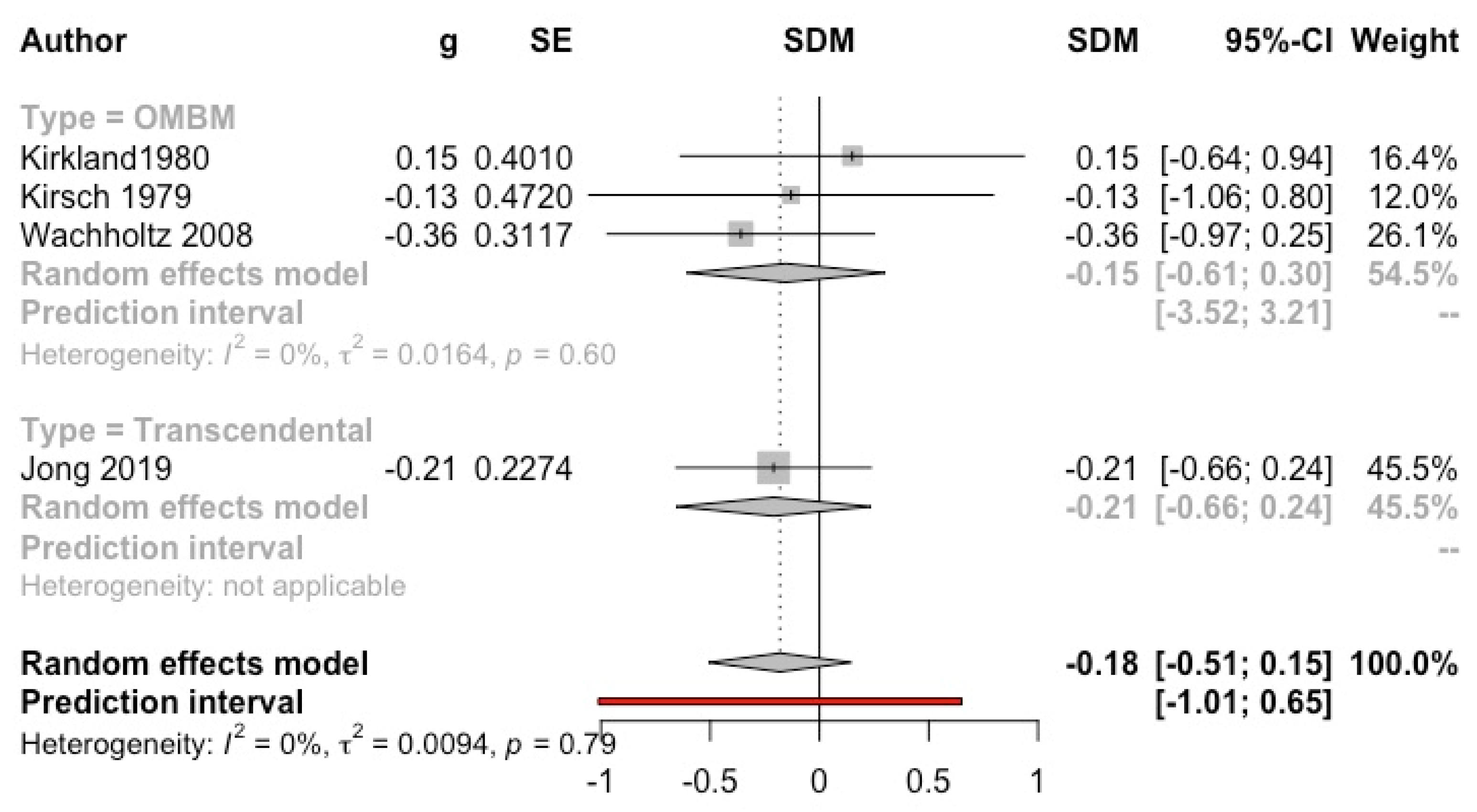
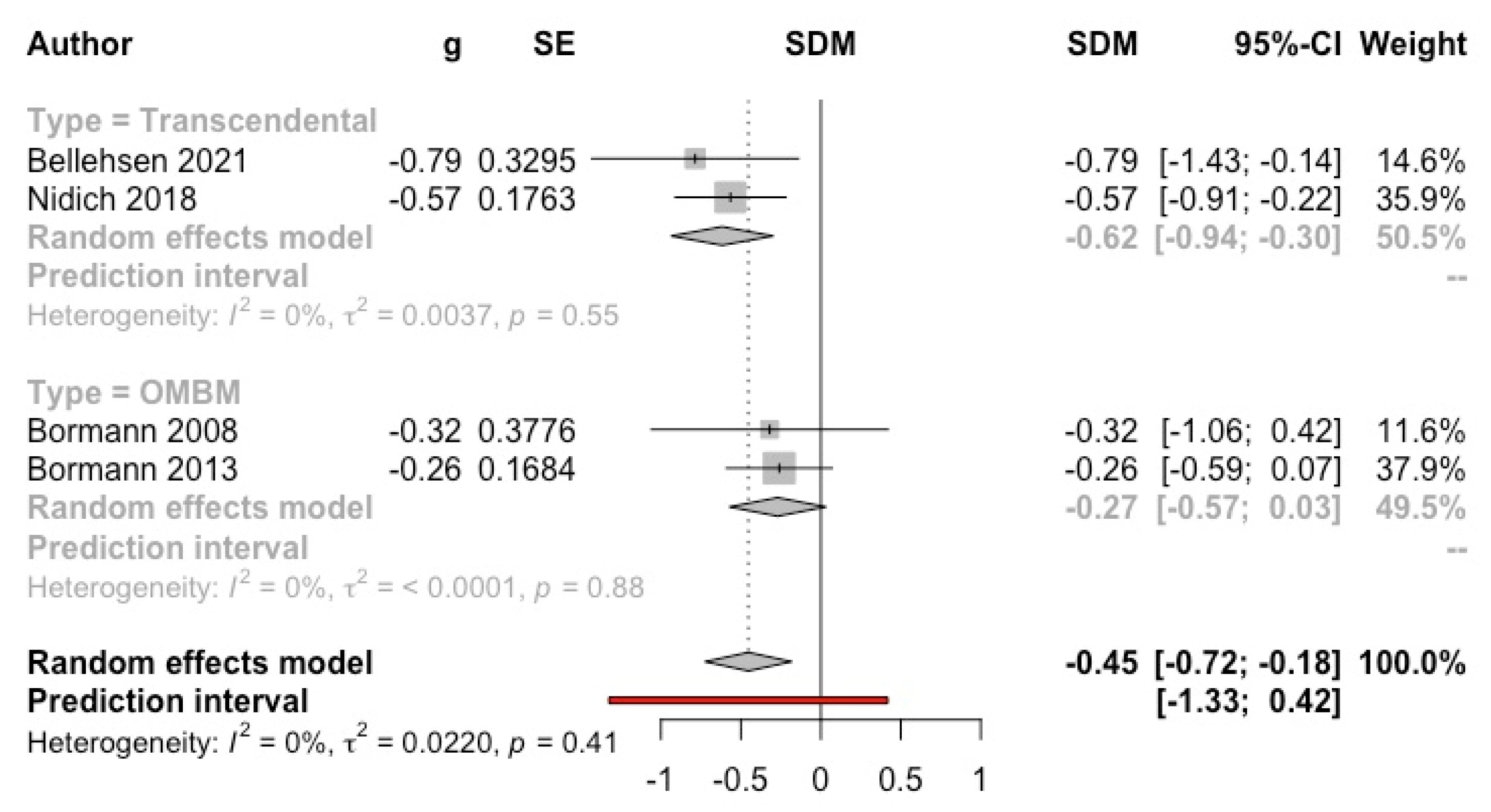
3.4.2. Depression
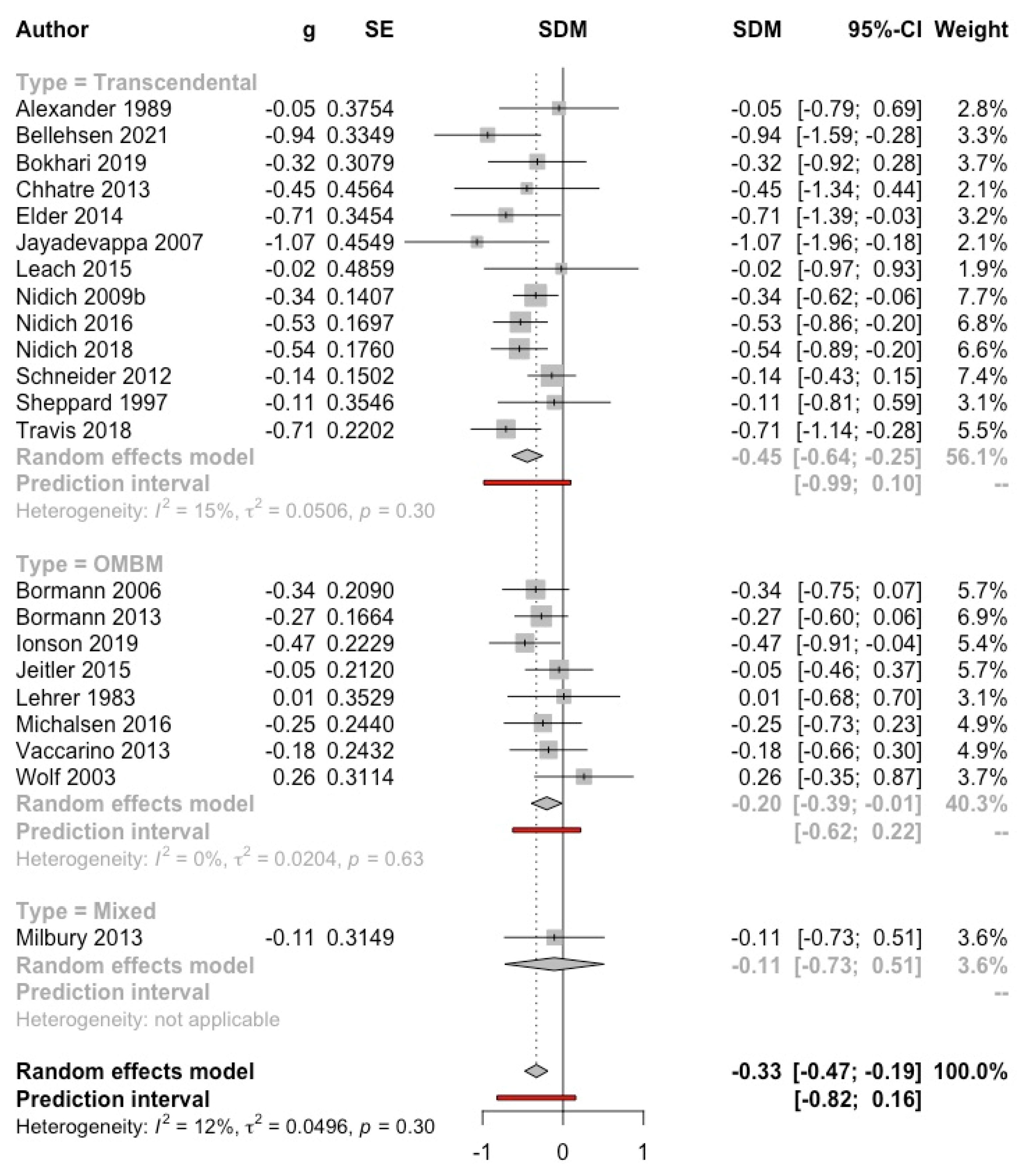
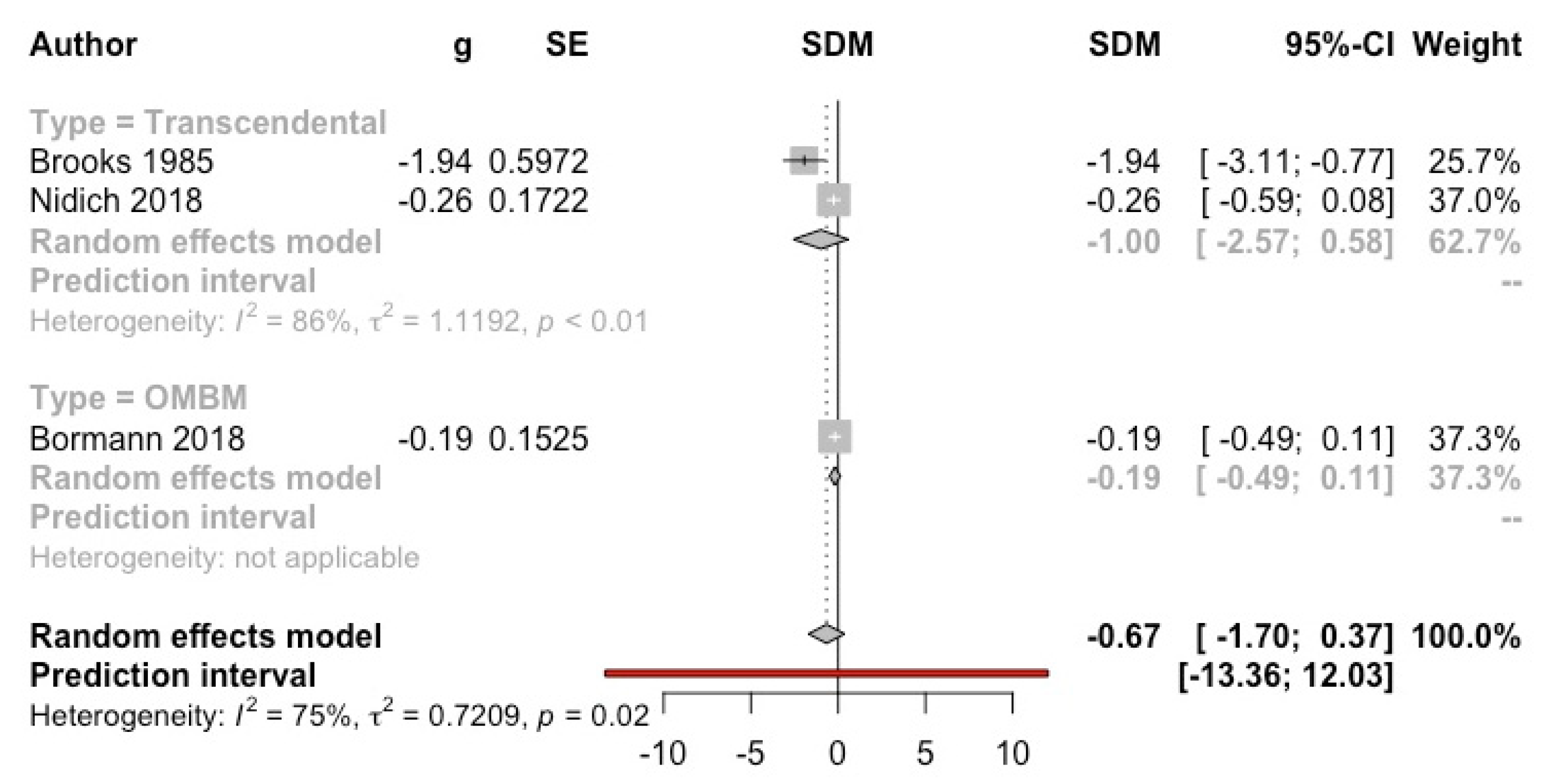
3.4.3. Stress
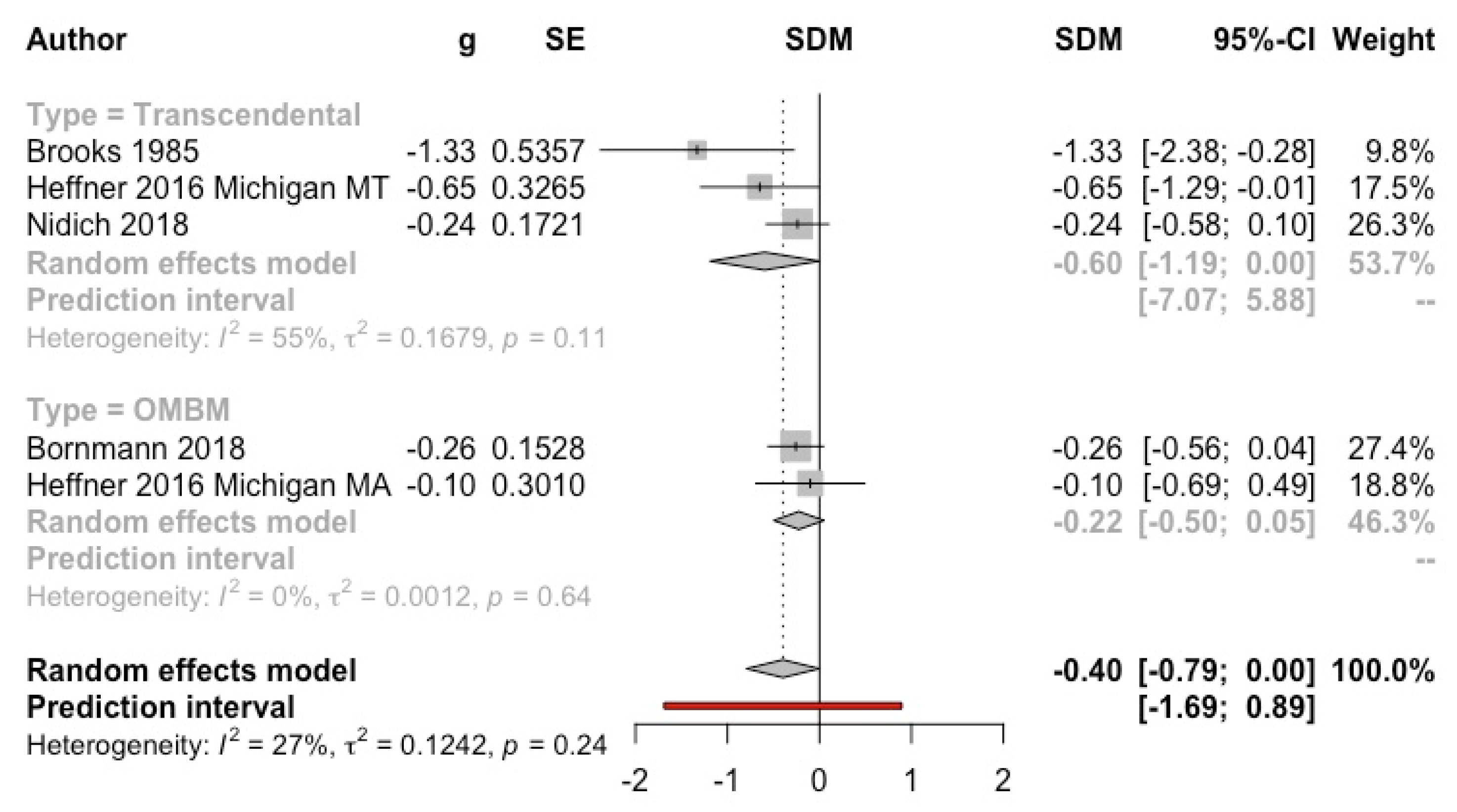
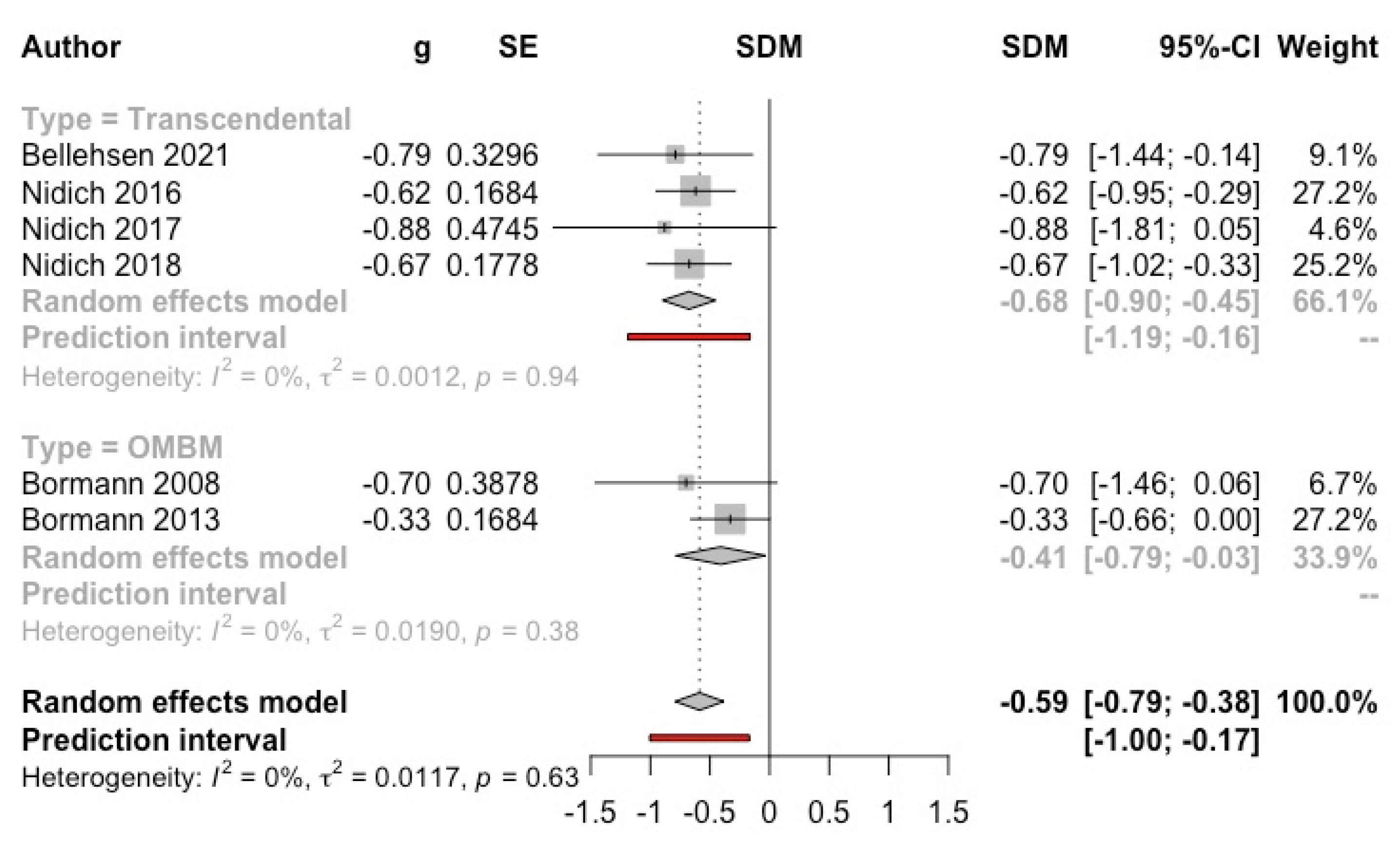
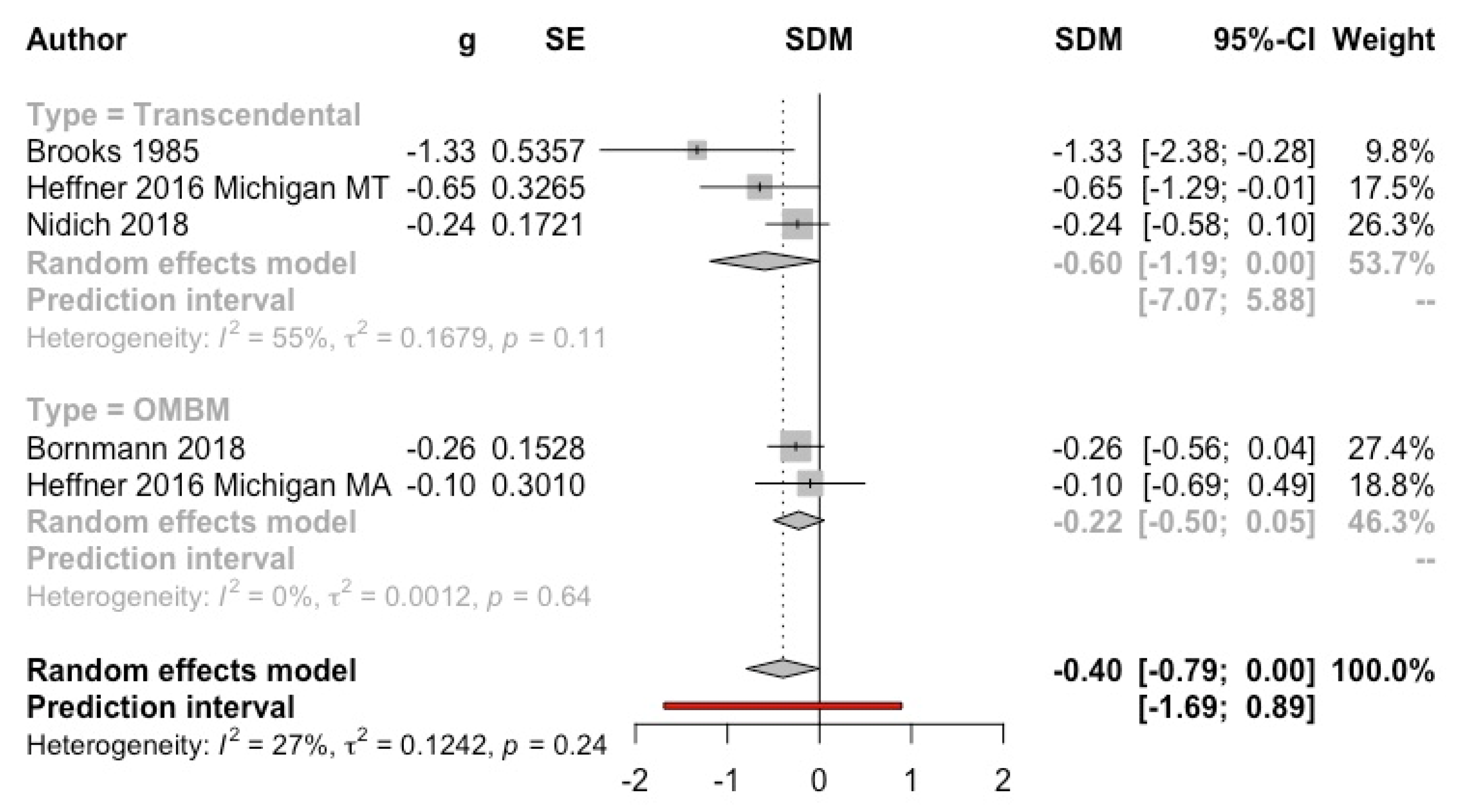
3.4.4. Post-Traumatic Stress Disorders’ Symptoms
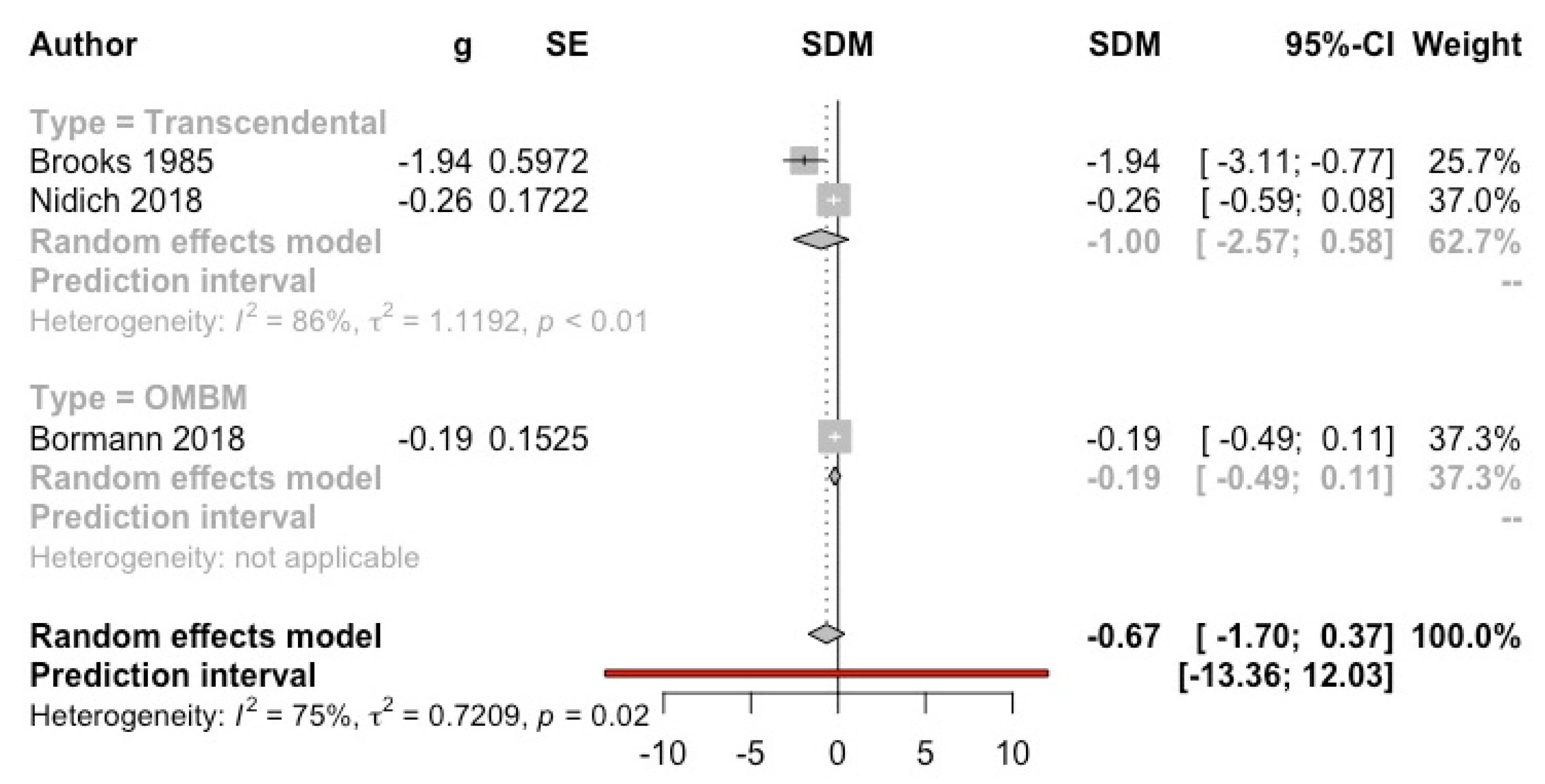
3.4.5. Burnout
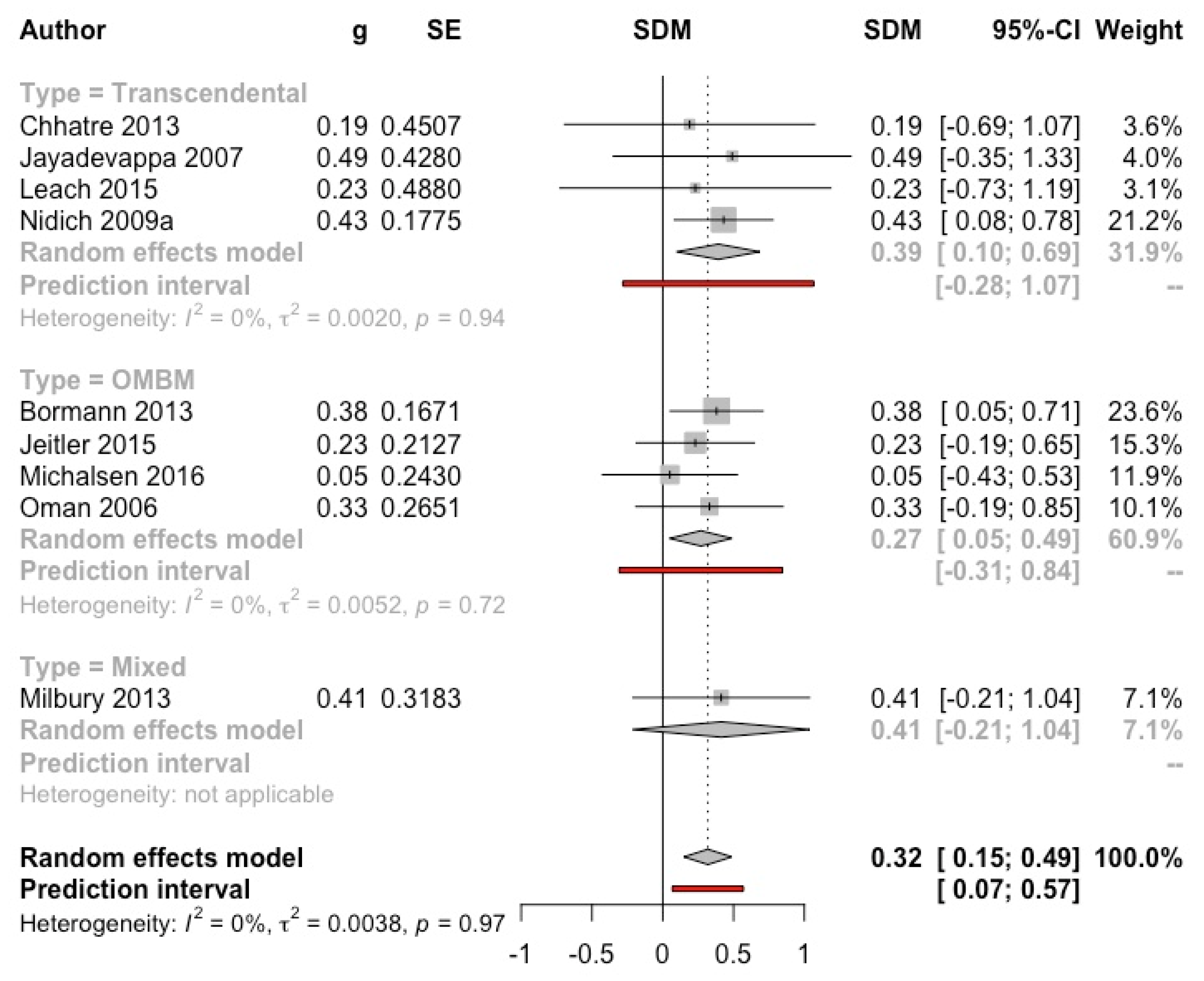
3.4.6. Mental Health-Related Quality of Life
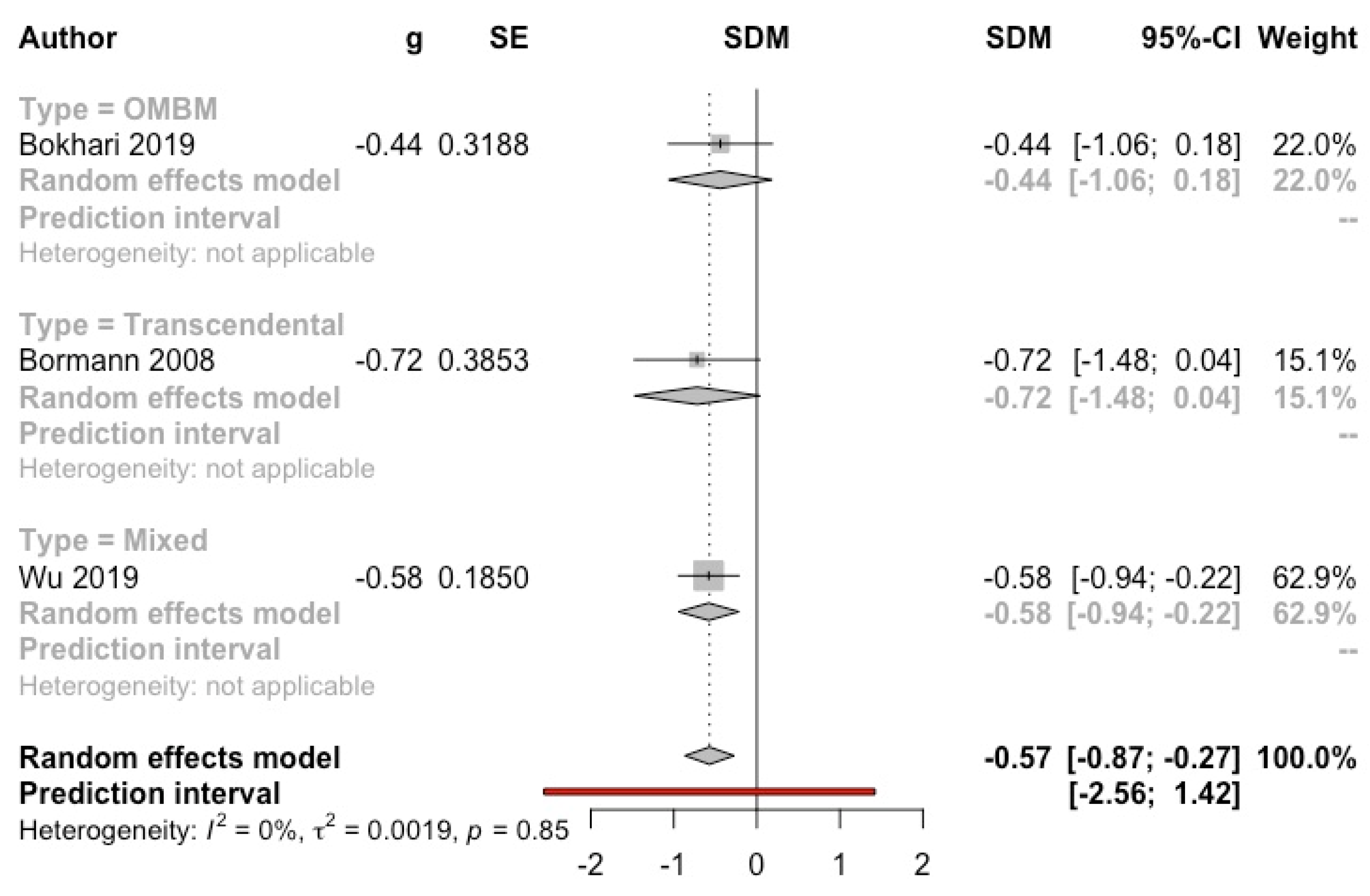
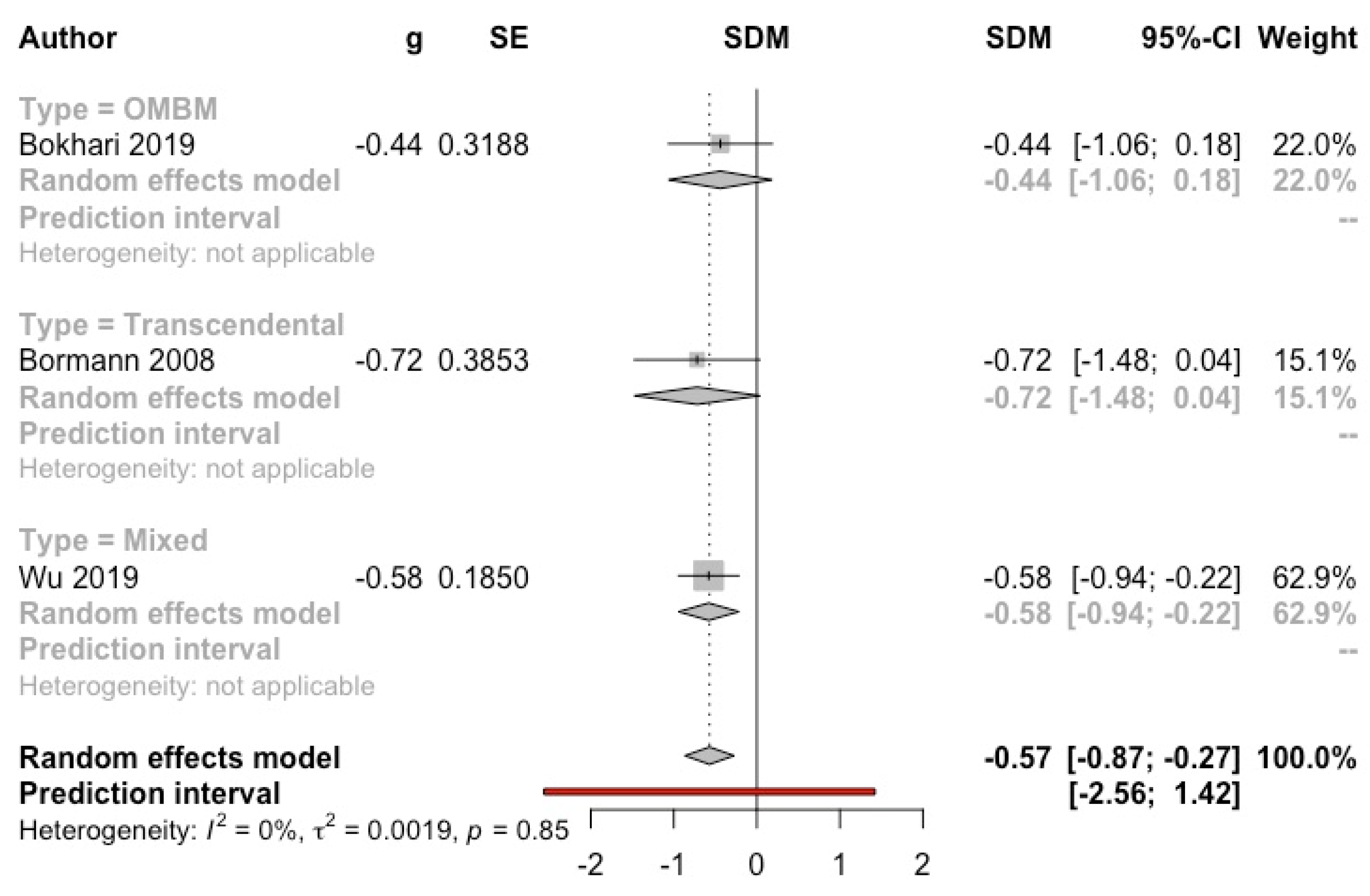
3.4.7. Sleep Quality
3.4.8. General Psychopathology
3.4.9. Substance Consumption
3.5. Safety
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rose, S.; Zell, E.; Strickhouser, J.E. The Effect of Meditation on Health: A Metasynthesis of Randomized Controlled Trials. Mindfulness 2020, 11, 507–516. [Google Scholar] [CrossRef]
- Tang, Y.-Y.; Hölzel, B.K.; Posner, M.I. The neuroscience of mindfulness meditation. Nat. Rev. Neurosci. 2015, 16, 312. [Google Scholar] [CrossRef]
- Walsh, R. Meditación. Nat. Medicat. 1996, 43, 16–22. [Google Scholar]
- Cahn, B.R.; Polich, J. Meditation (Vipassana) and the P3a event-related brain potential. Int. J. Psychophysiol. 2009, 72, 51–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shapiro, D.J. Overview: Clinical and physiological comparison of meditation with other self-control strategies. Am. J. Psychiatry 1982, 139, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.W.; Cohen, M. A Methodological Review of Meditation Research. Front. Psychiatry 2014, 5, 74. [Google Scholar] [CrossRef] [Green Version]
- Lynch, J.; Prihodova, L.; Dunne, P.J.; Carroll, Á.; Walsh, C.; McMahon, G.; White, B. Mantra meditation for mental health in the general population: A systematic review. Eur. J. Integr. Med. 2018, 23, 101–108. [Google Scholar] [CrossRef]
- Travis, F. Transcendental experiences during meditation practice. Ann. N. Y. Acad. Sci. 2014, 1307, 1–8. [Google Scholar] [CrossRef]
- Forem, J. Transcedental Meditation: The Essential Teachings of Maharishi Mahesh Yogi; Hay House: New York, NY, USA, 2012. [Google Scholar]
- Orme-Johnson, D.W.; Barnes, V.A. Effects of the Transcendental Meditation Technique on Trait Anxiety: A Meta-Analysis of Randomized Controlled Trials. J. Altern. Complementary Med. 2014, 20, 330–341. [Google Scholar] [CrossRef]
- Gathright, E.C.; Salmoirago-Blotcher, E.; DeCosta, J.; Balletto, B.L.; Donahue, M.L.; Feulner, M.M.; Cruess, D.G.; Wing, R.R.; Carey, M.P.; Scott-Sheldon, L.A.J. The impact of transcendental meditation on depressive symptoms and blood pressure in adults with cardiovascular disease: A systematic review and meta-analysis. Complementary Ther. Med. 2019, 46, 172–179. [Google Scholar] [CrossRef]
- Dunne, P.J.; Lynch, J.; Prihodova, L.; O’Leary, C.; Ghoreyshi, A.; Basdeo, S.A.; Cox, D.J.; Breen, R.; Sheikhi, A.; Carroll, Á.; et al. Burnout in the emergency department: Randomized controlled trial of an attention-based training program. J. Integr. Med. 2019, 17, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Bokhari, S.; Schneider, R.H.; Salerno, J.W.; Rainforth, M.V.; Gaylord-King, C.; Nidich, S.I. Effects of cardiac rehabilitation with and without meditation on myocardial blood flow using quantitative positron emission tomography: A pilot study. J. Nucl. Cardiol. 2021, 28, 1596–1607. [Google Scholar] [CrossRef] [PubMed]
- Nidich, S.; Mills, P.J.; Rainforth, M.; Heppner, P.; Schneider, R.H.; Rosenthal, N.E.; Salerno, J.; Gaylord-King, C.; Rutledge, T. Non-trauma-focused meditation versus exposure therapy in veterans with post-traumatic stress disorder: A randomised controlled trial. Lancet Psychiatry 2018, 5, 975–986. [Google Scholar] [CrossRef]
- Bormann, J.E.; Thorp, S.R.; Smith, E.; Glickman, M.; Beck, D.; Plumb, D.; Zhao, S.; Ackland, P.E.; Rodgers, C.S.; Heppner, P.; et al. Individual treatment of posttraumatic stress disorder using mantram repetition: A randomized clinical trial. Am. J. Psychiatry 2018, 175, 979–988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farias, M.; Maraldi, E.; Wallenkampf, K.C.; Lucchetti, G. Adverse events in meditation practices and meditation-based therapies: A systematic review. Acta Psychiatr. Scand. 2020, 142, 374–393. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [Updated March 2011]; The Cochrane Collaboration: 2011. Available online: https://training.cochrane.org/es/manual-cochrane-de-revisiones-sistem%C3%A1ticas-de-intervenciones (accessed on 24 January 2022).
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Evid.-Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Viechtbauer, W. Conducting Meta-Analyses in R with the metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef] [Green Version]
- Harrer, M.; Cuijpers, P.; Furukawa, T.; Ebert, D.D. Dmetar: Companion R Package for the Guide “Doing Meta-Analysis in R”, R Package Version 0.0.9000. Available online: http://dmetar.protectlab.org/ (accessed on 24 January 2022).
- Sidik, K.; Jonkman, J.N. Simple heterogeneity variance estimation for meta-analysis. J. R. Stat. Soc. Ser. C 2005, 54, 367–384. [Google Scholar] [CrossRef]
- Deeks, J.J.; Altman, D.G.; Bradburn, M.J. Statistical Methods for Examining Heterogeneity and Combining Results from Several Studies in Meta-Analysis. In Systematic Reviews in Health Care; BMJ Publishing Group: London, UK, 2001; pp. 285–312. [Google Scholar]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- So, K.T.; Orme-Johnson, D.W. Three randomized experiments on the longitudinal effects of the Transcedental Meditation technique on cognition. Intelligence 2001, 29, 419–440. [Google Scholar] [CrossRef]
- Alexander, C.N.; Langer, E.J.; Newman, R.I.; Chandler, H.M.; Davies, J.L. Transcendental meditation, mindfulness, and longevity: An experimental study with the elderly. J. Personal. Soc. Psychol. 1989, 57, 950–964. [Google Scholar] [CrossRef]
- Bellehsen, M.; Stoycheva, V.; Cohen, B.H.; Nidich, S. A Pilot Randomized Controlled Trial of Transcendental Meditation as Treatment for Posttraumatic Stress Disorder in Veterans. J. Trauma. Stress 2022, 35, 22–31. [Google Scholar] [CrossRef]
- Dillbeck, M.C. The effect of the transcendental meditation technique on anxiety level. J. Clin. Psychol. 1977, 33, 1076–1078. [Google Scholar] [CrossRef]
- Leach, M.J.; Francis, A.; Ziaian, T. Transcendental Meditation for the improvement of health and wellbeing in community-dwelling dementia caregivers [TRANSCENDENT]: A randomised wait-list controlled trial. BMC Complementary Altern. Med. 2015, 15, 145. [Google Scholar] [CrossRef] [Green Version]
- Nidich, S.I.; Rainforth, M.V.; Haaga, D.A.F.; Hagelin, J.; Salerno, J.W.; Travis, F.; Tanner, M.; Gaylord-King, C.; Grosswald, S.; Schneider, R.H. A randomized controlled trial on effects of the transcendental meditation program on blood pressure, psychological distress, and coping in young adults. Am. J. Hypertens. 2009, 22, 1326–1331. [Google Scholar] [CrossRef]
- Nidich, S.; O’connor, T.; Rutledge, T.; Duncan, J.; Compton, B.; Seng, A.; Nidich, R. Reduced Trauma Symptoms and Perceived Stress in Male Prison Inmates through the Transcendental Meditation Program: A Randomized Controlled Trial. Perm. J. 2016, 20, 43–47. [Google Scholar] [CrossRef] [Green Version]
- Sheppard, W.D.; Staggers, F.J.; John, L. The effects of a stress management program in a high security government agency. Anxiety Stress Coping 1997, 10, 341–350. [Google Scholar] [CrossRef]
- Travis, F.; Valosek, L.; Konrad, A.; Link, J.; Salerno, J.; Scheller, R.; Nidich, S. Effect of meditation on psychological distress and brain functioning: A randomized controlled study. Brain Cogn. 2018, 125, 100–105. [Google Scholar] [CrossRef]
- Zuroff, D.C.; Schwarz, J.C. Effects of transcendental meditation and muscle relaxation on trait anxiety, maladjustment, locus of control, and drug use. J. Consult. Clin. Psychol. 1978, 46, 264–271. [Google Scholar] [CrossRef]
- Anderson, V.L.; Levinson, E.M.; Barker, W.; Kiewra, K.R. The Effects of Meditation on Teacher Perceived Occupational Stress, State and Trait Anxiety, and Burnout 1. Sch. Psychol. Q. 1999, 14, 3–25. [Google Scholar] [CrossRef]
- Bormann, J.E.; Gifford, A.L.; Shively, M.; Smith, T.L.; Redwine, L.; Kelly, A.; Becker, S.; Gershwin, M.; Bone, P.; Belding, W. Effects of spiritual mantram repetition on HIV outcomes: A randomized controlled trial. J. Behav. Med. 2006, 29, 359–376. [Google Scholar] [CrossRef]
- Puryear, H.B.; Cayce, C.T.; Thurston, M.A. Anxiety reduction associated with meditation: Home study. Percept. Mot. Ski. 1976, 43, 527–531. [Google Scholar] [CrossRef]
- Vaccarino, V.; Kondwani, K.A.; Kelley, M.E.; Murrah, N.V.; Boyd, L.; Ahmed, Y.; Meng, Y.X.; Gibbons, G.H.; Hooper, W.C.; De Staercke, C.; et al. Effect of meditation on endothelial function in black Americans with metabolic syndrome: A randomized trial. Psychosom. Med. 2013, 75, 591–599. [Google Scholar] [CrossRef] [Green Version]
- Wachholtz, A.B.; Pargament, K.I. Is spirituality a critical ingredient of meditation? Comparing the effects of spiritual meditation, secular meditation, and relaxation on spiritual, psychological, cardiac, and pain outcomes. J. Behav. Med. 2005, 28, 369–384. [Google Scholar] [CrossRef] [PubMed]
- Bormann, J.E.; Thorp, S.R.; Wetherell, J.L.; Golshan, S.; Lang, A.J. Meditation-based mantram intervention for veterans with posttraumatic stress disorder: A randomized trial. Psychol. Trauma Theory Res. Pract. Policy 2013, 5, 259–267. [Google Scholar] [CrossRef]
- Heide, F.J.; Wadlington, W.L.; Lundy, R.M. Hypnotic responsivity as a predictor of outcome in meditation. Int. J. Clin. Exp. Hypn. 1980, 28, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Jeitler, M.; Brunnhuber, S.; Meier, L.; Lüdtke, R.; Büssing, A.; Kessler, C.; Michalsen, A. Effectiveness of jyoti meditation for patients with chronic neck pain and psychological distress—A randomized controlled clinical trial. J. Pain 2015, 16, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Kirkland, K.; Hollandsworth, J.G. Effective test taking: Skills-acquisition versus anxiety-reduction techniques. J. Consult. Clin. Psychol. 1980, 48, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Kirsch, I.; Henry, D. Self-desensitization and meditation in the reduction of public speaking anxiety. J. Consult. Clin. Psychol. 1979, 47, 536–541. [Google Scholar] [CrossRef] [PubMed]
- Lehrer, P.M.; Schoicket, S.; Carrington, P.; Woolfolk, R.L. Psychophysiological and cognitive responses to stressful stimuli in subjects practicing progressive relaxation and clinically standardized meditation. Behav. Res. Ther. 1980, 18, 293–303. [Google Scholar] [CrossRef]
- Michalsen, A.; Kunz, N.; Jeitler, M.; Brunnhuber, S.; Meier, L.; Lüdtke, R.; Büssing, A.; Kessler, C. Effectiveness of focused meditation for patients with chronic low back pain-A randomized controlled clinical trial. Complementary Ther. Med. 2016, 26, 79–84. [Google Scholar] [CrossRef]
- Parker, J.C.; Gilbert, G.S.; Thoreson, R.W. Reduction of autonomic arousal in alcoholics: A comparison of relaxation and meditation techniques. J. Consult. Clin. Psychol. 1978, 46, 879–886. [Google Scholar] [CrossRef] [PubMed]
- Boswell, P.C.; Murray, E.J. Effects of meditation on psychological and physiological measures of anxiety. J. Consult. Clin. Psychol. 1979, 47, 606–607. [Google Scholar] [CrossRef] [PubMed]
- Manocha, R.; Black, D.; Sarris, J.; Stough, C. A randomized, controlled trial of meditation for work stress, anxiety and depressed mood in full-time workers. Evid.-Based Complementary Altern. Med. 2011, 2011, 960583. [Google Scholar] [CrossRef] [PubMed]
- Vasudev, A.; Arena, A.; Burhan, A.M.; Ionson, E.; Hirjee, H.; Maldeniya, P.; Wetmore, S.; Newman, R.I. A training programme involving automatic self-transcending meditation in late-life depression: Preliminary analysis of an ongoing randomised controlled trial—Retracted. BJPsych Open 2016, 2, 195. [Google Scholar] [CrossRef] [Green Version]
- Ionson, E.; Limbachia, J.; Rej, S.; Puka, K.; Newman, R.I.; Wetmore, S.; Burhan, A.M.; Vasudev, A. Effects of Sahaj Samadhi meditation on heart rate variability and depressive symptoms in patients with late-life depression. Br. J. Psychiatry 2019, 214, 218–224. [Google Scholar] [CrossRef]
- Jong, M.C.; Boers, I.; van Wietmarschen, H.A.; Tromp, E.; Busari, J.O.; Wennekes, R.; Snoeck, I.; Bekhof, J.; Vlieger, A.M. Hypnotherapy or transcendental meditation versus progressive muscle relaxation exercises in the treatment of children with primary headaches: A multi-centre, pragmatic, randomised clinical study. Eur. J. Pediatr. 2019, 178, 147–154. [Google Scholar] [CrossRef] [Green Version]
- Raskin, M.; Bali, L.R.; Peeke, H.V. Muscle Biofeedback and Transcendental Meditation: A Controlled Evaluation of Efficacy in the Treatment of Chronic Anxiety. Arch. Gen. Psychiatry 1980, 37, 93–97. [Google Scholar] [CrossRef]
- Wachholtz, A.B.; Pargament, K.I. Migraines and meditation: Does spirituality matter? J. Behav. Med. 2008, 31, 351–366. [Google Scholar] [CrossRef]
- Brooks, J.; Scarano, T. Transcendental Meditation in the Treatment of Post-Vietnam Adjustment. J. Couns. Dev. 1985, 64, 212–215. [Google Scholar] [CrossRef]
- Elder, C.; Nidich, S.; Moriarty, F.; Nidich, R. Effect of transcendental meditation on employee stress, depression, and burnout: A randomized controlled study. Perm. J. 2014, 18, 19–23. [Google Scholar] [CrossRef]
- Jayadevappa, R.; Johnson, J.C.; Bloom, B.S.; Nidich, S.; Desai, S.; Chhatre, S.; Raziano, D.B.; Schneider, R. Effectiveness of transcendental meditation on functional capacity and quality of life of African Americans with congestive heart failure: A randomized control study. Ethn. Dis. 2007, 17, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Schneider, R.H.; Grim, C.E.; Rainforth, M.V.; Kotchen, T.; Nidich, S.I.; Gaylord-King, C.; Salerno, J.W.; Kotchen, J.M.; Alexander, C.N. Stress Reduction in the Secondary Prevention of Cardiovascular Disease. Circ. Cardiovasc. Qual. Outcomes 2012, 5, 750–758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chhatre, S.; Metzger, D.S.; Frank, I.; Boyer, J.; Thompson, E.; Nidich, S.; Montaner, L.J.; Jayadevappa, R. Effects of behavioral stress reduction Transcendental Meditation intervention in persons with HIV. AIDS Care 2013, 25, 1291–1297. [Google Scholar] [CrossRef] [Green Version]
- Wolf, D.B.; Abell, N. Examining the effects of meditation techniques on psychosocial functioning. Res. Soc. Work Pract. 2003, 13, 27–42. [Google Scholar] [CrossRef]
- Milbury, K.; Chaoul, A.; Biegler, K.; Wangyal, T.; Spelman, A.; Meyers, C.A.; Arun, B.; Palmer, J.L.; Taylor, J.; Cohen, L. Tibetan sound meditation for cognitive dysfunction: Results of a randomized controlled pilot trial. Psycho-Oncology 2013, 22, 2354–2363. [Google Scholar] [CrossRef]
- Oman, D.; Hedberg, J.; Thoresen, C.E. Passage meditation reduces perceived stress in health professionals: A randomized, controlled trial. J. Consult. Clin. Psychol. 2006, 74, 714–719. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.W.Y.; Gao, J.; Leung, H.K.; Sik, H.H. A Randomized Controlled Trial of Awareness Training Program (ATP), a Group-Based Mahayana Buddhist Intervention. Mindfulness 2019, 10, 1280–1293. [Google Scholar] [CrossRef] [Green Version]
- Severtsen, B.; Bruya, M.A. Effects of meditation and aerobic exercise on EEG patterns. J. Neurosci. Nurs. J. Am. Assoc. Neurosci. Nurses 1986, 18, 206–210. [Google Scholar] [CrossRef]
- Nidich, S.; Seng, A.; Compton, B.; O’connor, T.; Salerno, J.W.; Nidich, R. Transcendental Meditation and Reduced Trauma Symptoms in Female Inmates: A Randomized Controlled Study. Perm. J. 2017, 21, 16-008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rees, B.; Travis, F.; Shapiro, D.; Chant, R. Reduction in Posttraumatic Stress Symptoms in Congolese Refugees Practicing Transcendental Meditation. J. Trauma. Stress 2013, 26, 295–298. [Google Scholar] [CrossRef]
- Bormann, J.E.; Thorp, S.; Wetherell, J.L.; Golshan, S. A Spiritually Based Group Intervention for Combat Veterans With Posttraumatic Stress Disorder:Feasibility Study. J. Holist. Nurs. 2008, 26, 109–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heffner, K.L.; Crean, H.F.; Kemp, J.E. Meditation programs for veterans with posttraumatic stress disorder: Aggregate findings from a multi-site evaluation. Psychol. Trauma Theory Res. Pract. Policy 2016, 8, 365–374. [Google Scholar] [CrossRef]
- Nidich, S.I.; Fields, J.Z.; Rainforth, M.V.; Pomerantz, R.; Cella, D.; Kristeller, J.; Salerno, J.W.; Schneider, R.H. A Randomized Controlled Trial of the Effects of Transcendental Meditation on Quality of Life in Older Breast Cancer Patients. Integr. Cancer Ther. 2009, 8, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Murphy, T.J.; Pagano, R.R.; Marlatt, G.A. Lifestyle modification with heavy alcohol drinkers: Effects of aerobic exercise and meditation. Addict. Behav. 1986, 11, 175–186. [Google Scholar] [CrossRef]
- Tuab, E.; Steiner, S.S.; Weingarten, E.; Walton, K.G. Effectiveness of Broad Spectrum Approaches to Relapse Prevention in Severe Alcoholism: A long-term, randomized, controlled trial of transcendental meditiation, EMG biofeedback and electronic neurotherapy. Alcohol. Treat. Q. 1994, 11, 187–220. [Google Scholar] [CrossRef]
- Ottens, A.J. The effect of transcendental meditation upon modifying the cigarette smoking habit. J. Sch. Health 1975, 45, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Weibel, D.T.; McClintock, A.S.; Anderson, T. Does Loving-Kindness Meditation Reduce Anxiety? Results from a Randomized Controlled Trial. Mindfulness 2016, 8, 565–571. [Google Scholar] [CrossRef]
- Goyal, M.; Singh, S.; Sibinga, E.M.S.; Gould, N.F.; Rowland-Seymour, A.; Sharma, R.; Berger, Z.; Sleicher, D.; Maron, D.D.; Shihab, H.M.; et al. Meditation Programs for Psychological Stress and Well-being: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2014, 174, 357–368. [Google Scholar] [CrossRef] [Green Version]
- Zeng, X.; Chio, F.H.N.; Oei, T.P.S.; Leung, F.Y.K.; Liu, X. A Systematic Review of Associations between Amount of Meditation Practice and Outcomes in Interventions Using the Four Immeasurables Meditations. Front. Psychol. 2017, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cebolla, A.; Demarzo, M.; Martins, P.; Soler, J.; Garcia-Campayo, J. Unwanted effects: Is there a negative side of meditation? A multicentre survey. PLoS ONE 2017, 12, e0183137. [Google Scholar] [CrossRef] [Green Version]
- Britton, W.B. Can mindfulness be too much of a good thing? The value of a middle way. Curr. Opin. Psychol. 2019, 28, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Schlosser, M.; Sparby, T.; Vörös, S.; Jones, R.; Marchant, N.L. Unpleasant meditation-related experiences in regular meditators: Prevalence, predictors, and conceptual considerations. PLoS ONE 2019, 14, e0216643. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Álvarez-Pérez, Y.; Rivero-Santana, A.; Perestelo-Pérez, L.; Duarte-Díaz, A.; Ramos-García, V.; Toledo-Chávarri, A.; Torres-Castaño, A.; León-Salas, B.; Infante-Ventura, D.; González-Hernández, N.; et al. Effectiveness of Mantra-Based Meditation on Mental Health: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 3380. https://doi.org/10.3390/ijerph19063380
Álvarez-Pérez Y, Rivero-Santana A, Perestelo-Pérez L, Duarte-Díaz A, Ramos-García V, Toledo-Chávarri A, Torres-Castaño A, León-Salas B, Infante-Ventura D, González-Hernández N, et al. Effectiveness of Mantra-Based Meditation on Mental Health: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(6):3380. https://doi.org/10.3390/ijerph19063380
Chicago/Turabian StyleÁlvarez-Pérez, Yolanda, Amado Rivero-Santana, Lilisbeth Perestelo-Pérez, Andrea Duarte-Díaz, Vanesa Ramos-García, Ana Toledo-Chávarri, Alezandra Torres-Castaño, Beatriz León-Salas, Diego Infante-Ventura, Nerea González-Hernández, and et al. 2022. "Effectiveness of Mantra-Based Meditation on Mental Health: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 6: 3380. https://doi.org/10.3390/ijerph19063380
APA StyleÁlvarez-Pérez, Y., Rivero-Santana, A., Perestelo-Pérez, L., Duarte-Díaz, A., Ramos-García, V., Toledo-Chávarri, A., Torres-Castaño, A., León-Salas, B., Infante-Ventura, D., González-Hernández, N., Rodríguez-Rodríguez, L., & Serrano-Aguilar, P. (2022). Effectiveness of Mantra-Based Meditation on Mental Health: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 19(6), 3380. https://doi.org/10.3390/ijerph19063380