
Continuing Bonds after Loss by Suicide: A Systematic Review




Abstract
:1. Introduction
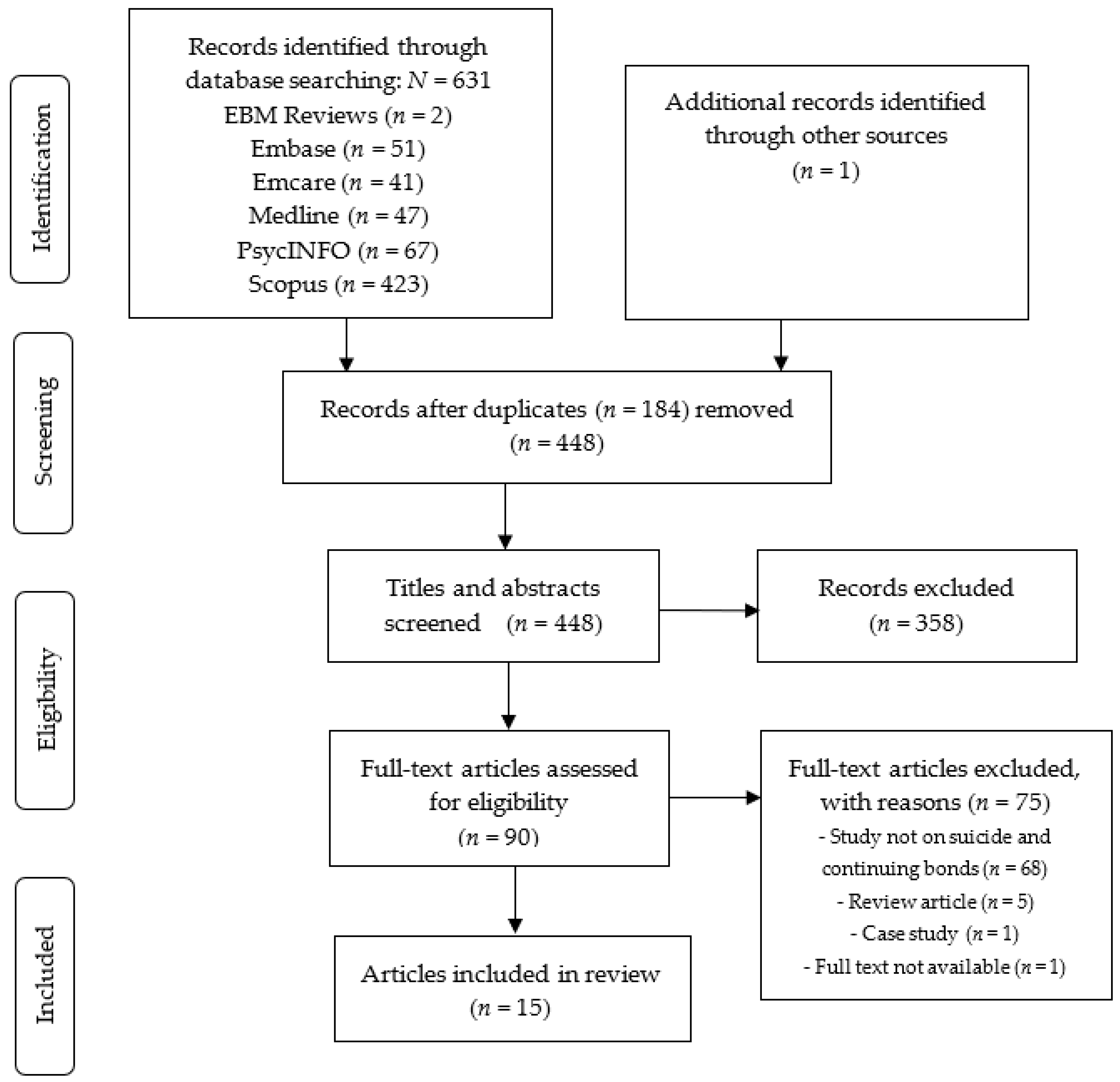
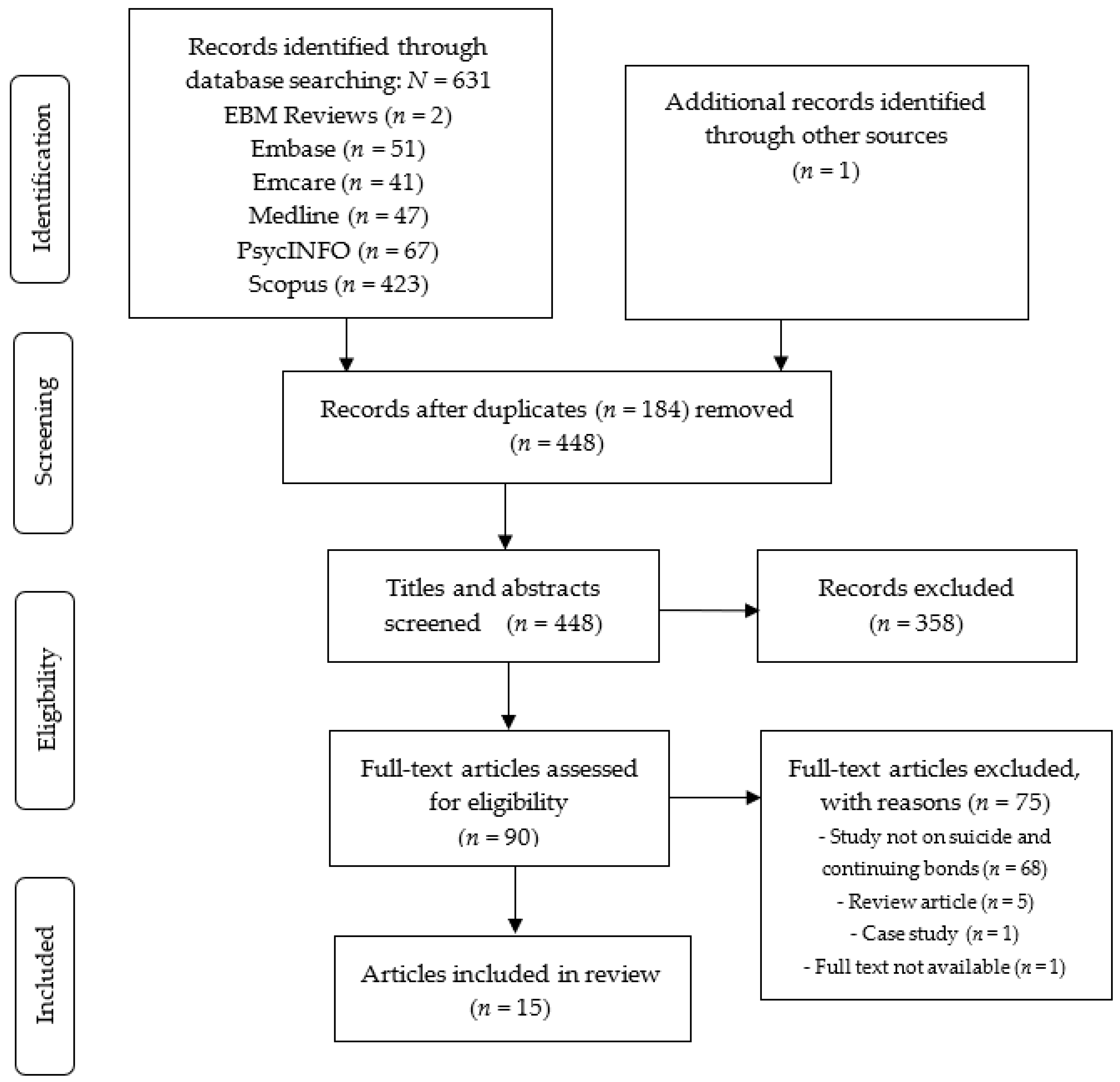
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Quality Assessment
3. Results
3.1. Study Characteristics
3.2. Quality Assessment
3.3. Study Findings
3.3.1. In What Way Can Continuing Bonds Manifest?
3.3.2. Continuing Bonds as a Positive or Negative Experience
4. Discussion
4.1. Factors That Affect the Manifestation of Continuing Bonds
4.2. Continuing Bonds as a Positive or a Negative Experience
4.3. Limitations
4.4. Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
Appendix A

{kind=link}
| Topic | Jahn & Spencer-Thomas, 2014 [19] | Levi-Belz, 2017 [24] |
|---|---|---|
| Selection | ||
| (1) Representativeness of the exposed cohort | ||
| (a) Truly representative (one star) | ||
| (b) Somewhat representative (one star) | ||
| (c) Selected group | X | X |
| (d) No description | ||
| (2) Selection of the non-exposed cohort | ||
| (a) Drawn from the same community as the exposed cohort (one star) | N/a | X |
| (b) Drawn from a different source | ||
| (c) No description | ||
| (3) Ascertainment of exposure | ||
| (a) Secure record (e.g., surgical record) (one star) | ||
| (b) Structured interview (one star) | ||
| (c) Written self-report | X | X |
| (d) No description | ||
| (e) Other | ||
| (4) Demonstration that outcome of interest was not present at start of study | ||
| (a) Yes (one star) | X | X |
| (b) No | ||
| Comparability | ||
| (1) Comparability of cohorts on the basis of the design or analysis controlled for confounders | ||
| (a) The study controls for age, sex and marital status (one star) | X | |
| (b) Study controls for other factors (list) (one star) | X | |
| (c) Controls are not comparable | ||
| Outcome | ||
| (1) Assessment of outcome | ||
| (a) Independent blind assessment (one star) | ||
| (b) Record linkage (one star) | ||
| (c) Self-report | X | X |
| (d) No description | ||
| (e) Other | ||
| (2) Was follow-up long enough for outcomes to occur | ||
| (a) Yes (one star) | X | X |
| (b) No | ||
| Indicate the mean duration of follow-up and a brief rationale for the assessment above | Range <1–20+ years | Range 2–540 months |
| (3) Adequacy of follow-up of cohorts | ||
| (a) Complete follow-up, all subjects accounted for (one star) | ||
| (b) Subjects lost to follow-up unlikely to introduce bias, number lost less than or equal to 20% or description of those lost suggested no different from those followed (one star) | ||
| (c) Follow-up rate less than 80% and no description of those lost | ||
| (d) No statement | X | X |
| Stars | ||
| Selection | 1 | 2 |
| Comparability | 0 | 2 |
| Outcome | 1 | 1 |
| Rating | Poor | Poor |
Appendix B
| Topic | Adams et al., 2019 [14] | Bailey et al., 2015 [21] | Bell et al., 2015 [22] | Castelli, 2018 [27] | Entilli et al., 2021 [15] | Gall et al., 2015 [26] | Hunt et al., 2019 [9] | Jahn et al., 2018 [20] | Leichtentritt et al., 2015 [25] | Maple et al., 2013 [16] | Ross et al., 2018 [17] | Sands et al., 2010 [18] | Wood et al., 2012 [23] | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Domain 1: Research team and reflexivity | ||||||||||||||
| Personal characteristics | ||||||||||||||
| 1 | Interviewer/facilitator | p. 2 324–325 | p. 4 | p. 337 | p. 59 | p. 3 | p. 103 | |||||||
| 2 | Credentials | p. 325 | p. 2 | p. 2 | p. 121 | |||||||||
| 3 | Occupation | p. 325 | p. 2 | p. 1107 | p. 59 | p. 3 | p. 121 | |||||||
| 4 | Gender | p. 324 | p. 2 | p. 337 | p. 2 | p.105/121 | ||||||||
| 5 | Experience and training | p. 325 | p. 4 | p. 2 | p. 1107 | p. 59 | p. 2 | p. 121 | ||||||
| Relationship with participants | ||||||||||||||
| 6 | Relationship established | p. 4 | p. 878 | |||||||||||
| 7 | Participant knowledge of the interviewer | p. 337 | p. 3 | |||||||||||
| 8 | Interviewer characteristics | p. 324–325 | p. 337 | p. 59 | p. 2 | |||||||||
| Domain 2: Study design | ||||||||||||||
| Theoretical framework | ||||||||||||||
| 9 | Methodological orientation and theory | p. 325 | p. 75 | p. 379 | p. 3–4 | p. 3 | p. 102 | p. 336 | p. 6 | p. 1105–1106 | p. 59 | p. 2–3 | p. 99–102 | p. 877 |
| Participant selection | ||||||||||||||
| 10 | Sampling | p. 325 | p. 74 | p. 378 | p. 4 | p. 2–3 | p. 101 | p. 336 | p. 5 | p. 1105 | p. 59 | p. 2 | p. 103 | p. 877 |
| 11 | Method of approach | p. 325 | p. 74 | p. 378 | p. 4 | p. 2 | p. 101–102 | p. 336–337 | p. 5–6 | p. 1105 | p. 59 | p. 2 | p. 103–104 | p. 877–879 |
| 12 | Sample size | p. 325 | p. 74 | p. 378 | p. 5 | p. 2 | p. 101 | p. 336 | p. 5 | p. 1105 | p. 59 | p. 2–3 | p. 103 | p. 877 |
| 13 | Non-participation | p. 325 | p. 2–3 | |||||||||||
| Setting | ||||||||||||||
| 14 | Setting of data collection | p. 325 | p. 75 | p. 4 | p. 2 | p. 336 | p. 5 | p. 59 | p. 2 | p. 103 | p. 878 | |||
| 15 | Presence of non-participants | p. 59 | ||||||||||||
| 16 | Description of sample | p. 325 | p. 74 | p. 378 | p. 5 | p. 2–3 | p. 101 | p. 336 | p. 5 | p. 1105 | p. 59 | p. 2–3 | p. 103 | p. 877–878 |
| Data collection | ||||||||||||||
| 17 | Interview guide | p. 325 | p. 74–75 | p. 378 | p. 3–4 | p. 2 | p. 102 | p. 337 | p. 5–6 | p. 1106 | p. 59 | p. 2 | p. 103–104 | p. 878–879 |
| 18 | Repeat interviews | p. 2 | p. 102 | p. 2 | ||||||||||
| 19 | Audio/visual recording | p. 325 | p. 75 | p. 378 | p. 4 | p. 2 | p. 102 | p. 337 | p. 1106 | p. 59 | p. 2 | p. 103 | p. 879 | |
| 20 | Field notes | p. 4 | p. 1107 | |||||||||||
| 21 | Duration | p. 325 | p. 75 | p. 4 | p. 3 | p. 101 | p. 1106 | p. 59 | p. 2 | p. 103–104 | p. 878 | |||
| 22 | Data saturation | p. 5 | p. 2 | p. 338 | p. 2–3 | |||||||||
| 23 | Transcripts returned | p. 5 | ||||||||||||
| Domain 3: Analysis and findings | ||||||||||||||
| Data analysis | ||||||||||||||
| 24 | Number of data coders | p. 325 | p. 3 | p. 102 | p. 337 | p. 6 | p. 3 | p. 105 | p. 879 | |||||
| 25 | Description of the coding tree | p. 326 | p. 3–6 | p. 337–338 | ||||||||||
| 26 | Derivation of themes | p. 325 | p. 75 | p. 378 | p. 4 | p. 3 | p. 102 | p. 337 | p. 6 | p. 1107 | p. 59 | p. 3 | p. 105–106 | p. 879 |
| 27 | Software | p. 4 | p. 3 | p. 6 | p. 3 | |||||||||
| 28 | Participant checking | p. 5 | p. 337 | |||||||||||
| Reporting | ||||||||||||||
| 29 | Quotations presented | p. 326–329 | p. 76–81 | p. 380–385 | p. 6–14 | p. 3–6 | p. 102–108 | p. 338–342 | p. 6–10 | p. 1108–1114 | p. 60–64 | p. 3–6 | p. 107–113 | p. 880–888 |
| 30 | Data and findings consistent | p. 329–331 | p. 81–83 | p. 383–386 | p. 14–17 | p. 6–10 | p. 108–110 | p. 342–343 | p. 10–11 | p. 1115–1117 | p. 65–67 | p. 7–8 | p. 114–117 | p. 888–894 |
| 31 | Clarity of major themes | p. 326–329 | p. 78–81 | p. 379–382 | p. 5–14 | p. 3–6 | p. 102–108 | p. 338–342 | p. 6–10 | p. 1107–1115 | p. 60–64 | p. 3 | p. 106–114 | p. 880–888 |
| 32 | Clarity of minor themes | p. 3–6 | p. 338–342 | p. 105–106 | p. 880–888 | |||||||||
| Rating | ||||||||||||||
| Domain 1: Research team and reflexivity | 6/8 (75%) | 0/8 (0%) | 0/8 (0%) | 3/8 (38%) | 4/8 (50%) | 0/8 (0%) | 4/8 (50%) | 0/8 (0%) | 2/8 (25%) | 4/8 (50%) | 7/8 (88%) | 5/8 (63%) | 1/8 (13%) | |
| Domain 2: Study design | 10/15 (67%) | 9/15 (60%) | 7/15 (47%) | 12/15 (80%) | 12/15 (80%) | 9/15 (60%) | 9/15 (60%) | 7/15 (47%) | 9/15 (60%) | 10/15 (67%) | 11/15 (73%) | 9/15 (60%) | 9/15 (60%) | |
| Domain 3: Analysis and findings | 6/9 (67%) | 4/9 (44%) | 4/9 (44%) | 6/9 (67%) | 8/9 (89%) | 5/9 (56%) | 8/9 (89%) | 6/9 (67%) | 4/9 (44%) | 4/9 (44%) | 6/9 (67%) | 6/9 (67%) | 6/9 (67%) | |
| Total | 22/32 (69%) | 13/32 (41%) | 11/32 (34%) | 21/32 (66%) | 24/32 (75%) | 14/32 (44%) | 21/32 (66%) | 13/32 (41%) | 15/32 (67%) | 18/32 (56%) | 24/32 (75%) | 20/32 (63%) | 16/32 (50%) | |
References
- World Health Organisation. Suicide; [Updated 17 June 2021]; World Health Organisation: Geneva, Switzerland, 2021; Available online: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed on 6 September 2021).
- Andriessen, K.; Rahman, B.; Draper, B.; Dudley, M.; Mitchell, P.B. Prevalence of exposure to suicide: A meta-analysis of population-based studies. J. Psychiatr. Res. 2017, 88, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Pitman, A.; Osborn, D.; King, M.; Erlangsen, A. Effects of suicide bereavement on mental health and suicide risk. Lancet Psychiatry 2014, 1, 86–94. [Google Scholar] [CrossRef]
- Jordan, J.R.; McIntosh, J.L. Grief after Suicide: Understanding the Consequences and Caring for the Survivors; Routledge: New York, NY, USA, 2011. [Google Scholar]
- Boerner, K.; Stroebe, M.; Schut, H.; Wortman, C.B. Theories of Grief and Bereavement. In Encyclopedia of Geropsychology; Pachana, N.A., Ed.; Springer: Singapore, 2015; pp. 1–10. [Google Scholar]
- Klass, D.; Silverman, P.R.; Nickman, S.; Nickman, S.L. Continuing Bonds: New Understandings of Grief; Taylor & Francis: Washington, DC, USA, 1996. [Google Scholar]
- Klass, D.; Steffen, E. Continuing Bonds in Bereavement: New Directions for Research and Practice; Routledge: New York, NY, USA, 2017. [Google Scholar]
- Neimeyer, R.A.; Baldwin, S.A.; Gillies, J. Continuing bonds and reconstructing meaning: Mitigating complications in bereavement. Death Stud. 2006, 30, 715–738. [Google Scholar] [CrossRef]
- Hunt, Q.A.; Young, T.A.; Hertlein, K.M. The process of long-term suicide bereavement: Responsibility, familial support, and meaning making. Contemp. Fam. Ther. 2019, 41, 335–346. [Google Scholar] [CrossRef]
- Rubin, S.S.; Nadav, O.B.; Malkinson, R.; Koren, D.; Goffer-Shnarch, M.; Michaeli, E. The two-track model of bereavement questionnaire (TTBQ): Development and validation of a relational measure. Death Stud. 2009, 33, 305–333. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. Newcastle-Ottawa Quality Assessment Scale Cohort Studies. University of Ottawa: Ottawa, ON, Canada, n.d. Available online: https://www.ncbi.nlm.nih.gov/books/NBK99082/bin/appb-fm4.pdf (accessed on 6 September 2021).
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Adams, E.; Hawgood, J.; Bundock, A.; Kõlves, K. A phenomenological study of siblings bereaved by suicide: A shared experience. Death Stud. 2019, 43, 324–332. [Google Scholar] [CrossRef]
- Entilli, L.; Ross, V.; De Leo, D.; Cipolletta, S.; Kõlves, K. Experiences of parental suicide-bereavement: A longitudinal qualitative analysis over two years. Int. J. Environ. Res. Public Health 2021, 18, 564. [Google Scholar] [CrossRef]
- Maple, M.; Edwards, H.E.; Minichiello, V.; Plummer, D. Still part of the family: The importance of physical, emotional and spiritual memorial places and spaces for parents bereaved through the suicide death of their son or daughter. Mortality 2013, 18, 54–71. [Google Scholar] [CrossRef]
- Ross, V.; Kõlves, K.; Kunde, L.; de Leo, D. Parents’ experiences of suicide-bereavement: A qualitative study at 6 and 12 months after loss. Int. J. Environ. Res. Public Health 2018, 15, 618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sands, D.; Tennant, M. Transformative learning in the context of suicide bereavement. Adult Educ. Q. 2010, 60, 99–121. [Google Scholar] [CrossRef]
- Jahn, D.; Spencer-Thomas, S. Continuing bonds through after-death spiritual experiences in individuals bereaved by suicide. J. Spiritual. Ment. Health 2014, 16, 311–324. [Google Scholar] [CrossRef]
- Jahn, D.; Spencer-Thomas, S. A qualitative examination of continuing bonds through spiritual experiences in individuals bereaved by suicide. Religions 2018, 9, 248. [Google Scholar] [CrossRef] [Green Version]
- Bailey, L.; Bell, J.; Kennedy, D. Continuing social presence of the dead: Exploring suicide bereavement through online memorialisation. New Rev. Hypermedia Multimed. 2015, 21, 72–86. [Google Scholar] [CrossRef]
- Bell, J.; Bailey, L.; Kennedy, D. ‘We do it to keep him alive’: Bereaved individuals’ experiences of online suicide memorials and continuing bonds. Mortality 2015, 20, 375–389. [Google Scholar] [CrossRef] [Green Version]
- Wood, L.; Byram, V.; Gosling, A.; Stokes, J. Continuing bonds after suicide bereavement in childhood. Death Stud. 2012, 36, 873–898. [Google Scholar] [CrossRef] [PubMed]
- Levi-Belz, Y. Relationship with the deceased as facilitator of posttraumatic growth among suicide-loss survivors. Death Stud. 2017, 41, 376–384. [Google Scholar] [CrossRef]
- Leichtentritt, R.D.; Yerushalmi, A.; Barak, A. Characteristics of the ongoing bond. Br. J. Soc. Work 2015, 45, 1102–1118. [Google Scholar] [CrossRef]
- Gall, T.L.; Henneberry, J.; Eyre, M. Spiritual beliefs and meaning-making within the context of suicide bereavement. J. Study Spiritual. 2015, 5, 98–112. [Google Scholar] [CrossRef]
- Castelli Dransart, D.A. Spiritual and religious issues in the aftermath of suicide. Religions 2018, 9, 153. [Google Scholar] [CrossRef] [Green Version]
- Krysinska, K.; Andriessen, K.; Corveleyn, J. Religion and spirituality in online suicide bereavement: An analysis of online memorials. Crisis 2014, 35, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Čepulienė, A.A.; Pučinskaitė, B.; Spangelytė, K.; Skruibis, P.; Gailienė, D. Spirituality and religiosity during suicide bereavement: A qualitative systematic review. Religions 2021, 12, 766. [Google Scholar] [CrossRef]
- Parker, C.M.; Laungani, P.; Young, B. Death and Bereavement across Cultures; Routledge: New York, NY, USA, 1997. [Google Scholar]
- Stroebe, M.; Schut, H. The dual process model of coping with bereavement: A decade on. Omega 2010, 61, 273–289. [Google Scholar] [CrossRef] [PubMed]
- Foster, T.L.; Gilmer, M.J.; Davies, B.; Dietrich, M.S.; Barrera, M.; Fairclough, D.L.; Vannatta, K.; Gerhardt, C.A. Comparison of continuing bonds reported by parents and siblings after a child’s death from cancer. Death Stud. 2011, 35, 420–440. [Google Scholar] [CrossRef] [PubMed]
- Grad, O.T.; Treven, M.; Krysinska, K. Suicide Bereavement and Gender. In Postvention in Action: The International Handbook of Suicide Bereavement; Andriessen, K., Krysinska, K., Grad, O., Eds.; Hogrefe: Gottingen, Germany, 2017; pp. 39–49. [Google Scholar]
- Milman, E.; Neimeyer, R.A.; Fitzpatrick, M.; MacKinnon, C.J.; Muis, K.R.; Cohen, S.R. Rumination moderates the role of meaning in the development of prolonged grief symptomatology. J. Clin. Psychol. 2019, 75, 1047–1065. [Google Scholar] [CrossRef]
- Root, B.L.; Exline, J.J. The role of continuing bonds in coping with grief: Overview and future directions. Death Stud. 2014, 38, 1–8. [Google Scholar] [CrossRef]
- Stroebe, M.; Schut, H.; Boerner, K. Continuing bonds in adaptation to bereavement: Toward theoretical integration. Clin. Psychol. Rev. 2010, 30, 259–268. [Google Scholar] [CrossRef] [Green Version]
- Krysinska, K.; Andriessen, K. Suicide Bereavement Online: Sharing Memories, Seeking Support, and Exchanging Hope. In Suicide Prevention and New Technologies. Evidence Based Practice; Mishara, B., Kerkhof, A., Eds.; Palgrave-Macmillan: New York, NY, USA, 2014; pp. 150–165. [Google Scholar]
- Krysinska, K.; Andriessen, K. Online memorialization and grief after suicide: An analysis of suicide memorials on the Internet. Omega 2015, 71, 19–47. [Google Scholar] [CrossRef]
- Sands, D. A tripartite model of suicide grief: Meaning-making and the relationship with the deceased. Grief Matters 2009, 12, 10–17. [Google Scholar]
- Evans, A.; Abrahamson, K. The influence of stigma on suicide bereavement: A systematic review. J. Psychosoc. Nurs. Ment. Health Serv. 2020, 58, 21–27. [Google Scholar] [CrossRef] [PubMed]
| Author, Year, Location | Eligibility Criteria | Sample Size | Male/Female | Age | Time since Bereavement | Relationship to Deceased | Setting | Study Design | Outcome Measures | Main Results |
|---|---|---|---|---|---|---|---|---|---|---|
| Levi-Belz (2017) Israel [24] | >18 y/o, identify as a bereaved family member. Excl.: <15 y/o at time of death, inability to speak or write in Hebrew or English. | N = 159 suicide loss survivors = 58, sudden-death bereavers = 48, expected-death bereavers = 53 (F = 81%) | M = 30 F = 129 suicide loss survivors: M = 13, F = 45 sudden-death bereavers: M = 6, F = 42 expected-death bereavers: M = 11, F = 42 | 18–73 suicide loss survivor M = 40.5, SD = 15.6, sudden-death bereavers M = 35.7, SD = 13.1, expected-death bereavers M = 33.1, SD = 12.3 | 2 m–45 y (M = 95 m, SD = 105.46 m) | 25 parents, 11 children, 26 siblings, 30 spouses, and 44 close family members, 9 unknown | Online questionnaire | Cross sectional | Level of functioning: Two-track bereavement questionnaire (TTBQ), Post-traumatic grief level: Stress-Related Growth Scale (SRGS) | Suicide-loss survivors reported lower levels of close positive continuing bonds with the deceased than did participants from the sudden- and expected-death bereaved groups. Intense grief and preoccupation were associated with less positive personal transformation, particularly among the suicide bereaved. This suggests that continuing bonds in those bereaved by suicide are more likely to be experienced negatively than in those bereaved by other causes. |
| Jahn et al. (2014) USA [19] | Survivors of suicide loss | N = 1301 | M = 135 F = 1155 U = 11 | 40–85 | 1 y–3 y (28.9%; n = 376), <1 y (25.7%; n = 334), 4 y–10 y (22.0%; n = 286), 11 y–20 y (12.2%; n = 159), and >20 y (8.2%; n = 107). | Parent (n = 362), sibling (n = 235), spouse/partner (n = 204), child (n = 180), friend (n = 112), niece/nephew (n = 21), grandchild (n = 9), another relationship (n = 119). | Two questionnaires—one demographics and one about experience of suicide. Both containing both qualitative and quantitative info | Descriptive statistics used to explore characteristics of loss and chi squared to examine demographical differences between responses | Two questionnaires: (i) demographic questionnaire, (ii) spiritual experiences of survivors of suicide, including questions about type and frequency of spiritual experiences | Most (n = 819, 63%) of those bereaved by suicide reported after-death spiritual experiences including dreams, feeling the presence of the person and profound coincidences. These experiences are often regarded as positive with 74.5% of participants (n = 610) finding them ‘helpful’ and only 4.8% (n = 39) viewing them as ‘harmful’ (19.9%, n = 163 saw them as neither helpful nor harmful). Being female and having a closer pre death relationship (family member as opposed to friend or client) was positively associated with spiritual experiences. |
| Author, Year, Location | Eligibility Criteria | Sample Size | Male/Female | Age (Years) | Time Since Bereavement | Relationship to Deceased | Setting | Study Design | Main Results |
|---|---|---|---|---|---|---|---|---|---|
| Adams et al. (2019) AUS [14] | Bereaved by suicide of sibling (sibling <20 y/o) in past 10 yrs | N = 7 | M = 4 F = 3 | 20–27 at time of interview (16–23 at time of suicide) | Average time = 3 y 9 m | Sibling | Telephone interview | Interpretive phenomen-ological analysis (IPA) | Identified 4 main themes: (a) the process of grief, (b) grief interactions (within families and outside), (c) continuing bonds, and (d) meaning-making and growth through grief. |
| Bailey et al. (2015) UK [21] | Family members and friends who own suicide memorial sites | N = 11 | M = 3 F = 8 | 20–60 | 5 m–4 y | Parent, siblings or friends | Face-to-face interviews—semi-structured narrative style | Qualitative interpretative approach, combining constant comparison techniques with thematic analysis | The most common motivating factor for starting a memorial page was to ‘keep the deceased alive’ and maintain a connection. Participants found that they were able to better construct and refine relationships with the deceased using online memorials. Whilst most people had positive experiences with memorial sites, the dangers of becoming overly attached and experiencing compounding grief or ‘double loss’ was highlighted. |
| Bell et al. (2015) UK [22] | Individuals who had set up or were managing memorial sites for those who dies by suicide | N = 11 | M = 3 F = 8 | 20–60 | 5 m–4 y | Parent, siblings or friends | Individual interviews | Qualitative interpretative approach, combining constant comparison techniques with thematic analysis | Provided insight into how online memorialisation allows more flexibility and depth in the exploration of grief than can traditional mourning objects—this allows users to reminisce on positive aspects of deceased life but can elicit negative experiences as users can’t control how memories are framed. |
| Castelli Dransart (2018) Switzerland [27] | Suicide-survivors: A person was considered as a survivor of suicide if: (1) he/she self-qualified as such; (2) he/she felt emotionally close to the deceased; and (3) his/her life had been disrupted by a suicide (self-perception). >18 y/o, able to speak Italian, French or German | N = 50 | M = 11 F = 39 | 14–73 | <12 m–16 y | 18 mothers, 5 fathers, 10 sisters, 3 brothers, 3 daughters, 1 son, 7 partners, 1 aunt, 2 friends | Face-to-face in depth interviews conducted by author or mental health carer, either at home or location chosen by bereaved | Grounded Theory using constant comparison of data and 3 steps of coding: open, axial & selective | Suicide triggered spiritual and religious thoughts and experiences for most participants. Even those who claimed to be atheist or agnostic noted religious rituals and spiritual symbols as being important contributors in forging and maintaining a continuing bond with the deceased and in honouring their memory. Interviewees believed loved ones continued to exist in an alternative dimension or space (regardless of religion). |
| Entilli et al. (2021) AUS [15] | Parents who had lost a child by suicide less than 6 months prior to starting the study | N = 14 at 6 and 12 months. N = 11 at 24 months | M = 7 F = 7 (6 and 12 months). M = 6 F = 5 (at 24 months) | Female mean = 60.1 years, range = 50–78 years and male mean = 59.9 years, range = 50–68 years | 6 m, 12 m and 24 m | Parents who had lost a child (aged 15–51) by suicide. Ten were bereaved of sons and four bereaved of daughters | Semi-structured interviews either phone or face-to-face | Longitudinal study using thematic analysis | Three key themes were identified in an earlier analysis (at 6 and 12 months post loss): searching for answers and sense-making, coping strategies and support, and finding meaning and purpose. Further exploration of these themes at 24 months revealed significant differences between mothers and fathers with the latter adopting more maladaptive coping strategies. Maintaining the relationship with the deceased and paranormal experiences were new themes at 24 months (not present at 6 and 12 months) and a shift from brooding to reflection/sense-making was seen at 24 months. The adaptation process was fluctuating and dynamic. |
| Gall et al. (2015) Canada [26] | Individuals who had personal experiences of suicide bereavement | N = 15 (11 bereaved and 4 mental health workers) | M = 2 F = 9 (bereaved) M = 1 F = 3 (MHW) | Mean age was 49 (bereaved) and 53 (MHW) | Mean = 13 y, minimum of 2 y | The deceased persons were: four sons, two fathers, two close friends, two uncles and one mother. | Semi-structured interviews | Phenomenological approach, thematic analysis | Individuals had difficulty reconciling the suicide death of a loved one with their religious views. This often led to a personally defined spirituality rather than a complete loss of faith. Many individuals (also non-religious) found meaning in the belief of an afterlife and/or felt hopeful that the deceased was in a better place and would someday reconnect with them. Engagement in activities to maintain a bond were common. |
| Hunt et al. (2019) USA [9] | >18 y/o, self-identified as suicide loss survivor, >5 years since death | N = 10 | M = 6 F = 4 | 30–72 (mean = 47.6) | 5 y–30 y (mean = 18.6 y) | 5 siblings, 2 partners, 2 parents and one participant who had lost a sibling, grandfather and cousin | Face-to-face semi-structured interviews at participants homes | Thematic analysis informed by grounded theory | Three major themes were identified:
|
| Jahn et al. (2018) USA [20] | Any person who identified as bereaved by suicide | N = 1301 | M = 135 F = 1155 U = 11 | 40–85 | 1 y–3 y (28.9%; n = 376), <1 y (25.7%; n = 334), 4 y–10 y (22.0%; n = 286), 11 y–20 y (12.2%; n = 159), and >20 y (8.2%; n = 107). | Anyone bereaved by suicide | Two questionnaires—one demographics and one about spiritual experiences after suicide bereavement. Both containing both qualitative and quantitative info | Inductive thematic analysis | Nine main themes were identified: (1) a helpful sense of comfort; (2) a helpful sense of connection with the deceased; (3) intense sadness evoked by the spiritual experiences; (4) confusion regarding the spiritual experiences; (5) negative reminders of the deceased or negative meanings of spiritual experiences; (6) evidence of an afterlife; (7) general importance of the spiritual experiences’ meaning; (8) impact of and on religious beliefs; and (9) others’ responses to disclosure of suicide or spiritual experiences. Generally, participants found spiritual experiences aided in healing and transformation and were regarded as positive. |
| Leichtentritt et al. (2015) Israel [25] | Having experienced the loss of a sibling to suicide and the death having occurred at least five years prior to the interview | N = 9 | M = 3 F = 6 | 29–63 | 5 y–37 y | Sibling | In-depth interviews | Relational dialect theory and narrative analysis used. | Five characteristics of the post death relationship were identified, each existing along a continuum: (1) concrete-symbolic (2) dynamic-static (3) conscious-unconscious (4) personal-public (5) monologue-dialogue Findings suggest that labelling post death relationships as ‘adaptive’ or ‘maladaptive’ is simplistic. Bereavement can be better understood when plotted within the 5 continua. |
| Maple et al. (2013) AUS [16] | Parents who lost a child by suicide | N = 22 | M = 6 F = 16 | NA | 6 m–>26 y | 22 parents (6 fathers and 16 mothers) from 18 families bereaved of 15 sons and 3 daughters. 14 participated individually and 4 as couples | In-depth interviews, mostly face-to-face (one phone) | Narrative Inquiry, recursive technique used to explore in more depth. | Contrary to traditional grief literature, it was found that parents needed to maintain a relationship with their deceased child. Manifestations of continuing bonds varied between parents. Commencing with the funeral, parents began developing rituals ensuring that their child’s life, and not the manner of death, was celebrated. Some participants were limited in their expression of grief due to social pressure to resolve grief. |
| Ross et al. (2018) AUS [17] | Parents bereaved by suicide loss of their child 6 months prior to commencement of study | N = 14 | M = 7 F = 7 | 50–78 (female mean = 60.1 years and range = 50–78, male mean = 59.9 years and range = 50–68) | 6 m and 12 m | Parents who had lost a child (aged 15–51) by suicide. Ten were bereaved of sons and four bereaved of daughters | Individual, semi-structured interviews either face-to-face or telephone | Longitudinal study with inductive qualitative approach. | Identified three key themes (searching for answers and sense-making, coping strategies and support, and finding meaning and purpose) in parental responses to suicide bereavement. The phases of sense-making and meaning-making experienced by participants and the range of both adaptive and maladaptive coping strategies indicated that adapting to bereavement is a dynamic and fluctuating process. |
| Sands et al. (2010) AUS [18] | Adults >19 y/o, bereaved through the suicide death of a significant person in their lives | N = 16 | NA | Aged 19+ | >2 m | Family members or spouses: partner grieving a partner, parent grieving a child, sibling grieving a sibling, and adult child grieving a parent | A series of workshops delivered over 12 weeks and 30 h–involved discussion, artwork, grief rituals and journal writing | Generic thematic analysis | Identified 3 core themes that assisted in meaning making in relationships with the themselves, the deceased, and with others. The 3 themes were: (i) Intentionality (‘tying on the shoes’ or adopting the perspective of the deceased), (ii) Reconstruction (‘walking in the shoes’), (iii) Repositioning (‘taking off the shoes’) |
| Wood et al. (2012) UK [23] | 8–15 y/o (M = 11.80, SD = 2.57), whose parent had died by suicide within the previous 13 to 53 months | N = 10 | M = 5 F = 5 | 8–15 | 13 m–53 m (M = 33.4, SD = 17.44) | Eight children bereaved of a father and two bereaved of a mother | Semi-structured interviews, face-to-face at participants’ homes | Interpretative Phenomen-ological Analysis | Found 3 main themes: thinking about the deceased; coping strategies; and connecting to the deceased. Highlighted differences in childhood suicide bereavement as well as factors which may influence adaptiveness. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goodall, R.; Krysinska, K.; Andriessen, K. Continuing Bonds after Loss by Suicide: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 2963. https://doi.org/10.3390/ijerph19052963
Goodall R, Krysinska K, Andriessen K. Continuing Bonds after Loss by Suicide: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(5):2963. https://doi.org/10.3390/ijerph19052963
Chicago/Turabian StyleGoodall, Rebecca, Karolina Krysinska, and Karl Andriessen. 2022. "Continuing Bonds after Loss by Suicide: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 5: 2963. https://doi.org/10.3390/ijerph19052963
APA StyleGoodall, R., Krysinska, K., & Andriessen, K. (2022). Continuing Bonds after Loss by Suicide: A Systematic Review. International Journal of Environmental Research and Public Health, 19(5), 2963. https://doi.org/10.3390/ijerph19052963