A Scoping Review on the Epidemiology of Chronic Low Back Pain among Adults in Sub-Saharan Africa



Abstract
1. Background
2. Materials and Methods
2.1. Scoping Review
2.2. Identification of the Research Question
- What is the prevalence of CLBP among adults in SSA?
- What are the risk factors associated with CLBP among adults in SSA?
- What are the comorbidities associated with CLBP among adults in SSA?
- What are the factors associated with CLBP disability among adults in SSA?
- What are the current management practices for CLBP in SSA?
2.3. Identification of Relevant Studies
2.4. Study Selection and Eligibility
2.5. Inclusion Criteria
- Prevalence of CLBP;
- Risk factors for CLBP;
- Comorbidities associated with CLBP;
- Factors associated with CLBP disability;
- Management of CLBP (how CLBP is managed).
2.6. Exclusion Criteria
2.7. Charting the Data
2.8. Collating and Summarising Findings
2.9. Methodological Quality Appraisal
3. Results
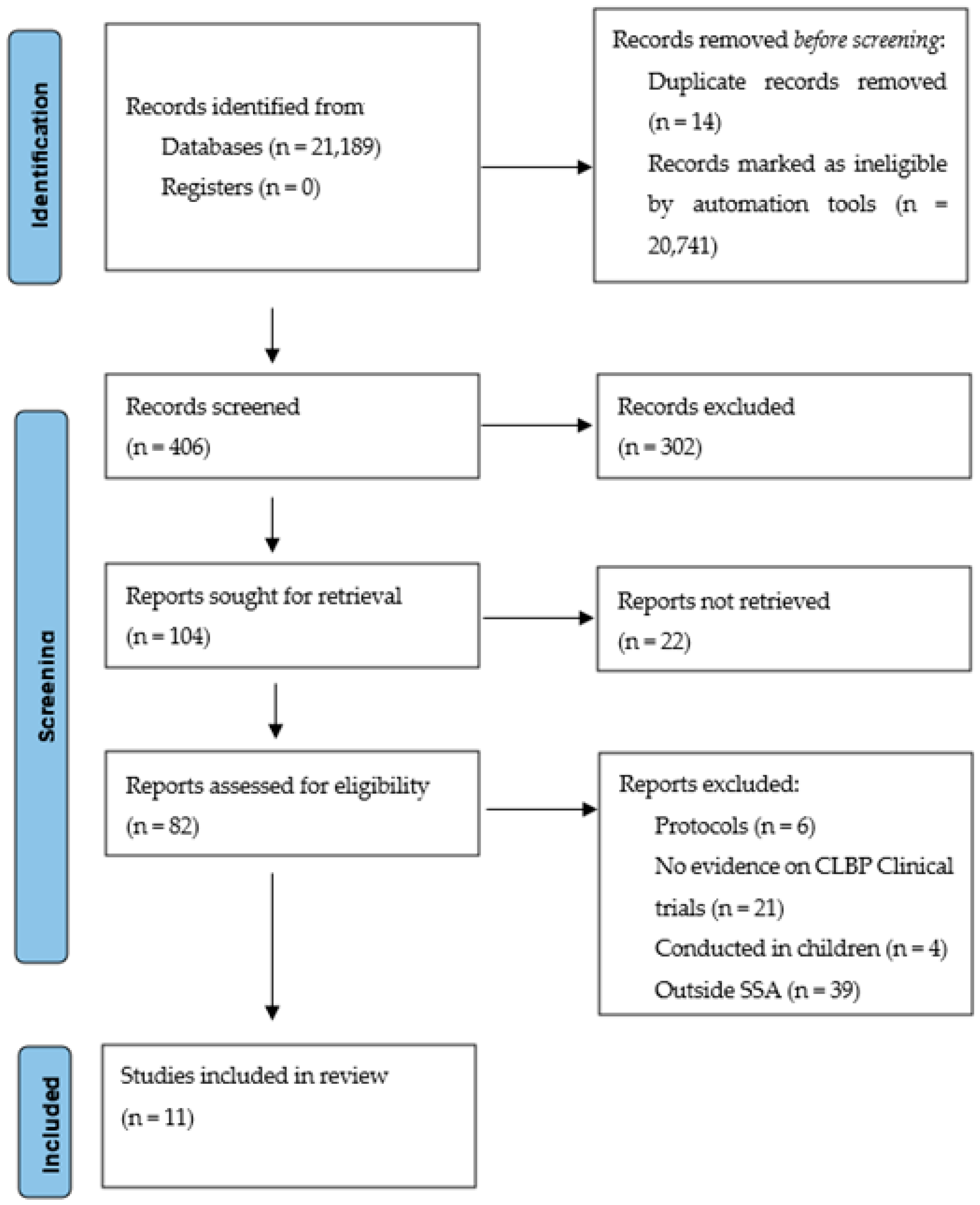
3.1. Characteristics of Included Studies
3.2. Prevalence of Chronic Low Back Pain
3.3. Risk Factors Associated with Chronic Low Back Pain
3.4. Chronic Low Back Pain Comorbidities and Disability
3.5. Patterns of CLBP Presentations, Hospital Admissions and Management Strategies
3.6. Regional and Gender-Based Differences
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kebede, A.; Abebe, S.M.; Woldie, H.; Yenit, M.K. Low Back Pain and Associated Factors among Primary School Teachers in Mekele City, North Ethiopia: A Cross-Sectional Study. Occup. Ther. Int. 2019, 2019, 3862946. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.; March, L.; Zheng, X.; Huang, J.; Wang, X.; Zhao, J.; Blyth, F.M.; Smith, E.; Buchbinder, R.; Hoy, D. Global low back pain prevalence and years lived with disability from 1990 to 2017: Estimates from the Global Burden of Disease Study 2017. Ann. Transl. Med. 2020, 8, 299. [Google Scholar] [CrossRef]
- Chen, S.; Chen, M.; Wu, X.; Lin, S.; Tao, C.; Cao, H.; Shao, Z.; Xiao, G. Global, regional and national burden of low back pain 1990–2019: A systematic analysis of the Global Burden of Disease study 2019. J. Orthop. Transl. 2022, 32, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef]
- Meucci, R.D.; Fassa, A.G.; Faria, N.M.X. Prevalence of chronic low back pain: Systematic review. Rev. De Saude Publica 2015, 49, 73. [Google Scholar] [CrossRef]
- Patrick, N.; Emanski, E.; Knaub, M.A. Acute and chronic low back pain. Med. Clin. 2014, 98, 777–789. [Google Scholar] [CrossRef] [PubMed]
- Van Middelkoop, M.; Rubinstein, S.M.; Verhagen, A.P.; Ostelo, R.W.; Koes, B.W.; van Tulder, M.W. Exercise therapy for chronic nonspecific low-back pain. Best Pract. Res. Clin. Rheumatol. 2010, 24, 193–204. [Google Scholar] [CrossRef]
- Maher, C.; Underwood, M.; Buchbinder, R. Non-specific low back pain. Lancet 2017, 389, 736–747. [Google Scholar] [CrossRef]
- Amundsen, P.A.; Evans, D.W.; Rajendran, D.; Bright, P.; Bjørkli, T.; Eldridge, S.; Buchbinder, R.; Underwood, M.; Froud, R. Inclusion and exclusion criteria used in non-specific low back pain trials: A review of randomised controlled trials published between 2006 and 2012. BMC Musculoskelet. Disord. 2018, 19, 113. [Google Scholar] [CrossRef]
- Foster, N.E. Barriers and progress in the treatment of low back pain. BMC Med. 2011, 9, 1–5. [Google Scholar] [CrossRef]
- Gore, M.; Sadosky, A.; Stacey, B.R.; Tai, K.-S.; Leslie, D. The burden of chronic low back pain: Clinical comorbidities, treatment patterns, and health care costs in usual care settings. Spine 2012, 37, E668–E677. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Chang, M.C. Chronic pain: Structural and functional changes in brain structures and associated negative affective states. Int. J. Mol. Sci. 2019, 20, 3130. [Google Scholar] [CrossRef] [PubMed]
- Meucci, R.D.; Fassa, A.G.; Faria, N.M.; Fiori, N.S. Chronic low back pain among tobacco farmers in southern Brazil. Int. J. Occup. Environ. Health 2015, 21, 66–73. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Louw, Q.A.; Morris, L.D.; Grimmer-Somers, K. The prevalence of low back pain in Africa: A systematic review. BMC Musculoskelet. Disord. 2007, 8, 105. [Google Scholar] [CrossRef]
- Morris, L.D.; Daniels, K.J.; Ganguli, B.; Louw, Q.A. An update on the prevalence of low back pain in Africa: A systematic review and meta-analyses. BMC Musculoskelet. Disord. 2018, 19, 1–15. [Google Scholar] [CrossRef]
- Walker, B.F. The prevalence of low back pain: A systematic review of the literature from 1966 to 1998. Clin. Spine Surg. 2000, 13, 205–217. [Google Scholar] [CrossRef]
- Hoy, D.; Bain, C.; Williams, G.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Vos, T.; Buchbinder, R. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012, 64, 2028–2037. [Google Scholar] [CrossRef]
- Edwards, J.; Hayden, J.; Asbridge, M.; Gregoire, B.; Magee, K. Prevalence of low back pain in emergency settings: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2017, 18, 1–12. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 1–9. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Kahere, M.; Ginindza, T. Mapping evidence on the prevalence, incidence, risk factors and cost associated with chronic low back pain among adults in Sub-Saharan Africa: A systematic scoping review protocol. Syst. Rev. 2020, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372. [Google Scholar] [CrossRef]
- Igwesi-Chidobe, C.N.; Coker, B.; Onwasigwe, C.N.; Sorinola, I.O.; Godfrey, E.L. Biopsychosocial factors associated with chronic low back pain disability in rural Nigeria: A population-based cross-sectional study. BMJ Glob. Health 2017, 2, e000284. [Google Scholar] [CrossRef] [PubMed]
- Omoke, N.I.; Amaraegbulam, P.I. Low back pain as seen in orthopedic clinics of a Nigerian Teaching Hospital. Niger. J. Clin. Pract. 2016, 19, 212–217. [Google Scholar] [CrossRef]
- Tella, B.A.; Akinbo, S.R.; Asafa, S.A.; Gbiri, C.A. Prevalence and impacts of low back pain among peasant farmers in south-west Nigeria. Int. J. Occup. Med. Environ. Health 2013, 26, 621–627. [Google Scholar] [CrossRef]
- Nakua, E.K.; Otupiri, E.; Dzomeku, V.M.; Owusu-Dabo, E.; Agyei-Baffour, P.; Yawson, A.E.; Folson, G.; Hewlett, S. Gender disparities of chronic musculoskeletal disorder burden in the elderly Ghanaian population: Study on global ageing and adult health (SAGE WAVE 1). BMC Musculoskelet. Disord. 2015, 16, 204. [Google Scholar] [CrossRef]
- Yosef, T.; Belachew, A.; Tefera, Y. Magnitude and Contributing Factors of Low Back Pain among Long Distance Truck Drivers at Modjo Dry Port, Ethiopia: A Cross-Sectional Study. J. Environ. Public Health 2019, 2019, 6793090. [Google Scholar] [CrossRef]
- Beyera, G.K.; O’Brien, J.; Campbell, S. Hospital admission and associated factors among individuals presenting to healthcare facilities for low back pain in Ethiopia. Int. J. Rheum. Dis. 2020, 23, 763–771. [Google Scholar] [CrossRef]
- Kahere, M.; Ginindza, T. The prevalence and risk factors of chronic low back pain among adults in KwaZulu-Natal, South Africa: An observational cross-sectional hospital-based study. BMC Musculoskelet. Disord. 2021, 22, 955. [Google Scholar] [CrossRef]
- Kahere, M.; Ginindza, T. The prevalence and psychosocial risk factors of chronic low back pain in KwaZulu-Natal. Afr. J. Prim. Health Care Fam. Med. 2022, 14, 8. [Google Scholar] [CrossRef] [PubMed]
- Major-Helsloot, M.E.; Crous, L.C.; Grimmer-Somers, K.; Louw, Q.A. Management of LBP at primary care level in South Africa: Up to standards? Afr. Health Sci. 2014, 14, 698–706. [Google Scholar] [CrossRef] [PubMed]
- Doualla, M.; Aminde, J.; Aminde, L.N.; Lekpa, F.K.; Kwedi, F.M.; Yenshu, E.V.; Chichom, A.M. Factors influencing disability in patients with chronic low back pain attending a tertiary hospital in sub-Saharan Africa. BMC Musculoskelet. Disord. 2019, 20, 25. [Google Scholar] [CrossRef] [PubMed]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Beyera, G.K.; O’Brien, J.; Campbell, S. Determinants of healthcare utilisation for low back pain: A population-based study in Ethiopia. Health Soc. Care Community 2020, 28, 1058–1070. [Google Scholar] [CrossRef]
- Heuch, I.; Hagen, K.; Heuch, I.; Nygaard, Ø.; Zwart, J.-A. The impact of body mass index on the prevalence of low back pain: The HUNT study. Spine 2010, 35, 764–768. [Google Scholar] [CrossRef]
- Noormohammadpour, P.; Mansournia, M.A.; Koohpayehzadeh, J.; Asgari, F.; Rostami, M.; Rafei, A.; Kordi, R. Prevalence of chronic neck pain, low back pain, and knee pain and their related factors in community-dwelling adults in Iran. Clin. J. Pain 2017, 33, 181–187. [Google Scholar] [CrossRef]
- Schopflocher, D.; Taenzer, P.; Jovey, R. The Prevalence of Chronic Pain in Canada. Pain Res. Manag. 2011, 16, 876306. [Google Scholar] [CrossRef]
- Balagué, F.; Mannion, A.F.; Pellisé, F.; Cedraschi, C. Non-specific low back pain. Lancet 2012, 379, 482–491. [Google Scholar] [CrossRef]
- Johannes, C.B.; Le, T.K.; Zhou, X.; Johnston, J.A.; Dworkin, R.H. The prevalence of chronic pain in United States adults: Results of an Internet-based survey. J. Pain 2010, 11, 1230–1239. [Google Scholar] [CrossRef]
- Jiménez-Sánchez, S.; Fernández-de-Las-Peñas, C.; Carrasco-Garrido, P.; Hernández-Barrera, V.; Alonso-Blanco, C.; Palacios-Ceña, D.; Jiménez-García, R. Prevalence of chronic head, neck and low back pain and associated factors in women residing in the Autonomous Region of Madrid (Spain). Gac. Sanit. 2012, 26, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Juniper, M.; Le, T.K.; Mladsi, D. The epidemiology, economic burden, and pharmacological treatment of chronic low back pain in France, Germany, Italy, Spain and the UK: A literature-based review. Expert Opin. Pharmacother. 2009, 10, 2581–2592. [Google Scholar] [CrossRef]
- Claus, M.; Kimbel, R.; Spahn, D.; Dudenhöffer, S.; Rose, D.-M.; Letzel, S. Prevalence and influencing factors of chronic back pain among staff at special schools with multiple and severely handicapped children in Germany: Results of a cross-sectional study. BMC Musculoskelet. Disord. 2014, 15, 1–9. [Google Scholar] [CrossRef]
- Buchbinder, R.; van Tulder, M.; Öberg, B.; Costa, L.M.; Woolf, A.; Schoene, M.; Croft, P.; Hartvigsen, J.; Cherkin, D.; Foster, N.E. Low back pain: A call for action. Lancet 2018, 391, 2384–2388. [Google Scholar] [CrossRef]
- Taechasubamorn, P.; Nopkesorn, T.; Pannarunothai, S. Prevalence of low back pain among rice farmers in a rural community in Thailand. J. Med. Assoc. Thail. 2011, 94, 616. [Google Scholar]
- Anannontsak, A.; Puapan, P. Effects of working postures on low back pain. J. Hum. Ergol. 1996, 25, 65–72. [Google Scholar]
- Xu, Y.; Bach, E.; Orhede, E. Work environment and low back pain: The influence of occupational activities. Occup. Environ. Med. 1997, 54, 741–745. [Google Scholar] [CrossRef]
- Mafuyai, M.; Babangida, B.; Mador, E.; Bakwa, D.; Jabil, Y. Postural Theory of Non-Specific Low Back Pain (NSLBP). World Appl. Sci. J. 2013, 28, 1818–4952. [Google Scholar]
- Netterstrøm, B.; Juel, K. Low back trouble among urban bus drivers in Denmark. Scand. J. Soc. Med. 1989, 17, 203–206. [Google Scholar] [CrossRef]
- Xu, L.; Wang, Z.; Song, T.; Zhao, X.; Wu, L.; Chen, B.; Peng, L.; He, L.; Wang, S.; Yang, L. Survey on prevalence of occupational musculoskeletal disorders among workers in a shipyard. Chin. J. Ind. Hyg. Occup. Dis. 2011, 29, 180–183. [Google Scholar]
- Szeto, G.P.; Lam, P. Work-related musculoskeletal disorders in urban bus drivers of Hong Kong. J. Occup. Rehabil. 2007, 17, 181–198. [Google Scholar] [CrossRef] [PubMed]
- Porter, J.M.; Gyi, D. The prevalence of musculoskeletal troubles among car drivers. Occup. Med. 2002, 52, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Jadhav, A.V. Comparative cross-sectional study for understanding the burden of low back pain among public bus transport drivers. Indian J. Occup. Environ. Med. 2016, 20, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Hoy, J.; Mubarak, N.; Nelson, S.; De Landas, M.S.; Magnusson, M.; Okunribido, O.; Pope, M. Whole body vibration and posture as risk factors for low back pain among forklift truck drivers. J. Sound Vib. 2005, 284, 933–946. [Google Scholar] [CrossRef]
- Shmagel, A.; Foley, R.; Ibrahim, H. Epidemiology of chronic low back pain in US adults: Data from the 2009–2010 National Health and Nutrition Examination Survey. Arthritis Care Res. 2016, 68, 1688–1694. [Google Scholar] [CrossRef] [PubMed]
- Heitz, C.A.M.; Hilfiker, R.; Bachmann, L.M.; Joronen, H.; Lorenz, T.; Uebelhart, D.; Klipstein, A.; Brunner, F. Comparison of risk factors predicting return to work between patients with subacute and chronic non-specific low back pain: Systematic review. Eur. Spine J. 2009, 18, 1829–1835. [Google Scholar] [CrossRef][Green Version]
- Nieminen, L.K.; Pyysalo, L.M.; Kankaanpää, M.J. Prognostic factors for pain chronicity in low back pain: A systematic review. PAIN Rep. 2021, 6, e919. [Google Scholar] [CrossRef]
- Pranjić, N.; Maleš-Bilić, L. Low back pain at new working ambient in era of new economy: A systematic review about occupational risk factors. Acta Med. Croat. 2015, 69, 49–58. [Google Scholar]
- Alhowimel, A.; AlOtaibi, M.; Radford, K.; Coulson, N. Psychosocial factors associated with change in pain and disability outcomes in chronic low back pain patients treated by physiotherapist: A systematic review. SAGE Open Med. 2018, 6. [Google Scholar] [CrossRef]
- Paul, C.; Ayis, S.; Ebrahim, S. Psychological distress, loneliness and disability in old age. Psychol. Health Med. 2006, 11, 221–232. [Google Scholar] [CrossRef]
- Pimenta, C.; Braga, P.; Corrêa, C. Disability related to chronic low back pain: Prevalence and associated factors. Rev. Da Esc. De Enferm. Da USP 2012, 46, 16–23. [Google Scholar]
- Pincus, T.; Burton, A.K.; Vogel, S.; Field, A.P. A Systematic Review of Psychological Factors as Predictors of Chronicity/Disability in Prospective Cohorts of Low Back Pain. Spine 2002, 27, E109–E120. [Google Scholar] [CrossRef] [PubMed]
- Ramond, A.; Bouton, C.; Richard, I.; Roquelaure, Y.; Baufreton, C.; Legrand, E.; Huez, J.-F. Psychosocial risk factors for chronic low back pain in primary care—A systematic review. Fam. Pract. 2011, 28, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Sikorski, J.M.; Stampfer, H.G.; Cole, R.M.; Wheatley, A.E. Psychological aspects of chronic low back pain. Aust. New Zealand J. Surg. 1996, 66, 294–297. [Google Scholar] [CrossRef]
- Beneciuk, J.M.; Bishop, M.D.; Fritz, J.M.; Robinson, M.E.; Asal, N.R.; Nisenzon, A.N.; George, S.Z. The STarT back screening tool and individual psychological measures: Evaluation of prognostic capabilities for low back pain clinical outcomes in outpatient physical therapy settings. Phys. Ther. 2013, 93, 321–333. [Google Scholar] [CrossRef]
- Traeger, A.; McAuley, J.H. STarT Back screening tool. J. Physiother. 2013, 59, 131. [Google Scholar] [CrossRef]
- Schmidt, P.-A.; Naidoo, V. Cross-cultural adaptation and validation of the STarT back screening tool in isiZulu. South Afr. J. Physiother. 2020, 76, 1402. [Google Scholar] [CrossRef]
- Karunanayake, A.L.; Pathmeswaran, A.; Kasturiratne, A.; Wijeyaratne, L.S. Risk factors for chronic low back pain in a sample of suburban S ri L ankan adult males. Int. J. Rheum. Dis. 2013, 16, 203–210. [Google Scholar] [CrossRef]
- Lionel, A. Risk factors for chronic low back pain. J. Community Med. Health Educ. 2014, 4. [Google Scholar] [CrossRef]


{kind=link}
| Author and Publication Year | Country | Study Setting | Design | Sample Size | Population Description | Age | Main Findings |
|---|---|---|---|---|---|---|---|
| Igwesi-Chidobe et al. [24] | Nigeria | Population-based | Cross-sectional | N = 200 Female = 112 Male = 88 | General population with low back pain | 48.6 (12.0) years | Risk factors for CLBP disability Abnormal illness perceptions, severe pain intensity, catastrophizing, FAB, anxiety, lack of social support and female gender |
| Omoke et al. [25] | Nigeria | Hospital-based | Cross-sectional | N = 291 Femalen = 143 Malen = 148 | General population with low back pain | 45.8 ± 1.67 years | Prevalence of CLBP (59.1%) Incidence M = 58.3% F = 41.7% Risk factors Heavy lifting, previous back injury, obesity, pregnancy, long-distance driving Comorbidities Hypertension, diabetes mellitus, peptic ulcer disease, hip and knee osteoarthritis, cervical spondylosis |
| Tella et al. [26] | Nigeria | Population based | Cross-sectional | N = 604 Femalen = 236 Malen = 368 | Farmers | CLBP prevalence (48.5%) Risk factors Prolonged bending | |
| Nakua et al. [27] | Ghana | Population-based | Cross-sectional | N = 4724 Rural: [N = 2799, Women = 1333 Men = 1466] Urban: [N = 1925, Women = 1 Men = 881] | General population | Rural: Female = 64.9 (95%CI: 64.4, 65.5) Male = 64.1 (95%CI: 63.6, 64.7) | CLBP prevalence (28.2%) Residence (rural and urban) did not appear to influence the prevalence of chronic back pain |
| Kebede et al. [1] | Ethiopia | Primary schools | Cross-sectional | N = 611 Femalen = 331 Malen = 280 | Teachers | 40 (±9.38) years | CLBP prevalence (30.1%) Risk factors sleeping disturbance, prolonged standing, physical inactivity |
| Yosef et al. [28] | Ethiopia | Port-based | Cross-sectional | N = 422 | Truck drivers | 37.7 (±9.13 SD) years | CLBP prevalence (52.37%) Risk factors cigarette smoking, physical inactivity, comorbid chronic diseases, heavy lifting, perceived improper sitting posture, perceived job stress |
| Beyera et al. [29] | Ethiopia | Population-based | Cross-sectional | N = 543 Femalen = 227 Malen = 316 | General population with low back pain | 43 years (interquartile range 33–55 years) | CLBP prevalence Lasting 1–5 years (38.7%), Lasting > 5 years (16.2%) Factors associated with admissions Female gender, advanced age, low socioeconomic status, alcohol consumption, severe pain intensity, presence of additional spinal pain |
| Kahere et al. [30] | South Africa | Hospital-based | Cross-sectional | N = 678 Femalen = 394 Malen = 284 | General population | CLBP prevalence (18.1%) Risk factors overweight, no formal education, lack of regular physical exercises, cigarette smoking, alcohol consumption, sedentary lifestyle, manual work, stooped posture | |
| Kahere et al. [31] | South Africa | Hospital-based | Cross-sectional | N = 554 Femalen = 228 Malen = 326 | General population | CLBP prevalence (22.2%) Risk factors female gender, middle aged adults 38–47 years, obesity, disease conviction, affective disturbance, denial, FAB | |
| Major-Helsloot et al. [32] | South Africa | Health facility based | Cross-sectional | N = 504 Famalen = 374 Malen = 130 | General population | 44.8 (SD ± 13.95) | CLBP prevalence (26.3%) Management Pain medication was the only form of treatment received Risk factors psychosocial distress |
| Doualla et al. [33] | Cameroon | Hospital-based | Cross-sectional | N = 136 Femalen = 87 Malen = 48 | General population with low back pain | 50.6 ± 12.2 | Prevalence of CLBP disability (88.1%) Factors associated with greater CLBP disability pain intensity, longer days of work absence, BBDS Factors associated with lesser CLBP disability alcohol consumption, higher psychological wellbeing scores |
| Score Weight | 0.2 | 0.08 | 0.2 | 0.2 | 0.08 | 0.08 | 0.08 | 0.08 | Total Score |
|---|---|---|---|---|---|---|---|---|---|
| Study ID | Was the Sampling Frame a True or Close Representation of the Target Population | Was the Sample Size Estimated? | Was Some Form of Random Selection Used to Select Sample or Was a Census Undertaken? | Was the Likelihood of Nonresponse Bias Minimal? | Were Data Collected Directly from the Subjects (as Opposed to a Proxy)? | Had the Study Instrument That Measured the Parameter of Interest (e.g., CLBP Prevalence) Been Tested for Reliability and Validity? | Was Data Collection Standardized? | Was a Human Body Drawing Used | |
| Igwesi-Chidobe et al. [24] | Yes | No | Yes | Yes | Yes | Yes | Yes | No | 0.84 |
| Omoke et al. [25] | Yes | No | No | Yes | Yes | Yes | Yes | No | 0.64 |
| Tella et al. [26] | Yes | No | No | No | Yes | Yes | Yes | No | 0.44 |
| Nakua et al. [27] | Yes | No | Yes | Yes | Yes | Yes | Yes | No | 0.84 |
| Kedebe et al. [1] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | 0.92 |
| Yosef et al. [28] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | 0.92 |
| Beyera et al. [29] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | 0.92 |
| Kahere et al. [30] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | 0.92 |
| Kahere et al. [31] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | 0.92 |
| Major-Helsloot et al. [32] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | 0.92 |
| Doualla et al. [33] | Yes | No | Ye | No | Yes | Yes | Yes | Yes | 0.84 |
| Author and Publication Year | Country | Study Setting | Design | Sampling Method | Sample Size | Population Description | Age |
|---|---|---|---|---|---|---|---|
| Igwesi-Chidobe et al. [24] | Nigeria | Population-based | Cross-sectional | Random | N = 200 Female = 112 Male = 88 | General population | 48.6 (12.0) years |
| Omoke et al. [25] | Nigeria | Hospital-based | Cross-sectional | NR | N = 291 Femalen = 143 Malen= 148 | General population | 45.8 ± 1.67 years |
| Tella et al. [26] | Nigeria | Population based | Cross-sectional | NR | N = 604 Femalen = 236 Malen = 368 | Farmers | NR |
| Nakua et al. [27] | Ghana | Population-based | Cross-sectional | NR | N = 4724 Rural: [N = 2799, Women = 1333 Men = 1466] Urban: [N = 1925, Women = 1 Men = 881] | General population | Rural: Female = 64.9 (95%CI: 64.4, 65.5) Male = 64.1 (95%CI: 63.6, 64.7) |
| Kahere et al. [30] | South Africa | Hospital-based | Cross-sectional | Random | N = 678 Femalen = 394 Malen = 284 | General population | NR |
| Kahere et al. [31] | South Africa | Hospital-based | Cross-sectional | Random | N = 554 Femalen = 326 Malen = 228 | General population | 45.8 ± 10.7 |
| Major-Helsloot et al. [32] | South Africa | Health facility based | Cross-sectional | Random | N = 504 Famalen = 374 Malen = 130 | General population | 44.8 (SD ± 13.95) |
| Kebede et al. [1] | Ethiopia | Primary schools | Cross-sectional | Random | N = 611 Femalen = 331 Malen = 280 | Teachers | 40 (±9.38) years |
| Yosef et al. [28] | Ethiopia | Port-based | Cross-sectional | Random | N = 422 | Truck drivers | 37.7 (±9.13 SD) years |
| Beyera et al. [29] | Ethiopia | Population-based | Cross-sectional | Random | N = 543 Femalen = 227 Malen = 316 | General population | 43 years (interquartile range 33–55 years) |
| Doualla et al. [33] | Cameroon | Hospital-based | Cross-sectional | Random | N = 136 Femalen = 87 Malen = 48 | General population | 50.6 ± 12.2 |
| Prevalence of CLBP among Occupations | ||||
|---|---|---|---|---|
| Author | Year | Country | Occupation | Prevalence of CLBP |
| Kebede et al. | 2019 | Ethiopia | Primary school teachers | 30.1% |
| Tella et al. | 2013 | Nigeria | Farmers | 48.5% |
| Yosef et al. | 2019 | Nigeria | Truck drivers | 55.5% |
| Prevalence of CLBP among LBP Patients | ||||
| Author | Year | Country | Population | Prevalence of CLBP |
| Omoke et al. | 2016 | Nigeria | LBP patients | 59.1% |
| Beyera et al. | 2020 | Ethiopia | LBP patients | 38.7% for >1 year |
| Doualla et al. | 2019 | Cameroon | LBP patients | 41.0% |
| Kahere et al. | 2022 | South Africa | LBP patients | 22.2% |
| Prevalence of CLBP among the General Population | ||||
| Nakua et al. | 2015 | Ghana | General population | 28.2% |
| Major-Helsloot et al. | 2014 | S. Africa | General population | 26.3% |
| Kahere et al. | 2021 | S. Africa | General population | 18.1% |
| SSA Region | Countries | No. of Studies | Outcome Measure (s) | Main Findings | Gender-Based Differences |
|---|---|---|---|---|---|
| West Africa | Nigeria, Ghana | 4 | CLBP Prevalence Risk factors CLBP disability Etiology Pattern of presentation CLBP burden | Prevalence of: CLBP—28.2–48.5% Self-reported CLBP disability—62.5% Performance-based disability—49.1% Risk factors of: CLBP—lifting heavy objects, history of back injury, obesity, pregnancy, long distance driving, prolonged bending Self-reported CLBP disability—abnormal illness perception, severe pain intensity, catastrophizing, fear avoidance beliefs, anxiety Performance-based disability—abnormal illness perception, lack of social support, fear avoidance beliefs, female gender Comorbidities—hypertension, peptic ulcers, diabetes mellitus, knee and hip osteoarthritis, cervical spondylosis Etiology Lumbosacral spondylosis, degenerative spondylolisthesis, | Prevalence of CLBP F(uneducated) (36.2%) > M(uneducated) (29.0%) F(professionals) (40.8%) > M(professionals) (28.0%) M(single) > M(married) F(married) > M(single) Incidence F (53.1%) > M (46.9%) Etiology Females—spondylosis, spondylolisthesis, sacroiliac joint strain and back strain Males—disc prolapse |
| East Africa | Ethiopia | 3 | CLBP Prevalence Admission rate Factors associated with healthcare presentation for LBP | Prevalence 30.1% Risk factors Smoking, physical inactivity, chronic diseases, frequent lifting and carrying heavy objects Admission rate 14.4% (95%CI: 11.4–17.3) Factors associated with LBP presentation Lack of social or family support (living alone) Alcohol consumption Severe pain Presence of additional spinal pain | Prevalence—no gender stratified analysis Risk factors—no gender stratified analysis Admission rate F (18.5%) > M (11.4%) |
| Southern Africa | South Africa | 3 | CLBP prevalence Risk factors Management | Prevalence 18.1–26.3 Risk factors Lifestyle: (Overweight, smoking, alcohol consumption, lack of regular physical exercise) Occupational: (prolonged sitting, manual work, stooped posture) Socioeconomic: (illiteracy) Psychological: (disease conviction, affective disturbance, denial, fear avoidance beliefs about work) Management Biomedically oriented, mainly pain medication, rare physiotherapy referral, no advice given, low level of patient satisfaction | Prevalence F (19.8—23.9) M (15.9—19.7) Risk Factors Female gander was a significant risk factor for CLBP (aOR = 12.4; 95%CI: 3.1–49.8; p-value < 0.001) Management Management was unrelated to the type of gender |
| Central Africa | Cameroon | 1 | CLBP disability | Risk factors Greater disability: (Pain intensity, longer days of work absenteeism, bladder and bowel dysfunction syndrome) Lesser disability: (alcohol consumption, psychological well-being) | F (64%); M (36%) No gender stratified analysis performed |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kahere, M.; Hlongwa, M.; Ginindza, T.G. A Scoping Review on the Epidemiology of Chronic Low Back Pain among Adults in Sub-Saharan Africa. Int. J. Environ. Res. Public Health 2022, 19, 2964. https://doi.org/10.3390/ijerph19052964
Kahere M, Hlongwa M, Ginindza TG. A Scoping Review on the Epidemiology of Chronic Low Back Pain among Adults in Sub-Saharan Africa. International Journal of Environmental Research and Public Health. 2022; 19(5):2964. https://doi.org/10.3390/ijerph19052964
Chicago/Turabian StyleKahere, Morris, Mbuzeleni Hlongwa, and Themba G. Ginindza. 2022. "A Scoping Review on the Epidemiology of Chronic Low Back Pain among Adults in Sub-Saharan Africa" International Journal of Environmental Research and Public Health 19, no. 5: 2964. https://doi.org/10.3390/ijerph19052964
APA StyleKahere, M., Hlongwa, M., & Ginindza, T. G. (2022). A Scoping Review on the Epidemiology of Chronic Low Back Pain among Adults in Sub-Saharan Africa. International Journal of Environmental Research and Public Health, 19(5), 2964. https://doi.org/10.3390/ijerph19052964