
Oral-Hygiene-Related Mobile Apps in the French App Stores: Assessment of Functionality and Quality

 ,
,  ,
,  , and
, and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Selection of Oral Health Professionals
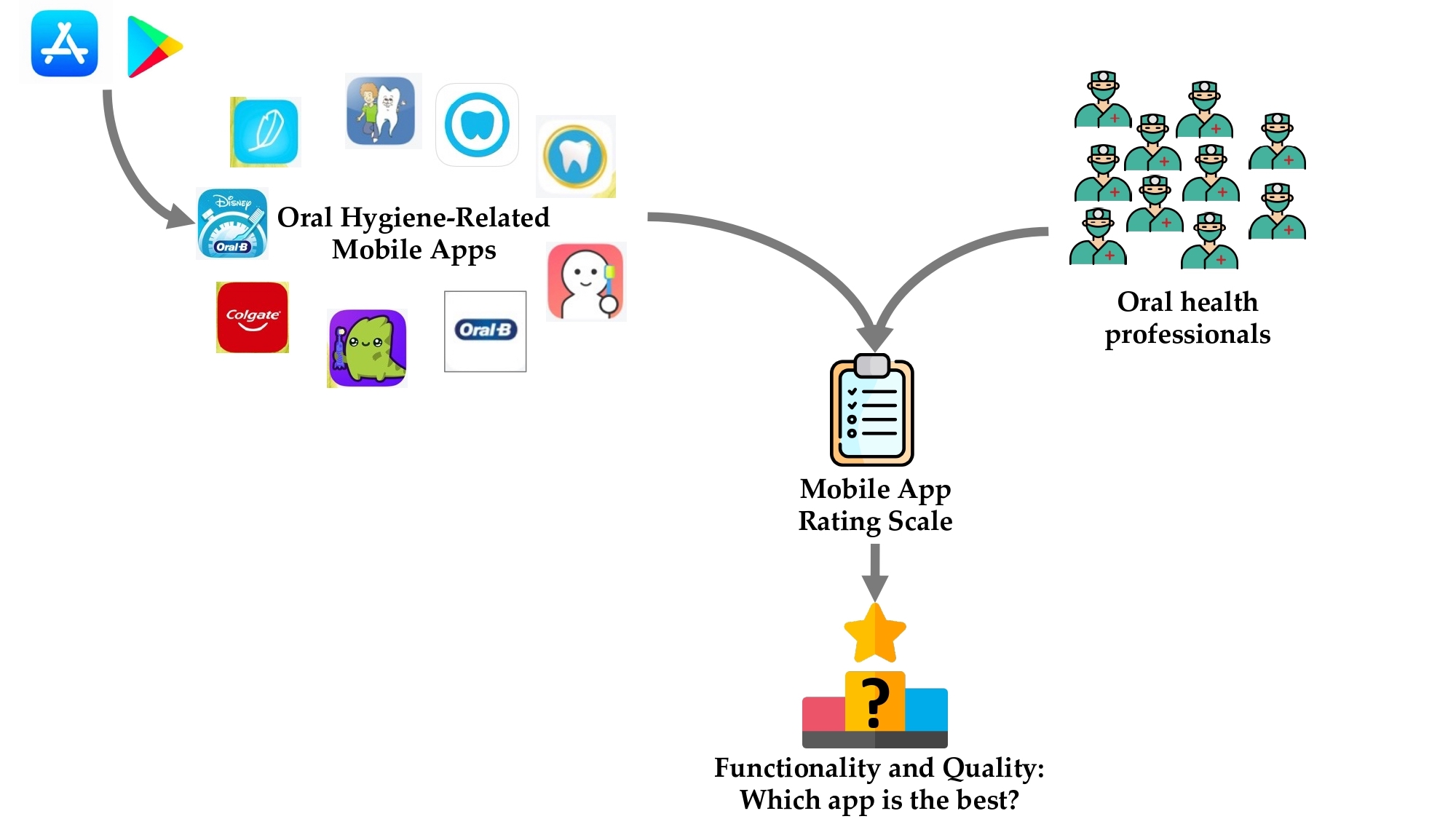
2.3. Selection of the Oral-Hygiene-Related Mobile Apps in the French App Stores
2.4. Evaluation of the Oral-Hygiene-Related Mobile Apps in the French App Stores
2.4.1. Use of the Standardized Rating Scale for Mobile Applications
2.4.2. Evaluation of the Apps by Raters
2.5. Statistical Analysis
3. Results
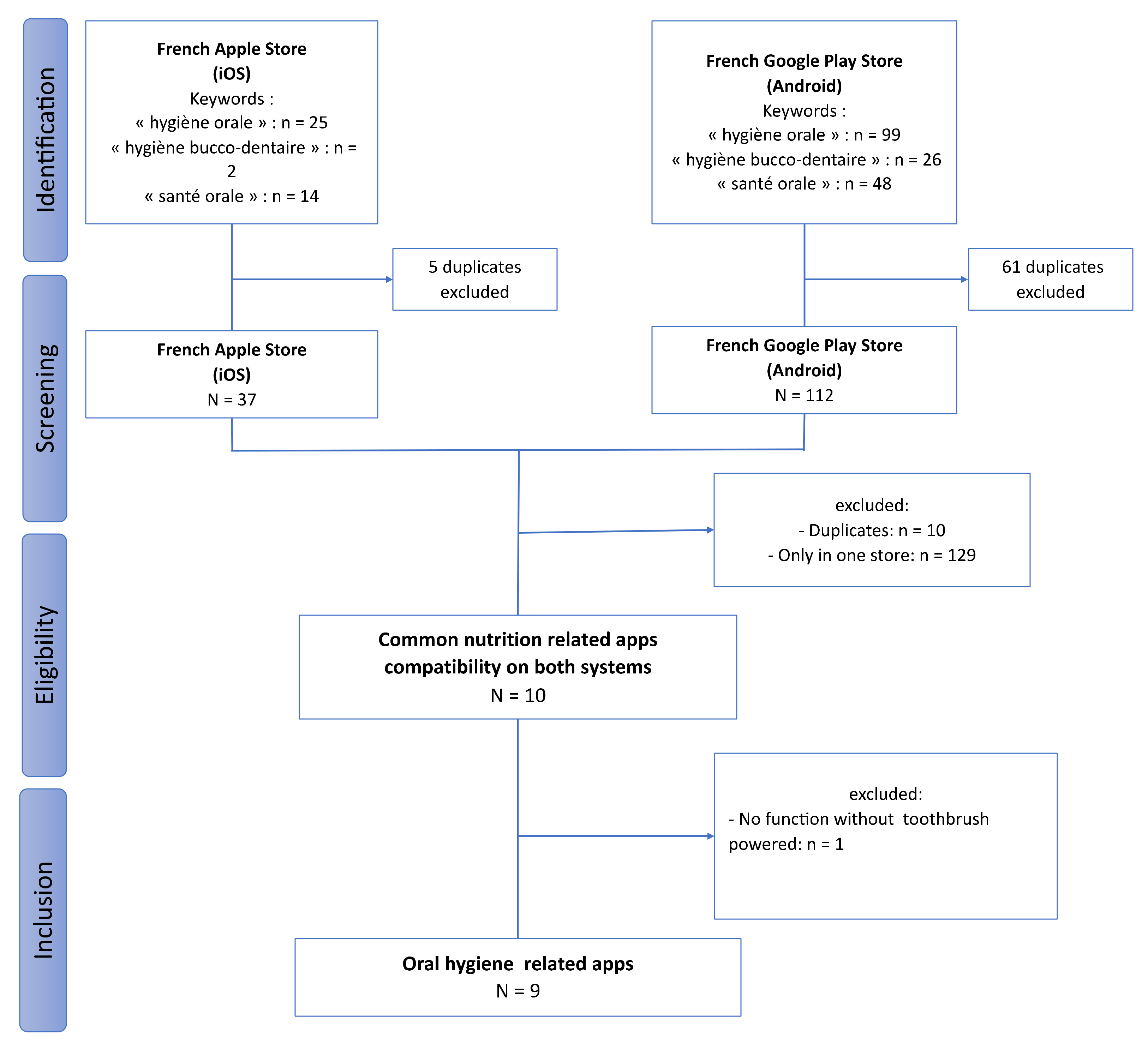
3.1. Selection of the Oral-Hygiene-Related Mobile Apps
3.2. Characteristics of the Oral-Hygiene-Related Mobile Apps
3.3. Reliability of the Evaluation
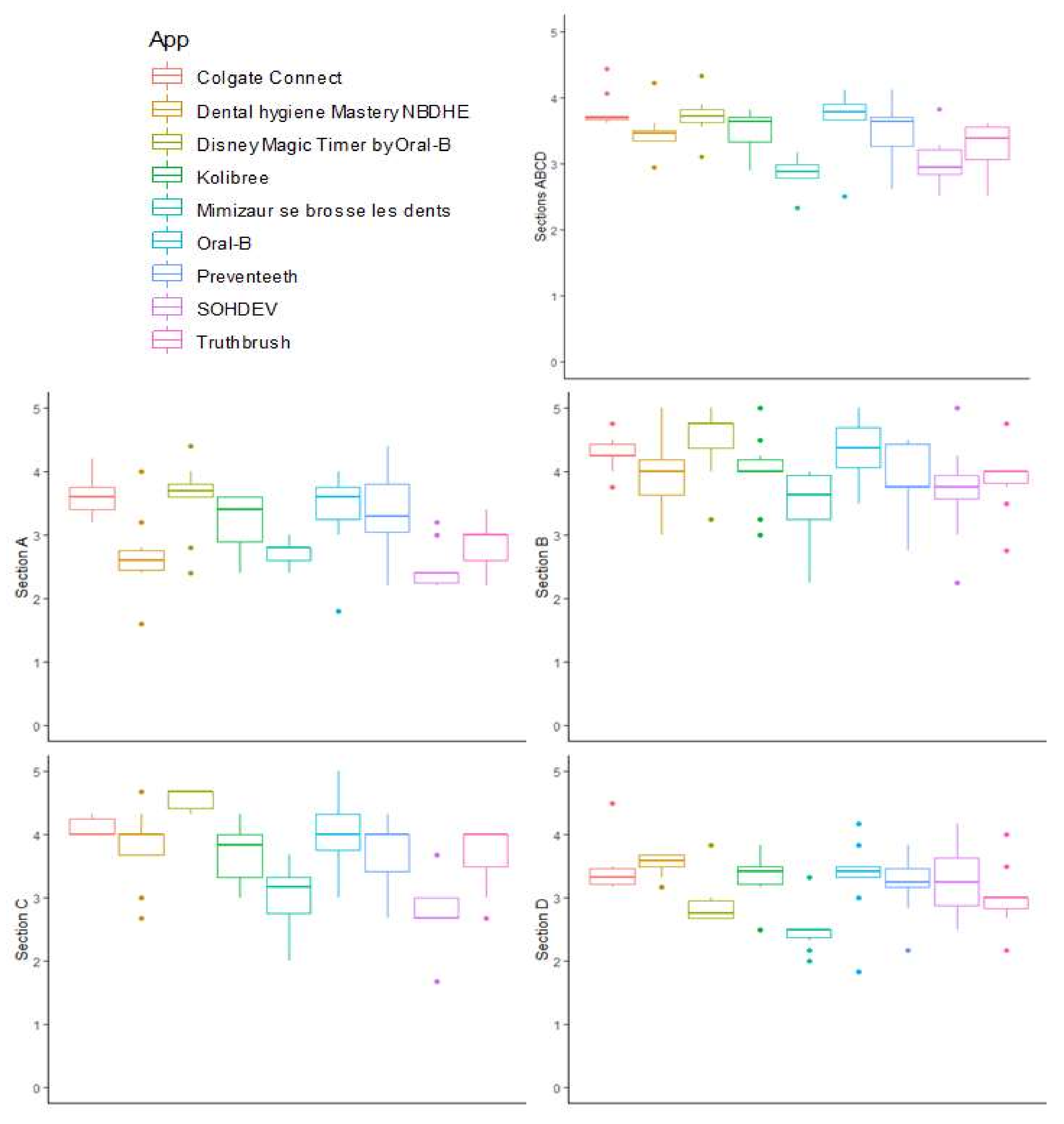
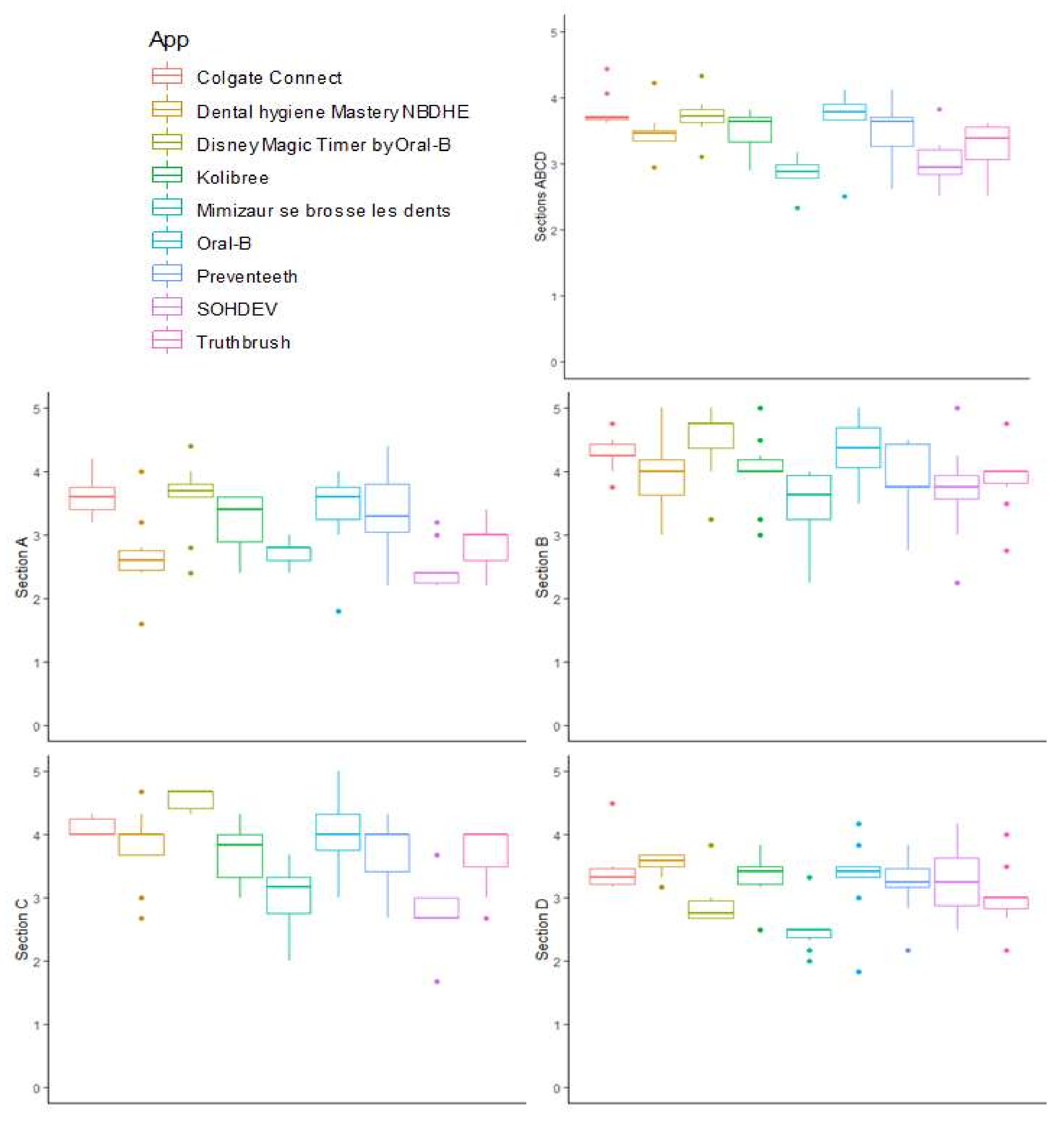
3.4. Qualitative Assessment of Oral-Health-Related Mobile App Content
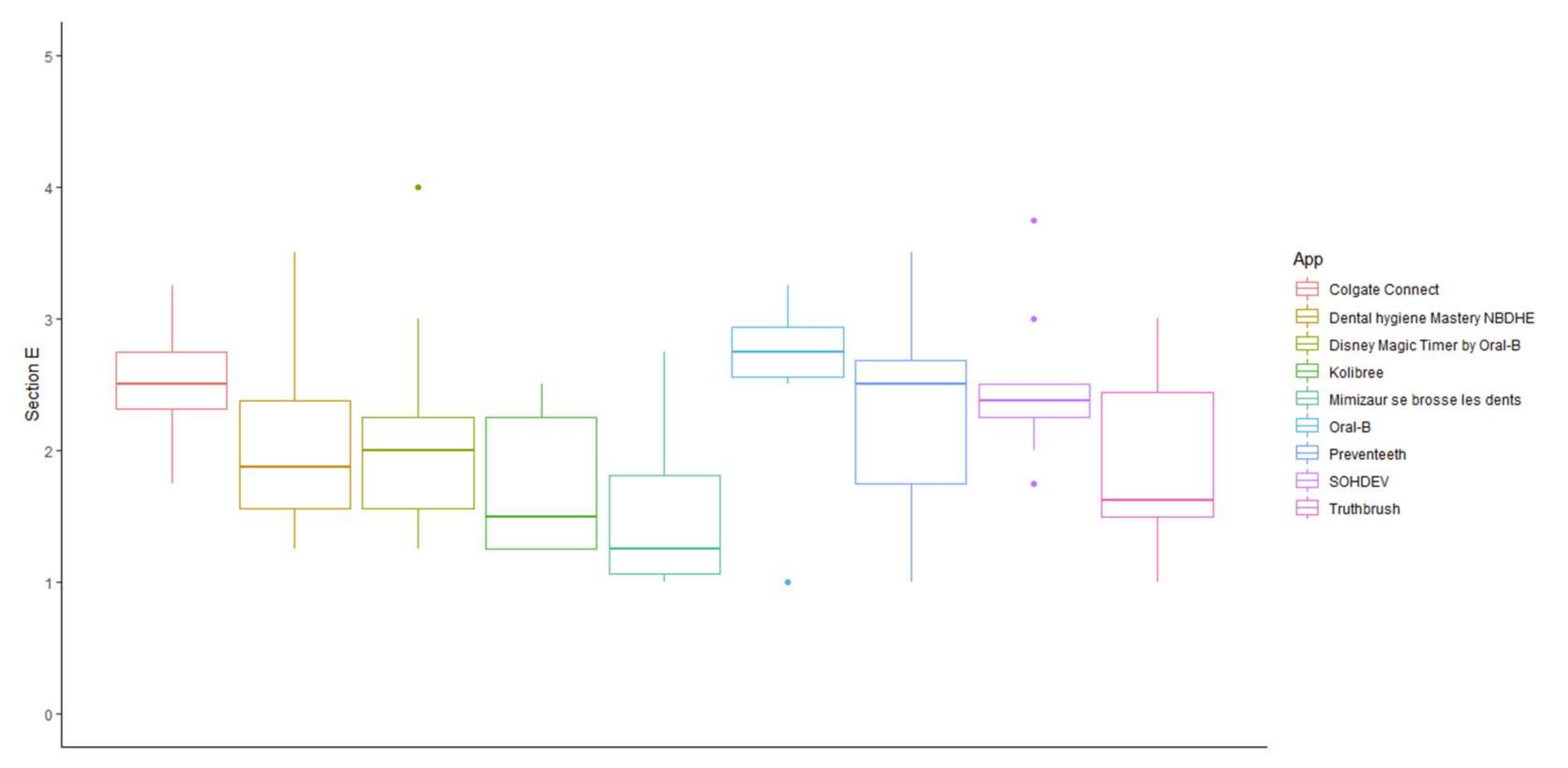
3.5. Assessing the Content Specificity of Oral-Health-Related Mobile Applications
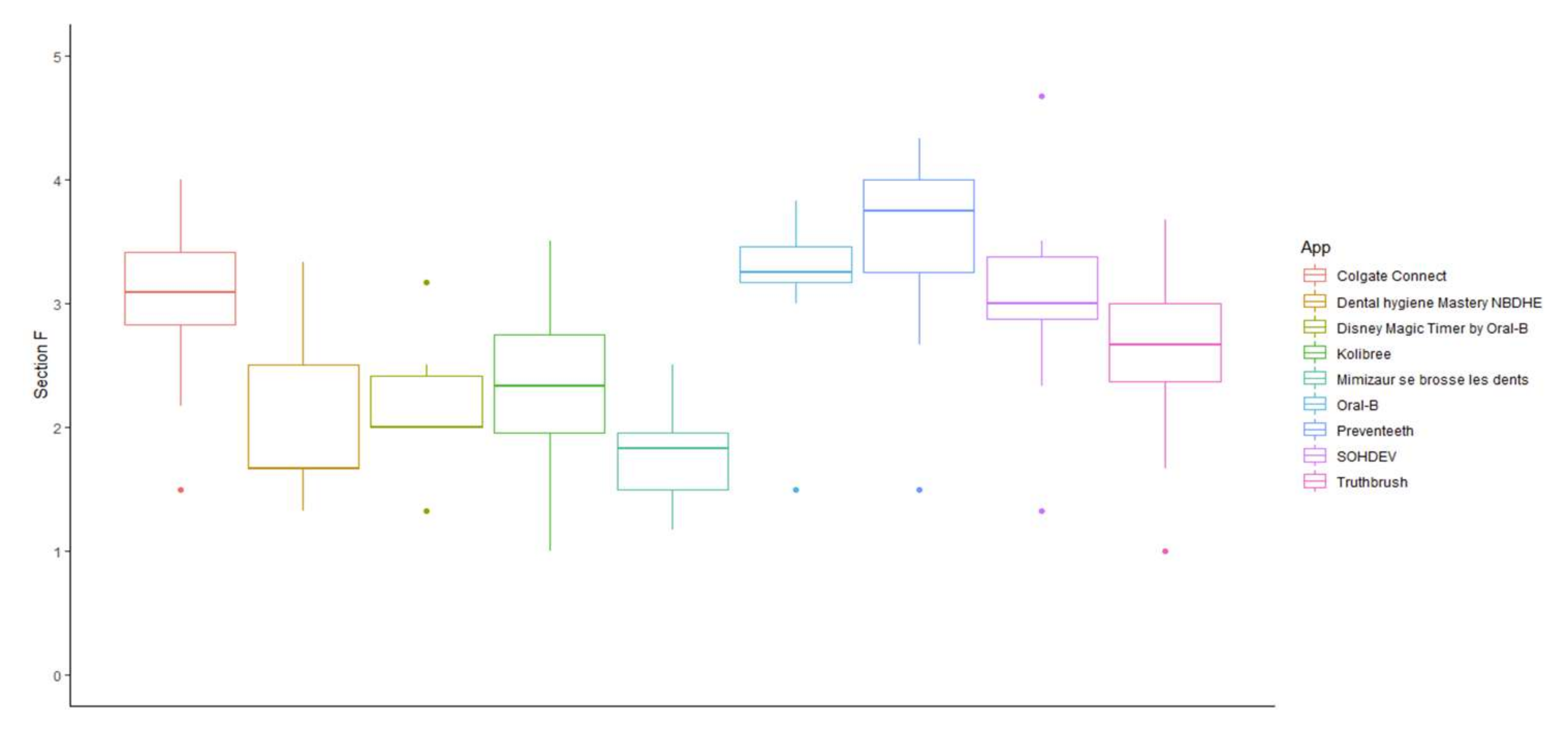
3.6. Strengths and Weaknesses of Each Oral-Health-Related Mobile Application
3.7. Comparison of MARS Score and Star Rating
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pitts, N.B.; Twetman, S.; Fisher, J.; Marsh, P.D. Understanding Dental Caries as a Non-Communicable Disease. Br. Dent. J. 2021, 231, 749–753. [Google Scholar] [CrossRef]
- Bawaskar, H.S.; Bawaskar, P.H. Oral Diseases: A Global Public Health Challenge. Lancet 2020, 395, 185–186. [Google Scholar] [CrossRef] [Green Version]
- Righolt, A.J.; Jevdjevic, M.; Marcenes, W.; Listl, S. Global-, Regional-, and Country-Level Economic Impacts of Dental Diseases in 2015. J. Dent. Res. 2018, 97, 501–507. [Google Scholar] [CrossRef]
- GBD 2017 Oral Disorders Collaborators; Bernabe, E.; Marcenes, W.; Hernandez, C.R.; Bailey, J.; Abreu, L.G.; Alipour, V.; Amini, S.; Arabloo, J.; Arefi, Z.; et al. Global, Regional, and National Levels and Trends in Burden of Oral Conditions from 1990 to 2017: A Systematic Analysis for the Global Burden of Disease 2017 Study. J. Dent. Res. 2020, 99, 362–373. [Google Scholar] [CrossRef]
- Wolf, T.G.; Cagetti, M.G.; Fisher, J.-M.; Seeberger, G.K.; Campus, G. Non-Communicable Diseases and Oral Health: An Overview. Front. Oral Health 2021, 2, 725460. [Google Scholar] [CrossRef]
- Bourgeois, D.; Gonçalves, L.S.; Lima-Junior, J.D.C.; Carrouel, F. Editorial: The Oral Microbiome Is a Key Factor in Oral and Systemic Health. Front. Microbiol 2022, 13, 855668. [Google Scholar] [CrossRef]
- Maitre, Y.; Mahalli, R.; Micheneau, P.; Delpierre, A.; Amador, G.; Denis, F. Evidence and Therapeutic Perspectives in the Relationship between the Oral Microbiome and Alzheimer’s Disease: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 11157. [Google Scholar] [CrossRef]
- Borsa, L.; Dubois, M.; Sacco, G.; Lupi, L. Analysis the Link between Periodontal Diseases and Alzheimer’s Disease: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 9312. [Google Scholar] [CrossRef]
- Bourgeois, D.; Inquimbert, C.; Ottolenghi, L.; Carrouel, F. Periodontal Pathogens as Risk Factors of Cardiovascular Diseases, Diabetes, Rheumatoid Arthritis, Cancer, and Chronic Obstructive Pulmonary Disease-Is There Cause for Consideration? Microorganisms 2019, 7, 424. [Google Scholar] [CrossRef] [Green Version]
- Gare, J.; Kanoute, A.; Meda, N.; Viennot, S.; Bourgeois, D.; Carrouel, F. Periodontal Conditions and Pathogens Associated with Pre-Eclampsia: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 7194. [Google Scholar] [CrossRef]
- Duangthip, D.; Chu, C.H. Challenges in Oral Hygiene and Oral Health Policy. Front. Oral Health 2020, 1, 7. [Google Scholar] [CrossRef]
- Bourgeois, D.; Bravo, M.; Llodra, J.-C.; Inquimbert, C.; Viennot, S.; Dussart, C.; Carrouel, F. Calibrated Interdental Brushing for the Prevention of Periodontal Pathogens Infection in Young Adults—A Randomized Controlled Clinical Trial. Sci. Rep. 2019, 9, 15127. [Google Scholar] [CrossRef] [Green Version]
- Bourgeois, D.; Saliasi, I.; Llodra, J.C.; Bravo, M.; Viennot, S.; Carrouel, F. Efficacy of Interdental Calibrated Brushes on Bleeding Reduction in Adults: A 3-Month Randomized Controlled Clinical Trial. Eur. J. Oral Sci. 2016, 124, 566–571. [Google Scholar] [CrossRef]
- Urquhart, O.; Tampi, M.P.; Pilcher, L.; Slayton, R.L.; Araujo, M.W.B.; Fontana, M.; Guzmán-Armstrong, S.; Nascimento, M.M.; Nový, B.B.; Tinanoff, N.; et al. Nonrestorative Treatments for Caries: Systematic Review and Network Meta-Analysis. J. Dent. Res. 2019, 98, 14–26. [Google Scholar] [CrossRef]
- Heilmann, A.; Tsakos, G.; Watt, R.G. Oral Health Over the Life Course. In A Life Course Perspective on Health Trajectories and Transitions; Burton-Jeangros, C., Cullati, S., Sacker, A., Blane, D., Eds.; Springer: Cham, Switzerland, 2015; ISBN 978-3-319-20483-3. [Google Scholar]
- Ahmadi, S.; Klingelhöfer, D.; Erbe, C.; Holzgreve, F.; Groneberg, D.A.; Ohlendorf, D. Oral Health: Global Research Performance under Changing Regional Health Burdens. Int. J. Environ. Res. Public Health 2021, 18, 5743. [Google Scholar] [CrossRef]
- Watt, R.G.; Daly, B.; Allison, P.; Macpherson, L.M.D.; Venturelli, R.; Listl, S.; Weyant, R.J.; Mathur, M.R.; Guarnizo-Herreño, C.C.; Celeste, R.K.; et al. Ending the Neglect of Global Oral Health: Time for Radical Action. Lancet 2019, 394, 261–272. [Google Scholar] [CrossRef]
- Grzesikowski, T.J. The Impact of Leadership and Research on Decision Making: Who Is Going to Lead the Transformation of Dental Hygiene? J. Dent. Hyg. 2016, 90, 73–74. [Google Scholar]
- Oral Health: Prevention Is Key. Lancet 2009, 373, 1. [CrossRef]
- Moorhead, S.A.; Hazlett, D.E.; Harrison, L.; Carroll, J.K.; Irwin, A.; Hoving, C. A New Dimension of Health Care: Systematic Review of the Uses, Benefits, and Limitations of Social Media for Health Communication. J. Med. Internet Res. 2013, 15, e1933. [Google Scholar] [CrossRef] [Green Version]
- Ma, X.; Lu, J.; Liu, W. Influencing Factors on Health Information to Improve Public Health Literacy in the Official WeChat Account of Guangzhou CDC. Front. Public Health 2021, 9, 657082. [Google Scholar] [CrossRef]
- WHO Global Observatory for eHealth. MHealth: New Horizons for Health through Mobile Technologies: Second Global Survey on EHealth; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Timmers, T.; Janssen, L.; Kool, R.B.; Kremer, J.A. Educating Patients by Providing Timely Information Using Smartphone and Tablet Apps: Systematic Review. J. Med. Internet Res. 2020, 22, e17342. [Google Scholar] [CrossRef]
- Tabi, K.; Randhawa, A.S.; Choi, F.; Mithani, Z.; Albers, F.; Schnieder, M.; Nikoo, M.; Vigo, D.; Jang, K.; Demlova, R.; et al. Mobile Apps for Medication Management: Review and Analysis. JMIR Mhealth Uhealth 2019, 7, e13608. [Google Scholar] [CrossRef] [Green Version]
- Martinon, P.; Fraticelli, L.; Giboreau, A.; Dussart, C.; Bourgeois, D.; Carrouel, F. Nutrition as a Key Modifiable Factor for Periodontitis and Main Chronic Diseases. J. Clin. Med. 2021, 10, 197. [Google Scholar] [CrossRef]
- Van Gaalen, A.E.J.; Brouwer, J.; Schönrock-Adema, J.; Bouwkamp-Timmer, T.; Jaarsma, A.D.C.; Georgiadis, J.R. Gamification of Health Professions Education: A Systematic Review. Adv. Health Sci. Educ. Theory Pract. 2021, 26, 683–711. [Google Scholar] [CrossRef]
- Kim, J.; Castelli, D.M. Effects of Gamification on Behavioral Change in Education: A Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 3550. [Google Scholar] [CrossRef]
- Underwood, B.; Birdsall, J.; Kay, E. The Use of a Mobile App to Motivate Evidence-Based Oral Hygiene Behaviour. Br. Dent. J. 2015, 219, E2. [Google Scholar] [CrossRef]
- Zahid, T.; Alyafi, R.; Bantan, N.; Alzahrani, R.; Elfirt, E. Comparison of Effectiveness of Mobile App versus Conventional Educational Lectures on Oral Hygiene Knowledge and Behavior of High School Students in Saudi Arabia. Patient Prefer. Adherence 2020, 14, 1901–1909. [Google Scholar] [CrossRef]
- Scheerman, J.F.M.; van Meijel, B.; van Empelen, P.; Verrips, G.H.W.; van Loveren, C.; Twisk, J.W.R.; Pakpour, A.H.; van den Braak, M.C.T.; Kramer, G.J.C. The Effect of Using a Mobile Application (“WhiteTeeth”) on Improving Oral Hygiene: A Randomized Controlled Trial. Int. J. Dent. Hyg. 2020, 18, 73–83. [Google Scholar] [CrossRef]
- Akmal Muhamat, N.; Hasan, R.; Saddki, N.; Mohd Arshad, M.R.; Ahmad, M. Development and Usability Testing of Mobile Application on Diet and Oral Health. PLoS ONE 2021, 16, e0257035. [Google Scholar] [CrossRef]
- Zolfaghari, M.; Shirmohammadi, M.; Shahhosseini, H.; Mokhtaran, M.; Mohebbi, S.Z. Development and Evaluation of a Gamified Smart Phone Mobile Health Application for Oral Health Promotion in Early Childhood: A Randomized Controlled Trial. BMC Oral Health 2021, 21, 18. [Google Scholar] [CrossRef]
- Haute Autorité de Santé. Assessment of Apps in the Mobile Health (MHealth) Sector-Overview and Quality Criteria of Medical Content for Referencing Digital Services in the Digital Health Space and the Professional Service Package; Haute Autorité de Santé: Saint-Denis, France, 2021; pp. 1–85. [Google Scholar]
- Zhao, J.; Harvey, G.; Vandyk, A.; Gifford, W. Social Media for ImpLementing Evidence (SMILE): Conceptual Framework. JMIR Form. Res. 2022, 6, e29891. [Google Scholar] [CrossRef] [PubMed]
- Saliasi, I.; Martinon, P.; Darlington, E.; Smentek, C.; Tardivo, D.; Bourgeois, D.; Dussart, C.; Carrouel, F.; Fraticelli, L. Promoting Health via MHealth Applications Using a French Version of the Mobile App Rating Scale: Adaptation and Validation Study. JMIR Mhealth Uhealth 2021, 9, e30480. [Google Scholar] [CrossRef] [PubMed]
- Stoyanov, S.R.; Hides, L.; Kavanagh, D.J.; Zelenko, O.; Tjondronegoro, D.; Mani, M. Mobile App Rating Scale: A New Tool for Assessing the Quality of Health Mobile Apps. JMIR Mhealth Uhealth 2015, 3, e27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grainger, R.; Townsley, H.; White, B.; Langlotz, T.; Taylor, W.J. Apps for People with Rheumatoid Arthritis to Monitor Their Disease Activity: A Review of Apps for Best Practice and Quality. JMIR Mhealth Uhealth 2017, 5, e7. [Google Scholar] [CrossRef] [Green Version]
- Masterson Creber, R.M.; Maurer, M.S.; Reading, M.; Hiraldo, G.; Hickey, K.T.; Iribarren, S. Review and Analysis of Existing Mobile Phone Apps to Support Heart Failure Symptom Monitoring and Self-Care Management Using the Mobile Application Rating Scale (MARS). JMIR Mhealth Uhealth 2016, 4, e74. [Google Scholar] [CrossRef] [PubMed]
- Salazar, A.; de Sola, H.; Failde, I.; Moral-Munoz, J.A. Measuring the Quality of Mobile Apps for the Management of Pain: Systematic Search and Evaluation Using the Mobile App Rating Scale. JMIR Mhealth Uhealth 2018, 6, e10718. [Google Scholar] [CrossRef] [PubMed]
- Shrout, P.E.; Fleiss, J.L. Intraclass Correlations: Uses in Assessing Rater Reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Tiffany, B.; Blasi, P.; Catz, S.L.; McClure, J.B. Mobile Apps for Oral Health Promotion: Content Review and Heuristic Usability Analysis. JMIR Mhealth Uhealth 2018, 6, e11432. [Google Scholar] [CrossRef]
- Sharif, M.O.; Alkadhimi, A. Patient Focused Oral Hygiene Apps: An Assessment of Quality (Using MARS) and Knowledge Content. Br. Dent. J. 2019, 227, 383–386. [Google Scholar] [CrossRef]
- Parker, K.; Bharmal, R.V.; Sharif, M.O. The Availability and Characteristics of Patient-Focused Oral Hygiene Apps. Br. Dent. J. 2019, 226, 600–604. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Santo, K.; Wong, G.; Sohn, W.; Spallek, H.; Chow, C.; Irving, M. Mobile Apps for Dental Caries Prevention: Systematic Search and Quality Evaluation. JMIR Mhealth Uhealth 2021, 9, e19958. [Google Scholar] [CrossRef] [PubMed]
- Petker, W.; Weik, U.; Margraf-Stiksrud, J.; Deinzer, R. Oral Cleanliness in Daily Users of Powered vs. Manual Toothbrushes—A Cross-Sectional Study. BMC Oral Health 2019, 19, 96. [Google Scholar] [CrossRef] [PubMed]
- Eidenhardt, Z.; Ritsert, A.; Shankar-Subramanian, S.; Ebel, S.; Margraf-Stiksrud, J.; Deinzer, R. Tooth Brushing Performance in Adolescents as Compared to the Best-Practice Demonstrated in Group Prophylaxis Programs: An Observational Study. BMC Oral Health 2021, 21, 359. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General. J. Calif. Dent. Assoc. 2000, 28, 685–695. [Google Scholar]
- De Chantal, P.-L.; Chagnon, A.; Cardinal, M.; Faieta, J.; Guertin, A. Evidence of User-Expert Gaps in Health App Ratings and Implications for Practice. Front. Digit. Health 2022, 4, 765993. [Google Scholar] [CrossRef]
- Schumer, H.; Amadi, C.; Joshi, A. Evaluating the Dietary and Nutritional Apps in the Google Play Store. Healthc. Inform. Res. 2018, 24, 38–45. [Google Scholar] [CrossRef] [Green Version]
- Fijačko, N.; Gosak, L.; Cilar, L.; Novšak, A.; Creber, R.M.; Skok, P.; Štiglic, G. The Effects of Gamification and Oral Self-Care on Oral Hygiene in Children: Systematic Search in App Stores and Evaluation of Apps. JMIR Mhealth Uhealth 2020, 8, e16365. [Google Scholar] [CrossRef]
- Stoyanov, S.R.; Hides, L.; Kavanagh, D.J.; Wilson, H. Development and Validation of the User Version of the Mobile Application Rating Scale (UMARS). JMIR Mhealth Uhealth 2016, 4, e72. [Google Scholar] [CrossRef] [Green Version]
- Martinon, P.; Saliasi, I.; Bourgeois, D.; Smentek, C.; Dussart, C.; Fraticelli, L.; Carrouel, F. Nutrition-Related Mobile Apps in the French App Stores: Assessment of Functionality and Quality. JMIR Mhealth Uhealth 2022, 10, e35879. [Google Scholar] [CrossRef]
- Becker, S.; Miron-Shatz, T.; Schumacher, N.; Krocza, J.; Diamantidis, C.; Albrecht, U.-V. MHealth 2.0: Experiences, Possibilities, and Perspectives. JMIR Mhealth Uhealth 2014, 2, e3328. [Google Scholar] [CrossRef] [PubMed]
- Talwar, D.; Yeh, Y.-L.; Chen, W.-J.; Chen, L.-S. Characteristics and Quality of Genetics and Genomics Mobile Apps: A Systematic Review. Eur. J. Hum. Genet. 2019, 27, 833–840. [Google Scholar] [CrossRef] [PubMed]
- Ciapponi, A.; Donato, M.; Gülmezoglu, A.M.; Alconada, T.; Bardach, A. Mobile Apps for Detecting Falsified and Substandard Drugs: A Systematic Review. PLoS ONE 2021, 16, e0246061. [Google Scholar] [CrossRef] [PubMed]
- Mandracchia, F.; Llauradó, E.; Tarro, L.; Valls, R.M.; Solà, R. Mobile Phone Apps for Food Allergies or Intolerances in App Stores: Systematic Search and Quality Assessment Using the Mobile App Rating Scale (MARS). JMIR Mhealth Uhealth 2020, 8, e18339. [Google Scholar] [CrossRef]
- Romero, R.L.; Kates, F.; Hart, M.; Ojeda, A.; Meirom, I.; Hardy, S. Quality of Deaf and Hard-of-Hearing Mobile Apps: Evaluation Using the Mobile App Rating Scale (MARS) With Additional Criteria from a Content Expert. JMIR Mhealth Uhealth 2019, 7, e14198. [Google Scholar] [CrossRef]
- Escriche-Escuder, A.; De-Torres, I.; Roldán-Jiménez, C.; Martín-Martín, J.; Muro-Culebras, A.; González-Sánchez, M.; Ruiz-Muñoz, M.; Mayoral-Cleries, F.; Biró, A.; Tang, W.; et al. Assessment of the Quality of Mobile Applications (Apps) for Management of Low Back Pain Using the Mobile App Rating Scale (MARS). Int. J. Environ. Res. Public Health 2020, 17, E9209. [Google Scholar] [CrossRef]
- DiFilippo, K.N.; Huang, W.; Chapman-Novakofski, K.M. A New Tool for Nutrition App Quality Evaluation (AQEL): Development, Validation, and Reliability Testing. JMIR Mhealth Uhealth 2017, 5, e163. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | App (n = 9), n (%) 1 |
|---|---|
| Focus or target | |
| Increase happiness or wellbeing | 9 (100) |
| Behavior change | 8 (88.9) |
| Entertainment | 8 (88.9) |
| Goal-setting | 7 (77.8) |
| Theoretical background or strategies | |
| Assessment | 6 (66.7) |
| Feedback | 5 (55.6) |
| Information/Education | 9 (100) |
| Monitoring/Tracking | 6 (66.7) |
| Goal-setting | 7 (77.8) |
| Advice/Tips/Strategies/Skills training | 7 (77.8) |
| CBT–Behavioral (positive events) | 6 (66.7) |
| Gratitude | 7 (77.8) |
| Strengths-based | 5 (55.6) |
| Age group | |
| Children (under 12 years) | 3 (33.3) |
| Adolescents (13–17 years) | 7 (77.8) |
| Young adults (18–25 years) | 7 (77.8) |
| Adults | 7 (77.8) |
| Technical aspects of app | |
| Allows sharing (Facebook, Twitter, etc.) | 2 (22.2) |
| Allows password-protection | 3 (33.3) |
| Requires login | 3 (33.3) |
| Sends reminders | 5 (55.6) |
| Colgate Connect | Dental Hygiene Mastery NBDHE | Disney magic Timer by Oral-B | Kolibree | Mimizaur se brosse les dents | Oral-B | Preventeeth | SOHDEV | Truthbrush | |
|---|---|---|---|---|---|---|---|---|---|
| Section A | |||||||||
| Item 1—Entertainment | 3.2 | 2.5 | 4.3 | 3.5 | 3.5 | 3.5 | 3.9 | 3.1 | 2.7 |
| Item 2—Interest | 3.3 | 3.1 | 4 | 3.5 | 3.3 | 3.9 | 4 | 3.3 | 3 |
| Item 3—Customisation | 3.8 | 2.9 | 2.9 | 3 | 1.9 | 2.9 | 3 | 1.4 | 2.9 |
| Item 4—Interactivity | 3.8 | 2.1 | 2.7 | 2.9 | 1.3 | 2.8 | 2.4 | 1 | 2.6 |
| Item 5—Target group | 4 | 2.8 | 4 | 3.3 | 3.6 | 3.8 | 3.7 | 3.6 | 3 |
| Section B | |||||||||
| Item 6—Performance | 4.6 | 4.2 | 4.6 | 4 | 4 | 4.4 | 3.5 | 3.9 | 4.1 |
| Item 7—Ease of use | 4.1 | 3.8 | 4.6 | 3.8 | 3.7 | 4.3 | 4.3 | 4 | 3.5 |
| Item 8—Navigation | 4.2 | 3.9 | 4.7 | 4.1 | 2.8 | 4.1 | 4 | 3.3 | 3.9 |
| Item 9—Gestural design | 4.3 | 4 | 4.2 | 4.1 | 3.5 | 4.7 | 3.9 | 3.6 | 4 |
| Section C | |||||||||
| Item 10—Layout | 4 | 3.9 | 4.1 | 4 | 3.3 | 4 | 3.7 | 2.7 | 3.8 |
| Item 11—Graphics | 4.4 | 3.9 | 4.9 | 3.7 | 2.9 | 4.3 | 3.8 | 2.7 | 3.7 |
| Item 12—Visual appeal | 3.9 | 3.6 | 4.7 | 3.5 | 2.8 | 3.9 | 3.5 | 2.8 | 3.6 |
| Section D | |||||||||
| Item 13—Accuracy | 3.9 | 3.7 | 3.2 | 3.7 | 3.6 | 3.9 | 3.4 | 3.4 | 3.2 |
| Item 14—Goals | 3.9 | 4 | 3.1 | 3.6 | 2.2 | 3.5 | 3.1 | 3 | 3.2 |
| Item 15—Quality of information | 4 | 3.6 | 3 | 3.7 | 2.3 | 3.6 | 3.8 | 3.4 | 3.4 |
| Item 16—Quantity of information | 3.6 | 4 | 2.3 | 3.8 | 2.3 | 3.7 | 3.2 | 3.4 | 3.7 |
| Item 17—Visual information | 4 | 4 | 4.5 | 4 | 2.8 | 3.9 | 4 | 3.5 | 3.4 |
| Item 18—Credibility | 1.2 | 1.9 | 1.2 | 1.2 | 1.7 | 1.4 | 1.7 | 2.9 | 1.1 |
| Section E | |||||||||
| Item 20—Recommendations | 3 | 2 | 2.2 | 1.5 | 1.5 | 2.9 | 2.8 | 3.1 | 1.6 |
| Item 21—Usage | 3.1 | 2.2 | 2.5 | 2.2 | 1.7 | 3.2 | 2.2 | 2.7 | 2.2 |
| Item 22—Price | 1 | 1.4 | 1.2 | 1 | 1 | 1 | 1.2 | 1.2 | 1 |
| Item 23—Overall rating | 3.2 | 2.7 | 2.7 | 2.3 | 1.8 | 3.4 | 3.1 | 2.9 | 2.8 |
| Section F | |||||||||
| Awareness | 2.9 | 1.8 | 2.3 | 2 | 1.9 | 3.7 | 3.7 | 2.8 | 2.8 |
| Knowledge | 2.9 | 4.1 | 1.7 | 2.2 | 1.1 | 2.9 | 3.3 | 3 | 2.4 |
| Attitude | 3.1 | 1.8 | 2.5 | 2.8 | 2.1 | 3.7 | 3.6 | 3 | 2.6 |
| Intention to change | 3.1 | 1.8 | 2.5 | 2.2 | 1.9 | 3.2 | 3.4 | 3.2 | 2.3 |
| Help seeking | 2.7 | 1.5 | 2 | 2 | 1.6 | 1.8 | 3.4 | 2.9 | 2.6 |
| Behaviour change | 3.2 | 1.5 | 2.4 | 2.7 | 2.1 | 3.6 | 3.4 | 3.2 | 2.6 |
| App Name | MARS Overall Star Rating (Item 23) | Overall Quality MARS Score | Star Rating in the iOS App Store (No. of Raters) | Star Rating in the Android App Store (No. of Raters) |
|---|---|---|---|---|
| Colgate Connect | 3.2 ± 0.63 | 3.7 ± 0.26 | 4.3 (104) | 3.1 (148) |
| Dental Hygiene Mastery NBDHE | 2.7 ± 0.67 | 3.4 ± 0.35 | NA | NA |
| Disney Magic Timer by Oral-B | 2.7 ± 0.94 | 3.7 ± 0.30 | 4.3 (974) | 4.4 (55,000) |
| Kolibree | 2.3 ± 0.82 | 3.5 ± 0.29 | 4.1 (28) | 3.5 (173) |
| Mimizaur se brosse les dents | 1.8 ± 0.78 | 2.8 ± 0.22 | 4.5 (22) | 4.6 (661) |
| Oral-B | 3.4 ± 0.96 | 3.7 ± 0.45 | 4.6 (10,989) | 4.5 (67,000) |
| Preventeeth | 3.1 ± 1.10 | 3.4 ± 0.43 | 5 (18) | NA |
| Santé orale—SOHDEV | 2.9 ± 0.73 | 3.0 ± 0.46 | 5 (1) | 4.6 (9) |
| Truthbrush | 2.8 ± 0.78 | 3.2 ± 0.36 | 5 (1) | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carrouel, F.; Bourgeois, D.; Clément, C.; Tardivo, D.; Martinon, P.; Guiral, S.; Lan, R.; Viennot, S.; Dussart, C.; Fraticelli, L. Oral-Hygiene-Related Mobile Apps in the French App Stores: Assessment of Functionality and Quality. Int. J. Environ. Res. Public Health 2022, 19, 7293. https://doi.org/10.3390/ijerph19127293
Carrouel F, Bourgeois D, Clément C, Tardivo D, Martinon P, Guiral S, Lan R, Viennot S, Dussart C, Fraticelli L. Oral-Hygiene-Related Mobile Apps in the French App Stores: Assessment of Functionality and Quality. International Journal of Environmental Research and Public Health. 2022; 19(12):7293. https://doi.org/10.3390/ijerph19127293
Chicago/Turabian StyleCarrouel, Florence, Denis Bourgeois, Céline Clément, Delphine Tardivo, Prescilla Martinon, Sébastien Guiral, Romain Lan, Stéphane Viennot, Claude Dussart, and Laurie Fraticelli. 2022. "Oral-Hygiene-Related Mobile Apps in the French App Stores: Assessment of Functionality and Quality" International Journal of Environmental Research and Public Health 19, no. 12: 7293. https://doi.org/10.3390/ijerph19127293
APA StyleCarrouel, F., Bourgeois, D., Clément, C., Tardivo, D., Martinon, P., Guiral, S., Lan, R., Viennot, S., Dussart, C., & Fraticelli, L. (2022). Oral-Hygiene-Related Mobile Apps in the French App Stores: Assessment of Functionality and Quality. International Journal of Environmental Research and Public Health, 19(12), 7293. https://doi.org/10.3390/ijerph19127293