
The Effect of Acute High-Intensity Interval Training on Executive Function: A Systematic Review

 , , , , and
, , , , and
Abstract
1. Introduction
2. Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Quality Assessment
2.4. Data Extraction
3. Results
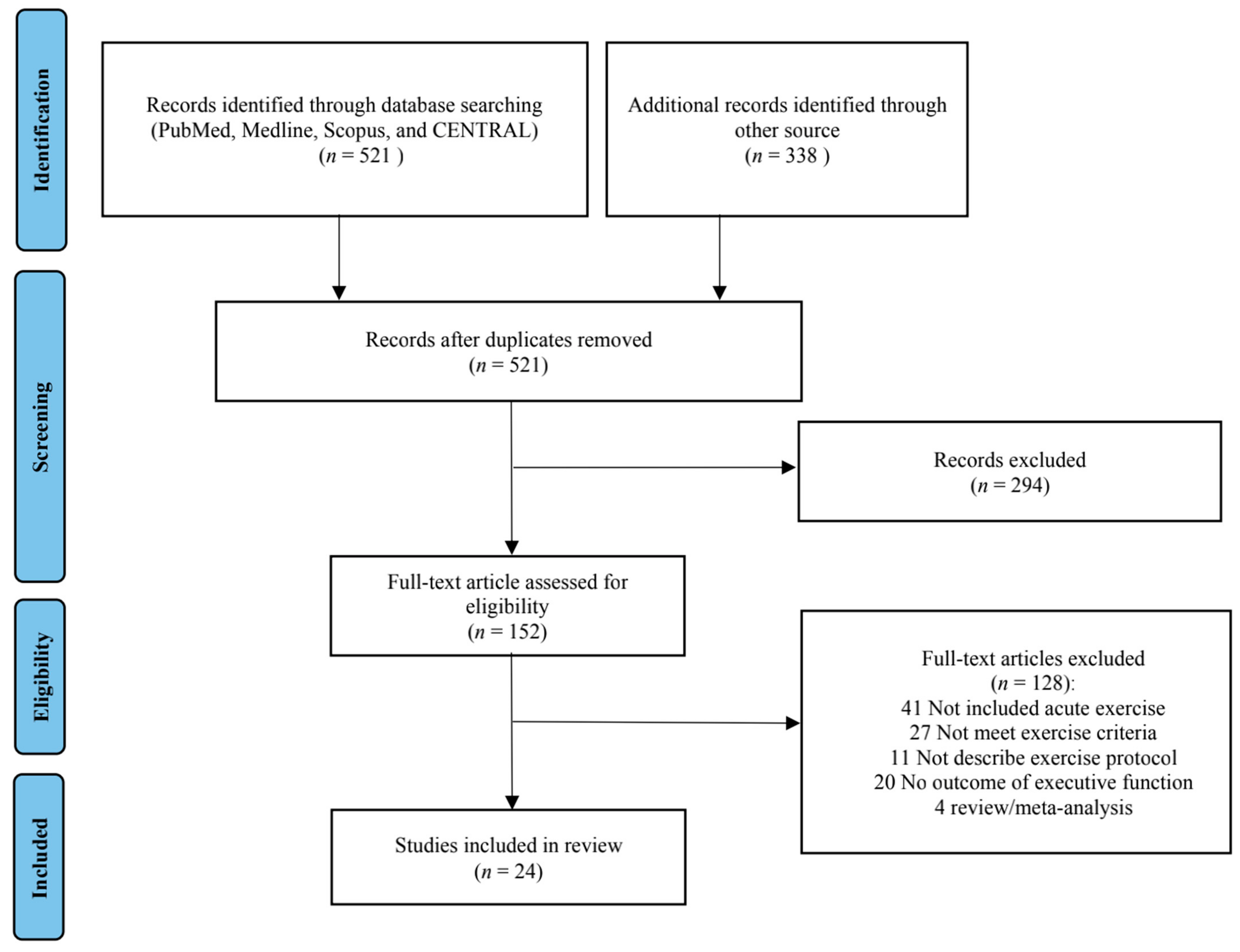
3.1. Search Results and Overall EF
3.2. EF Assessment
3.3. Exercise Intervention
3.4. Sample and Study Characteristics
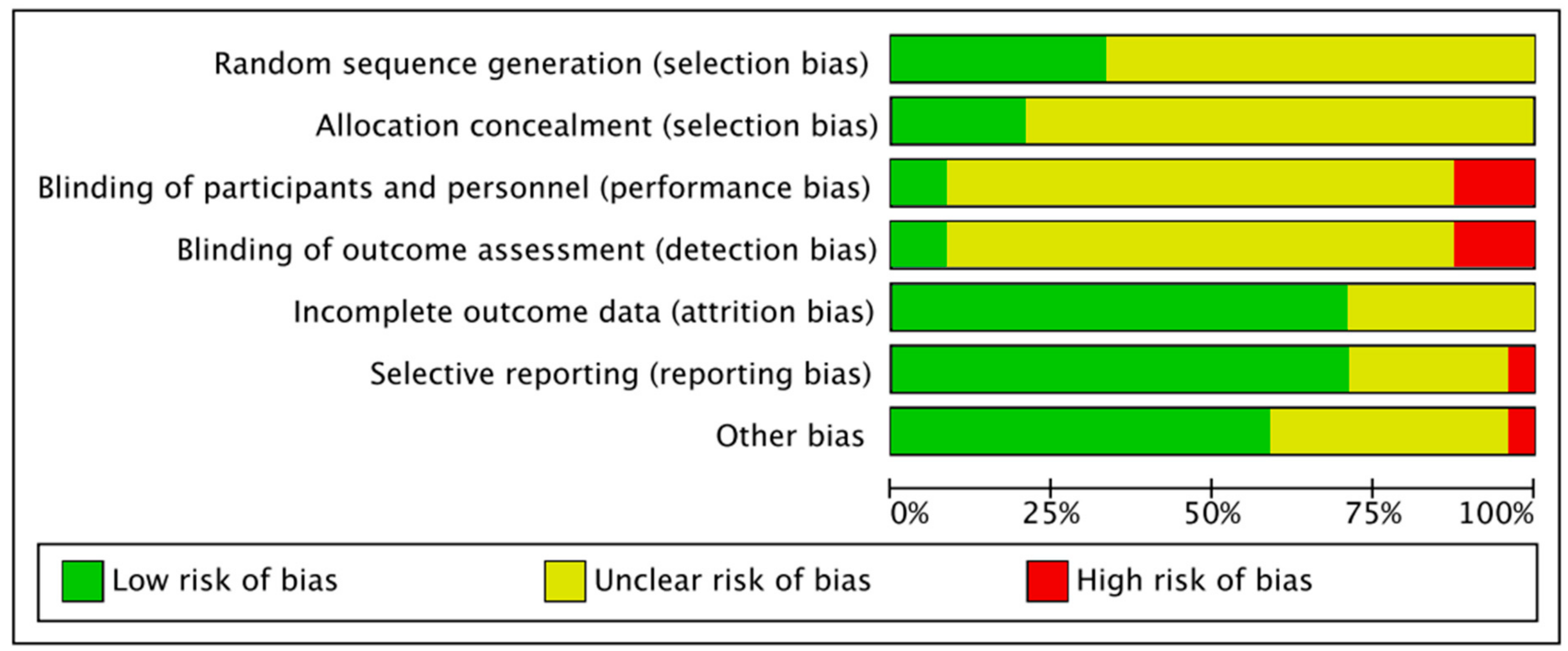
3.5. Quality Assessment
4. Discussion
4.1. Overall Effect
4.2. EF Assessment
4.3. Exercise Intervention
4.4. Sample and Study Characteristics
4.5. Strength and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chang, Y.K.; Labban, J.D.; Gapin, J.I.; Etnier, J.L. The effects of acute exercise on cognitive performance: A meta-analysis. Brain Res. 2012, 1453, 87–101. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, P.D.; Blough, J.; Crawford, L.; Ryu, S.; Zou, L.; Li, H. The Temporal Effects of Acute Exercise on Episodic Memory Function: Systematic Review with Meta-Analysis. Brain Sci. 2019, 9, 87. [Google Scholar] [CrossRef] [PubMed]
- Pindus, D.M.; Drollette, E.S.; Raine, L.B.; Kao, S.C.; Khan, N.; Westfall, D.R.; Hamill, M.; Shorin, R.; Calobrisi, E.; John, D.; et al. Moving fast, thinking fast: The relations of physical activity levels and bouts to neuroelectric indices of inhibitory control in preadolescents. J. Sport Health Sci. 2019, 8, 301–314. [Google Scholar] [CrossRef] [PubMed]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The physical activity guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef]
- Bento-Torres, J.; Bento-Torres, N.V.O.; Stillman, C.M.; Grove, G.A.J.; Huang, H.; Uyar, F.; Watt, J.C.; Wollam, M.E.; Erickson, K.I. Associations between cardiorespiratory fitness, physical activity, intraindividual variability in behavior, and cingulate cortex in younger adults. J. Sport Health Sci. 2019, 8, 315–324. [Google Scholar] [CrossRef]
- Audiffren, M.; André, N. The exercise-cognition relationship: A virtuous circle. J. Sport Health Sci. 2019, 8, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Diamond, A. Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef]
- Chen, F.T.; Chan, K.H.; Feng, S.H.; Wu, T.Y.; Kao, S.C.; Chang, Y.K. New perspective: Effect of exercise and nutritional supplements on cognitive function in older adults. Phys. Educ. J. 2019, 52, 1–15. [Google Scholar] [CrossRef]
- Chang, Y.K.; Chen, F.T.; Kuan, G.; Wei, G.X.; Chu, C.H.; Yan, J.; Chen, A.G.; Hung, T.M. Effects of acute exercise duration on the inhibition aspect of executive function in late middle-aged adults. Front. Aging Neurosci. 2019, 11, 227. [Google Scholar] [CrossRef] [PubMed]
- Peiffer, R.; Darby, L.A.; Fullenkamp, A.; Morgan, A.L. Effects of acute aerobic exercise on executive function in older women. J. Sports Sci. Med. 2015, 14, 574–583. [Google Scholar] [PubMed]
- Tsukamoto, H.; Takenaka, S.; Suga, T.; Tanaka, D.; Takeuchi, T.; Hamaoka, T.; Isaka, T.; Hashimoto, T. Impact of exercise intensity and duration on postexercise executive function. Med. Sci. Sports Exerc. 2017, 49, 774–784. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.H.; Karageorghis, C.I.; Wang, C.C.; Chu, C.H.; Kao, S.C.; Hung, T.M.; Chang, Y.K. Effects of acute aerobic and resistance exercise on executive function: An ERP study. J. Sci. Med. Sport 2019, 22, 1367–1372. [Google Scholar] [CrossRef]
- Chu, C.H.; Kramer, A.F.; Song, T.F.; Wu, C.H.; Hung, T.M.; Chang, Y.K. Acute exercise and neurocognitive development in preadolescents and young adults: An ERP study. Neural Plast. 2017, 2017, 2631909. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.K.; Alderman, B.L.; Chu, C.H.; Wang, C.C.; Song, T.F.; Chen, F.T. Acute exercise has a general facilitative effect on cognitive function: A combined ERP temporal dynamics and BDNF study. Psychophysiology 2017, 54, 289–300. [Google Scholar] [CrossRef]
- Mehren, A.; Diaz Luque, C.; Brandes, M.; Lam, A.P.; Thiel, C.M.; Philipsen, A.; Özyurt, J. Intensity-dependent effects of acute exercise on executive function. Neural Plast. 2019, 2019, 8608317. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Men, W.W.; Chang, Y.K.; Fan, M.X.; Li, L.; Wei, G.X. Acute aerobic exercise increases cortical activity during working memory: A functional MRI study in female college students. PLoS ONE 2014, 9, e99222. [Google Scholar] [CrossRef] [PubMed]
- Ludyga, S.; Gerber, M.; Brand, S.; Holsboer-Trachsler, E.; Pühse, U. Acute effects of moderate aerobic exercise on specific aspects of executive function in different age and fitness groups: A meta-analysis. Psychophysiology 2016, 53, 1611–1626. [Google Scholar] [CrossRef] [PubMed]
- Li, J.W.; O’Connor, H.; O’Dwyer, N.; Orr, R. The effect of acute and chronic exercise on cognitive function and academic performance in adolescents: A systematic review. J. Sci. Med. Sport 2017, 20, 841–848. [Google Scholar] [CrossRef] [PubMed]
- Moreau, D.; Chou, E. The acute effect of high-intensity exercise on executive function: A meta-analysis. Perspect. Psychol. Sci. 2019, 14, 734–764. [Google Scholar] [CrossRef] [PubMed]
- Norton, K.; Norton, L.; Sadgrove, D. Position statement on physical activity and exercise intensity terminology. J. Sci. Med. Sport 2010, 13, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Gibala, M.J.; Little, J.P.; Macdonald, M.J.; Hawley, J.A. Physiological adaptations to low-volume, high-intensity interval training in health and disease. J. Physiol. 2012, 590, 1077–1084. [Google Scholar] [CrossRef] [PubMed]
- Gray, S.R.; Ferguson, C.; Birch, K.; Forrest, L.J.; Gill, J.M. High-intensity interval training: Key data needed to bridge the gap from laboratory to public health policy. Br. J. Sports Med. 2016, 50, 1231–1232. [Google Scholar] [CrossRef]
- Costa, E.C.; Hay, J.L.; Kehler, D.S.; Boreskie, K.F.; Arora, R.C.; Umpierre, D.; Szwajcer, A.; Duhamel, T.A. Effects of high-intensity interval training versus moderate-intensity continuous training on blood pressure in adults with pre-to established hypertension: A systematic review and meta-analysis of randomized trials. Sports Med. 2018, 48, 2127–2142. [Google Scholar] [CrossRef] [PubMed]
- Costigan, S.A.; Eather, N.; Plotnikoff, R.C.; Taaffe, D.R.; Lubans, D.R. High-intensity interval training for improving health-related fitness in adolescents: A systematic review and meta-analysis. Br. J. Sports Med. 2015, 49, 1253–1261. [Google Scholar] [CrossRef] [PubMed]
- Gibala, M.J.; Gillen, J.B.; Percival, M.E. Physiological and health-related adaptations to low-volume interval training: Influences of nutrition and sex. Sports Med. 2014, 44 (Suppl. 2), S127–S137. [Google Scholar] [CrossRef]
- Batacan, R.B.; Duncan, M.J.; Dalbo, V.J.; Tucker, P.S.; Fenning, A.S. Effects of high-intensity interval training on cardiometabolic health: A systematic review and meta-analysis of intervention studies. Br. J. Sports Med. 2017, 51, 494–503. [Google Scholar] [CrossRef]
- Hsieh, S.S.; Chueh, T.Y.; Huang, C.J.; Kao, S.C.; Hillman, C.H.; Chang, Y.K.; Hung, T.M. Systematic review of the acute and chronic effects of high-intensity interval training on executive function across the lifespan. J. Sports Sci. 2020, 39, 10–22. [Google Scholar] [CrossRef] [PubMed]
- Cooper, S.B.; Dring, K.J.; Nevill, M.E. High-Intensity Intermittent Exercise: Effect on Young People’s Cardiometabolic Health and Cognition. Curr. Sports Med. Rep. 2016, 15, 245–251. [Google Scholar] [CrossRef]
- Costigan, S.A.; Eather, N.; Plotnikoff, R.C.; Hillman, C.H.; Lubans, D.R. High-intensity interval training for cognitive and mental health in adolescents. Med. Sci. Sports Exerc. 2016, 48, 1985–1993. [Google Scholar] [CrossRef]
- Chang, Y.K.; Erickson, K.I.; Stamatakis, E.; Hung, T.M. How the 2018 US physical activity guidelines are a call to promote and better understand acute physical activity for cognitive function gains. Sports Med. 2019, 49, 1625–1627. [Google Scholar] [CrossRef]
- Álvarez-Bueno, C.; Pesce, C.; Cavero-Redondo, I.; Sánchez-López, M.; Martínez-Hortelano, J.A.; Martínez-Vizcaíno, V. The effect of physical activity interventions on children’s cognition and metacognition: A systematic review and meta-analysis. J. Am. Acad. Child. Adolesc. Psychiatry 2017, 56, 729–738. [Google Scholar] [CrossRef] [PubMed]
- Browne, S.E.; Flynn, M.J.; O’Neill, B.V.; Howatson, G.; Bell, P.G.; Haskell-Ramsay, C.F. Effects of acute high-intensity exercise on cognitive performance in trained individuals: A systematic review. Prog. Brain Res. 2017, 234, 161–187. [Google Scholar] [CrossRef] [PubMed]
- Lambourne, K.; Tomporowski, P. The effect of exercise-induced arousal on cognitive task performance: A meta-regression analysis. Brain Res. 2010, 1341, 12–24. [Google Scholar] [CrossRef] [PubMed]
- Etnier, J.L.; Chang, Y.K. Exercise, cognitive function, and the brain: Advancing our understanding of complex relationships. J. Sport Health Sci. 2019, 8, 299–300. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.T.; Etnier, J.L.; Chan, K.H.; Chiu, P.K.; Hung, T.M.; Chang, Y.K. Effects of exercise training interventions on executive function in older adults: A systematic review and meta-analysis. Sports Med. 2020, 50, 1451–1467. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Liu, S.; Yu, Q.; Li, Z.; Cunha, P.M.; Zhang, Y.; Kong, Z.; Lin, W.; Chen, S.; Cai, Y. Effects of Acute and Chronic Exercises on Executive Function in Children and Adolescents: A Systemic Review and Meta-Analysis. Front. Psychol. 2020, 11, 554915. [Google Scholar] [CrossRef]
- Alves, C.R.R.; Tessaro, V.H.; Teixeira, L.A.C.; Murakava, K.; Roschel, H.; Gualano, B.; Takito, M.Y. Influence of acute high-intensity aerobic interval exercise bout on selective attention and short-term memory tasks. Percept. Mot. Skills 2014, 118, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Xie, C.; Alderman, B.L.; Meng, F.; Ai, J.; Chang, Y.K.; Li, A. Acute high-intensity interval exercise improves inhibitory control among young adult males with obesity. Front. Psychol. 2020, 11, 1291. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Loprinzi, P.D.; Guan, H.; Zou, L.; Kong, Z.; Hu, Y.; Shi, Q.; Nie, J. The effects of high-intensity interval exercise and hypoxia on cognition in sedentary young adults. Medicina 2019, 55, 43. [Google Scholar] [CrossRef]
- Quintero, A.P.; Bonilla-Vargas, K.J.; Correa-Bautista, J.E.; Domínguez-Sanchéz, M.A.; Triana-Reina, H.R.; Velasco-Orjuela, G.P.; García-Hermoso, A.; Villa-González, E.; Esteban-Cornejo, I.; Correa-Rodríguez, M.; et al. Acute effect of three different exercise training modalities on executive function in overweight inactive men: A secondary analysis of the BrainFit study. Physiol. Behav. 2018, 197, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Dupuy, O.; Billaut, F.; Raymond, F.; Benraiss, A.; Theurot, D.; Bosquet, L.; Fraser, S.; Tremblay, J. Effect of acute intermittent exercise on cognitive flexibility: The role of exercise intensity. J. Cogn. Enhanc. 2018, 2, 146–156. [Google Scholar] [CrossRef]
- Schwarck, S.; Schmicker, M.; Dordevic, M.; Rehfeld, K.; Müller, N.; Müller, P. Inter-individual differences in cognitive response to a single bout of physical exercise—A randomized controlled cross-over study. J. Clin. Med. 2019, 8, 1101. [Google Scholar] [CrossRef] [PubMed]
- Wilke, J. Functional high-intensity exercise is more effective in acutely increasing working memory than aerobic walking: An exploratory randomized, controlled trial. Sci. Rep. 2020, 10, 1–7. [Google Scholar] [CrossRef]
- Burin, D.; Liu, Y.; Yamaya, N.; Kawashima, R. Virtual training leads to physical, cognitive and neural benefits in healthy adults. Neuroimage 2020, 222, 117297. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, T.; Tsukamoto, H.; Takenaka, S.; Olesen, N.D.; Petersen, L.G.; Sørensen, H.; Nielsen, H.B.; Secher, N.H.; Ogoh, S. Maintained exercise-enhanced brain executive function related to cerebral lactate metabolism in men. FASEB J. 2018, 32, 1417–1427. [Google Scholar] [CrossRef]
- Kujach, S.; Byun, K.; Hyodo, K.; Suwabe, K.; Fukuie, T.; Laskowski, R.; Dan, I.; Soya, H. A transferable high-intensity intermittent exercise improves executive performance in association with dorsolateral prefrontal activation in young adults. Neuroimage 2018, 169, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Kujach, S.; Olek, R.A.; Byun, K.; Suwabe, K.; Sitek, E.J.; Ziemann, E.; Laskowski, R.; Soya, H. Acute sprint interval exercise increases both cognitive functions and peripheral neurotrophic factors in humans: The possible involvement of lactate. Front. Neurosci. 2020, 13, 1455. [Google Scholar] [CrossRef] [PubMed]
- Tsukamoto, H.; Suga, T.; Takenaka, S.; Tanaka, D.; Takeuchi, T.; Hamaoka, T.; Isaka, T.; Hashimoto, T. Greater impact of acute high-intensity interval exercise on post-exercise executive function compared to moderate-intensity continuous exercise. Physiol. Behav. 2016, 155, 224–230. [Google Scholar] [CrossRef]
- Chang, H.; Kim, K.; Jung, Y.J.; Kato, M. Effects of acute high-Intensity resistance exercise on cognitive function and oxygenation in prefrontal cortex. J. Exerc. Nutr. Biochem. 2017, 21, 1–8. [Google Scholar] [CrossRef]
- Solianik, R.; Bružas, V.; Mockus, P.; Vadopalas, K.; Streckis, V. Acute effects of high-intensity interval training on cognition and retinal microcirculation in experienced amateur boxers. J. Sports Med. Phys. Fit. 2020. [Google Scholar] [CrossRef]
- Ligeza, T.S.; Maciejczyk, M.; Kałamała, P.; Szygula, Z.; Wyczesany, M. Moderate-intensity exercise boosts the N2 neural inhibition marker: A randomized and counterbalanced ERP study with precisely controlled exercise intensity. Biol. Psychol. 2018, 135, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Gmiat, A.; Micielska, K.; Kozłowska, M.; Flis, D.J.; Smaruj, M.; Kujach, S.; Jaworska, J.; Lipińska, P.; Ziemann, E. The impact of a single bout of high intensity circuit training on myokines’ concentrations and cognitive functions in women of different age. Physiol. Behav. 2017, 179, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Díaz, I.C.; Escobar-Muñoz, M.C.; Carrasco, L. Acute effects of high-intensity interval training on brain-derived neurotrophic factor, cortisol and working memory in physical education college students. Int. J. Environ. Res. Public Health 2020, 17, 8216. [Google Scholar] [CrossRef] [PubMed]
- Ludyga, S.; Pühse, U.; Lucchi, S.; Marti, J.; Gerber, M. Immediate and sustained effects of intermittent exercise on inhibitory control and task-related heart rate variability in adolescents. J. Sci. Med. Sport 2019, 22, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Kao, S.C.; Drollette, E.S.; Ritondale, J.P.; Khan, N.; Hillman, C.H. The acute effects of high-intensity interval training and moderate-intensity continuous exercise on declarative memory and inhibitory control. Psychol. Sport Exerc. 2018, 38, 90–99. [Google Scholar] [CrossRef]
- Kao, S.C.; Westfall, D.R.; Soneson, J.; Gurd, B.; Hillman, C.H. Comparison of the acute effects of high-intensity interval training and continuous aerobic walking on inhibitory control. Psychophysiology 2017, 54, 1335–1345. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.G.; Hanson, N.; Tennyck, J.; Plantz, K. A comparison of high-intensity interval training (HIIT) volumes on cognitive performance. J. Cogn. Enhanc. 2019, 3, 168–173. [Google Scholar] [CrossRef]
- Slusher, A.L.; Patterson, V.T.; Schwartz, C.S.; Acevedo, E.O. Impact of high intensity interval exercise on executive function and brain derived neurotrophic factor in healthy college aged males. Physiol. Behav. 2018, 191, 116–122. [Google Scholar] [CrossRef]
- Cooper, S.B.; Bandelow, S.; Nute, M.L.; Dring, K.J.; Stannard, R.L.; Morris, J.G.; Nevill, M.E. Sprint-based exercise and cognitive function in adolescents. Prev. Med. Rep. 2016, 4, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Lambrick, D.; Stoner, L.; Grigg, R.; Faulkner, J. Effects of continuous and intermittent exercise on executive function in children aged 8–10 years. Psychophysiology 2016, 53, 1335–1342. [Google Scholar] [CrossRef]
- McMorris, T. History of research into the acute exercise–cognition interaction: A cognitive psychology approach. In Exercise-cognition Interaction: Neuroscience Perspectives; Elsevier Academic Press: Amsterdam, The Netherlands, 2016. [Google Scholar]
- McMorris, T.; Tallon, M.; Williams, C.; Sproule, J.; Draper, S.; Swain, J.; Potter, J.; Clayton, N. Incremental exercise, plasma concentrations of catecholamines, reaction time, and motor time during performance of a noncompatible choice response time task. Percept. Mot. Skills 2003, 97, 590–604. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.L.; Lin, Y.T.; Chuang, P.C.; Bohr, V.A.; Mattson, M.P. BDNF and exercise enhance neuronal DNA repair by stimulating CREB-mediated production of apurinic/apyrimidinic endonuclease 1. Neuromol. Med. 2014, 16, 161–174. [Google Scholar] [CrossRef] [PubMed]
- Saucedo Marquez, C.M.; Vanaudenaerde, B.; Troosters, T.; Wenderoth, N. High-intensity interval training evokes larger serum BDNF levels compared with intense continuous exercise. J. Appl. Physiol. 2015, 119, 1363–1373. [Google Scholar] [CrossRef] [PubMed]
- Oberste, M.; Javelle, F.; Sharma, S.; Joisten, N.; Walzik, D.; Bloch, W.; Zimmer, P. Effects and moderators of acute aerobic exercise on subsequent interference control: A systematic review and meta-analysis running title: Acute exercise and interference control. Front. Psychol. 2019, 10, 2616. [Google Scholar] [CrossRef]
- Van der Linden, M.; Brédart, S.; Beerten, A. Age-related differences in updating working memory. Br. J. Psychol. 1994, 85, 145–152. [Google Scholar] [CrossRef]
- Eldreth, D.A.; Patterson, M.D.; Porcelli, A.J.; Biswal, B.B.; Rebbechi, D.; Rypma, B. Evidence for multiple manipulation processes in prefrontal cortex. Brain Res. 2006, 1123, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Friederich, H.C.; Herzog, W. Cognitive-behavioral flexibility in anorexia nervosa. In Behavioral Neurobiology of Eating Disorders; Springer: Berlin/Heidelberg, Germany, 2010; pp. 111–123. [Google Scholar]
- Chang, Y.K.; Chu, C.H.; Wang, C.C.; Wang, Y.C.; Song, T.F.; Tsai, C.L.; Etnier, J.L. Dose-response relation between exercise duration and cognition. Med. Sci. Sports Exerc. 2015, 47, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.T.; Etnier, J.L.; Wu, C.H.; Cho, Y.M.; Hung, T.M.; Chang, Y.K. Dose-response relationship between exercise duration and executive function in older adults. J. Clin. Med. 2018, 7, 279. [Google Scholar] [CrossRef] [PubMed]
- Yerkes, R.M.; Dodson, J.D. The relation of strength of stimulus to rapidity of habit-formation. J. Comp. Neur. 1908, 18, 459–482. [Google Scholar] [CrossRef]
- Dietrich, A.; Audiffren, M. The reticular-activating hypofrontality (RAH) model of acute exercise. Neurosci. Biobehav. Rev. 2011, 35, 1305–1325. [Google Scholar] [CrossRef] [PubMed]
- Calverley, T.A.; Ogoh, S.; Marley, C.J.; Steggall, M.; Marchi, N.; Brassard, P.; Lucas, S.J.E.; Cotter, J.D.; Roig, M.; Ainslie, P.N. HIITing the brain with exercise: Mechanisms, consequences and practical recommendations. J. Physiol. 2020, 598, 2513–2530. [Google Scholar] [CrossRef] [PubMed]
- Charness, G.; Gneezy, U.; Kuhn, M.A. Experimental methods: Between-subject and within-subject design. J. Econ. Behav. Organ. 2012, 81, 1–8. [Google Scholar] [CrossRef]
- Bishop, N.A.; Lu, T.; Yankner, B.A. Neural mechanisms of ageing and cognitive decline. Nature 2010, 464, 529–535. [Google Scholar] [CrossRef]
- Martland, R.; Mondelli, V.; Gaughran, F.; Stubbs, B. Can high-intensity interval training improve physical and mental health outcomes? A meta-review of 33 systematic reviews across the lifespan. J. Sports Sci. 2020, 38, 430–469. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study | Participant | Design | Exercise Intervention | EF Assessment | |||||
|---|---|---|---|---|---|---|---|---|---|
| Author (year), Location | N (males %) Mean age (SD) Fitness level | Exp. Design Comparator | Total time | Type | Protocol: Set, WRT (rest interval) | Intensity | Time exam. | Task | Comp. |
| Alves et al. (2014) [40] Brazil | N = 22 (41%) 53.7 (4.7) Fit | Within-subject Active | 20 min | Aerobic exercise (cycling) | 10 sets, 1 min and 1 min (active) | Submax. | Immediate | Digit span test-backward Stroop test | Updating Inhibition |
| Burin.et al. (2020) [47] Japan | N = 45 (53%) 23.7 (4.5) Fit | Within-subject Passive | 8 min | Aerobic exercise (running) | 8 sets, 30 s and 30 s (active) | Maximal | Immediate | Stroop test | Inhibition |
| Chang et al. (2017) [52] Korea | N = 36 (0%) 21.4 (1.6) Fit | Between-subject Passive | 30 min | Combined exercise (circuit training) | 3 sets, 1:2 (passive) | Submax. | 15 min | Stroop test | Inhibition |
| Cooper et al. (2016) [62] UK | N = 44 (48%) 12.6 (0.6) Fit | Within-subject Passive | 10 min | Aerobic exercise (running) | 10 sets, 10 s and 50 s (active) | Maximal | Immediate, 45 min | Corsi block test Stroop test-complex level | Updating Inhibition |
| Dupuy et al. (2018) [44] France | N = 20 (100%) 28.0 (4.8) Fit | Within-subject Passive | 36 min | Aerobic exercise (cycling) | 6 sets, 3 min and 3 min (passive) | Submax. | 15, 30, 45, and 60 min | Modified Stroop test-interference | Shifting |
| Gmiat et al. (2017) [55] Poland | N = 14 (0%) 22.7 (3), 41.7 (4) Sedentary | Between-subject Passive | 27 min | Combined exercise (circuit training) | 3 sets, 30 s and 10 s (passive) | Maximal | 60 min | Corsi block test Stroop test | Inhibition Updating |
| Hashimoto et al. (2018) [48] Japan | N = 14 (100%) 24 (1) Sedentary | Within-subject Passive | 28 min | Aerobic exercise (cycling) | 4 sets, 4 min and 3 min (active) | Submax. | Immediate, 10, 20, 30, 40, 50 min | Stroop test | Inhibition |
| Kao et al. (2018) [58] USA | N = 36 (50%) 21.5 (0.5) Sedentary | Within-subject Passive | 16 min | Aerobic exercise (running) | 8 sets, 1 min and 1 min (active) | Submax. | 12 min | Flanker task-interference score | Inhibition |
| Kao et al. (2017) [59] USA | N = 64 (42%) 19.2 (0.8) Sedentary | Within-subject Passive | 7.5 min | Aerobic exercise (running) | 3 sets, 1.5 min and 1 min (active) | Submax. | 20 min | Flanker task-incongruent | Inhibition |
| Kujach et al. (2018) [49] Japan | N = 25 (64%) 21.0 (1.6) Sedentary | Within-subject Passive | 8 min | Aerobic exercise (cycling) | 8 sets, 30 s and 30 s (passive) | Submax. | 15 min | Stroop test | Inhibition |
| Kujach et al. (2019) [50] Japan | N = 36 (100%) 21 (1.29) Fit-low | Between-subject Passive | 30 min | Aerobic exercise (cycling) | 6 sets, 30 s and 4.5 min (passive) | Maximal | 20 min | Stroop test TMT-B | Inhibition Shifting |
| Lambrick et al. (2016) [63] UK | N = 20 (45%) 8.8 (0.8) Sedentary | Within-subject Passive | 15 min | Aerobic exercise (running) | 6 sets, 55 s and 95 s (active) | Maximal | 1 min, 15 min, and 30 min | Stroop test | Inhibition |
| Ligeza et al. (2018) [54] Poland | N = 18 (100%) 24.9 (2.2) Fit | Within-subject Passive | 24 min | Aerobic exercise (cycling) | 4 sets, 3 min, 3 min (active) | Submax. | 13 min | Flanker task-incongruent | Inhibition |
| Ludyga et al. (2019) [57] Switzerland | N = 94 (100%) 13.9 (0.7) Sedentary | Between-subject Passive | 16 min | Combined exercise (circuit training) | 10 sets, 60 s and 30 s, 30 s and 30 s (passive) | Maximal | Immediate, 30 min, 60 min | Flanker task-incongruent | Inhibition |
| Martínez et al. (2020) [56] Spain | N = 25 (100%) (2.1) Fit | Within-subject Passive | 20 min | Aerobic exercise (cycling) | 10 sets, 1 min and 1 min (passive) | Submax. | Immediate, 30 min | Digit span test | Updating |
| Miller et al. (2019) [60] USA | N = 25 (48%) 23 (2.79) Fit | Within-subject Passive | 10 min (LV) and 20 min (MV) | Aerobic exercise (cycling) | 5 sets, 1 min and 1 min (active) (LV); 10 set, 1 min and 1 min (active) (MV) | Submax. | 1 min | Stroop test | Inhibition |
| Quintero et al. (2018) [43] Colombia | N = 36 (100%) 23.55 (3.4) Sedentary | Between-subject Passive | 32 min | Aerobic exercise (running) | 4 sets, 4 min and 4 min (active) | Submax. | Immediate | Stroop test-interference | Inhibition |
| Schwarck et al. (2019) [45] Germany | N = 39 (100%) 23.33 (3.23) Fit | Between-subject Passive | 25 min | Aerobic exercise (running) | 5 sets, 2 min and 3 min (active) | Submax. | 10 min | Stroop test-incongruent TMT-B | Inhibition Shifting |
| Slusher et al. (2018) [61] USA | N = 13 (100%) 23.62 (1.06) Sedentary | Within-subject Passive | 5 min | Aerobic exercise (cycling) | 10 sets, 20 s and 10 s. (active) | Maximal | Immediate | Wisconsin card sorting task | Updating |
| Solianik et al. (2020) [53] Lithuania | N = 11 (100%) 22.8 (2.9) Fit | Within-subject passive | 12 min | Aerobic exercise (boxing) | 3 sets, 3 min and 1 min (passive) | Maximal | 21–30 min | Go/No-Go task Procedural reaction time Mathematical processing | Inhibition Shifting Updating |
| Sun et al. (2019) [42] China | N = 20 (50%) 23.9 (2.5) Sedentary | Within-subject Passive | 6 min | Aerobic exercise (cycling) | 10 sets, 6 s and 30 s (passive) | Maximal | Immediate | Go/No-Go task | Inhibition |
| Tsukamoto et al. (2016) [51] Japan | N = 12 (100%) 22.9 (0.4) Fit | Within-subject Passive | 28 min | Aerobic exercise (cycling) | 4 sets, 4 min and 3 min (active) | Submax. | Immediate, 10, 20, and 30 min | Stroop test-incongruent | Inhibition |
| Wilke et al. (2020) [46] Japan | N = 35 (49%) 26.7 (3.6) Fit | Between-subject Passive | 15 min | Combined exercise (circuit training) | 30 sets, 20 s and 10 s (passive) | Maximal | Immediate | Stroop TMT-B Digit span test | Inhibition Shifting Updating |
| Xie et al. (2020) [41] China | N = 16 (100%) 24.5 (5.09) Sedentary | Within-subject Passive | 20 min | Aerobic exercise (cycling) | 10 sets, 1 min and 1 min (active) | Submax. | 15 min | Flanker task-incongruent | Inhibition |
| Inhibition | Updating | Shifting | Planning |
|---|---|---|---|
| Go/No-Go task Flanker task Stroop test | Corsi blocks test Digit span test-backward Mathematical processing Symbol digits modality Wisconsin card sorting task | Modified Stroop test Procedural reaction time Switching task-costs Trail making task-B | None |
| N of Outcome | N of Positive Effect (%) | N of Null Effect (%) | |
|---|---|---|---|
| Overall | 57 | 35 (61%) | 22 (39%) |
| EF assessment | |||
| Component | |||
| Inhibition | 39 | 27 (69%) | 12 (31%) |
| Updating | 11 | 6 (55%) | 5 (45%) |
| Shifting | 7 | 2 (29%) | 5 (71%) |
| Planning | -- | -- | -- |
| Time examination | |||
| ≤10 min | 24 | 16 (67%) | 8 (33%) |
| 11–20 min | 11 | 9 (88%) | 2 (12%) |
| 21–30 min | 10 | 7 (70%) | 3 (30%) |
| >30 min | 12 | 3 (25%) | 9 (75%) |
| Exercise intervention | |||
| Total time | |||
| ≤10 min | 8 | 3 (38%) | 5 (62%) |
| 11–20 min | 24 | 17 (71%) | 7 (29%) |
| 21–30 min | 20 | 13 (65%) | 7 (35%) |
| >30 min | 5 | 2 (40%) | 3 (60%) |
| Type | |||
| Aerobic exercise | 43 | 28 (65%) | 15 (35%) |
| Combined exercise | 14 | 7 (50%) | 7 (50%) |
| Modality | |||
| Running | 12 | 7 (58%) | 5 (42%) |
| Cycling | 28 | 19 (69%) | 9 (31%) |
| Circuit training | 14 | 7 (50%) | 7 (50%) |
| Boxing | 3 | 2 (67%) | 1 (33%) |
| Rest interval | |||
| Active | 30 | 21 (70%) | 9 (30%) |
| Passive | 27 | 14 (52%) | 13 (48%) |
| Work recovery ratio | |||
| >1 | 25 | 16 (64%) | 9 (36%) |
| <1 | 13 | 7 (54%) | 6 (46%) |
| =1 | 19 | 12 (63%) | 7 (37%) |
| Intensity | |||
| Maximal | 21 | 12 (57%) | 9 (43%) |
| Submaximal | 36 | 23 (64%) | 13 (36%) |
| Sample and study characteristics | |||
| Age | |||
| ≤18 years | 13 | 7 (54%) | 6 (46%) |
| 19~40 years | 40 | 27 (68%) | 13 (32%) |
| >40 years | 4 | 1 (25%) | 3 (75%) |
| Gender | |||
| >50% male | 33 | 22 (67%) | 11 (33%) |
| <50% male | 23 | 12 (52%) | 11 (48%) |
| Equal | 1 | 1 (50%) | 1 (50%) |
| Fitness level | |||
| Fit | 53 | 33 (62%) | 20 (38%) |
| Sedentary | 4 | 2 (50%) | 2 (50%) |
| Study Design | |||
| Within-subject | 38 | 25 (66%) | 13 (34%) |
| Between subject | 19 | 10 (53%) | 9 (47%) |
| Comparator | |||
| Active control | 2 | 1 (50%) | 1 (50%) |
| Passive control | 55 | 34 (62%) | 21 (38%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ai, J.-Y.; Chen, F.-T.; Hsieh, S.-S.; Kao, S.-C.; Chen, A.-G.; Hung, T.-M.; Chang, Y.-K. The Effect of Acute High-Intensity Interval Training on Executive Function: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 3593. https://doi.org/10.3390/ijerph18073593
Ai J-Y, Chen F-T, Hsieh S-S, Kao S-C, Chen A-G, Hung T-M, Chang Y-K. The Effect of Acute High-Intensity Interval Training on Executive Function: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(7):3593. https://doi.org/10.3390/ijerph18073593
Chicago/Turabian StyleAi, Jing-Yi, Feng-Tzu Chen, Shu-Shih Hsieh, Shih-Chun Kao, Ai-Guo Chen, Tsung-Min Hung, and Yu-Kai Chang. 2021. "The Effect of Acute High-Intensity Interval Training on Executive Function: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 7: 3593. https://doi.org/10.3390/ijerph18073593
APA StyleAi, J.-Y., Chen, F.-T., Hsieh, S.-S., Kao, S.-C., Chen, A.-G., Hung, T.-M., & Chang, Y.-K. (2021). The Effect of Acute High-Intensity Interval Training on Executive Function: A Systematic Review. International Journal of Environmental Research and Public Health, 18(7), 3593. https://doi.org/10.3390/ijerph18073593