
Exercise Intensity in Patients with Cardiovascular Diseases: Systematic Review with Meta-Analysis




Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Study Selection and Data Extraction
2.5. Assessment of Potential Bias
2.6. Data Treatment and Analysis
3. Results
3.1. Risk of Bias
3.2. Study and Participant Characteristics
3.3. Intervention Characteristics
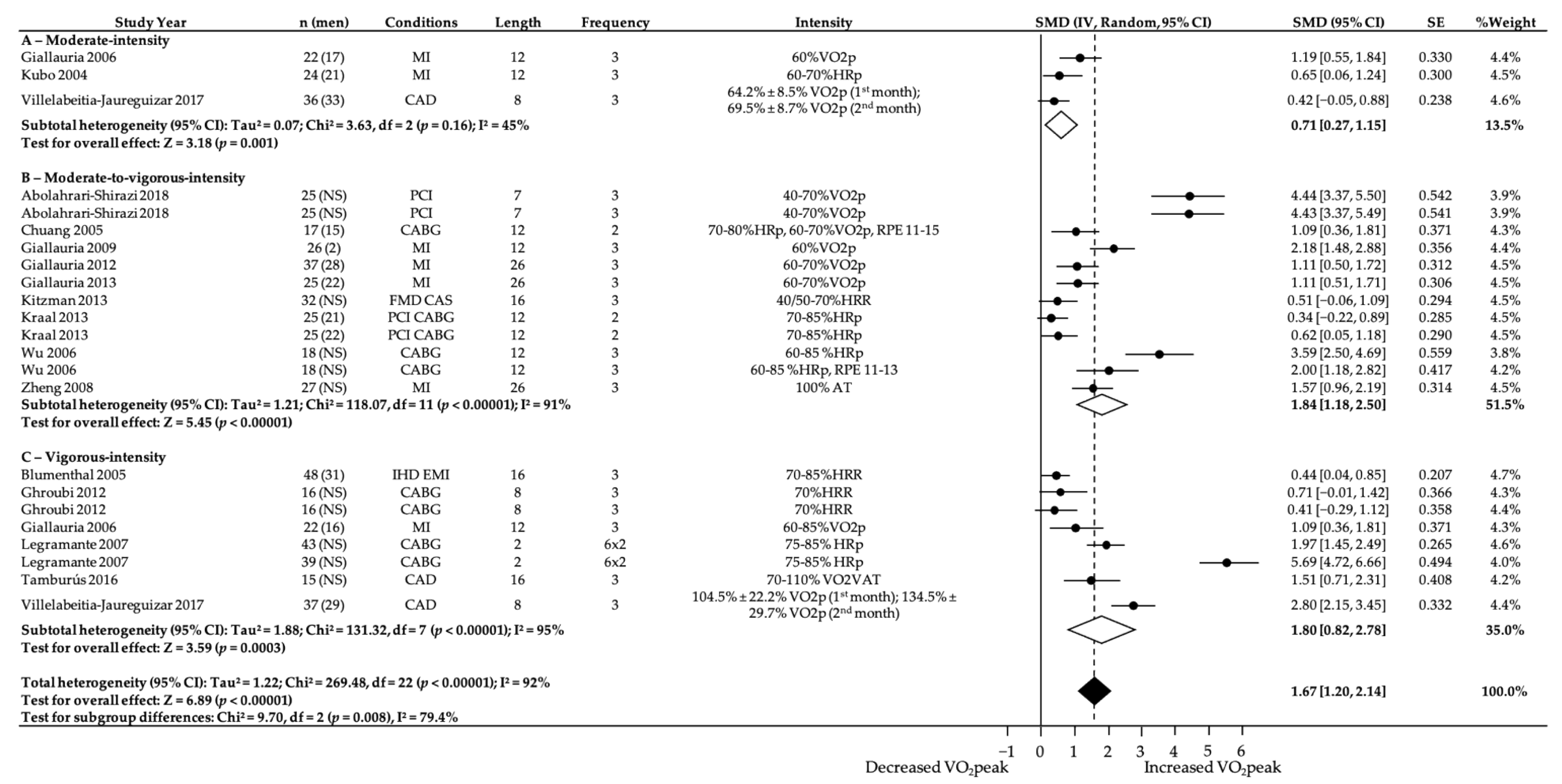
3.4. Subgroup Analyses—Intensity
3.5. Subgroup Analyses—Intensity and Length
3.6. Publication Bias
4. Discussion
5. Conclusions
- ►
- Cardiovascular diseases are the leading causes of mortality in today’s society. They are responsible for up to 30% of all deaths worldwide and 48% of deaths in Europe, and it is expected that these figures will increase in the coming years.
- ►
- Exercise programs in patients with cardiovascular disease have several beneficial effects on cardiovascular functional capacity, quality of life, risk factors modification, psychological profile, hospital readmissions, and mortality.
- ►
- Exercise-based interventions seem to significantly improve cardiorespiratory fitness in patients following a cardiac event or surgery, but little is known regarding the differential effects of prescribed exercise intensity.
- ►
- Exercise interventions for patients with cardiovascular disease tend include large ranges of exercise intensities based on heart rate responses to exercise.
- ►
- The most effective doses of exercise intensity to optimize cardiorespiratory fitness were moderate-to-vigorous and vigorous-intensity exercises, being more effective when conducted for 6 to 12 weeks.
- ►
- More research is needed to understand within the moderate-to-vigorous- and vigorous-intensity categories the percentage that specifically helps to increase cardiorespiratory fitness and the ability to establish specific prescription protocols.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Cardiovascular Disease; Fact Sheet N 317; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- EACPR Committee for Science Guidelines; Corrà, U.; Piepoli, M.F.; Carré, F.; Heuschmann, P.; Hoffmann, U.; Verschuren, M.; Halcox, J.; Giannuzzi, P.; Saner, H.; et al. Secondary prevention through cardiac rehabilitation: Physical activity counselling and exercise training: Key components of the position paper from the Cardiac Rehabilitation Section of the European Association of Cardiovascular Prevention and Rehabilitation. Eur. Heart J. 2010, 31, 1967–1974. [Google Scholar] [CrossRef]
- Mohammed, H.G.; Shabana, A.M. Effect of cardiac rehabilitation on cardiovascular risk factors in chronic heart failure patients. Egypt Heart J. 2018, 70, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef]
- Anderson, L.; Oldridge, N.; Thompson, D.R.; Zwisler, A.-D.; Rees, K.; Martin, N.; Taylor, R.S. Exercise-Based Cardiac Rehabilitation for Coronary Heart Disease. J. Am. Coll. Cardiol. 2016, 67, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Mezzani, A.; Hamm, L.F.; Jones, A.M.; McBride, P.E.; Moholdt, T.; Stoner, J.A.; Urhausen, A.; Williams, A.M. Aerobic exercise intensity assessment and prescription in cardiac rehabilitation: A joint position statement of the European Association for Cardiovascular Prevention and Rehabilitation, the American Association of Cardiovascular and Pulmonary Rehabilitation and the Canadian Association of Cardiac Rehabilitation. Eur. J. Prev. Cardiol. 2013, 20, 442–467. [Google Scholar] [CrossRef]
- Moholdt, T.; Aamot, I.L.; Granøien, I.; Gjerde, L.; Myklebust, G.; Walderhaug, L.; Brattbakk, L.; Hole, T.; Graven, T.; Stølen, O.T.; et al. Aerobic interval training increases peak oxygen uptake more than usual care exercise training in myocardial infarction patients: A randomized controlled study. Clin. Rehabil. 2011, 26, 33–44. [Google Scholar] [CrossRef]
- Wisloff, U.; Stoylen, A.; Loennechen, J.P.; Bruvold, M.; Rognmo, Ø.; Haram, P.M.; Tjonna, A.E.; Stig, J.H.; Slørdahl, S.A.; Lee, S.J.; et al. Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients: A randomized study. Circulation 2007, 115, 3086–3094. [Google Scholar] [CrossRef] [PubMed]
- Rojhani-Shirazi, Z.; Abolahrari-Shirazi, S.; Kojuri, J.; Bagheri, Z. Efficacy of combined endurance-resistance training versus endurance training in patients with heart failure after percutaneous coronary intervention: A randomized controlled trial. J. Res. Med. Sci. 2018, 23, 12. [Google Scholar] [CrossRef] [PubMed]
- Giallauria, F.; Lucci, R.; D’Agostino, M.; Vitelli, A.; Maresca, L.; Mancini, M.; Aurino, M.; Del Forno, D.; Giannuzzi, P.; Vigorito, C. Two-year multicomprehensive secondary prevention program: Favorable effects on cardiovascular functional capacity and coronary risk profile after acute myocardial infarction. J. Cardiovasc. Med. 2009, 10, 772–780. [Google Scholar] [CrossRef] [PubMed]
- Giallauria, F.; Acampa, W.; Ricci, F.; Vitelli, A.; Maresca, L.; Mancini, M.; Grieco, A.; Gallicchio, R.; Xhoxhi, E.; Spinelli, L.; et al. Effects of exercise training started within 2 weeks after acute myocardial infarction on myocardial perfusion and left ventricular function: A gated SPECT imaging study. Eur. J. Prev. Cardiol. 2012, 19, 1410–1419. [Google Scholar] [CrossRef] [PubMed]
- Giallauria, F.; Acampa, W.; Ricci, F.; Vitelli, A.; Torella, G.; Lucci, R.; Del Prete, G.; Zampella, E.; Assante, R.; Rengo, G.; et al. Exercise training early after acute myocardial infarction reduces stress-induced hypoperfusion and improves left ventricular function. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 315–324. [Google Scholar] [CrossRef]
- Villelabeitia-Jaureguizar, K.; Vicente-Campos, D.; Senen, A.B.; Jiménez, V.H.; Garrido-Lestache, M.E.B.; Chicharro, J.L. Effects of high-intensity interval versus continuous exercise training on post-exercise heart rate recovery in coronary heart-disease patients. Int. J. Cardiol. 2017, 244, 17–23. [Google Scholar] [CrossRef]
- Tamburús, N.Y.; Kunz, V.C.; Salviati, M.R.; Simões, V.C.; Catai, A.M.; Da Silva, E. Interval training based on ventilatory anaerobic threshold improves aerobic functional capacity and metabolic profile: A randomized controlled trial in coronary artery disease patients. Eur. J. Phys. Rehabil Med. 2015, 52, 1–11. [Google Scholar] [PubMed]
- Beckie, T.M.; Beckstead, J.W.; Kip, K.E.; Fletcher, G. Improvements in Heart Rate Recovery Among Women After Cardiac Rehabilitation Completion. J. Cardiovasc. Nurs. 2014, 29, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Rivera-Brown, A.M.; Frontera, W.R. Principles of exercise physiology: Responses to acute exercise and long-term adaptations to training. PM R. 2012, 4, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.; McKenzie, D.C.; Haykowsky, M.J.; Taylor, A.; Shoemaker, P.; Ignaszewski, A.P.; Chan, S.Y. Effectiveness of High-Intensity Interval Training for the Rehabilitation of Patients with Coronary Artery Disease. Am. J. Cardiol. 2005, 95, 1080–1084. [Google Scholar] [CrossRef]
- Rognmo, Ø.; Hetland, E.; Helgerud, J.; Hoff, J.; Slørdahl, S.A. High intensity aerobic interval exercise is superior to moderate intensity exercise for increasing aerobic capacity in patients with coronary artery disease. Eur. J. Cardiovasc. Prev. Rehabil. 2004, 11, 216–222. [Google Scholar] [CrossRef]
- Cornish, A.K.; Broadbent, S.; Cheema, B.S. Interval training for patients with coronary artery disease: A systematic review. Graefe’s Arch. Clin. Exp. Ophthalmol. 2010, 111, 579–589. [Google Scholar] [CrossRef] [PubMed]
- Ghroubi, S.; Elleuch, W.; Abid, L.; Kammoun, S.; Elleuch, M.-H. The effects of cardiovascular rehabilitation after coronary stenting, Apport de la readaptation cardiovasculaire dans les suites d’une angioplastie transluminale. Ann. Phys. Rehabil. Med. 2012, 55, e307–e309. [Google Scholar] [CrossRef][Green Version]
- Blumenthal, J.A.; Sherwood, A.; Babyak, M.A.; Watkins, L.L.; Waugh, R.; Georgiades, A.; Bacon, S.L.; Hayano, J.; Coleman, E.R.; Hinderliter, A. Effects of exercise and stress management training on markers of cardiovascular risk in patients with ischemic heart disease—A randomized controlled trial. JAMA 2005, 293, 1626–1634. [Google Scholar] [CrossRef]
- Kitzman, D.W.; Brubaker, P.H.; Herrington, D.M.; Morgan, T.M.; Stewart, K.P.; Hundley, W.G.; Abdelhamed, A.; Haykowsky, M.J. Effect of endurance exercise training on endothelial function and arterial stiffness in older patients with heart failure and preserved ejection fraction: A randomized, controlled, single-blind trial. J. Am. Coll. Cardiol. 2013, 62, 584–592. [Google Scholar] [CrossRef]
- Mitchell, B.L.; Lock, M.J.; Davison, K.; Parfitt, G.; Buckley, J.P.; Eston, R.G. What is the effect of aerobic exercise intensity on cardiorespiratory fitness in those undergoing cardiac rehabilitation? A systematic review with meta-analysis. Br. J. Sports Med. 2018, 53, 1341–1351. [Google Scholar] [CrossRef] [PubMed]
- Hannan, A.L.; Hing, W.; Simas, V.; Climstein, M.; Coombes, J.S.; Jayasinghe, R.; Byrnes, J.; Furness, J. High-intensity interval training versus moderate-intensity continuous training within cardiac rehabilitation: A systematic review and meta-analysis. Open Access J. Sports Med. 2018, 9, 1–17. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons Ltd.: Chichester, UK, 2011. [Google Scholar]
- Leonardo, R. PICO: Model for Clinical Questions. Evid. Based Med. Pract. 2018, 3, 1–2. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Lippincott Williams & Wilkins: Baltimore, MD, USA, 2017. [Google Scholar]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive Statistics for Studies in Sports Medicine and Exercise Science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef]
- Review Manager (RevMan); Version 5.3.; The Nordic Cochrane Centre, The Cochrane Collaboration: Copenhagen, Denmark, 2014; Available online: http://community.cochrane.org/tools/review-production-tools/revman-5 (accessed on 21 January 2021).
- Elbourne, D.R.; Altman, D.G.; Higgins, J.P.T.; Curtin, F.; Worthingtond, H.V.; Vaile, A. Meta-analyses involving cross-over trials: Methodological issues. Int. J. Epidemiol. 2002, 31, 140–149. [Google Scholar] [CrossRef]
- Sandercock, G.; Hurtado, V.; Cardoso, F. Changes in cardiorespiratory fitness in cardiac rehabilitation patients: A meta-analysis. Int. J. Cardiol. 2013, 167, 894–902. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.K.; Lin, Y.W.; Chen, C.L.; Tsai, S.W. Cardiac rehabilitation vs. home exercise after coronary artery bypass graft surgery: A comparison of heart rate recovery. Am. J. Phys. Med. Rehabil. 2006, 85, 711–717. [Google Scholar] [CrossRef]
- Chuang, T.-Y.; Sung, W.-H.; Lin, C.-Y. Application of a Virtual Reality–Enhanced Exercise Protocol in Patients After Coronary Bypass. Arch. Phys. Med. Rehabil. 2005, 86, 1929–1932. [Google Scholar] [CrossRef]
- Zheng, H.; Luo, M.; Shen, Y.; Kang, W. Effects of 6 months exercise training on ventricular remodelling and autonomic tone in patients with acute myocardial infarction and percutaneous coronary intervention. J. Rehabil. Med. 2008, 40, 776–779. [Google Scholar] [PubMed]
- Giallauria, F.; De Lorenzo, A.; Pilerci, F.; Manakos, A.; Lucci, R.; Psaroudaki, M.; D’Agostino, M.; Del Forno, D.; Vigorito, C. Long-term effects of cardiac rehabilitation on end-exercise heart rate recovery after myocardial infarction. Eur. J. Cardiovasc. Prev. Rehabil. 2006, 13, 544–550. [Google Scholar] [CrossRef] [PubMed]
- Legramante, J.M.; Iellamo, F.; Massaro, M.; Sacco, S.; Galante, A. Effects of residential exercise training on heart rate recovery in coronary artery patients. Am. J. Physiol. Circ. Physiol. 2007, 292, H510–H515. [Google Scholar] [CrossRef] [PubMed]
- Kubo, N.; Ohmura, N.; Nakada, I.; Yasu, T.; Katsuki, T.; Fujii, M.; Saito, M. Exercise at ventilatory threshold aggravates left ventricular remodeling in patients with extensive anterior acute myocardial infarction. Am. Heart J. 2004, 147, 113–120. [Google Scholar] [CrossRef]
- Kraal, J.J.; Peek, N.; Van den Akker-Van Marle, M.E.; Kemps, M.C.H. Effects and costs of home-based training with telemonitoring guidance in low to moderate risk patients entering cardiac rehabilitation: The FIT@Home study. BMC Cardiovasc. Disord. 2013, 13, 82. [Google Scholar] [CrossRef]
- Harbord, R.M.; Harris, R.J.; Sterne, J.A.C. Updated Tests for Small-study Effects in Meta-analyses. Stata J. Promot. Commun. Stat. Stata 2009, 9, 197–210. [Google Scholar] [CrossRef]
- Conn, V.S.; Hafdahl, A.R.; Moore, S.M.; Nielsen, P.J.; Brown, L.M. Meta-analysis of interventions to increase physical activity among cardiac sub-jects. Int. J. Cardiol. 2009, 133, 307–320. [Google Scholar] [CrossRef]
- Vromen, T.; Kraal, J.J.; Kuiper, J.; Spee, R.F.; Peek, N.; Kemps, H.M. The influence of training characteristics on the effect of aerobic exercise training in patients with chronic heart failure: A meta-regression analysis. Int. J. Cardiol. 2016, 208, 120–127. [Google Scholar] [CrossRef]
- Anderson, L.; Taylor, R.S. Cardiac rehabilitation for people with heart disease: An overview of Cochrane systematic reviews. Cochrane Database Syst. Rev. 2014, 12, CD011273. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| %VO2max | %HRpeak | %HRreserve/%VO2reserve | Perceived Exertion * | |
|---|---|---|---|---|
| Light | 37–45 | 57–63 | 30–39 | RPE 9–11 |
| Moderate | 46–63 | 64–76 | 40–59 | RPE 12–13 |
| Vigorous | 64–90 | 77–95 | 60–89 | RPE 14–17 |
| Near maximal to maximal | ≥91 | ≥95 | ≥90 | RPE ≥ 18 |
| Research Studies | Peak VO2 | |||||
|---|---|---|---|---|---|---|
| Group | N | References | MD (95% CI) | I2 | pa | p-Difference b |
| No. of participants | ||||||
| <20 | 4 | Ghroubi et al. [20], Tamburus et al. [14], Wu et al. [33], Chuang et al. [34] | 2.62 (1.65, 3.58) | 88 | <0.001 | 0.78 |
| ≥20 | 12 | Abolahrari-Shirazi et al. [9], Blumenthal et al. [21], Giallauria et al. [10,11,12,36], Kitzman et al. [22], Kraal et al. [36], Kubo et al. [38], Legramante et al. [37], Villelabeitia et al. [13], Zheng et al. [35] | 2.75 (2.58, 2.93) | 97 | <0.001 | |
| Age, years | ||||||
| <60 | 9 | Abolahrari-Shirazi et al. [9], Ghroubi et al. [20], Giallauria et al. [10,12,36], Kraal et al. [39], Kubo et al. [38], Tamburus et al. [14], Villelabeitia et al. [13] | 4.40 (0.79, 8.01) | 97 | 0.02 | 0.75 |
| ≥60 | 6 | Blumenthal et al. [21], Chuang et al. [34], Giallauria et al. [11], Kitzman et al. [22], Legramante et al. [37], Wu et al. [33] | 3.48 (2.09, 4.87) | 79 | <0.001 | |
| Not reported | 1 | Zheng et al. [35] | 3.10 (2.06, 4.14) | 0 | <0.001 | |
| Diagnosis | ||||||
| CAD only | 3 | Blumenthal et al. [21], Tamburus et al. [14], Villelabeitia et al. [13] | 6.41 (−2.70, 15.53) | 99 | 0.17 | 0.03 |
| CABG only | 4 | Chuang et al. [34], Ghroubi et al. [20], Legramante et al. [37], Wu et al. [33] | 4.27 (1.60, 6.94) | 85 | 0.002 | |
| PCI only | 1 | Abolahrari-Shirazi et al. [9] | 8.20 (4.68, 11.72) | 0 | <0.001 | |
| CABG/PCI | 1 | Kraal et al. [39] | 3.20 (0.36, 6.04) | 0 | 0.03 | |
| MI | 6 | Giallauria et al. [10,11,12,36], Kubo et al. [38], Zheng et al. [35] | 2.65 (0.56, 4.74) | 91 | 0.01 | |
| FMD | 1 | Kitzman et al. [22] | 1.60 (−0.13, 3.33) | 0 | 0.07 | |
| Study location | ||||||
| America | 2 | Kitzman et al. [22], Tamburus et al. [14] | 1.38 (0.39, 2.36) | 0 | 0.006 | 0.01 |
| Africa | 1 | Ghroubi et al. [20] | 1.70 (−1.07, 4.47) | 0 | 0.23 | |
| Asia | 5 | Abolahrari-Shirazi et al. [9], Chuang et al. [34], Kubo et al. [38], Wu et al. [33], Zheng et al. [35] | 5.33 (2.90, 7.76) | 80 | <0.001 | |
| Europe | 8 | Blumenthal et al. [21], Giallauria et al. [10,11,12,36], Kraal et al. [39], Legramante et al. [37], Villelabeitia et al. [13] | 4.23 (1.50, 6.95) | 98 | 0.002 | |
| Research Studies | Peak VO2 | ||||||
|---|---|---|---|---|---|---|---|
| Group | N | References | MD (95% CI) | I2 | pa | p-Difference b | |
| Length, weeks | |||||||
| <6 | 1 | Legramante et al. [37] | 2.60 (2.41, 2.79) | 0 | <0.001 | 0.42 | |
| 6–12 | 9 | Abolahrari-Shirazi et al. [9], Chuang et al. [34], Ghroubi et al. [20], Giallauria et al. [10,36], Kraal et al. [39], Kubo et al. [38], Villelabeitia et al. [13], Wu et al. [33] | 5.31 (1.24, 9.38) | 97 | 0.01 | ||
| >12 | 6 | Blumenthal et al. [21], Giallauria et al. [11,12], Kitzman et al. [22], Tamburus et al. [14], Zheng et al. [35] | 2.50 (1.60, 3.41) | 52 | <0.001 | ||
| Frequency, sessions/week | |||||||
| 1–2 | 2 | Chuang et al. [34], Kraal et al. [39] | 3.98 (1.96, 6.01) | 0 | 0.001 | 0.17 | |
| 3–4 | 13 | Abolahrari-Shirazi et al. [9], Blumenthal et al. [21], Ghroubi et al. [20], Giallauria et al. [10,11,12,36], Kitzman et al. [22], Kubo et al. [38], Tamburus et al. [14], Villelabeitia et al. [13], Wu et al. [33], Zheng et al. [35] | 4.21 (1.82, 6.60) | 96 | 0.006 | ||
| 5–7 | 1 | Legramante et al. [37] | 2.60 (2.41, 2.79) | 0 | <0.001 | ||
| Supervision | |||||||
| Clinic | 12 | Blumenthal et al. [21], Chuang et al. [34], Ghroubi et al. [20], Giallauria et al. [10,11,12], Kitzman et al. [22], Kubo et al. [38], Legramante et al. [37], Tamburus et al. [14], Villelabeitia et al. [13], Zheng et al. [35] | 4.01 (2.30, 5.72) | 96 | <0.001 | 0.02 | |
| Home | 1 | Wu et al. [33] | 8.50 (5.78, 11.22) | 0 | <0.001 | ||
| Mixed | 3 | Abolahrari-Shirazi et al. [9], Giallauria et al. [36], Kraal et al. [39] | 2.99 (−2.89, 8.87) | 94 | 0.32 | ||
| Intervention type | |||||||
| Continuous | 13 | Abolahrari-Shirazi et al. [9], Blumenthal et al. [21], Chuang et al. [34], Giallauria et al. [11,12,36], Kitzman et al. [22], Kraal et al. [39], Kubo et al. [38], Legramante et al. [37], Wu et al. [33], Zheng et al. [35] | 3.27 (2.23, 4.32) | 87 | <0.001 | 0.44 | |
| Interval | 2 | Tamburus et al. [14], Villelabeitia et al. [13] | 8.67 (−5.86, 23.21) | 99 | 0.24 | ||
| Mixed | 1 | Ghroubi et al. [20] | 1.70 (−1.07, 4.47) | 0 | 0.23 | ||
| Mode | |||||||
| Cycle ergometer | 7 | Ghroubi et al. [20], Giallauria et al. [10,11,12], Tamburus et al. [14], Villelabeitia et al. [13], Zheng et al. [35] | 4.90 [1.52, 8.27) | 97 | 0.005 | 0.23 | |
| Treadmill | 1 | Chuang et al. [34] | 4.80 (1.91, 7.69) | 0 | 0.001 | ||
| Walking | 1 | Blumenthal et al. [21] | 1.90 (0.20, 3.60) | 0 | 0.03 | ||
| Mixed (treadmill, walking, cycling, calisthenics or/and arm/leg ergometer) | 7 | Abolahrari-Shirazi et al. [9], Giallauria et al. [36], Kitzman et al. [22], Kraal et al. [39], Kubo et al. [37], Legramante et al. [37], Wu et al. [33] | 3.28 (1.17, 5.39) | 92 | 0.002 | ||
| Exercise type | |||||||
| Aerobic | 13 | Blumenthal et al. [21], Chuang et al. [34], Ghroubi et al. [20], Giallauria et al. [10,12,36], Kitzman et al. [22], Kraal et al. [39], Kubo et al. [38], Tamburus et al. [14], Villelabeitia et al. [13], Wu et al. [33], Zheng et al. [35] | 3.94 (1.55, 6.34) | 96 | 0.001 | 0.86 | |
| Aerobic and Resistance | 3 | Abolahrari-Shirazi et al. [9], Giallauria et al. [11], Legramante et al. [37] | 4.24 (1.82, 6.67) | 81 | 0.001 | ||
| Intensity | |||||||
| Moderate | 3 | Giallauria et al. [10], Kubo et al. [38], Villelabeitia et al. [13] | 2.90 (1.64, 4.16) | 0 | <0.001 | 0.03 | |
| Moderate-to-vigorous | 10 | Abolahrari-Shirazi et al. [9], Chuang et al. [34], Giallauria et al. [11,12,36], Kitzman et al. [22], Kraal et al. [39], Wu et al. [33], Zheng et al. [35] | 5.07 (3.43, 6.72) | 92 | <0.001 | ||
| Vigorous | 3 | Blumenthal et al. [21], Ghroubi et al. [20], Giallauria et al. [10], Legramante et al. [37], Tamburus et al. [14], Villelabeitia et al. [13] | 2.43 (1.33, 3.54) | 75 | <0.001 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gonçalves, C.; Raimundo, A.; Abreu, A.; Bravo, J. Exercise Intensity in Patients with Cardiovascular Diseases: Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 3574. https://doi.org/10.3390/ijerph18073574
Gonçalves C, Raimundo A, Abreu A, Bravo J. Exercise Intensity in Patients with Cardiovascular Diseases: Systematic Review with Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(7):3574. https://doi.org/10.3390/ijerph18073574
Chicago/Turabian StyleGonçalves, Catarina, Armando Raimundo, Ana Abreu, and Jorge Bravo. 2021. "Exercise Intensity in Patients with Cardiovascular Diseases: Systematic Review with Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 7: 3574. https://doi.org/10.3390/ijerph18073574
APA StyleGonçalves, C., Raimundo, A., Abreu, A., & Bravo, J. (2021). Exercise Intensity in Patients with Cardiovascular Diseases: Systematic Review with Meta-Analysis. International Journal of Environmental Research and Public Health, 18(7), 3574. https://doi.org/10.3390/ijerph18073574