Abstract
Introduction: Sleep disorders, especially insomnia, are very common in different kinds of cancers, but their prevalence and incidence are not well-known. Disturbed sleep in cancer is caused by different reasons and usually appears as a comorbid disorder to different somatic and psychiatric diagnoses, psychological disturbances and treatment methods. There can be many different predictors for sleep disturbances in these vulnerable groups, such as pre-existing sleep disorders, caused by the mental status in cancer or as side effect of the cancer treatment. Methods: A systematic literature review of 8073 studies was conducted on the topic of sleep and sleep disorders in cancer patients. The articles were identified though PubMed, PsycInfo and Web of Knowledge, and a total number of 89 publications were qualified for analysis. Results: The identified eighty-nine studies were analyzed on the topic of sleep and sleep disorders in cancer, twenty-six studies on sleep and fatigue in cancer and sixty-one studies on the topic of sleep disorders in cancer. The prevalence of sleep disturbences and/or sleep disorders in cancer was up to 95%. Discussion: Sleep disturbances and sleep disorders (such as insomnia, OSAS, narcolepsy and RLS; REM-SBD) in cancer patients can be associated with different conditions. Side effects of cancer treatment and cancer-related psychological dysfunctions can be instigated by sleep disturbances and sleep disorders in these patients, especially insomnia and OSAS are common. An evidence-based treatment is necessary for concomitant mental and/or physical states.
1. Introduction
Sleep disturbances and different sleep disorders (e.g., insomnia and sleep-related breathing disorder (SRBD)/obstructive sleep apnea syndrome (OSAS)) are common and considerable complaints of cancer patients. Narcolepsy, restless legs syndrome (RLS) and REM-sleep behavior disorder (REM-SBD) are rarely found. Up to 95% of cancer patients complain of sleep disturbances/disorders during diagnosis, treatment and after 10 years of survivorship. Sleep disturbances/disorders and excessive daytime sleepiness (EDS) have been reported to influence fatigue [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27] and its perceptions. Savard et al. studied cancer survivors and showed that 52% of them reported sleeping difficulties, and 58% reported that cancer either caused or aggravated their sleeping problems [28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88], especially [58].
Disturbed sleep appears before, while and after cancer diseases. The personalized treatment of the most frequent sleep disorders, e.g., insomnia or sleep-related breathing disorder, could improve both their mental and physical health, specifically for diseases such as cancer. The analyses for this review were very challenging, specifically with regards to systematizing the complex and nonhomogeneous literature about sleep, sleep disturbances and different sleep disorders, their prevalence and the severity of sleep complaints in cancer patients, especially because the cancer population is very heterogenous.
The aim of this systematic review was to evaluate critically the prevalence, severity and efficacy of treatments in cancer-related sleep disorders (CRSD).
2. State-of-the-Art
2.1. Sleep Disturbances in the Case of Cancer-Related Fatigue (CrF)
In spite of severe cancer-related fatigue (CrF) [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27] and its perceptions [43,54,58,63,64,67] in cancer patients, there is often also a high prevalence of sleep disturbances (30–50%) in which the proportion of poor sleep or bad sleep quality is significantly higher than in the general population [6,21,23,58,64] (Table 2). Due to frequent “naps” during the day caused by CrF, an additional increase in nocturnal problems can observed [1].
For the research of sleep and quality of sleep, the easy-to-use actigraphy is commonly used [89,90]. Actigraphy data from various studies have shown that there is a strong correlation between the changes in subjectively experienced CrF and sleep quality [2,10,16]. Therefore, CrF-induced sleep disorders can be used as a well-quantifiable CrF-induced event to diagnose and control the course of CrF. Table 1 shows the four sleep-specific phenotypes according to which patients with chronic fatigue syndrome can be classified by means of the more elaborate, but more informative, polysomnography [11].

Table 1.
Sleep-specific phenotypes of fatigue (according to Reference [11]).
2.2. Insomnia in Cancer
Insomnia is a very common and frequent comorbidity in cancer patients. The cancer-related insomnia rate is nearly three times higher than that in the general population. Different analyses have shown that 30–50% (up to 95%) of cancer patients have severe sleep difficulties, such as insomnia symptoms or insomnia syndromes (Tables 3–5). Cancer-related insomnia is characterized by a delayed sleep onset, sleep maintenance disorders, reduced total sleep time and/or early-morning awakenings and is associated with excessive daytime sleepiness, fatigue, impaired performance and daytime wellbeing. Furthermore, we established a connection between insomnia and pain, depression, anxiety and/or a reduced quality of life [27,43,53,54,58,63,64,65]. Various types of treatments for insomnia include pharmacological therapies (e.g., hypnotica, sedativa, antidrepressiva, neuroleptics, antihistamine, hormones (melatonin) and herbal extracts) [28,30,42,44,48,57] and nonpharmacological therapies (like Psychoeducational intervention, Cognitive Behavior Therapy (CBT), Professionally administered CBT (PCBT), Video-based CBT (VCBT), Behavioral Therapy (BT), Individualized Sleep Promotion Plan (ISPP), Mindfulness-Based Stress Reduction (MBSR), Valencia model of Waking hypnosis, Internet intervention/Sleep Healthy Using The internet (SHUTi), Progressive Muscle Relaxation (PMR), Autogenic Training (AT), (Electro)Acupuncture (EA), Tai Chi Chih (TCC), Cool Pad Pillow Topper (CPPT), Combined multimodal-aerobic Treatment (CT), Multimodal Treatment (MT) and Aerobic Treatment (AeT)) [29,31,32,33,34,35,36,37,38,39,40,41,44,46,47,49,50,51,52,55,56,57,59,61,62,66,67,68,69,70,71]. Most of the patients with comorbid cancer-related insomnia (that means around 25–50%) are treated pharmacologically [31]. Especially, cancer patients have many side effects and sevaral physical problems from this kind of treatment, so there are numerous limitations that emerge from these pharmacological treatments. Such side effects generally include headaches, dizziness, fatigue, excessive daytime sleepiness and residual daytime sedation and could be potentiated in cancer patients [31]. There is a need and use of complementary and alternative medical methods in cancer patients with cancer-related insomnia. Recent research has shown that complementary and alternative treatments may provide a clinically relevant benefit in cancer-related insomnia [29,31,32,33,34,35,36,37,38,39,40,41,44,46,47,49,50,51,52,55,56,57,59,61,62,66,67,68,69,70,71].
2.3. Sleep-Related Breathing Disorder (SRBD)/Obstructive Sleep Apnea Syndrome (OSAS) in Cancer
Sleep-related breathing disorders (SRBD), especially obstructive sleep apnea syndrome, (OSAS) are common disorders that are characterised by repetitive interruptions of ventilation during sleep. They are caused by recurrent (upper) airway collapses and follwed by sleep fragmentation, intermitted hypoxia and oxidative stress. Systemic and vascular inflammations with endothelial dysfunctions cause diverse multiorgan chronic morbidities and mortalities that affect the cerebrovascular, cardiovascular and metabolic systems in the progress to cancer. Sleep-related breathing disorders are an independent risk factor for cerebrovascular diseases, cardiovascular diseases, metabolic diseases and cognitive decline and are associated with high rates of morbidity and mortality [72,73,74,75,76,77,78,79,80,81,82].
Chronic and intermittent hypoxias seem to play a key role in the regulation of various stages of tumor formation and their progressions. In recent years, some important studies have shown that OSAS patients tend to have a higher prevalence and incidence of cancer and even a higher prevalence of cancer-related mortality [72,73,74,75,76,77,78,79,80,81,82]. One article was able to show that early CPAP treatment can reduce these prevalences: In vitro studies have shown that, in OSAS, there are pro-oncogenic hypoxia properties that are mediate mainly by enhanced posttranslational HIF effects. Intermittant hypoxia results in the increased expression of vascular endothelial growth factor (VEGF) and in tumor growth and metastasis. An effective OSAS treatment coud prevent cancer, its growth and/or metastasis [74] (Tables 3 and 6).
2.4. Narcolepsy in Cancer
The cancer risk as a comorbidity profile of narcoleptic patients has been rarely analyzed [83,84,85] (Tables 3 and 7). There exist only two case studies, and one evaluated the Taiwan nationwide database. Tseng et al. researched the risk of cancer (incidence) among adult narcoleptics [85]. They found that adult narcoleptic patients have a higher risk for developing cancer, but the study was not able to describe the underlying mechanisms for this [83,84,85]. Further research is needed to understand the association between narcolepsy and the development of cancer.
2.5. Restless Legs Syndrome (RLS) in Cancer
Decreased sleep quality, sleep disturbences and/or sleep disruption are very common in cancer patients, especially when they receive chemotherapy [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26] (Tables 3 and 7). Until now the processes and their pathophysiology have not been completely understood, but most likely, they are multifactorial [86]. Additionally, disturbed sleep and sleep disorders like insomnia and OSAS as disorders and/or diseases with pain, fatigue and mood disturbances often occur in clusters. These clusters can negatively impact the quality of life and the outcome of diseases [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26]. Sleep disturbance, fatigue and mood disorders (like depression and anxiety) can be based on distinct biologic processes. These processes could be the trigger for inflammatory signaling as a contributing factor of restless legs syndrome (RLS) [86].
The prevalence and/or incidence of restless legs syndrome in cancer is insufficiently researched. A recent study of Saini et al. showed that RLS is frequent in patients with cancer during chemotherapy. They demonstrated that the prevalence is approximately double compared to the normal population (around 18%). In most cases, restless legs syndrome was correlated with depression, anxiety and a decreased quality of life [86].
2.6. REM Sleep Behavior Disorder in Cancer
Rapid Eye Movement Sleep Behavior Disorders (REM-SBD) and cancer are very seldom reported [83,87,88] (Tables 3 and 9). REM-SBD are forms of parasomnias. They are characterised by severe dream-related behavior and increased abnormal electromyographic activity during REM sleep. Sometimes, they are associated with nightmares and parvor nocturnus [83,87,88]. The excessive electromyographic activity during REM sleep reflects the dysfunction of the brainstem structures in REM-SBD patients [87]; acutely, they can be caused by different medications, such as antidepressants or anticholinergic drugs [88].
3. Method
3.1. Data Sources
This review was guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting process where applicable [91].
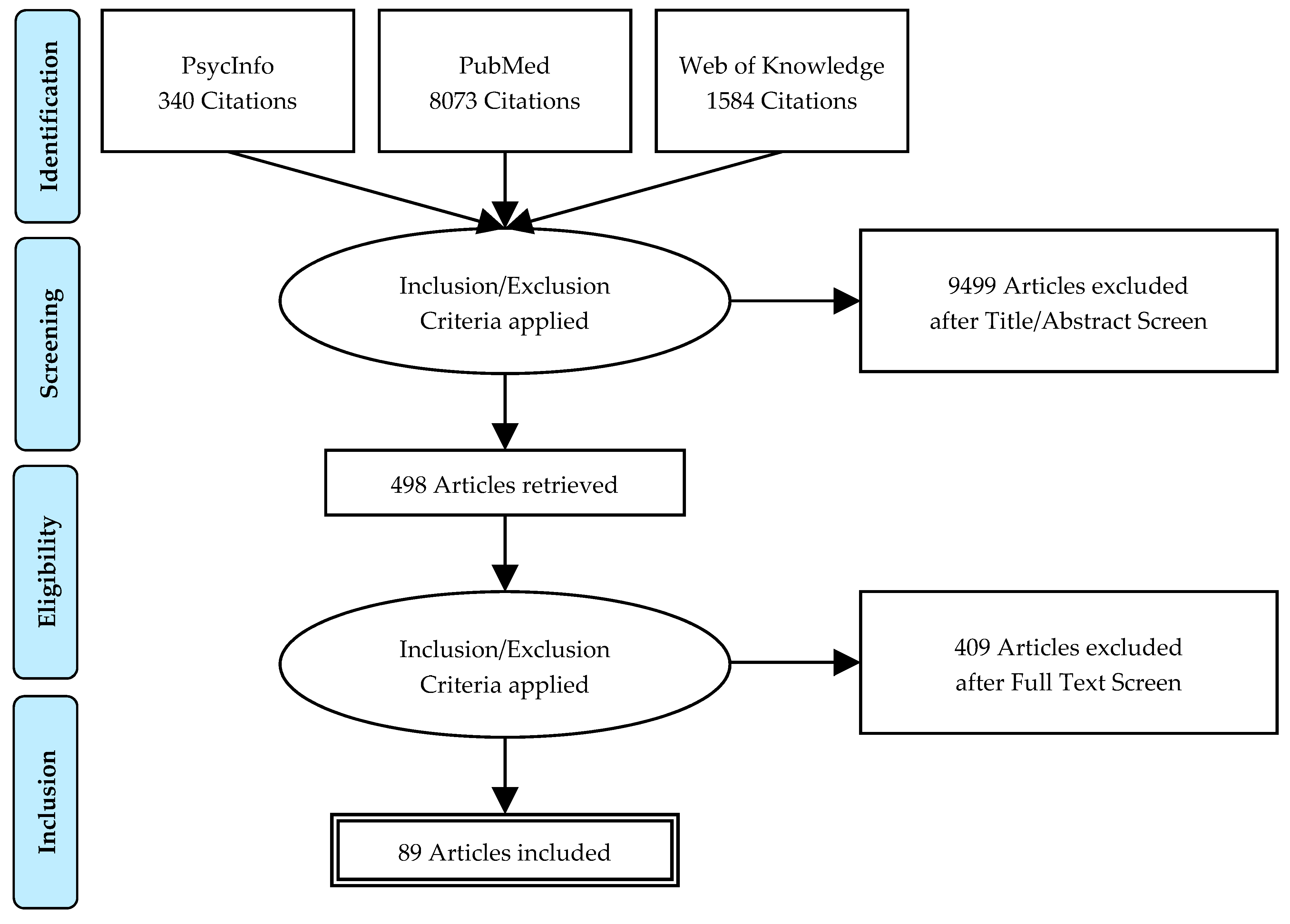
A systematic literature search was carried out on January 2019 of the databases PubMed, PsycInfo and Web of Knowledge (Figure 1).
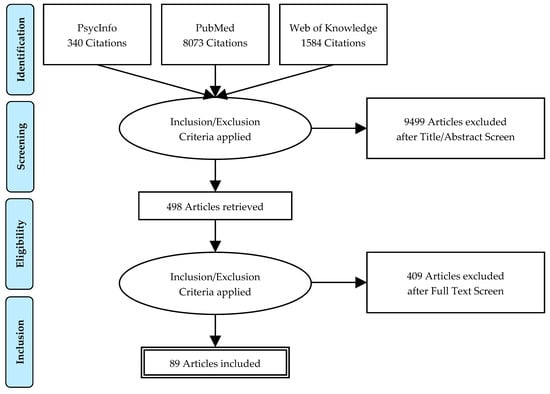
Figure 1.
PRISMA flowchart of a systematic review of sleep andand fatigue in cancer.
The search terms included the following keywords and keyword combinations (sleep OR sleep quality OR sleep disorders OR insomnia OR sleep-related breathing disorder OR obstructive sleep apnea syndrome OR narcolepsy OR restless legs syndrome) OR REM sleep behavior disorder (REM-SBD) AND (cancer) (AND (fatigue)) in English. The keywords were combined as pairs, e.g., sleep disorders AND cancer.
In addition, the reference lists of all of the obtained studies were evaluated. Hard copies of all of the articles were obtained, and they were fully read.
For the analyses of sleep disorders in cancer, only studies from the period 1999/2000–2018 were included in the review, with three exceptions: two studies about sleep and cancer-related fatigue (CrF) in cancer from 1983 to 1993 and a study about OSAS and cancer from 1988. For the analysis of sleep and fatigue in cancer, we even included some older ones.
The 8073 publications were found in the three databases—498 articles were read, and a total number of 89 publications were included in the final analysis.
3.2. Types of Studies
Randomized controlled trials (RCTs) and quasi-randomized controlled trials (qRCTs), prospective and retrospective studies, cross-sectional surveys, uncontrolled studies and controlled trials without randomization methods, a special article and case studies were included in this systematic review, because important literature was very rare and inconsistent. We only excluded any forms of qualitative studies.
3.3. Types of Participants
Participants who were diagnosed with a sleep disorder (insomnia, sleep-related breathing disorder (SRBD)/obstructive sleep apnea syndrome (OSAS), narcolepsy, restless legs syndrome (RLS) and REM-sleep behavior disorder (REM-SBD)) due to cancer (regardless of gender and age) were included.
3.4. Types of Intervention
The review included studies that evaluated different types of insomnia interventions: nonpharmacological interventions—Psychoeducational intervention, Cognitive Behavior Therapy (CBT), Professionally administered CBT (PCBT), Video-based CBT (VCBT), Behavioral Therapy (BT), Individualized Sleep Promotion Plan (ISPP)), Mindfulness-Based Stress Reduction (MBSR), Valencia model of Waking hypnosis, Internet intervention/Sleep Healthy Using The internet (SHUTi), Progressive Muscle Relaxation (PMR), Autogenic Training (AT), (Electro)Acupuncture (EA), Tai Chi Chih (TCC), Cool Pad Pillow Topper (CPPT), Combined multimodal-aerobic Treatment (CT), Multimodal Treatment (MT) and Aerobic Treatment (AeT) and pharmacological interventions, for example, —melatonin (hormone), mirtazapine (hypnoticum); herbal extracts—valerian.
3.5. Types of Outcomes
3.5.1. Primary Outcomes
- 1.
- The prevalence and/or the incidence of sleep disturbences and/or sleep disorders in cancer were evaluated firstly by objective measurements—polysomnography (PSG)/gold standard and polygraphy (PG) for OSAS or actigraphy. The important sleep parameters included total sleep time (TST), time in bed (TIB), sleep efficiency (SE), sleep quality (SQ), sleep onset latency (SOL), wake after sleep onset or total waking time (WASO).
- 2.
- The prevalence and/or the incidence of sleep disturbences and/or sleep disorders in cancer are measured secondly by subjective measurements—by scales or indices for the sleep quality (e.g., the Pittsburgh Sleep Quality Index (PSQI)) or special sleep disorders: insomnia (e.g., Insomnia Severity Index (ISI), Athens Insomnia Scale (ASI)), OSAS (e.g., Berlin questionnaire), Narcolepsy (e.g., Narcolepsy Symptom Questionnaire (NSQ)) or RLS (International Restless Legs Syndrome Study Group rating scale (IRLS)).
3.5.2. Secondary Outcomes
The effectiveness of insomnia treatments are measured with sleep diaries. Generally, they include various subjective approaches or several items for reflecting the subjective assessment of daily night’s sleep, including the total sleep time (TST), time in bed (TIB), sleep efficiency (SE), sleep quality (SQ), satisfaction of sleep onset latency (SOL), wake after sleep onset, total waking time (WASO), number of awakenings and morning woken-up time.
3.6. Selection of Studies and Data Extraction
The databases PubMed, PsycInfo and Web of Knowledge were searched and potentially studies screened: After the initial screening with checking the titles and abstracts, all the full-text articles were read. The articles that were included in the review were identified, and the data, according to predefined criteria, were extracted. Information such as samples (e.g., kind and number of participants), interventions (in the case of insomnia), measuring instruments, measuring times, methods, outcomes and results were obtained and documented from each study.
4. Results
Twenty-six studies for the topic of sleep and fatigue in cancer and sixty-one studies for the topic of sleep disorders in cancer were analyzed, one for sleep disorders generally, forty-four studies for the topic “Insomnia in Cancer” (eight for the “Prevalence of Insomnia in Cancer” and thrirty-six for the “Treatment of Insomnia in Cancer”), twelve studies for the topic “Sleep-Related Breathing Disorder (SRBD)/Obstructive Sleep Apnea Syndrome (OSAS) in Cancer”, three studies for the topic “Narcolepsy in Cancer”and one study for the topic “Restless Legs Syndrome (RLS) in Cancer” (Table 2, Table 3, Table 4, Table 5, Table 6, Table 7, Table 8 and Table 9).
Table 2.
Studies on Sleep and Cancer-related Fatigue (CrF) in cancer/Connection between sleep and fatigue in oncological diseases.
Table 3.
Study on Sleep Disorders in cancer.
Table 4.
Studies on Insomnia in cancer.
Table 5.
Studies on Insomnia Treatment in cancer.
Table 6.
Studies on Sleep-Related Breathing Disorder (SRBD)/Obstructive Sleep Apnea Syndrome (OSAS) in Cancer.
Table 7.
Studies on Narcolepsy in cancer.
Table 8.
Studies on Restless Legs Syndrome (RLS) in cancer.
Table 9.
Studies on REM Sleep Behaviour Disorder (REM-SBD) in cancer.
5. Discussion
Sleep disturbances and sleep disorders in cancer patients are very common and have different backgrounds compared with sleep difficulties in normal populations because of the differences in the risk factors, vulnerability and cancer-specific life events.
A personalized treatment of sleep disorders in patients with cancer could improve both their mental and physical health.
The goal of this review was to illuminate approaches that might influence sleep, sleep quality and sleep disorders in cancer patients and treatment possibilities in cancer-related insomnia. However, before treatment trials in different sleep disorders (insomnia, OSAS, narcolepsy, RLS and REM-SBD) can be started, prospective and objective studies are needed to unterstand the baseline levels of sleep, sleep difficulties and circadian rhythm in cancer. Sleep disruption in cancer can be caused by many different reasons, such as stress, mental disorders (like depression and anxiety), pain and treatment side effects.
Bad sleep quality, the degree of sleep disruption and sleep disorders have a very important impact on cancer and can used as predictors. Sleep disruptions and disruptions in the circadian rhythms affecting the sleep quality and the circadian rhythm themselves can result in a variety of psychological and physiological mechanisms, which can foster the developent and persistance of cancer-related fatigue. The role of naps in fatigued cancer patients is unclear; it could be that naps are not helpful to decrease cancer-related fatigue—they could have the opposite effect [17]. In noncancer patients, it is known that daytime naps reduce the nightly sleep quality and total sleep time.
Although the relationship between fatigue, sleep and circadian rhythms in cancer is known, there is a very small quantity of scientific reseach about this topic, and the quality is mostly very poor. The existing literature and research is inhomogeneous, and there are many methodological limitations: the types of studies (e.g., randomized controlled trials, quasi-randomized controlled trials, prospective and retrospective studies, cross-sectional surveys, uncontrolled studies and controlled trials without randomization methods, a special article and case studies); participants (different kinds of cancer patients—e.g., with or without treatment and with different entities); interventions (in the case of insomnia: nonpharmacological and pharmacological interventions); outcomes (objective and/or subjective measurements) are not comparable and the sample sizes are mostly very small.
Davidson et al. found in a big sample size with nearly a thousand patients that the total prevalence scores of RLS were present in nearly half of the researched cancer patients, of overly sleepy and of insomnia in around one-third of the patients, of sleeping more than usual and repetitive leg movements in almost one-fifth of them and of breathing interruptions in approximately ten percent [27].
The causes of decreased sleep quality; chronic sleep difficulties and the different sleep disorders (insomnia, OSAS, narcolepsy, RLS and REM-SBD) are multifaceted, and in recent studies, the attention that was paid this problem was too insufficient. Until now, the pathogenesis of cancer-related sleep disorders and the development such as the progression of cancer based on sleep disorders has been unclear. More research about these topics is needed to understand the nature, duration and severity of the different sleep disorders in cancer or their relationship with it.
The prevention of sleep disorders generally and in cancer patients especially and an early personalized treatment can contribute to reducing cancer-related fatigue and severe mental disorders (like depression and anxiety) and can possibily prevent the development, preservation and/or aggravation of cancer.
5.1. Expert Recommendations
Sleep disturbances; disruptions of the circadian rhythms and different sleep disorders (e.g., insomnia and sleep-related breathing disorder (SRBD)/obstructive sleep apnea syndrome (OSAS)) could be predictors of cancer development and treatment success (look above). Due to that, cancer patients should be screened by sleep anamnesis and/or by sleep diaries, including the structured exploration of predisposing and precipitating cancer factors, and should be diagnosed—in the case of any kind of sleep-wake difficulties—by polysomnography.
Screening should explore unrefreshing sleep: prolonged sleep latency, frequent awakening and reduced sleep efficiency; daytime sleepiness and fatigue; loud snoring; inadequate nightly behavior and/or nightmares.
Both screening and/or the diagnosis of sleep disturbances; disruptions of the circadian rhythm and/or sleep disorders, as well as adequate sleep health education (including sleep hygiene, rules for good sleep quality and information about the consequences of unhealthy and/or untreated sleep disorders for mental and physical health) should be implemented to minimize the health risks caused by sleep disorders.
Tailored programs are needed and could be helpful to reduce cancer-related fatigue and/or severe mental disorders (like depression and anxiety) to support the outcome of the treatment of patients with cancer and comorbid sleep disorders.
Currently, sleep–wake solutions in cancer are mostly aimed only by responding to emergency reasons and based on isolated and/or fragmented interventions, e.g., the treatment of insomnia: cognitive behavioral therapy for insomnia, nightmares: rehearsal therapy and SRBD: CPAP adherence.
Peronalized medical services for cancer patients should include integrated coaching or the early treatment of the most common sleep disorders and web-based telehealth programs [92] to reduce the preservation and/or aggravation of cancer an/or serious implications, including increased cerebrovascular, cardiovascular and/or metabolic diseases; excessive daytime sleepiness and/or cancer-related fatigue.
5.2. References Classification
Studies on Sleep and Cancer-related Fatigue (CrF) in cancer/Connection between sleep and fatigue in oncological diseases [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26]; Sleep Disorders (generally) [27]; Insomnia (total) [28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71]; Sleep-Related Breathing Disorder (SRBD)/Obstructive Sleep Apnea Syndrome (OSAS) [72,73,74,75,76,77,78,79,80,81,82]; Narcolepsy [83,84,85]; Restless Legs Syndrome (RLS) [86]; REM Sleep Behaviour Disorder (REM-SBD) [83,87,88]; Others (Devices & Methods) [89,90,91,92].
6. Conclusions
Cancer patients can suffer under different sleep disturbances and sleep disorders, and these difficulties can be associated with different mental and/or physical problems. Side effects of cancer treatment and cancer-related psychological dysfunctions can be triggered it. Especially insomnia and OSAS are very common in cancer. Because of it, an evidence-based and tailored treatment is necessary.
Author Contributions
Literature research, discussion, evaluation and conceptualization: A.B.-T., Y.-T.K. and K.R.; writing—original draft: A.B.-T. and writing—review and editing: A.B.-T., K.R. and T.O. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Conflicts of Interest
All the authors state that they do not have any conflicts of interest.
Abbreviations
| Disorders | |
| CA | Carcinoma |
| CrF | Cancer-related Fatigue |
| CRFS | Cancer-related Fatigue Syndrome |
| CRSD | Cancer-Related Sleep Disorders |
| OSA(S) | Obstructive Sleep Apnea (Syndrome) |
| REM-SBD | REM-Sleep Behavior Disorder |
| RLS | Restless Legs Syndrome |
| SRBD | Sleep-Related Breathing Disorder |
| Measurements | |
| MESAM | Madaus Electronic Sleep Apnea Monitor |
| MRI | Magnetic Resonance Imaging |
| OSP | Objective Sleep Parameters |
| PG | Polygraphy |
| PSG | Polysomnography |
| SSP | Subjective Sleep Parameters |
| Anthropomeric and Clinical Data | |
| CRP | C-Reactive Protein |
| IFN-γ | Interferon gamma |
| IL-6/-1β | Interleukin-6/Interleukin-1-beta |
| IL-1RA | Interleukin-1 Receptor Antagonist |
| QoL | Quality of Life |
| TNF | Tumor Necrosis Factor |
| Therapies | |
| AeT | Aerobic Treatment |
| AT | Autogenic Training |
| BT | Behavioral Therapy |
| CBT | Cognitive Behavior Therapy |
| CPPT | Cool Pad Pillow Topper |
| CPAP | Continuous Positive Airway Pressure |
| CT | Combined Multimodal-Aerobic Treatment |
| EA | Electro-Acupuncture |
| ISPP | Individualized Sleep Promotion Plan |
| MBSR | Mindfulness-Based Stress Reduction |
| MT | Multimodal Treatment |
| PMR | Progressive Muscle Relaxation |
| PCBT | Professionally administered CBT |
| SHUTi | Sleep Healthy Using the Internet |
| SC | Standard Care |
| TCC | Tai Chi Chi |
| VCBT | Video-based CBT |
| Sleep Parameters | |
| TST | Total Sleep Time |
| TIB | Time in Bed |
| SE | Sleep Efficiency |
| SQ | Sleep Quality |
| SOL | Sleep*Onset*Latency |
| SWS | Slow Wave Sleep |
| WASO | Wake after Sleep*Onset or Total Waking Time |
| Questionnaires | |
| ABS | Adherence to Behavioral Strategies |
| ASI | Athens Insomnia Scale |
| BCPT | Breast Cancer Prevention Trial |
| BDI | Becks Depression Inventory |
| BDSS | Blood Deficiency Scoring System |
| BFI | Brief Fatigue Inventory |
| CES-D | Center for Epidemiologic Studies—Depression Scale |
| CFS-D | Cancer Fatigue Scale |
| C-LSEQ | Chonnam National University Hospital—Leeds Sleep Evaluation Questionnaire |
| CrQoL | Cancer-Related Quality of Life |
| CTCAE | Common Terminology Criteria for Adverse Events |
| DBAS | Dysfunctional Beliefs and Attitudes about Sleep Scale |
| ESS | Epworth Sleepiness Scale |
| EQ-5D | Euro QoL |
| FACT | Functional Assessment Cancer Therapy |
| FOSQ | Functional Outcomes of Sleep Questionnaire |
| FSI | Fatigue Symptom Inventory |
| GSDS | General Sleep Disturbance Scale |
| HADS | Hospital Anxiety and Depression Scale |
| HDI | Hamilton Depression Inventory |
| NCCTG | North Central Cancer Treatment Group |
| PSQI | Pittsburgh Sleep Quality Index |
| IES-R | Revised Impact of Event Scale |
| IIS | Insomnia Interview Schedule |
| ISI | Insomnia Severity Index |
| IRLS | International Restless Legs Syndrome Study Group rating scale |
| MADRS | Montgomery-Asberg Depression Rating Scale |
| MFSI-SF | Multidimensional Fatigue Symptom Inventory |
| MoCA | Montreal Cognitive Assessment |
| MOS | Medical Outcomes Study |
| MOOS | Medical Outcomes Survey Sleep |
| MSAS | Memorial Symptom Assessment Scale |
| NRS | Numerical Rating Scales (Pain intensity) |
| PANAS | Positive and Negative Affect Scale |
| POMS | Profile of Mood States |
| PROMIS | Problem Index Patient-reported Outcomes Measurement Information System |
| PSQ | Physical Symptoms Questionnaire |
| QLQ-C30+ 3 | European Organization for Research and Treatment of Cancer Quality of Life Questionnaire |
| SF-12/-36 | Short Form of Health Survey |
| STAI | State Trait Anxiety Inventory |
| TAPQ | Therapeutic Alliance Perception Questionnaire |
| TEPCQ | Treatment Expectancies and Perceived Credibility Questionnaire |
| TNAS | Toxicity Numeric Analogue Scale |
| UQ | Internet Intervention Utility Questionnaire |
References
- Ancoli-Israel, S.; Moore, P.J.; Jones, V. The relationship between fatigue and sleep in cancer patients: A review. Eur. J. Cancer Care 2001, 10, 245–255. [Google Scholar] [CrossRef] [Green Version]
- Ancoli-Israel, S.; Liu, L.; Marler, M.R.; Parker, B.A.; Jones, V.; Sadler, G.R.; Dimsdale, J.; Cohen-Zion, M.; Fiorentino, L. Fatigue, sleep, and circadian rhythms prior to chemotherapy for breast cancer. Support. Care Cancer 2006, 14, 201–209. [Google Scholar] [CrossRef] [Green Version]
- Ancoli-Israel, S.; Liu, L.; Rissling, M.; Natarajan, L.; Neikrug, A.B.; Palmer, B.; Mills, P.J.; Parker, B.A.; Sadler, G.R.; Maglione, J. Sleep, fatigue, depression, and circadian activity rhythms in women with breast cancer before and after treatment: A 1-year longitudinal study. Support. Care Cancer 2014, 22, 2535–2545. [Google Scholar] [CrossRef]
- Banthia, R.; Malcarne, V.L.; Ko, C.M.; Varni, J.W.; Sadler, G.R. Fatigued breast cancer survivors: The role of sleep quality, depressed mood, stage and age. Psychol. Heal. 2009, 24, 965–980. [Google Scholar] [CrossRef] [Green Version]
- Berger, A.M.; Farr, L. The influence of daytime inactivity and nighttime restlessness on cancer-related fatigue. Oncol. Nurs. Forum 1999, 26, 1663–1671. [Google Scholar] [PubMed]
- Chang, V.T.; Hwang, S.S.; Feuerman, M.; Kasimis, B.S. Symptom and quality of life survey of medical oncology patients at a Veterans Affairs medical center. Cancer 2000, 88, 1175–1183. [Google Scholar] [CrossRef]
- Cimprich, B. Pretreatment symptom distress in women newly diagnosed with breast cancer. Cancer Nurs. 1999, 22, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Clevenger, L.; Schrepf, A.; Christensen, D.; DeGeest, K.; Bender, D.; Ahmed, A.; Goodheart, M.J.; Penedo, F.; Lubaroff, D.M.; Sood, A.K.; et al. Sleep disturbance, cytokines, and fatigue in women with ovarian cancer. Brain Behav. Immun. 2012, 26, 1037–1044. [Google Scholar] [CrossRef] [Green Version]
- Engstrom, C.A.; Strohl, R.A.; Rose, L.; Lewandowski, L.; Stefanek, M.E. Sleep alterations in cancer patients. Cancer Nurs. 1999, 22, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Fiorentino, L.; Rissling, M.; Liu, L.; Ancoli-Israel, S. The symptom cluster of sleep, fatigue and depressive symptoms in breast cancer patients: Severity of the problem and treatment options. Drug Discov. Today Dis. Model. 2011, 8, 167–173. [Google Scholar] [CrossRef] [Green Version]
- Gotts, Z.M.; Deary, V.; Newton, J.; Van der Dussen, D.; De Roy, P.; Ellis, J.G. Are there sleep-specific phenotypes in patients with chronic fatigue syndrome? A cross-sectional poly-somnography analysis. BMJ Open 2013, 3, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Illi, J.; Miaskowski, C.; Cooper, B.; Levine, J.D.; Dunn, L.; West, C.; Dodd, M.; Dhruva, A.; Paul, S.M.; Baggott, C.; et al. Association between pro- and anti-inflammatory cytokine genes and a symptom cluster of pain, fatigue, sleep disturbance, and depression. Cytokine 2012, 58, 437–447. [Google Scholar] [CrossRef] [Green Version]
- Kaye, J.; Kaye, K.; Madow, L. Sleep pattern in patients with cancer and cardiac disease. J. Psychol. 1983, 114, 107–113. [Google Scholar] [CrossRef]
- Liu, L.; Fiorentino, L.; Natarajan, L.; Parker, B.A.; Mills, P.J.; Sadler, G.R.; Dimsdale, J.E.; Rissling, M.; He, F.; Ancoli-Israel, S. Pre-treatment symptom cluster in breast cancer patients is associated with worse sleep, fatigue and depression during chemotherapy. Psycho Oncol. 2009, 18, 187–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, L.; Rissling, M.; Natarajan, L.; Fiorentino, L.; Mills, P.J.; Dimsdale, J.E.; Sadler, G.R.; Parker, B.A.; Ancoli-Israel, S. The Longitudinal Relationship between Fatigue and Sleep in Breast Cancer Patients Undergoing Chemothera-py. Sleep 2012, 35, 237–245. [Google Scholar] [CrossRef]
- Liu, L.; Mills, P.J.; Rissling, M.; Fiorentino, L.; Natarajan, L.; Dimsdale, J.E.; Sadler, G.R.; Parker, B.A.; Ancoli-Israel, S. Fatigue and sleep quality are associated with changes in inflammatory markers in breast cancer patients undergoing chemotherapy. Brain Behav. Immun. 2012, 26, 706–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miaskowski, C.h.; Lee, K.A. Pain, Fatigue, and Sleep Disturbances in Oncology Outpatients Receiving Radiation Therapy for Bone Metastasis: A Pilot Study. J. Pain Symptom Manag. 1999, 17, 320–332. [Google Scholar] [CrossRef]
- Mormont, M.C.; De Prins, J.; Levi, F. Study of circadian rhythms of activity by actometry: Preliminary results in 30 patients with metastat-ic colorectal cancer. Pathol. Biol. (Paris) 1996, 44, 165–171. [Google Scholar]
- Mormont, M.C.; Waterhouse, J.; Bleuzen, P.; Giacchetti, S.; Jami, A.; Bogdan, A.; Lellouch, J.; Misset, J.L.; Touitou, Y.; Lévi, F. Marked 24-h rest/activity rhythms are associated with better quality of life, better response, and longer survival in patients with metastatic colorectal cancer and good performance status. Clin. Cancer Res. 2000, 6, 3038–3045. [Google Scholar] [PubMed]
- Roscoe, J.A.; Morrow, G.R.; Hickok, J.T.; Bushunow, P.; Matteson, S.; Rakita, D.; Andrews, P.L. Temporal interrelationships among fatigue, circadian rhythm and de-pression in breast cancer patients undergoing chemotherapy treatment. Support Care Cancer 2002, 10, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Mustian, K.M.; Sprod, L.K.; Janelsins, M.; Peppone, L.J.; Mohile, S. Exercise Recommendations for Cancer-Related Fatigue, Cognitive Impairment, Sleep problems, Depression, Pain, Anxiety, and Physical Dysfunction: A Review. Oncol. Hematol. Rev. (US) 2012, 8, 81–88. [Google Scholar] [CrossRef] [Green Version]
- Owen, D.C.; Parker, K.P.; McGuire, D.B. Comparison of subjective sleep quality in patients with cancer and healthy subjects. Oncol. Nurs. Forum 1999, 26, 1649–1651. [Google Scholar]
- Palesh, O.G.; Roscoe, J.A.; Mustian, K.M.; Roth, T.; Savard, J.; Ancoli-Israel, S.; Heckler, C.; Purnell, J.; Janelsins, M.C.; Morrow, G.R. Prevalence, Demographics, and Psychological Associations of Sleep Disruption in Patients with Cancer: University of Rochester Cancer Center–Community Clinical Oncology Program. J. Clin. Oncol. 2010, 28, 292–298. [Google Scholar] [CrossRef]
- Reyes-Gibby, C.C.; Wu, X.; Spitz, M.; Kurzrock, R.; Fisch, M.; Bruera, E.; Shete, S. Molecular epidemiology, cancer-related symptoms, and cytokines pathway. Lancet Oncol. 2008, 9, 777–785. [Google Scholar] [CrossRef] [Green Version]
- Roscoe, J.A.; Kaufman, M.E.; Matteson-Rusby, S.E.; Palesh, O.G.; Ryan, J.L.; Kohli, S.; Perlis, M.L.; Morrow, G.R. Cancer-Related Fatigue and Sleep Disorders. Oncol. 2007, 12, 35–42. [Google Scholar] [CrossRef] [Green Version]
- Silberfarb, P.M.; Hauri, P.J.; Oxman, E.T.; Schnurr, P. Assessment of sleep in patients with lung cancer and breast cancer. J. Clin. Oncol. 1993, 11, 997–1004. [Google Scholar] [CrossRef]
- Davidson, J.R.; MacLean, A.W.; Brundage, M.D.; Schulze, K. Sleep disturbance in cancer patients. Soc. Sci. Med. 2002, 54, 1309–1321. [Google Scholar] [CrossRef]
- Barton, D.L.; Atherton, P.J.; Bauer, B.A.; Moore, D.F., Jr.; Mattar, B.I.; LaVasseur, B.I.; Rowland, K.M., Jr.; Zon, R.T.; Lelindqwister, N.A.; Nagargoje, G.G.; et al. The Use of Valeriana Officinalis (Valerian) in Improving Sleep in Patients Who Are Undergoing Treatment for Cancer: A Phase III Randomized, Placebo-Controlled, Double-Blind Study: NCCTG Trial, N01C5. J. Support. Oncol. 2011, 9, 24–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, A.M.; Kuhn, B.R.; Farr, L.A.; Lynch, J.C.; Agrawal, S.; Chamberlain, J.; Von Essen, S.G. Behavioral therapy intervention trial to improve sleep quality and cancer-related fatigue. Psycho Oncol. 2008, 18, 634–646. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.Y.; Giobbie-Hurder, A.; Gantman, K.; Savoie, J.; Scheib, R.; Parker, L.M.; Schernhammer, E.S. A randomized, placebo-controlled trial of melatonin on breastcancer survivors: Impact on sleep, mood, and hot flashes. Breast Cancer Res Treat. 2014, 145, 381–388. [Google Scholar] [CrossRef] [Green Version]
- Choi, T.-Y.; Kim, J.I.; Lim, H.-J.; Lee, M.S. Acupuncture for Managing Cancer-Related Insomnia: A Systematic Review of Randomized Clinical Trials. Integr. Cancer Ther. 2017, 16, 135–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dupont, A.; Bower, J.E.; Stanton, A.L.; Ganz, P.A. Cancer-related intrusive thoughts predict behavioral symptoms following breast cancer treatment. Heal. Psychol. 2014, 33, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Epstein, D.R.; Dirksen, S.R. Randomized Trial of a Cognitive-Behavioral Intervention for Insomnia in Breast Cancer Survivors. Oncol. Nurs. Forum 2007, 34, 51–59. [Google Scholar] [CrossRef]
- Espie, C.A.; Fleming, L.; Cassidy, J.; Samuel, L.; Taylor, L.M.; White, C.A.; Douglas, N.J.; Engleman, H.M.; Kelly, H.L.; Paul, J.; et al. Randomized Controlled Clinical Effectiveness Trial of Cognitive Behavior Therapy Compared with Treat-ment As Usual for Persistent Insomnia in Patients with Cancer. J. Clin. Oncol. 2008, 26, 4651–4658. [Google Scholar] [CrossRef]
- Fiorentino, L.; McQuaid, J.R.; Liu, L.; Natarajan, L.; He, F.; Cornejo, M.; Lawton, S.; Parker, B.A.; Sadler, G.R.; Ancoli-Israel, S.; et al. Individual cognitive behavioral therapy for insomnia in breast cancer survivors: A randomized con-trolled crossover pilot study. Nature and Science of Sleep 2010, 2, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Fleming, L.; Randell, K.; Harvey, C.-J.; Espie, C.A. Does cognitive behaviour therapy for insomnia reduce clinical levels of fatigue, anxiety and depression in cancer patients? Psycho Oncol. 2014, 23, 679–684. [Google Scholar] [CrossRef] [Green Version]
- Garland, S.N.; Carlson, L.; Antle, M.C. I-CAN SLEEP: Rationale and design of a non-inferiority RCT of Mindfulness-based Stress Reduction and Cognitive Behavioral Therapy for the treatment of Insomnia in CANcer survivors. Contemp. Clin. Trials 2011, 32, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Garland, S.N.; Carlson, L.E.; Stephens, A.J.; Antle, M.C.; Samuels, C.; Campbell, T.S. Mindfulness-Based Stress Reduction Compared with Cognitive Behavioral Therapy for the Treatment of Insomnia Comorbid with Cancer: A Randomized, Partially Blinded, Noninferiority Trial. J. Clin. Oncol. 2014, 32, 1–9. [Google Scholar] [CrossRef]
- Garland, S.N.; Johnson, J.A.; Savard, J.; Gehrman, P.; Perlis, M.; Carlson, L.; Campbell, T. Sleeping well with cancer: A systematic review of cognitive behavioral therapy for insomnia in cancer patients. Neuropsychiatr. Dis. Treat. 2014, 10, 1113–1124. [Google Scholar] [PubMed] [Green Version]
- Garland, S.N.; Rouleau, C.R.; Campbell, T.; Samuels, C.; Carlson, L.E. The Comparative Impact of Mindfulness-Based Cancer Recovery (MBCR) and Cognitive Behavior Therapy for Insomnia (CBT-I) on Sleep and Mindfulness in Cancer Patients. Explore (N Y) 2015, 11, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Garland, S.N.; Gehrman, P.; Barg, F.K.; Xie, S.X.; Mao, J.J. CHoosing Options for Insomnia in Cancer Effectively (CHOICE): Design of a patient centered com-parative effectiveness trial of acupuncture and cognitive behavior therapy for insomnia. Contemp. Clin. Trials 2016, 47, 349–355. [Google Scholar] [CrossRef]
- Garland, S.N.; Roscoe, J.A.; Heckler, C.E.; Barilla, H.; Gehrman, P.; Findley, J.C.; Peoples, A.R.; Morrow, G.R.; Kamen, C.; Perlis, M.L.; et al. Effects of armodafinil and cognitive behavior therapy for insomnia on sleep continuity and daytime sleepiness in cancer survivors. Sleep Med. 2016, 20, 18–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graci, G. Pathogenesis and management of cancer-related insomnia. J. Support. Oncol. 2005, 3, 349–359. [Google Scholar] [PubMed]
- Heckler, C.E.; Garland, S.N.; Peoples, A.R.; Perlis, M.L.; Shayne, M.; Morrow, G.R.; Kamen, C.; Hoefler, J.; Roscoe, J.A. Cognitive behavioral therapy for insomnia, but not armodafinil, improves fatigue in cancer survivors with insomnia: A randomized placebo-controlled trial. Supportive Care Cancer 2016, 24, 2059–2066. [Google Scholar] [CrossRef] [PubMed]
- Howell, D.; Oliver, T.K.; Keller-Olaman, S.; Davidson, J.R.; Garland, S.; Samuels, C.; Savard, J.; Harris, C.; Aubin, M.; Olson, K.; et al. Sleep disturbance in adults with cancer: A systematic review of evidence for best practices in assessment and management for clinical practice. Ann. Oncol. 2014, 25, 791–800. [Google Scholar] [CrossRef]
- Irwin, M.R.; Olmstead, R.; Breen, E.C.; Witarama, T.; Carrillo, C.; Sadeghi, N.; Arevalo, J.M.G.; Ma, J.; Nicassio, P.; Ganz, P.A.; et al. Tai Chi, Cellular Inflammation, and Transcriptome Dynamics in Breast Cancer Survivors with Insomnia: A Randomized Controlled Trial. J. Natl. Cancer Inst. Monogr. 2014, 2014, 295–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.; Kim, J.-E.; Lee, H.-Y.; Kim, A.-R.; Park, H.-J.; Kwon, O.-J.; Kim, B.-K.; Cho, J.H.; Kim, J.-H. Electroacupuncture for treating insomnia in patients with cancer: A study protocol for a randomised pilot clinical trial. BMJ Open 2017, 7, e016269. [Google Scholar] [CrossRef]
- Kim, S.-W.; Shin, I.-S.; Kim, J.-M.; Kim, Y.-C.; Kim, K.-S.; Kim, K.-M.; Yang, S.-J.; Yoon, J.-S. Effectiveness of mirtazapine for nausea and insomnia in cancer patients with depression. Psychiatry Clin. Neurosci. 2008, 62, 75–83. [Google Scholar] [CrossRef]
- Kröz, M.; Reif, M.; Glinz, A.; Berger, B.; Nikolaou, A.; Zerm, R.; Brinkhaus, B.; Girke, M.; Büssing, A.; Gutenbrunner, C.; et al. Impact of a combined multimodal-aerobic and multimodal intervention compared to standard aerobic treatment in breast cancer survivors with chronic cancer-related fatigue—Results of a three-armed pragmatic trial in a com-prehensive cohort design. BMC Cancer 2017, 17, 166. [Google Scholar] [CrossRef] [Green Version]
- Lengacher, C.A.; Reich, R.R.; Paterson, C.L.; Jim, H.S.; Ramesar, S.; Alinat, C.B.; Budhrani-Shani, P.; Farias, J.R.; Shelton, M.M.; Moscoso, M.S.; et al. The effects of mindfulness-based stress reduction on objective and subjective sleep parameters in women with breast cancer: A randomized controlled trial. Psycho Oncol. 2014, 24, 424–432. [Google Scholar] [CrossRef] [Green Version]
- Marshall-McKenna, R.; Morrison, A.; Stirling, L.; Hutchison, C.; Rice, A.M.; Hewitt, C.; Paul, J.; Rodger, M.; MacPherson, I.R.; McCartney, E. A randomised trial of the cool pad pillow topper versus standard care for sleep disturbance and hot flushes in women on endocrine therapy for breast cancer. Support. Care Cancer 2015, 24, 1821–1829. [Google Scholar] [CrossRef]
- Mendoza, M.; Capafons, A.; Gralow, J.; Syrjala, K.; Suárez-Rodríguez, J.; Fann, J.; Jensen, M. Randomized controlled trial of the Valencia model of waking hypnosis plus CBT for pain, fatigue, and sleep management in patients with cancer and cancer survivors. Psycho-Oncology 2016, 26, 1832–1838. [Google Scholar] [CrossRef]
- Minton, O.; Stone, P. A comparison of cognitive function, sleep and activity levels in disease-free breast cancer patients with or without cancer-related fatigue syndrome. BMJ Support. Palliat. Care 2012, 2, 231–238. [Google Scholar] [CrossRef] [Green Version]
- Park, B.; Youn, S.; Hann, C.W.C.; Yi, K.; Lee, S.; Lee, J.S.; Chung, S. Prevalence of Insomnia among Patients with the Ten Most Common Cancers in South Korea: Health Insur-ance Review and Assessment Service-National Patient Sample. Sleep Med. Res. 2016, 7, 48–54. [Google Scholar] [CrossRef]
- Peoples, A.R.; Garland, S.; Perlis, M.L.; Savard, J.; Heckler, C.E.; Kamen, C.S.; Ryan, J.L.; Mustian, K.M.; Janelsins, M.C.; Peppone, L.J.; et al. Effects of cognitive behavioral therapy for insomnia and armodafinil on quality of life in cancer survivors: A randomized placebo-controlled trial. J. Cancer Surviv. 2017, 11, 401–409. [Google Scholar] [CrossRef]
- Ritterband, L.M.; Bailey, E.T.; Thorndike, F.P.; Lord, H.R.; Farrell-Carnahan, L.; Baum, L.D. Initial evaluation of an Internet intervention to improve the sleep of cancer survivors with insomnia. Psycho Oncol. 2012, 21, 695–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roscoe, J.A.; Garland, S.; Heckler, C.E.; Perlis, M.L.; Peoples, A.R.; Shayne, M.; Savard, J.; Daniels, N.P.; Morrow, G.R. Randomized Placebo-Controlled Trial of Cognitive Behavioral Therapy and Armodafinil for Insomnia After Cancer Treatment. J. Clin. Oncol. 2015, 33, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Savard, J.; Simard, S.; Blanchet, J.; Ivers, H.; Morin, C.M. Prevalence, Clinical Characteristics, and Risk Factors for Insomnia in the Context of Breast Cancer. Sleep 2001, 24, 583–590. [Google Scholar] [CrossRef] [Green Version]
- Quesnel, C.; Savard, J.; Simard, S.; Ivers, H.; Morin, C.M. Efficacy of cognitive-behavioral therapy for insomnia in women treated for nonmetastatic breast cancer. J. Consult. Clin. Psychol. 2003, 71, 189–200. [Google Scholar] [CrossRef]
- Savard, J.; Davidson, J.R.; Ivers, H.; Quesnel, C.; Rioux, D.; Dupéré, V.; Lasnier, M.; Simard, S.; Morin, C.M. The association between nocturnal hot flashes and sleep in breast cancer survivors. J. Pain Symptom Manag. 2004, 27, 513–522. [Google Scholar]
- Savard, J.; Simard, S.; Ivers, H.; Morin, C.M. Randomized Study on the Efficacy of Cognitive-Behavioral Therapy for Insomnia Secondary to Breast Cancer, Part I: Sleep and Psychological Effects & Part II: Immunologic Effects. JCO 2005, 23, 6097–6106. [Google Scholar]
- Tremblay, V.; Savard, J.; Ivers, H. Predictors of the effect of cognitive behavioral therapy for chronic insomnia comorbid with breast cancer. J. Consult. Clin. Psychol. 2009, 77, 742–750. [Google Scholar] [CrossRef] [PubMed]
- Savard, J.; Villa, J.; Ivers, H.; Simard, S.; Morin, C.M. Prevalence, Natural Course, and Risk Factors of Insomnia Comorbid with Cancer Over a 2-Month Period. J. Clin. Oncol. 2009, 27, 5233–5239. [Google Scholar] [CrossRef]
- Savard, J.; Ivers, H.; Villa, J.; Caplette-Gingras, A.; Morin, C.M. Natural Course of Insomnia Comorbid with Cancer: An 18-Month Longitudinal Study. J. Clin. Oncol. 2011, 29, 3580–3586. [Google Scholar] [CrossRef] [PubMed]
- Savard, J.; Hervouet, S.; Ivers, H. Prostate cancer treatments and their side effects are associated with increased insomnia. Psycho-Oncology 2012, 22, 1381–1388. [Google Scholar] [CrossRef] [PubMed]
- Casault, L.; Savard, J.; Ivers, H.; Savard, M.-H. A randomized-controlled trial of an early minimal cognitive-behavioural therapy for insomnia comorbid with cancer. Behav. Res. Ther. 2013, 67, 45–54. [Google Scholar] [CrossRef]
- Savard, J.; Savard, H.-M. Insomnia and Cancer. Prevalence, Nature, and Nonpharmacologic Treatment. Sleep Med. Clin. 2013, 8, 373–387. [Google Scholar] [CrossRef]
- Savard, J.; Ivers, H.; Savard, M.H.; Morin, C.M. Is a Video-Based Cognitive Behavioral Therapy for Insomnia as Efficacious as a Professionally Adminis-tered Treatment in Breast Cancer? Results of a Randomized Controlled Trial. Sleep 2014, 37, 1305–1314. [Google Scholar] [CrossRef]
- Savard, J.; Ivers, H.; Savard, M.-H.; Morin, C.M. Long-Term Effects of Two Formats of Cognitive Behavioral Therapy for Insomnia Comorbid with Breast Cancer. Sleep 2016, 39, 813–823. [Google Scholar] [CrossRef] [Green Version]
- Simeit, R.; Deck, R.; Conta-Marx, B. Sleep management training for cancer patients with insomnia support care. Support Care Cancer 2004, 12, 176–183. [Google Scholar] [CrossRef]
- Zhou, E.S.; Vrooman, L.M.; Manley, P.E.; Crabtree, V.M.; Recklitis, C.J. Adapted Delivery of Cognitive-Behavioral Treatment for Insomnia in Adolescent and Young Adult Cancer Survivors: A Pilot Study. Behav. Sleep Med. 2016, 15, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Campos-Rodriguez, F.; Martinez-Garcia, M.A.; Martinez, M.; Duran-Cantolla, J.; Peña, M.D.L.; Masdeu, M.J.; Gonzalez, M.; Campo, F.D.; Gallego, I.; Marin, J.M.; et al. Association between Obstructive Sleep Apnea and Cancer Incidence in a Large Multicenter Spanish Cohort. Am. J. Respir. Crit Care Med. 2013, 187, 99–105. [Google Scholar] [CrossRef] [Green Version]
- Cao, J.; Feng, J.; Li, L.; Chen, B. Obstructive sleep apnea promotes cancer development and progression: A concise review. Sleep Breath. 2015, 19, 453–457. [Google Scholar] [CrossRef]
- Dewan, N.A.; Nieto, F.J.; Somers, V.K. Intermittent hypoxemia and OSA: Implications for comorbidities. Chest 2015, 147, 266–274. [Google Scholar] [CrossRef] [Green Version]
- Faiz, S.A.; Balachandran, D.; Hessel, A.C.; Lei, X.; Beadle, B.M.; William, N.W.; Bashoura, L. Sleep-Related Breathing Disorders in Patients with Tumors in the Head and Neck Region. Oncologist 2014, 19, 1200–1206. [Google Scholar] [CrossRef] [Green Version]
- Gómez-Merino, E.; Arriero, J.M.; Chiner, E.; Signes-Costa, J.; Marco, J. Obstructive Sleep Apnea Syndrome as First Manifestation of Pharyngeal Non-Hodgkin’s Lym-phoma. Respiration 2003, 70, 107–109. [Google Scholar] [CrossRef]
- Kendzerska, T.; Leung, R.S.; Hawker, G.; Tomlinson, G.; Gershon, A.S. Obstructive sleep apnea and the prevalence and incidence of cancer. Can. Med. Assoc. J. 2014, 186, 985–992. [Google Scholar] [CrossRef] [Green Version]
- Marshall, N.S.; Wong, K.K.; Cullen, S.R.; Knuiman, M.W.; Grunstein, R.R. Sleep Apnea and 20-Year Follow-Up for All-Cause Mortality, Stroke, and Cancer Incidence and Mortal-ity in the Busselton Health Study Cohort. JCSM 2014, 10, 355–362. [Google Scholar] [CrossRef] [Green Version]
- Martínez-García, M.Á.; Campos-Rodriguez, F.; Farre, R. Sleep apnoea and cancer: Current insights and future perspectives. Eur. Respir. J. 2012, 40, 1315–1317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieto, F.J.; Peppard, P.E.; Young, T.; Finn, L.; Hla, K.M.; Farré, R. Sleep-disordered Breathing and Cancer Mortality Results from the Wisconsin Sleep Cohort Study. Am. J. Respir Crit Care Med. 2012, 186, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Partinen, M.; Jamieson, A.; Guilleminault, C. Long-term Outcome for Obstructive Sleep Apnea Syndrome Patients. Chest 1988, 94, 1200–1204. [Google Scholar] [CrossRef]
- Seidell, J. Waist circumference and waist/hip ratio in relation to all-cause mortality, cancer and sleep apnea. Eur. J. Clin. Nutr. 2009, 64, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Adams, C.; McKeon, A.; Silber, M.H.; Kumar, R. Narcolepsy, REM sleep behavior disorder, and supranuclear gaze palsy associated with Ma1 and Ma2 antibodies and tonsillar carcinoma. Arch. Neurol. 2011, 68, 521–524. [Google Scholar] [CrossRef] [Green Version]
- Landolfi, J.C.; Nadkarni, M. Paraneoplastic limbic encephalitis and possible narcolepsy in a patient with testicular cancer: Case study. Neuro Oncol. 2003, 5, 214–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tseng, C.-M.; Chen, Y.-T.; Tao, C.-W.; Ou, S.-M.; Hsiao, Y.-H.; Li, S.-Y.; Chen, T.-J.; Perng, D.-W.; Chou, K.-T. Adult narcoleptic patients have increased risk of cancer: A nationwide population-based study. Cancer Epidemiology 2015, 39, 793–797. [Google Scholar] [CrossRef]
- Saini, A.; Berruti, A.; Strambi, L.F.; Castronovo, V.; Rametti, E.; Giuliano, P.L.; Ramassotto, B.; Picci, R.L.; Negro, M.; Campagna, S.; et al. Restless Legs Syndrome as a Cause of Sleep Disturbances in Cancer Patients Receiving Chemotherapy. J. Pain Symptom Manag. 2013, 46, 56–64. [Google Scholar] [CrossRef]
- Jianhua, C.; Xiuqin, L.; Quancai, C.; Heyang, S.; Yan, H. Rapid Eye Movement Sleep Behavior Disorder in a Patient with Brainstem Lymphoma. Intern. Med. 2013, 52, 617–621. [Google Scholar] [CrossRef] [Green Version]
- Shinno, H.; Kamei, M.; Maegawa, T.; Satake, A.; Inami, Y.; Horiguchi, J.; Nakamura, Y. Three Patients with Cancer Who Developed Rapid-Eye-Movement Sleep Behavior Disorder. J. Pain Symptom Manag. 2010, 40, 449–452. [Google Scholar] [CrossRef] [PubMed]
- Acker, J.G.; Becker-Carus, C.; Büttner-Teleaga, A.; Cassel, W.; Danker-Hopfe, H.; Dück, A.; Frohn, C.; Hein, H.; Penzel, T.; Rodenbeck, A.; et al. The role of actigraphy in sleep medicine. Somnologie Schlafforschung Schlafmed. 2021, 25, 89–98. [Google Scholar] [CrossRef]
- Acker, J.; Golubnitschaja, O.; Büttner-Teleaga, A.; Richter, K. Wrist actigraphic approach in primary, secondary and tertiary care based on the principles of predictive, preventive and personalised (3P) medicine. EPMA J. 2021, 12, 349–363. [Google Scholar] [CrossRef]
- Translator Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Peter, L.; Reindl, R.; Zauter, S.; Hillemacher, T.; Richter, K. Effectiveness of an Online CBT-I Intervention and a Face-to-Face Treatment for Shift Work Sleep Disorder: A Comparison of Sleep Diary Data. Int. J. Environ. Res. Public Heal. 2019, 16, 3081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).