
Objective Measurement of 24-Hour Movement Behaviors in Preschool Children Using Wrist-Worn and Thigh-Worn Accelerometers

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol
2.2. Measurements
2.2.1. ActivPAL Accelerometer
2.2.2. Axivity Accelerometer
2.2.3. Short Questionnaire
2.3. Data Reduction and Analysis
2.3.1. ActivPAL Accelerometer
2.3.2. Axivity Accelerometer
2.4. Data Analysis
3. Results
3.1. Descriptive Characteristics of the Sample
3.2. Feasibility of Using the ActivPAL and Axivity Accelerometers in Preschool Children
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Guidelines on Physical Activity, Sedentary Behaviour and Sleep for Children under 5 Years of Age. Available online: https://apps.who.int/iris/handle/10665/311664 (accessed on 5 May 2020).
- Chaput, J.P.; Carson, V.; Gray, C.E.; Tremblay, M.S. Importance of all movement behaviors in a 24 h period for overall health. Int. J. Environ. Res. Public Health 2014, 11, 12575–12581. [Google Scholar] [CrossRef] [PubMed]
- Rollo, S.; Antsygina, O.; Tremblay, M.S. The whole day matters: Understanding 24-hour movement-guideline adherence and relationships with health indicators across the lifespan. J. Sport Health Sci. 2020, 9, 493–510. [Google Scholar] [CrossRef] [PubMed]
- De Craemer, M.; McGregor, D.; Androutsos, O.; Manios, Y.; Cardon, G. Compliance with 24-hour movement behaviour guidelines among belgian pre-school children: The ToyBox-Study. Int. J. Environ. Res. Public Health 2018, 15, 2171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, B.; Bernard, J.Y.; Padmapriya, N.; Yao, J.; Goh, C.; Tan, K.H.; Yap, F.; Chong, Y.S.; Shek, L.; Godfrey, K.M.; et al. Socio-demographic and maternal predictors of adherence to 24-hour movement guidelines in Singaporean children. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaput, J.P.; Colley, R.C.; Aubert, S.; Carson, V.; Janssen, I.; Roberts, K.C.; Tremblay, M.S. Proportion of preschool-aged children meeting the Canadian 24-Hour Movement Guidelines and associations with adiposity: Results from the Canadian Health Measures Survey. BMC Public Health 2017, 17, 829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cliff, D.P.; McNeill, J.; Vella, S.A.; Howard, S.J.; Santos, R.; Batterham, M.; Melhuish, E.; Okely, A.D.; de Rosnay, M. Adherence to 24-Hour Movement Guidelines for the Early Years and associations with social-cognitive development among Australian preschool children. BMC Public Health 2017, 17, 857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corder, K.; van Sluijs, E.M.; Wright, A.; Whincup, P.; Wareham, N.J.; Ekelund, U. Is it possible to assess free-living physical activity and energy expenditure in young people by self-report? Am. J. Clin. Nutr. 2009, 89, 862–870. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, U.; Tomkinson, G.; Armstrong, N. What proportion of youth are physically active? Measurement issues, levels and recent time trends. Br. J. Sports Med. 2011, 45, 859–865. [Google Scholar] [CrossRef] [PubMed]
- Pate, R.R.; O’Neill, J.R.; Mitchell, J. Measurement of physical activity in preschool children. Med. Sci. Sports Exerc. 2010, 42, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef] [PubMed]
- De Decker, E.; De Craemer, M.; Santos-Lozano, A.; Van Cauwenberghe, E.; De Bourdeaudhuij, I.; Cardon, G. Validity of the ActivPAL and the ActiGraph monitors in preschoolers. Med. Sci. Sports Exerc. 2013, 45, 2002–2011. [Google Scholar] [CrossRef] [PubMed]
- Prioreschi, A.; Brage, S.; Hesketh, K.D.; Hnatiuk, J.; Westgate, K.; Micklesfield, L.K. Describing objectively measured physical activity levels, patterns, and correlates in a cross sectional sample of infants and toddlers from South Africa. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, G.; Reilly, J.J.; McGowan, A.J.; Dall, P.M.; Granat, M.H.; Paton, J.Y. Validity, practical utility, and reliability of the activPAL in preschool children. Med. Sci. Sports Exerc. 2012, 44, 761–768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, Y.; Huang, W.Y.; Yu, J.J.; Sheridan, S.; Sit, C.H.; Wong, S.H. Compliance and Practical Utility of Continuous Wearing of activPAL in Adolescents. Pediatr. Exerc. Sci. 2019, 31, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Janssen, X.; Cliff, D.P.; Reilly, J.J.; Hinkley, T.; Jones, R.A.; Batterham, M.; Ekelund, U.; Brage, S.; Okely, A.D. Validation of activPAL defined sedentary time and breaks in sedentary time in 4- to 6-year-olds. Pediatr. Exerc. Sci. 2014, 26, 110–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willetts, M.; Hollowell, S.; Aslett, L.; Holmes, C.; Doherty, A. Statistical machine learning of sleep and physical activity phenotypes from sensor data in 96,220 UK Biobank participants. Sci. Rep. 2018, 8, 7961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doherty, A.R.; Hodges, S.E.; King, A.C.; Smeaton, A.F.; Berry, E.; Moulin, C.J.; Lindley, S.; Kelly, P.; Foster, C. Wearable cameras in health: The state of the art and future possibilities. Am. J. Prev. Med. 2013, 44, 320–323. [Google Scholar] [CrossRef] [PubMed]
- Cliff, D.P.; Reilly, J.J.; Okely, A.D. Methodological considerations in using accelerometers to assess habitual physical activity in children aged 0–5 years. J. Sci. Med. Sport 2009, 12, 557–567. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| ActivPAL Accelerometer | Axivity Accelerometer | Mean Difference | |||||
|---|---|---|---|---|---|---|---|
| % of the Day | Mean ± SD | Min–Max | % of the Day | Mean ± SD | Min–Max | ||
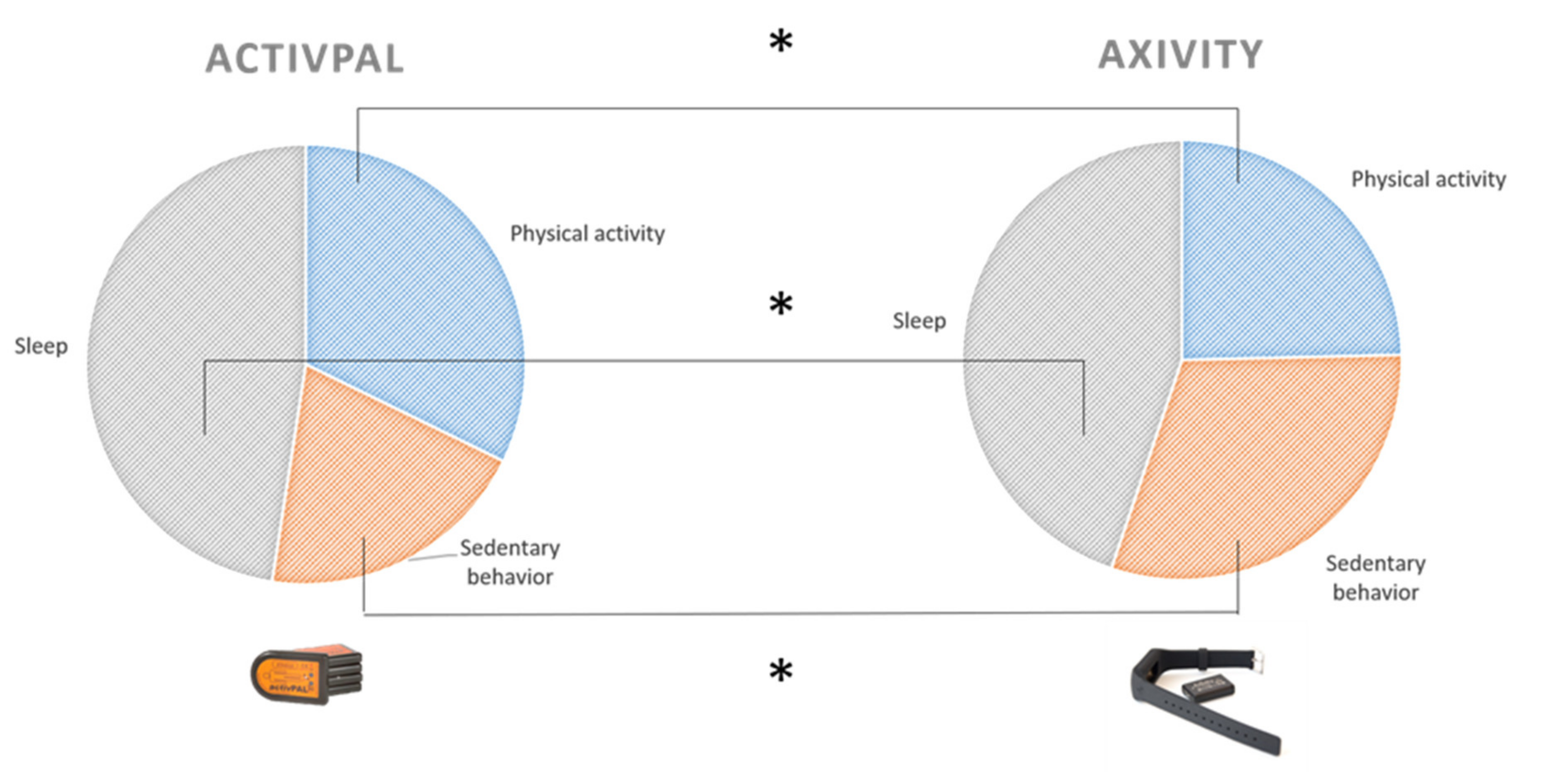
| Volume of physical activity/24 h | 32.3 | 464.44 ± 64.00 | 335–590 | 24.6 | 354.94 ± 57.46 | 235–454 | 109.50 * |
| Volume of sedentary behavior/24 h | 20.2 | 290.94 ± 55.05 | 162–358 | 30.6 | 440.50 ± 50.01 | 317–496 | −149.56 * |
| Volume of sleep/24 h | 47.5 | 684.63 ± 51.96 | 589–788 | 44.8 | 645.69 ± 46.78 | 543–735 | 38.94 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Craemer, M.; Decraene, M.; Willems, I.; Buysse, F.; Van Driessche, E.; Verbestel, V. Objective Measurement of 24-Hour Movement Behaviors in Preschool Children Using Wrist-Worn and Thigh-Worn Accelerometers. Int. J. Environ. Res. Public Health 2021, 18, 9482. https://doi.org/10.3390/ijerph18189482
De Craemer M, Decraene M, Willems I, Buysse F, Van Driessche E, Verbestel V. Objective Measurement of 24-Hour Movement Behaviors in Preschool Children Using Wrist-Worn and Thigh-Worn Accelerometers. International Journal of Environmental Research and Public Health. 2021; 18(18):9482. https://doi.org/10.3390/ijerph18189482
Chicago/Turabian StyleDe Craemer, Marieke, Marga Decraene, Iris Willems, Feija Buysse, Ellen Van Driessche, and Vera Verbestel. 2021. "Objective Measurement of 24-Hour Movement Behaviors in Preschool Children Using Wrist-Worn and Thigh-Worn Accelerometers" International Journal of Environmental Research and Public Health 18, no. 18: 9482. https://doi.org/10.3390/ijerph18189482
APA StyleDe Craemer, M., Decraene, M., Willems, I., Buysse, F., Van Driessche, E., & Verbestel, V. (2021). Objective Measurement of 24-Hour Movement Behaviors in Preschool Children Using Wrist-Worn and Thigh-Worn Accelerometers. International Journal of Environmental Research and Public Health, 18(18), 9482. https://doi.org/10.3390/ijerph18189482