1. Introduction
Caffeine belongs to the methylxanthines group and it is the most consumed psychostimulant (alkaloid) worldwide because it is present in coffee, which is the second most consumed liquid in the world, after water [
1].
Coffee is the main source of caffeine in adults. This drink also contains phenolic acids, among which acylquinic acid and hydroxycinnamic acid stand out. These acids have been related to the decrease in the incidence of cardiovascular diseases, metabolic syndrome, and cancer [
2]. Due to its potential pharmaceutical activity, coffee can be considered as a nutraceutical [
3]. On the other hand, in studies conducted in adults, it has been observed that caffeine increases mental and physical performance [
4].
Despite the beneficial effects of coffee in the adult population, its involvement in vulnerable groups as children remains unclear [
5]. Half of the caffeine intake in children comes from cola drinks [
6], and the energy drink consumption in this group has increased by 6% in the past decade [
7,
8,
9].
Caffeine intake in children depends on the social context and culture [
10]. For instance, supermarkets and restaurants, especially fast-food ones, are the places where caffeinated foods are the most easily found in Europe and the United States [
11]. In Mexico, this intake also occurs in many socially significant scenarios, such as children’s parties, family gatherings, and school recess [
12].
Caffeine consumption in the youth is a controversial topic. On one hand, the literature has shown evidence of alterations in children’s growth and development, such as iron absorption deficiencies and weight loss [
13,
14,
15]. On the other hand, the physical, mental, attention-performance, and neuroprotective effects of caffeine have been demonstrated [
13,
15,
16].
Seifert et al. [
16] highlighted the cognitive and attention improvement effect in children when the alkaloid was supplied in small doses (under 2.5 mg/kg). Still, they concluded that caffeine intake in minors could lead to severe health consequences, especially when it was ingested together with other substances like taurine, as found in energy drinks.
Indeed, the physiological alterations produced by this substance depend on the amount ingested. Tieges et al. [
17] and Ruxton et al. [
18], described the amounts considered low (1 mg.kg.d), medium (3 mg.kg.d), and high (5 mg.kg.d) in children because these amounts differ in comparison with adults. The physiological effects of caffeine have been observed from moderate to high doses while no reports of organic changes were found at low doses.
Because the effects of caffeine are widely described in adults but not in children, a thorough review of the literature is necessary. Likewise, it is considered necessary to know if there are different effects produced depending on the dose and the source of intake.
For that reason, the aim of this systematic review of the literature was to investigate the main effects of caffeine in children. The benefits that could be obtained from this knowledge include providing accurate dietary guidance, considering caffeine as a risk factor to children’s health or a therapeutic agent in paedopsychiatric alterations, such as ADHD. By carrying out this systematic review, we aim to show the changes that caffeine produces in children’s metabolism, providing a physical, cognitive, and psychological panorama. This insight could favor the creation of strategies to limit or regulate the consumption of caffeine, depending on its negative or positive effects.
2. Materials and Methods
This work was based on the PRISMA method (
Figure 1) for systematic literature reviews, adapted from Urrútia and Bonfil [
19]. The checklist developed by González et al. [
20] was also followed.
2.1. Elegibility Criteria
For this review of the literature, the following concepts were proposed to obtain information:
Caffeine is an alkaloid consumed in large amounts worldwide.
It leads to physiological changes in consumers.
These changes can be beneficial or detrimental to health.
The changes produced are dose dependent.
Cross-sectional and longitudinal studies dealing with any aspect related to the physiological changes produced by caffeine were included. Only works conducted on humans and published in journals included in the Journal Citation Report (JCR) were considered.
2.2. Sources of Information
The search for information was conducted electronically in the digital repository of the Autonomous University of the State of Hidalgo, specifically in the digital collections.
Four search engines were found in this digital library: EBSCO, ScienceDirect, PubMed, and Clarivate Analytics. These search engines were selected due to their relevance since the publications in them possess a high impact factor. The search for information started on July 2nd, 2018 and concluded on December 20th in the same year.
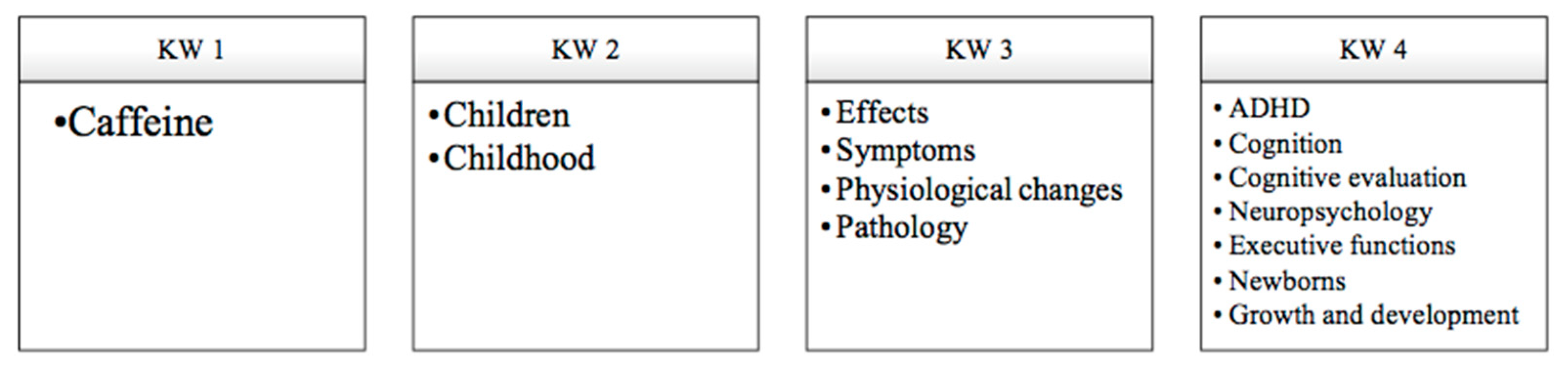
2.3. Search for Information
The search terms, combination, and acronyms are described in
Figure 2.
The lower limit of the search for information was year 1975 while year 2018 was the upper one. It was decided to start the search from articles published in 1975 since that was the year in which the first article on the effects of caffeine in children (with minimal brain dysfunction) was found. After a first look at the information, the search period was limited to 2008–2018, considering the articles published after 2008 were of higher relevance to this review.
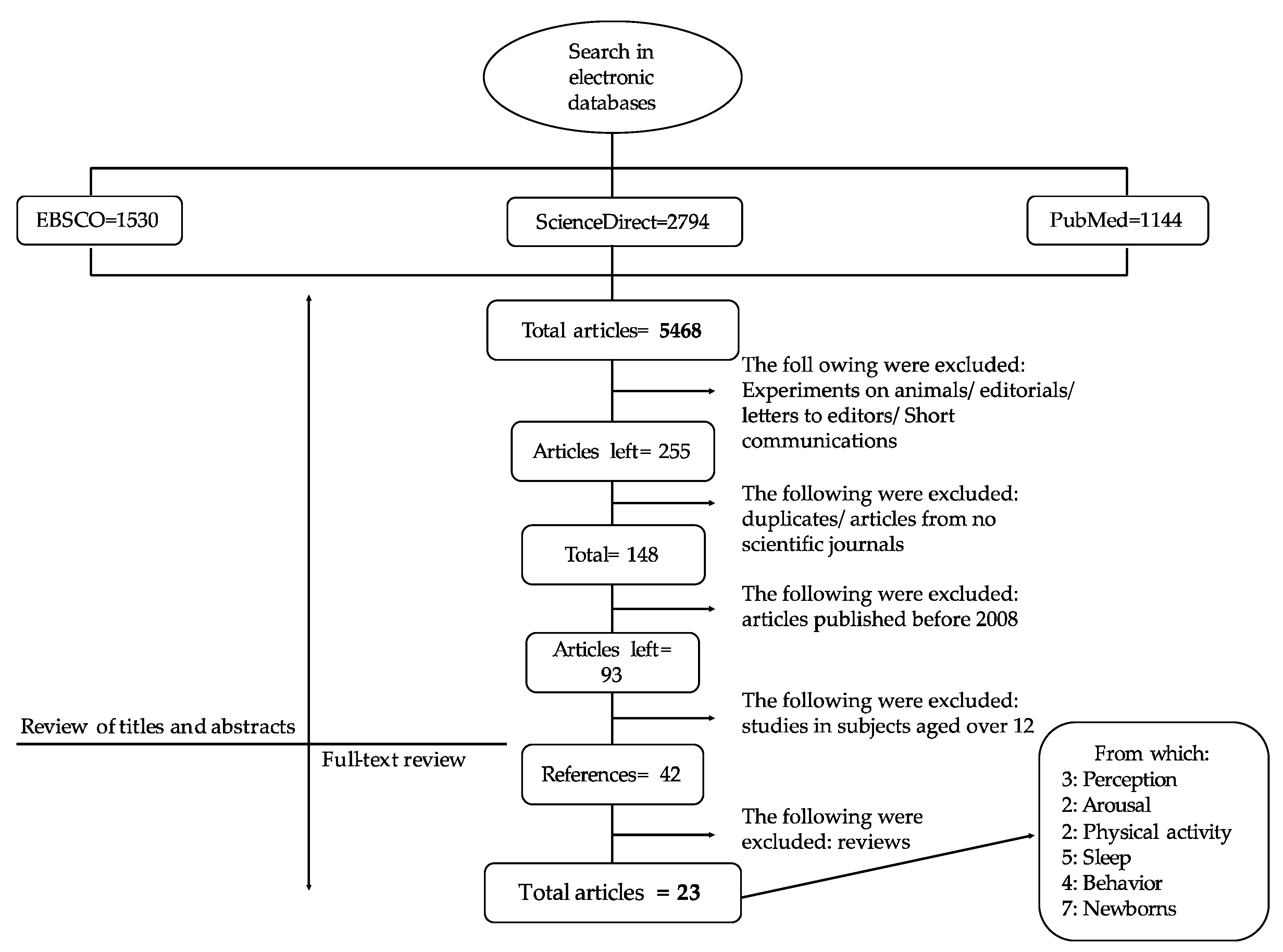
A total number of 5,468 articles were found: 1530 in EBSCO; 1144 in PubMed; 1929 in ScienceDirect, and 865 in Clarivate Analytics, as shown in
Figure 3.
Afterwards, experiments in animals, editorials, letters to editors, and brief communications were excluded, and 255 articles were retained. After a manual cross-check, duplicated reports were eliminated. Only articles published in scientific journals were included and 148 articles were obtained. From them, 93 articles were published from 2008 to date. Only 42 studies matched the inclusion criteria. They were subclassified according to the effect produced by caffeine as follows:
Sixteen articles studied the effect of caffeine in children. Three articles were based on the concept of caffeine by consumers, two articles on the general activation state (arousal), two articles on physical activity, five articles on sleep cycle, and four articles on affective states.
Seven articles were based on the secondary effects produced by caffeine in the treatment of respiratory disorders in newborns.
Eighteen were review studies.
After a final selection, review articles were discarded and thus only the results of 24 articles were considered.
2.4. Study Selection
The inclusion criteria which led to the selection of the 24 papers from among the initially found articles were established according to the Participants, Interventions, Comparisons, Outcomes, and Studies (PICOS) design format adapted from Robinson et al. [
21]:
Participants: Children up to age 17 (upper limit) were considered. However, those studies with children under 12 years were preferred because there is evidence that sensitivity to caffeine is modified in adolescence and physiological, cognitive, and behavioral responses are different from those shown by children [
22]. Both genders were considered, with or without pathologies, exhibiting a secondary physiological change after caffeine intake or administration at different doses.
Interventions: Primary works on caffeine intake or administration and their effects on health were included. The type of survey used to determine the perception of caffeine, was also included.
Comparisons and Outcomes: Studies using reliable evaluation instruments, measurement of effects of caffeine by image studies or physical tests sensitive to measurement of the alkaloid were included.
Study design: All types of study design were included, with the exception of reviews and meta-analyses.
The exclusion criteria were:
Studies not providing fundamental data on the effect of caffeine in children’s health.
Studies in which caffeine was the result of a metabolic process and was not ingested or administered.
Studies published before 2008.
2.5. Data Collection
An extraction database was designed considering the eligibility criteria of the articles. All the proposed methods in the research articles were analyzed and the database was completed with results, discussion, and conclusion analysis of each of the selected works. Once obtained, the information was synthesized, compared, and contrasted qualitatively between articles.
2.6. Result Synthesis
The experimental studies analyzed were catalogued in the topics on caffeine presented in
Table 1. The years of publication are also shown.
4. Discussion
In the literature reviewed for this study, some methodological problems were evidenced:
The position (if there were positive or negative effects) of the studies on caffeine consumption in minors was unclear.
The analyzed studies do not compare positive and negative effects of caffeine.
The studies do not consider the different metabolic processes in children and adults.
There were few longitudinal studies, so the long-term effect of caffeine could not be known.
The age limits between the studies were poorly specified and most cases did not differentiate children from adolescents.
Few studies analyzed considered the different doses of caffeine, so the comparison of effects according to dose could not be performed.
The present review tried to avoid the previous misunderstandings and methodological complications. The separation of references in two groups allowed for a better analysis of the information. This review emphasizes that the alkaloid is metabolized differently in children and adults and some physiological processes considered beneficial to adults may not be desirable in children. Then, a more accurate orientation towards the effects of caffeine in children’s metabolism is possible.
Furthermore, the results of this research showed that consumers possess little to no knowledge on the effects produced by caffeine in the organism, although they assume there is a negative effect on health. In all cases, the perception of caffeine was clearly negative and independent of the intake recommendations. Evidently, the population knows the possible health risks these products possess, although this perception does not agree with current advertisements.
If the classification proposed by Tieges et al. [
17] and Ruxton et al. [
18] is exclusively taken into account, children with a caffeine intake of 1 mg.kg.day would have a low intake, 3 mg.kg.day a medium intake and 5 mg.kg.day a high intake. Although no correlation was found between doses and effects in the literature analyzed, evidence found in this research shows that the deleterious effects of caffeine may occur, above all, at moderate and high doses. However, the authors of this review consider that the effects on the sleep cycle that low doses might cause should not be underestimated.
Understanding that caffeine in moderate and high doses is deleterious to healthy children can be useful to provide a real nutritional guidance to the youth. Additionally, it could help in the creation of advertising strategies in order to not compromise children’s health. For example, in nutrition guidelines it could be proposed that caffeine is “no consumption” or “moderate consumption” for children.
From the systematic review of the current literature on the physiological changes produced by caffeine in children, the evidence indicates that caffeine could be recommended for the youth with especial conditions (ADHD and apnea of prematurity) but not suggested for healthy children, especially in moderate and high doses that reportedly cause physiological alterations.
Considering the published studies, two main groups were established according to the effects (positive or negative) of caffeine consumption in children.
The positive effects of caffeine found in children’s metabolism were:
Improvement of energy distribution in the central nervous system. Regarding this factor, the studies analyzed [
26,
27], did not take into account the weight of the children, so they did not consider the consumption level, whether high, medium or low. Besides, the studies did not include other populations or physiological conditions; even the symptoms that were reduced as a consequence of a better energy management in the brain were not specified. That is the reason why further investigation considering the consumption level is considered necessary.
Improvement of physical performance. Caffeine could improve the physical performance of children in a dose-dependent manner. Nevertheless, different doses are difficult to control, and it must be considered that children are more sensitive to the alkaloid, although the cause is unknown.
Improvement of the respiratory function. These effects were especially positive when there is an alteration in the brain or respiratory dynamic, as ADHD or apnea of prematurity. In those cases, caffeine could be a first-line therapeutic agent or an adjuvant of the medical treatment. Apnea of prematurity is a medical condition frequently present in newborns under 32 weeks of gestation. The treatment of respiratory disorders using caffeine has been reported to be effective for the cognitive performance in the short and long term.
Furthermore, the negative effects of the alkaloid in moderate and high doses were (1) alterations in the sleep cycle and (2) the affective states. In the first case, children’s metabolism is increased at night. Their sleep cycle demands stability and consistency as well as more hours in bed than adults [
39]. As observed, any alteration in the sleep cycle indirectly compromises the adequate mental and physical development of children. The ingestion of caffeine is one of the leading factors interfering with these processes. It would be important to know if there are variations depending on different doses.
Alterations of affective states as anxiety and depression produced by caffeine are directly proportional to the amount ingested. Since children’s body mass is lower than that of adults, they consume more caffeine but in fewer products [
43]. This effect seems to be more harmful in the case of affective states. Children’s emotional health seems to be one of the aspects affected by caffeine intake and its dosage influence. Therefore, this information may suggest that children are more sensitive to the effects of the alkaloid, although the cause remains unclear.
Finally, caffeine affects the way in which energy is distributed in the central nervous system. Additionally, metabolic effects, such as changes in heart rate, blood pressure, and the ventilatory function should also be taken into account. These effects occur mostly among young people, probably as a result of the dosage problem that has been discussed throughout this manuscript. Therefore, this factor should be included in a paedopsychiatric and medical evaluation.
However, in special cases as those of children who suffer pathologies that compromise the brain dynamic and respiratory function, caffeine could be considered as an adjuvant of the treatment. Still, the treatment with caffeine could compromise the children’s growth and development if the symptoms persist. Therefore, it can be said that caffeine is innocuous only under special conditions
5. Conclusions
The effects of caffeine in children can be divided into positive and negative. The first ones are found at cognitive level (elevated short-term arousal and increased motor activity, perception, and intelligence in the long term) and improved physical performance both in aerobic and anaerobic conditions. On the other hand, the negative effects include changes in the sleep cycle, which could indirectly alter the weight and growth of children, and greater sensitivity to the alkaloid at an emotional level (anxiety and depression).
Limits, Advantages and Potential Applications
Due to this systematic review provides accessible evidence about the effects that caffeine produces in the children’s organism, it could cater knowledge that could guide consumption behavior in this particular population.
Likewise, in this review it was evidenced that the general population considered that the intake of this alkaloid could produce negative effects on the health of school children. Therefore, this material could be useful to provide scientific evidence on the effects it produces and reinforce the general knowledge that the population has about caffeine.
The investigations analyzed in this systematic review of the literature did not take into account the different consumption doses of their study population. Thus, it was difficult to establish a correlation between the consumption doses and the observed effects. Future research is considered necessary to correlate doses with effects.
Despite the fact that this review emphasizes that caffeine is metabolized differently in children and adults, more research is considered necessary on the metabolic effects that occur in children compared to adults, for example in the change of enzyme markers.
In the same order of ideas, further investigation of the effects of caffeine in the field of paidopsychiatry is considered necessary, since in this review, a lack of consensus was observed on whether the effects it produces in these pathologies could be considered positive or negative.

 ,
, 





{kind=link}
{kind=link}
{kind=link}