Cross-Lagged Associations between Depressive Symptoms and Response Style in Adolescents

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measures
2.3.1. Depressive Symptoms
2.3.2. Response Style.
2.3.3. Control Variables
2.4. Statistical Analyses
2.5. Drop Out and Missing Vvalues
3. Results
3.1. Descriptives
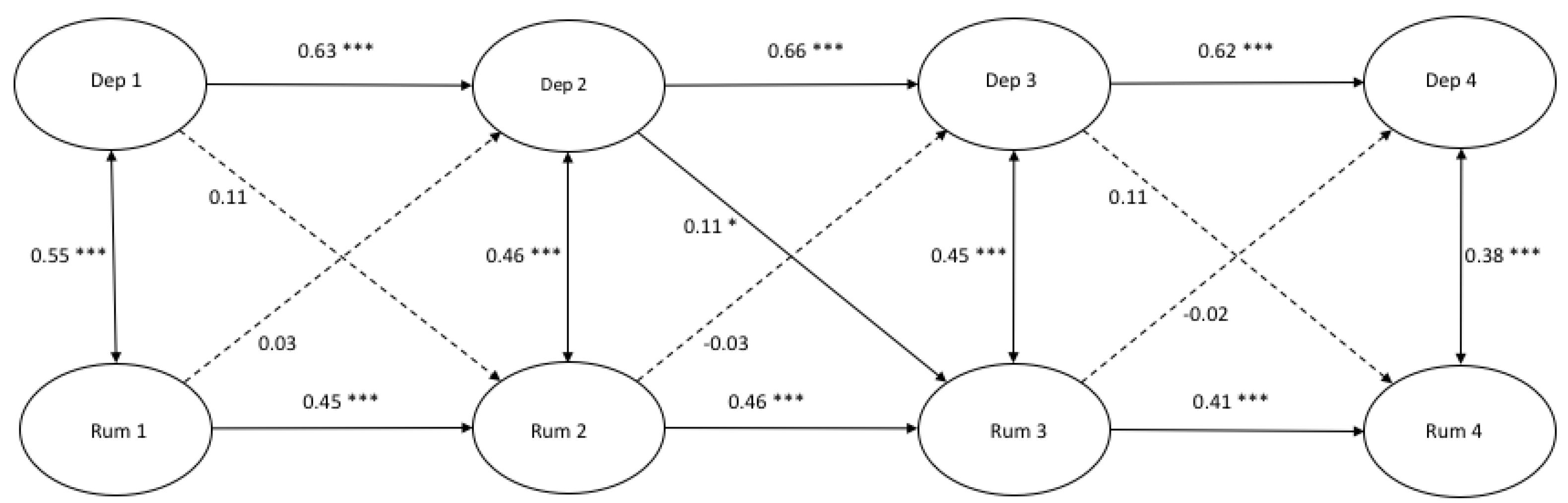
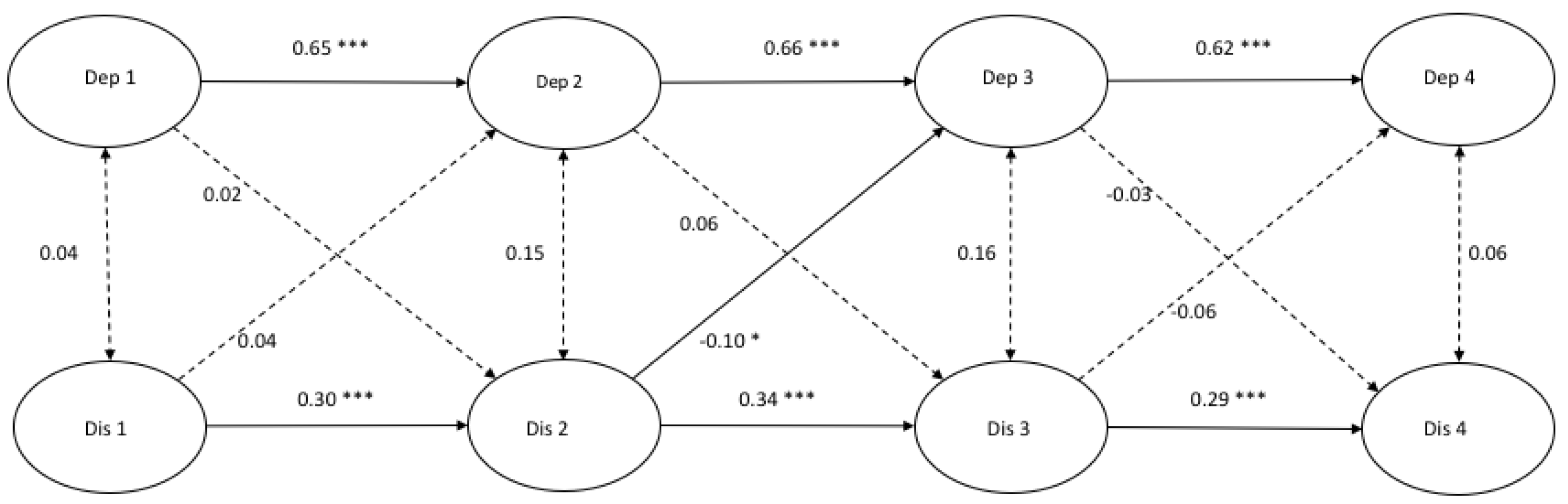
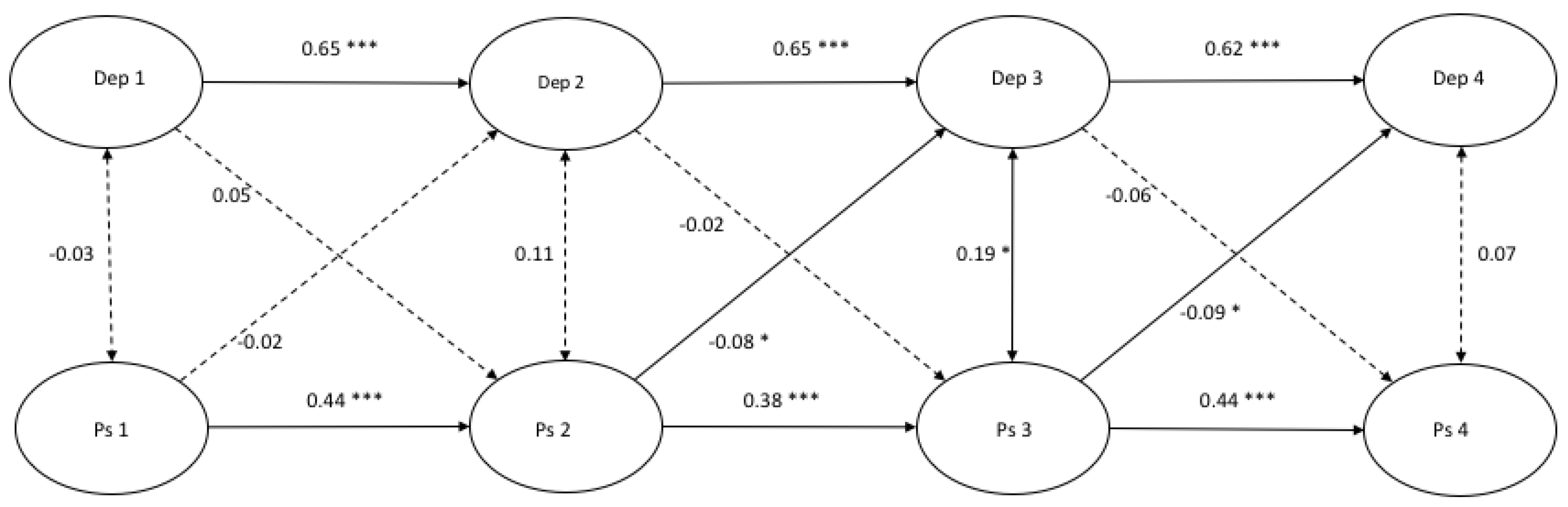
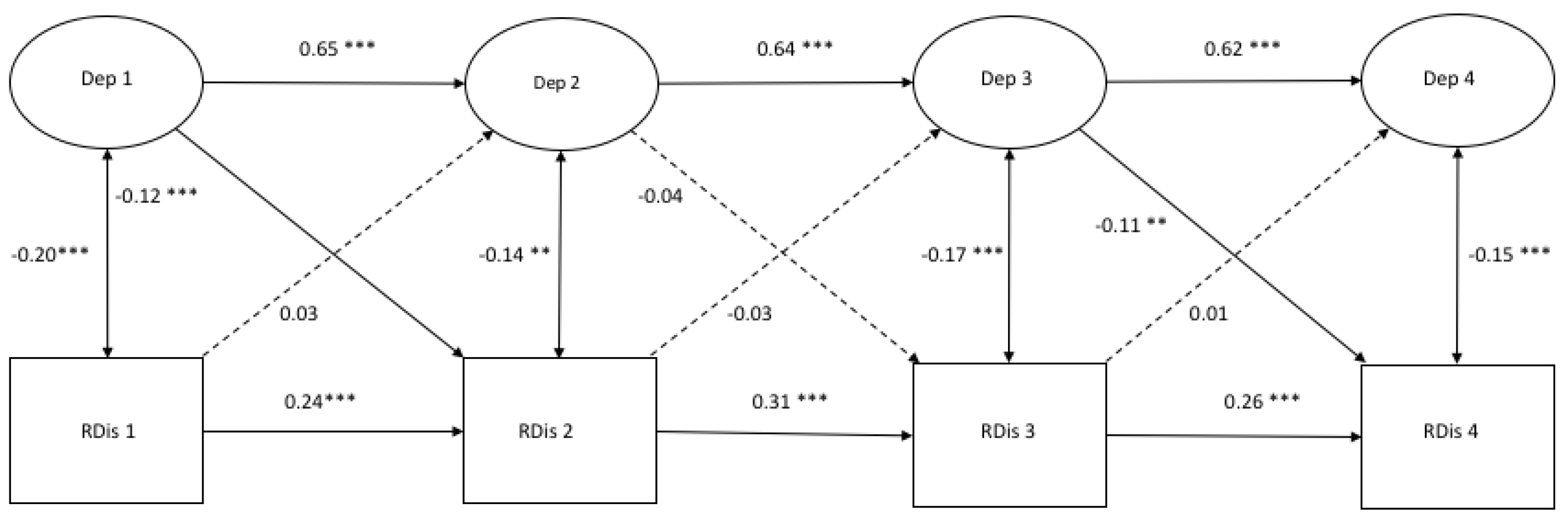
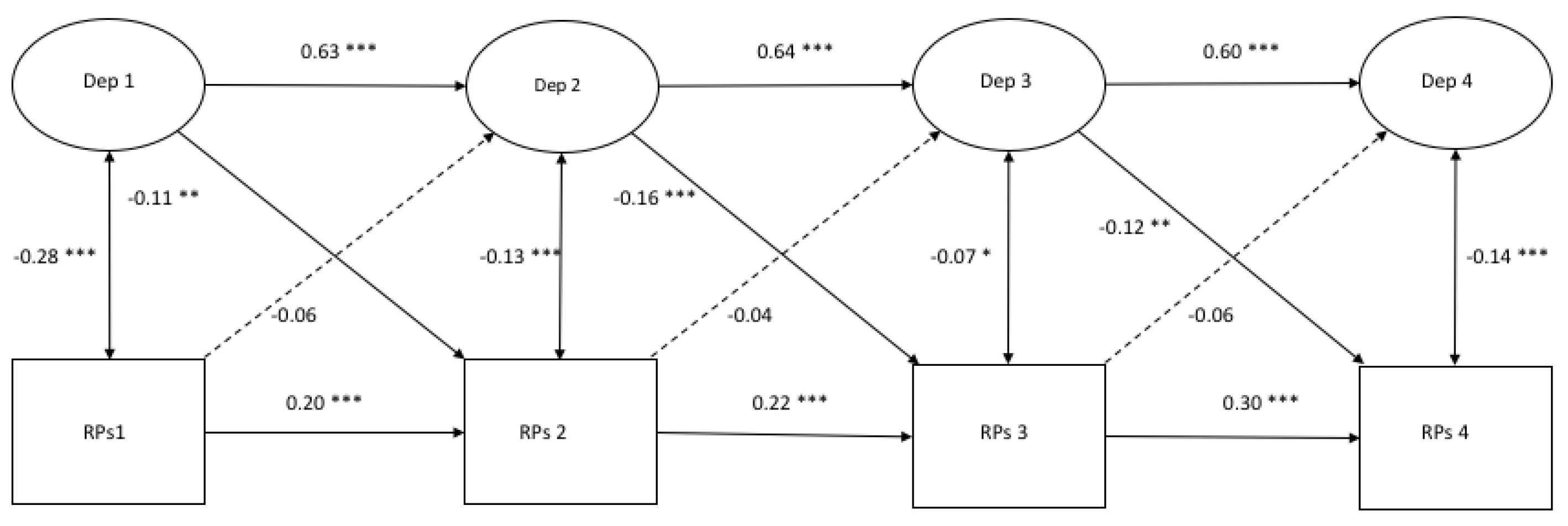
3.2. Cross-Lagged Models of Depressive Symptoms with Response Styles (Traditional Scores)
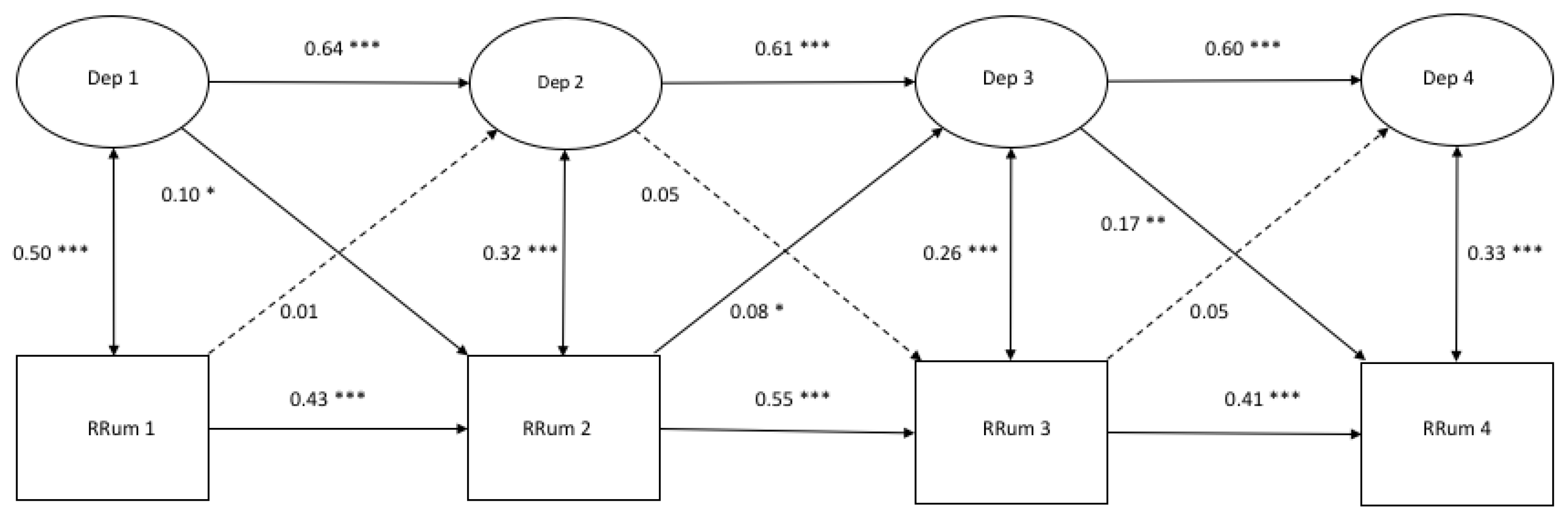
3.3. Cross-Lagged Models of Depressive sSymptoms with Response Styles (Ratio Scores)
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Depression | Rumination | Distraction | Problem Solving | |||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T1 | T2 | T3 | T4 | T1 | T2 | T3 | T4 | T1 | T2 | T3 | T4 | T1 | T2 | T3 | T4 | |||||||||||||||||
| β | p | β | p | β | p | β | p | β | p | β | p | β | p | β | p | β | p | β | p | β | p | β | p | β | p | β | p | β | p | β | p | |
| Gender | 0.06 | 0.03 | −0.02 | 0.59 | 0.03 | 0.40 | 0.00 | 0.88 | 0.23 | 0.00 | 0.10 | 0.00 | 0.12 | 0.00 | 0.15 | 0.00 | 0.13 | 0.00 | 0.14 | 0.00 | 0.15 | 0.00 | 0.15 | 0.00 | 0.26 | 0.00 | 0.04 | 0.27 | 0.18 | 0.00 | 0.13 | 0.00 |
| School L | 0.05 | 0.15 | 0.03 | 0.48 | 0.07 | 0.02 | 0.00 | 0.98 | 0.06 | 0.12 | 0.08 | 0.00 | 0.06 | 0.10 | −0.01 | 0.80 | −0.06 | 0.28 | 0.08 | 0.06 | 0.03 | 0.41 | 0.02 | 0.68 | 0.06 | 0.24 | 0.06 | 0.09 | 0.07 | 0.13 | −0.00 | 0.94 |
| Condition | −0.02 | 0.60 | −0.03 | 0.48 | 0.06 | 0.04 | −0.08 | 0.02 | 0.00 | 0.99 | −0.03 | 0.36 | 0.04 | 0.21 | −0.00 | 0.94 | −0.03 | 0.61 | −0.10 | 0.01 | 0.04 | 0.25 | 0.08 | 0.03 | −0.06 | 0.21 | −0.03 | 0.33 | 0.04 | 0.30 | 0.01 | 0.75 |
| Age | 0.11 | 0.01 | 0.00 | 0.97 | −0.07 | 0.02 | 0.05 | 0.20 | 0.04 | 0.31 | −0.02 | 0.55 | 0.01 | 0.79 | 0.06 | 0.04 | −0.11 | 0.01 | −0.05 | 0.25 | −0.00 | 0.93 | 0.03 | 0.50 | −0.01 | 0.89 | −0.06 | 0.08 | 0.05 | 0.19 | 0.00 | 0.99 |
| Parental P | −0.13 | 0.00 | 0.00 | 0.87 | −0.03 | 0.28 | −0.05 | 0.23 | −0.13 | 0.00 | 0.01 | 0.80 | −0.05 | 0.10 | −0.01 | 0.83 | −0.09 | 0.02 | 0.04 | 0.23 | 0.03 | 0.37 | 0.04 | 0.33 | −0.04 | 0.27 | −0.02 | 0.61 | 0.02 | 0.48 | 0.00 | 0.96 |
| Ethnic B | −0.05 | 0.10 | 0.00 | 0.97 | 0.03 | 0.27 | 0.03 | 0.35 | −0.01 | 0.83 | −0.01 | 0.62 | −0.05 | 0.15 | 0.06 | 0.07 | −0.00 | 0.95 | −0.07 | 0.06 | −0.05 | 0.28 | −0.02 | 0.68 | 0.06 | 0.12 | −0.02 | 0.63 | −0.01 | 0.77 | 0.03 | 0.50 |
| Depression | Rumination | Distraction | Problem Solving | |||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T1 | T2 | T3 | T4 | T1 | T2 | T3 | T4 | T1 | T2 | T3 | T4 | T1 | T2 | T3 | T4 | |||||||||||||||||
| β | p | β | p | β | p | β | p | β | p | β | p | β | p | β | p | β | p | β | p | β | p | β | p | β | p | β | p | β | p | β | p | |
| Gender | 0.07 | 0.03 | −0.02 | 0.66 | 0.02 | 0.61 | 0.00 | 0.99 | 0.06 | 0.02 | 0.07 | 0.00 | 0.00 | 0.93 | 0.05 | 0.09 | −0.18 | 0.00 | 0.00 | 0.99 | −0.06 | 0.06 | −0.06 | 0.12 | 0.15 | 0.00 | −0.01 | 0.81 | 0.10 | 0.00 | 0.05 | 0.09 |
| School Level | 0.05 | 0.15 | 0.03 | 0.48 | 0.06 | 0.03 | −0.00 | 0.96 | 0.06 | 0.04 | 0.04 | 0.14 | 0.03 | 0.26 | −0.01 | 0.80 | −0.09 | 0.02 | −0.01 | 0.88 | −0.04 | 0.22 | 0.01 | 0.68 | 0.07 | 0.04 | −0.01 | 0.74 | 0.02 | 0.66 | 0.01 | 0.67 |
| Condition | −0.02 | 0.61 | −0.03 | 0.49 | 0.06 | 0.06 | −0.08 | 0.02 | 0.03 | 0.31 | 0.02 | 0.38 | −0.01 | 0.74 | −0.05 | 0.11 | −0.00 | 0.91 | −0.06 | 0.04 | −0.01 | 0.66 | 0.08 | 0.01 | −0.03 | 0.29 | 0.02 | 0.47 | 0.00 | 0.93 | −0.02 | 39 |
| Age | 0.11 | 0.00 | 0.00 | 0.95 | −0.07 | 0.02 | 0.05 | 0.21 | 0.05 | 0.11 | 0.02 | 0.55 | −0.02 | 0.38 | 0.03 | 0.27 | −0.11 | 0.00 | −0.01 | 0.69 | −0.06 | 0.09 | −0.01 | 0.65 | 0.05 | 0.08 | −0.01 | 0.76 | 0.08 | 0.02 | −0.03 | 0.28 |
| Parental P | −0.13 | 0.00 | 0.00 | 0.89 | −0.03 | 0.35 | −0.05 | 0.25 | −0.08 | 0.03 | −0.00 | 0.93 | −0.09 | 0.03 | −0.05 | 0.32 | 0.01 | 0.82 | 0.03 | 0.24 | 0.04 | 0.22 | 0.04 | 0.23 | 0.07 | 0.01 | −0.04 | 0.38 | 0.04 | 0.19 | −0.01 | 0.75 |
| Ethnic B | −0.05 | 0.11 | 0.00 | 0.94 | 0.03 | 0.25 | 0.03 | 0.32 | −0.03 | 0.35 | 0.01 | 0.69 | −0.01 | 0.66 | 0.05 | 0.15 | −0.02 | 0.57 | −0.06 | 0.06 | −0.02 | 0.61 | −0.08 | 0.01 | 0.06 | 0.04 | 0.04 | 0.24 | 0.03 | 0.40 | 0.02 | 0.68 |
References
- Kessler, R.C.; Petukhova, M.; Sampson, N.A.; Zaslavsky, A.M.; Wittchen, H.U. Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. Int J. Methods Psychiatr Res. 2012, 21, 169–184. [Google Scholar] [CrossRef] [PubMed]
- Monshouwer, K.; Smit, F.; Ruiter, M.; Ormel, H.; Verhulst, F.; Vollebergh, W.; Oldehinkel, T. Identifying target groups for the prevention of depression in early adolescence: The TRAILS study. J. Affect. Disord 2012, 138, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Jane Costello, E.; Erkanli, A.; Angold, A. Is there an epidemic of child or adolescent depression? J. Child. Psychol. Psychiatry 2006, 47, 1263–1271. [Google Scholar] [CrossRef] [PubMed]
- Lewinsohn, P.M.; Hops, H.; Roberts, R.E.; Seeley, J.R.; Andrews, J.A. Adolescent psychopathology: I. Prevalence and incidence of depression and other DSM-III-R disorders in high school students. J. Abnorm. Psychol. 1993, 102, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Lewinsohn, P.M.; Rohde, P.; Seeley, J.R. Major depressive disorder in older adolescents: Prevalence, risk factors, and clinical implications. Clin. Psychol. Rev. 1998, 18, 765–794. [Google Scholar] [CrossRef]
- Hankin, B.L.; Abramson, L.Y.; Moffitt, T.E.; Silva, P.A.; McGee, R.; Angell, K.E. Development of depression from preadolescence to young adulthood: Emerging gender differences in a 10-year longitudinal study. J. Abnorm. Psychol. 1998, 107, 128–140. [Google Scholar] [CrossRef]
- Fergusson, D.M.; Horwood, L.J. The Christchurch Health and Development Study: Review of findings on child and adolescent mental health. Aust N Z J. Psychiatry 2001, 35, 287–296. [Google Scholar] [CrossRef]
- Kessler, R.C.; Demler, O.; Frank, R.G.; Olfson, M.; Pincus, H.A.; Walters, E.E.; Wang, P.; Wells, K.B.; Zaslavsky, A.M. Prevalence and treatment of mental disorders, 1990 to 2003. N. Engl. J. Med. 2005, 352, 2515–2523. [Google Scholar] [CrossRef]
- Collins, W.A. More than myth: The developmental significance of romantic relationships during adolescence. J. Res. Adolesc. 2003, 13, 1–24. [Google Scholar] [CrossRef]
- Steinberg, L. Cognitive and affective development in adolescence. Trends Cogn. Sci. 2005, 9, 69–74. [Google Scholar] [CrossRef]
- Angold, A.; Costello, E.J.; Worthman, C.M. Puberty and depression: The roles of age, pubertal status and pubertal timing. Psychol. Med. 1998, 28, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Babore, A.; Trumello, C.; Candelori, C.; Paciello, M.; Cerniglia, L. Depressive Symptoms, Self-Esteem and Perceived Parent–Child Relationship in Early Adolescence. Front. Psychol. 2016, 7. [Google Scholar] [CrossRef] [PubMed]
- Rawana, J.S.; Morgan, A.S. Trajectories of depressive symptoms from adolescence to young adulthood: The role of self-esteem and body-related predictors. J. Youth Adolesc. 2014, 43, 597–611. [Google Scholar] [CrossRef] [PubMed]
- Beck, A. Depression: Causes and Treatment; University of Pennsylvania Press: Philadelphia, PA, USA, 1967. [Google Scholar]
- Metalsky, G.I.; Joiner, T.E.; Hardin, T.S.; Abramson, L.Y. Depressive reactions to failure in a naturalistic setting: A test of the hopelessness and self-esteem theories of depression. J. Abnorm. Psychol. 1993, 102, 101. [Google Scholar] [CrossRef] [PubMed]
- Balazs, J.; Miklosi, M.; Kereszteny, A.; Hoven, C.W.; Carli, V.; Wasserman, C.; Apter, A.; Bobes, J.; Brunner, R.; Cosman, D.; et al. Adolescent subthreshold-depression and anxiety: Psychopathology, functional impairment and increased suicide risk. J. Child. Psychol Psychiatry 2013, 54, 670–677. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, J.M. Adolescent depression: Diagnosis, treatment, and educational attainment. Health Econ. 2008, 17, 1215–1235. [Google Scholar] [CrossRef] [PubMed]
- Verboom, C.E.; Sijtsema, J.J.; Verhulst, F.C.; Penninx, B.W.; Ormel, J. Longitudinal associations between depressive problems, academic performance, and social functioning in adolescent boys and girls. Dev. Psychol. 2014, 50, 247–257. [Google Scholar] [CrossRef]
- Fried, L.E.; Williams, S.; Cabral, H.; Hacker, K. Differences in risk factors for suicide attempts among 9th and 11th grade youth: A longitudinal perspective. J. Sch. Nurs. 2013, 29, 113–122. [Google Scholar] [CrossRef]
- Fergusson, D.M.; Woodward, L.J. Mental health, educational, and social role outcomes of adolescents with depression. Arch. Gen. Psychiatry 2002, 59, 225–231. [Google Scholar] [CrossRef]
- Birmaher, B.; Ryan, N.D.; Williamson, D.E.; Brent, D.A.; Kaufman, J.; Dahl, R.E.; Perel, J.; Nelson, B. Childhood and adolescent depression: A review of the past 10 years. Part I. J. Am. Acad Child. Adolesc Psychiatry 1996, 35, 1427–1439. [Google Scholar] [CrossRef]
- Abravanel, B.T.; Sinha, R. Emotion dysregulation mediates the relationship between lifetime cumulative adversity and depressive symptomatology. J. Psychiatr Res. 2015, 61, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Campbell-Sills, L.; Barlow, D.H. Incorporating emotion regulation into conceptualizations and treatments of anxiety and mood disorders. In Handbook of Emotion Regulation; The Guilford Press: Loden, NY, USA, 2007. [Google Scholar]
- Mennin, D.S.; Holaway, R.M.; Fresco, D.M.; Moore, M.T.; Heimberg, R.G. Delineating components of emotion and its dysregulation in anxiety and mood psychopathology. Behav. Ther. 2007, 38, 284–302. [Google Scholar] [CrossRef] [PubMed]
- Nolen-Hoeksema, S. Responses to depression and their effects on the duration of depressive episodes. J. Abnorm. Psychol. 1991, 100, 569–582. [Google Scholar] [CrossRef] [PubMed]
- Nolen-Hoeksema, S.; Harrell, Z.A. Rumination, depression, and alcohol use: Tests of gender differences. J. Cogn. Psychother. 2002, 16, 391–404. [Google Scholar] [CrossRef]
- Just, N.; Alloy, L.B. The response styles theory of depression: Tests and an extension of the theory. J. Abnorm. Psychol. 1997, 106, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Sarin, S.; Abela, J.; Auerbach, R. The response styles theory of depression: A test of specificity and causal mediation. Cogn. Emot. 2005, 19, 751–761. [Google Scholar] [CrossRef]
- Abela, J.R.; Aydin, C.M.; Auerbach, R.P. Responses to depression in children: Reconceptualizing the relation among response styles. J. Abnorm. Child Psychol. 2007, 35, 913–927. [Google Scholar] [CrossRef]
- Abela, J.R.; Brozina, K.; Haigh, E.P. An examination of the response styles theory of depression in third- and seventh-grade children: A short-term longitudinal study. J. Abnorm. Child Psychol. 2002, 30, 515–527. [Google Scholar] [CrossRef]
- Burwell, R.A.; Shirk, S.R. Subtypes of rumination in adolescence: Associations between brooding, reflection, depressive symptoms, and coping. J. Clin. Child. Adolesc. Psychol. 2007, 36, 56–65. [Google Scholar] [CrossRef]
- Grabe, S.; Hyde, J.S.; Lindberg, S.M. Body Objectification and Depression in Adolescents: The Role of Gender, Shame, and Rumination. Psychol. Women Q. 2007, 31, 164–175. [Google Scholar] [CrossRef]
- Nolen-Hoeksema, S.; Stice, E.; Wade, E.; Bohon, C. Reciprocal relations between rumination and bulimic, substance abuse, and depressive symptoms in female adolescents. J. Abnorm. Psychol. 2007, 116, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Ziegert, D.I.; Kistner, J.A. Response styles theory: Downward extension to children. J. Clin. Child. Adolesc. Psychol. 2002, 31, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Abela, J.R.; Vanderbilt, E.; Rochon, A. A test of the integration of the response styles and social support theories of depression in third and seventh grade children. J. Soc. Clin. Psychol. 2004, 23, 653–674. [Google Scholar] [CrossRef]
- Hilt, L.M.; McLaughlin, K.A.; Nolen-Hoeksema, S. Examination of the response styles theory in a community sample of young adolescents. J. Abnorm. Child. Psychol. 2010, 38, 545–556. [Google Scholar] [CrossRef]
- Lewinsohn, P.M.; Steinmetz, J.L.; Larson, D.W.; Franklin, J. Depression-related cognitions: Antecedent or consequence? J. Abnorm. Psychol. 1981, 90, 213–219. [Google Scholar] [CrossRef]
- Beevers, C.G.; Rohde, P.; Stice, E.; Nolen-Hoeksema, S. Recovery from major depressive disorder among female adolescents: A prospective test of the scar hypothesis. J. Consult. Clin. Psychol 2007, 75, 888–900. [Google Scholar] [CrossRef]
- Kindt, K.C.; Kleinjan, M.; Janssens, J.M.; Scholte, R.H. Evaluation of a school-based depression prevention program among adolescents from low-income areas: A randomized controlled effectiveness trial. Int. J. Environ. Res. Public Health 2014, 11, 5273–5293. [Google Scholar] [CrossRef]
- Kindt, K.C.; van Zundert, R.; Engels, R.C. Evaluation of a Dutch school-based depression prevention program for youths in highrisk neighborhoods: Study protocol of a two-armed randomized controlled trial. BMC Public Health 2012, 12, 212. [Google Scholar] [CrossRef]
- Kovacs, M. The children’s depression inventory (CDI). Psychopharmacol. Bull. 1985, 21, 995–998. [Google Scholar]
- Evers, A.; van Vliet-Mulder, J.C.; Groot, C.J. Documentatie van Tests en Testresearch in Nederland; Dean, O., Ed.; urn:nbn:nl:ui:12-85684; Koninklijke Van Gorcum BV: Assen, The Netherlands, 2000. [Google Scholar]
- Muthén, L.; Muthén, B. The Comprehensive Modelling Program for Applied Researchers: User’s Guide; Muthén & Muthén: Los Angeles, CA, USA , 2015. [Google Scholar]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef]
- Steiger, J.H. A note on multiple sample extensions of the RMSEA fit index. Struct. Equ. Model. A Multidiscip. J. 1998, 5, 5. [Google Scholar] [CrossRef]
- Marsh, H.W.; Hau, K.-T.; Wen, Z. In search of golden rules: Comment on hypothesis-testing approaches to setting cutoff values for fit indexes and dangers in overgeneralizing Hu and Bentler’s (1999) findings. Struct. Equ. Model. 2004, 11, 320–341. [Google Scholar] [CrossRef]
- Yang, C.; Nay, S.; Hoyle, R.H. Three approaches to using lengthy ordinal scales in structural equation models: Parceling, latent scoring, and shortening scales. Appl. Psychol. Meas. 2010, 34, 122–142. [Google Scholar] [CrossRef] [PubMed]
- Sass, D.A.; Smith, P.L. The effects of parceling unidimensional scales on structural parameter estimates in structural equation modeling. Struct. Equ. Model. 2006, 13, 566–586. [Google Scholar] [CrossRef]
- Little, T.D.; Cunningham, W.A.; Shahar, G.; Widaman, K.F. To parcel or not to parcel: Exploring the question, weighing the merits. Struct. Equ. Model. 2002, 9, 151–173. [Google Scholar] [CrossRef]
- Chen, F.F. Sensitivity of goodness of fit indexes to lack of measurement invariance. Struct. Equ. Model. A Multidiscip. J. 2007, 14, 464–504. [Google Scholar] [CrossRef]
- Cheung, G.W.; Rensvold, R.B. Evaluating goodness-of-fit indexes for testing measurement invariance. Struct. Equ. Model. 2002, 9, 233–255. [Google Scholar] [CrossRef]
- Garber, J.; Keiley, M.K.; Martin, N.C. Developmental trajectories of adolescents’ depressive symptoms: Predictors of change. J. Consult. Clin. Psychol. 2002, 70, 79. [Google Scholar] [CrossRef]
- Yaroslavsky, I.; Pettit, J.W.; Lewinsohn, P.M.; Seeley, J.R.; Roberts, R.E. Heterogeneous trajectories of depressive symptoms: Adolescent predictors and adult outcomes. J. Affect. Disord. 2013, 148, 391–399. [Google Scholar] [CrossRef]
- Sameroff, A.J.; Mackenzie, M.J. Research strategies for capturing transactional models of development: The limits of the possible. Dev. Psychopathol. 2003, 15, 613–640. [Google Scholar] [CrossRef]
- Muris, P.; Roelofs, J.; Meesters, C.; Boomsma, P. Rumination and worry in nonclinical adolescents. Cogn. Ther. Res. 2004, 28, 539–554. [Google Scholar] [CrossRef]
- Papadakis, A.A.; Prince, R.P.; Jones, N.P.; Strauman, T.J. Self-regulation, rumination, and vulnerability to depression in adolescent girls. Dev. Psychopathol. 2006, 18, 815–829. [Google Scholar] [CrossRef]
- Huijding, J. Implicit attitudes and psychopathology. Neth. J. Psychol. 2006, 62, 58–70. [Google Scholar] [CrossRef]
- de Haan-Rietdijk, S.; Voelkle, M.C.; Keijsers, L.; Hamaker, E.L. Discrete-vs. continuous-time modeling of unequally spaced experience sampling method data. Front. Psychol. 2017, 8, 1849. [Google Scholar] [CrossRef] [PubMed]
- Aalto-Setälä, T.; Marttunen, M.; Tuulio-Henriksson, A.; Poikolainen, K.; Lönnqvist, J. Depressive symptoms in adolescence as predictors of early adulthood depressive disorders and maladjustment. Am. J. Psychiatry 2002, 159, 1235–1237. [Google Scholar] [CrossRef]
- Pine, D.S.; Cohen, E.; Cohen, P.; Brook, J. Adolescent depressive symptoms as predictors of adult depression: Moodiness or mood disorder? Am. J. Psychiatry 1999, 156, 133–135. [Google Scholar] [CrossRef]
- Cuijpers, P.; Van Straten, A.; Warmerdam, L. Behavioral activation treatments of depression: A meta-analysis. Clin. Psychol. Rev. 2007, 27, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Tak, Y.R.; Lichtwarck-Aschoff, A.; Gillham, J.E.; Van Zundert, R.M.; Engels, R.C. Universal school-based depression prevention ‘Op Volle Kracht’: A longitudinal cluster randomized controlled trial. J. Abnorm. Child Psychol. 2016, 44, 949–961. [Google Scholar] [CrossRef]






| Standardized Factor Loadings | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| χ2 | df | p | RMSEA | CFI | ∆CFI | ∆RMSEA | Mean | SD | Min | Max | ||
| depressive symptoms | configural invariance | 94.86 | 74 | 0.052 | 0.015 | 0.998 | 0.82 | 0.04 | 0.72 | 0.87 | ||
| metric invariance | 111.04 | 83 | 0.022 | 0.016 | 0.997 | 0.001 | 0.001 | |||||
| strong invariance | 133.84 | 92 | 0.003 | 0.019 | 0.995 | 0.003 | 0.002 | |||||
| rumination | configural invariance | 35.58 | 30 | 0.222 | 0.012 | 0.999 | 0.89 | 0.03 | 0.85 | 0.94 | ||
| metric invariance | 52.49 | 36 | 0.037 | 0.019 | 0.998 | 0.007 | 0.001 | |||||
| strong invariance | 62.13 | 42 | 0.023 | 0.019 | 0.997 | 0.000 | 0.001 | |||||
| distraction | configural invariance | 40.70 | 30 | 0.092 | 0.016 | 0.996 | 0.67 | 0.08 | 0.56 | 0.79 | ||
| metric invariance | 47.83 | 36 | 0.090 | 0.016 | 0.995 | 0.000 | 0.001 | |||||
| strong invariance | 63.24 | 42 | 0.019 | 0.020 | 0.992 | 0.004 | 0.003 | |||||
| problem-solving | configural invariance | 37.76 | 30 | 0.156 | 0.014 | 0.998 | 0.75 | 0.08 | 0.58 | 0.84 | ||
| metric invariance | 40.69 | 36 | 0.272 | 0.010 | 0.999 | −0.004 | −0.001 | |||||
| strong invariance | 56.04 | 42 | 0.072 | 0.016 | 0.996 | 0.006 | 0.003 | |||||
| Total | Boys | Girls | t-Value | Cohen’s d | |
|---|---|---|---|---|---|
| T1 Depressive Symptoms | 8.23 (6.26) | 7.76(6.28) | 8.66 (6.22) | 2.55 * | 0.14 |
| T2 Depressive Symptoms | 9.08 (7.42) | 8.86 (8.16) | 9.27 (6.69) | 0.92 | 0.05 |
| T3 Depressive Symptoms | 9.23(7.84) | 8.77 (8.29) | 9.63 (7.42) | 1.69 | 0.11 |
| T4 Depressive Symptoms | 9.23(8.17) | 8.94 (8.79) | 9.47 (7.61) | 1.00 | 0.06 |
| T1 Rumination | 20.18 (7.40) | 18.40(6.20) | 21.85 (8.02) | 8.36 *** | 0.48 |
| T2 Rumination | 20.53 (7.79) | 18.76 (7.00) | 22.17 (8.13) | 7.40 *** | 0.45 |
| T3 Rumination | 20.36 (7.79) | 18.48 (7.28) | 21.89 (7.85) | 6.96 *** | 0.46 |
| T4 Rumination | 20.16 (7.64) | 18.16 (6.47) | 21.83 (8.13) | 7.72 *** | 0.50 |
| T1 Distraction | 13.24 (3.92) | 12.79 (4.01) | 13.66 (3.80) | 3.90 *** | 0.22 |
| T2 Distraction | 12.80 (4.00) | 12.19 (4.24) | 13.35 (3.69) | 4.83 *** | 0.29 |
| T3 Distraction | 12.58 (3.94) | 11.81 (4.11) | 13.25 (3.65) | 5.59 *** | 0.37 |
| T4 Distraction | 12.39 (3.94) | 11.61 (3.98) | 13.03 (3.79) | 5.73 *** | 0.37 |
| T1 Problem-Solving | 8.63 (3.20) | 7.74 (2.90) | 9.46 (3.24) | 9.72 *** | 0.56 |
| T2 Problem-Solving | 8.43 (3.14) | 7.87 (3.13) | 8.93 (3.06) | 5.65 *** | 0.34 |
| T3 Problem-Solving | 8.39 (3.24) | 7.53 (3.11) | 9.13 (3.16) | 7.67 *** | 0.51 |
| T4 Problem-Solving | 8.44 (3.29) | 7.62 (3.02) | 9.13 (3.34) | 7.34 *** | 0.47 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Dep. symptoms T1 | 0.58 ** | 0.53 ** | 0.41 ** | 0.48 ** | 0.30 ** | 0.29 ** | 0.22 ** | −0.20 ** | −0.16 ** | −0.17 ** | −0.09 ** | −0.24 ** | −0.15 ** | −0.11 ** | −0.12 ** | |
| 2. Dep. symptoms T2 | 0.58 ** | 0.57 ** | 0.45 ** | 0.32 ** | 0.40 ** | 0.26 ** | 0.26 ** | −0.10 ** | −0.20 ** | −0.11 ** | −0.13 ** | −0.21 ** | −0.20 ** | −0.17 ** | −0.14 ** | |
| 3. Dep. symptoms T3 | 00.53 ** | 0.57 ** | 0.58 ** | 0.27 ** | 0.30 ** | 0.37 ** | 0.31 ** | −0.09 * | −0.15 ** | −0.20 ** | −0.14 ** | −0.18 ** | −0.16 ** | −0.18 ** | −0.16 ** | |
| 4. Dep. symptoms T4 | 0.41 ** | 0.44 ** | 0.57 ** | 0.21 ** | 0.24 ** | 0.25 ** | 0.42 ** | −0.06 | −0.13 ** | −0.11 ** | −0.21 ** | −0.15 ** | −0.12 ** | −0.17 ** | −0.21 ** | |
| 5. Rumination T1 | 0.50 ** | 0.34 ** | 0.30 ** | 0.18 ** | 0.48 ** | 0.39 ** | 0.29 ** | −0.50 ** | −0.27 ** | −0.26 ** | −0.16 ** | −0.43 ** | −0.20 ** | −0.11 ** | −0.14 ** | |
| 6. Rumination T2 | 0.34 ** | 0.50 ** | 0.32 ** | 0.25 ** | 0.51 ** | 0.58 ** | 0.41 ** | −0.25 ** | −0.53 ** | −0.33 ** | −0.24 ** | −0.18 ** | −0.42 ** | −0.21 ** | −0.19 ** | |
| 7. Rumination T3 | 0.30 ** | 0.33 ** | 0.47 ** | 0.28 ** | 0.42 ** | 0.50 ** | 0.48 ** | −0.16 ** | −0.31 ** | −0.52 ** | −0.24 ** | −0.21 ** | −0.23 ** | −0.43 ** | −0.23 ** | |
| 8. Rumination T4 | 0.23 ** | 0.27** | 0.30 ** | 0.41 ** | 0.32 ** | 0.43 ** | 0.45 ** | −0.11 ** | −0.19 ** | −0.22 ** | −0.49 ** | −0.16 ** | −0.21 ** | −0.24 ** | −0.46 ** | |
| 9. Distraction T1 | 0.04 | 0.07 * | 0.05 | −0.02 | 0.33 ** | 0.12 ** | 0.15 ** | 0.05 | 0.27 ** | 0.25 ** | 0.18 ** | −0.49 ** | −0.02 | −0.11 ** | −0.08 * | |
| 10. Distraction T2 | 0.04 | 0.11 ** | 0.01 | 0.00 | 0.15 ** | 0.41 ** | 0.11 ** | 0.07 * | 0.31 ** | 0.33 ** | 0.26 ** | −0.01 | −0.47 ** | −0.01 | −0.03 | |
| 11. Distraction T3 | 0.03 | 0.09 * | 0.14 ** | 0.04 | 0.12 ** | 0.11 ** | 0.43 ** | 0.13 ** | 0.28 ** | 0.34 ** | 0.28 ** | 0.02 | −0.03 | −0.47 ** | −0.07 | |
| 12. Distraction T4 | 0.06 | −0.03 | 0.03 | 0.04 | 0.14 ** | 0.16 ** | 0.18 ** | 0.48 ** | 0.16 ** | 0.25 ** | 0.32 ** | −0.03 | −0.03 | −0.06 | −0.46 ** | |
| 13. Problem−solving T1 | 0.01 | −0.01 | −0.03 | −0.07 * | 0.42 ** | 0.22 ** | 0.20 ** | 0.13 ** | 0.49 ** | 0.29 ** | 0.29 ** | 0.20 ** | 0.22 ** | 0.22 ** | 0.23 ** | |
| 14. Problem−solving T2 | 0.05 | 0.10 ** | 0.02 | 0.02 | 0.23 ** | 0.50 ** | 0.17 ** | 0.16 ** | 0.24 ** | 0.56 ** | 0.25 ** | 0.24 ** | 0.37 ** | 0.25 ** | 0.25 ** | |
| 15. Problem−solving T3 | 0.05 | 0.05 | 0.12 ** | 0.01 | 0.20 ** | 0.20 ** | 0.52 ** | 0.19 ** | 0.19 ** | 0.26 ** | 0.60 ** | 0.27 ** | 0.35 ** | 0.33 ** | 0.34 ** | |
| 16. Problem−solving T4 | 0.04 | 0.03 | 0.01 | 0.02 | 0.16 ** | 0.17 ** | 0.21 ** | 0.51 ** | 0.12 ** | 0.15 ** | 0.26 ** | 0.60 ** | 0.29 ** | 0.29 ** | 0.40 ** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Ettekoven, K.M.; Rasing, S.P.A.; Vermulst, A.A.; Engels, R.C.M.E.; Kindt, K.C.M.; Creemers, D.H.M. Cross-Lagged Associations between Depressive Symptoms and Response Style in Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 1380. https://doi.org/10.3390/ijerph17041380
van Ettekoven KM, Rasing SPA, Vermulst AA, Engels RCME, Kindt KCM, Creemers DHM. Cross-Lagged Associations between Depressive Symptoms and Response Style in Adolescents. International Journal of Environmental Research and Public Health. 2020; 17(4):1380. https://doi.org/10.3390/ijerph17041380
Chicago/Turabian Stylevan Ettekoven, Kim M., Sanne P. A. Rasing, Ad A. Vermulst, Rutger C. M. E. Engels, Karlijn C. M. Kindt, and Daan H. M. Creemers. 2020. "Cross-Lagged Associations between Depressive Symptoms and Response Style in Adolescents" International Journal of Environmental Research and Public Health 17, no. 4: 1380. https://doi.org/10.3390/ijerph17041380
APA Stylevan Ettekoven, K. M., Rasing, S. P. A., Vermulst, A. A., Engels, R. C. M. E., Kindt, K. C. M., & Creemers, D. H. M. (2020). Cross-Lagged Associations between Depressive Symptoms and Response Style in Adolescents. International Journal of Environmental Research and Public Health, 17(4), 1380. https://doi.org/10.3390/ijerph17041380