Factors Associated with Dental Plaque, Gingivitis, and Caries in a Pediatric Population: A Records-Based Cross-Sectional Study


Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Subject Characteristics and Demographics
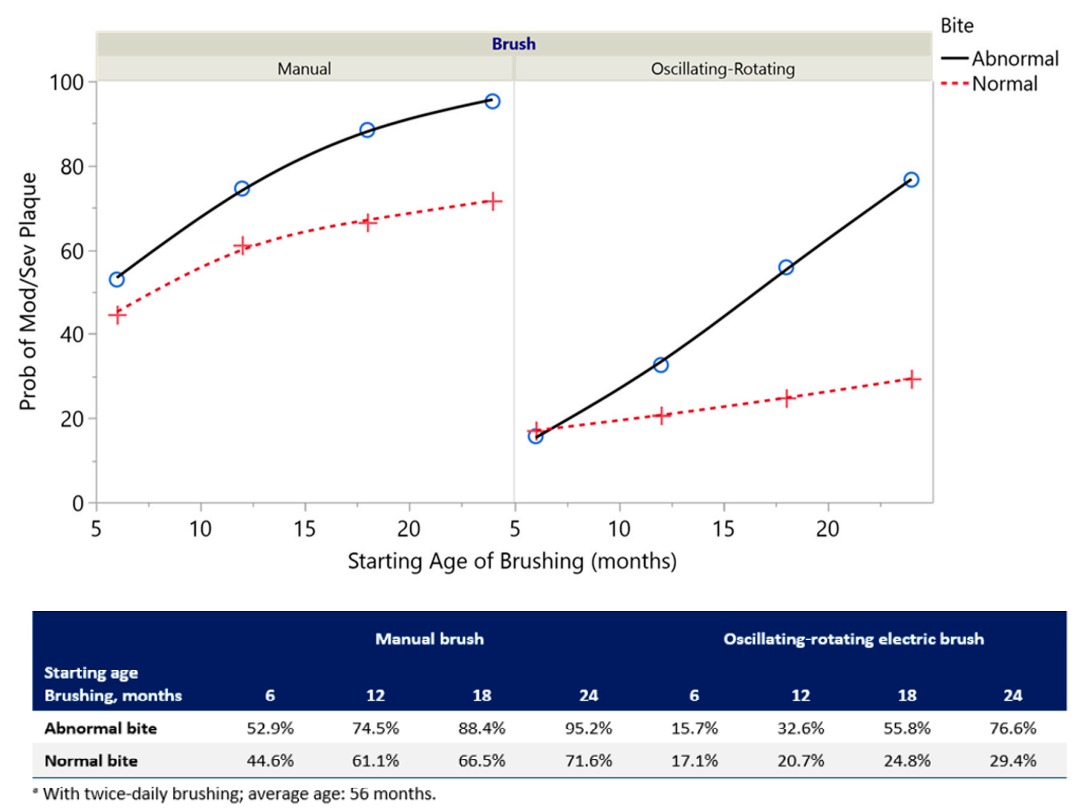
3.2. Dental Plaque Modeling
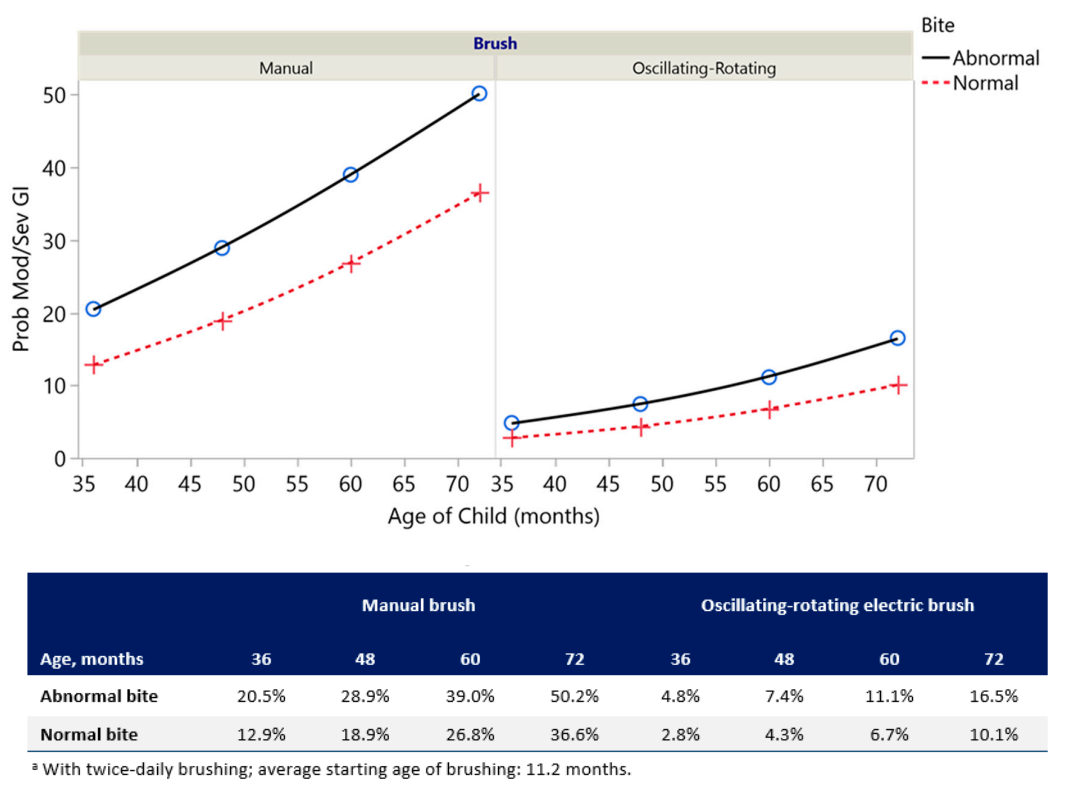
3.3. Gingivitis Modeling
3.4. Caries Modeling
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef]
- Moynihan, P.J.; Kelly, S.A. Effect on caries of restricting sugars intake: Systematic review to inform WHO guidelines. J. Dent. Res. 2014, 93, 8–18. [Google Scholar] [CrossRef] [PubMed]
- A global outlook on sugar. BDJ Team 2017, 4, 17045. Available online: https://www.nature.com/articles/bdjteam201745?platform=hootsuite (accessed on 2 November 2020). [CrossRef][Green Version]
- Chi, D.L.; Scott, J.M. Added sugar and dental caries in children: A scientific update and future steps. Dent. Clin. N. Am. 2019, 63, 17–33. [Google Scholar] [CrossRef]
- Marshall, T.A.; Levy, S.M.; Broffitt, B.; Warren, J.J.; Eichenberger-Gilmore, J.M.; Burns, T.L.; Stumbo, P.J. Dental caries and beverage consumption in young children. Pediatrics 2003, 112 Pt 1, e184–e191. [Google Scholar] [CrossRef]
- Anil, S.; Anand, P.S. Early Childhood Caries: Prevalence, risk factors, and prevention. Front. Pediatr. 2017, 5, 157. [Google Scholar] [CrossRef]
- Zijnge, V.; van Leeuwen, M.B.; Degener, J.E.; Abbas, F.; Thurnheer, T.; Gmur, R.; Harmsen, H.J.M. Oral biofilm architecture on natural teeth. PLoS ONE 2010, 5, e9321. [Google Scholar] [CrossRef]
- Aliakbari, E.; Gray-Burrows, K.A.; Vinall-Collier, K.A.; Edwebi, S.; Marshman, Z.; McEachan, R.R.C.; Day, P.F. Home-based toothbrushing interventions for parents of young children to reduce dental caries: A systematic review. Int. J. Paediatr. Dent. 2020. [Google Scholar] [CrossRef]
- Pari, A.; Ilango, P.; Subbareddy, V.; Katamreddy, V.; Parthasarthy, H. Gingival diseases in childhood—A review. J. Clin. Diagn. Res. 2014, 8, ZE01–ZE04. [Google Scholar] [CrossRef]
- Eskyte, I.; Gray-Burrows, K.; Owen, J.; Sykes-Muskett, B.; Zoltie, T.; Gill, S.; Smith, V.; McEachan, R.; Marshman, Z.; West, R.; et al. HABIT-an early phase study to explore an oral health intervention delivered by health visitors to parents with young children aged 9-12 months: Study protocol. Pilot Feasibility Stud. 2018, 4, 68. [Google Scholar] [CrossRef]
- Marshman, Z.; Ahern, S.M.; McEachan, R.R.C.; Rogers, H.J.; Gray-Burrows, K.A.; Day, P.F. Parents’ experiences of toothbrushing with children: A qualitative study. JDR Clin. Trans. Res. 2016, 1, 122–130. [Google Scholar] [CrossRef]
- Kurtz, B.; Reise, M.; Klukowska, M.; Grender, J.M.; Timm, H.; Sigusch, B.W. A randomized clinical trial comparing plaque removal efficacy of an oscillating-rotating power toothbrush to a manual toothbrush by multiple examiners. Int. J. Dent. Hyg. 2016, 14, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Yaacob, M.; Worthington, H.V.; Deacon, S.A.; Deery, C.; Walmsley, A.D.; Robinson, P.G.; Glenny, A.-M. Powered versus manual toothbrushing for oral health. Cochrane Database Syst. Rev. 2014, 6, CD002281. [Google Scholar] [CrossRef] [PubMed]
- Grender, J.; Williams, K.; Walters, P.; Klukowska, M.; Reick, H. Plaque removal efficacy of oscillating-rotating power toothbrushes: Review of six comparative clinical trials. Am. J. Dent. 2013, 26, 68–74. [Google Scholar] [PubMed]
- Grender, J.; Adam, R.; Zou, Y. The effects of oscillating-rotating electric toothbrushes on plaque and gingival health: A meta-analysis. Am. J. Dent. 2020, 33, 3–11. [Google Scholar]
- Van der Weijden, F.A.; Slot, D.E. Efficacy of homecare regimens for mechanical plaque removal in managing gingivitis a meta review. J. Clin. Periodontol. 2015, 42 (Suppl. 16), S77–S91. [Google Scholar] [CrossRef]
- Clark-Perry, D.; Levin, L. Systematic review and meta-analysis of randomized controlled studies comparing oscillating-rotating and other powered toothbrushes. J. Am. Dent. Assoc. 2020, 151, 265–275. [Google Scholar] [CrossRef]
- Davidovich, E.; Shafir, S.; Shay, B.; Zini, A. Plaque removal by a powered toothbrush versus a manual toothbrush in children: A systematic review and meta-analysis. Pediatr. Dent. 2020, 42, 280–287. [Google Scholar]
- Davidovich, E.; Ccahuana-Vasquez, R.A.; Timm, H.; Grender, J.; Cunningham, P.; Zini, A. Randomised clinical study of plaque removal efficacy of a power toothbrush in a paediatric population. Int. J. Paediatr. Dent. 2017, 27, 558–567. [Google Scholar] [CrossRef]
- Davidovich, E.; Ccahuana-Vásquez, R.; Timm, H.; Grender, J.; Zini, A. Randomised clinical study of plaque removal efficacy of an electric toothbrush in primary and mixed dentition. Int. J. Paediatr. Dent. 2020, in press. [Google Scholar]
- Quigley, G.A.; Hein, J.W. Comparative cleansing efficiency of manual and power brushing. J. Am. Dent. Assoc. 1962, 65, 26–29. [Google Scholar] [CrossRef] [PubMed]
- Turesky, S.; Gilmore, N.D.; Glickman, I. Reduced plaque formation by the chloromethyl analogue of victamine C. J. Periodontol. 1970, 41, 41–43. [Google Scholar] [CrossRef] [PubMed]
- Lobene, R.R.; Weatherford, T.; Ross, N.M.; Lamm, R.A.; Menaker, L. A modified gingival index for use in clinical trials. Clin. Prev. Dent. 1986, 8, 3–6. [Google Scholar] [PubMed]
- Hilgert, L.A.; Leal, S.C.; Bronkhorst, E.M.; Frencken, J.E. Long-term Effect of Supervised Toothbrushing on Levels of Plaque and Gingival Bleeding Among Schoolchildren. Oral Health Prev. Dent. 2017, 15, 537–542. [Google Scholar]
- Walsh, T.; Worthington, H.V.; Glenny, A.M.; Marinho, V.C.; Jeroncic, A. Fluoride toothpastes of different concentrations for preventing dental caries. Cochrane Database Syst. Rev. 2019, 3, CD007868. [Google Scholar] [CrossRef] [PubMed]
- Jackson, R.J.; Newman, H.N.; Smart, G.J.; Stokes, E.; Hogan, J.I.; Brown, C.; Seres, J. The effects of a supervised toothbrushing programme on the caries increment of primary school children, initially aged 5-6 years. Caries Res. 2005, 39, 108–115. [Google Scholar] [CrossRef]
- Declerck, D.; Leroy, R.; Martens, L.; Lesaffre, E.; Garcia-Zattera, M.-J.; Broucke, S.V.; Debyser, M.; Hoppenbrouwers, K. Factors associated with prevalence and severity of caries experience in preschool children. Community Dent. Oral Epidemiol. 2008, 36, 168–178. [Google Scholar] [CrossRef]
- Martens, L.; Vanobbergen, J.; Leroy, R.; Lesaffre, E.; Declerck, D. Variables associated with oral hygiene levels in 7-year-olds in Belgium. Community Dent. Health 2004, 21, 4–10. [Google Scholar]
- American Academy of Pediatric Dentistry. Caries-risk assessment and management for infants, children, and adolescents. In The Reference Manual of Pediatric Dentistry; American Academy of Pediatric Dentistry: Chicago, IL, USA, 2019; pp. 220–224. Available online: https://www.aapd.org/research/oral-health-policies--recommendations/caries-risk-assessment-and-management-for-infants-children-and-adolescents/ (accessed on 2 November 2020).
- Colak, H.; Dulgergil, C.T.; Dalli, M.; Hamidi, M.M. Early childhood caries update: A review of causes, diagnoses, and treatments. J. Nat. Sci. Biol. Med. 2013, 4, 29–38. [Google Scholar] [CrossRef]
- Milsom, K.M.; Blinkhorn, A.S.; Tickle, M. The incidence of dental caries in the primary molar teeth of young children receiving National Health Service funded dental care in practices in the North West of England. Br. Dent. J. 2008, 205, E14, discussion 384–385. [Google Scholar] [CrossRef]
- Calcagnile, F.; Pietrunti, D.; Pranno, N.; Di Giorgio, G.; Ottolenghi, L.; Vozza, I. Oral health knowledge in pre-school children: A survey among parents in central Italy. J. Clin. Exp. Dent. 2019, 11, e327–e333. [Google Scholar] [CrossRef] [PubMed]
- Tull, K.; Gray-Burrows, K.A.; Bhatti, A.; Owen, J.; Rutter, L.; Zoltie, T.; Purdy, J.; Giles, E.; Paige, C.; Patel, M.; et al. “Strong Teeth”—A study protocol for an early-phase feasibility trial of a complex oral health intervention delivered by dental teams to parents of young children. Pilot Feasibility Stud. 2019, 5, 100. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, S.; Seshadri, D. Conducting record review studies in clinical practice. J. Clin. Diagn. Res. 2014, 8, JG01–JG04. [Google Scholar] [CrossRef] [PubMed]
- Pitchika, V.; Pink, C.; Volzke, H.; Welk, A.; Kocher, T.; Holtfreter, B. Long-term impact of powered toothbrush on oral health: 11-year cohort study. J. Clin. Periodontol. 2019, 46, 713–722. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | (N = 1000) |
|---|---|
| Age, years | |
| Mean | 4.7 |
| Median (range) | 4.8 (2.5 to 7.0) |
| Gender, % | |
| Female | 53.3 |
| Male | 46.7 |
| Dentition, % | |
| Primary | 83.9 |
| Mixed | 16.1 |
| Bite, % | |
| Normal | 73.6 |
| Open bite | 25.9 |
| Cross-bite | 0.5 |
| Brush type, % | |
| Manual | 63.5 |
| Oscillating-rotating electric | 36.3 |
| Sonic electric | 0.2 |
| Brushing frequency, % | |
| Twice-daily | 72.0 |
| Morning only | 8.8 |
| Evening only | 19.2 |
| Age at start of tooth brushing, months | |
| Mean | 11.2 |
| Median (range) | 12.0 (6.0 to 24.0) |
| Supervised brushing, % | 74.7 |
| Pacifier use, % a | 21.5 |
| Thumb sucker, % a | 0.2 |
| Plaque severity, % | |
| Mild | 45.0 |
| Moderate | 47.5 |
| Severe | 7.5 |
| Gingivitis severity, % | |
| Mild | 73.6 |
| Moderate | 23.4 |
| Severe | 3.0 |
| Caries present, % | 38.8 |
| Factor a | p-Value | Odds Ratio (95% CI) b |
|---|---|---|
| Brush Type (oscillating—rotating/manual) | <0.001 | 6.03 (4.40, 8.27) |
| Brushing Frequency (2×/1×) | <0.001 | 4.36 (3.04, 6.25) |
| Bite Type (normal/abnormal) c | 0.012 | 1.68 (1.12, 2.52) |
| Age (months) | <0.001 | 1.03 (1.02, 1.04) |
| Starting Age of Brushing (months) | <0.001 | NA since Starting Age of Brushing × Bite Type in model |
| Starting Age of Brushing × Bite | 0.012 |
| Factor a | p-Value | Odds Ratio (95% CI) b |
|---|---|---|
| Brush type (oscillating-rotating/manual) | <0.001 | 5.12 (3.41, 7.69) |
| Brushing frequency (2×/1×) | <0.001 | 3.08 (2.22, 4.28) |
| Bite (normal/abnormal) | 0.006 | 1.75 (1.17, 2.60) |
| Starting Age of brushing (months) | 0.001 | 1.05 (1.02, 1.08) |
| Age (months) | <0.001 | 1.04 (1.02, 1.05) |
| Factor a | p-Value | Odds Ratio (95% CI) b |
|---|---|---|
| Brushing frequency (2×/1×) | <0.001 | 1.67 (1.25, 2.24) |
| Brush type (oscillating-rotating/manual) | 0.013 | 1.43 (1.08, 1.91) |
| Starting Age of brushing (months) | <0.001 | 1.05 (1.02, 1.07) |
| Age (months) | 0.045 | NA since age × age in model |
| Age × Age (months) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davidovich, E.; Grender, J.; Zini, A. Factors Associated with Dental Plaque, Gingivitis, and Caries in a Pediatric Population: A Records-Based Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 8595. https://doi.org/10.3390/ijerph17228595
Davidovich E, Grender J, Zini A. Factors Associated with Dental Plaque, Gingivitis, and Caries in a Pediatric Population: A Records-Based Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2020; 17(22):8595. https://doi.org/10.3390/ijerph17228595
Chicago/Turabian StyleDavidovich, Esti, Julie Grender, and Avi Zini. 2020. "Factors Associated with Dental Plaque, Gingivitis, and Caries in a Pediatric Population: A Records-Based Cross-Sectional Study" International Journal of Environmental Research and Public Health 17, no. 22: 8595. https://doi.org/10.3390/ijerph17228595
APA StyleDavidovich, E., Grender, J., & Zini, A. (2020). Factors Associated with Dental Plaque, Gingivitis, and Caries in a Pediatric Population: A Records-Based Cross-Sectional Study. International Journal of Environmental Research and Public Health, 17(22), 8595. https://doi.org/10.3390/ijerph17228595