Abstract
Anti-atherogenic therapy is crucial in halting the progression of inflammation-induced intimal hyperplasia. The aim of this concise review was to methodically assess the recent findings of the different approaches, mainly on the recruitment of chemokines and/or cytokine and its effects in combating the intimal hyperplasia caused by various risk factors. Pubmed and Scopus databases were searched, followed by article selection based on pre-set inclusion and exclusion criteria. The combination of keywords used were monocyte chemoattractant protein-1 OR MCP-1 OR TNF-alpha OR TNF-α AND hyperplasia OR intimal hyperplasia OR neointimal hyperplasia AND in vitro. These keywords combination was incorporated in the study and had successfully identified 77 articles, with 22 articles were acquired from Pubmed, whereas 55 articles were obtained from Scopus. However, after title screening, only twelve articles meet the requirements of defined inclusion criteria. We classified the data into 4 different approaches, i.e., utilisation of natural product, genetic manipulation and protein inhibition, targeted drugs in clinical setting, and chemokine and cytokines induction. Most of the articles are working on genetic manipulation targeted on specific pathway to inhibit the pro-inflammatory factors expression. We also found that the utilisation of chemokine- and cytokine-related treatments are emerging throughout the years. However, there is no study utilising the combination of approaches that might give a better outcome in combating intimal hyperplasia. Hopefully, this concise review will provide an insight regarding the usage of different novel approaches in halting the progression of intimal hyperplasia, which serves as a key factor for the development of atherosclerosis in cardiovascular disease.
1. Introduction
1.1. Vascular Intimal Hyperplasia, Risk Factors and Current Therapy
Cardiovascular disease (CVD) is a primary cause of death for certain regions in the world, which can be a great hindrance to a continuity of human life [1]. Atherosclerosis is recognized as a major leading cause for CVD [2,3] causing obstruction of the vessels, through soft plaque calcification [4], which hardens, thickens and narrows the inner wall arteries [5,6]. Atherosclerosis progresses into coronary artery disease, causing the shortage or reduction of oxygen-rich blood flow [7] to the cardiac muscle. This condition will eventually contribute to critical cardiac problems, including myocardial infarction [8] and chronic cardiac failure [9]. Intimal thickening is considered as a precursor to lesion progression in atherosclerosis, but the primary factors contributing to its emergence remain elusive. In general, atherogenesis can be divided into several key phases [10], which include the endothelial dysfunction or impairment, generation of lipid within the intimal region, cell growth and migration of smooth muscle cells and leukocytes across the vascular wall, formation of foam cell and deterioration of extracellular matrix [11].
Intimal hyperplasia (IH) is an abnormal cell aggregation that has been observed in various developments of vascular diseases [12], mainly in atherosclerosis, occlusion of veins [13] and synthetic vascular grafts, in-stent restenosis and coronary angioplasty [14]. This process is closely related to the increment of cell numbers [15,16]; thus, its formation is frequently associated with vascular cell activation [17]. There are a few types of cells that are linked to the development and continuation of this process, predominantly vascular smooth muscle cells (VSMCs) [18], vascular adventitial fibroblast cells [19], vascular endothelial progenitor cells [20] and bone marrow derived progenitor cells [21], which originated from the different lining. VSMCs is crucial for the progression of intimal stiffening and development of neointimal hyperplasia [22], via cell migration from the media to intima layer and deposition of increased extracellular matrix, which finally comprise about 60–80% of the intimal region [23]. This may result in high cellular density within the lesion in the subintimal area, eventually decreasing the size of the lumen and contributing to thrombosis in the blood vessels [24].
Recent studies reported the numerous risk factors promoting the development of IH. Most of the main risk factors for IH are due to vascular wall injury, especially in the event of balloon angioplasty [25] and stents positioning [26]. These events remarkably exacerbate both thrombosis and increase the rate of IH [27], infiltration of inflammatory cells that regulate inflammatory response, which play a crucial role in intimal thickening after coronary stenting [28] and ageing of human arteries [29].
Over the past few decades, various interventions performed by the clinicians to circumvent atherosclerosis, particularly by percutaneous transluminal angioplasty (PTA) [30], placement of medical devices such as stents [31] or drug-eluting stents [32], the use of human saphenous vein (HSV) grafts in coronary artery bypass grafting (CABG) surgery [33] or peripheral bypass surgery [34] and coronary endarterectomy [35]. In spite of the numerous advantages, these interventions remained unsuccessful in preventing arterial restenosis caused by neointimal hyperplasia [36,37]. To date, an effective strategy to counteract this unsatisfactory outcome is yet to be discovered. This review article will explicate the essential values of different factors and their significant effects towards an alternative intervention in combating IH development.
1.2. Chemokines and/or Cytokines Effects in Inhibiting Intimal Hyperplasia Development
Active involvement of chemokines and/or cytokines is mostly connected with diverse biological processes. These processes are primarily consisting of cellular attachment, proliferation, migration, differentiation, growth, maintenance and signal transduction, inter and intracellular communication and activation of various immune response. In recent years, several reports suggested that selecting chemokines with the combination of cytokines may have a promising effect on halting the progression of IH. A wide range of anti-inflammatory or pro-inflammatory cytokines and/or chemokines has been studied and proven to gradually decrease the inflammatory events in the IH and atherosclerosis.
Atherosclerotic vascular disease pathological event involves inflammatory response, which promotes macrophages and lymphocytes infiltration into the vascular wall. The mediators contributing to this process are normally chemokines and their receptors [38]. Monocyte chemoattractant protein-1 (MCP-1) is expressed by macrophages, endothelial cells (ECs) and vascular smooth muscle cells (VSMCs) [39]. It is a member of the C-C chemokine family and has a great impact on the migration of monocytes or macrophages that contributes to inflammatory response in atherogenesis. Monocyte chemoattractant protein (MCP)-1 is one of the pro-inflammatory chemokine that is positively expressed in atherosclerotic plaque and in the intimal area during the arterial injury. CC chemokine receptor 2 (CCR2) is recognized as a functional receptor for MCP-1. Roque et al. (2002) [40] showed that CCR2 has a significant role in affecting the growth of smooth muscle cell and the progression of IH in an animal model of chronic arterial injury. This study had also proved that infiltration of macrophages was not significant, when rapid adherence of leukocytes to the arterial surface injury are maintained. On the contrary, Furukawa and co-workers (1999) [41] demonstrated that the use of anti–MCP-1 treatment significantly attenuated the development of neointimal hyperplasia, before and immediately after the carotid arterial injury. These findings can further clarify the IH inhibitory effects of the MCP-1 in vivo.
Another one of such pro-inflammatory cytokines that is secreted by macrophages/monocytes upon severe inflammation is tumour necrosis factor-alpha (TNF-α). TNF-α plays a key role in a various cell signalling events [42] and is recognized as one of the many cytokines that significantly upregulated in various diseases. It is also thought to be as one of the pathological factors for a number of common arterial diseases, such as atherosclerosis and preeclamptic hypertension [43,44]. The most recent study by Maleknia and colleagues (2020) [45] reported that TNF-α and interleukin-1 (IL-1) in the early inflammation decreased IH leading to restenosis, by inducing the production of insulin-like growth factor binding proteins (IGFBPs) in the vascular wall.
Chemokines such as MCP-1 are potent chemotactic agents for monocytes [46]. The cytokines such as pleiotrophin and TNF-α were recognized as key factors in promoting trans differentiation of monocytic cells to endothelial-like cells [47]. Based on the significant effects of chemokines/cytokines, we suggest that they could be used with combination of the scaffold to inhibit the progression of intimal hyperplasia. In the future, the coating of scaffold with these chemokines and cytokines may therefore facilitate the attraction of monocytes to the scaffold and induce differentiation into endothelial-like cells to line the scaffold and attenuate the thrombus formation, intimal thickening and beneficial remodelling. Moreover, the scaffold will induce in situ cell recruitment and differentiation [48], which will avoid the need for ex vivo tissue engineering, which is costly and time-consuming. Thus, we suggest that future modification using coated chemokines/cytokines to the scaffold is required to improve the graft performance and this novelty could minimize the operating time, clinical risks, and expenses.
Therefore, the synergistic effect of the proinflammatory cytokines and growth factors in the pathologic event of restenosis can be considered as an early promising factor for future application of alternative cardiac therapies. In this short review, we concentrate on recent novel discoveries using anti-inflammatory and pro-inflammatory chemokines and cytokines as a therapeutic agent, particularly in the suppression of IH, restenosis and atherosclerosis.
2. Methods
2.1. Search Strategy in Selected Databases
The review procedures were methodically carried out by screening all published journal articles that are related to the effects of using different chemokines and cytokines for cardiovascular disease therapy. There are two separate databases that were systematically used to explore the related study, which are Pubmed and Scopus. The combination of keywords used were monocyte chemoattractant protein-1 OR MCP-1 OR TNF-alpha OR TNF-α AND hyperplasia OR intimal hyperplasia OR neointimal hyperplasia AND in vitro.
2.2. Criteria of Selection
Studies published in English within a 5-year limit ranging from 2015 to 2020 have been reviewed. Only published articles that provide free full text articles were considered. Titles and abstracts that fill the topic requirements were systematically screened. All research articles related to the effect of cytokines and chemokines for the treatment of cardiovascular disease were included. The selection criteria exclude all case reports, clinical trials, systematic reviews, letters, technical reports and editorial publications.
2.3. Management of Data Extraction Table
Data from selected articles were extracted by two reviewers. The articles selection underwent several screening processes before being included in the data extraction table. Titles were carefully screened to meet the requirement of the topic of interest. Next, unrelated articles were omitted based on the abstracts of the shortlisted articles. At the end of the process, all identical papers were removed. Extracted information were outlined in a data extraction table as follows: (1) authors, (2) type of cells, (3) type of cytokines/chemokines involved, (4) type of disease, (5) methodology, (6) results and (8) conclusions.
3. Results
3.1. Search Results
The delineated inclusion and exclusion criteria of selected articles were separately evaluated by two reviewers to ensure objectivity of final articles selection. This was followed by discussion between authors to establish a consensus in assessing the differences surfaced upon articles assessment. The combination of keywords used during the search process successfully identified 22 articles acquired from Pubmed, whereas 55 articles were obtained from Scopus database. From that, 17 articles from Pubmed and 41 articles from Scopus were excluded after thorough title screening, followed by the removal of 2 duplicate articles, and thus, we were left with 17 articles to work with. At the end of the review process, 11 articles were removed from the final article selection, as they were unrelated to cardiovascular disease. Therefore, only six related articles were included in the data extraction table. The article selection process is summarized in Figure 1.
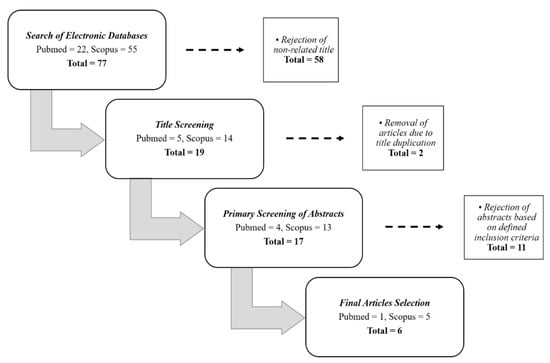
Figure 1.
The process flow of the final articles selection from both Pubmed and Scopus databases.
3.2. Study Characteristics
In this review, the search that was conducted through Pubmed and Scopus databases identifies six related articles, which are related to intimal hyperplasia, atherosclerosis and cardiovascular disease, whereas the rest of the studies were related to hypertension and stroke. From those articles, there are several types of cells that were used in the experiment, which are the vascular smooth muscle cells (VSMC), human umbilical vein endothelial cells (HUVECs), human saphenous vein cell lines, HeLa cell lines, human micro-vascular endothelial cells (HMEC-1) bone-marrow derived macrophages, adipocytes derived mesenchymal stem cells, peripheral blood mononuclear cells (MNCs), somatic cell nuclear transfer (SCNT) and the whole blood-derived leukocytes. Most of these cells are primarily acquired from human, pig and rat samples. All of these studies also reported the use of different agents, such as cytokine, i.e., tumour necrosis factor alpha (TNF-α) and interleukin 1 beta (IL-1b); transcriptional factor or coactivator, i.e., nuclear factor kappa beta (NF-κB) and P300/CBP-associated factor (PCAF); growth factor or chemokine, i.e., platelet-derived growth factor (PDGF-BB); extracellular matrix protein, i.e., microfibrillar-associated protein 4 (MFAP4); homoisoflavonoid or compound from plant extract, i.e., 7-O-methylpunctatin (MP) extracted from bulbs of Bellevalia eigii (herbaceous plants), hypaphorine (Hy) extracted from Erythrina velutina (leguminous tree), garcinol extracted from Garcinia indica fruit rind (mangosteen), ganoderma triterpenoids (GT) extracted from Ganoderma lucidum (mushroom) and antidiabetic drug or insulin-sensitizing agents, i.e., rosiglitazone (ROS) and pioglitazone (PGZ) that were categorized in the thiazolidinedione class. Meanwhile, the other studies used the collagen gel and collagen external scaffold as part of the treatment. These factors are recognized to possess anti-atherogenic effects, thus may play a major role in preventing intimal hyperplasia caused by inflammation. Three studies conducted both in vitro and in vivo study, while the rest focused on only in vitro studies. Ultimately, the selected articles have shown that the uses of different agents, particularly the chemokines and/or cytokines, are able to promote remarkable effects in preventing intimal hyperplasia. All articles were summarized in Table 1 and Table 2. We also provide a schematic on targeted signalling pathway involved in endothelial cells (ECs) activation and vascular smooth muscle cells (VSMCs) proliferation and migration during intimal hyperplasia in Figure 2.

Table 1.
Summary of the 4 articles conducted in vitro that were selected from both Pubmed and Scopus databases.
Table 2.
Summary of the 8 articles conducted in vitro and in vivo that were selected from both Pubmed and Scopus databases.
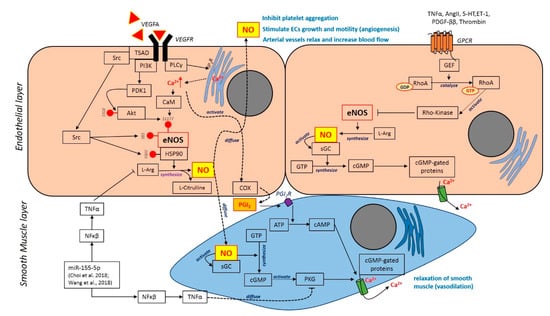
Figure 2.
Targeted signalling pathway involved in endothelial cells (ECs) activation and vascular smooth muscle cells (VSMCs) proliferation and migration during intimal hyperplasia. The binding of vascular endothelial growth factor A (VEGFA) to its receptor VEGFR2 on ECs activates the PI3K pathway. Activated PDK1 phosphorylates Akt at Thr308 then phosphorylates eNOS at Ser1177 activating eNOS. VEGFA aslo activates the PLCγ pathway which increase Ca2+ concentration and activates eNOS via calmodulin (CaM). The binding of VEGFA also activates Src kinase which then activates eNOS through two mechanisms: (1) phosphorylation of Tyr83 on eNOS; (2) phosphorylation of heat shock protein 90 (HSP90) at Tyr300. Those phosphorylation causes the binding of HSP90 to eNOS and activates NO synthesis. Activated eNOS converts L-arginine in the presence of oxygen to L-citrulline and diffusible signalling molecule NO. NO secreted by ECs inhibits platelet aggregation to avoid thrombosis. NO diffuses into vessel walls, causing arterial vessels to relax and increase blood flow. The binding of agonist to G-protein–coupled receptors (GPCR) induces activation of Rho-kinase activity via GEF activation. The activity of RhoA is controlled by the guanine nucleotide exchange factors (GEFs) that catalyse the exchange of GDP for GTP. Rho-kinase activity is enhanced by binding to the active GTP-bound RhoA. However, this mechanism is negatively regulating eNOS activation for NO production. Diffused NO binds to its intracellular receptor soluble GC (sGC) which produces cGMP from GTP. The increase in intracellular cGMP concentration bind to cGMP-dependent protein kinases (PKGs) and cGMP-gated ion channels results the increase of Ca2+ and relaxation of smooth muscle.
4. Discussion
For the past few decades, inflammation has been perceived as a pivotal body defence mechanism. However, a consistent escalation of certain proinflammatory factors leads to acute inflammation, thus creating an effect called hypercytokinemia or cytokine storms. Hypercytokinemia occurs in any part of the human body and affects the internal organs, including the human heart, which is predominantly due to atherosclerosis that triggers the formation of intimal hyperplasia at the early stage [61,62,63]. Inflammation within the vascular wall is a hurdle, and manipulating the inflammatory cytokines and chemokines is possibly the key piece in solving the puzzle. Other than that, research related to inhibition of intimal hyperplasia has also been extensively done using various approaches, which utilized gene therapy and vector-mediated gene delivery [49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64], anti-inflammatory and anti-proliferative drugs [57], compounds with anti-inflammatory actions such as plants [55,65], herbal medications [50], marine sources [52] and polyunsaturated fatty acids [56].
4.1. Utilisation of Natural Product to Combat IH
A novel approach in mitigating intimal hyperplasia includes the recruitments of compound from plant, herbal medicine and marine sources. A study reported by Hsu and co-workers [55] suggested the efficacy of atheroprotective properties in Ganoderma triterpenoids (GT), a ganoderma mushroom, which was proven to play a significant role in preventing atherogenesis, via the elimination of disturbed flow-induced oxidative stress and inflammation. They reported that GT extract inhibited the induction of a series of atherogenic factors, including endothelin-1, von Willebrand factor and MCP-1 in carotid-artery-ligation mouse model.
A previous study by Sotokawauchi and colleagues [65] postulated that the supplementation of sulforaphane-rich broccoli sprout extract has beneficial effects in exhibiting anti-inflammatory actions. They reported that the extract reduced the gene expression of MCP-1, intercellular adhesion molecule-1 (ICAM-1), while increased the endothelial nitric oxide synthase (eNOS) mRNA levels in HUVECs. However, the active component in sulforaphane-rich broccoli sprout extract needs to be further analysed along with in vivo and clinical studies. Other extracts such as hypaphorine (Hy), which is extracted from marine source, had been also shown to exert anti-inflammatory properties by inhibiting TNF-α, interleukin-1β (IL-1β), MCP-1 and vascular cellular adhesion molecule-1 (VCAM-1) in human mammary epithelial cells (HMECs). Thus, it could be considered as one of a potential alternative therapy in inhibiting inflammatory diseases, although the underlying molecular mechanism involving Hy remains unclear [52].
A study by Fardoun and colleague has successfully looked into the effect of a novel homoisoflavonoid known as 7-O-methylpunctatin (MP) on FBS-induced arteriolar SMC inflammation (microVSMCs), a model mimicking mild arteriolar inflammation. MP has been shown inhibited FBS-induced arteriolar SMC proliferation, migration, invasion and adhesion which aid in the ameliorating arteriolar inflammation in hypertension pathological conditions. Most instances of the utilisation of plant extracts were established in in vitro, which would certainly need to be further analysed along with in vivo before application in clinical studies. This VSMCs proliferation and migration inhibition hallmarks by those extracts would confer anti-inflammatory effects in mitigating intimal hyperplasia.
4.2. Genetic Manipulation and Protein Inhibition to Attenuate the Progression of IH
Other manipulation also can be performed by targeting a specific gene at the molecular level, which could also reduce the inflammatory factors. This has been done by generating a knock-out mouse as a model to demonstrate the effect of specific protein deficiency in elucidating their role in vivo.
Recent studies by de Jong and co-workers [53] demonstrated that the deficiency of P300/CBP-associated factor (PCAF) has led to the reduction of inflammatory cytokines release in vitro. The PCAF inhibition also alleviated infiltration of leukocytes that caused arterial injury, thus attenuating the progression of intimal hyperplasia in PCAF-knock-out (PCAF-KO) mice. The research work successfully identified the potential role of the lysine acetyltransferase PCAF in promoting the inflammation post-arterial injury and enhancing the proliferation of vascular smooth muscle cells.
Another study by Schlosser and colleague produced Mfap4-deficient mice to investigate microfibrillar-associated protein 4 (Mfap4) function in intima formation in vivo. The Mfap4-deficient mice showed delayed intimal formation after 14-days of formation of carotid arteries ligation. Mfap4 is localised in the ECM arteries, which is secreted by VSMC. At the cellular level, Mfap4 induced phosphorylation of FAK and activated the downstream protein involved in focal adhesion. FAK also acted through PI3K pathways, which were involved in VSMC migration and proliferation. Therefore, deficient of Mfap4 inhibited the intimal hyperplasia formation.
In another set of studies by Choi and colleague (2017), microRNA-155 (miR-155) has been used to target 3’UTR of cGMP-dependent protein kinase 1 (PKG1) mRNA. PKG1 is one of the downstream proteins in nitric oxide pathway that play an important role in VSMC vasorelaxation and phenotype control by Ca2+ channel. Therefore, downregulation of PKG1 by miR-155 implicates the Ca2+ regulation in the maintenance of VSMC vasorelaxation. The miR-155 also has been shown to enhance neointima formation through the autocrine and paracrine effects of smooth muscle-like cell-derived RANTES and thus can be targeted for neointima inhibition.
4.3. Targeted Drugs in Clinical Setting to Suppress IH
Pharmacotherapy targeted at different steps of the pathogenesis of neointimal hyperplasia can be used to prevent and treat this condition, specifically to block SMCs migration and proliferation. Currently, there are two types of drugs eluting stents that have been used, everolimus-eluting stents (EES) and paclitaxel-eluting stents (PES). These drugs block SMC migration and proliferation.
In a previous study by Sanders and co-workers [57], the utilization of anti-inflammatory and anti-proliferative agents, mainly both rosiglitazone (ROS) and pioglitazone (PGZ), has a significant effect in decreasing inflammation and cell proliferation and being able to supply a longer drug delivery to the adjoining tissue. The glitazone drugs, primarily ROS and PGZ, possess anti-inflammatory effects, which were used to induce adipose tissue to produce the vascular protective protein such as adiponectin. Their aim was to characterize the efficacy of ROS or PGZ combined with fat in vitro and in vivo. They also evaluated the feasibility of fat integrated with PGZ storage in decreasing intimal hyperplasia development in animal model. This novel approach of utilizing anti-inflammatory agents could possibly be considered as an alternative therapy to suppress arterial stenosis caused by intimal hyperplasia [57].
4.4. Emerging Role of Chemokines and Cytokines Induction to Combat IH/Cardiovascular Disease
Previous studies have shown that the production of the pro-inflammatory cytokines and chemokines expedite the atherogenesis process by enhancing the secretion of adhesion molecules such as MCP-1 and fractalkine [66]. This finally will lead to early recruitment of both monocyte and lymphocyte in the intimal region [67]. The presence of these molecules thus acts as a biomarker of coronary artery injury [68]. In fact, these pro-inflammatory cytokines and chemokines have been regarded as predictors of chronic heart failure [69].
The efficacy of anti-inflammatory and pro-inflammatory chemokines and cytokines, as the initial prevention to cardiovascular disease, has been researched on. Kitagaki and colleague [70] demonstrated that tumour necrosis factor receptor 1 (TNFR1) antagonist treatment successfully alleviates the severity of inflammation in arteries, thus attenuating intimal hyperplasia in a mice model. TNFR1 is actively involved in arterial inflammation; however, the underlying mechanisms of this factor in inhibiting intimal hyperplasia is yet to be elucidated. This study offers a promising outcome, which suggests that the intraperitoneal injections of TNFR1 antagonist can alleviate the growth of smooth muscle cells and reduce arterial inflammation, by inhibiting nuclear factor kappa B (NF-κB). TNF-α is known to possess a pro-inflammatory property that actively participates in immunity. TNF-α might also play a major role in arterial inflammation, which contributes to intimal hyperplasia [71,72].
Inflammation response is one of the mechanisms of action by our body against detrimental things such as infections, toxins and injuries, as an attempt to heal itself. In this case, damaged endothelial layer especially during vascular intervention has caused the formation of intimal hyperplasia. In this event, pro-inflammatory factors such as TNF-α and MCP-1 are released. This is what most of the current studies focused on by inhibiting pro-inflammatory factors without considering the equilibrium with anti-inflammatory factors and the consequences of the inhibition. On the other hand, researchers could enhance the expression of anti-inflammatory factors or fine-tune both expressions dynamically, which may compensate with other physiological changes. Incorporating biomaterial as a scaffold, inner and outer vessel could also reduce the formation of intimal hyperplasia by inhibiting the VSMCs migration and aneurysm, respectively. Therefore, complete information needs to be gathered to have a bird’s-eye view for halting the intimal hyperplasia development.
Different approaches can be performed to suppress intimal hyperplasia and heal the damaged lining according to the sequences of the intimal hyperplasia progression. At the early stages of damaged endothelial lining, induction of MCP-1 could be used to attract more monocytes recruiting on the damaged area. Therefore, external/additional MCP-1 protein can be introduced for the recruitment. Other cytokines or chemokines such as fractalkine (CX3CL1) can also be used to enhance the recruitment process. Fractalkine plays a major role in binding to CX3CR1 rapidly and firmly, which may directly contribute to monocyte tethering and arrest. In the meantime, introduction of 7-O-methyl punctatin (MP) as discussed previously can be used to halt the VSMCs migration and proliferation to avoid intimal thickening during the recruitment process. Once recruited, another induction can be used to induce the recruited monocyte to differentiate into macrophages and later differentiate into endothelial-like cells. Induction factors such as GM-CSF, VEGF and PDGF could be used to achieve the endothelial cell differentiation. While using the MCP-1, a pro-inflammatory factor, as a monocyte attraction, Ganoderma triterpenoids (GT) extracts could also be used as it has an anti-atherogenic effects in terminating inflammation in vein. GT could be used to buffer the reaction of MCP-1 in case it is overexpressed. Combination approaches like MCP-1, fractalkine, MP, differentiation factors and GT will eventually heal the damaged lining.
5. Conclusions
Intimal hyperplasia formation involves numerous cellular and molecular components. From this review, the utilisation of various factors effective in halting the formation of intimal hyperplasia, solely. However, their effectiveness as a whole has yet to be elucidated as researchers have only focused on single factors to combat this event. Combining different types of methods could possibly enhance the effectiveness of inhibition of intimal hyperplasia formation prior to being conducted in clinical trial. Despite the significant effects proven previously, there are several important aspects that shall be noted. Upon initiation of any inflammatory-associated research, the selection of cells, medium formulation, immunomodulatory agents and the subject used for proof-of-concept should be thoroughly discussed. These elements of selection are essential as they may influence the outcome of the study, which eventually could have a great impact on translating the scientific findings into medical therapies.
Author Contributions
Conceptualization, R.C.M., N.S., M.F.I., R.B.H.I., M.R.A.R. and M.D.Y.; methodology, N.S., M.F.I., M.D.Y.; software, N.S., M.D.Y.; validation, R.C.M., N.S., M.F.I. and M.D.Y.; formal analysis, R.C.M., N.S., M.F.I. and M.D.Y.; investigation, R.C.M., R.B.H.I., M.R.A.R. and M.D.Y.; resources, R.C.M., N.S., M.F.I. and M.D.Y.; data curation, R.C.M., N.S., M.F.I. and M.D.Y.; writing—original draft preparation, R.C.M., N.S., M.F.I. and M.D.Y.; writing—review and editing, R.C.M., N.S., R.B.H.I. and M.D.Y.; visualization, R.C.M., N.S., M.F.I. and M.D.Y.; supervision, R.B.H.I., M.R.A.R., N.S. and M.D.Y.; project administration, N.S., R.B.H.I., M.R.A.R. and M.D.Y.; funding acquisition, N.S., R.B.H.I., M.R.A.R. and M.D.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by an International Matching Fund (MyPAIR)-UK-MY Joint Partnership on Non-Communicable Diseases (NCD): NEWTON-MEDICAL RESEARCH COUNCIL 2020-1 (Grant code: NEWTON-MRC/2020/001).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Clark, H. NCDs: A challenge to sustainable human development. Lancet 2013, 381, 510–511. [Google Scholar] [CrossRef]
- Kim, H.; Kim, S.; Han, S.; Rane, P.P.; Fox, K.M.; Qian, Y.; Suh, H.S. Prevalence and incidence of atherosclerotic cardiovascular disease and its risk factors in Korea: A nationwide population-based study. BMC Public Health 2019, 19, 1112. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Zhang, S.; Wu, J.; Wu, S.; Xu, G.; Wei, D. Essential role of nonessential amino acid glutamine in atherosclerotic cardiovascular disease. DNA Cell Biol. 2020, 39, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Shioi, A.; Ikari, Y. Plaque calcification during atherosclerosis progression and regression. J. Atheroscler. Thromb. 2018, 25, 294–303. [Google Scholar] [CrossRef]
- Kumar, S.; Chen, M.; Li, Y.; Wong, F.H.; Thiam, C.W.; Hossain, M.Z.; Poh, K.K.; Hirohata, S.; Ogawa, H.; Angeli, V.; et al. Loss of ADAMTS4 reduces high fat diet-induced atherosclerosis and enhances plaque stability in ApoE-/- mice. Sci. Rep. 2016, 6, 31130. [Google Scholar] [CrossRef]
- Rajamani, K.; Fisher, M. An overview of atherosclerosis. Prim. Cerebrovasc. Dis. Second Ed. 2017, 105–108. [Google Scholar] [CrossRef]
- Warboys, C.M.; Amini, N.; De Luca, A.; Evans, P.C. The role of blood flow in determining the sites of atherosclerotic plaques. F1000 Med. Rep. 2011, 3. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Annweiler, C.; Duval, G.; Karras, S.; Tirabassi, G.; Salvio, G.; Balercia, G.; Kimball, S.; Kotsa, K.; Mascitelli, L.; et al. Vitamin D and cardiovascular disease: From atherosclerosis to myocardial infarction and stroke. Int. J. Cardiol. 2017, 230, 577–584. [Google Scholar] [CrossRef]
- Best, P.J.M.; Lerman, A. Endothelin in cardiovascular disease: From atherosclerosis to heart failure. J. Cardiovasc. Pharmacol. 2000, 35, S61–S63. [Google Scholar] [CrossRef]
- Ross, R.; Agius, L. The process of atherogenesis—Cellular and molecular interaction: From experimental animal models to humans. Diabetologia 1992, 35, S34–S40. [Google Scholar] [CrossRef]
- Stary, H.C.; Chandler, A.B.; Glagov, S.; Guyton, J.R.; Insull, W., Jr.; Rosenfeld, M.E.; Schaffer, S.A.; Schwartz, C.J.; Wagner, W.D.; Wissler, R.W. A definition of initial, fatty streak, and intermediate lesions of atherosclerosis. Circulation 1994, 89, 2462–2478. [Google Scholar] [CrossRef] [PubMed]
- Tran, P.-K.; Tran-Lundmark, K.; Soininen, R.; Tryggvason, K.; Thyberg, J.; Hedin, U. Increased intimal hyperplasia and smooth muscle cell proliferation in transgenic mice with heparan sulfate–deficient perlecan. Circ. Res. 2004, 94, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Sigel, B.; Swami, V.; Can, A.; Parsons, R.E.; Golub, R.M.; Kolecki, R.; Kitamura, H. Intimal hyperplasia producing thrombus organization in an experimental venous thrombosis model. J. Vasc. Surg. 1994, 19, 350–360. [Google Scholar] [CrossRef]
- Gupta, G.K.; Agrawal, T.; Rai, V.; Del Core, M.G.; Hunter, W.J.; Agrawal, D.K. Vitamin D supplementation reduces intimal hyperplasia and restenosis following coronary intervention in atherosclerotic swine. PLoS ONE 2016, 11, e0156857. [Google Scholar] [CrossRef] [PubMed]
- Casscells, W. Migration of smooth muscle and endothelial cells: Critical events in restenosis. Circulation 1992, 86, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Louis, S.F.; Zahradka, P. Vascular smooth muscle cell motility: From migration to invasion. Exp. Clin. Cardiol. 2010, 15, e75–e85. [Google Scholar] [PubMed]
- Jennette, J.C.; Stone, J.R. Diseases of medium-sized and small vessels. In Cellular and Molecular Pathobiology of Cardiovascular Disease; Elsevier: Amsterdam, The Netherlands, 2014; pp. 197–219. [Google Scholar] [CrossRef]
- Ducasse, E.; Cosset, J.M.; Eschwège, F.; Chevalier, J.; De Ravignan, D.; Puppinck, P.; Lartigau, E. Hyperplasia of the arterial intima due to smooth muscle cell proliferation. Current data, experimental treatments and perspectives. J. Mal. Vasc. 2003, 28, 130–144. [Google Scholar] [PubMed]
- Zalewski, A.; Shi, Y.; Johnson, A.G. Diverse origin of intimal cells. Circ. Res. 2002, 91, 652–655. [Google Scholar] [CrossRef]
- Patel, S.; Waltham, M.; Wadoodi, A.; Burnand, K.; Smith, A. The role of endothelial cells and their progenitors in intimal hyperplasia. Ther. Adv. Cardiovasc. Dis. 2010, 4, 129–141. [Google Scholar] [CrossRef]
- Tsai, S.; Butler, J.; Rafii, S.; Liu, B.; Kent, K.C. The role of progenitor cells in the development of intimal hyperplasia. J. Vasc. Surg. 2009, 49, 502–510. [Google Scholar] [CrossRef]
- Xu, K.; Al-Ani, M.K.; Pan, X.; Chi, Q.; Dong, N.; Qiu, X. Plant-derived products for treatment of vascular intima hyperplasia selectively inhibit vascular smooth muscle cell functions. Evidence-Based Complement. Altern. Med. 2018, 2018, 1–17. [Google Scholar] [CrossRef]
- Lemson, M.; Tordoir, J.; Daemen, M.; Kitslaar, P. Intimal hyperplasia in vascular grafts. Eur. J. Vasc. Endovasc. Surg. 2000, 19, 336–350. [Google Scholar] [CrossRef]
- Zubilewicz, T.; Wronski, J.; Bourriez, A.; Terlecki, P.; Guinault, A.M.; Muscatelli-Groux, B.; Michalak, J.; Méllière, D.; Becquemin, J.; Allaire, E. Injury in vascular surgery-the intimal hyperplastic response. Med. Sci. Monit. 2001, 7, 316–324. [Google Scholar]
- Gellman, J.; Ezekowitz, M.D.; Sarembock, I.J.; Azrin, M.A.; Nochomowitz, L.E.; Lerner, E.; Haudenschild, C.C. Effect of lovastatin on intimal hyperplasia after balloon angioplasty: A study in an atherosclerotic hypercholesterolemic rabbit. J. Am. Coll. Cardiol. 1991, 17, 251–259. [Google Scholar] [CrossRef][Green Version]
- Carrozza, J.P.; Kuntz, R.E.; Fishman, R.F.; Baim, D.S. Restenosis after arterial injury caused by coronary stenting in patients with diabetes mellitus. Ann. Intern. Med. 1993, 118, 344–349. [Google Scholar] [CrossRef]
- Salam, T.A.; Taylor, B.; Suggs, W.D.; Hanson, S.R.; Lumsden, A.B. Reaction to injury following balloon angioplasty and intravascular stent placement in the canine femoral artery. Am. Surg. 1994, 60, 353–357. [Google Scholar] [PubMed]
- Kornowski, R.; Hong, M.K.; Tio, F.O.; Bramwell, O.; Wu, H.; Leon, M.B. In-stent restenosis: Contributions of inflammatory responses and arterial injury to neointimal hyperplasia. J. Am. Coll. Cardiol. 1998, 31, 224–230. [Google Scholar] [CrossRef]
- Lacolley, P.; Regnault, V.; Avolio, A.P. Smooth muscle cell and arterial aging: Basic and clinical aspects. Cardiovasc. Res. 2018, 114, 513–528. [Google Scholar] [CrossRef] [PubMed]
- Miyakoshi, A.; Hatano, T.; Tsukahara, T.; Murakami, M.; Arai, D.; Yamaguchi, S. Percutaneous transluminal angioplasty for atherosclerotic stenosis of the subclavian or innominate artery: Angiographic and clinical outcomes in 36 patients. Neurosurg. Rev. 2011, 35, 121–126. [Google Scholar] [CrossRef]
- Cooper, C.J.; Murphy, T.P.; Cutlip, D.E.; Jamerson, K.; Henrich, W.; Reid, D.M.; Cohen, D.J.; Matsumoto, A.H.; Steffes, M.; Jaff, M.R.; et al. Stenting and medical therapy for atherosclerotic renal-artery stenosis. N. Engl. J. Med. 2014, 370, 13–22. [Google Scholar] [CrossRef]
- Higo, T.; Ueda, Y.; Oyabu, J.; Okada, K.; Nishio, M.; Hirata, A.; Kashiwase, K.; Ogasawara, N.; Hirotani, S.; Kodama, K. Atherosclerotic and thrombogenic neointima formed over sirolimus drug-eluting stent. JACC Cardiovasc. Imaging 2009, 2, 616–624. [Google Scholar] [CrossRef] [PubMed]
- Mackensen, G.; Swaminathan, M.; Ti, L.K.; Grocott, H.P.; Phillips-Bute, B.G.; Mathew, J.P.; Newman, M.F.; Milano, C.A.; Stafford-Smith, M. Preliminary report on the interaction of apolipoprotein E polymorphism with aortic atherosclerosis and acute nephropathy after CABG. Ann. Thorac. Surg. 2004, 78, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Osgood, M.J.; Hocking, K.M.; Voskresensky, I.V.; Li, F.D.; Komalavilas, P.; Cheung-Flynn, J.; Brophy, C.M. Surgical vein graft preparation promotes cellular dysfunction, oxidative stress, and intimal hyperplasia in human saphenous vein. J. Vasc. Surg. 2013, 60, 202–211. [Google Scholar] [CrossRef] [PubMed]
- Hellings, W.E.; Moll, F.L.; De Vries, J.P.P.; Ackerstaff, R.G.; Seldenrijk, K.A.; Met, R.; Velema, E.; Derksen, W.J.; De Kleijn, D.P.; Pasterkamp, G. Atherosclerotic plaque composition and occurrence of restenosis after carotid endarterectomy. JAMA J. Am. Med. Assoc. 2008, 299, 547–554. [Google Scholar] [CrossRef]
- Liu, M.W.; Roubin, G.S.; King, S.B. Restenosis after coronary angioplasty. Potential biologic determinants and role of intimal hyperplasia. Circulation 1989, 79, 1374–1387. [Google Scholar] [CrossRef]
- Rosenfield, K.; Schainfeld, R.; Pieczek, A.; Haley, L.; Isner, J.M. Restenosis of endovascular stents from stent compression. J. Am. Coll. Cardiol. 1997, 29, 328–338. [Google Scholar] [CrossRef]
- Charo, I.F.; Taubman, M.B. Chemokines in the pathogenesis of vascular disease. Circ. Res. 2004, 95, 858–866. [Google Scholar] [CrossRef]
- Gu, L.; Tseng, S.C.; Rollins, B.J. Monocyte chemoattractant protein-1. Chem. Immunol. 1999, 72, 7–29. [Google Scholar] [CrossRef]
- Roque, M.; Kim, W.J.; Gazdoin, M.; Malik, A.; Reis, E.D.; Fallon, J.T.; Badimon, J.J.; Charo, I.F.; Taubman, M.B. CCR2 deficiency decreases intimal hyperplasia after arterial injury. Arter. Thromb. Vasc. Biol. 2002, 22, 554–559. [Google Scholar] [CrossRef]
- Furukawa, Y.; Matsumori, A.; Ohashi, N.; Shioi, T.; Ono, K.; Harada, A.; Matsushima, K.; Sasayama, S. Anti-monocyte chemoattractant protein-1/monocyte chemotactic and activating factor antibody inhibits neointimal hyperplasia in injured rat carotid arteries. Circ. Res. 1999, 84, 306–314. [Google Scholar] [CrossRef]
- Idriss, H.T.; Naismith, J.H. TNFα and the TNF receptor superfamily: Structure-function relationship(s). Microsc. Res. Tech. 2000, 50, 184–195. [Google Scholar] [CrossRef]
- Shaw, J.; Tang, Z.; Schneider, H.; Saljé, K.; Hansson, S.R.; Guller, S. Inflammatory processes are specifically enhanced in endothelial cells by placental-derived TNF-α: Implications in preeclampsia (PE). Placenta 2016, 43, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Brand, K.; Page, S.; Rogler, G.; Barstch, A.; Brandl, R.; Knuechel, R.; Page, M.; Kaltschmidt, C.; Baeuerle, P.A.; Neumeier, D. Activated transcription factor nuclear factor-kappa B is present in the atherosclerotic lesion. J. Clin. Investig. 1996, 97. [Google Scholar] [CrossRef] [PubMed]
- Maleknia, M.; Ansari, N.; Haybar, H.; Maniati, M.; Saki, N. Inflammatory growth factors and in-stent restenosis: Effect of cytokines and growth factors. SN Compr. Clin. Med. 2020, 2, 397–407. [Google Scholar] [CrossRef]
- Deshmane, S.L.; Kremlev, S.; Amini, S.; Sawaya, B.E. Monocyte chemoattractant protein-1 (MCP-1): An overview. J. Interf. Cytokine Res. 2009, 29, 313–326. [Google Scholar] [CrossRef]
- Li, B.; Pozzi, A.; Young, P.P. TNFα accelerates monocyte to endothelial transdifferentiation in tumors by the induction of integrin α5 expression and adhesion to fibronectin. Mol. Cancer Res. 2011, 9, 702–711. [Google Scholar] [CrossRef]
- Ko, I.K.; Lee, S.J.; Atala, A.; Yoo, J.J. In situ tissue regeneration through host stem cell recruitment. Exp. Mol. Med. 2013, 45, e57. [Google Scholar] [CrossRef]
- Choi, S.; Park, M.; Kim, J.; Park, W.; Kim, S.; Lee, D.-K.; Hwang, J.Y.; Choe, J.; Won, M.-H.; Ryoo, S.; et al. TNF-α elicits phenotypic and functional alterations of vascular smooth muscle cells by miR-155-5p–dependent down-regulation of cGMP-dependent kinase 1. J. Biol. Chem. 2018, 293, 14812–14822. [Google Scholar] [CrossRef]
- Fardoun, M.; Iratni, R.; Dehaini, H.; Eeid, A.; Ghaddar, T.; El-Elimat, T.; Alali, F.; Badran, A.; Eid, A.H.; Baydoun, E.; et al. 7-O-methylpunctatin, a novel homoisoflavonoid, inhibits phenotypic switch of human arteriolar smooth muscle cells. Biomolecules 2019, 9, 716. [Google Scholar] [CrossRef]
- Kenagy, R.D.; Civelek, M.; Kikuchi, S.; Chen, L.; Grieff, A.; Sobel, M.; Lusis, A.J.; Clowes, A.W. Scavenger receptor class A member 5 (SCARA5) and suprabasin (SBSN) are hub genes of coexpression network modules associated with peripheral vein graft patency. J. Vasc. Surg. 2016, 64, 202–209.e6. [Google Scholar] [CrossRef]
- Sun, H.; Zhu, X.; Cai, W.; Qiu, L.Y. Hypaphorine attenuates lipopolysaccharide-induced endothelial inflammation via regulation of TLR4 and PPAR-γ dependent on PI3K/Akt/mTOR signal pathway. Int. J. Mol. Sci. 2017, 18, 844. [Google Scholar] [CrossRef]
- De Jong, R.C.M.; Ewing, M.M.; De Vries, M.R.; Karper, J.C.; Bastiaansen, A.J.N.M.; Peters, H.A.B.; Baghana, F.; Elsen, P.J.V.D.; Gongora, C.; Jukema, J.W.; et al. The epigenetic factor PCAF regulates vascular inflammation and is essential for intimal hyperplasia development. PLoS ONE 2017, 12, e0185820. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Chai, S.; Dai, L.; Gu, C. Collagen external scaffolds mitigate intimal hyperplasia and improve remodeling of vein grafts in a rabbit arteriovenous graft model. Biomed Res. Int. 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Hsu, P.L.; Lin, Y.C.; Ni, H.; Mo, F.E. Ganoderma triterpenoids exert antiatherogenic effects in mice by alleviating disturbed flow-induced oxidative stress and inflammation. Oxidative Med. Cell. Longev. 2018, 2018, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Pang, D.; Yuan, T.; Li, Z.; Li, Z.; Zhang, M.; Ren, W.; Ouyang, H.; Tang, X. N-3 polyunsaturated fatty acids attenuates triglyceride and inflammatory factors level in hfat-1 transgenic pigs. Lipids Health Dis. 2016, 15, 89. [Google Scholar] [CrossRef]
- Sanders, W.G.; Li, H.; Zhuplatov, I.; He, Y.; Kim, S.E.; Cheung, A.K.; Agarwal, J.; Terry, C.M. Autologous fat transplants to deliver glitazone and adiponectin for vasculoprotection. J. Control. Release 2017, 264, 237–246. [Google Scholar] [CrossRef]
- Schlosser, A.; Pilecki, B.; Hemstra, L.E.; Kejling, K.; Kristmannsdottir, G.B.; Wulf-Johansson, H.; Moeller, J.B.; Füchtbauer, E.M.; Nielsen, O.; Kirketerp-Møller, K.; et al. MFAP4 promotes vascular smooth muscle migration, proliferation and accelerates neointima formation. Arterioscler. Thromb. Vasc. Biol. 2016, 36. [Google Scholar] [CrossRef]
- Wang, K.; Deng, P.; Sun, Y.; Ye, P.; Zhang, A.; Wu, C.; Yue, Z.; Chen, Z.; Xia, J. MicroRNA-155 promotes neointimal hyperplasia through smooth muscle-like cell-derived RANTES in arteriovenous fistulas. J. Vasc. Surg. 2018, 67. [Google Scholar] [CrossRef]
- Yang, B.; Brahmbhatt, A.; Torres, E.N.; Thielen, B.; McCall, D.L.; Engel, S.; Bansal, A.; Pandey, M.K.; Dietz, A.B.; Leof, E.B.; et al. Tracking and therapeutic value of human adipose tissue-derived mesenchymal stem cell transplantation in reducing venous neointimal hyperplasia associated with arteriovenous fistula. Radiology 2016, 279. [Google Scholar] [CrossRef]
- Moreira, D.M.; da Silva, R.L.; Vieira, J.L.; Fattah, T.; Lueneberg, M.E.; Gottschall, C.A.M. Role of vascular inflammation in coronary artery disease: Potential of anti-inflammatory drugs in the prevention of atherothrombosis: Inflammation and anti-inflammatory drugs in coronary artery disease. Am. J. Cardiovasc. Drugs 2015, 15, 1–11. [Google Scholar] [CrossRef]
- Christodoulidis, G.; Vittorio, T.J.; Fudim, M.; Lerakis, S.; Kosmas, C.E. Inflammation in coronary artery disease. Cardiol. Rev. 2014, 22, 279–288. [Google Scholar] [CrossRef]
- Kosmas, C.E.; Silverio, D.; Tsomidou, C.; Salcedo, M.D.; Montan, P.D.; Guzman, E. The impact of insulin resistance and chronic kidney disease on inflammation and cardiovascular disease. Clin. Med. Insights Endocrinol. Diabetes 2018, 11. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.L.; Yeh, J.L.; Tsai, P.C.; Chang, T.H.; Huang, W.C.; Lee, S.T.; Wassler, M.; Geng, Y.J.; Sulistyowati, E. Inhibition of neointima hyperplasia, inflammation, and reactive oxygen species in balloon-injured arteries by HVJ envelope vector-mediated delivery of superoxide dismutase gene. Transl. Stroke Res. 2018, 10, 413–427. [Google Scholar] [CrossRef]
- Sotokawauchi, A.; Ishibashi, Y.; Matsui, T.; Yamagishi, S.I. Aqueous extract of glucoraphanin-rich broccoli sprouts inhibits formation of advanced glycation end products and attenuates inflammatory reactions in endothelial cells. Evidence-Based Complement. Altern. Med. 2018, 2018, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Galkina, E.V.; Ley, K. Immune and inflammatory mechanisms of atherosclerosis. Ann. Rev. Immunol. 2009, 27, 165–197. [Google Scholar] [CrossRef] [PubMed]
- Tedgui, A.; Mallat, Z. Cytokines in atherosclerosis: Pathogenic and regulatory pathways. Physiol. Rev. 2006, 86, 515–581. [Google Scholar] [CrossRef]
- Bucova, M.; Bernadic, M.; Buckingham, T. C-reactive protein, cytokines and inflammation in cardiovascular diseases. Bratisl Lek List. 2008, 109, 333–340. [Google Scholar]
- Liu, M.; Chen, J.; Huang, D.; Ke, J.; Wu, W. A meta-analysis of proinflammatory cytokines in chronic heart failure. Hear. Asia 2014, 6, 130–136. [Google Scholar] [CrossRef]
- Kitagaki, M.; Isoda, K.; Kamada, H.; Kobayashi, T.; Tsunoda, S.; Tsutsumi, Y.; Niida, T.; Kujiraoka, T. Inflammatory reactions in the pathogenesis of atherosclerosis inflammation and intimal hyperplasia in Mice. J. Atheroscler. Thromb. 2012, 19, 36–46. [Google Scholar] [CrossRef]
- Wajant, H.; Pfizenmaier, K.; Scheurich, P. Tumor necrosis factor signaling. Cell Death Differ. 2003, 10, 45–65. [Google Scholar] [CrossRef]
- Fan, J.; Watanabe, T. Inflammatory reactions in the pathogenesis of atherosclerosis. J. Atheroscler. Thromb. 2003, 10, 63–71. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).