Promoting Factors for Physical Activity in Children with Asthma Explored through Concept Mapping

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Recruitment
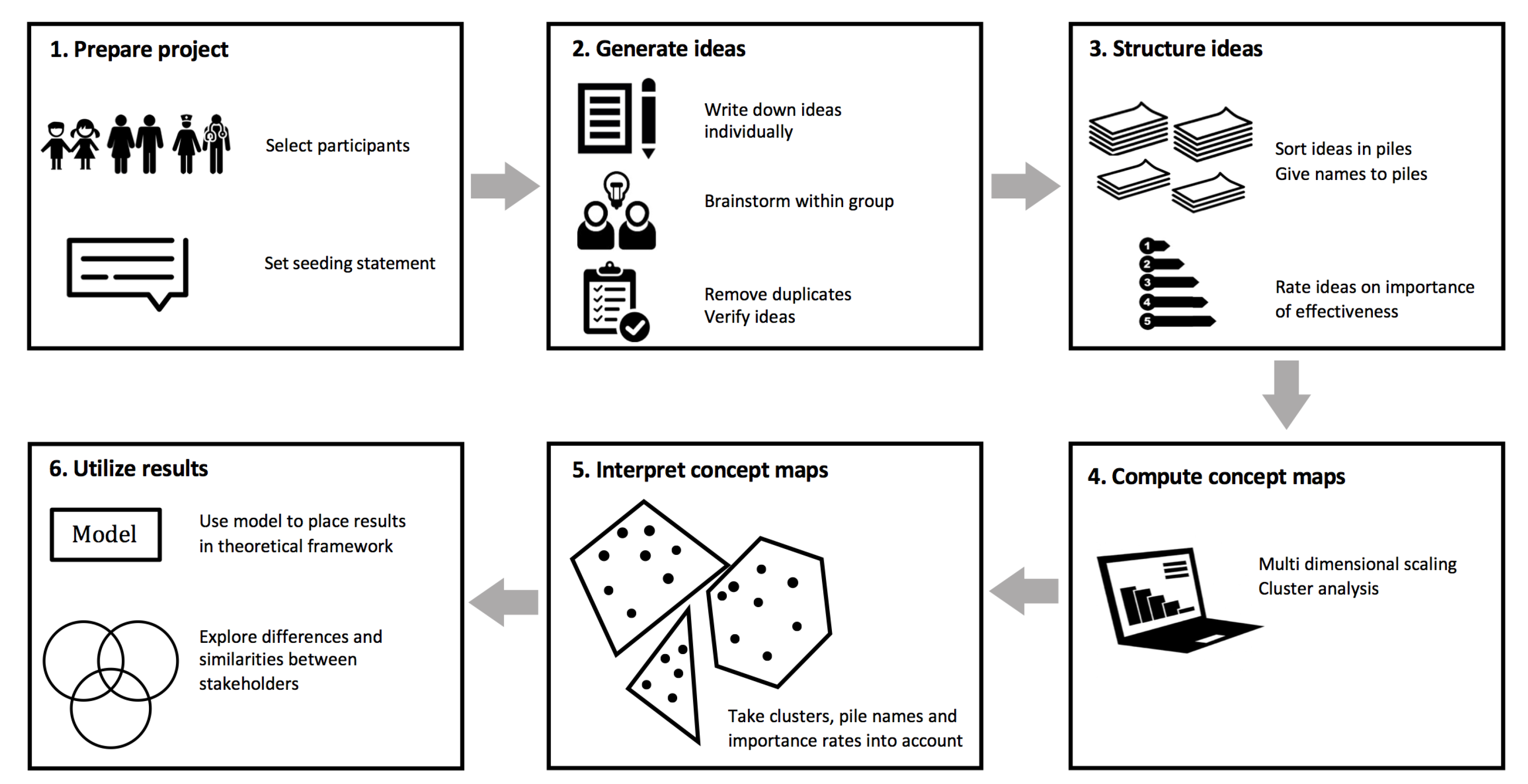
2.2. Procedures
2.2.1. Concept Mapping Sessions with Children and Parents
2.2.2. Concept Mapping Sessions with Healthcare Providers
2.2.3. Generating the Concept Maps
2.2.4. Interpreting the Concept Maps
3. Results
3.1. Participant Characteristics
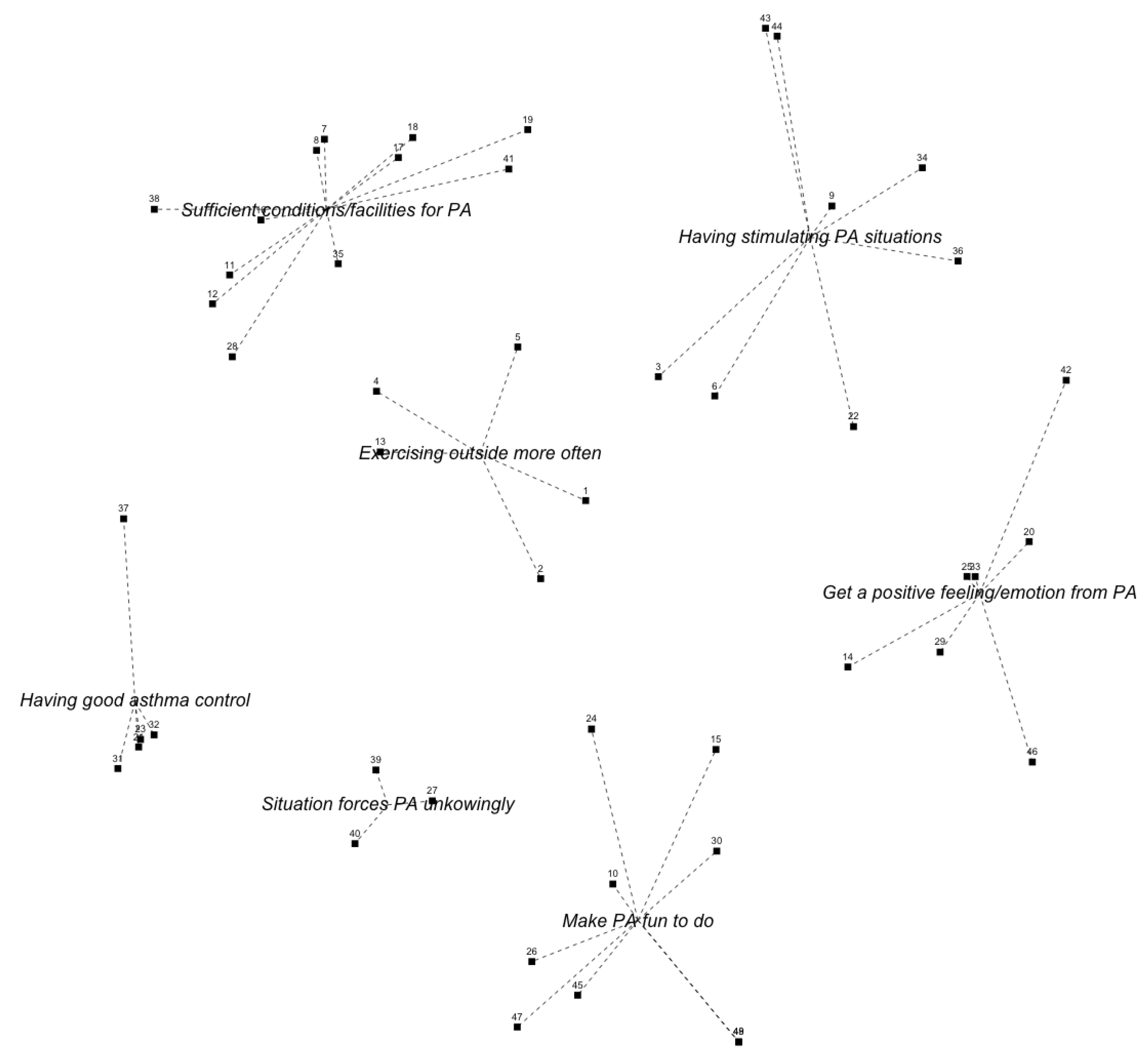
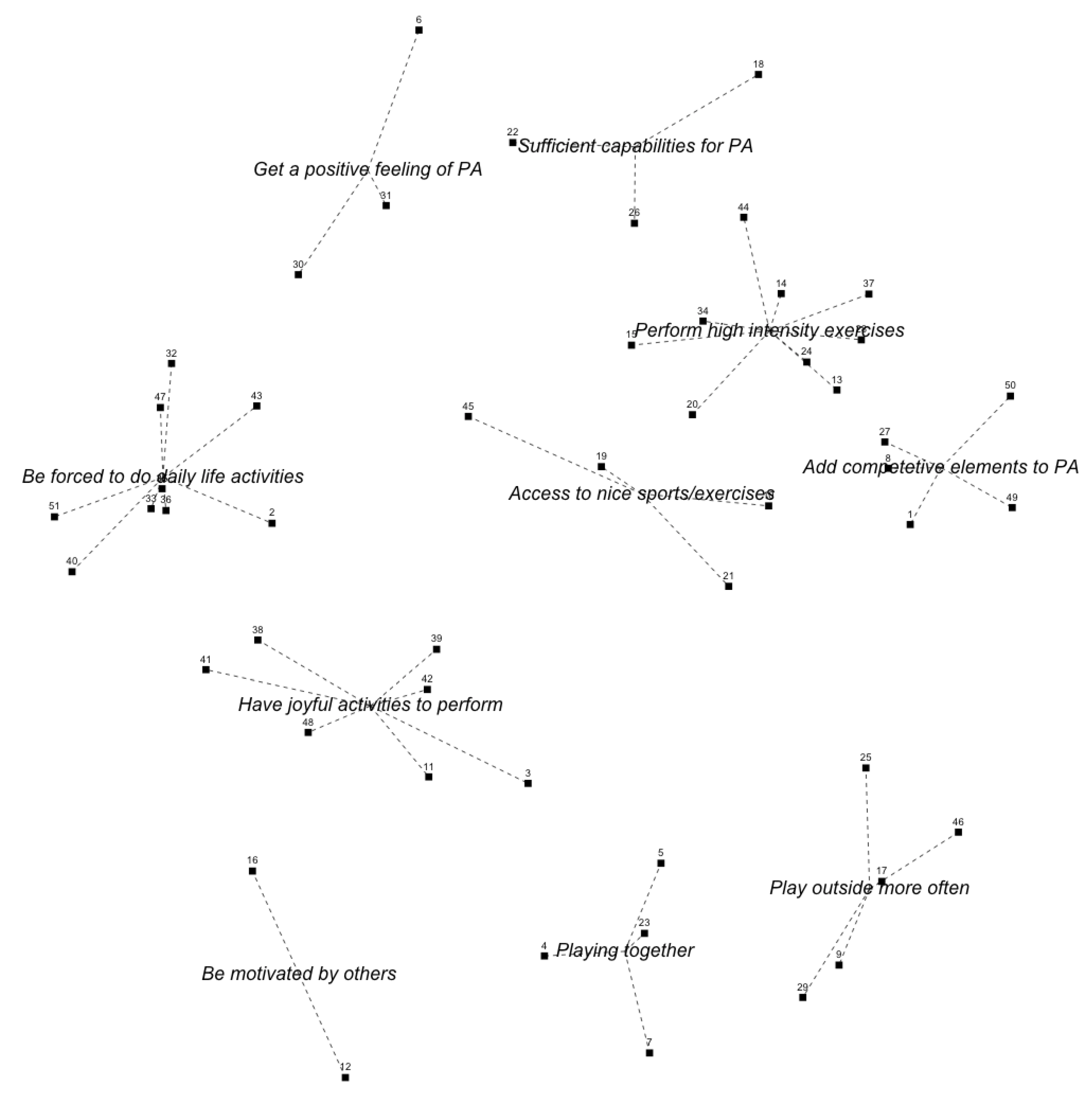
3.2. Children’s Clusters
3.3. Parents’ Clusters
3.4. Healthcare Providers’ Clusters
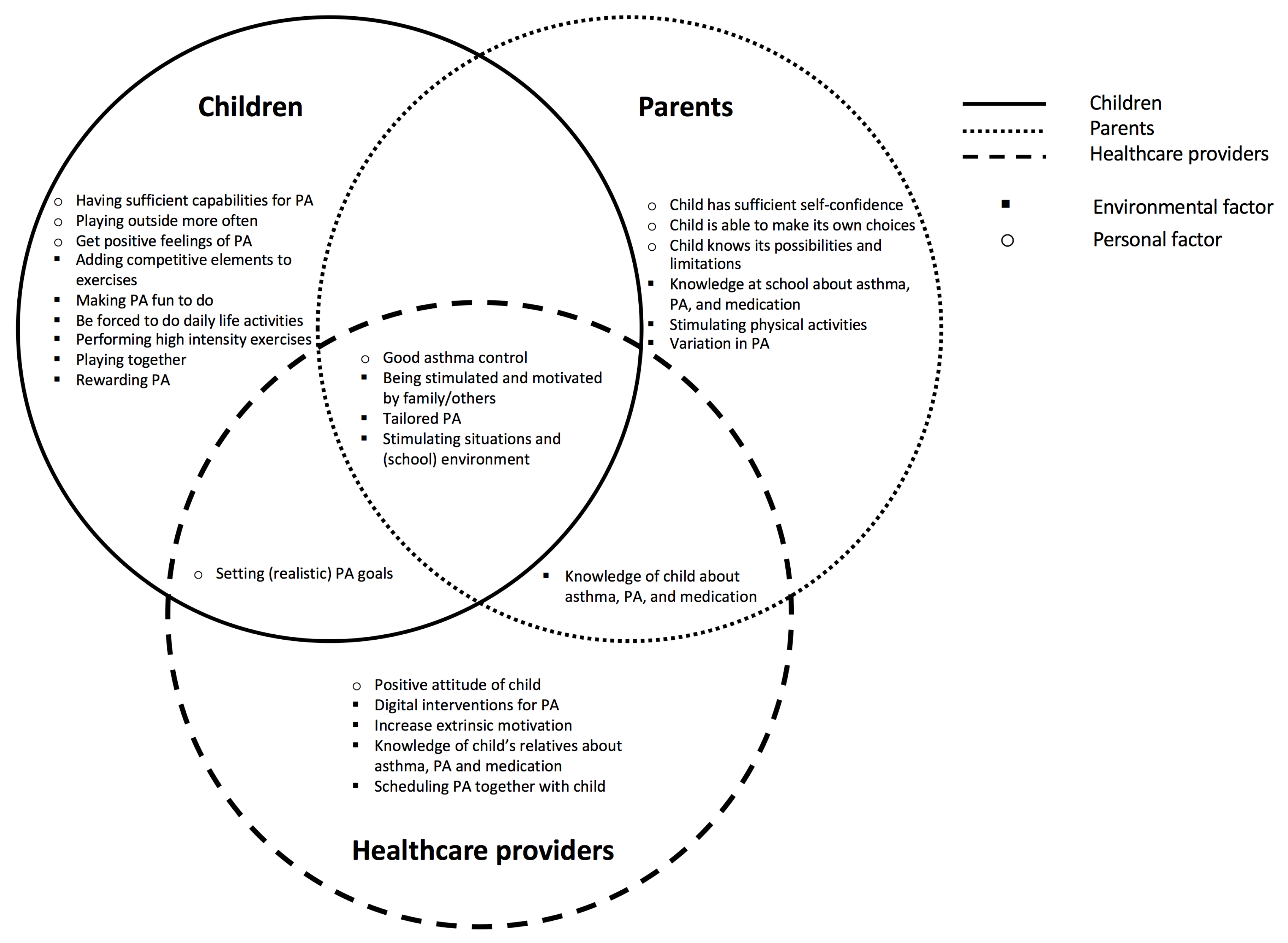
3.5. Combined Results of All Stakeholder Groups
4. Discussion
4.1. Principal Results
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CM | Concept Mapping |
| MSD | Multi Dimensional Scaling |
| PA | Physical Activity |
| PAD | Physical Activity for people with a Disability |
| SD | Standard Deviation |
Appendix A. Final Concept Maps and Ideas of All Groups
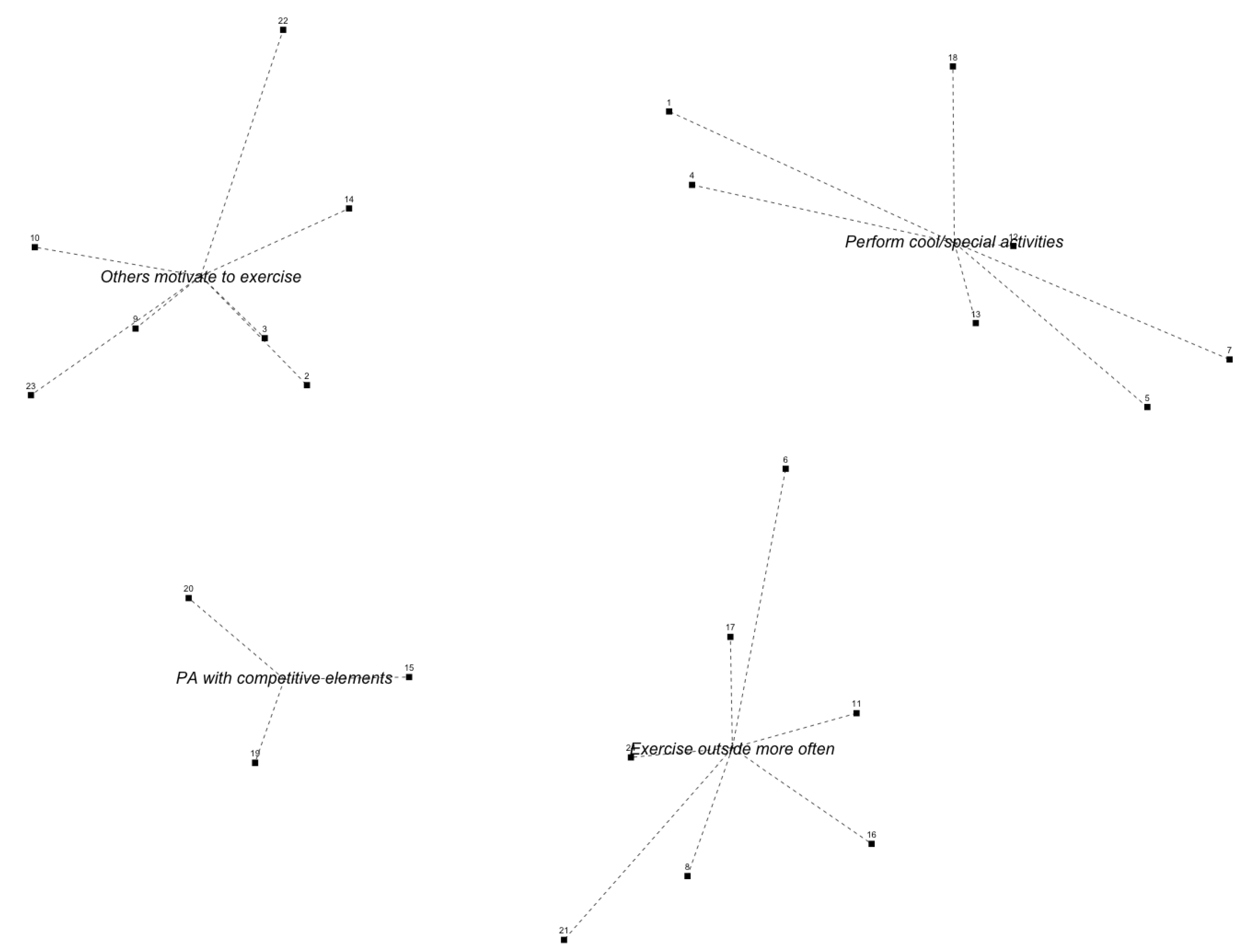
Appendix A.1. Children Group 1


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Be forced to do daily life activities | Have joyful activities to perform | |||||
| 2 | If I would drink and eat a lot | 2.56 ± 1.01 | 3 | When you do something you like | 4.33 ± 0.87 | |
| 32 | If I can walk somewhere | 2.56 ± 1.59 | 11 | When you like something | 4.11 ± 1.36 | |
| 43 | If I would think | 2.00 ± 1.41 | 48 | If you would hear a sound that supports you to move more | 2.89 ± 1.45 | |
| 40 | If I had to inflate the tires of my bike | 1.89 ± 1.05 | 42 | If I would play with construction materials | 2.78 ± 1.09 | |
| 33 | If I would get up from the chair | 1.22 ± 0.44 | 38 | If I could demolish things | 2.56 ± 1.01 | |
| 51 | If I would walk to the bathroom | 1.22 ± 0.44 | 41 | If I would talk about exercising | 2.11 ± 0.78 | |
| 36 | If I would turn on a light | 1.11 ± 0.33 | 39 | If I can sing | 1.78 ± 1.3 | |
| 35 | If I would fall | 1.00 ± 0.00 | Sufficient capabilities for PA | |||
| 47 | If I would get something to drink | 1.00 ± 0.00 | 26 | If I would take my inhalation medication | 3.78 ± 1.48 | |
| Playing outside more often | 22 | If I have self-confidence | 3.56 ± 1.48 | |||
| 9 | If you make a game of it | 3.56 ± 0.88 | 18 | If you receive certificates or medals | 3.44 ± 1.51 | |
| 17 | If I can pay outside a lot | 2.14 ± 1.46 | Be motivated by others | |||
| 25 | If I can swing | 2.11 ± 0.60 | 12 | If you get support from your parents and friends | 4.11 ± 1.05 | |
| 46 | If I would play “man overboard” | 1.54 ± 1.00 | 16 | If I look at others to see how they are doing it | 3.33 ± 1.12 | |
| 29 | If I would play “Pokemon Go” | 2.00 ± 1.05 | Get a positive feeling of PA | |||
| Have access to nice sports and exercises | 30 | If I stay healthy after being active | 4.33 ± 0.71 | |||
| 10 | If you could do sports that you enjoy | 4.44 ± 0.73 | 6 | If I would receive points and I would be rewarded for being active is | 3.89 ± 0.93 | |
| 45 | If your whole body starts to move | 4.00 ± 1.32 | 31 | If I would be brave enough to do so | 3.44 ± 1.33 | |
| 19 | If you can dance | 3.25 ± 1.58 | Playing together | |||
| 21 | If you can go skiing | 2.89 ± 1.05 | 4 | If I do it together with my parents | 4.22 ± 0.67 | |
| Perform high intensity exercises | 5 | If I go to “Jumping Jack” with my friends | 3.67 ± 1.22 | |||
| 14 | If you can play sports | 4.33 ± 1.00 | 7 | If I am together with my friends | 3.57 ± 1.40 | |
| 34 | If I would have gym classes at school more often | 3.78 ± 0.67 | 23 | If I can play with my friend | 3.50 ± 0.76 | |
| 15 | If I can run | 3.56 ± 0.88 | Add competitive elements to PA | |||
| 37 | If I would combine different types of sports | 3.56 ± 0.88 | 8 | If I would swim | 4.11 ± 0.93 | |
| 20 | If I can bike | 3.11 ± 1.45 | 27 | If I could swim at a competition | 3.00 ± 1.22 | |
| 28 | If I can play water polo | 2.67 ± 1.50 | 1 | If I can kick a ball | 2.67 ± 1.22 | |
| 44 | If I would not sport too much | 2.44 ± 1.01 | 50 | If I can play soccer outside | 2.67 ± 1.80 | |
| 24 | If I can do freerunning | 2.25 ± 1.04 | 49 | If I can play “curbs” | 1.89 ± 1.05 | |
| 13 | If I can be the goalkeeper | 2.22 ± 1.20 | ||||
Appendix A.2. Children Group 3

| Being motivated by others to exercise | Play outside more often | |||||
| 22 | When there would be more gym classes at school | 4.00 ± 1.15 | 8 | If you would play active outdoor games | 3.86 ± 1.46 | |
| 23 | If you receive an reward when you are active | 3.29 ± 1.50 | 6 | If children with asthma would always use a bike to go somewhere | 3.57 ± 1.51 | |
| 9 | If someone motivates a child to win | 2.86 ± 1.86 | 21 | If there were nice walking routes for children | 3.29 ± 1.11 | |
| 3 | If children with asthma still try to do something that they are excited about | 2.71 ± 1.11 | 11 | If a child with asthma would play in an indoor playground | 3.14 ± 1.35 | |
| 14 | If there is a build-up training schedule | 2.71 ± 1.38 | 24 | If the weather would be better more often | 3.00 ± 1.15 | |
| 10 | If children with asthma are paying attention to what they do and whether they can sustain it | 2.14 ± 1.07 | 17 | If scouting activities are offered more often by scouting clubs | 2.86 ± 1.21 | |
| 2 | Prove that you can do so in case others think that you cannot | 2.00 ± 1.26 | 16 | If you can play a nice outdoor game with your friends | 2.43 ± 1.51 | |
| Perform cool and special activities | Add competitive elements to PA | |||||
| 12 | If a child with asthma would go “disco swimming” | 4.00 ± 1.00 | 15 | If you would talk with other children more often | 2.57 ± 1.51 | |
| 5 | If a child with asthma would play Just Dance more often | 3.43 ± 1.13 | 20 | If you need to reach a specific distance in a specific time frame | 2.43 ± 1.13 | |
| 7 | When you create a game with a motion sensor | 3.43 ± 1.40 | 19 | If you occasionally have to run to school | 2.29 ± 1.25 | |
| 13 | If a child would go to a “trampoline park” | 3.43 ± 1.51 | ||||
| 18 | If you would perform dancing at a dance centre | 2.67 ± 1.37 | ||||
| 1 | If a child with asthma would jump rope more often | 2.43 ± 0.98 | ||||
| 4 | If a child with asthma would skydive more often | 2.43 ± 1.51 | ||||
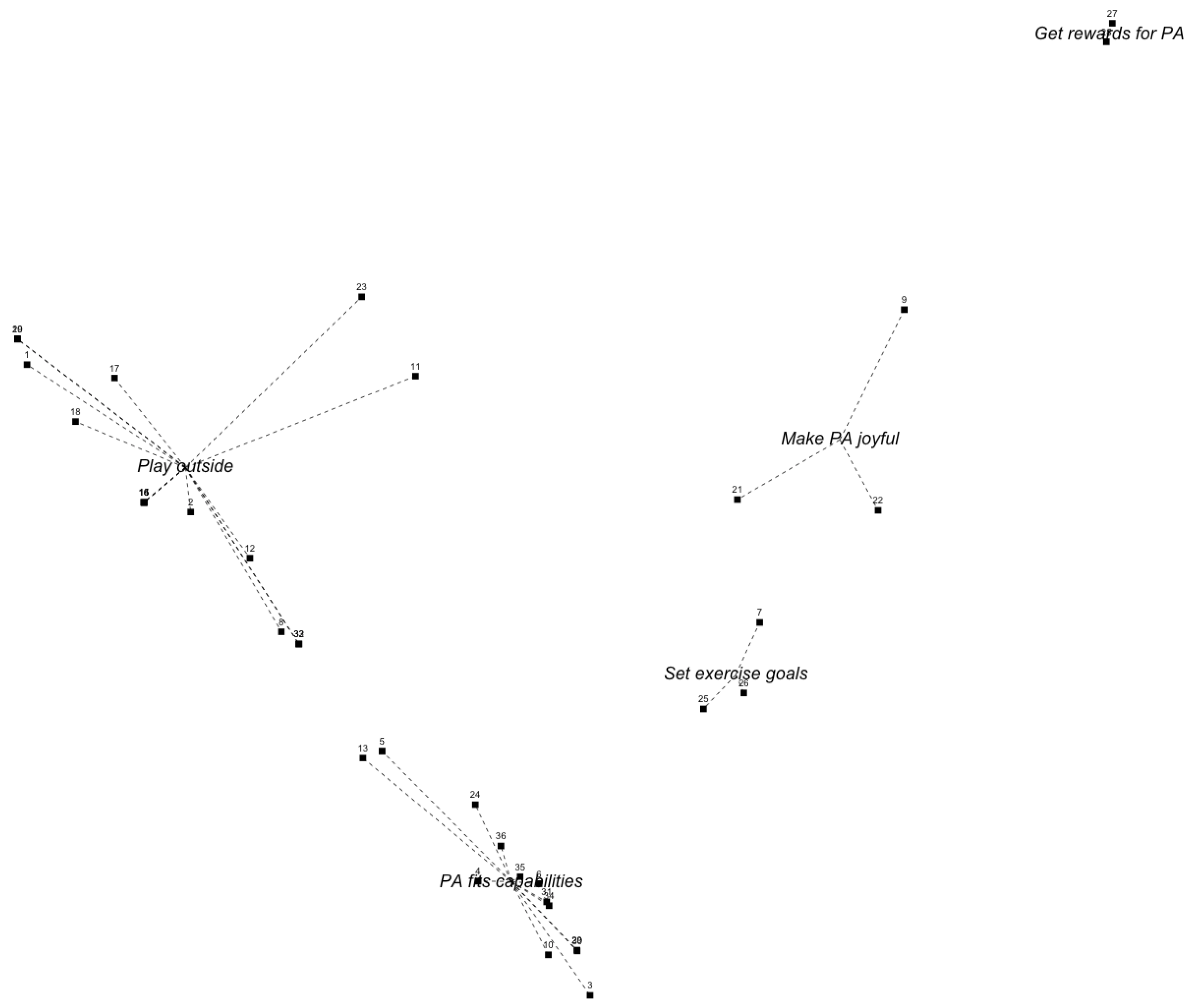
Appendix A.3. Children Group 4

| Set exercise goals | Make exercises joyful | |||||
| 25 | If a child with asthma has an activity goal | 3.40 ± 1.34 | 22 | If there were film clips for children with asthma with “weird” movements to imitate | 4.00 ± 1.73 | |
| 26 | If you choose an activity that you can do well in order to win | 3.20 ± 1.79 | 9 | If the activity is being rewarded with something nice | 3.60 ± 0.55 | |
| 7 | If children with asthma would dance in order to deal with their emotions | 2.20 ± 1.64 | 21 | If a child with asthma would do “The Netherlands in motion” with their grandmother | 3.40 ± 1.82 | |
| Get rewards for doing exercises or PA | Play outside more often | |||||
| 28 | If children receive rewards for working hard | 4.20 ± 0.45 | 32 | If we play “trefbal” more often in gym classes at school so that you are very active | 4.60 ± 0.55 | |
| 27 | If children will feel happy after doing working hard | 3.60 ± 1.14 | 8 | If gym classes are fun and challenging so that you can always actively participate | 4.40 ± 0.89 | |
| Tailored PA | 17 | If a child with asthma would more often go to school by bike | 4.20 ± 0.84 | |||
| 30 | If children with asthma would distribute their energy during sports activities in order to sustain | 4.60 ± 0.55 | 15 | If you can be active together with your friends and play a match | 4.00 ± 0.71 | |
| 5 | If a child with asthma is replaced in time and/or more frequently during a soccer game | 4.20 ± 0.84 | 14 | If children with asthma would play outside, especially if they are bored | 4.00 ± 1.00 | |
| 6 | If children with asthma would dance more often in order to train their condition | 4.20 ± 0.84 | 33 | If I can play “trefbal” with many balls | 4.00 ± 1.00 | |
| 29 | If children with asthma, who suffer a lot, would do sports that they can maintain well | 4.20 ± 0.84 | 16 | If a child with asthma more often plays active outdoor games | 3.80 ± 1.30 | |
| 34 | If you would dance with crazy moves | 4.20 ± 0.84 | 12 | If a child with asthma would go to the swimming pool by bike | 3.75 ± 0.50 | |
| 36 | If a child with asthma could do horse riding | 4.20 ± 1.79 | 1 | If a child with asthma would play outside more often | 3.60 ± 1.14 | |
| 13 | If a child with asthma would run every day | 4.00 ± 1.41 | 23 | If a child with asthma would go roller skating together with its family | 3.60 ± 1.14 | |
| 10 | If children with asthma would do sports that they really like to do | 3.80 ± 1.10 | 19 | If your would jump rope at school in breaks | 3.20 ± 0.45 | |
| 3 | If children with asthma would participate more often in less intensive sports | 3.60 ± 1.14 | 20 | If you would use the break at school better | 3.00 ± 1.58 | |
| 4 | If children with asthma join sports clubs so that they are expected to join the training | 3.60 ± 1.95 | 18 | If you can play tag more often so that you can get tired together with other children | 3.00 ± 1.87 | |
| 35 | When there are more often funny games during the warming up | 3.40 ± 1.34 | 11 | When the parents of a child with asthma would not have a car | 3.00 ± 1.87 | |
| 24 | If there would be a special asthma team sport in which it is allowed to replace players frequently | 3.00 ± 1.41 | 2 | If a child with asthma would more often do bicycle matches with other children | 2.80 ± 0.84 | |
| 31 | If sports have a steady increase in activities and intensity | 2.80 ± 1.79 | ||||
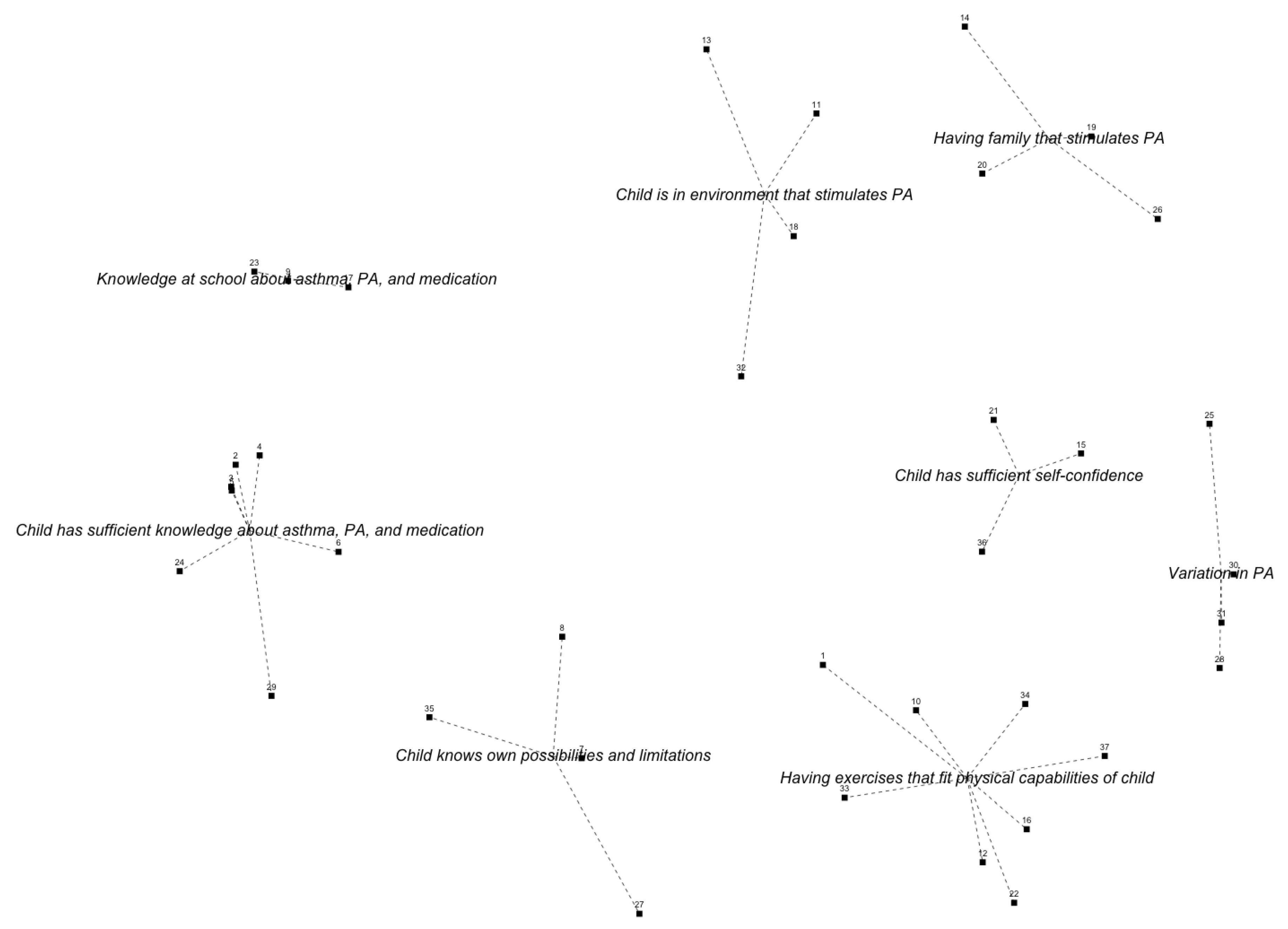
Appendix A.4. Parents Group 1

| Tailored PA | Child knows its possibilities and limitations | |||||
| 34 | If a child with asthma experiences success more often | 4.25 ± 0.87 | 8 | If a child knows its limits | 3.92 ± 1.00 | |
| 1 | If a child has confidence that the exercise will not lead to an asthma attack | 4.25 ± 0.97 | 7 | Find out together achievability in terms of movement | 3.75 ± 0.87 | |
| 16 | If a child can do the same exercises as other children | 3.67 ± 1.15 | 35 | Find out together achievability in terms of allergy | 2.83 ± 1.40 | |
| 37 | If there is an element of competition in the activity | 3.58 ± 1.31 | 27 | If child with asthma does not use asthma as an excuse | 2.75 ± 1.48 | |
| 22 | If an activity is accessible and easy to go to | 3.50 ± 1.17 | Child has sufficient knowledge about asthma, PA, and medication | |||
| 33 | If a child with asthma can keep his physical fitness level stable | 3.50 ± 1.31 | 2 | Correct use of medication | 4.50 ± 0.90 | |
| 10 | If a child with asthma likes the activity just as much as children without asthma | 3.33 ± 1.44 | 3 | If a child with asthma uses the right dose of medication | 4.42 ± 1.08 | |
| 12 | Meeting sports heroes that also have asthma | 2.92 ± 1.56 | 6 | Knowing that a normal breathing pattern is | 3.75 ± 1.36 | |
| Having family that stimulates PA | 4 | If a child with asthma knows what asthma is | 3.50 ± 1.09 | |||
| 14 | If children have enough time and possibilities to exercise at home | 3.92 ± 1.16 | 24 | When there would be an action plan and the child knows how to use it | 3.25 ± 1.48 | |
| 19 | If parents exercise together with the child | 3.67 ± 0.89 | 5 | If a child with asthma knows the effect of the medication | 3.17 ± 1.40 | |
| 20 | If parents watch the exercising child | 3.50 ± 1.45 | 29 | If a child with asthma always carries its medication with him/her | 3.08 ± 1.38 | |
| 26 | If screen time is reduced | 2.83 ± 1.27 | School has sufficient knowledge about asthma, PA, and medication | |||
| Variation in physical activities | 9 | The school environment of a child with asthma knows what asthma is | 3.50 ± 1.17 | |||
| 30 | If there is variability in activities | 4.33 ± 0.78 | 17 | If a school knows more about asthma | 3.42 ± 0.79 | |
| 31 | If there is a moment of rest within an activity | 3.42 ± 1.124 | 23 | If there are agreements with teachers about exercise and medication of the child | 3.33 ± 1.07 | |
| 25 | If exercising is being rewarded | 3.33 ± 1.30 | Child is in environment that stimulates PA | |||
| 28 | If active and passive periods are alternated | 3.33 ± 1.30 | 13 | If children have enough time and space to exercise at school | 3.42 ± 1.07 | |
| Child has sufficient self-confidence | 11 | If others (parents, friends, school, therapists) motivate the child | 3.33 ± 1.37 | |||
| 21 | If a child with asthma has enough self-esteem to dare to move | 4.08 ± 0.79 | 32 | if a healthcare provider emphasises exercise and sports positively | 3.25 ± 1.29 | |
| 15 | If children do things that they like | 4.00 ± 1.04 | 32 | If a child with asthma is stimulated to keep being active during a period of illness | 3.25 ± 1.42 | |
| 36 | Meeting a hero who also has asthma | 2.75 ± 1.54 | ||||
Appendix A.5. Parents Group 2

| Child is in environment that stimulates PA | Good asthma control despite triggers | |||||
| 23 | If there were more possibilities for indoor activities focussed on PA | 4.00 ± 0.00 | 2 | When there is asthma control | 4.20 ± 1.30 | |
| 3 | If the child is guided well during sports performances | 3.60 ± 0.55 | 35 | If the air would be cleaner | 4.00 ± 1.22 | |
| 29 | If there is a structure in weekly exercises | 3.60 ± 0.89 | 36 | If smoking near children would be forbidden | 4.00 ± 1.41 | |
| 13 | If PA is facilitated by the environment | 3.60 ± 1.14 | 34 | When the side effects of asthma medication would be less | 3.40 ± 1.52 | |
| 27 | When a child has to sit, it can sit on a gym ball | 2.60 ± 0.89 | Exemplary behaviour of relatives regarding PA | |||
| School environment and policy stimulate PA | 25 | If parents would set a good example regarding sports is | 4.40 ± 0.89 | |||
| 21 | If more exercise materials would be offered at school during the break | 4.60 ± 0.55 | 30 | If a child exercises together with other people | 4.40 ± 1.34 | |
| 20 | When gym classes at school are offered at least twice a week | 4.20 ± 0.45 | 24 | If parents would set a good example regarding screen time | 4.20 ± 1.10 | |
| 22 | If teachers stimulate PA during the break | 4.20 ± 0.84 | 9 | If a child plays an active digital game | 4.00 ± 1.22 | |
| 28 | If activities at school are really done instead of shown in a screen | 4.00 ± 0.00 | 12 | If exercising is an implied condition to play a game | 4.00 ± 1.22 | |
| 5 | If there is sufficient variance during gym classes | 3.80 ± 1.10 | 14 | If a hobby is also related to physical activity | 3.80 ± 0.45 | |
| 4 | During school lessons being motivated to be active | 3.40 ± 0.89 | 26 | If other help children in deciding what to do | 3.80 ± 0.45 | |
| 32 | If phones are forbidden at schools | 3.40 ± 2.19 | 18 | If the child is being rewarded | 3.80 ± 0.45 | |
| Child is able to make its own choices | 8 | If there is not too much distraction because of screens | 3.80 ± 1.64 | |||
| 1 | If they can perform sports that they really like | 4.80 ± 0.45 | 33 | If a child wants to join a group that exercises a lot | 3.60 ± 0.89 | |
| 17 | If the child understands how many activities he/she has performed | 4.00 ± 0.71 | 31 | If a child performs active tasks | 3.60 ± 1.14 | |
| 10 | If children accept each other’s physical problems and children are not excluded | 3.60 ± 0.89 | 11 | If there are games in which children with asthma can participate at different intensity levels | 3.40 ± 0.55 | |
| 6 | If the child starts to use medication when needed | 3.40 ± 1.34 | 19 | If physical activity includes elements of competition | 3.40 ± 0.55 | |
| 7 | If the child is not ashamed of using medication during sports | 3.00 ± 0.71 | 16 | If not only sports are labelled as physical activity | 3.20 ± 1.30 | |
| 15 | If a child does not sit all the time | 3.00 ± 0.71 | ||||
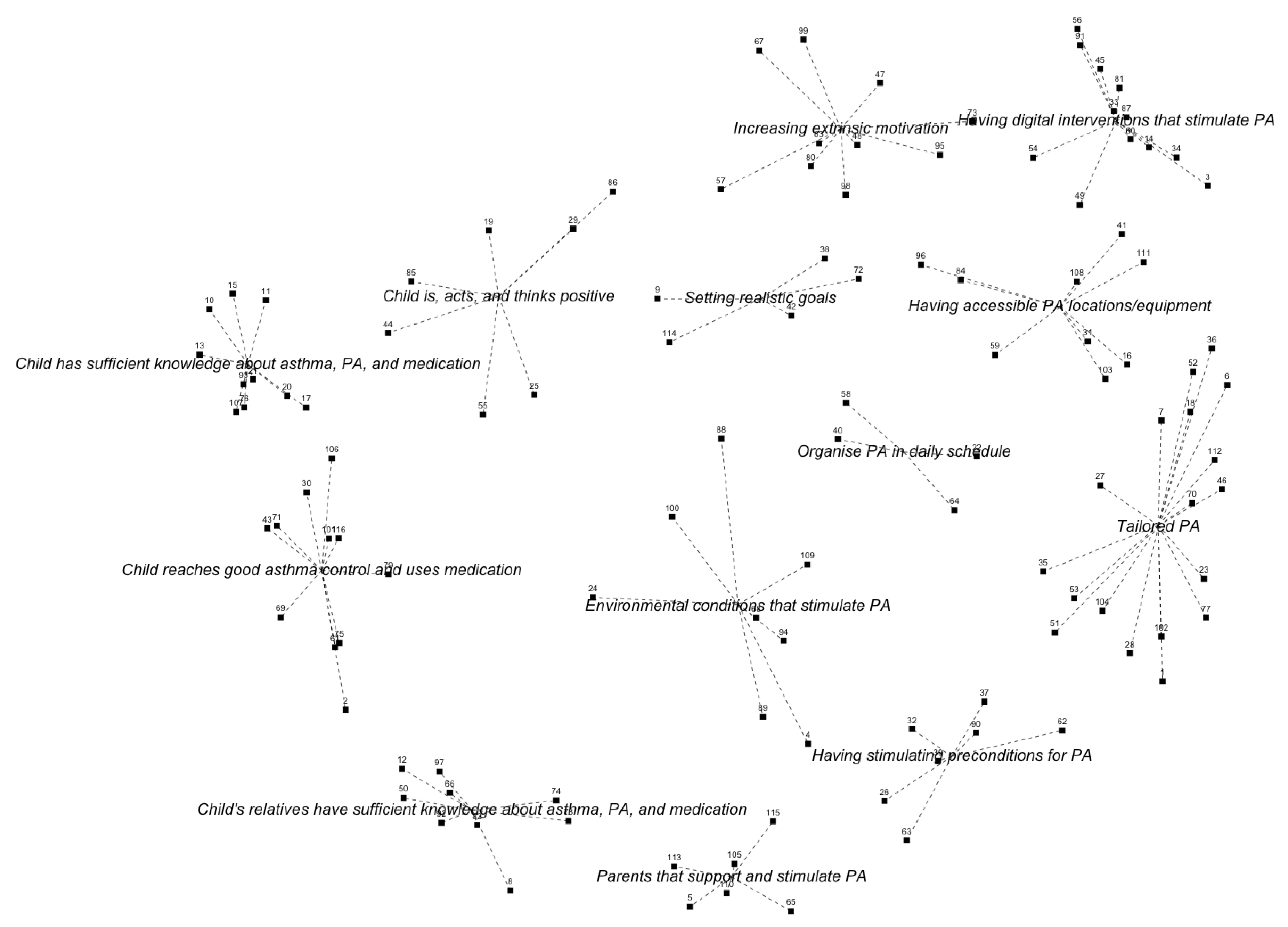
Appendix A.6. Healthcare Providers

| Child is, acts, and thinks positive | Having accessible PA locations/equipment | |||||
| 44 | Show children what they can do themselves to be less short of breath | 4.48 ± 0.98 | 96 | If enjoyment of PA is increased | 4.29 ± 0.78 | |
| 29 | If PA experiences are positive and without association of pain and dyspnea | 4.43 ± 0.60 | 84 | If exercises are offered structurally or children get a reminder | 4.19 ± 0.75 | |
| 86 | If there is a good balance between exercise and relaxation | 4.29 ± 0.72 | 103 | If the exercise can be done with either good weather or bad weather | 4.14 ± 0.65 | |
| 85 | If they know and respect their physical limits well | 4.10 ± 0.94 | 41 | If children can invite friends to participate in a game or sports program | 4.05 ± 0.92 | |
| 55 | If the child has a good physical capacity | 3.62 ± 0.92 | 16 | If sports programs are in line with the trends of the moment | 3.76 ± 0.94 | |
| 19 | If they get example of famous Dutch people having asthma and playing sports too | 2.90 ± 0.77 | 59 | If activities are offered as alternatives for watching television | 3.67 ± 0.80 | |
| 25 | If the paediatrician gives them a book with ideas and tips about physical activity | 2.86 ± 0.96 | 108 | If periods of watching television are alternated with PA and this is rewarded | 3.14 ± 1.20 | |
| Having digital interventions that stimulate PA | 31 | If a child would walk instead of bike to be active for a longer time | 2.76 ± 1.14 | |||
| 49 | If exercise is made joyful with use of a game | 4.48 ± 0.60 | 111 | If the child would receive a cheap treadmill with a game to walk at home | 2.10 ± 1.14 | |
| 14 | If there is an app or game that can be used indoors and stimulates exercise | 4.29 ± 0.64 | Parents that support and stimulate PA | |||
| 56 | If there is an app that monitors PA and rewards PA in a nice way | 4.24 ± 0.83 | 105 | If parents would also be enthusiastic about physical activity | 4.71 ± 0.46 | |
| 60 | If there is an exercise game that they can play together with other children to stimulate each other | 4.19 ± 0.75 | 113 | If parents would show that they are proud of their children | 4.67 ± 0.48 | |
| 54 | If exercising would be challenging | 4.10 ± 0.77 | 110 | If parents support the child to be physically active and are a good example | 4.62 ± 0.59 | |
| 3 | If there is a rewarding system for PA | 4.05 ± 0.97 | 115 | If parents would participate in interventions with different goals | 4.29 ± 0.78 | |
| 91 | If there is a (computer) game where you can collect points and achieve higher levels when being active | 4.00 ± 0.89 | 5 | If parents would not be too protective is | 3.95 ± 0.92 | |
| 87 | When exercises are delivered through different media (tablet, phone, activity tracker) | 4.00 ± 0.89 | 65 | If parent positively support children during sports games instead of shouting | 2.71 ± 1.27 | |
| 45 | If there is a smartphone app that links PA behaviour to peers with competition elements | 3.76 ± 0.89 | Tailored PA | |||
| 81 | When there would be different exercise apps with different themes | 3.62 ± 0.86 | 77 | If the school yard is a challenging environment to exercise | 4.38 ± 0.59 | |
| 34 | If there are inspiring outdoor tasks. For instance with google maps and taking pictures | 3.62 ± 1.02 | 27 | If tailored PA is offered | 4.05 ± 0.92 | |
| 33 | If there exist virtual reality exercise games | 2.95 ± 1.24 | 53 | If children walk/bike to school instead of going by car | 4.05 ± 1.02 | |
| Increasing extrinsic motivation | 104 | If it is possible to do the exercise inside instead of outside in winter times | 4.05 ± 0.67 | |||
| 98 | If they gain success experiences | 4.71 ± 0.46 | 18 | If there is a group training instead of an individual training | 3.81 ± 0.81 | |
| 48 | If the exercises correspond to the child’s strengths | 4.43 ± 0.60 | 70 | If they have the opportunity to try out different sports | 3.76 ± 0.89 | |
| 95 | If they can determine what they want to do in terms of PA | 4.14 ± 0.85 | 6 | If exciting materials are offered for all ages | 3.71 ± 0.90 | |
| 47 | If exercise is addictive: being active is rewarded and being inactive is not | 4.00 ± 0.84 | 23 | If there is variation in sports options | 3.71 ± 0.78 | |
| 99 | If there exists an app for children with asthma with useful tips and tricks | 4.00 ± 1.14 | 51 | If children with asthma are matched to those who are very active | 3.57 ± 1.03 | |
| 73 | If they are rewarded for good PA behaviour | 3.95 ± 1.02 | 35 | If the difference with peers in physical capacity is not that big | 3.52 ± 0.81 | |
| 80 | If exercising results in measurable results like physical fitnett or increased muscle strength | 3.57 ± 1.08 | 36 | If they exercise together with other children with asthma | 3.38 ± 1.12 | |
| 57 | If they have contact with other children suffering from asthma | 3.52 ± 0.81 | 46 | If they exercise together with other children with a chronic disease | 3.38 ± 1.12 | |
| 83 | If the child is offered a questionnaire to help determining what he/she likes | 3.29 ± 1.10 | 102 | If there is open access to sports facilities | 3.24 ± 1.14 | |
| 67 | If the child watches recordings of his own activities to see what he/she did | 2.81 ± 1.08 | 112 | If they temporarily exercise in a group with lifestyle interventions | 3.14 ± 0.91 | |
| Child reaches good asthma control and uses medication | 28 | If a sports day is organised for children with asthma | 2.76 ± 1.22 | |||
| 101 | If the correct medication and dosage are used before/during sports | 4.67 ± 0.58 | 52 | If exercise materials can be borrowed from friends | 2.71 ± 1.06 | |
| 61 | If asthma control is reached | 4.43 ± 0.68 | 1 | If presence at sports is rewarded with membership awards | 2.71 ± 1.27 | |
| 43 | If the correct medication is used and there is good medication adherence | 4.38 ± 0.92 | 7 | If daily life activities are combined with exercises | 2.43 ± 0.98 | |
| 69 | If the child, parents, and teachers know about the use of bronchodilators | 4.38 ± 0.97 | Organise PA in daily schedule for child | |||
| 71 | If the child always carries its medication with him/her | 4.29 ± 1.01 | 58 | If people see the strengths of a child | 3.33 ± 1.12 | |
| 106 | If fear for an asthma attack is reduced (both for the child and its relatives) | 4.29 ± 1.06 | 22 | If there exists apps in which family is involved to play against each other | 4.00 ± 0.84 | |
| 30 | If it is clear that the child with asthma needs to be as physically active as its healthy peers | 4.19 ± 0.93 | 64 | If they join an exercise program like Fitkids | 3.29 ± 1.15 | |
| 79 | If it is not stupid to take medication | 4.05 ± 1.07 | 40 | If an exercise period is planned | 3.05 ±1.32 | |
| 116 | If medication is easy to take with you | 4.00 ± 1.10 | Having stimulating preconditions for PA | |||
| 75 | If an irritated nose is treated | 3.48 ± 1.25 | 32 | If parents exercise with together with children to stimulate PA | 4.19 ± 0.87 | |
| 2 | If children with asthma are not overweighted too | 3.14 ± 1.35 | 26 | If there would be financial support for families with financial problems | 4.14 ± 0.79 | |
| Chid has sufficient knowledge about asthma, PA, and medication | 37 | If there is a living environment in which they can play | 4.14 ± 0.91 | |||
| 107 | If the child has enough knowledge about the disease | 4.76 ± 0.44 | 39 | If the environment is safe for exercising | 4.10 ± 0.70 | |
| 76 | If the child knows that exercising does not result in physical damage | 4.52 ± 0.60 | 62 | If there are more gym classes at school | 4.10 ± 1.18 | |
| 15 | If a child knows the difference between shortness of breath and dyspnea | 4.38 ± 0.97 | 90 | If there would be enough sports facilities in their neighbourhood | 4.00 ± 0.63 | |
| 10 | If a child knows the difference between feeling short of breath and being short of breath | 4.33 ± 1.00 | 63 | If being different is accepted as such | 3.90 ± 1.04 | |
| 93 | If a child does not have to be dyspneic after exercising | 4.19 ± 1.21 | Setting realistic goals | |||
| 20 | If the importance of physical activity is clear | 4.05 ± 0.74 | 9 | Setting realistic goals | 4.24 ± 1.00 | |
| 21 | If the child knows about physical capacity and having less energy during an exacerbation | 4.00 ± 1.00 | 114 | Setting realistic together with and for the child | 4.14 ± 1.01 | |
| 11 | If the child is aware of the importance of a good physical fitness | 3.90 ± 0.77 | 42 | If exercising has a purpose other than health benefits | 3.43 ± 0.98 | |
| 13 | If it is clear that, there could be other reasons, in addition to asthma, why the child feels short of breath | 3.90 ± 1.14 | 72 | If the exercise is not too hard to perform | 3.33 ± 1.06 | |
| 17 | If the child knows how to perform a warming up and cooling down correctly | 3.29 ± 1.23 | 38 | If gross and fine motor skills are alternated | 2.38 ± 0.92 | |
| Chid’s relatives have sufficient knowledge about asthma, PA, and medication | Environmental conditions that stimulate PA | |||||
| 8 | If the child is less exposed to smoke | 4.38 ± 1.12 | 68 | If playing outside would be stimulated | 4.48 ± 0.60 | |
| 74 | If sports teachers and trainers help the child when it experiences asthma symptoms | 4.29 ± 0.78 | 94 | If time is made for PA | 4.33 ± 0.73 | |
| 66 | If sports teachers know more about the “do’s and don’ts” in children with asthma | 4.29 ± 0.85 | 100 | If the child can gain PA experiences from an early age | 3.50 ± 0.76 | |
| 97 | If there is sufficient knowledge among sports teachers and clubs about the impact of asthma on a child | 4.29 ± 0.90 | 4 | If everyone stimulated a child with asthma to participate in activities | 4.29 ± 0.72 | |
| 92 | If there is information for the parents about PA, physical fitness, and psychosocial development | 4.24 ± 0.70 | 89 | If the child has a good bicycle to go to school | 3.76 ± 1.09 | |
| 82 | If parents would be less afraid that the child could get an asthma attack during physical activity | 4.24 ± 0.77 | 88 | If a week schedule is made with several options per day | 3.67 ± 1.06 | |
| 50 | If school is well informed that the child could get an asthma attack during physical activity | 4.24 ± 0.77 | 24 | If screen time is limited | 3.62 ± 1.02 | |
| 12 | If there is information about asthma and the impact on a child for all cultures | 4.05 ± 0.80 | 109 | If physiotherapists help inactive children in choosing sports | 3.29 ± 1.19 | |
| 78 | If peers and adults show that they understand the complaints of a child | 4.05 ± 0.92 | ||||
References
- Janssen, I.; LeBlanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 40. [Google Scholar] [CrossRef] [PubMed]
- Morris, P.J. Physical activity recommendations for children and adolescents with chronic disease. Curr. Sport. Med. Rep. 2008, 7, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Riner, W.F.; Sellhorst, S.H. Physical activity and exercise in children with chronic health conditions. J. Sport Health Sci. 2013, 2, 12–20. [Google Scholar] [CrossRef]
- World Health Organization. Fact Sheet Asthma; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Bindels, P.; Van de Griendt, E.J.; Grol, M.; Hensbergen, W.V.; Steenkamer, T.; Uijen, H.; Burgers, J.; Geijer, R.; Tuut, M. NHG-Standaard Astma bij kinderen (derde herziening). Huisarts Wet 2014 2014, 57, 70–80. [Google Scholar]
- Fanelli, A.; Lucia, A.; Cabral, B.; Neder, J.A.; Martins, M.A.; Ricardo, C.; Carvalho, F.; Paulo, S.; Vargas, H.D. Exercise on Disease Control and Quality of Training Life in Asthmatic Children. Med. Sci. Sport. Exerc. 2007, 39, 1474–1481. [Google Scholar] [CrossRef]
- Welsh, L.; Gemp, J.G.; Roberts, R.G. Effects of Physical Conditioning on Children and Adolescents with Asthma. Sport. Med. 2005, 35, 127–141. [Google Scholar] [CrossRef]
- Eichenberger, P.A.; Diener, S.N.; Kofmehl, R.; Spengler, C.M. Effects of exercise training on airway hyperreactivity in asthma: A systematic review and meta-analysis. Sport. Med. 2013, 43, 1197–2035. [Google Scholar] [CrossRef]
- Glazebrook, C.; McPherson, A.C.; Macdonald, I.A.; Swift, J.A.; Ramsay, C.; Newbould, R.; Smyth, A. Asthma as a Barrier to Children’s Physical Activity: In Reply. Pediatrics 2006, 118, 2443–2449. [Google Scholar] [CrossRef]
- Lang, D.M.; Butz, A.M.; Duggan, A.K.; Serwint, J.R. Physical Activity in Urban School-Aged Children with Asthma. Pediatrics 2004, 113, 341–346. [Google Scholar] [CrossRef]
- Yiallouros, P.K.; Economou, M.; Kolokotroni, O.; Savva, S.C.; Gavatha, M.; Ioannou, P.; Karpathios, T.; Middleton, N. Gender differences in objectively assessed physical activity in asthmatic and non-asthmatic children. Pediatr. Pulmonol. 2015, 50, 317–326. [Google Scholar] [CrossRef]
- Wanrooij, V.H.M.; Willeboordse, M.; Dompeling, E.; Van De Kant, K.D.G. Exercise training in children with asthma: A systematic review. Br. J. Sport. Med. 2014, 48, 1024–1031. [Google Scholar] [CrossRef] [PubMed]
- Bloemen, M.A.T.; Backx, F.J.G.; Takken, T.; Wittink, H.; Benner, J.; Mollema, J.; de Groot, J.F. Factors associated with physical activity in children and adolescents with a physical disability: A systematic review. Dev. Med. Child Neurol. 2015, 57, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Van der Ploeg, H.P. Physical activity for people with a disability. Sport. Med. 2004, 34, 639–649. [Google Scholar] [CrossRef] [PubMed]
- Kornblit, A.; Cain, A.; Bauman, L.J.; Brown, N.M.; Reznik, M. Parental Perspectives of Barriers to Physical Activity in Urban Schoolchildren With Asthma. Acad. Pediatr. 2018, 18, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Powell, A.; Hoskins, G.; Neville, R. Exploring and explaining low participation in physical activity among children and young people with asthma: A review. BMC Fam. Pract. 2008, 9, 1–11. [Google Scholar] [CrossRef]
- Burke, J.G.; O’Campo, P.; Peak, G.L.; Gielen, A.C.; McDonnell, K.A.; Trochim, W.M. An introduction to concept mapping as a participatory public health research method. Qual. Health Res. 2005, 15, 1392–1410. [Google Scholar] [CrossRef]
- Trochim, W.; Kane, M. Concept mapping: An introduction to structured conceptualization in health care. Int. J. Qual. Health Care 2005, 17, 187–191. [Google Scholar] [CrossRef]
- Jongste, J.; Vrijlandt, E. Astma bij kinderen; herziene richtlijnen van de sectie kinderlongziekten van de NVK [Asthma in Children; Revised Guidelines of the Paediatric Department of the Dutch Paediatric Society]; Jurriaans Lindenbaum Grafimedia: Amsterdam, The Netherlands, 2007. [Google Scholar]
- Kruskal, W.H.; Wallis, W.A. Use of ranks in one-criterion variance analysis. J. Am. Stat. Assoc. 1952, 47, 583–621. [Google Scholar] [CrossRef]
- Bar, H.; Mentch, L. R-CMap—An open-source software for concept mapping. Eval. Program Plan. 2017, 60, 284–292. [Google Scholar] [CrossRef]
- Noonan, R.J.; Boddy, L.M.; Fairclough, S.J.; Knowles, Z.R. Write, draw, show, and tell: A child-centred dual methodology to explore perceptions of out-of-school physical activity. BMC Public Health 2016, 16, 326. [Google Scholar] [CrossRef]
- Willis, C.E.; Reid, S.; Elliott, C.; Rosenberg, M.; Nyquist, A.; Jahnsen, R.; Girdler, S. A realist evaluation of a physical activity participation intervention for children and youth with disabilities: What works, for whom, in what circumstances, and how? BMC Pediatr. 2018, 18, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Bingham, P.M.; Crane, I.; Manning, S.W. Illness Experience, Self-Determination, and Recreational Activities in Pediatric Asthma. Games Health J. 2017, 6, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Buffart, L.M.; Westendorp, T.; Berg-emons, R.J.V.D.; Stam, H.J.; Roebroeck, M.E. Original Report Perceived Barriers To and Facilitators of Physical Activity in Young Adults With Childhood-onset Physical Disabilities. J. Rehabil. Med. 2009, 41, 881–885. [Google Scholar] [CrossRef] [PubMed]
- Brussel, M.V.; Net, J.V.D.; Hulzebos, E. The Utrecht Approach to Exercise in Chronic Childhood Conditions: The Decade in Review. Pediatr. Phys. Ther. 2011, 6, 2–14. [Google Scholar] [CrossRef] [PubMed]
- Hidding, L.M.; Altenburg, T.M.; Ekris, E.V.; Chinapaw, M.J.M. Why Do Children Engage in Sedentary Behavior? Child- and Parent-Perceived Determinants. Int. J. Environ. Res. Public Health 2017, 14, 671. [Google Scholar] [CrossRef] [PubMed]



 = children,
= children,  = parents, and
= parents, and  = healthcare providers. The symbols indicate the category of the cluster with: ○ = personal factor and ■ = environmental factor. The clusters are listed in random order.
= children, = parents, and = healthcare providers. The symbols indicate the category of the cluster with: ○ = personal factor and ■ = environmental factor. The clusters are listed in random order.
= healthcare providers. The symbols indicate the category of the cluster with: ○ = personal factor and ■ = environmental factor. The clusters are listed in random order.
= children, = parents, and = healthcare providers. The symbols indicate the category of the cluster with: ○ = personal factor and ■ = environmental factor. The clusters are listed in random order.
| Having good asthma control | Make PA fun to do | |||||
| 32 | If I am not ill | 5.00 ± 0.00 | 48 | If the exercise is new | 5.00 ± 0.00 | |
| 23 | If I can breath properly | 4.75 ± 0.50 | 24 | If I could exercise together with other children | 4.50 ± 1.00 | |
| 21 | If I am not short of breath | 4.50 ± 0.58 | 30 | If there is a game in which you have to exercise | 4.50 ± 0.58 | |
| 31 | If I would not have asthma (symptoms) | 4.00 ± 2.00 | 49 | If I see someone else doing something new | 4.50 ± 1.00 | |
| 37 | If I would be able to play in different places | 3.00 ± 1.63 | 45 | If I can learn someone else an exercise | 4.00 ± 1.15 | |
| Sufficient conditions/facilities for PA | 10 | If there is music | 3.50 ± 1.00 | |||
| 11 | If I could run | 4.50 ± 0.58 | 15 | If I can show others what a joy being active is | 3.25 ± 1.26 | |
| 41 | If I could jump on a trampoline | 4.50 ± 1.00 | 47 | If I see that someone else is exercising | 3.00 ± 1.63 | |
| 18 | If I could bike | 4.25 ± 0.96 | 26 | If am distracted while exercising | 2.25 ± 1.50 | |
| 19 | If there would be playground equipment | 4.00 ± 0.82 | Situation forces PA unknowingly | |||
| 28 | If I would not have fear of heights | 4.00 ± 2.00 | 40 | If I don’t have to sit down | 4.00 ± 2.00 | |
| 38 | If I could run in the forest | 4.00 ± 1.15 | 27 | If I am distracted while being physically active | 3.50 ± 1.91 | |
| 12 | If I could walk | 3.50 ± 0.58 | 39 | If I’m not being active very often | 1.00 ± 0.00 | |
| 17 | If I would go to school by bike | 3.50 ± 1.00 | Exercising outside more often | |||
| 7 | If the weather is nice | 3.25 ± 1.71 | 2 | If I can do sports | 4.25 ± 0.96 | |
| 8 | If it is not raining | 3.25 ± 1.71 | 5 | If II would go to play outside | 4.00 ± 1.41 | |
| 35 | If I walk in a theme park or museum | 2.75 ± 0.50 | 13 | If I can show someone else what a joy playing outside is | 3.50 ± 1.91 | |
| 16 | If I would not go to school by car | 2.25 ± 1.50 | 1 | If there are facilities in the neighbourhood to play outside | 2.75 ± 1.50 | |
| Having stimulating PA situations | 4 | If I could climb in trees | 2.25 ± 1.89 | |||
| 43 | If we could play “boys against girls” | 4.75 ± 0.50 | Get a positive feeling/emotion from PA | |||
| 22 | If I am alive | 4.33 ± 1.15 | 29 | If it is fun to do | 5.00 ± 0.00 | |
| 44 | If it is a game | 4.25 ± 0.96 | 25 | If I am happy | 4.75 ± 0.50 | |
| 9 | If I would participate in gym classes | 3.25 ± 1.50 | 33 | If PA is not boring | 4.75 ± 0.50 | |
| 3 | If I would play soccer outside | 3.00 ± 1.41 | 14 | If I can go crazy | 3.75 ± 0.96 | |
| 6 | If I am not home alone | 3.00 ± 1.63 | 42 | If it is exciting to do | 3.50 ± 1.73 | |
| 36 | If there is a simulator for being in a theme park | 2.25 ± 0.96 | 46 | If I can imitate someone or something | 3.50 ± 1.29 | |
| 34 | If there is a simulator for being outside | 1.75 ± 0.96 | 20 | If I am short of breath | 2.25 ± 1.26 | |
| Children Group 1 | Children Group 2 | Children Group 3 | Children Group 4 | ||||
|---|---|---|---|---|---|---|---|
| ● | Get a positive feeling of PA 3.9 ± 0.4 | ★ | Having good asthma control 4.3 ± 0.8 | ● | Play outside more often 3.2 ± 0.5 | ✻ | Get rewards for doing exercises or PA 3.9 ± 0.4 |
| ▲ | Playing together 3.7 ± 0.3 | ♣ | Get positive feeling and emotion from PA 3.9 ± 1.0 | ✻ | Have cool and special activities 3.1 ± 0.6 | ✻ | Tailored PA 3.8 ± 0.5 |
| ▲ | Be motivated by others 3.7 ± 0.6 | ✻ | Make PA fun to do 3.8 ± 0.9 | ▲ | Being motivated by others to exercise 2.8 ± 0.7 | ✻ | Make exercises joyful 3.7 ± 0.3 |
| ◆ | Sufficient capabilities for PA 3.6 ± 0.2 | ✻ | Sufficient conditions and facilities for PA 3.6 ± 0.7 | ✻ | Add competitive elements to PA 2.4 ± 0.1 | ● | Play outside more often 3.7 ± 0.6 |
| ✻ | Have access to nice sports and exercises 3.6 ± 0.7 | ● | Exercising outside more often 3.4 ± 0.8 | ● | Set exercise goals 2.9 ± 0.3 | ||
| ● | Perform high intensity exercises 3.1 ± 0.8 | ✻ | Having stimulating PA situations 3.3 ± 1.1 | ||||
| ✻ | Add competitive elements to PA 2.9 ± 0.8 | ✻ | Situation forces PA unknowingly 2.8 ± 1.6 | ||||
| ✻ | Have joyful activities to perform 2.9 ± 0.6 | ||||||
| ● | Play outside more often 2.4 ± 0.7 | ||||||
| ✻ | Be forced to do daily life activities 1.6 ± 0.6 | ||||||
| Healthcare Providers Group 1 | Parents Group 1 | Parents Group 2 | |||
|---|---|---|---|---|---|
| ✻ | Child’s relatives have sufficient knowledge about asthma, PA, and medication 4.2 ± 0.1 | ◆ | Child has sufficient knowledge about asthma, PA, and medication 3.7 ± 0.6 | ★ | Good asthma control despite triggers 3.9 ± 0.3 |
| ▲ | Parents that support and stimulate PA 4.2 ± 0.8 | ✻ | Tailored PA 3.6 ± 0.4 | ✻ | School environment and policy stimulate PA 3.9 ± 0.3 |
| ✻ | Having stimulating preconditions for PA 4.1 ± 0.1 | ✻ | Variation in physical activities 3.6 ± 0.5 | ▲ | Exemplary behaviour of relatives regarding PA 3.8 ± 0.4 |
| ◆ | Child has sufficient knowledge about asthma, PA, and medication 4.1 ± 0.4 | ■ | Child has sufficient self-confidence 3.6 ± 0.7 | ■ | Child is able to make its own choices 3.6 ± 0.7 |
| ★ | Child reaches good asthma control 4.1 ± 0.4 | ▲ | Having family that stimulates PA 3.5 ± 0.5 | ✻ | Child is in environment that stimulates PA 3.5 ± 0.5 |
| ✻ | Environmental conditions that stimulate PA 4.0 ± 0.4 | ✻ | School has sufficient knowledge about asthma, PA, and medication 3.4 ± 0.1 | ||
| ✻ | Having digital interventions that stimulate PA 3.9 ± 0.4 | ✻ | Child is in environment that stimulates PA 3.3 ± 0.1 | ||
| ✻ | Increasing extrinsic motivation 3.8 ± 0.6 | ■ | Child knows its possibilities and limitations 3.3 ± 0.6 | ||
| ♣ | Child is, acts and thinks positive 3.8 ± 0.7 | ||||
| ▲ | Organise PF in daily schedule for child 3.7 ± 0.6 | ||||
| ✻ | Having accessible PA locations/equipment 3.6 ± 0.8 | ||||
| ✻ | Tailored PA 3.5 ± 0.6 | ||||
| ● | Setting realistic goals 3.5 ± 0.8 | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brons, A.; Braam, K.; Timmerman, A.; Broekema, A.; Visser, B.; van Ewijk, B.; Terheggen-Lagro, S.; Rutjes, N.; van Leersum, H.; Engelbert, R.; et al. Promoting Factors for Physical Activity in Children with Asthma Explored through Concept Mapping. Int. J. Environ. Res. Public Health 2019, 16, 4467. https://doi.org/10.3390/ijerph16224467
Brons A, Braam K, Timmerman A, Broekema A, Visser B, van Ewijk B, Terheggen-Lagro S, Rutjes N, van Leersum H, Engelbert R, et al. Promoting Factors for Physical Activity in Children with Asthma Explored through Concept Mapping. International Journal of Environmental Research and Public Health. 2019; 16(22):4467. https://doi.org/10.3390/ijerph16224467
Chicago/Turabian StyleBrons, Annette, Katja Braam, Annieck Timmerman, Aline Broekema, Bart Visser, Bart van Ewijk, Suzanne Terheggen-Lagro, Niels Rutjes, Hellen van Leersum, Raoul Engelbert, and et al. 2019. "Promoting Factors for Physical Activity in Children with Asthma Explored through Concept Mapping" International Journal of Environmental Research and Public Health 16, no. 22: 4467. https://doi.org/10.3390/ijerph16224467
APA StyleBrons, A., Braam, K., Timmerman, A., Broekema, A., Visser, B., van Ewijk, B., Terheggen-Lagro, S., Rutjes, N., van Leersum, H., Engelbert, R., Kröse, B., Chinapaw, M., & Altenburg, T. (2019). Promoting Factors for Physical Activity in Children with Asthma Explored through Concept Mapping. International Journal of Environmental Research and Public Health, 16(22), 4467. https://doi.org/10.3390/ijerph16224467