
Timing of Prostin E2 Administration After Poor Response to Propess: Impact on Induction-to-Birth Interval and Maternal/Neonatal Outcomes



Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Statements
2.2. Study Design and Population
Inclusion and Exclusion Criteria
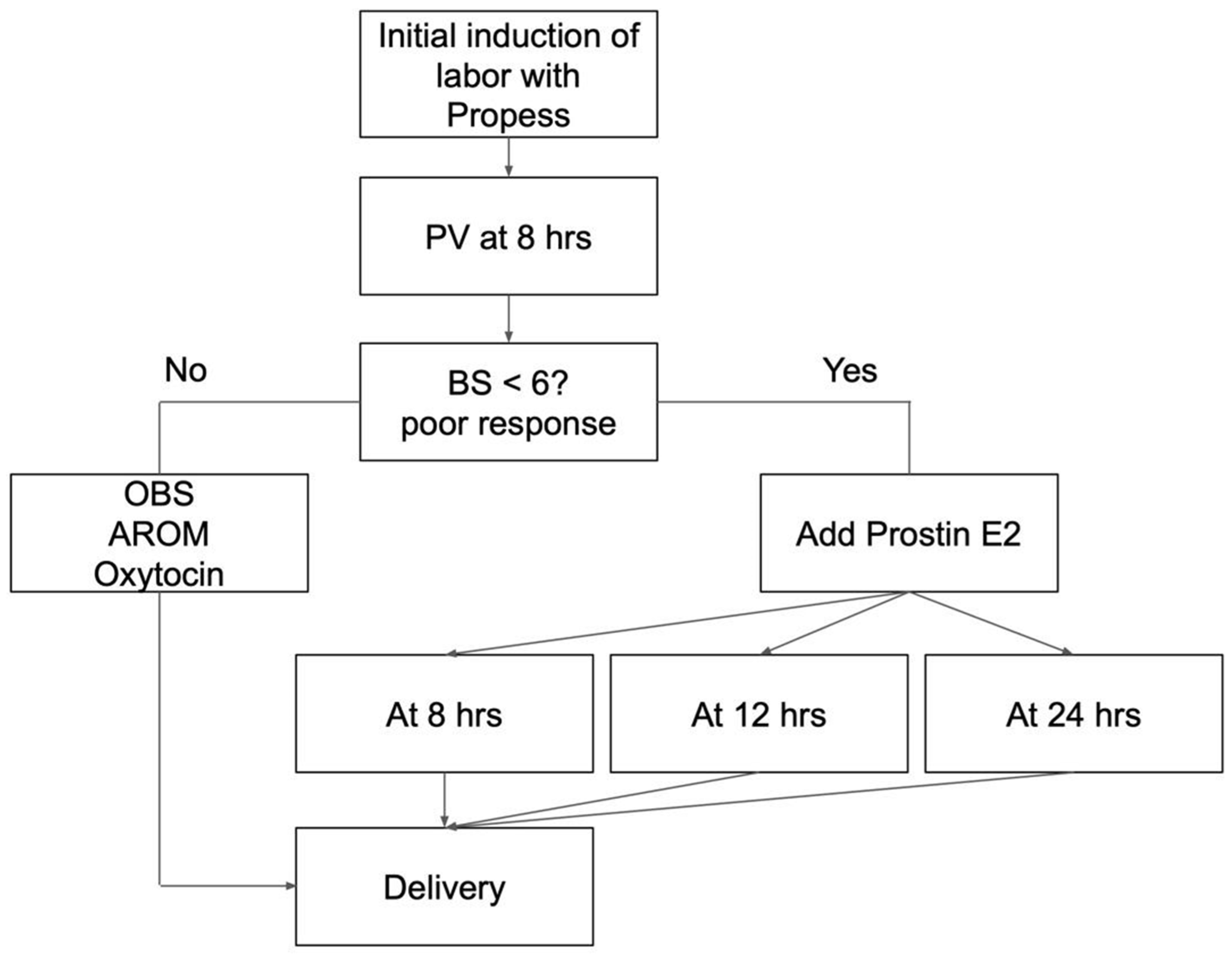
2.3. Procedure of Induction of Labor
2.4. Data Collection
2.5. Outcome Measures
2.6. Statistical Analysis
3. Results
3.1. Basic Characteristics of Patients
3.2. Maternal Outcomes
3.3. Neonatal Outcomes
3.4. Risk Factors Associated with the Duration of Labor Induction
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| IOL | induction of labor |
| PGE2 | prostaglandin E2 |
| AROM | artificial rupture of membranes |
| BMI | body mass index |
References
- Swift, E.M.; Gunnarsdottir, J.; Zoega, H.; Bjarnadottir, R.I.; Steingrimsdottir, T.; Einarsdottir, K. Trends in Labor Induction Indications: A 20-Year Population-Based Study. Acta Obstet. Gynecol. Scand. 2022, 101, 1422–1430. [Google Scholar] [CrossRef] [PubMed]
- Bukola, F.; Idi, N.; M’Mimunya, M.; Jean-Jose, W.-M.; Kidza, M.; Isilda, N.; Faouzi, A.; Archana, S.; Paulo, S.J.; Matthews, M.; et al. Unmet Need for Induction of Labor in Africa: Secondary Analysis from the 2004–2005 WHO Global Maternal and Perinatal Health Survey (A Cross-Sectional Survey). BMC Public Health 2012, 12, 722. [Google Scholar] [CrossRef] [PubMed]
- Yosef, T.; Getachew, D. Proportion and Outcome of Induction of Labor among Mothers Who Delivered in Teaching Hospital, Southwest Ethiopia. Front. Public Health 2021, 9, 686682. [Google Scholar] [CrossRef] [PubMed]
- Grobman, W.A.; Caughey, A.B. Elective Induction of Labor at 39 Weeks Compared with Expectant Management: A Meta-Analysis of Cohort Studies. Am. J. Obstet. Gynecol. 2019, 221, 304–310. [Google Scholar] [CrossRef]
- Penfield, C.A.; Wing, D.A. Labor Induction Techniques: Which Is the Best? Obstet. Gynecol. Clin. N. Am. 2017, 44, 567–582. [Google Scholar] [CrossRef]
- Ashwal, E.; Hiersch, L.; Melamed, N.; Manor, Y.; Wiznitzer, A.; Hod, M.; Yogev, Y. Pre-Induction Cervical Ripening: Comparing between Two Vaginal Preparations of Dinoprostone in Women with an Unfavorable Cervix. J. Matern. Fetal Neonatal Med. 2014, 27, 1874–1879. [Google Scholar] [CrossRef]
- Itoh, H.; Ishii, K.; Shigeta, N.; Itakura, A.; Hamada, H.; Nagamatsu, T.; Ishida, T.; Bungyoku, Y.; Falahati, A.; Tomisaka, M.; et al. Efficacy and Safety of Controlled-Release Dinoprostone Vaginal Delivery System (PROPESS) in Japanese Pregnant Women Requiring Cervical Ripening: Results from a Multicenter, Randomized, Double-Blind, Placebo-Controlled Phase III Study. J. Obstet. Gynaecol. Res. 2021, 47, 216–225. [Google Scholar] [CrossRef]
- Lyrenäs, S.; Clason, I.; Ulmsten, U. In Vivo Controlled Release of PGE2 from a Vaginal Insert (0.8 Mm, 10 Mg) during Induction of Labour. Br. J. Obstet. Gynaecol. 2001, 108, 169–178. [Google Scholar]
- Salvator, M.; Girault, A.; Sibiude, J.; Mandelbrot, L.; Goffinet, F.; Cohen, E. Failed Induction of Labor in Term Nulliparous Women with an Unfavorable Cervix: Comparison of Cervical Ripening by Two Forms of Vaginal Prostaglandins (slow-Release Pessary and Vaginal Gel). J. Gynecol. Obstet. Hum. Reprod. 2023, 52, 102546. [Google Scholar] [CrossRef]
- Ting, N.-S.; Ding, D.-C.; Wei, Y.-C. Comparison of the Dinoprostone Vaginal Insert and Dinoprostone Tablet for the Induction of Labor in Primipara: A Retrospective Cohort Study. J. Clin. Med. Res. 2022, 11, 3519. [Google Scholar] [CrossRef]
- Nien, Y.-C.; Kung, H.-F.; Chen, M.-J.; Chen, W.-C. Dinoprostone Tablet versus Continuous Vaginal Insert (Propess®) for Elective Induction in Low-Risk Nulliparous Women at Term. Taiwan. J. Obstet. Gynecol. 2023, 62, 858–862. [Google Scholar] [CrossRef] [PubMed]
- Hung, C.-H.; Chen, H.-Y.; Kang, J.; Tai, Y.-Y.; Lin, S.-Y.; Lee, C.-N. Propess versus Prostin for Induction of Labour in Term Primiparous Women. J. Formos. Med. Assoc. 2023, 122, 785–789. [Google Scholar] [CrossRef] [PubMed]
- Coste Mazeau, P.; Hessas, M.; Martin, R.; Eyraud, J.-L.; Margueritte, F.; Aubard, Y.; Sallee, C.; Sire, F.; Gauthier, T. Is There an Interest in Repeating the Vaginal Administration of Dinoprostone (Propess®), to Promote Induction of Labor of Pregnant Women at Term? (RE-DINO): Study Protocol for a Randomized Controlled Trial. Trials 2020, 21, 51. [Google Scholar] [CrossRef] [PubMed]
- Murray, S.R.M.; Dundas, K.C.D.; Byrne-Leitch, J.B.L.; Poon, W.Y.P.; Dick, A.D. PL. 46 A Retrospective Review Comparing the Efficiency and Outcomes of Propess and Prostin Gel as a Method of Inducing Labour. Arch. Dis. Child. Fetal Neonatal Ed. 2013, 98, A67. [Google Scholar] [CrossRef]
- Tirlapur, S.; Zhang, W.; Batish, A.; Nakash, A.; Wright, A. Comparing Efficiency and Outcomes of Propess (dinoprostone Slow Release Pessary) and Prostin Gel as a Method of Inducing Labour. Arch. Dis. Child. Fetal Neonatal Ed. 2010, 95, Fa70. [Google Scholar] [CrossRef]
- Anzeljc, V.; Mujezinović, F. A Randomised Controlled Trial Comparing Induction of Labour with the Propess Vaginal System to the Prostin Vaginal Tablet in Premature Rupture of Membranes at Term. J. Clin. Med. 2022, 12, 174. [Google Scholar] [CrossRef]
- Lawson, G.W. Naegele’s Rule and the Length of Pregnancy-A Review. Aust. N. Z. J. Obstet. Gynaecol. 2021, 61, 177–182. [Google Scholar] [CrossRef]
- Antonazzo, P.; Laoreti, A.; Personeni, C.; Grossi, E.; Martinelli, A.; Cetin, I. Vaginal Dinoprostone Versus Intravenous Oxytocin for Labor Induction in Patients Not Responsive to a First Dose of Dinoprostone: A Randomized Prospective Study. Reprod. Sci. 2016, 23, 779–784. [Google Scholar] [CrossRef]
- Coste-Mazeau, P.; Gallot, D.; Siegerth, F.; Garuchet-Bigot, A.; Decroisette, E.; Blanc, J.; Cantaloube, M.; Crépin, S.; Magne, J.; Labrunie, A.; et al. Results of the RE-DINO Multicenter Randomized Trial on the Repeated Use of Vaginal Dinoprostone (Propess®) for Labor Induction in Patients at Term. Am. J. Obstet. Gynecol. MFM 2024, 6, 101510. [Google Scholar] [CrossRef]
- Yang, S.H.; Roh, C.R.; Kim, J.H. Transvaginal Ultrasonography for Cervical Assessment before Induction of Labor. J. Ultrasound Med. 2004, 23, 375–382, quiz 384–385. [Google Scholar] [CrossRef]
- Lemancewicz, A.; Urban, R.; Skotnicki, M.Z.; Karpiuk, A.; Urban, J. Uterine and Fetal Doppler Flow Changes after Misoprostol and Oxytocin Therapy for Induction of Labor in Post-Term Pregnancies. Int. J. Gynaecol. Obstet. 1999, 67, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Urban, R.; Lemancewicz, A.; Urban, J.; Skotnicki, M.Z.; Kretowska, M. Misoprostol and Dinoprostone Therapy for Labor Induction: A Doppler Comparison of Uterine and Fetal Hemodynamic Effects. Eur. J. Obstet. Gynecol. Reprod. Biol. 2003, 106, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Brun, R.; Spoerri, E.; Schäffer, L.; Zimmermann, R.; Haslinger, C. Induction of Labor and Postpartum Blood Loss. BMC Pregnancy Childbirth 2019, 19, 265. [Google Scholar] [CrossRef] [PubMed]
- Kumar, B.; Kumari, S.; Hughes, S.; Savill, S. Prospective Cohort Study of Induction of Labor: Indications, Outcome and Postpartum Hemorrhage. Eur. J. Midwifery 2021, 5, 53. [Google Scholar] [CrossRef]
- Zhang, Q.-J.; Chen, S.-W.; Xu, X.; Zhang, H.-L.; Yan, J.-Y. Effect of Induction of Labor on Maternal and Perinatal Outcomes in Low-Risk Singleton Pregnancies: A Retrospective Case-Control Study. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 5918–5925. [Google Scholar]
- Razavi, A.S.; Chasen, S.T.; Chambers, F.; Kalish, R.B. Induction of Labor in Twin Gestation: Can We Predict Success? J. Perinat. Med. 2018, 46, 771–775. [Google Scholar] [CrossRef]
- Pinheiro, R.L.; Areia, A.L.; Mota Pinto, A.; Donato, H. Advanced Maternal Age: Adverse Outcomes of Pregnancy, A Meta-Analysis. Acta Med. Port. 2019, 32, 219–226. [Google Scholar] [CrossRef]
- Ohkuchi, A.; Onagawa, T.; Usui, R.; Koike, T.; Hiratsuka, M.; Izumi, A.; Ohkusa, T.; Matsubara, S.; Sato, I.; Suzuki, M.; et al. Effect of Maternal Age on Blood Loss during Parturition: A Retrospective Multivariate Analysis of 10,053 Cases. J. Perinat. Med. 2003, 31, 209–215. [Google Scholar] [CrossRef]
- Sachs, M.K.; Kapfhammer, E.; Brun, R.; Kandler, L.; Ochsenbein, N.; Haslinger, C. Epidural Anesthesia during Labor and Delivery and Postpartum Hemorrhage. J. Perinat. Med. 2025. [Google Scholar] [CrossRef]
- Bofill, J.A.; Darby, M.M.; Castillo, J.; Sawardecker, S.U.; Magann, E.F.; Morrison, J.C. Tachysystole Following Cervical Ripening and Induction of Labor Is Not Associated with Adverse Outcomes. Gynecol. Obstet. Invest. 2017, 82, 487–493. [Google Scholar] [CrossRef]
- Pierce, S.; Bakker, R.; Myers, D.A.; Edwards, R.K. Clinical Insights for Cervical Ripening and Labor Induction Using Prostaglandins. AJP Rep. 2018, 8, e307–e314. [Google Scholar] [CrossRef] [PubMed]
- Sims, M.E. Legal Briefs: Tachysystole, Uterine Rupture, and a Bad Outcome. Neoreviews 2019, 20, e110–e112. [Google Scholar] [CrossRef] [PubMed]
- Eser, A.; Ozkaya, E.; Abide, C.Y.; Eser, T.; Eser, G.Y.; Abike, F.; Tayyar, A.T.; Eroglu, M. Transcervical Foley Balloon Catheter and Vaginal Prostaglandin E2 Insert Combination vs. Vaginal Prostaglandin E2 Insert Only for Induction of Labor at Term: A Randomized Clinical Trial. Arch. Gynecol. Obstet. 2019, 299, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Arthuis, C.; Potin, J.; Winer, N.; Tavernier, E.; Paternotte, J.; Ramos, A.; Perrotin, F.; Diguisto, C. Contribution of Ultrasonography to the Prediction of the Induction-Delivery Interval: The ECOLDIA Prospective Multicenter Cohort Study. J. Gynecol. Obstet. Hum. Reprod. 2021, 50, 102196. [Google Scholar] [CrossRef]
- Warner, L.L.; Hunter Guevara, L.R.; Barrett, B.J.; Arendt, K.W.; Peterson, A.A.; Sviggum, H.P.; Duncan, C.M.; Thompson, A.C.; Hanson, A.C.; Schulte, P.J.; et al. Creating a Model to Predict Time Intervals from Induction of Labor to Induction of Anesthesia and Delivery to Coordinate Workload. Int. J. Obstet. Anesth. 2021, 45, 115–123. [Google Scholar] [CrossRef]
- Opipari, A.E.; Burns, L.P.; Kobernik, E.; Triebwasser, J.E.; Moniz, M.; Langen, E.S.; Stout, M.J. The Price of Waiting: Hospital Utilization among Elective Inductions of Labor at Increasing Gestational Age. Am. J. Obstet. Gynecol. 2022, 226, S85. [Google Scholar] [CrossRef]
- McCarthy, C.M.; Meaney, S.; McCarthy, M.; Conners, N.; Russell, N. Induction of Labor: Reviewing the Past to Improve the Future. AJOG Glob. Rep. 2022, 2, 100099. [Google Scholar] [CrossRef]

{kind=link}
| PGE2 (8 h) | PGE2 (12 h) | PGE2 (24 h) | p-Value | |
|---|---|---|---|---|
| Case number | 19 | 23 | 21 | |
| GA (weeks) | 38.23 ± 0.34 | 38.41 ± 0.54 | 39 ± 0.78 | <0.001 |
| Age (years) | 30.74 ± 5 | 28.09 ± 4.23 | 30.86 ± 6.42 | 0.153 |
| BMI (kg/m2) | 29.08 ± 4.1 | 29.4 ± 5.32 | 27.6 ± 3.7 | 0.376 |
| Painless, n (%) | 18 (94.74) | 21 (91.3) | 20 (95.24) | 0.843 |
| AROM, n (%) | 14 (73.68) | 17 (73.91) | 12 (57.14) | 0.407 |
| Piton, n (%) | 13 (68.42) | 15 (65.22) | 17 (80.95) | 0.483 |
| Timing of Prostin E2 Addition | 8 h | 12 h | 24 h | p-Value |
|---|---|---|---|---|
| Blood loss (mL) | 250.37 ± 110.06 | 178.26 ± 63.65 | 261.90 ± 142.21 | 0.027 |
| Tachysystole, n (%) | 1 (5.26) | 1 (4.35) | 1 (4.76) | 0.990 |
| Variable deceleration, n (%) | 3 (15.79) | 0 (0) | 2 (9.52) | 0.160 |
| BS at PGE2 administration (mean ± SD) | 3.21 ± 1.47 | 3.35 ± 2.06 | 4.67 ± 2.03 | 0.029 |
| BS after 12 h of Propess use (mean ± SD) | 3.84 ± 2.01 | 3.35 ± 2.06 | 3 ± 2.57 | 0.492 |
| BS after 24 h of Propess use (mean ± SD) | 9.63 ± 4.22 | 6.44 ± 2.94 | 4.67 ± 1.93 | <0.001 |
| Mode of birth, n (%) | 0.464 | |||
| VED + NSD | 17 (89.47) | 20 (86.96) | 16 (76.19) | |
| Cesarean section | 2 (10.53) | 3 (13.04) | 5 (23.81) | |
| Induction-to-birth interval (hours) | ||||
| VED + NSD | 26.87 ± 9.27 | 31.89 ± 8.31 | 44.11 ± 9.18 | <0.001 |
| Cesarean section | 44.28 ± 5.41 | 37.84 ± 8.4 | 47.82 ± 5.26 | 0.168 |
| Time of Prostin E2 Addition | 8 h | 12 h | 24 h | p-Value |
|---|---|---|---|---|
| Birth weight (g) | 2912.58 ± 217.04 | 3057.22 ± 311.16 | 3043.48 ± 388.03 | 0.286 |
| Apgar scores at 1 min (mean ± SD) | 7.74 ± 1.05 | 8 ± 0.74 | 7.95 ± 1.12 | 0.659 |
| Apgar scores at 5 min (mean ± SD) | 8.89 ± 0.57 | 8.87 ± 0.46 | 8.9 ± 0.3 | 0.964 |
| Variable | Univariable | Multivariable | ||||
|---|---|---|---|---|---|---|
| Beta | SE | p | Beta | SE | p | |
| Age | 0.38 | 0.27 | 0.159 | 0.34 | 0.17 | 0.051 |
| BMI | 0.44 | 0.32 | 0.173 | 0.46 | 0.23 | 0.053 |
| GA | 5.64 | 2.01 | 0.007 | 3.33 | 1.32 | 0.015 |
| Blood loss | 0.03 | 0.01 | 0.006 | 0.01 | 0.01 | 0.169 |
| Painless | 3.23 | 5.86 | 0.583 | 3.20 | 3.85 | 0.410 |
| AROM | 0.11 | 3.08 | 0.973 | 1.73 | 1.97 | 0.383 |
| Oxytocin use | 11.58 | 2.80 | 0.000 | 2.75 | 2.15 | 0.207 |
| Bishop score at Propess | −0.18 | 0.94 | 0.849 | 0.18 | 0.67 | 0.792 |
| BS after PGE2 12 h | −1.62 | 0.62 | 0.011 | 0.31 | 0.51 | 0.546 |
| BS after PGE2 24 h | −2.22 | 0.25 | <0.001 | −1.99 | 0.28 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ting, N.-S.; Wei, Y.-C.; Ding, D.-C. Timing of Prostin E2 Administration After Poor Response to Propess: Impact on Induction-to-Birth Interval and Maternal/Neonatal Outcomes. Medicina 2025, 61, 1255. https://doi.org/10.3390/medicina61071255
Ting N-S, Wei Y-C, Ding D-C. Timing of Prostin E2 Administration After Poor Response to Propess: Impact on Induction-to-Birth Interval and Maternal/Neonatal Outcomes. Medicina. 2025; 61(7):1255. https://doi.org/10.3390/medicina61071255
Chicago/Turabian StyleTing, Ning-Shiuan, Yu-Chi Wei, and Dah-Ching Ding. 2025. "Timing of Prostin E2 Administration After Poor Response to Propess: Impact on Induction-to-Birth Interval and Maternal/Neonatal Outcomes" Medicina 61, no. 7: 1255. https://doi.org/10.3390/medicina61071255
APA StyleTing, N.-S., Wei, Y.-C., & Ding, D.-C. (2025). Timing of Prostin E2 Administration After Poor Response to Propess: Impact on Induction-to-Birth Interval and Maternal/Neonatal Outcomes. Medicina, 61(7), 1255. https://doi.org/10.3390/medicina61071255