
Improved Glycemic Control through Robot-Assisted Remote Interview for Outpatients with Type 2 Diabetes: A Pilot Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Issues
2.2. Study Population
2.3. Definitions
2.4. Robot-Assisted Interview
2.5. Evaluation of Robot-Assisted Interviews by Certified Diabetes Care and Education Specialists
2.6. Assessment of Robot-Assisted Interviews with Participating Individuals with Diabetes
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kudoh, R.; Shibayama, T.; Hidaka, K. Nurses’ knowledge, attitude, and practice regarding oral management for outpatients with type 2 diabetes: A national survey on certified diabetes educators. Diabetol. Int. 2022, 13, 407–420. [Google Scholar] [CrossRef] [PubMed]
- Powers, M.A.; Bardsley, J.K.; Cypress, M.; Funnell, M.M.; Harms, D.; Hess-Fischl, A.; Hooks, B.; Isaacs, D.; Mandel, E.D.; Maryniuk, M.D.; et al. Diabetes Self-management Education and Support in Adults with Type 2 Diabetes: A Consensus Report of the American Diabetes Association, the Association of Diabetes Care and Education Specialists, the Academy of Nutrition and Dietetics, the American Academy of Family Physicians, the American Academy of PAs, the American Association of Nurse Practitioners, and the American Pharmacists Association. J. Am. Assoc. Nurse Pract. 2020, 33, 1314–1331. [Google Scholar] [PubMed]
- Rodriguez, K.; Ryan, D.; Dickinson, J.K.; Phan, V. Improving Quality Outcomes: The Value of Diabetes Care and Education Specialists. Clin. Diabetes 2022, 40, 356–365. [Google Scholar] [CrossRef] [PubMed]
- Horiguchi, T.; Inagaki, M.; Tasaki, K. The Self-Care Behaviors of Adults With Type 2 Diabetes Within 10 Years After Diagnosis: Relationship Between Self-Care Behaviors, Knowledge and Education. J. Jpn. Soc. Nurs. Res. 2021, 44, 613–622. [Google Scholar]
- Kavookjian, J.; Bzowyckyj, A.S.; DiNardo, M.M.; Kocurek, B.; Kolb, L.E.; Noe, D.; Ryan, D.; Saunders, M.M.; See, M.; Uelmen, S. Current and Emerging Trends in Diabetes Care and Education: 2021 National Practice and Workforce Survey. Sci. Diabetes Self Manag. Care 2022, 48, 307–323. [Google Scholar] [CrossRef] [PubMed]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th ed. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed]
- Iijima, K.; Arai, H.; Akishita, M.; Endo, T.; Ogasawara, K.; Kashihara, N.; Hayashi, Y.K.; Yumura, W.; Yokode, M.; Ouchi, Y. Toward the development of a vibrant, super-aged society: The future of medicine and society in Japan. Geriatr. Gerontol. Int. 2021, 21, 601–613. [Google Scholar] [CrossRef] [PubMed]
- Blanson Henkemans, O.A.; Bierman, B.P.; Janssen, J.; Neerincx, M.A.; Looije, R.; van der Bosch, H.; van der Giessen, J.A. Using a robot to personalise health education for children with diabetes type 1: A pilot study. Patient Educ. Couns. 2013, 92, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Henkemans, O.A.B.; Bierman, B.P.B.; Janssen, J.; Looije, R.; Neerincx, M.A.; van Dooren, M.M.M.; de Vries, J.L.E.; van der Burg, G.J.; Huisman, S.D. Design and evaluation of a personal robot playing a self-management education game with children with diabetes type 1. Int. J. Hum. Comput. Stud. 2017, 106, 63–76. [Google Scholar] [CrossRef]
- Lau, Y.; Chee, D.G.H.; Chow, X.P.; Wong, S.H.; Cheng, L.J.; Lau, S.T. Humanoid robot-assisted interventions among children with diabetes: A systematic scoping review. Int. J. Nurs. Stud. 2020, 111, 103749. [Google Scholar] [CrossRef] [PubMed]
- Araki, E.; Goto, A.; Kondo, T.; Noda, M.; Noto, H.; Origasa, H.; Osawa, H.; Taguchi, A.; Tanizawa, Y.; Tobe, K.; et al. Japanese Clinical Practice Guideline for Diabetes 2019. Diabetol Int. 2020, 11, 165–223. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Professional Practice, C. 2. Diagnosis and Classification of Diabetes: Standards of Care in Diabetes-2024. Diabetes Care 2024, 47, S20–S42. [Google Scholar] [CrossRef] [PubMed]
- Maalouly, E.; Hirano, T.; Yamazaki, R.; Nishio, S.; Ishiguro, H. Encouraging prosocial behavior from older adults through robot teleoperation: A feasibility study. Front. Comput. Sci. 2023, 5, 1157925. [Google Scholar] [CrossRef]
- Available online: https://cocorostore.sharp.co.jp/robohon/ (accessed on 1 January 2024). (In Japanese).
- Japan Diabetes Clinical Data Management Study Group (JDDM). 2023. Available online: http://jddm.jp/public-information/index-2022/#data_03 (accessed on 1 January 2024).
- Available online: https://www.jpn-geriat-soc.or.jp/publications/other/diabetes_treatment_guideline.html (accessed on 1 January 2024). (In Japanese).
- Fan, J.; Ullal, A.; Beuscher, L.; Mion, L.C.; Newhouse, P.; Sarkar, N. Field Testing of Ro-Tri, a Robot-Mediated Triadic Interaction for Older Adults. Int. J. Soc. Robot. 2021, 13, 1711–1727. [Google Scholar] [CrossRef] [PubMed]
- Damholdt, M.F.; Norskov, M.; Yamazaki, R.; Hakli, R.; Hansen, C.V.; Vestergaard, C.; Seibt, J. Attitudinal Change in Elderly Citizens Toward Social Robots: The Role of Personality Traits and Beliefs About Robot Functionality. Front. Psychol. 2015, 6, 1701. [Google Scholar] [CrossRef] [PubMed]
- Nishio, T.; Yoshikawa, Y.; Sakai, K.; Iio, T.; Chiba, M.; Asami, T.; Isoda, Y.; Ishiguro, H. The Effects of Physically Embodied Multiple Conversation Robots on the Elderly. Front. Robot. AI 2021, 8, 633045. [Google Scholar] [CrossRef] [PubMed]
- Fasola, J.; Mataric, M.J. Using Socially Assistive Human–Robot Interaction to Motivate Physical Exercise for Older Adults. Proc. IEEE 2012, 100, 2512–2526. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category 1: Functional quality of RoBoHoN-mediated interview | |
| QC-01 | Did RoBoHoN speak clearly? |
| QC-02 | Did RoBoHoN speak at an appropriate speed to be understood? |
| QC-03 | Do you feel satisfied that you have told RoBoHoN what you wanted to say? |
| QC-04 | Did RoBoHoN ask questions in timely and in natural? |
| QC-05 | Were RoBoHoN’s questions difficult to understand? |
| QC-06 | Did RoBoHoN reply in a natural time? |
| QC-07 | Was RoBoHoN’s response natural? |
| Category 2: Impression of RoBoHoN | |
| QC-08 | Was RoBoHoN cute? |
| QC-09 | Did you feel afraid of RoBoHoN (scary, cold, etc.)? |
| QC-10 | Did you feel attached to RoBoHoN while talking with him? |
| QC-11 | Did you feel familiar with the way RoBoHoN speaks? |
| QC-12 | Did you want to talk more with RoBoHoN? |
| Category 3: Advantages of RoBoHoN-mediated interviews over usual CDCESs’ | |
| QC-13 | Did you feel more comfortable talking to RoBoHoN than to a medical professional? |
| QC-14 | Was it easier to talk about difficult things with RoBoHoN than with a medical professional? |
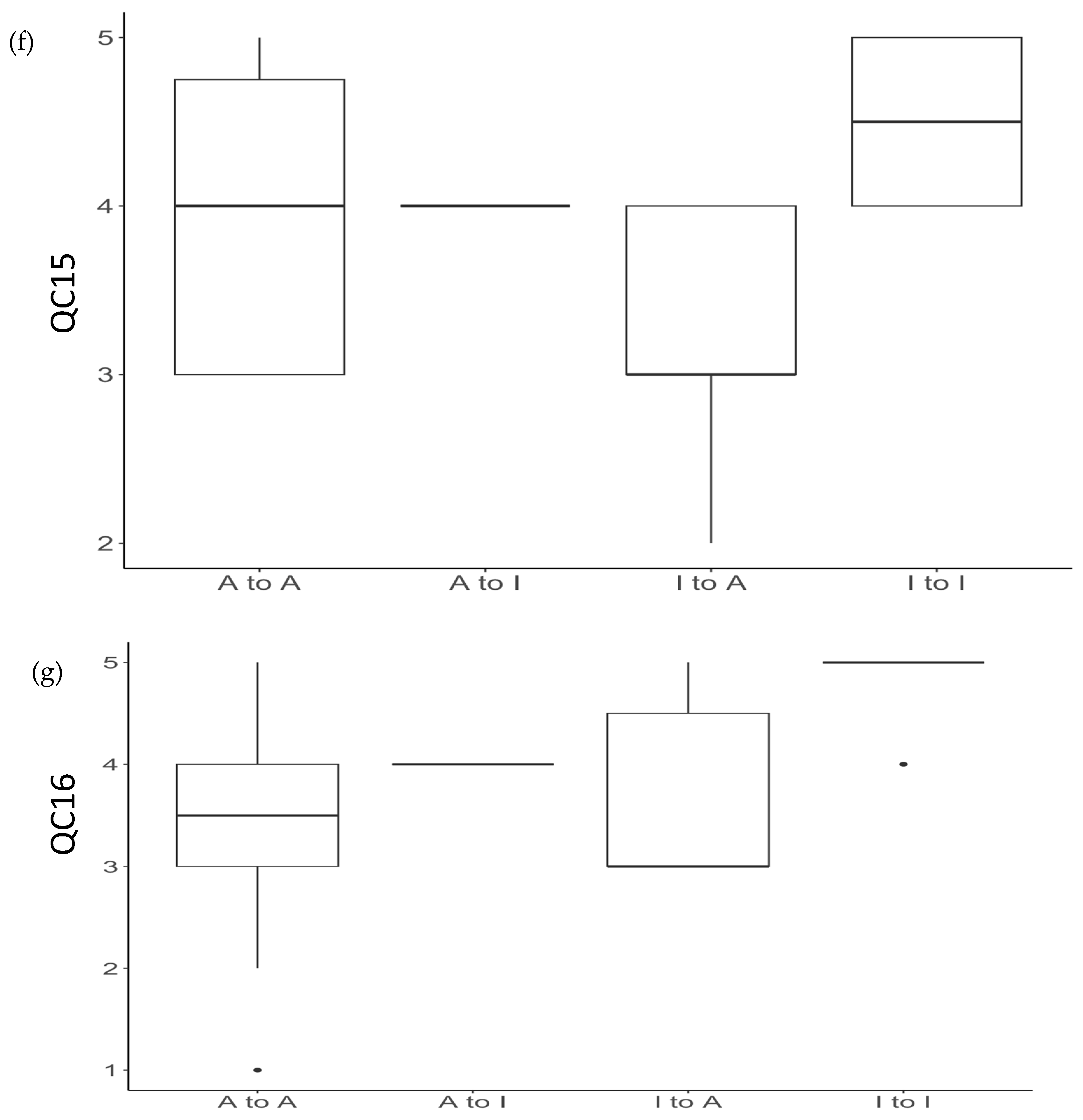
| QC-15 | Did you feel more pressure of tested when talking to a RoBoHoN than when communicating with a medical professional? |
| QC-16 | Did you feel uncomfortable discussing personal matters because of RoBoHoN’s childish way of speaking? |
| QC-17 | Did you feel that coming to the clinic was more fun? |
| Category 4: RoBoHoN’s effect on reflection on diabetes self-care | |
| QC-18 | Did your conversation with RoBoHoN make you reflect on your own knowledge about diabetes? |
| QC-19 | Did your conversation with RoBoHoN give you an opportunity to reflect on your own diet and eating habits regarding diabetes? |
| QC-20 | Did your conversation with RoBoHoN give you an opportunity to reflect on your own activity level and exercise habits regarding diabetes? |
| QC-21 | Did your conversation with RoBoHoN cause you to reflect on medications (oral medications and insulin) in relation to diabetes? |
| QC-22 | Did your conversation with RoBoHoN cause you to reflect over your glycemic management? |
| Characteristics | Variables |
|---|---|
| Number of subjects | 28 |
| Age, years old | 69.5 ± 12.7, 70.5 [63.75, 79.25] |
| Gender (Male/Female) | 20/8 |
| HbA1c (0M), % | 7.06 ± 0.69, 7.1 [6.75, 7.45] |
| HbA1c (2M), % | 6.86 ± 0.62, 6.9 [6.675, 7.125] |
| ΔHbA1c, % | −0.19 ± 0.29, −0.2 [−0.4, 0] |
| Glycemic control (0M) Adequate/Inadequate | 15/13 |
| Glycemic control (2M) Adequate/Inadequate | 21/7 |
| BMI, Kg/m2 | 24.9 ± 4.9, 24.2 [22.25, 27.4] |
| Number of diabetes medications | 2.1 ± 1.1, 2 [1,3] |
| Subjects with diabetic complications | 5 |
| Treated with insulin injections | 3 (11%) |
| Treated with GLP-1 analog injections | 7 (25%) |
| Treated with biguanide | 7 (25%) |
| Treated with sulfonylureas and glinides | 10 (36%) |
| Treated with SGLT2 inhibitors | 18 (64%) |
| Treated with DPP-4 inhibitors | 16 (57%) |
| Treated with thiazolidine | 3 (11%) |
| Treated with imeglimin | 3 (11%) |
| Grade of diabetes care behavior (6–18) | 9.50 [8.00, 12.00] |
| Understanding of diabetes therapy (3–9) | 4.00 [3.75, 5.00] |
| Acceptance of diabetes (3–6) | 4.00 [4.00, 5.00] |
| Effectiveness of Robot interview (2–4) | 4.00 [4.00, 4.00] |
| QC-01 (1–5) | 5.00 [4.00, 5.00] |
| QC-02 (1–5) | 5.00 [4.00, 5.00] |
| QC-03 (1–5) | 4.00 [4.00, 5.00] |
| QC-04 (1–5) | 4.00 [3.75, 5.00] |
| QC-05 (1–5) | 3.00 [3.00, 4.00] |
| QC-06 (1–5) | 4.00 [3.00, 5.00] |
| QC-07 (1–5) | 4.00 [3.00, 5.00] |
| QC-08 (1–5) | 4.00 [3.75, 5.00] |
| QC-09 (1–5) | 5.00 [4.00, 5.00] |
| QC-10 (1–5) | 3.00 [3.00, 4.00] |
| QC-11 (1–5) | 4.00 [3.00, 5.00] |
| QC-12 (1–5) | 3.00 [3.00, 4.00] |
| QC-13 (1–5) | 3.00 [3.00, 4.00] |
| QC-14 (1–5) | 3.00 [3.00, 4.00] |
| QC-15 (1–5) | 4.00 [3.00, 4.25] |
| QC-16 (1–5) | 4.00 [3.00, 5.00] |
| QC-17 (1–5) | 3.00 [2.75, 3.00] |
| QC-18 (1–5) | 4.00 [3.00, 4.00] |
| QC-19 (1–5) | 4.00 [3.00, 5.00] |
| QC-20 (1–5) | 4.00 [3.00, 4.25] |
| QC-21 (1–5) | 3.00 [3.00, 4.00] |
| QC-22 (1–5) | 4.00 [3.00, 5.00] |
| Adequate GMS after 2 Months | Inadequate GMS after 2 Months | |
|---|---|---|
| Adequate GMS at baseline | 14 | 1 |
| Inadequate GMS at baseline | 7 | 6 |
| Adequate to Adequate | Inadequate to Adequate | Inadequate and Adequate to Inadequate | Kruskal–Wallis Analyses among 3 Groups (p-Value) | |
|---|---|---|---|---|
| Number of subjects | 14 | 7 | 7 | |
| Age, years old | 70.50 [62.00, 79.25] | 71.00 [64.00, 73.50] | 69.00 [65.50, 79.50] | 0.958 |
| Gender (M/F) | 10/4 | 6/1 | 4/3 | 0.497 |
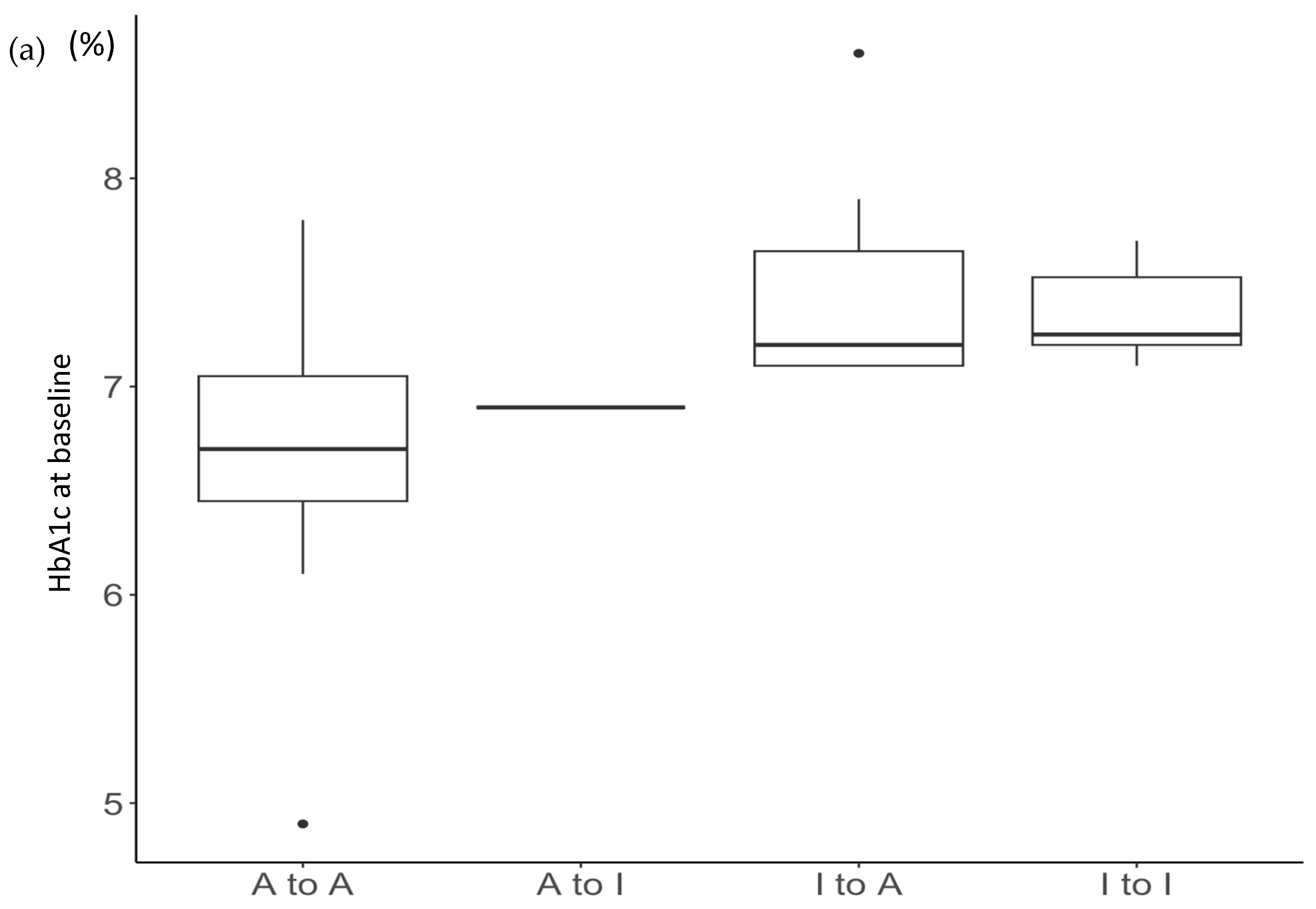
| HbA1c (0M), % | 6.70 [6.45, 7.05] | 7.20 [7.10, 7.65] | 7.20 [7.15, 7.45] | 0.022 |
| HbA1c (2M), % | 6.70 [6.32, 6.97] | 6.90 [6.80, 7.05] | 7.10 [7.10, 7.30] | 0.020 |
| ΔHbA1c, % | −0.15 [−0.27, −0.03] | −0.50 [−0.55, −0.30] | 0.00 [−0.15, 0.20] | 0.016 |
| BMI | 24.25 [23.10, 26.65] | 26.20 [23.25, 28.95] | 22.30 [20.75, 23.85] | 0.286 |
| Number of diabetes medications | 2.00 [1.00, 2.75] | 2.00 [2.00, 3.00] | 2.00 [1.00, 2.50] | 0.536 |
| Subjects with diabetic complications | 4 | 0 | 1 | 0.262 |
| Grade of diabetes care behavior (6–18) | 10.00 [7.50, 11.75] | 10.00 [9.00, 12.50] | 8.00 [8.00, 9.00] | 0.264 |
| Understanding of diabetes therapy (3–9) | 4.00 [3.00, 4.00] | 4.00 [4.00, 5.50] | 4.00 [4.00, 4.50] | 0.440 |
| Acceptance of diabetes (3–6) | 4.00 [4.00, 5.00] | 5.00 [4.00, 5.00] | 4.00 [3.50, 4.00] | 0.104 |
| Effectiveness of Robot interview (2–4) | 4.00 [4.00, 4.00] | 4.00 [4.00, 4.00] | 4.00 [3.50, 4.00] | 0.357 |
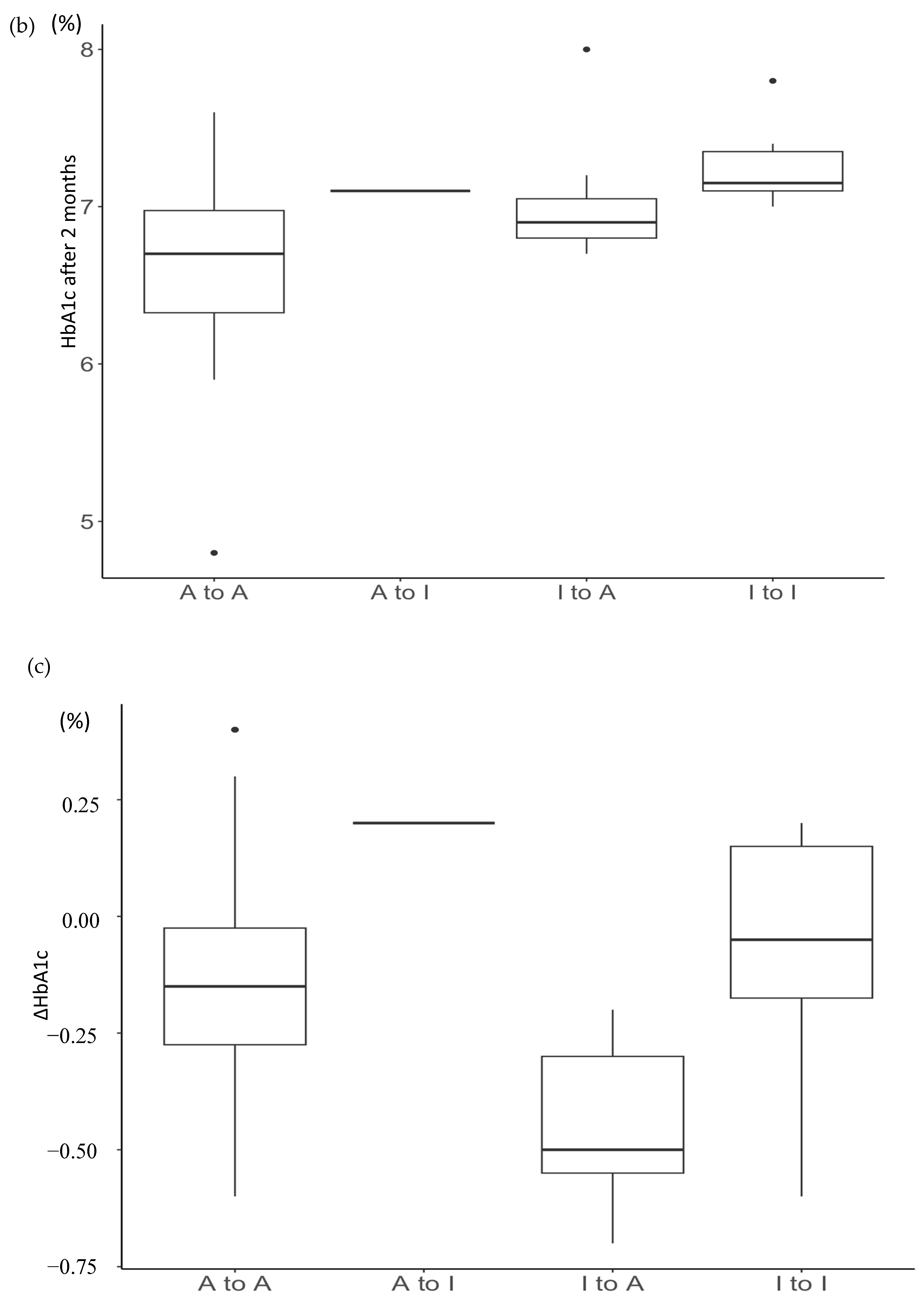
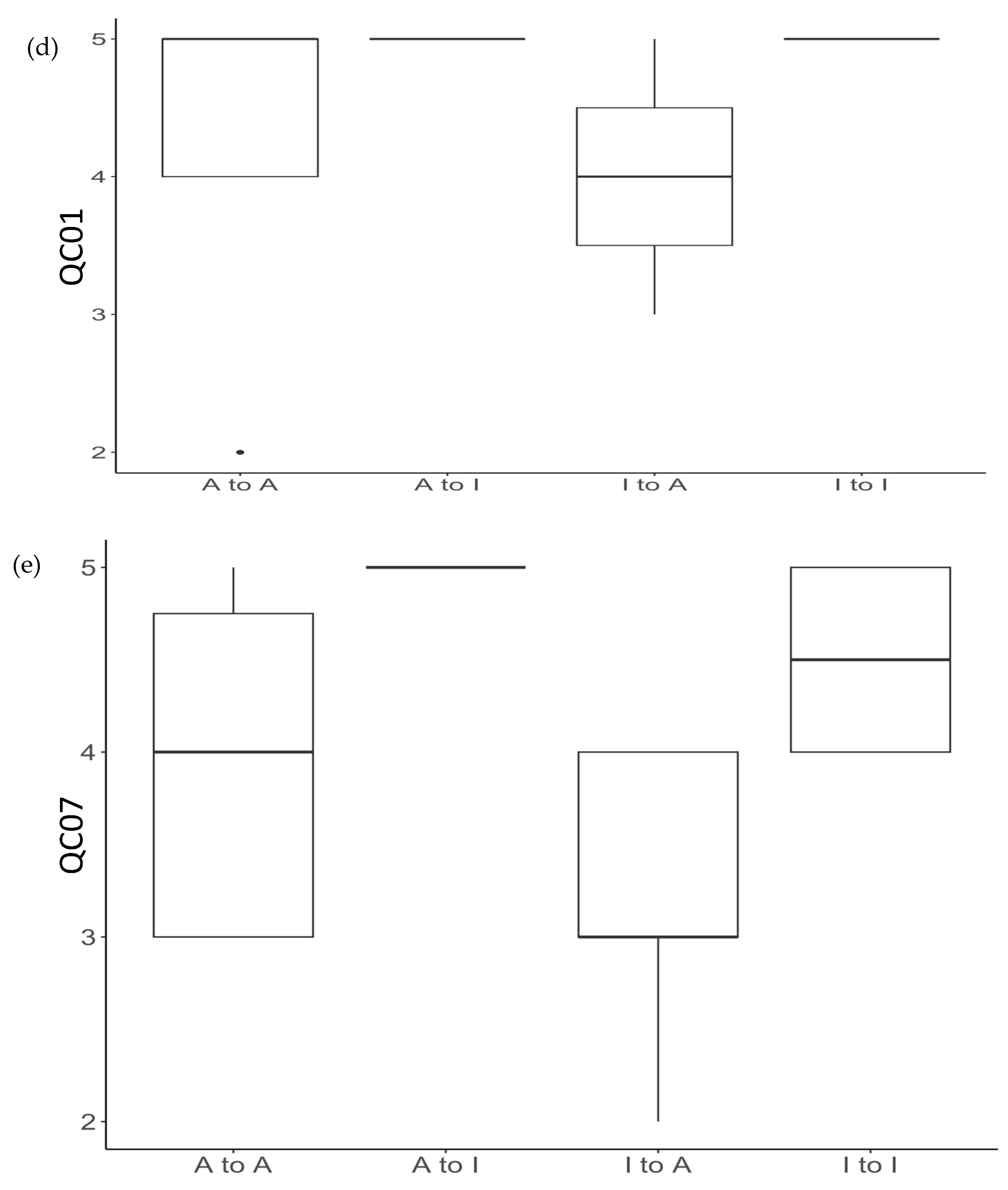
| QC-01 (1–5) | 5.00 [4.00, 5.00] | 4.00 [3.50, 4.50] | 5.00 [5.00, 5.00] | 0.024 |
| QC-02 (1–5) | 5.00 [4.00, 5.00] | 4.50 [4.00, 5.00] | 5.00 [5.00, 5.00] | 0.166 |
| QC-03 (1–5) | 4.50 [4.00, 5.00] | 4.00 [3.00, 4.00] | 5.00 [4.50, 5.00] | 0.057 |
| QC-04 (1–5) | 4.00 [4.00, 4.00] | 3.50 [3.00, 4.50] | 5.00 [4.50, 5.00] | 0.120 |
| QC-05 (1–5) | 3.50 [3.00, 4.00] | 3.00 [3.00, 3.00] | 4.00 [3.50, 4.50] | 0.333 |
| QC-06 (1–5) | 4.00 [3.00, 4.75] | 3.00 [3.00, 4.00] | 4.00 [4.00, 5.00] | 0.260 |
| QC-07 (1–5) | 4.00 [3.00, 4.75] | 3.00 [3.00, 4.00] | 5.00 [4.00, 5.00] | 0.022 |
| QC-08 (1–5) | 4.00 [3.00, 5.00] | 4.50 [4.00, 5.00] | 5.00 [4.00, 5.00] | 0.400 |
| QC-09 (1–5) | 4.50 [4.00, 5.00] | 4.00 [3.50, 5.00] | 5.00 [4.50, 5.00] | 0.404 |
| QC-10 (1–5) | 3.00 [2.25, 4.00] | 3.00 [3.00, 3.00] | 3.00 [3.00, 5.00] | 0.355 |
| QC-11 (1–5) | 4.00 [3.00, 4.75] | 4.00 [3.00, 4.00] | 4.00 [4.00, 5.00] | 0.209 |
| QC-12 (1–5) | 3.00 [3.00, 3.75] | 3.00 [3.00, 3.50] | 3.00 [2.50, 4.00] | 0.947 |
| QC-13 (1–5) | 3.00 [3.00, 3.00] | 3.00 [3.00, 3.50] | 3.00 [2.50, 4.00] | 0.973 |
| QC-14 (1–5) | 3.00 [3.00, 3.75] | 3.00 [3.00, 4.00] | 3.00 [2.50, 4.00] | 0.612 |
| QC-15 (1–5) | 4.00 [3.00, 4.75] | 3.00 [3.00, 4.00] | 4.00 [4.00, 5.00] | 0.041 |
| QC-16 (1–5) | 3.50 [3.00, 4.00] | 3.00 [3.00, 4.50] | 5.00 [4.50, 5.00] | 0.037 |
| QC-17 (1–5) | 3.00 [2.25, 3.00] | 3.00 [3.00, 3.00] | 3.00 [2.00, 3.00] | 0.506 |
| QC-18 (1–5) | 4.00 [3.00, 4.00] | 4.00 [3.50, 4.00] | 4.00 [4.00, 4.50] | 0.357 |
| QC-19 (1–5) | 3.50 [3.00, 4.00] | 4.00 [3.00, 4.50] | 4.00 [3.50, 5.00] | 0.735 |
| QC-20 (1–5) | 3.00 [3.00, 4.00] | 4.00 [3.50, 4.00] | 5.00 [4.00, 5.00] | 0.138 |
| QC-21 (1–5) | 3.00 [3.00, 4.00] | 3.00 [3.00, 4.00] | 4.00 [3.00, 4.50] | 0.740 |
| QC-22 (1–5) | 3.50 [3.00, 4.00] | 4.00 [4.00, 5.00] | 4.00 [4.00, 5.00] | 0.126 |
| Independent Variables | Coefficient | SE | p-Value |
|---|---|---|---|
| HbA1c (0M), % | −0.05219 | 0.18283 | 0.7780 |
| QC01 | −0.36472 | 0.15504 | 0.0280 |
| QC07 | −0.35337 | 0.16189 | 0.0400 |
| QC15 | −0.28527 | 0.20757 | 0.1832 |
| QC16 | 0.03855 | 0.14311 | 0.7901 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yagi, K.; Inagaki, M.; Asada, Y.; Komatsu, M.; Ogawa, F.; Horiguchi, T.; Yamaaki, N.; Shikida, M.; Origasa, H.; Nishio, S. Improved Glycemic Control through Robot-Assisted Remote Interview for Outpatients with Type 2 Diabetes: A Pilot Study. Medicina 2024, 60, 329. https://doi.org/10.3390/medicina60020329
Yagi K, Inagaki M, Asada Y, Komatsu M, Ogawa F, Horiguchi T, Yamaaki N, Shikida M, Origasa H, Nishio S. Improved Glycemic Control through Robot-Assisted Remote Interview for Outpatients with Type 2 Diabetes: A Pilot Study. Medicina. 2024; 60(2):329. https://doi.org/10.3390/medicina60020329
Chicago/Turabian StyleYagi, Kunimasa, Michiko Inagaki, Yuya Asada, Mako Komatsu, Fuka Ogawa, Tomomi Horiguchi, Naoto Yamaaki, Mikifumi Shikida, Hideki Origasa, and Shuichi Nishio. 2024. "Improved Glycemic Control through Robot-Assisted Remote Interview for Outpatients with Type 2 Diabetes: A Pilot Study" Medicina 60, no. 2: 329. https://doi.org/10.3390/medicina60020329
APA StyleYagi, K., Inagaki, M., Asada, Y., Komatsu, M., Ogawa, F., Horiguchi, T., Yamaaki, N., Shikida, M., Origasa, H., & Nishio, S. (2024). Improved Glycemic Control through Robot-Assisted Remote Interview for Outpatients with Type 2 Diabetes: A Pilot Study. Medicina, 60(2), 329. https://doi.org/10.3390/medicina60020329